Embed Size (px)
Citation preview

Treatment of Failed Back Surgery Syndrome
Alessandro Dario, MD*† ▪ Gianpaolo Fortini, MD*‡ ▪ Daniele Bertollo, MD*‡ ▪Alessandro Bacuzzi, MD*‡ ▪ Carlo Grizzetti, MD*‡ ▪ Salvatore Cuffari, MD*‡
*Center of Neurostimulation, †Department of Neurosurgery; ‡Pain Management Department,Varese Regional Hospital and Macchi Foundation, Como, Italy
� ABSTRACTObjectives. To evaluate the long-term results of different and several therapeutic courses were necessary to con-
trol the pain. Two patients treated medically had sub-therapies for failed back surgery syndrome (FBSS).Materials and Methods. From 1992 to 1997, 49 patients stantial side effects. All but two patients treated with
SCS demonstrated good results for their leg pain;were treated for FBSS. Twenty patients were treatedmedically. Twenty-four patients, who did not respond to whereas those treated for back pain with SCS had poor
results. Two patients still needed continuous drug admin-medical therapy, underwent spinal cord stimulator (SCS)implant and five underwent further spine surgery. All pa- istration.
Conclusions. Medical therapy is effective for leg andtients were evaluated by VAS, PDI, and the OswestryScales before treatment and at follow-up. Leg pain, back pain; nevertheless, several courses of therapymay
be necessary. SCS is an effective treatment for leg pain,back pain, work status or daily activities, drug side ef-fects, and use of analgesic medications after implanta- however, its effectiveness on back pain appears to be
inadequate. �tion were examined. Follow-up ranged from 24 to 84months (mean 42 months).Results. At last follow-up, the patients treated medically
KEYWORDS: back pain, failed back surgery syndrome,demonstrated good results on leg and low back painin eight cases; in other cases, good results were transitory spinal cord stimulation.
INTRODUCTION appreciated causes of FBSS is inappropriate initialpatient selection or diagnosis. Because of these nu-
The term, failed back surgery syndrome (FBSS), re-merous factors, the treatment of this syndrome can
fers to a condition in patients who continue to havebe difficult and it can require several approaches.
back pain or leg pain despite lumbar spine opera-We report our clinical experience with FBSS and
tion. In the literature, failure rates for lumbar surgicalpain control.
intervention range from 5% to 50%(1). There aremany potential primary factors leading to FBSS: lat-eral or central stenosis, recurrent disc herniation,epidural fibrosis, adhesive arachnoiditis, symptom- MATERIALS AND METHODSatic pseudoarthrosis, spondylolisthesis(2), as well as
From 1992 to 1997, 49 patients were treated forcentral pain. Moreover, one of the leading and under-FBSS in our center. The main complaint in thesepatients was lumbosciatic pain: 21 patients with
Address all correspondence and reprint requests to: Alessandro Dariolumbosciatic pain had predominant leg pain (60–MD, Macchi Foundation, Via Torriani, 32, Como I-22100, Italy.
70% leg pain, 30–40% back pain), 22 had only legpain and six had only back pain. Of the 49 patients,
� 2001 International Neuromodulcaiton Society, 1094–7159/00/$15.00/0Neuromodulation, Volume 4, Number 3, 2001 105–110 15 patients showing predominant leg pain under-

106 � DARIO ET AL.
went intravenous pharmacologic testing(3) with ad- day) and methylprednisolone (dose, 40 mg/week);in three patients, a morphine infusion (dose, 1 mg/ministration of 2.5–5 mg/kg lidocaine over 30
minutes to assess whether the patient had neuro- day) was added. Occasionally we added an infusionof clonidine (dose,150 mcgs/day). All side effectspathic pain or not. Three days later, this test was
followed with intravenous bolus of 0.3 mg/kg of of the administered medications were reported.After six months of inefficacious medical therapy,morphine to assess the amount of mechanical pain
present. A test with intravenous bolus of propofol, patients underwent implantation of an epidural spi-nal cord stimulation system (Itrel 2 or Itrel 3, Med-0.2 mg/kg, was used to exclude pain of central ori-
gin(4). Five patients with back pain were prescribed tronic Inc., Minneapolis, MN); 22 patients wereimplanted with percutaneous electrodes (Pisces-lumbar corset for two months only, for the sake of
achieving temporary therapeutic effect. Quad, Medtronic Inc.), while two patients wereimplanted with plate-type electrodes (Resume, Med-There were 26 (53.1%) males, and 23 (46.9%)
females; the mean age was 53.5 years (range 35–81 tronic Inc.). Permanent implant was carried out onlyafter a successful trial (reduction of VAS of equalyears). Imaging diagnosis was made routinely using
post contrast CT-scanning and/or by magnetic reso- or greater than 50%) for a period of 30 days. Allelectrodes were implanted between T9 and T12 andnance imaging. Myelography, performed in the su-
pine and standing position, was used to exclude paresthesia coverage and overlap was almost 80%in all cases.variations in the lumbar disc after stress and to ob-
serve the presence or not of arachnoiditis. Lumbar Efficacy of therapy on leg and back pain, returnto work status for the employed, and activities offunctional X-rays were also performed in all patients
to distinguish grade of spondylolisthesis, if present. daily living for the retired, were evaluated beforetreatment and at follow-up, after therapy. The con-Discography was not used. All patients had pain for
at least one year after the last operation. The mean comitant use of medications and doses after neuro-stimulator implant was also assessed. Statisticalnumber of lumbar operations before treatment was
2.4 operations (range 1–7 operations); the diagnosis analysis of data was performed using the Wilcoxon,signed-rank test.at first operation was herniated lumbar disc in 39
patients (79.6%), spinal stenosis in eight patients(16.3%) and spinal instability in two patients (4%).
