Embed Size (px)
Citation preview

TMTHDT
tpsps
n2
opoawdp
PdtNRtttodbpfdwhpea
u
A
ASe
©P
LTC
AR
DIA
C
reatment of Peripartum Cardiomyopathy Withechanical Assist Devices and Cardiac
ransplantationannah Zimmerman, MD, Raj Bose, MD, Rich Smith, MSEE, and Jack G. Copeland, MD
epartment of Surgery, Section of Cardiothoracic Surgery, University of Arizona Health Sciences Center, University of Arizona,
ucson, Arizonatby
3mosabpmima
AD
U
Background. Peripartum cardiomyopathy is a lifehreatening illness. If maximal medical therapy fails,atients may then be treated with mechanical circulatoryupport devices and (or) cardiac transplantation. Oururpose is to demonstrate the long-term efficacy of theseurgical interventions.
Methods. A retrospective review of 18 patients diag-osed with peripartum cardiomyopathy from 1994 to009 was conducted.Results. Eighteen patients were referred with a median
f seven year delay between onset of symptoms andresentation. Eight (44%) had medical therapy with onlyne death at five years, seven are alive, and two patientsre awaiting transplantation. Six patients were implantedith devices. From this group, there were two hospitaleaths, one native heart recovery, and three heart trans-
lants with 100% survival. Four patients (21%) werepfacA
tfhstf
trowfjJmhtcsta
ciences Center, 1501 N. Campbell Ave, Room 4402, Tucson, AZ 85724;-mail: [email protected].
2010 by The Society of Thoracic Surgeonsublished by Elsevier Inc
reated with transplantation alone and all survived. Com-ined device and (or) transplant survival was 80% at oneear.Conclusions. The natural history of this group varied;
8% of the medically treated patients are stable onedical therapy (3 of 8) and 67% of the device patients (4
f 6) are alive. One of six device patients (17%) wasuccessfully bridged to native heart recovery. Mechanicalssist devices can be used as a bridge to recovery or as aridge to cardiac transplantation for the treatment oferipartum cardiomyopathy patients who fail medicalanagement. In addition, cardiac transplantation alone
s also a viable treatment option for patients who failedical management and do not require a mechanical
ssist device.(Ann Thorac Surg 2010;89:1211–7)
© 2010 by The Society of Thoracic Surgeons
eripartum cardiomyopathy is defined as congestiveheart failure resulting from left ventricular systolic
ysfunction in the last month of pregnancy or the withinhe first five months after delivery [1]. In 2000, the
ational Heart, Lung and Blood Institute and Office ofare Disease Workshop noted the importance of main-
aining this time frame of the last month of pregnancy tohe first five months postdelivery as part of the definitiono ensure that preexisting conditions were not the causef the patient’s cardiomyopathy. Furthermore, patientsiagnosed with peripartum cardiomyopathy cannot haveeen diagnosed with heart disease earlier in pregnancy,rior to pregnancy, or have an identifiable cause for heart
ailure. It is important to note that this diagnosis can beifficult to determine in the last month of pregnancyhen many women experience symptoms similar toeart failure, such as shortness of breath, fatigue, andedal edema. The diagnosis is confirmed by a standardchocardiogram that shows left ventricular dysfunctionnd decreased contractility [2].The true incidence of peripartum cardiomyopathy is
ncertain; the estimated range is between 1 per 100 to 1
ccepted for publication Dec 30, 2009.
ddress correspondence to Dr Copeland, University of Arizona Health
er 15,000 deliveries. Reports have demonstrated a dif-erence in the definition among countries [3]. Multiparitynd multiple gestational pregnancies tend to be in-reased. There also seems to be an increased incidence infrica, and in African American patients.The initial treatment for peripartum cardiomyopathy is
raditional medical management for congestive heartailure, including an angiotensin-converting enzyme in-ibitor, beta blocker, diuretic, and potassium� (K�)paring diuretic. Mechanical assist device and cardiacransplantation are the next available treatment optionsor patients who fail medical management.
