Embed Size (px)
Citation preview

Treatment of chronic hepatitis C in drug-naïve patients
8th International Workshop on HIV & Hepatitis Co-infectionMadrid, 31. May 2012
Christoph SarrazinJ. W. Goethe-University Hospital
Medizinische Klinik IFrankfurt am Main, Germany

Hepatitis C: New treatment era with approval of NS3 protease-inhibitors
EMA Market Authorisation European Union18.7.2011
HCV NS3 Protease-InhibitorTelaprevir
Triple-TherapyHCV Genotype 1
HCV NS3 Protease-InhibitorBoceprevir
Triple-TherapyHCV Genotype 1
EMA Market Authorisation European Union19.9.2011

Triple-Therapies: Improved SVR ratesTreatment-naïve Genotype 1 pts.ADVANCE
RGT, TVR 12 vs. 8 wksSPRINT-2
Lead-in(LI), RGT vs. non-RGT
Jacobson et al. NEJM 2011
0
10
20
30
40
50
60
70
80
Sust
aine
d vi
rolo
gic
resp
onse
Response guided
TVR 12 wks+ PEG2a+ Riba
75%69%
44%
PEG2a + Riba
(48 wks)
Response guided
TVR 8 wks+ PEG2a
+ Riba
Poordad et al. NEJM 2011
0
10
20
30
40
50
60
70
80
Response guidedLI BOC+ PEG2b+ Riba
63% 66%
38%
PEG2b+ Riba
(48 wks)
LI BOC+ PEG2b
+ Riba(48 wks)
TVR TVR SOC BOC BOC SOC

Triple-Therapies: Improved SVR ratesTreatment-experienced Genotype 1 pts.
REALIZE(+/- Lead-in) TVR 12 wks + PEG2a + Riba
48 weeks
RESPOND-2/PROVIDE*Lead-in (+/-RGT) BOC + PEG2b + Riba
36 / 48 weeks
0
20
40
60
80
100
Sust
aine
d vi
rolo
gic
resp
onse
15%24%
REL
57%
31%
86%
TVR SOC
5%
P-NR NULL
Relapser (REL): negative at end-of-treatment but relapse thereafterPartial Non-Responder (P-NR): ≥2log wk12 but pos HCV RNA wk 24Null-Responder (NULL): <2log wk 12
TVR SOC TVR SOC 0
20
40
60
80
100
7%
29%
REL
BOC SOC
P-NR NULL
BOC SOC
75%
52%
Bacon et al., NEJM 2011*PROVIDE study, Vierling et al., AASLD 2011Zeuzem et al., NEJM 2011
36%*

0
1
2
3
4
5
6
GT 1 GT 2 GT 3 GT 4 GT 5 GT 6
Antiviral activities of Telaprevir / Boceprevir in other HCV genotypes
Mean maximum log10 HCV RNA decline during mono-therapies 7-14 days
Telaprevr 750mg TID; Reesink et al., Gastro 2006, Foster et al., Gastro 2011, Benhamou et al., EASL 2009
HC
V R
NA
log1
0 de
clin
e
4,43,9
0,5 0,9
Boceprevir 400mg TID (current dose 800mg TID); Sarrazin et al., Gastroenterology 2007; Silva et al., APASL 2011
2,11,4
1,7no data

Triple-Therapies: HIV co-infectionLimited efficacy and long duration of PEG/R
Characteristic APRICOT1 ACTG 50712 RIBAVIC3 Barcelona4
Number enrolled 868 133 412 95
PEG-IFN 2a 2a 2b 2b
RBV 800mg 600mg up to 1g 800mg 800mg up to 1.2g
HIV and CD4 status
>200/mm3 or 100–200/mm3
if HIV-RNA <5,000
copies/mL
>100/mm3 + HIV-RNA <10,000
copies/mLor >300/mm3, tx
naïve + not starting ART during trial
>200/mm3>250/mm3 and
HIV-RNA <10,000 copies/mL
ALT “elevated” NA NA >1.5 ULN
Genotype 1, % 60–61 77–78 48 49
Bridging fibrosis or cirrhosis, % 15–16 9–11 (cirrhosis) 39 30
SVR, n/N (%) Genotype 1 51/176 (29) 7/51 (14) 21/123 (17)* 22/59 (38)*
1.Torriani FJ, et al. N Engl J Med 2004;351:438–450 2. Chung RT, et al. N Engl J Med 2004;351:451–459
3. Carrat F, et al. JAMA 2004;292:2839–2484 4. Laguno M, et al. AIDS 2004;18:F27–36
*Genotype 1 or 4IFN: interferon; RBV: ribavirin; ALT: alanine aminotransferaseULN: upper limit of normal; SVR: sustained virologic response

