Embed Size (px)
Citation preview
Treatment of Surgical Site Infection Meeting Quality Statement 6
Prof Peter Wilson
University College London Hospitals

TEG Quality Standard 6
Treatment and effective antibiotic prescribing: People with a surgical site infection are offered treatment with an antibiotic that covers the likely causative organisms and is selected based on local resistance patterns and the results of microbiological tests.
Monitoring progress against the standard

Surgical site infection
Substantial burden on health care
Hospital stay doubled: £65 million/year in UK
Surgical site infection used as a performance indicator
League tables but rates very dependent on post discharge follow up

Monitoring compliance
Evidence of antibiotic treatment covering the likely pathogens chosen on local resistance and clinical sample results
Measure number appropriate choice / total surgical site infections
Surveillance nurse, antimicrobial stewardship round, medical liaison

Monitoring Impact
Length of stay
Antibiotics
District nurse visits
ICU, HDU, ward stay
Local anaesthetic drainage
General anaesthesia drainage
Wound dressing

Pathogens
Staphylococcus aureus
Coagulase negative staphylococci
Coryneforms
Streptococcus group A
Coliforms
Pseudomonas spp.
Anaerobes
Candida spp.

Effect of pathogens
Each species of pathogen has a different effect on wound infection
Host susceptibility important
Assessment of the wound important in diagnosis, treatment and audit
Treatment of infection determined by the likely pathogen

Host factors
Category of wound
Presence of prosthesis or drain
Prolonged surgery
End of operation list
Surgeon
Aseptic technique
Preoperative stay

Host factors
Carriage of S. aureus
Old age
Chronic illness
Steroid therapy
Obesity
Diabetes
Mechanical breakdown of wound

Oct –Dec 2012 UCLH
In 737/931 (79%) of operations surveyed patients were contacted at one month
26% ASEPSIS >10 (abnormal wound)
8.8% ASEPSIS >20 (infection)
6.8% CDC defined wound infection
54% of infections detected post discharge only

Antibiotics
Prophylaxis 1 dose or 24h – no benefit beyond 4 h post surgery
Increasing ESBL so meropenem usage doubling every year
High dose short duration
Quickly isolate patients with diarrhoea

Treatment
Dressings – keep the wound clean
Topical application – sugar paste, irrigation, vacuum dressing
Surgical drainage of pus
Debridement
Antibiotics
Take care with urgency of treatment

Staphylococcus aureus
Localised purulent infection
Flucloxacillin, teicoplanin, vancomycin
Drain any abscess
Alginates, hydrocolloids, sugar paste
Avoid packing of wound

Streptococcus group A
Spreading cellulitis - little pus
Necrotizing fasciitis: urgent surgical debridement + high dose penicillin
Cellulitis: benzyl penicillin or clindamycin
All wounds covered and kept dry

Coagulase negative staphylococci
Can be similar to S. aureus infection
Remove any prosthetic material or sutures if possible
Teicoplanin or vancomycin
Rifampicin may penetrate biofilm
Alginates, hydrocolloids, sugar paste

Coliforms
Necrotic wound - cleaning most important
Alginates, sugar paste
Mechanical debridement
Correct leaking anastomosis
Antibiotics less important - cefuroxime, ceftazidime, piptazobactam

Pseudomonas aeruginosa
Abdominal wounds, burns or ulcers
Cleaning or debridement of the wound
Avoid topical antibiotics
Hydrocolloids
Enzyme treatments if necrotic
Antibiotics rarely indicated

Anaerobes
Usually mixed with coliforms
Exposure to air - debridement important
Alginates, sugar paste
Correction of bowel leakage
Metronidazole or clindamycin

Topical
Do not treat bacterial colonisation
Irrigants not tested in trials
Sugar paste sterile, does not harm granulation tissue

SSI Prevention Care Bundle
MRSA screening & decontamination
2% chlorhexidine
Antibiotic prophylaxis
Hair removal not shaving
Glucose control
Maintain body temperature
Optimise closure methods
Wound charts
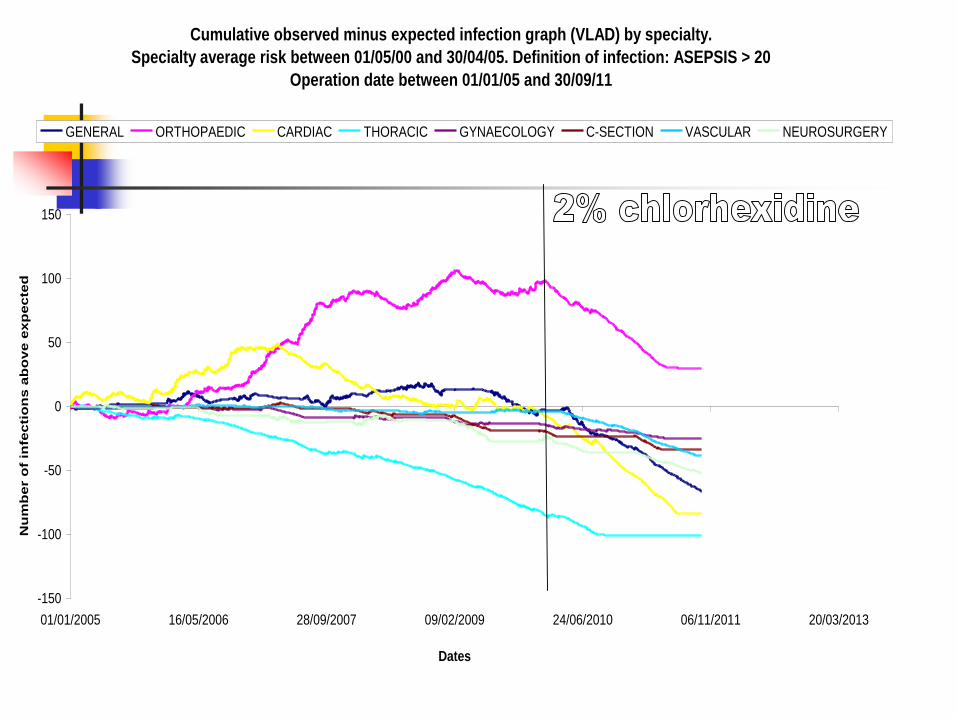
Cumulative observed minus expected infection graph (VLAD) by specialty.
Specialty average risk between 01/05/00 and 30/04/05. Definition of infection: ASEPSIS > 20
Operation date between 01/01/05 and 30/09/11
-150
-100
-50
0
50
100
150
01/01/2005 16/05/2006 28/09/2007 09/02/2009 24/06/2010 06/11/2011 20/03/2013
Dates
Nu
mb
er o
f in
fec
tio
ns
ab
ov
e e
xp
ec
ted
GENERAL ORTHOPAEDIC CARDIAC THORACIC GYNAECOLOGY C-SECTION VASCULAR NEUROSURGERY

Preoperative nasal mupirocin
ICHE 2012 33 152
Two stage revision surgery for infected joint costs $100,000
Culture $96, mupirocin 5 day $6
26% S aureus carriage, screening 85%
Empirical treatment with mupirocin and no screening cheapest
Screen vs treat all both cost effective vs no treatment

Remember If Streptococcus pyogenes suspected:
no pus, spreading infection, act very quickly, get a Gram stain of discharge
Staphylococcal infections must be drained of pus
Pseudomonal infections are often colonization and do not need antibiotic treatment

Conclusion
Skin preparation, body temperature, glucose control, antibiotic prophylaxis
In patient infection much more costly but outpatient infection more common





