In 1994, Keogh and colleagues [4] demonstrated thathere was no difference in survival rates for women whoeceived a cardiac transplant for peripartum cardiomy-pathy or for other etiologies. However, in the study itas noted that women treated with a cardiac transplant
or peripartum cardiomyopathy had higher rates of re-ection within the first six months after transplantation.ohnson and colleagues [5] showed similar results in a
ultiinstitutional study of 3,244 patients and stated that aistory of pregnancy, not the female gender, increased
he risk of rejection after heart transplantation. Aziz andolleagues [6], in 1999, published a case report of auccessful treatment of peripartum cardiomyopathy inhree women with cardiac transplantation. Rickenbacher
nd colleagues [7] followed patients transplanted for0003-4975/10/$36.00doi:10.1016/j.athoracsur.2009.12.064

pptwat
sptbToa(p1toa
ac
dtbadtc
M
WwsWRpf
Ffl
T
P
11
11
1
1
1
1
1212 ZIMMERMAN ET AL Ann Thorac SurgTREATMENT OF PERIPARTUM CARDIOMYOPATHY 2010;89:1211–7
AD
ULT
CA
RD
IAC
eripartum cardiomyopathy for 4.5 years � 3.2 years. Theeripartum cardiomyopathy group was identical to pa-
ients transplanted for idiopathic dilated cardiomyopathyhen comparing clinical presentation, laboratory values,
nd hemodynamic status at six months postcardiacransplantation.
There have been numerous reports of the treatment ofevere peripartum cardiomyopathy with cardiac trans-lantation, but only a few studies that demonstrate the
reatment with mechanical assist device support as eitherridge to transplantation or as a bridge to recovery.here have been three case reports published that dem-nstrate the successful use of either a left ventricularssist device (LVAD) or biventricular assist devicesBiVADs) as a bridge to cardiac transplantation in peri-artum cardiomyopathy. Lewis and colleagues [8], in997, described the use of a BiVAD as a bridge to cardiacransplantation in a 30-year-old black female. In twother patients, Tandler and colleagues [9] and Hovsepiannd colleagues [10] reported successful the use of LVADs
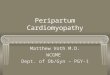
ig 1. Peripartum cardiomyopathy survivalow sheet.
able 1. Treatment of Peripartum Cardiomyopathy With Med
atient Inotropic Therapy Coreg
2 No 3.125 mg BID3 Dobutamine at 3 mcg/
kg/minNo
4 No 6.25 mg BID5 No 12.5 mg BID
6 No 25 mg BID
7 No 6.25 mg BID
8 No Not taking
9 Primacor, Dobutamine No
s a bridge to cardiac transplantation in peripartumardiomyopathy patients.
Thus, when patients diagnosed with peripartum car-iomyopathy fail medical therapy (including inotropic
herapy), mechanical assist device support as either aridge to recovery or bridge to cardiac transplantationnd primary cardiac transplantation are options. Weemonstrate in our institutional study that transplanta-
ion and bridge to transplantation groups can have suc-essful survival outcomes.
aterial and Methods
e conducted a retrospective chart review of 18 patientsho had been referred for treatment of severe unre-
olved peripartum cardiomyopathy from 1994 to 2009.e received institutional Human Subjects Institutional
eview Board approval and a waiver for the need foratient consent for this study. Inclusion criteria included
emales diagnosed with peripartum cardiomyopathy that
Therapy
SA KCL Lasix Lisinopril
g QD 40 mEq TID 60 mg TID 2.5 mg BIDNo No No
g QD No 40 mg QD 5 mg QDg QD No 40 mg BID 10 mg QD
No 20 mg PRN 40 mg QD
g QD No 20 mg QD 2.5 mg QD
80 mEq QD 40 mg TID No
100 mEq QD 80 mg BID No
ical
A
81 mNo
81 m81 m
No
81 m
No
No
Continued

hocseitWopf
R
AcuaawActOtchcooenbgkdpth
gnfnoHTvwsamb
i(ttpanpwoW(saotcBwmpwl6
T
AA
1213Ann Thorac Surg ZIMMERMAN ET AL2010;89:1211–7 TREATMENT OF PERIPARTUM CARDIOMYOPATHY
AD
ULT
CA
RD
IAC
ad persisted for greater than five months after deliveryf their child or children. We evaluated demographics,linical status, hemodynamics, nuclear and echo studies,erologies, cytotoxic antibodies, and standard transplantvaluation laboratory tests. The patients were dividednto the following groups based upon therapy: medicalherapy, mechanical assist device, and transplantation.
e also evaluated the time to referral and treatment byur heart failure management team, survival at one-yearosttransplantation, overall survival, and complications
rom mechanical assist devices and transplantation.