All patients were evaluated using a Visual Analog RESULTSScale (VAS) with a 0–100 scale, where 0 representedno pain and 100 represented worst pain; the Pain Neuroradiologic examinations excluded pathology
susceptible to direct surgical repair in 44 patients.Disability Index (PDI), with a 0–60 score; and theOswestry Scale, with a 0–50 score. All scores were Of the 49 patients in this study, four patients had
predominantly greater leg pain than back pain,evaluated before treatment and every three monthsafter treatment; the follow-up ranged from 24 to 84 which was caused by recurrent disc herniations in
two patients and by lateral stenosis in two patients.months with a mean duration of treatment of 42months (last follow-up, 1999). The follow-up range One patient with spondylolisthesis presented only
with back pain which required spinal fixation forfor the medical group was 46 months, and for theimplanted group, 43 months. instability. By last follow-up, all of these patients had
resolution of their symptoms. In the 44 remainingMedical therapy was carried out at first by admin-istration of dexamethasone, 4–12 mg/day, and non- patients, epidural fibrosis and/or, more rarely, adhe-
sive arachnoiditis (3%) was found.steroidal anti-inflammatory analgesics. After thisinitial treatment, medical management was followed Of the 15 patients with predominant leg pain,
the intravenous lidocaine test for neuropathic painby administration of medications in the followingorder: carbamazepine, 200–600 mg/day, or valproic was positive in all. The morphine test for mechanical
pain was also positive in four of 15 patients; theacid, 300 mg/day, amitriptyline, 20–75 mg/day, andbaclofen, 10–30 mg/day or diazepam, 4–7.5 mg/day. propofol test was negative in all but one of these
patients. This patient suffered from leg and backIf necessary, tramadol, 50–150 mg/day was used. Inour center, gabapentin was introduced in 1997. pain. Of the five patients with back pain, the use
of a lumbar corset was found to benefit two.If an epidural was used, continuous spinal infu-sion consisted of bupivacaine, 0.25% (dose, 50 mg/ Twenty patients were treated only with medical

Treatment of FBSS � 107
therapy (8/20 had only leg pain, 7/20 had predomi-nant leg pain, and 5/20 had only back pain). Ofthese 20 patients, six patients needed spinal epi-dural infusion for 1–2 months. Nine of the 20 pa-tients with medical therapy alone had definiteimprovement. Of these nine patients, five who wereon disability returned to work and four, who wereretired, resumed their activities of daily living.Eleven of the 20 patients with medical therapy alonehad only intermittent improvement and requiredseveral and repeated courses of their therapy. Ofthese 11 patients, four were employed and sevenwere retired. Three of the four employed individualswere forced to reduce their workload and the fourthwas forced to stop work. Five retired patients re-duced and two stopped their activities of daily living.
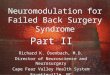
Medical therapy improved both back and leg pain.The mean VAS score before treatment was 76 (range91–62), the mean VAS, at last follow-up, was 25(range 31–18, Fig. 1). The mean PDI score in themedical management group before treatment was42 (range 55–32), the mean at follow-up was 4(range 8–2,Fig. 2A). The mean Oswestry scale scorein this group before treatment was 23, the mean atfollow-up was 6 (range 35–10, Fig. 3A). Two patientsin the medical management group experienced non-fatal lowering of their leukocytes; almost all patients Figure 2. PDI range score at last follow-up of the patients
treated by (A) medical therapy (A1, maximum; A2, mean; A3,had sedative effects of their therapy. These effectsminimum) and (B) spinal cord stimulation (B1, maximum; B2,were reported as particularly unpleasant in eight ofmean; B3, minimum).20 patients.
