Embed Size (px)
Citation preview

Treatment of Adult ALL
Vinod Pullarkat, MD, MRCP
Associate Professor
Hematology and Hematopoietic Cell Transplantation

Epidemiology
• Around 6000 cases annually in the US
• Half the cases in childhood and teen age
• About 75% are B-ALL in adults
• Higher incidence rates in Hispanics (IRR of 1.9 age 20-54)
• Higher incidence of Ph-like subset in Hispanics related to
inherited GATA-3 variant
Pullarkat ST et al. Cancer Epidemiol Biomarkers Prev 2009; 18: 611-5
Perez-Andreu et al. Blood 2015; 125: 680-86

Perez-Andreu et al. Blood 2015; 125: 680-86
Ethnic variation in Ph-like ALL

Average annual age-specific incidence and mortality rates for ALL, 1973-2009, U.S. National Cancer Institute Surveillance
Epidemiology and End-Results (SEER) program (www.SEER.cancer.gov).
Age-specific incidence of ALL

Hunger SP, Mullighan CG. N Engl J Med 2015; 373: 1541
Outcome of pediatric ALL

5-54 yrs
Secular trends of ALL annual relative survival rates in patients diagnosed at 55+ years of age, 1973-2009,
Surveillance, Epidemiology and End-Results Program. (www.SEER.cancer.gov).
55+
Survival of adult ALL

Moorman AV. Blood Rev 2012; 26: 123
Cytogenetics of ALL

Good Risk Intermediate Risk Poor Risk
Hyperdiploidy (51-65 chr)
t(12;21)/ETV6-RUNX1 fusion
t(1;19)(q23;p13.3)
14q32/IGH translocations
Deletion 6q
Abnormal 9p
Abnormal 11q (not MLL translocations)
Dup 1q
Monosomy 7
dic(9;20)(p13;q11
dic(9;12)(p13;p11)
Normal karyotype
Any other abnormality
t(9;22), t(4;11)
Other MLL translocations
iAMP21
Near haploidy (<30 chr)
Low hypodiploidy/triploidy (30-39)/60-78
chr)
t(17;19)(q22;p13.3)
Abnormal 17p
Loss of 13q
Complex karyotype*
*defined as ≥ 5 unrelated chromosomal abnormalities in the absence of other established abnormality
Cytogenetic risk classification

Ph-like ALL
• Gene expression profile similar to BCR-ABL1 (Ph+) ALL
• 10% childhood and up to 30% adult ALL
• More common with Hispanic and native American ancestry
• IKZF1 alterations common
• Activation of various receptor kinases including CRLF2, ABL,
JAK2, EPOR
• Associated with poor outcome

Hunger SP, Mullighan CG. Blood 2015; 125: 3977
Genetics of Ph-like ALL

Outcome of Ph-like ALL
Roberts et al. N Engl J Med
2014; 371: 1005-15
Treat adults like children
• Outcomes of adult ALL are superior when treated with pediatric-
type regimens compared to ‘adult’ regimens e.g. hyper CVAD
• Long term EFS and OS in 60- 70% range
• Results similar for T-cell and pre B-ALL
• Allogeneic HCT cannot be uniformly recommended as
consolidation therapy in newly diagnosed adult ALL

Principles of pediatric-type adult ALL regimens
• Mostly based on Berlin Frankfurt Munster (BFM) backbone
• Multiple cycles of non-cross resistant agents
• Early and frequent CNS prophylaxis
• Repeated doses of L-asparaginase
• Prolonged maintenance
• Less myelosuppression
• Higher cumulative doses of active agents

Adolescents and Young Adults (AYA)
• NCI definition: 15-39 years old
• Better definition : ? Up to Age 60
• Pediatric-type regimens have been safely administered up to
age 60

Pediatric type regimens for AYA
Boissel N, Sender LA. JAYAO 2015; 4: 118

Pediatric vs. adult regimens for AYA with ALL
Boissel N, Sender LS. JAYAO 2015; 4: 118

4 yr OS: 67% (n=92) 4 yr DFS: 69% (n=78)
DeAngelo DJ et al. Leukemia 2015; 29: 526
Age 18-50
DFCI Pediatric ALL consortium regimen