esults
total of 18 patients with a diagnosis of peripartumardiomyopathy were referred to our institution for eval-ation and treatment between 1994 and 2009. The aver-ge age of the women was 34 years. The average heightnd weight were 165 cm and 72.5 kg, respectively. Theyere of the following ethnicities: 11 Caucasian, 2 Nativemerican, 4 African American, 1 Hispanic, and 1 undis-
losed. New York Heart Association (NYHA) classifica-ions were the following: class I, 0; II, 1; III, 9; and IV, 9.ne-third had automatic internal cardiac defibrillators at
he time of referral; two additional automatic internalardiac defibrillators were implanted, one in a recoveredeart and one posttransplant. The number of pregnan-ies ranged from 1 to 8 with a mean of 2.6, and a medianf 2. Only two women had a pregnancy after diagnosis;ne woman had her fourth and the other woman had herighth pregnancy. All the other women were not preg-ant after diagnosis. Overall 15 patients had one hus-and, two patients had two husbands, two patients hadreater than two husbands, and one patient was un-nown. There was only one patient with children fromifferent husbands and she is living 16 years posttrans-lant but has had chronic humeral rejection for the entire
ime, resulting in graft diastolic dysfunction and multipleospitalizations for plasmapheresis.
able 1. Continued
Spironolactone Digoxin HydralazineLengthFollow-
25 mg QD 0.31 mg QD No 9 year25 mg QD 0.31 mg QD No 4 year
25 mg QD 0.31 mg QD No 2 year50 mg QD 0.25 mg QD No 16 year
25 mg QD 0.31 mg QD 25 mg TID 7 year
25 mg QD 0.125 mg QD No 4 year
25 mg QD No No 8 year
No 0.125 mg QD No 5 year
SA � acetylsalicylic acid; BID � twice a day; EF � ejection fracssociation; PRN � as needed; QD � every day; TID � three times
Many patients presented to either the clinic or emer-ency room with severe heart failure. Initial hemody-amic measurements for the entire group included the
ollowing: right atrial mean pressure, 8 mm Hg; pulmo-ary capillary artery wedge pressure, 18 mm Hg; cardiacutput, 4.3 L/minute; transpulmonary gradient, 9.5 mmg; and pulmonary vascular resistance, 2.4 Wood units.he multiple gated acquisition showed an average leftentricular ejection fraction (LVEF) of 0.27 in comparisonith the transthoracic echocardiogram that demon-
trated an average LVEF of 0.18. The following are theverage laboratory values: sodium 136, creatinine 1.2g/dL, glomerular filtration rates 69.5 mL/minute, total
ilirubin 1.05 mg/dL, and albumin 3.4g/dL.The patients were divided into three groups: (1) med-
cal treatment alone � listed for cardiac transplantation;2) mechanical assist device bridge to cardiac transplan-ation or bridge to recovery; and (3) cardiac transplanta-ion (Fig 1). Group 1 (medical treatment) includes eightatients. Only two of these required short-term dobut-mine therapy upon admission. The hemodynamics wereot severely disturbed: right atrial, mean 6 mm Hg;ulmonary artery systolic, 30 mm Hg; pulmonary arteryedge, mean 11 mm Hg; transpulmonary gradient, meanf 9 mmg; and pulmonary vascular resistance of 1.8ood units. Three have been listed for transplantation
Table 1 and Fig 1). Of those three women, one diedecondary to a sudden cardiac arrest and the other twore awaiting transplantation for four and nine years. Twothers were judged sick enough to list for transplanta-ion, though they had contraindications, including non-ompliance in one and pulmonary carcinoid in the other.oth are alive at 5 and 16 years after diagnosis. Threeomen have been stable and judged well enough foredical therapy alone for two to seven years. Nearly all
atients, in spite of the span of this study, were treatedith carvedilol, spironolactone, lisinopril, digoxin, and
asix. This group was followed for 2 to 16 years (mean of.9 years) with one death for a 12.5% mortality. One
Listed forTransplant Alive Comments
Yes Yes —Yes Yes —
No Yes —No Yes Not listed secondary to carcinoid
tumor of the lungNo Yes Not listed secondary to NYHA II,
Depression, HypothyroidismNo Yes Recovered 2 years after diagnosis
on medications, EF 55-60%No Yes Initially listed, non-compliant,
taken of the listYes No Died at an outside institution of
a cardiac arrest
ofup
ss
s
s
s
s
tion; KCL � potassium chloride; NYHA � New York Heartdaily.

