Embed Size (px)
Citation preview

Pédiatrie Dentistry
Treatment of posterior crossbite in the primary and early mixeddentitionsPeter W, Ngan* / Stephen H. Y, Wei**
This paper presents the etiology and rationale for early correction of posterior cross-bites in the primary and early mixed dentitions. Six cases have been selected to demon-strate the principles and philosophy of various treatment modalities so that practition-ers wilt be able to recognize and understand the etiology of crossbite conditions and toformulate an approach for ihe diagnosis and the best method of treatment for the cor-rection of posterior crossbite in the young child. ('Quintessence Int 1990:21:451-459.)
Introduction
The diagnosis and treatment of posterior crossbite hasbeen extensively reviewed in the literature,' ' This pa-per describes six patients who required early ortho-dontie eorrection of posterior erosshites in the pri-mary and early mixed dentitions. These cases havebeen seleeted to demonstrate the principies and phi-losophies of various treatment modalities so that prac-titioners will be able to reeognize and understand theetiology of crossbite conditions and to formulate anapproach for the diagnosis and select the best methodsof treatment for the correction of posterior crossbilcin the young child.
Rationale for early correction of posterior crossbites
Most of the literature supports an early correction ofprimary crossbites in the primary dentition,'"^ For ex-ample, a longitudinal study by Kutin and Hawes'
* Assistant Professor, Department of Orthodontics, Ohio StateUniversity, College of Dentistry, Postie Hall, 305 West t2thAvenue, Columbus, Ohio 43210-1241,
** Professor and Head, Deparlmenl of Children's Dentistry andOrthodontics, Dean, Faculty of Dentistry, University of HongKong, Prince Philip Dental Hospital, 34 Hospital Road, HongKong.
Address aii correspondence to Professor Stephen H, Y. Wei,
studied the early treatment of posterior crossbites inthe primary dentition over several years. They foundthat 44 of 48 first permanent molars erupted in thesame crossbite relationship as did the untreated pri-mary molars. The premoiars in uncorrected crossbitecases also erupted in the same erossbite relationshipas did their primary counterparts. In eontrast, the pre-moiars and permanent molars in the corrected casesail erupted into a normal relationship, Kutin andHawes'' eoncluded that the early correction of poste-rior crossbites in the primary dentition is indicated,because crossbites do not automatically improve withthe eruption of the permanent teeth.
In a study by Schroder and Schroder' on early treat-ment of unilateral posterior erosshite in the primarydentition, 27 of the 32 patients showed normal trans-verse relations between the first permanent molars,Schroder and Schroder' eoncluded that the earlier thecorrective treatment is instituted, the higher will hethe frequency of normal transverse first molar rela-tionships in the permanent dentitions,
A crossbite that is accompanied by a mandibularshift should usually be corrected as soon as it is dis-covered. An uncorrected mandibular shift can produceundesirable growth modifications and dental compen-sations leading to a permanent deviation and crani-ofacial asymmetry at a later time, as well as potentiallyharmful functional masticatory patterns,' The func-tional matrix theory of facial bone development in-dieates that the tensions and pressures of the envelopeof soft tissues surrounding the developing, malleable,immature facial bones actually help shape these
Qu inlespence -intérnatioiTâl Volume 2Í^[^]^umber 6/1990 451

Pédiatrie Dentistry
Fig 1 A 57-year-oid patient with s unilateral posteriorcrossbite and a mandibular shift that was not corrected ata younger age. Stie now presents with grossly asymmetricmandible.
bones.^ Therefore, if abiionnal tetisions and pressuresofthe masticatory and other facial muscles are apphedto the dentofacial hony complex for a long period oftime, such as in the case of an untreated posteriorcrossbite, the symmetry of the face of the child can bealtered significantly beyond the range of what is ac-cepted as normal. According to Thilander,' forced lat-eral and anterior crossbites cause asymmetric muscleactivity and muscular hyperactivity on the crossbiteside. Muscle hyperactivities have been shown to influ-ence the morphology of the developing temporoman-dibular joint, Epidemiologic studies have also shownthat crossbites are often associated with increasingpresence of condylar deviation,'° a significantly higherprevalence of joint sounds is found in older childrenwith buccal crossbites than in those with normal oc-clusion." Figure 1 shows an example ofa 57-year-oldpatient with a severe posterior crossbite and a markedmandibular shift and facial asymmetry as a result oflack of early correction and treatment.