Outcome of USC ALL regimen for Philadelphia–negative patients.
Dan Douer et al. JCO 2014;32:905-911
©2014 by American Society of Clinical Oncology
OS DFS
Age 18-57 yrs

Stock W et al. Proc ASH 2014 Abstract 796
US Intergroup C10403

Kantarjian H et al. Cancer 2004; 101; 2788-2801
Hyper CVAD for ALL
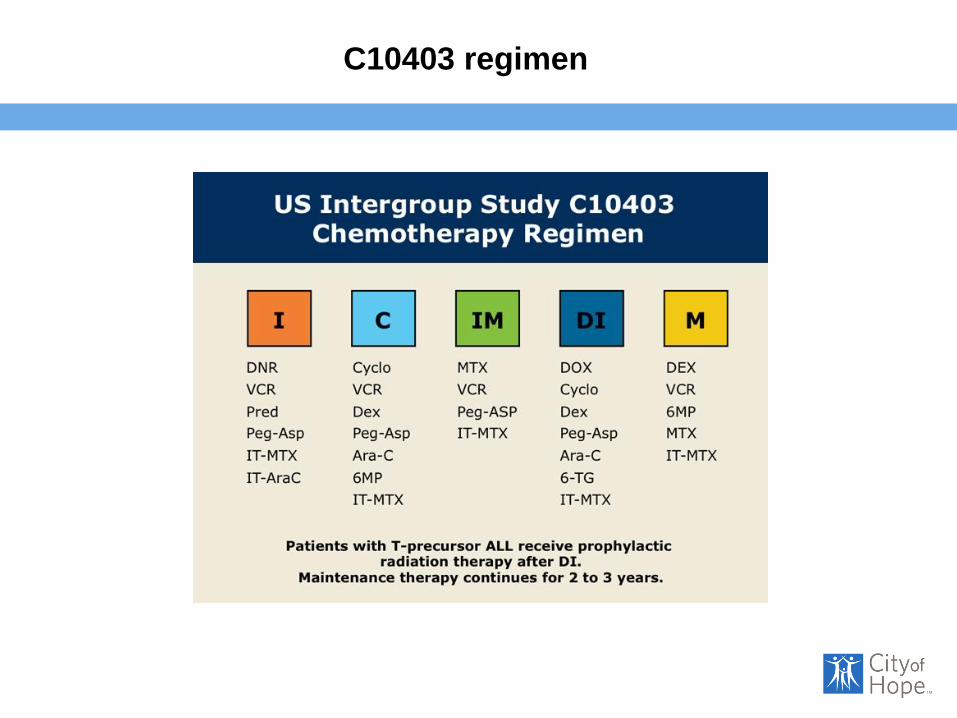
C10403 regimen

USC ALL regimen
Dan Douer et al. JCO 2014;32:905-911
©2014 by American Society of Clinical Oncology
= PEG-asparaginase 2000U/m2

Aldoss I, Pullarkat V . Contemporary management of ALL .
Pullarkat V (Ed)
Jaypee Publishing.
USC ALL regimen

Curran E and Stock W. Blood 2015; 125:3702
1. Aldoss I, Pullarkat V . Contemporary Management of ALL .
Pullarkat V (Ed)
Jaypee Publishing. 2. Douer D et al. J Clin Oncol 2014;32:
905
C10403 USC ALL
Role of asparaginase
• Key drug in pediatric-type adult ALL regimens
• PEG-formulation associated with less hypersensitivity and longer
half life
• Doses of PEG-Asp 2000-2500 U/m2 well tolerated up to 60 years of
age
• Pharmacokinetic dosing may be preferable based on
asparaginase level or asparagine depletion
• Premedication reduces allergic reactions