Triple-Therapies: HIV co-infectionPotential of DDIs with Telaprevir/Boceprevir
Telaprevir Boceprevir
RTV1,2 ↓ TVR ↑ RTV ↓ BOC
Peg-IFN2 n/a ↔ BOC
EFV2,3 ↓ TVR ↓ EFV ↓ BOC ↑ EFV
TDF2,3 ↓ TVR ↑ TDF ↑ BOC ↑ TDF
ATV/r3 ↓ TVR ↑ ATV n/a
DRV/r3 ↓ TVR ↓ DRV n/a
FPV/r3 ↓ TVR ↓ FPV n/a
LPV/r3 ↓ TVR ↔ LPV n/a
Methadone4 ↔ TVR ↓ R-methadone (↑ free fraction) n/a
Cyclosporine5 ↔ TVR ↑ cyclosporine n/a
Tacrolimus5 ↔ TVR ↑ tacrolimus n/a
Midazolam2 n/a ↑ MDZ
Diflunisal2 n/a ↔ BOC
Clarithromycin2 n/a ↔ BOC
Ketoconazole2,6 ↑ TVR ↑ KET ↑ BOC
Oral contraceptives2,6 ↓ EE ↔ NOR ↑ DRSP ↓ EE
Renal impairment7 ↔ TVR n/a
1. Garg V, et al. CROI 2011. Abstract 629; 2. Kassera C, et al. CROI 2011. Abstract 118; 3. van Heeswijk R, et al. CROI 2011. Abstract 1194. van Heeswijk R, et al. J Hepatol 2011;54(Suppl. 1): S491; 5. Garg V, et al. ATC 2011. Abstract 65; 6. Telaprevir French cohort
ATU Protocol. Available at http://www.afssaps.fr; 7. van Heeswijk R, et al. J Hepatol 2011;54(Suppl. 1): S492

Triple-Therapies: HIV co-infectionTelaprevir Triple-Therapy Study
Dieterich et al., CROI 2012
Part A: no ART
Follow-upPR48 (control) PR
SVRPbo + PR
T/PR TVR + PR Follow-upSVR
PR
Follow-upPR48 (control) PR
SVRPbo + PR
T/PR TVR + PR Follow-upSVR
PR
Part B: ART (EFV/TDF/FTC or ATV/r + TDF + FTC or 3TC)
(EFV)=efavirenz; (TDF)=tenofovir; (FTC)=emtricitabine; (ATV/r)=ritonavir-boosted atazanavir; (3TC)=lamivudine; (T) TVR=telaprevir 750 mg q8h or 1125 mg q8h (with EFV); Pbo=Placebo; (P) Peg-IFN=pegylated interferon alfa-2a (40 kD) 180 µg/wk; (R) RBV=ribavirin 800 mg/day or weight-based (1000 mg/day if weight <75 kg, 1200 mg/day for if weight ≥75 kg; France, Germany, n=5 patients)Roche COBAS® TaqMan® HCV test v2.0, LLOQ of 25 IU/mL, LOD of <10 IU/mL
240 48 72Weeks 12 36 60
SVR12
SVR12
SVR12
SVR121:1
2:1

Triple-Therapies: HIV co-infectionTelaprevir Triple-Therapy Study
Dieterich et al., CROI 2012
Pat
ient
s w
ith S
VR
(%)
No ART EFV/TDF/FTC ATV/r/TDF/FTC Total
n/N = 5/7 11/16 12/15 28/38
T/PR PR2/6 4/8 4/8 10/22
71
33
69
50
80
50
74
45
0
10
20
30
40
50
60
70
80
90
100
*Patient was defined as SVR12 if HCV RNA was < LLOQ in the visit window

Triple-Therapies: HIV co-infectionBoceprevir Triple-Therapy
Mallolas et al., EASL 2012