Etiology of po.-iierior crossbite
Few malocclusions can be traced to a single specificcause. Malocclusion is the result ofthe interaction of
many factors affecting a developing sy í̂em '̂ hat hasiti, own growth pattern. According Kt Moyers, thereare three different types of crossbites to be considered,namely, dental, mtiscular, and ossentts. Dental cross-bites involve only the tipping of teeth, while muscularcrossbites involve muscular alterations caused bytooth interferences, and osseous crossbites are relatedto skeletal disharmonies.
The diagnosis, treatment and retention of posteriorcrossbite in six patients will be presented according tothe etiology of the problem. Figure 2 describes the sixpossible combinations of posterior crossbite molar re-lationships.'^
Case 1
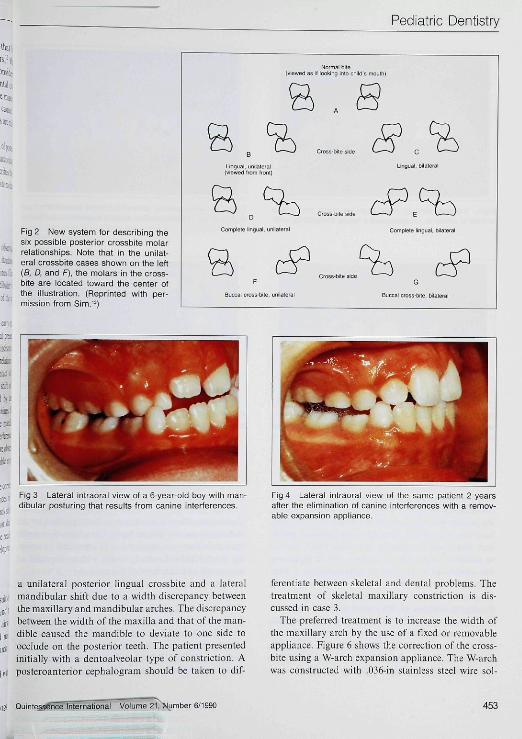
The simplest form of posterior crossbite observed inthe primary dentition or the early mixed dentition iscaused by interferences ofthe primary canines. Canineinterferences can lead to a lateral mandibular shiftand, in some cases, a forward posturing of the tnan-dible.
Figure 3 shows a 6-year-old boy with an early mixeddentition. In centric occlusion, the patient presentedwith an anterior crossbite ofthe maxillary incisors anda Class Til molar relationship. In centric relation clo-sure, the patient exhibited an initial contact of theprimary canines followed by an anterior shift of themandible. This problem can be treated by initialgrinding or equilibration of the primary canines. If nocorrection results, then expansion of the maxillaryarch is needed to eliminate the canine interferences.'*Figure 4 shows the clinical changes that were observed2 years following treatment with a removable expan-sion appliance.
Although some of these crossbites can be correctedsimply by eliminating the canine interferences or bymaxillary expansion, proper diagnostic records shouldbe taken to ensttre that the crossbites are not due toa skeletal dysplasia. These patients should be recalledperiodically to monitor their growth and development.
Case 2
Bilateral maxillary constriction may be the result of avariety of etiologic factors, including finger and pa-cifier sucking, cheek biting, compromised nasal airwayfrom enlarged adenoid, tonsils, or a deviated nasalseptum, as well as medically related problems such asallergies, asthma, or chronic sinusitis.