Twenty-four patients after six months of ineffica-cious medical therapy underwent implantation oftemporary epidural spinal cord stimulation elec- trodes. Of these 24 patients, 14 had only leg pain
and 10 had predominant leg pain with some backpain. Twenty-three of 24 patients underwent perma-nent implantation, having successfully finished atrial of temporary stimulation. At last follow-up, 21of 23 patients continued to have good results; ofthese 21 patients, eight resumed work and 13 (fourretired, nine unemployed) resumed daily activities.Three of 23 patients implanted (1 temporary im-plant, 2 permanent implants after 12 and 14 monthsof therapy, respectively) had poor results. Of thesethree patients with poor results, two were forcedto stop work and one patient could not resume hisown daily activities. In two patients of this groupwith poor results, an intrathecal drug infusion sys-tem (Synchromed 8611 H, Medtronic Inc.) was im-planted for pain relief.Figure 1. VAS range score at last follow-up of the patients
Of the 10 patients of the 24 patients who under-treatedbymedical therapy (A1,maximum; A2,mean; A3,mini-mum). went temporary SCS electrode placement pre-

108 � DARIO ET AL.
Figure 3. Oswestry scale range score at last follow-up of thepatients treated by (A) medical therapy (A1, maximum; A2,mean; A3, minimum) and (B) spinal cord stimulation (B1, maxi-
Figure 4. VAS score range of the leg pain (A) and back painmum; B2, mean; B3, minimum).(B) at last follow-up of the patients treated by spinal cord stimu-lation.
senting with both back pain and leg pain,improvement (VAS > 50%) in back pain was found Two patients with SCS still required continuousin only 1 patient. The mean VAS score for patients drug administration; whereas, five patients requiredwith only leg pain, before treatment, was 85 (range occasional drug administration.92–77). The mean VAS, at last follow-up, was 22(range 17–27 Fig. 4A). The mean VAS score for backpain, before treatment, was 45 (range 39–50), the DISCUSSIONmean at follow-up was 40 (range 36–45, Fig. 4B).There was a statistically significant difference (p < Medical therapy in our series proved to be useful
in controlling both back and leg pain in 20 patients.0.01) between these two groups.The mean PDI score before treatment was 51 The fluctuations of the VAS scores seen were most
probably due to the different pain relief dura-(range 40–60); the mean at follow-up was 7 (range2–10, Fig. 2B). There was no statistical difference tions(2). Nevertheless, the need for several cycles
of medical therapy must be emphasized. With thisbetween the medical therapy and SCS groups. Themean Oswestry scale score before treatment was therapy, one should always be aware of the develop-
ment of side effects. Neurostimulation only partially12 (range 17–6); the mean at follow-up was 9 (range16–5, Fig. 3B). Between the medical therapy and resolves the need for chronic medical therapy in
patients not responding to medical therapy alone;the SCS groups there was a statistically significantdifference (p < 0.05). and in our opinion, this therapy should be offered

Treatment of FBSS � 109
to patients who are responsive to medical therapy, patients without radiologic instability but with posi-tive facet block tests, a previously performed spinalbut still require recurrent courses of treatment.
The main radiologic finding at diagnosis for FBSS arthrodesis was inefficacious.We, the authors, believe that establishing a cor-in our series was epidural fibrosis (43 patients) fol-
lowed by recurrent disk herniation (2 patients), and rect pain diagnosis is fundamental to the successfultreatment of this syndrome. There are mechanisticlateral stenosis and arachnoiditis (1 patient). We
were not able to demonstrate any correlation be- differences between nociceptive pain, neuropathicpain, mixed nociceptive and neuropathic pain, andtween the amount of fibrosis and the intensity or
the duration of the pain(5). The scanty number of sympathetically maintained or sympathetically inde-pendent pain syndromes(16), which determine thepatients with spondylolisthesis in our series is proba-
bly due to the high number of herniated lumbar best and most appropriate therapeutic modality tobe used. This understanding of mechanisms operantdiscs seen in middle-aged patients without spon-
dylosis as first cause of FBSS. FBSS should be consid- in the development of mixed pain aids greatly indetermining appropriate therapy. In particular, weered a chronic disease. This was borne out in our
series by the fact that this group of patients needed advise performance of all intravenous pharmaco-logic testing for cases of FBSS.ongoing therapy for prolonged periods of time. The
definitive resolution of symptoms in this group with In epidural fibrosis with resultant leg pain of pre-dominantly neuropathic origin, SCS has proven effi-medical therapy could be explained by the reduc-
tion of inflammation around the epidural fibrous cacious. Recent literature, however, on the use ofnewer neuromodulatory tools has shown that dualtissue(6) by the therapy. Nevertheless, the persis-
tence of the pain over time could also be explained channel electrostimulation and the intraspinal infu-sion of differing admixtures of intrathecal analgesicby neuromechanic factors such as traction of fibrotic
nerve roots(6). The presence of persistent back pain agents could be promising therapy for chronic, axiallow back pain(17).could also be explained by chronic mechanical neu-
ral irritation of the disc sensory nerve fibers passingthrough sinuvertebral nerves(7). As a matter of fact,back pain in our experience, only responds to drugs REFERENCESactive against neuropathic pain(8).