Stock W et al. Leuk Lymphoma 2011; 52: 2237-2253
Toxicity of asparaginase

Managing asparaginase toxicity
• Hyperbilirubinemia more common in Cycle 1 (OR 22.5) No cases
of hepatic failure in 522 doses administered
• Hepatotoxicity does not preclude readministration of
asparaginase
• Hepatotoxicity was associated with higher BMI and hispanic
ethnicity
• Bleeding and thrombosis extremely rare when cryoprecipitate use
is limited to fibrinogen 60mg/dl. More common in cycle 1
Aldoss I et al. Eur J Haematology 2015 Jun 10. doi:
10.1111/ejh.12600. [Epub ahead of print]

Managing asparaginase toxicity
• Hypersensitivity, clinical pancreatitis and venous thrombosis are
contraindications to retreatment with asparaginase
• Bleeding rare when thrombocytopenia is avoided
• Routine use of cryoprecipitate, FFP and ATIII concentrate is not
required
• Allergic reactions are rare with use of premedications and
steroids

Optimizing asparaginase therapy
• Monitoring asparaginase level; now clinically available
• Hypersensitivity associated with antibody production:
Switch to Erwinia asparaginase
• Silent hypersentivity: ? switch to Erwinia asparaginase

Risk stratification of ALL
• Conventional factors (e.g. age, WBC count, immunophenotype)
have limited value
• High risk cytogenetics include Ph chromosome, hypodiploidy,
MLL rearrangement, iAMP21
• Ph-like ALL and IKZF1 alterations have poor prognosis
• MRD assessment critical in risk stratification

Beldjord et al. Blood 2014; 123: 3739
IKZF1 alterations in ALL
Ph- ALL
P=0.001

MRD to guide ALL therapy
• Detection of disease not detectable by light microscopy
• Detection of Immunoglobulin or T-cell receptor sequences by
PCR based methods or aberrant immunophenotype by multicolor
flow cytometry
• Detection limit in range of 10-3-10-6 (0.1-0.001%)
• Measurement at end of induction-2/Conslidation-1 (day 71-week
16)
• MRD persistence (≥ 10 -4) after consolidation-1 represents a high
risk group

van Dongen et al. Blood 2015; 125: 3996
MRD

MRD
PCR-based
detection
≥ 10-4
Gokbuget et al Blood 2012; 120: 1868
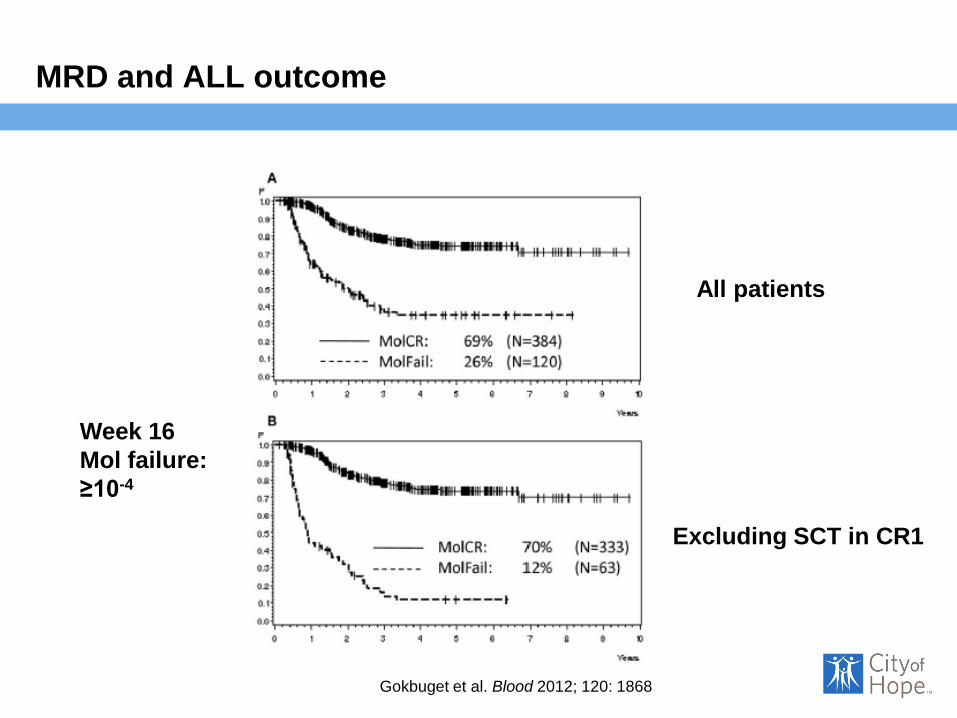
Gokbuget et al. Blood 2012; 120: 1868
MRD and ALL outcome
All patients
Excluding SCT in CR1
Week 16
Mol failure:
≥10-4