pm
apstdaooaoHpTsCtsCwrtstTtdtTaaCrfwttcssotfaeriBasvdadBb1
ble
2.Pe
ripa
rtum
Car
diom
yopa
thy
Trea
tmen
tW
ithM
echa
nica
lA
ssis
tD
evic
eSu
ppor
t
ien
tD
evic
eD
ura
tion
onD
evic
eC
omp
licat
ion
sO
ther
Pro
ced
ure
sC
omp
licat
ion
ss/
pO
ther
Pro
ced
ure
Tra
nsp
lan
tR
ecov
ery
Aliv
e
Th
orat
ecB
iVA
D30
day
sH
emor
rhoi
ds
Sep
sis
-E
nte
roba
cter
Non
eN
AY
esN
oY
esT
hor
atec
BiV
AD
64d
ays
Non
eN
one
NA
Yes
No
No
Th
orat
ecB
iVA
D25
day
sN
one
Non
eN
AY
esN
oY
esT
hor
atec
BiV
AD
24d
ays
Ble
edin
gat
9d
ays
Non
eN
AN
oY
esY
es2
year
san
d10
mon
ths
Th
orat
ecB
iVA
D29
day
sP
eric
ard
ial
tam
pon
ade,
med
iast
init
isat
22d
ays
Rem
oval
ofT
hor
atec
and
pla
cem
ent
ofR
VA
Dta
nd
emh
eart
and
rem
oved
and
pla
cem
ent
ofa
Car
dio
Wes
tT
AH
at29
day
s
Acu
tere
nal
failu
re&
seiz
ure
at2
day
s,C
VA
at5
day
s,d
eath
No
No,
dea
that
14d
ays
pos
tC
ard
ioW
est
TA
Hse
con
dar
yto
CV
A
Car
dio
Wes
tT
AH
328
day
sSe
izu
re,t
ricu
spid
valv
eE
ntr
apm
ent
wit
ha
cen
tral
line,
Cdi
ffco
litis
,Mal
nu
trit
ion
,GI
blee
d,a
spir
atio
np
neu
mon
ia
Non
eN
AN
oN
oN
od
eath
at32
8d
ays
pos
tC
ard
ioW
est
TA
Hse
con
dar
yto
Sep
sis
AD
�bi
ven
tric
ula
ras
sist
dev
ice;
CV
A�
card
iova
scu
lar
acci
den
t;G
I�
gast
roin
test
inal
;R
VA
D�
righ
tve
ntr
icu
lar
assi
std
evic
e;T
AH
�to
tal
arti
fici
alh
eart
.
1214 ZIMMERMAN ET AL Ann Thorac SurgTREATMENT OF PERIPARTUM CARDIOMYOPATHY 2010;89:1211–7
AD
ULT
CA
RD
IAC
atient returned to NYHA class II, all others have re-ained either class III or IV.In group 2, patients were treated with mechanical
ssist devices between 1999 and 2009; there were sixatients with seven devices (Table 2). These were veryick patients who failed maximal medical and inotropicherapy. All were NYHA functional class IV. Prior toevice implantation, all the patients were on dobut-mine, three of six were also on milrinone, and (or) threef six were also on dopamine. Hemodynamics measuredn inotropic support reflected severe failure, with a righttrial mean of 13 mm Hg, pulmonary artery systolic meanf 48 mm Hg, pulmonary artery wedge mean of 26 mmg, transpulmonary gradient mean of 11 mm Hg, andulmonary vascular resistance mean of 3.2 Wood units.he mean body surface area for this group was 1.7qm (square meters). The two patients who receivedardioWest TAHs (total artificial hearts) (SynCardia Sys-
ems, Tucson, AZ) had body surface areas of 2.1, and 1.7qm (1.7 sqm is often used as a minimum size forardioWest implantation). Five patients were treatedith a Thoratec BiVAD (biventricular assist device) (Tho-
atec Corp, Pleasanton, CA) (duration of support from 24o 64 days), and two with a CardioWest TAH (duration ofupport 328 days and 12 days). One of the five patients,he only bridge to bridge patient in this series, received ahoratec BiVAD that was removed 29 days later. Next, in
hat same patient, a right ventricular assist device tan-em heart was placed, followed on the same day by