Triple-Therapies: HIV co-infectionBoceprevir Triple-Therapy
Mallolas et al., EASL 2012

Triple-Therapies: HIV co-infectionBoceprevir Triple-Therapy
Mallolas et al., EASL 2012

Telaprevir / Boceprevir Triple-TherapiesAdverse events
Bacon et al. NEJM 2011, Poordad et al. NEJM 2011, Jacobson et al. NEJM 2011, Zeuzem et al. NEJM 2011, Sherman et al. NEJM 2011
% of patients (Phase II / III-studies) Telaprevir/PRN = 1.346
Placebo/PRN = 764
Discont. Telaprevir / Placebo due to AEs 14 4Pruritus 51 26Rash 55 33Nausea 39 29Diarrhea 26 19Anorectal symptoms 26 6Anemia 29 12
% of patients (Phase III-studies) Boceprevir/PR N = 1.057
Placebo/PR N = 443
Discont. entire treatment due to AEs 8-16 2-16Anemia 43-49 20-29Dysgeusia 37-45 11-18Neutropenia (500 to < 750/mm3) 19-25 9-14
Dry skin 21 8

Triple-TherapyPredictors of response
Predictors for lower SVR
• Non-Response PEG-IFN / Ribavirin pre-treatment
• Non-CC IL28B-Genotype (rs12979860)
• High HCV-RNA baseline level (> 8 x 105 IU/ml)
• Advanced Fibrosis (F3 / F4)
• Low LDL
• HCV-Subtype 1a (approx. 10% lower SVR rate)
Importance for treatment algorithm in mono-infected pts. Poordad et al. NEJM 2011 Zeuzem et al. NEJM 2011
Bacon et al. NEJM 2011Berg et al., AASLD 2011
Jacobson et al. NEJM 2011

IL28B (rs12979860)Correlation with SVR / Importance for treatment
algorithm?
Treatment-naive pts. without cirrhosis: Shortening of Triple-Therapy in patients
with IL28B CC-genotype ?
Therapy Boceprevir(SVR)
Telaprevir (SVR)
PEG/R (SVR)
Tx naive(RGT-arms)
CC 82% 90% 64 − 78%CT/TT 62% 72% 25 − 27%
Tx experienced(48 weeks)
CC 77% 79% 29 − 46%CT/TT 73% 61% 15 − 26%
Poordad et al. EASL 2011, Pol et al. EASL 2011

Hézode C, et al. N Engl J Med 2009;360:1839–50
T12P12 (n=78)(no RBV)
PR48 (n=82)
T12PR12 (n=82)
0Weeks
24 4812 36
TVR + Peg-IFN
Peg-IFN + RBV Placebo
+ Peg-IFN + RBV
TVR + Peg-IFN +
RBV Peg-IFN + RBV
TVR + Peg-IFN
+ RBV
T12PR24 (n=81)
46%
69%
60%
36%
SVR rate
Telaprevir Phase 2 Study (PROVE2)SVR Rates

T12P12 (n=78)(no RBV)
PR48 (n=82)
T12PR12 (n=82)
0Weeks
24 4812 36
TVR + Peg-IFN
Peg-IFN + RBV Placebo
+ Peg-IFN + RBV
TVR + Peg-IFN +
RBV Peg-IFN + RBV
TVR + Peg-IFN
+ RBV
T12PR24 (n=81)
46%
69%
60%
36%
SVR rate
Bronowicki et al, EASL 2012, poster (1094)
The IL28B genotype (rs12979860) was determined in specimens at the PROVE2 French sites
Telaprevir Phase 2 Study (PROVE2)SVR Rates

Short treatment in IL28B CC patients
T12P12 (n=78)(no RBV)
PR48 (n=82)
T12PR12 (n=82)
0Weeks
24 4812 36
TVR + Peg-IFN
Peg-IFN + RBV Placebo
+ Peg-IFN + RBV
TVR + Peg-IFN +
RBV Peg-IFN + RBV
TVR + Peg-IFN
+ RBV
T12PR24 (n=81)
46%
69%
36%
SVR rate
SVR: 100% for 12/12 patients with IL28B CC2
Bronowicki et al, EASL 2012, poster (1094)
Prospective ongoing study (CONCISE) for 12 weeks triple therapy with TVR BID in treatment naïve genotype 1, CC patients