Dhedin et al. Blood 2015; 125: 2486
MRD and ALL outcome

Allo HCT in CR1
• Conventional risk factors do not predict allogeneic HCT outcome
• MRD is the most important predictor of HCT outcome
• Need to identify MRD+ patients who benefit from HCT
• Need to determine benefit of novel therapies in MRD+ patients
prior to HCT

AlloHCT vs. Pediatric-type Chemotherapy Ph-neg ALL in CR1
Seftel et al. Am J Hematol 2016 (Epub)
OS
DFS
RI
TRM
Age 18-50
Surv
ival P
robabili
ty
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Time (Years) from Date of Transplant
0 1 2 3 4 5 6 7 8 9 10 11
Cytogenetic Risk
Good/IntermediatePoor
Surv
ival P
robabili
ty
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Time (Years) from Date of Transplant
0 1 2 3 4 5 6 7 8 9 10 11
Cytogenetic Risk
Good/IntermediatePoor
Cum
ula
tive Incid
ence
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Time (Years) from Date of Transplant
0 1 2 3 4 5 6 7 8 9 10 11
Cytogenetic Risk
Good/IntermediatePoor
Cu
mu
lative
In
cid
ence
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Time (Years) from Date of Transplant
0 1 2 3 4 5 6 7 8 9 10 11
Cytogenetic Risk
Good/IntermediatePoor
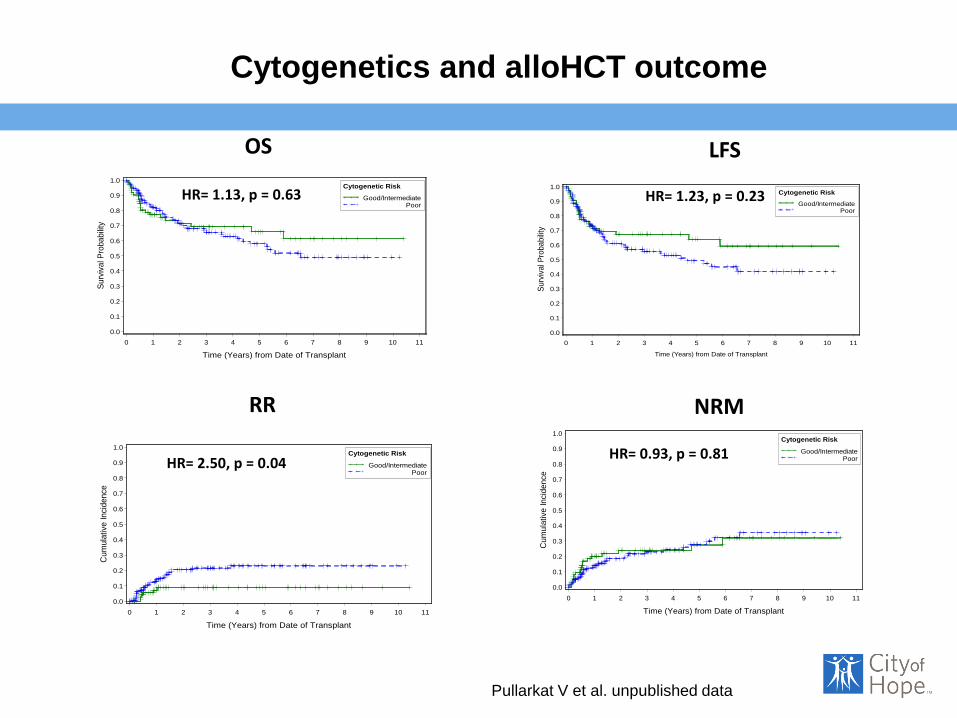
OS LFS
RR NRM
HR= 1.13, p = 0.63 HR= 1.23, p = 0.23
HR= 2.50, p = 0.04 HR= 0.93, p = 0.81
Pullarkat V et al. unpublished data
Cytogenetics and alloHCT outcome