Figure 5 shows a 5-year-old boy who pri_-î,ci-ited with
452 Qu i ntes senca6/1990
Pédiatrie Dentistry
Fig 2 New system for describing thesix possible posterior erossbite molarrelationships. Note ttiat in the unilat-eral crossbite eases shown on ttie left(S. D, and F), the molars in the cross-bite are located toward the center otthe illustration, (Reprinted with per-tnission trom Sitn."l
«d IS il loiKIng Inio child's iroulh)
CrDss-BltE sidQ
Cioss.bita sideu
Complete lingual, unilaierel Complete lingual, bilarei
Buccal crcs^-bile. unila(era
G
is-bile. bilatBi
Fig 3 Lateral intraoral view of a 6-year-old boy with man-dibular posturing that results from canine interferences.
Fig 4 Lateral intraoral view of ttie same patient 2 yearsatter the elimination of canine interferences with a remov-able expansion appliance.
a nnilateral posterior lingual crossbite and a lateralmandibular shift due to a width discrepancy betweenthe maxillary and mandibular arches. The discrepancybetween the width ofthe maxilla and that ofthe man-dible caused the mandible to deviate to one side toocclude on the posterior teeth. The patient presentedinitially with a dentoalveolar type of constriction. Aposteroanterior cephalogram should be taken to dif-
ferentiate between skeletal and dental problems. Thetreatment of skeletal maxillary constriction is dis-cussed in case 3.
The preferred treatment is to increase the width ofthe maxiliary arch by the use of a fixed or removableappliance. Figure 6 shows the correction of the cross-bite using a W-arch expansion appliance. The W-archwas constructed with .036-in stainless steel wire sol-
Quinte^séncé International Volume 21?>tjjtnber 6/1990 453
Pédiatrie Dentistry
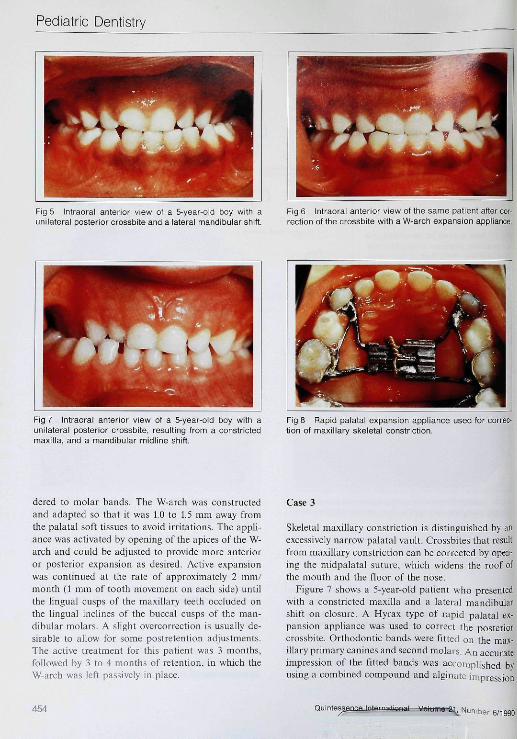
Fig 5 Intraoral anterior view of a 5-year-old boy with aunilateral posterior crossbite and a lateral mandibular shift.
Fig 6 Intraoral anterior view of the same patient after cor-rection of ttie crossbite with a W-arch expansion appliance.
Fig 7 intraoral anterior view of a 5-year-oid boy with aunilateral posterior crossbite, resulting from a constrictedmaxilla, and a mandibular midline shift.
Fig 8 Rapid palatal expansion appiiance used for correc-tion of maxillary skeietal constriction.
deied to molar bands. The W-arch was constructedand adapted so that it was 1.0 to L5 mm away fromthe palatal .soft tissues to avoid irritations. The appli-ance was activated by opening of the apices of the W-arch and could be adjusted to provide more anterioror posterior expansion as desired. Active expansionwas continued at the rate of approximately 2 mm./month {1 mm of tooth movement on each side) untilthe lingual cusps of the maxillary teeth occluded onthe hngual inclines of the buccal cusps of the man-dibular molars. A shght overeorrection is usually de-sirable to allow for some postretention adjustments.The active treatment for this patient was 3 months,followed by 3 to 4 months of retention, in which theW-arch was left passively in place.