andem heart removal and implantation of a CardioWestAH (SynCardia Systems) for recurrent profound heartnd multisystem organ failure. This patient died 44 daysfter initial BiVAD implantation and 12 days post-ardioWest implantation. Our treatment strategy was to
etain the native heart favoring BiVAD use and hopingor native heart recovery. In the other patient implantedith a CardioWest TAH, rapid hemodynamic deteriora-
ion with multiple organ failure was the indication forotal heart support. There were two deaths in this me-hanical support group (33% mortality). The deaths wereecondary to a cerebral embolic event in one case andepsis in another. Three of the four patients who receivednly a Thoratec BiVAD went on to be transplanted andhe fourth patient had recovery of her native cardiacunction. The device was explanted and she is currentlylive three years post-explant with a left ventricularjection fraction of 0.45 and NYHA functional class II oneduced oral heart failure therapy and with an automaticnternal cardiac defibrillator. Two patients in this ThorateciVAD only group had complications of enterobacter sepsisnd bleeding. One patient on the CardioWest TAH diedecondary to entrapment of a central line in the tricuspidalve of the device, followed by an eight minute period ofevice shutdown, and irreversible brain injury leading tocomatose state and seizures. She died of sepsis after 328ays of support. The other CardioWest patient had had aiVAD, then a TandemHeart (CardiacAssist, Inc, Pitts-urgh, PA), and after severe decompensation died after
2 days of TAH support. Other complications in the Ta Pat
1 2 3 4 5 6 BiV

pk
ttwtHg2hfya
taswp2rlaTt
Aitgtis
C
Ptwogcdsssft
isatsacutt
ble
3.Pe
ripa
rtum
Car
diom
yopa
thy
Trea
tmen
tW
ithO
rtho
topi
cH
eart
Tran
spla
ntat
ion
ien
tD
evic
eP
rior
toT
ran
spla
nta
tion
Com
plic
atio
ns
Aft
erT
ran
spla
nta
tion
Aliv
eSu
rviv
alD
eath
Cau
seof
Dea
th
Yes
Ost
eop
enia
at2
mon
ths,
chol
eth
iasi
sat
3ye
ars,
gast
roen
teri
tis
at6
year
s,co
ron
ary
vasc
ulo
pat
hy
at7
year
sY
es9
year
s—
—
Yes
Hu
mer
alre
ject
ion
day
0,C
occi
pn
eum
onia
at1
year
,d
isse
min
ated
HSV
at3
year
sN
o2.
33ye
ars
Yes
Failu
reto
take
med
icat
ion
sfo
r2
wee
ksY
esR
ejec
tion
at21
day
s,6
mon
ths,
3ye
ars
&2
mon
ths
Yes
4.5
year
s—
—N
oA
cute
hu
mer
alre
ject
ion
atd
ay9,
reje
ctio
nat
37d
ays,
3y
&9
mo,
6y
Yes
15ye
ars
——
No
Non
eY
es7
year
s—
—N
oC
ocai
ne
&am
ph
etam
ine
over
dos
eat
18d
ays,
acu
tere
ject
ion
at6
mon
ths,
pye
lon
eph
riti
sat
10m
onth
s,N
o11
mon
ths
Yes
Dru
gov
erd
ose
No
Aft
er1s
ttr
ansp
lan
t-
CM
Vp
osit
ive
at2
mon
ths,
gast
ric
ulc
erat
3m
onth
s,H
SVat
7m
onth
s,re
ject
ion
at6
year
s,co
ron
ary
vasc
ulo
pat
hy
No
17ye
ars
s/p
1sttr
ansp
lan
tY
esM
ult
isys
tem
orga
nfa
ilure
No
Aft
er2n
dtr
ansp
lan
t–
reje
ctio
n&
C.d
iffco
litis
at1.
5m
onth
s,re
ject
ion
at4
mon
ths,
ren
alfa
ilure
at7
mon
ths
No
1.2
year
ss/
p2n
dtr
ansp
lan
t(1
8.2
yrs
cum
ula
tive
)Y
esM
ult
isys
tem
orga
nfa
ilure
V�
cyto
meg
alov
iru
s;H
SV�
her
pes
sim
ple
xvi
rus.