Treatment of older adults (60y)
• Induction mortality can be high; supportive care during induction is critical
• Infection is a major cause of early mortality
• ? Limiting anthracycline use
• Preferable to avoid asparaginase in induction; can be given in subsequent cycles
• Consideration of RIC HCT in suitable candidates who remain MRD+

DFS OS
Outcome of older adults with ALL
Ribera J-M et al. Leuk Res 2016: 41: 12-20 Age 55yrs

RIC alloHCT for ALL
Mohty M et al. Blood 2010; 116: 4439-43
LFS
RR
N=576, RIC 127, MAC= 449
Age ≥ 45 yrs
NRM
OS
MAC
RIC
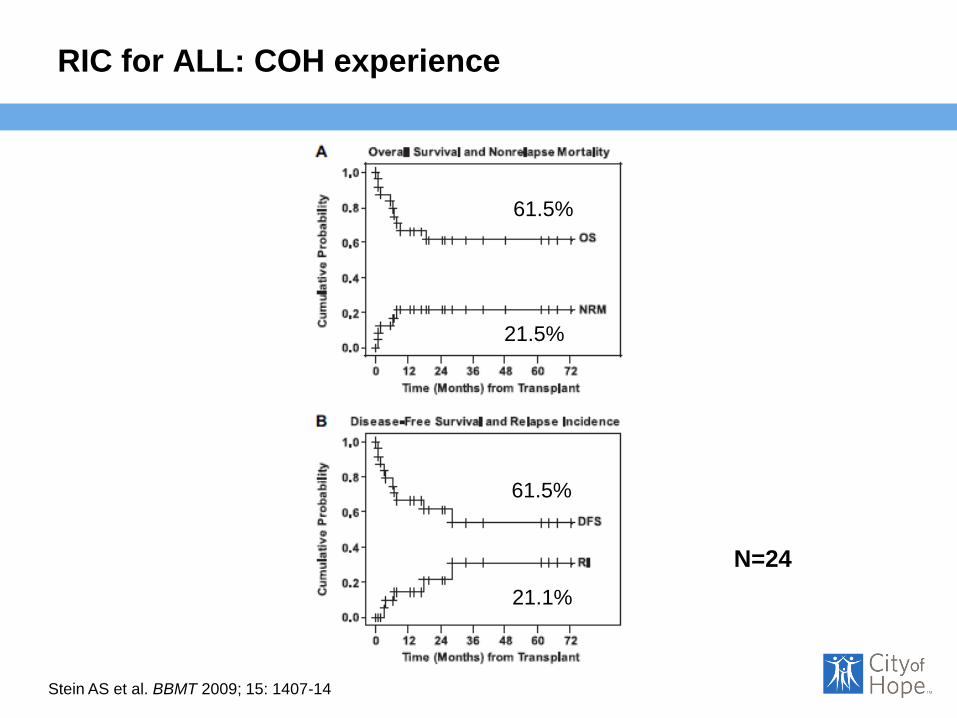
RIC for ALL: COH experience
N=24
61.5%
61.5%
21.5%
Stein AS et al. BBMT 2009; 15: 1407-14
21.1%

SWOG S1318
Ph + patients get dasatinib and
steroid induction followed by
dasatinib + blinatumomab
followed by dasatinib
maintenance
Cohort 2
Age ≥ 65

Mature B-cell ALL
• Needs brief duration, high intensity chemotherapy with growth factor support
• Rituximab critical component of such regimens
• CNS therapy critical
• No maintenance phase
• Active regimens include hyper R- CVAD, CODOX/M-IVAC, EPOCH-R
• Late relapses are rare

Hoelzer et al Blood 2014; 124: 3870-79 N=363 Age 16-85
Outcome of mature B-cell ALL
OS PFS