Case 3
Skeletal maxillary constriction is distinguished hy anexcessively narrow palatal vault. Crossbites that resultfrom maxillary constriction can be corrected by open-ing the midpalatal suture, which widens the roof ofthe mouth and the floor of the nose.
Figure 7 shows a 5-year-old patient who presentedwith a constricted maxilla and a lateral mandibuiarshift on closure. A Hyrax type of rapid palatal ex-pansion appliance was used to correct the posteriorcrossbite. Orthodontic bands were fitted on the max-illary primary canines and second molars. An accurateimpression of the fitted bands was accomplished byusing a combined compound and algiaaie impression
454 6/1990

Pédiatrie Dentistry
Fig 9 intraoral anterior view ot a &-year-old boy with aunilateral posterior crossbite eorrected witti a rapid paiatalexpansion applianee. Note the midline diastema formed byskeletal expansion.
Fig 10 Intraorai anterior view ot a 5-year-old girl witti auniiateral buccai posterior crossbite.
technique. The impression compound gave a positiveseating of the orthodontic bands m the impression,whereas the alginate material gave an accurate impres-sion of the palatai soft tissues. The appliance wasactivated twice daily (0.25 mm per tum) by the patient(Fig 8).
The treating dentist should make absolutely certainthat the amount and the area of expansion needed areboth confirmed by measurements. The expansion pro-ceeds faster and to a greater extent at the anteriorportion of the palate due to the buttressing effect ofthe other maxillary structures in the posterior region,';.A large diastema usually appears between the centralineisors as the bones separate in this area. The dias-tema closes spontaneously during the next few weeksbecause of the pull of the supracrestal gingival fibers.Also both the maxillary bones and the posterior teethtip shghtly. This tipping leads to interferences betweenthe lingual cusps of the maxillary molars and the man-dibular posterior teeth and causes a transitional biteopening. The expansion is usually continued until themaxillary lingual cusps occlude with the lingual in-clines of the buccal eusps of the mandibular molarsto allow for relapses {Fig 9),
The appliance was worn by this pafient for 3 monthsto allow bone remodeling to be completed in the mid-sagittal suture. Some skeletal relapse can begin almostimmediately, even though the teeth are held in posi-tion. The net treatment effect is a combination of skel-etal and dental effects. After the 3-month retentionwith the fixed appliance, a removable Hawley appli-
ance was used as a retainer for another 3 months. Anadequate retention period is essential to assure sta-bility of the treated case.
Case 4
A unilateral posterior bticcal crossbite is relatively rareand its treatment has not been frequently reported inthe literature. Contrary to a hngual crossbite, a com-plete buccal posterior crossbite is due to a severe con-strietion of the mandibular arch instead of the max-illary arch. The transverse diserepancy can be the re-sult of a skeletal disharmony between the maxilla andthe mandible. Patients with Class II malocclusionshave a higher tendency for posterior crossbites (alltypes) than do persons with normal occlusions.'*
Figure 10 shows a 5-year-old girl who presented witha Class II malocclusion and a retrognathic mandible.In centric closure, the wider portion of the maxillaryarch was oecluding on the narrow portion of the man-dibular arch, forcing the mandible to deviate to oneside to allow the patient to occlude on the posteriorteeth. As a resttlt of the buccal crossbite, the mandi-bular posterior teeth were lingually tipped on the side.The crossbite caused an asymmetry of the dental arch.In addition, the patient also presented with a deepoverbite with impingement of the mandibular incisorson the palatal soft tissues. An early reciprocal clickingof the left lemporomandibular joint was also noted.