Triple TherapyNew response definitions
Abbreviation Meaning Comment
SVR Sustained virologic response HCV-RNA undetectable 24 weeks after end of treatment
Relapse Relapse after end of treatment
Partial Non-Response
Week 12 ≥ 2 log-decline of HCV-RNA but HCV RNA detectable at week 24
Null-Response < 2 log-decline of HCV-RNA at week 12
RVR rapid virologic response HCV-RNA negative at week 4
eRVR (TVR) extended RVR Telaprevir HCV-RNA negative at week 4 and 12
eRVR (BOC) extended RVR Boceprevir HCV-RNA negative at week 8 and 24
Breakthrough Virologic breakthorough HCV-RNA positive after undetectability orincrease of > 1 log step

= undetectable HCV RNA
Boceprevir Telaprevir
TW8 TW28 TW48TW24TW4 TW36TW0
32W‐BOC4W‐LI 12W PR
Naive24W‐BOC4W‐LI
Part.Resp.Relapser
Null Resp.F4 Fibrosis
44W‐BOC4W‐LI
NaiveRelapser
Part.Resp.Null Resp.
F4 Fibrosis
32W‐BOC4W‐LI 12W PR
TW24 TW48TW12TW4TW0
36W PR
12W‐TVR 12W PR
12W‐TVR
+/-
36W PR12W‐TVR
36W PR12W‐TVR
Treatment algorithms for HCV mono-infected patients: Lead-in

Lead-in versus no Lead-inIndividual decision
Individual decision on
further treatment
Tolerability ofPEG-IFN /
Ribavirin aloneduring Lead-in
Adherenceon PEG-IFN /
Ribavirin alone during Lead-in
Treatment experienced patient with Null-
Response, F4 and < 1 log-decline during
Lead-in
Treatment-naive patient with RVR
during Lead-in and possibility of 24 weeks PEG/Riba

TVR/BOC sparing treatmentRVR during lead-in with PEG/Riba
Rates of RVR (HCV RNA undetectable / <12-50 IU/ml at week 4) in treatment-naive patients with chronic hepatitis
genotype 1 infection and treatment with PEG-IFN / Ribavirin alone range from 12-65% in different studies from the U.S.,
Europe and Asia
Response group
INDIV-2 Study (genotype 1, treatment-naïve)PEG-Interferon alfa 2b plus Ribavirin
Treatment duration (weeks)
ITT population (n=398) PP population (n=346)
HCV RNA negative* at
Baseline viral load
n (%) SVR (%) n SVR (%)
week 4 <800.000 IU/ml
24 41 (10) 36 (88) 36 36 (100)
week 4 ≥800.000 IU/ml
30 7 (2) 6 (86) 6 6 (100)
* HCV RNA undetectable by TMA Assay (<5-10 IU/ml)
Sarrazin et al. Gastroenterology 2011
Fried et al., J Hepatol 2011, McHutchison et al., NEJM 2009, Ferenci et al., Gastroenterology 2008, Mangia et al., Hepatology 2008, Berg et al., Gastroenterology 2006, Sarrazin et al., Gastroenterology 2011, Sanchez-Tapias et al., Gastroenterology 2006,
Bronowicki et al., Gastroenterology 2006, Buti et al., Hepatology 2010, Yu et al., Hepatology 2008, Liu et al., Clin Infect Dis 2008

Boceprevir – Stopping rulesBoceprevir
Stopping rules for Boceprevir :HCV RNA > 100 IU/ml at TW12HCV RNA detectable at TW24
TW28TW24TW4 TW36TW0
32W‐BOC4W‐LI 12W PR
Naive24W‐BOC4W‐LI
Part.Resp.Relapser
Null Resp.F4 Fibrosis
44W‐BOC4W‐LI
32W‐BOC4W‐LI 12W PR
TW12

Stopping rules Boceprevir Triple
Jacobson et al. AASLD 2011
Treatment naive: SPRINT-2-Study, n = 734 Entire treatment was discontinued within the study if HCV RNA was detectable at week 24
Week 8 Week 12Rate of pts.
with stopmissed SVR
Rate of pts.with stop
missed SVR
≥ 50 IU/ml 147 (20%) 26 78 (11%) 4≥ 100 IU/ml 120 (16%) 16 65 (9%) 0< 3 log-decline 34 (5%) 1 34 (5%) 0
Retrospective analysis for introduction of early stopping rules