Thomas et al Cancer 2006; 106: 1569-80
Hyper CVAD for mature B-cell ALL

Rituximab
• CD20 expression in 30-50% B-ALL
• Has been used with hyper CVAD and pediatric type
regimens
• EFS improved in randomized study. OS better only
after excluding patients who underwent SCT
• Toxicity profile in ALL needs further study

Rituximab for Ph-neg ALL
Sebastien Maury et al. Blood 2015; 126: 1 (abstract)
Age 18-59
16-18 doses

Treatment of relapsed/refractory ALL
• Goal is to achieve CR with minimal toxicity in order to
proceed to allogeneic HCT in suitable candidates
• Options include chemotherapy reinduction,
blinatumomab, CAR-T cells, immunoconjugates

Outcome of relapsed adult ALL
Oriol A et al. Haematologica 2010; 95: 589-96

T-cell ALL
• Outcome appears similar to precursor B-ALL when
pediatric type regimens are used
• Immunophenotype not useful in assessing prognosis
• HCT outcome also appears similar to pre B-cell ALL
• Limited options for relapsed disease; Nelarabine only
approved agent
Treatment of Ph+ ALL
• Potent activity of TKIs have enabled use of lesser intensity
chemotherapy regimens with lower early mortality
• Allogeneic HCT in CR1 remains standard of care
• Autologous HCT (in patients with MMoR) or continued
chemotherapy with TKI may be option in patients not eligible for
alloHCT
• Role of maintenance TKI after HCT is unclear
Chalandon Y et al. Blood 2015; 125: 3711-19
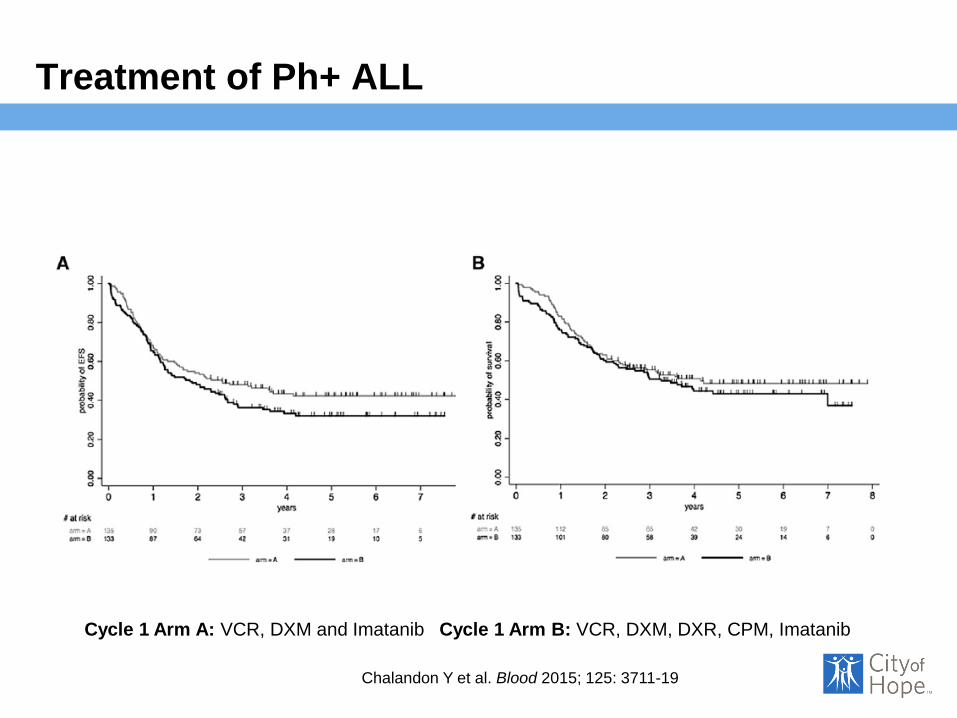
Treatment of Ph+ ALL
Chalandon Y et al. Blood 2015; 125: 3711-19
Cycle 1 Arm A: VCR, DXM and Imatanib Cycle 1 Arm B: VCR, DXM, DXR, CPM, Imatanib