The treatment consisted initially of the placementof a removable maxillary expansion/eonlraction ap-
Quintes umber 6/1990 455

Pédiatrie Dentistry
pliance with posterior oeclusal coverage (Fig 11) anda mandibular expansion appliance. The bitepiane wasincorporated to open the bite and to minimize occlusalinterference during correction of the crossbite, A totalof 7 mm of mandibular expansion was accomplishedwith the appliance over a 6-month period.
Fnrther treatment to correct the skeletal Class IIdisharmony and the excess overbite was performedafter careful diagnosis, treatment planning, and con-sultation with an orthodontist. The appliance optionsfor this patient included cervical headgears, functionalappliances, or fixed appliances. This patient was treat-ed with functional appliance after correction of thecrossbite. The functional appliance was constructedwith a moderate vertical bite opening and with mod-erate forward posturing of the mandible. An expan-sion screw for transverse expansion was built in theapphance for mandibular expansion if needed. Figure12 shows the result after 2 years of treatment with thefunctional apphance. The transverse correction wasmaintained after the sagittal and vertical correctionshad been achieved.
Case 5
A posterior crossbite that is not accompanied by amandibular shift on centric closure can be caused bya marked bilateral maxillary constriction that pro-duces no interferences on closure. Occasionally, a pa-tient may present with a true unilateral maxillary pos-terior constriction. These cases can be diagnosed bythe presence of a unilateral posterior crossbite in cen-tric relation and centric occlusion and the absence ofa lateral shift to compensate. A poste roan te dor ce-phalogram may be taken to rule out the possibility ofan asymmetry of the mandible. Unilateral posteriorexpansion can be accomplished by a fixed appliance,such as the W-arch, which is unilaterally activated, ora split-plate removable apphance that incorporates awire spring or jackscrew for force generation.
Figure 13 shows a 6-year-old patient who presentedwith a unilateral constriction of the maxilla as a resultof the early exfoliation and mesial drifting of the pri-mary second molar. The amount of asymmetry wasroughly estimated by the use of a grid. The correctionof the crossbite was achieved using a split-plate re-movable appliance (Fig 14),
Case 6
Patients with signitlcant skeletal disharmony, such asin the case of mandibular prognathism or maxillary
deficiency, may present with posterior orossbttes thatare not related to the width of the Jctita! arches. Inthese patients, the sagittal discrepancy between themaxilla and the mandible causes the wider portion ofthe mandibular arch to occlude on the narrower por-tion of the maxillary arch, giving an appearance of aposterior crossbite. Patients presenting with skeletaldisharmony should be diagnosed and treatmentplanned with a complete set of diagnostic records thatincludes easts, complete-mouth radiographs or a pan-oramic radiograph, lateral and posteroanlerior ce-phalometric films, and frontal, lateral, and intraoral35-mm color transparencies. In addition, longitudinalheight and weight charts will help to evaluate thegrowth pattern as well as the treatment result. Anorthodontic consultation is strongly advised beforethe inifiation of treatment. A guide to cephalometricanalysis can be found in an orthodontic textbook."
Figure 15 shows an 8-year-old patient who presentedwith a Class III relation and concave profile that re-sulted from maxillary retrusion. Clinically, she had a2-mm horizontal centric occlusion-eentrie relationdiscrepancy on closure. In ecntrie occlusion, she hada bilateral posterior crossbite because of an abnormalanteroposteriorrelationshipof the maxilla to the man-dible and an anterior erossbite (Fig 16), Cephalometricanalysis (Fig 17) showed a moderate skeletal Class III(pattern point A-nasion-point B = —5'; average =-1-2°), The sella-nasion-point A angle of 75° (normal= 82°) suggested a retrusive maxilla. The maxillaryineisors were inclined normally (maxillary incisor tosella-nasion = 107°), and the mandibular incisorswere hngually inclined (mandibular ineisor to man-dibular plane = 83°; normal = 90°),
In general, the treatment of a patient presentingwith a maxiliary retrusion and posterior erossbite (notrecommended for a patient with mandibular prog-nathism) consists of a combination maxillary expan-sion and protraction chin cup therapy as described byTurley," Palatal expansion is used to "disarticulate"the maxilla and to initiate cellular response in the su-turae, allowing a more positive reaction to protractionforces. It also initiates a downward and forward move-ment of the retruded maxilla.'^ Another advantage ofmaxillary expansion is the correction of the posteriorcrossbite as well as providing space for alignment ofthe maxillary ineisors.