1215Ann Thorac Surg ZIMMERMAN ET AL2010;89:1211–7 TREATMENT OF PERIPARTUM CARDIOMYOPATHY
AD
ULT
CA
RD
IAC
atients in group 2 included seizure, mediastinitis, andidney and liver failure (Table 2).In group 3, four patients were treated with heart
ransplants alone. Their hemodynamics were similar tohose in the medical group. All were initially supportedith one inotrope. Hemodynamic mean values included
he following: right atrial, 4 mm HG; PA systolic, 29 mmg; PA wedge pressure; 13 mm Hg; transpulmonary
radient, 7 mmHg; and pulmonary vascular resistance,.2 Wood units. One of the four patients who received aeart transplant alone was retransplanted after 17 years
or coronary vasculopathy and lived for a total of 18.2ears (Table 3). One died at 11 months posttransplant ofdrug overdose.Looking at all seven patients who received an ortho-
opic heart transplant, including three who had a Thor-tec BiVAD as a bridge to transplant, the posttransplanturvival of the patients ranged from 0.92 to 18.2 yearsith a mean of 7.1 years and a median of 5.8 years. Fouratients are currently alive, with three late deaths (Tablesand 3). The complications range from acute humeral
ejection, rejection, coronary vasculopathy, cytomega-ovirus infection, disseminated herpes simplex virus,nd C. difficile colitis (all are listed in Tables 2 and 3).here was 86% (6 of 7) one-year survival after cardiac
ransplantation.Survival for the three groups is summarized in Figure 1.mong the three groups, long-term survival was found
n four of six device patients, three of four primaryransplant patients, and seven of eight of the medicalroup. Four of the medical group should be listed forransplant, but only two are listed and two have contra-ndications. Thus, only three in the medical group aretable and off the waiting list.
omment
eripartum cardiomyopathy is defined as heart failurehat develops within the last month of pregnancy and (or)ithin the first five months postpartum. All other causesf heart failure are excluded. Echocardiography is theold standard for diagnosis. Most cases of peripartumardiomyopathy can be medically managed. Table 1ocuments that the medical therapy for patients in thistudy has consistently been a beta blocker, an angioten-in-converting enzyme inhibitor, a diuretic, and a potas-ium sparing diuretic, the traditional standard heartailure medical regimen. This is true even though theime of referral varied from 1994 to 2009.
For those patients who fail oral medical management,notropic medical support (typically dobutamine) istarted and then additional inotropes such as milrinonend dopamine may be added. If such a patient continueso deteriorate on medical therapy based on the patient’symptoms and hemodynamic status, then mechanicalssist device and (or) cardiac transplantation can beonsidered, depending on the severity of the heart fail-re. We have demonstrated that for the sicker patients
he Thoratec BiVAD is an option as a bridge to transplan-
ation as well as a bridge to recovery. We had only one Ta Pat 1 2 3 8 9 10 11 11 CM

rrpsaheaooah
iutdittc2otatotstlwffuost
tpfprtt7
stc(MoTvtpps
tdpmsTttl
toop(aos
utmatmnocwctTs
amthdtdNasdaarmwt
R
1216 ZIMMERMAN ET AL Ann Thorac SurgTREATMENT OF PERIPARTUM CARDIOMYOPATHY 2010;89:1211–7
AD
ULT
CA
RD
IAC
ecovery patient, perhaps because of selection bias. Still,ecovery in one of five patients in this small seriesrovides the basis for a strategy that favors a supportystem that preserves the native heart. For patients whore not sick enough for a mechanical assist device thoughave failed medical therapy and are progressively wors-ning on either oral medical therapy or inotropic supports well, cardiac transplantation is the next treatmentption. The CardioWest TAH may also be used, butbviously not as a bridge to recovery. Rather, it was useds a rescue device in patients who were judged to needigh cardiac outputs and low venous pressures.Once again the time span of this study can be mislead-
ng with respect to mechanical circulatory support devicese. As time has passed, the availability of devices and
he indications for their uses has changed. Fortunately,uring the period from 1999 to 2008 when all of the
mplants in this series were done, we have had threeypes of LVADs, one type of extracorporeal BiVAD, andhe CardioWest TAH available. Our algorithm for devicehoice was published in the Annals of Thoracic Surgery in001 [11]. Further, we reviewed all multivariate analysesn VADs as well as our own analysis of risk factors usinghe total artificial heart [13] and have not changed ourpproach. Briefly, for unstable rapidly deteriorating pa-ients with early signs of multiorgan failure and (or)bvious biventricular failure, we use two prosthetic ven-ricles; extracorporeal BiVADs for small patients withmall hearts based on the patient’s body surface area andhe CardioWest TAH for larger patients or patients witharge hearts. We have reserved LVAD use for patientsho are relatively stable and are free of renal and hepatic
ailure, without a history of recent cardiac surgery, andree of any sign of right heart failure. The current trend tose short-term support with extracorporeal membranexygenation was not followed in this study, with thehortest duration of support being 24 days in the patienthat recovered.