Discography has been reported to be useful in 1. Follett KA, Dirks BA. Etiology and evaluationof the failed back surgery syndrome. Neurosurg Qthe diagnosis of low back pain, but it still remains a
controversial modality(9–11). While some clinicians 1993;3:40–59.2. Burton CV, Kirkaldy-Willis WH, Yong-Hing K,believe that discography helps to identify painful
discs and internal disc disruption, clinicians adverse Heithoff KB. Causes of failure of surgery on thelumbar spine. Clin Orthop 1991;157:191–199.to discography think that this test has no proven
validity in improving patients’ outcomes. Discogra- 3. Sorensen J, Kalman S, Tropp H, BengtssonM. Can a pharmacological pain analysis be used inphy has been poorly reported in patients with
FBSS(12), since the use of this diagnostic tool, in this the assessment of chronic low back pain? Eur SpineJ 1996;5:236–242.particular syndrome, has not been well established.
Nevertheless, discography is able to identify the 4. Canavero S, Bonicalzi V, Pagni CA, CastellanoG, Mercante R, Gentile S. Propofol analgesia in cen-painful disc or discs. It still remains to be seen
whether this information has any prognostic tral pain: preliminary clinical observations. J Neurol1995;242:561–567.value(11). Although back pain in some of our pa-
tients was not too disabling, moderate low back 5. Nygaard OP, Kloster R, Dullerud R, JacobsenEA, Mellgren SI. No association between periduralpain of more than six months’ duration should be
treated(13). scar and outcome after lumbar microdiscectomy.Acta Neurochir 1997;139:1095–1100.Back pain could be due to the so–called facet
syndrome; this syndrome, confirmed by facet block 6. Robertson JT. Role of peridural fibrosis in thefailed back: a review. Eur Spine J 1996;5 (Suppl. 1):showing at least 70% relief of pain, can be resolved
by postero-lateral spinal arthrodesis(14). Neverthe- S2–S6.7. Suseki K, Takahashi Y, Takahashi K, Chiba T,less, this predictive value of facet block has not
been confirmed in other studies(15). In two of the Yamagata M, Moriya H. Sensory nerve fibers from

110 � DARIO ET AL.
lumbar intervertebral discs pass through rami com- cography of lumbar discs after surgical treatmentfor disc herniation. Spine 1997;22:1606–1609.municants. A possible pathway for discogenic low
back pain. J Bone Joint Surg Br 1998;80:737–742. 13. Gill K, Frymoyer JW. The management oftreatment failures after decompressive surgery. Sur-8. Atkinson JH, Slater MA, Williams RA, et al. A
placebo-controlled randomized clinical trial of nor- gical alternatives and results. In: Frymoyer JW, ed.The Adult Spine. Principles and Practice. New York:triptyline for chronic low back pain. Pain 1998;76:
287–296. Raven Press, 1991:191–210.14. Lovely TY, Rastogi P. The value of provocative9. Ito M, Incorvaia KM, Yu SF, Fredrickson BE,
Yuan HA, Rosenbaum AE. Predictive signs of disco- facet blocking as a predictor of success in lumbarspine fusion. J Spine Dis 1997;10:512–517.genic lumbar pain on magnetic resonance imaging
with discography correlation. Spine 1998;23: 15. Hanley EN, David SM. Lumbar arthrodesis forthe treatment of back pain. J Bone Joint Surg Am1252–1260.
10. Carragee EJ, Tanner CM, Yang B, Brito JL, 1999;81:716–730.16. Sorensen J, Bengtsson M. Intravenous phen-Truong T. False-positive findings on lumbar discogra-
phy. Reliability of subjective concordance assess- tolamine test; an aid in the evaluation of patientswith persistent pain after low-back surgery ? Actament during provocative disc injection. Spine 1999;
24:2542–2547. Anaesthesiol Scand 1997;41:581–585.17. Devulder J, Laat M, Rolly G. Dual channel11. Bogduk N, Modic MT. Controversy. Lumbar
discography. Spine 1996;21:402–404. electrostimulation in pain. Acta Neurol Belg 1998;98:195–198.12. Heggeness MH, Watters WC, Gray PM, Jr. Dis-