The patient in Fig 15 was treated with palatal ex-pander 1 week prior to the delivery of the protractionappliance. The protraction headgear v.'as secured tothe face by the stretehing of elastics from the hooks
1. Niinibi 6/1990

Pédiatrie Dentistry
ISM];
Fig 11 Maxillary expansion/contraction appliance withposterior occlusal coverage designed to turn backwards,ie, to close, rather than open, the spaces for the constrictionof the maxilla.
Fig 12 The same patient 2 years after correction of cross-bife and treatment with a functionai appliance.
(cat Fig 13 Intraorai iateral view of a 6-year-old girl with a truej is unilateral posterior crossbite.
Fig 14 Correction of tine true unilaterai posterior crossbiteusing removable split-palate expansion appliance.
QuintessSncimternafional Volume 21, f*jmber 6/1990
h g, 1
Fig 16 Intraoral lateral view of the same patient showingthe presence of anterior and posterior crossbites.
Fig 15 Profile of an 8-year-old patient with a maxillaryskeletal deficiency and a posterior crossbite.
457

Pédiatrie Dentistry
Fig 17 Pretreatment cephalometric radiograph otsame patient showing retrusion ot maxilla.
Fig 18 Posttrcatment intraoral lateral view of tbe patientafter rapid palatal expansion and protraction headgeartherapy.
Fig 20 Postfreatment cephalometric radiograph showingtbe correction of anterior crossbite.
Fig 19 Posttreatment Iaterai profile of tbe same patientsbowing improvement in facial harmony.
on the rnaxillary molars to the crossbow of the facemask. Heavy forces are generated, usually through theuse of %-in, 14-oz elastics bilaterally. Lighter forcesmay be used during the break-in period, but the forcesshould be increased as the patient adjusts to the ap-pliance.
This patient was instrLicted to wear the headgear 12to 16 hours each day. A Class I molar relationship wasestablished after 4 months of treatment (Fig 18). Fig-ure 19 shows the improvement ofthe facia! profile. A
cephalotnetric analysis was performed after the cor-rection of the anterior atid posterior crossbites (Fig20). The simultaneous use of rapid palatal expansionapphance and protraction headgear produced a slightforward movement of point A atid a slight downwardand forward tnovement of the tnaxilla (Fig 21). Thepatient was advised to continue wearing the protrac-tion headgear for night time for an additional 4 to 6months, A Class III bionator can be used for retentionafter the active appliance therapy.
458

Pédiatrie Dentistry
Discussion
Six patients were treated for corrections of posteriorcrossbites in the primary and early mixed dentitions.Fixed and removable orthodontic appliances wereused to correct simple and more complicated posteriorcrossbites of various etiologies. In each of these cases,the proper diagnosis and knowledge about the causesof posterior crossbite will allow normal growth anddevelopment to take place and may simplify any futureorthodontic treatment, if needed. On the other hand,there are risks of orthodontic therapy if treatment isnot controlled properly. For example, the use of rapidpalatal expansion appliance can cause overexpausionof the maxillary arch and anterior bite opening inpatients with a clockwise growth pattern. Inadequateretention following the use of expansion appliancesmay invite relapses, depending on the etiology of max-illary constrictions. Similarly, the use of protractionheadgear without proper expansion and anchoragesupport may lead to unnecessary movement of an-chorage teeth instead of the expected skeletal correc-tions. Thus, proper diagnosis and treatment planningwith appropriate records is of paramount importanceto the successful outcome of the treated case. Evenwhen there is a "simple" problem that the family den-tist can and will be able to correct, a consultativerelationship with the orthodontist can avoid mis-diagnoses and malpractice. This paper was intendedto help the family dentist recognize these problems inthe young child and understand the possible treatmentmodalities.