Overwhelming evidence exists that cardiac transplan-ation is a successful option for the treatment of severeeripartum cardiomyopathy. Our data showed success-
ul outcomes with cardiac transplantation with sevenatients who received a transplant and one patient whoeceived a retransplant. The posttransplant survival ofhe patients ranged from 0.92 to 17 years from initialransplant (18.2 years with retransplant) with a mean of.1 years (Table 3).In addition to cardiac transplantation, mechanical as-
ist devices have also been used for treatment of peripar-um cardiomyopathy, though the literature is limited toase reports describing the use of the Novacor LVADWorld Heart Inc, Oakland, CA), and BiVAD [8–10].
echanical assist device support for peripartum cardiomy-pathy included the Thoratec BiVAD and the CardioWestAH in our institution with six patients and seven de-ices (Table 2). Farrar and colleagues [12] demonstratedhe option of bridge to recovery in the Thoratec VAD inatients with cardiomyopathies including patients witheripartum cardiomyopathy. In this multiinstitutional
tudy, two of the four patients diagnosed with peripar-um cardiomyopathy who received a mechanical assistevice were transplanted [12, 13]. Bridge to recovery is aossible option for the treatment of peripartum cardio-yopathy with the use of a Thoratec VAD as demon-
trated by our institution and by Farrar and colleagues.hough the evidence for bridge to recovery in peripar-
um cardiomyopathy is limited, this is an excellent set-ing for native heart recovery because this patient popu-ation is relatively young and healthy.
Though we have demonstrated good results for thereatment of peripartum cardiomyopathy, one limitationf our study is the small number of patients. We followedur patients for up to 18 years and we only accrued 18atients, with ten who had a mechanical assist device and
or) cardiac transplantation. The literature for mechanicalssist devices in the treatment of peripartum cardiomy-pathy is limited to case reports. We demonstrate a smalleries and one unique experience of bridge to recovery.
We conclude that mechanical assist devices can besed as a bridge to recovery or as a bridge to cardiac
ransplantation for the treatment of peripartum cardio-yopathy patients who fail medical management. In
ddition, cardiac transplantation alone is also a viablereatment option for patients who fail medical manage-
ent and do not require a mechanical assist device. Theatural history of this group varied. Sixty-seven percentf the device patients (4 of 6) are alive. Only one of thesehronic heart failure patients was successfully bridgedith mechanical circulatory support to native heart re-
overy. Seventy-five percent of primary transplant pa-ients survived over 2.33 years (range, 2.33 to 18.2 years).hirty-eight percent of the medically treated patients aretable on medical therapy (3 of 8).
In summary, we recommend the following treatmentlgorithm for peripartum cardiomyopthy. Initial treat-ent should start with traditional medical heart failure
herapy including an angiotensin-converting enzyme in-ibitor, a beta blocker, a diuretic, and an K� sparingiuretic. If the patient does not improve on oral medical
herapy, inotropic support should be started includingobutamine and possibly milrinone and (or) dopamine.ext, if the patient continues to become symptomatically
nd hemodynamically worse, cardiac transplantationhould be considered. If the patient’s clinical statuseteriorates further, based again on the hemodynamicsnd the clinical presentation, we recommend mechanicalssist device support with a BiVAD for possible bridge toecovery. If the patient’s clinical status demonstratesultiorgan failure such as hepatic and (or) renal failure,e recommend a CardioWest TAH as a bridge to
ransplantation.
eferences
1. Abboud J, Murad Y, Chen-Scarabelli C, Saravolatz L, Scara-belli TM. Peripartum cardiomyopathy: a comprehensivereview. Int J Cardiol 2007;118:295–303.
2. Pearson GD, Veille JC, Rahimtoola S, et al. Peripartumcardiomyopathy National Heart, Lung and Blood Institute
and Office of Rare Diseases (National Institutes of Health)
1
1
1
1
I
Cetibv1etasgpt
pwobn1bt
fb
1217Ann Thorac Surg ZIMMERMAN ET AL2010;89:1211–7 TREATMENT OF PERIPARTUM CARDIOMYOPATHY
©P
AD
ULT
CA
RD
IAC
workshop recommendations and review. JAMA 2000;283:1183–8.
3. Tidswell, Mark. Peripartum cardiomyopathy. Crit Care Clin2004;20:777–88.
4. Keogh A, Macdonald P, Spratt P, Marshman D, LarbalestierR, Kaan A. Outcome in peripartum cardiomyopathy afterheart transplantation. J Heart Lung Transplant 1994;13:202–7.