Treatment of Ph+ALL
Chalandon Y et al. Blood 2015; 125: 3711-19

Pharmacogenomics of ALL therapy
• Results have been conflicting; multiple variants determine
efficacy and toxicity
• TPMT most relevant; requires lowering 6-MP dose by 30-70%
• Other variants could be important eg. SLCO1B1 for MTX toxicity,
CYP3A5 and CEP72 for VCR neuropathy
• Could be important to personalize therapy in future clinical trials
by NGS approach
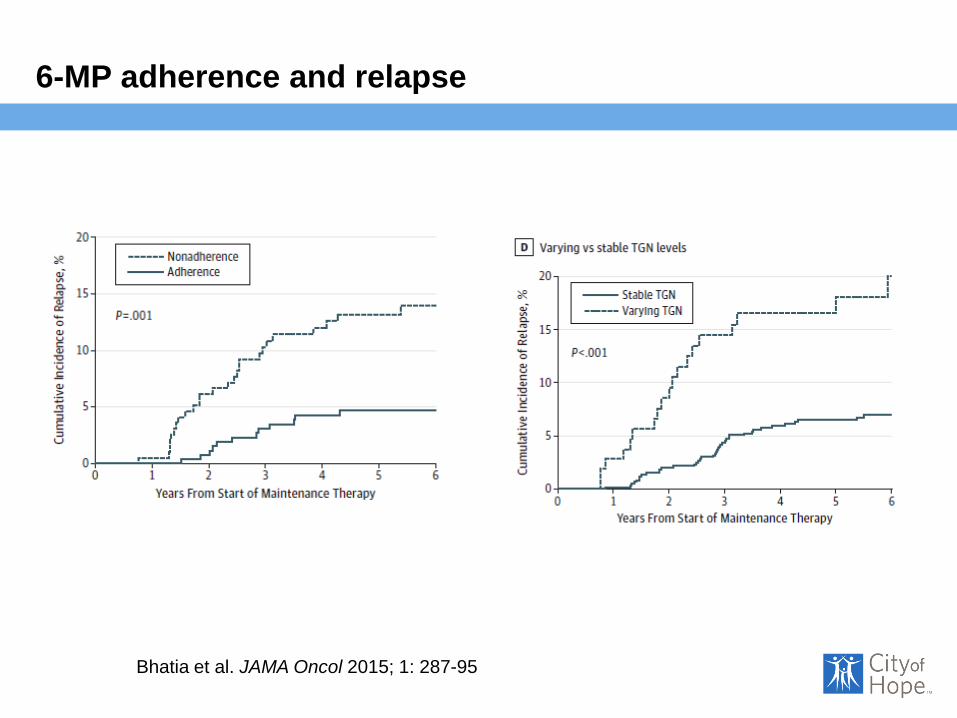
Bhatia et al. JAMA Oncol 2015; 1: 287-95
6-MP adherence and relapse

New agents for ALL
• Monoclonal antibodies (CD22: epratuzumab )
• Immunoconjugates (CD22: inotuzumab, CD19: denintuzumab)
• Bispecific antibodies (CD19/CD3: blinatunomab)
• CAR-T cells (CD19, CD22, CD123)
• Small molecules (NOTCH1, DOTL1)
Inotuzumab for R/R pre B-ALL
• Calicheamicin-CD22 antibody conjugate
• Calicheamicin released in cells; induces dsDNA breaks
• CD22 expression in 60-85 % of B-ALL
• Phase 2 trial: 58% response rate (CR + CRi) with median remission duration of 7 mo (n=90)
• 40% proceeded to allo HCT
• Weekly schedule was less toxic and associated with less VOD after alloHCT
Kantarjian et al. Cancer 2013; 119: 2728-36

Challenges to therapy of adults with ALL
• Most adults treated off protocol
• Lack of adult oncologists’ familiarity with pediatric ALL regimens
• Compliance with oral drugs
• Excessive concern about toxicity
• Therapy in tertiary care centers leads to better outcomes

Future directions
• Integrating novel agents into upfront therapy
• Standardizing approach to poor responders
• Identifying MRD+ patients who can be salvaged with alloHCT
• ? Mininizing chemotherapy side effects in good risk patients
• Application of pharmacogenomic data to guide therapy