References
t . Fields HW: Treatment of non-sketetal problems in préadoles-cent children, in Proffit WR, Fields HW (eds): ComemporaryOntiodomics. St Louis, CV Mosby Co, (985, pp 341-346.
2. Ngan PW, Wei SHY: Early orlhodontic treatment in the mixeddentition, in Wei SHY (ed): Pédiatrie Demistry: Total PatientCare. Philadelphia, Lea & Febiger, 1988, pp 474-482.
3. Breitner C: The influence of moving deciduous teelh on thepermanent successor Am J Oral Surg l<)5O;36:il52-1177.
4. Mathews R: Translational movement of first deciduous molarinto second molar position. Am J Onliod t969:55:276-2g5.
5. Clifford FO: Cross-bite correction in the decidtjous dentition:principles and procedures. Am J Onliod 1971:59:343-349.
6. Kutin G, Hawes RR: Posterior crosshites in the deciduous andmixed dentition. Am J Onlwd 1%9;56:491-504.
7. Schroder U, Schroder I: Early treatment of unilateral posteriorcrossbite in children with bilateral contracted maxillae. Eur JOrlhod 1984;6:65-69.
Fig 21 Su peri m position of pretreatment and posttreatmentlateral head cephalometric radiographs showing the for-ward movement of point A and a slight downward andforward movement of the maxilla.
S. Moss ML: The functional matrix, in Kraus BS, Reidel RA (eds):Vis!as in Orthodontie\. Philadelphia, Lea & Febiger, 1962, ppS5 98.
9. Thilander B: Temporomandibular joint problems in children, inCarlson DS, McNamara JA, Ribbens KA (eds): DevelopmemAspects oj Temporiimandihular Join! Disorders. Monograph No.16, Craniofacial Growth Series. Center for Human Growth andDevelopment, Ann Arbor, University of Michigan, 1984, pp89-104.
10. Solberg WK, Bibb CA, Nordstrom BB, et al: Malocclusion as-sociated with temporomandibular joint tbanges in young adultsat autopsy. Am J Onlwd 19R6:»9:326-330.
11. Riolo ML, Brandt D, Ten Have TR: Associations between oc-clusal characteristics and signs and symptoms of temporoman-dibular joint dysfunction in children and young adults. Am JOnliod Demofae Oniiop 1987;92:467-477.
12. Moyers RE: Handbook of Onhndomics, ed 3. Chicago, YearBook Medical Publ, 1973.
13. SITU JM: Minor Toolh Movemen! in Children, ed 2. St Louis, CVMosby Co, 1977, pp 278.
14. Thilander B, Wahlund S, Lennartson B: The etïect of earlyinterceptive treatment m children with posterior cross-bile. EurJ Onlwd 1984:6:25-34.
15. Staley RN. Stuntz WR, Peterson LC: A comparison of archwidths in adults with normal occlusion and adults with ClassII, Division 1 malocclusion.l^m / Onliod 1985;88:163-169.
16. Proffit WR, Ackerman JL: Orthodontic diagnosis: the devel-opment of a problem list, in ProfTit WR, Fields HW (eds):Contemporary Orthodontic.^. St Louis, CV Mosby Co, 1985. pp138-156.
17. TurleyPK:OrthopediccorrectionofClass III malocclusion withpalatal expansion and custom protraction headgear. J Clin Or-i/ioJ 1988:22:314-325.
18. Hass AJ: Palatal expansion: just the beginning of dentofacialorthopedics. Am J Orthod 1970:57:219-255. Q
International Volume 21. tîumber 6/1990 459





