5. Johnson MR, Naftel DC, Hobbs RE, et al. The incrementalrisk of female sex in heart transplantation: a multi-institutional study of peripartum cardiomyopathy and preg-nancy. J Heart Lung Transplant 1997;16:801–12.
6. Aziz TM, Burgess MI, Acladious NN, et al. Heart transplan-tation for peripartum cardiomyopathy: a report of threecases and a literature review. J Cardiovasc Surg 1999;7:565–7.
7. Rickenbacher PR, Rizeq MN, Hunt SA, Billingham ME,Fowler MB. Long-term outcome after heart transplanta-tion for peripartum cardiomyopathy. Am Heart J 1994;127:1318 –23.
8. Lewis R, Mabie WC, Burlew B, Sibai BM. Biventricular assistdevice as a bridge to cardiac transplantation in the treatment
for peripartum cardiomyopathy. South Med J 1997;90:955–8.iventricular device might be more favorable for this
clermpsoach
F
UCSCe
R
1
2010 by The Society of Thoracic Surgeonsublished by Elsevier Inc
9. Tandler R, Schmid C, Weyand M, Scheld HH. NovacorLVAD bridge to transplantation in peripartum cardiomyop-athy. Eur J Cardiothorac Surg 1997;11:394–6.
0. Hovsepian PG, Ganzel B, Sohi GS, Kupersmith J, Gray L Jr.Peripartum cardiomyopathy treated with a left ventricularassist device as a bridge to cardiac transplantation. SouthMed J 1989;82:527–8.
1. Copeland JG 3rd, Smith RG, Arabia FA, et al. Comparison ofthe CardioWest total artificial heart, the Novacor left ven-tricular assist system and the Thoratec ventricular assistsystem in bridge to transplantation. Ann Thorac Surg 2001;71:S92–7.
2. Farrar DJ, Holman WR, McBride LR, et al. Long-term fol-low-up of Thoratec ventricular assist device bridge to recov-ery patients successfully removed from support after recov-ery of ventricular function. J Heart Lung Transplant 2002;21:516–21.
3. Copeland JG, Smith RG, Bose RK, Tsau PH, Nolan PE,Slepian MJ. Risk factor analysis for bridge to transplantationwith the CardioWest total artificial heart: an approach tomechanical circulatory support device selection. Ann Thorac
Surg 2008;85:1639–44.NVITED COMMENTARY
opeland and colleagues [1] present their single-centerxperience from the University of Arizona at Tucson inhe treatment of peripartum cardiomyopathy with med-cal therapy, assist devices, and transplantation in a smallut important subgroup of heart failure patients with aery high priority—at least to their child [1]. They treated8 patients, and the report covers 15 years of theirxperience. Nevertheless, much has changed during thatime, especially in medical treatment and also in the usend quality of the assist devices. The authors report atepwise approach to treat these young patients withood overall results, which was developed as timeassed, but also report tragic fates of individuals and
heir families.Although medical treatment in heart failure has im-
roved steadily in recent years, in emergency situationsith acute heart failure, assist devices are still the onlyption for these patients. Severity of this disease haseen shown because biventricular support is mostlyeeded, and weaning from assist devices was possible inpatient only. Therefore cardiac transplantation seems toe the only hope and treatment end point for most of
hese patients with severe peripartum cardiomyopathy.But the article also reflects one of the major problems
or the surgeon, cardiologist, and intensivist. What sort of
ritical patient population? Implantation of a biventricu-ar assist device while leaving the heart in place is lessmotional for a surgeon. It restores the chance for cardiacesuscitation in case of device failure and preserves theinor chance of removal after cardiac recovery. If im-
lantation is anatomically feasible, a total artificial hearteems to be much more effective by means of cardiacutput and might also be superior in patient comfort, butlso reflects the point of no return, with the patientompletely dependent on the function of the artificialeart and fixing the need for cardiac transplantation.
riedrich S. Eckstein, MD
niversity Hospital Basellinic for Cardiac Surgerypitalstrasse 21H-4031 Basel, Switzerland-mail: [email protected]
eference
. Zimmerman H, Bose R, Smith R, Copeland JG. Treatment ofperipartum cardiomyopathy with mechanical assist devices
and cardiac transplantation. Ann Thorac Surg 2010;89:1211–7.0003-4975/10/$36.00doi:10.1016/j.athoracsur.2010.02.013