Telaprevir – Stopping rules
Stopping rules for Telaprevir:HCV RNA > 1000 IU/ml at TW4 or TW12HCV RNA detectable at TW24
Telaprevir
NaiveRelapser
Part.Resp.Null Resp.
F4 Fibrosis
TW24 TW48TW12TW4TW0
36W PR
12W‐TVR 12W PR
12W‐TVR
+/-
36W PR12W‐TVR
36W PR12W‐TVR

Adda et al. HepDart 2011
Stopping rules Telaprevir Triple
Treatment-naive: ADVANCE-Study, n = 903 Telaprevir was discontinued within study if HCV-RNA > 1.000
IU/ml at week 4 and entire treatment was discontinued if < 2 log decline of HCV RNA at week 12 / HCV-RNA positive at week 24
Week 4 Week 12Rate of pts.
with stopmissed
SVRRate of pts.
with stopmissed
SVR
≥ 100 but< 1.000 IU/ml 19 (2%) 5 10 (1%) ?
≥ 1.000 IU/ml 15 (2%) 0 9 (1%) 0
Retrospective analysis for introduction of early stopping rules

Viral kinetics of triple-therapy
Adda et al. HepDart 2011
104
105
106
107
108
1043
102
101
0 2 4 6 8 10 12Weeks /therapy
HC
V-R
NA
IU/m
l
104
105
106
107
108
1043
102
101
0 2 4 6 8 10 12Weeks /Therapy
HC
V-R
NA
IU/m
l
Treatment naive (n = 15) Treatment experienced (n = 15)

= undetectable HCV RNA
Boceprevir Telaprevir
TW8 TW28 TW48TW24TW4 TW36TW0
32W‐BOC4W‐LI 12W PR
Naive24W‐BOC4W‐LI
Part.Resp.Relapser
Null Resp.F4 Fibrosis
44W‐BOC4W‐LI
NaiveRelapser
Part.Resp.Null Resp.
F4 Fibrosis
32W‐BOC4W‐LI 12W PR
TW24 TW48TW12TW4TW0
36W PR
12W‐TVR 12W PR
12W‐TVR
+/-
36W PR12W‐TVR
36W PR12W‐TVR
Telaprevir / Boceprevir Treatment algorithmsDetermination of extended rapid virologic response

Response guided Triple-TherapieDefinition of extended RVR
Telaprevir
eRVR HCV RNA undetectable* at week 4 and 12
* Below the limit of detection (approx. 10 IU/ml)
Boceprevir
eRVR HCV RNA undetectable* at week 8 and 24
* Below the limit of detection (approx. 10 IU/ml)
Importance of residual viremia? Differences between different HCV RNA assays?
Boceprevir & Telaprevir Studies: HPS/Cobas TaqMan Assay

Response guided Triple TherapyDefinitions of extended RVR
HCV RNA concentrations <25 IU/ml are frequently observed during TVR/BOC triple-therapies (52-67% in Phase 3 studies with TVR/BOC until week 4/8)
Overall increased probability of treatment failure in patients with residual viremia (<25 IU/ml but detectable HCV RNA) at week 4/8 during Telaprevir / Boceprevir triple-therapies
Harrington et al., Hepatology 2011

Response guided Triple TherapyDefinitions of extended RVR
Higher Relapse-Rates in patients with residual viremia(<25 IU/ml) at week 4 / 12 in patients with shortened treatment duration (24 weeks).
Harrington et al., Hepatology 2011
Study Time Duration SVR RelapseBoceprevirSPRINT-1
<25 IU/ml wk. 8 28 wks 5/13 (38%) 5/10 (50%)48 wks 9/12 (75%) 0/9 (0%)
negative wk. 8 28 wks 53/62 (85%) 4/57 (7%)48 wks 62/66 (94%) 0/62 (9%)
Telaprevir 104 / PROVE1/2
<25 IU/ml wk. 4 24 wks 6/15 (40%) 4/9 (44%)48 wks 4/7 (57%) 2/6 (33%)
negative wk. 4 24 wks 89/120 (74%) 6/88 (7%)48 wks 49/64 (77%) 0/44 (0%)

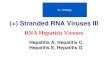
International commercially available HCV RNA assays
100
101
102
103
104
105
106
107
108IU/ml
615 5005-10 50 10
TMA bDNA kPCRVersantTM
Siemens(CE/FDA für TMA/bDNA)
qual. quant. real-time AmplicorTM vs2 TaqManTM
Roche Diagnostics(CE/FDA)
real-timeRealTime HCVTM
Abbott(CE/FDA)
101034
HCV RTartusTM
Qiagen(CE)

Response guided Triple TherapyDifferences between assays
Fevery et al., EASL 2012
• Samples obtained from the TMC435 PILLAR study (TMC435-C205)
o Treatment-naïve patients received once-daily TMC435 in combination with PegIFNα-2a/RBV
o 79-86% of TMC435-treated patients were eligible for shortened treatment of 24 weeks, of whom 85-96% achieved SVR24
• In PILLAR, HCV RNA was assessed using Roche High-Pure-System/COBAS® TaqMan assay v2 (HPS)
• A total of 1411 plasma sampleswith sufficient volume were selected from 290 of 309 TMC435-treated patients, and re-analysed in a blinded fashion with the Abbott RealTime(ART) assay
Visit Number of samplesScreening 113Baseline 16Day 3 28Week 1 135Week 2 186Week 3 164Week 4 261Week 6 108Week 8 140Week 12 260Total 1411

Differences between HCV RNA AssaysOverall HCV RNA quantification
Fevery et al.,EASL 2012
1 2 3 4 5 6 7Roche TaqMan (HPS), log10 IU/mL
Abb
ott R
ealT
ime
(AR
T), l
og10
IU/m
L
(r2=0.978)
LLOQ ART
LLO
Q H
PS
N=326
1
2
3
4
5
6
7
*censored values excluded

Fevery et al., EASL 2012
Abbott RealTime (ART)
<12 IU/mLnot detected
<12 IU/mLdetected
12 IU/mLbut
<25 IU/mL25 IU/mL
Roc
he T
aqM
an(H
PS)
<25 IU/mL not detected 549 181 28 8
<25 IU/mLdetected 35 128 86 65
25 IU/mL 0 5 19 307
217/766 (28.3%)
• 217/766 (28.3%) samples from different time points with HCV RNA undetectable by HPS had detectable/quantifiable HCV RNA by ART
• 35/584 (6.0%) samples undetectable by ART had detectable/quantifiableHCV RNA by RCT
• For both assays, the majority of these discrepant samples had HCV RNA levels <25 IU/mL
35/584 (6.0%)
Differences between HCV RNA AssaysHCV RNA undetectability

Fevery et al., EASL 2012
Differences between HCV RNA AssaysAssessment of rapid virologic response
At Week 4, 197/261 (75.5%) samples were undetectable by HPS whereas 129/261 (49.4%) were undetectable and 79/261 (30.3%) <12 IU/mL detectable by ART, leading to a different determination of RVR in 68/261 (26.1%) of cases
75,5
16,58,0
0
20
40
60
80
100
Not detected <25 IU/mLdetected
≥25 IU/mL
Abbott RealTime (ART)
49,4
30,3
7,7 12,6
0
20
40
60
80
100
Notdetected
<12 IU/mLdetected
≥12 and<25 IU/mL
≥25 IU/mL
75.5% <25 IU/mL undetectable 49.4% <12 IU/mL
undetectable
79.7% <12 IU/mL
Prop
ortio
n of
pat
ient
s, %
Prop
ortio
n of
pat
ient
s, %
Roche TaqMan (HPS)

Summary
New era with Boceprevir / Telaprevir triple-therapies- significant improvement of SVR rates- genotype 1 only- high efficacy also in HIV co-infected patients- complex management, high pill burden, additionalAEs, DDI and limited efficacy in non-responders
Response guided therapy according to HCV RNA viral kinetics (stopping rules, eRVR)
Lead-in may be used for testing tolerability, PI sparing and prediction of non-response to PIs
IL28B may be used to tailor treatment in the future
Importance of HCV RNA assays