Embed Size (px)
Citation preview

Treatment as preventionHow academic sector support for
programme implementation on life-long treatment and care
Kiat RuxrungthamProfessor of Medicine
Faculty of Medicine, Chulalongkorn University; and HIV-NAT, Thai Red Cross AIDS Research Center
Bangkok, Thailand

Ending AIDS PolicyHow and When?
THAILAND
Petchsri SirinirundAdvisor on HIV/AIDS Policy and ProgrammeDepartment of Disease Control, ThailandICAAP 11, 21 Nov 2013, Bangkok

50% reductionNew Infection
In 5 Years
End AIDSIn 20 years
Ending AIDS Working Definition1. New infection <1000/yr2. MTCT rate = 03. Target population treatment is well coverage
Adapted from Dr. Petchsri Sirinirund

Is Ending AIDS in Thailand feasible and implementable ?
Yes, But……….

Several Factors Support “Yes”1. The national AIDS committee has approved this policy
together with a significant supported budget
2. HIV treatment and care system have been well established and continuingly improved in Thailand
3. Thailand does have a very powerful e-registry database “National AIDS Program plus pr NAP+” and it has been used to monitor and improve the quality of care
4. Key relevant information are available: HIV care cascade, key-affected populations, key geographical targets
5. A large implementing research on test &treat in MSM among 8 provinces have been started. This will help to guide the other 27major effected provinces to implement their Test&Treat policy

Courtesy of Dr. Sorkit
This NAP+ databaseare driven by 1. Free ARV supply2. CD4, VL , DR cost
reimbursement

How to detect failure and DR?Time-course of HAART Failure
Clinical
Started HAART
1 2 3 4 5
Non-Adherence
Viral load
Resistance CD4 drop
Time (months –years)
Thai NHSO guidelines: VL q 6 mo, until VL<50, then q 1 yrCD4: q 6 mo, until CD4 >350, q 1 yr

Current Thailand NAP policy for free CD4 and VL monitoring support
Lab test Number of free tests per year
Viral load 2 /yr until undetectablethen 1 yearly
CD4 2 /yr until CD4 ≥350, then 1 /yr(Remark: in practice if CD4>500, we may not need to FU CD4, as long as the VL is <50 c/ml)
HIV Resistant test
When VL>1000 c/ml

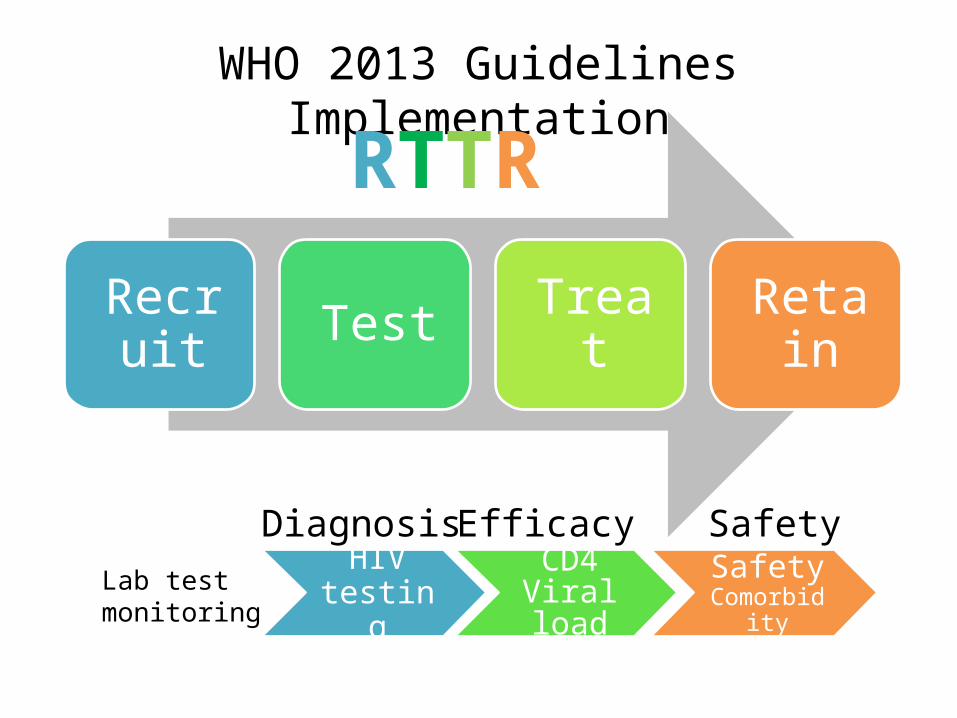
Recruit Test Treat Retain
WHO 2013 Guidelines Implementation
HIV testing
CD4Viral load
Safety Comorbidity
Diagnosis Efficacy SafetyLab testmonitoring
RTTR

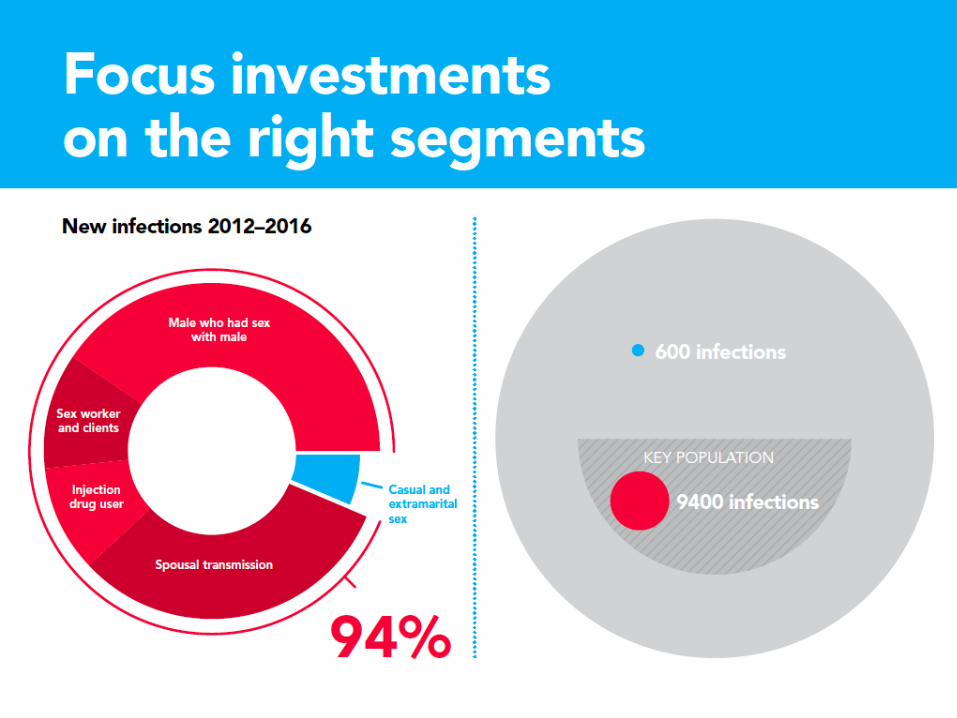

Key steps to Test and Treat Effective
MSM
CSWs+Clients PWIDs
Spousal Tm New Diagnosed Cases
With high CD4 count
Media
Reach Out Routine TestingAnnual Check up
How to significantly increase testing uptake?In at least 25 of 76 provinces (contributing to 2/3 of total new infection)
Getting ART
Indicators
No. of caseBL CD4 increased
Retained on ART with good VC
New infection rate monitoring
Time to Dx to ART% on ART
% Drop out% VL tested% VL<50% VF with 2nd Line
New infection <1000/y
Normalize HIV
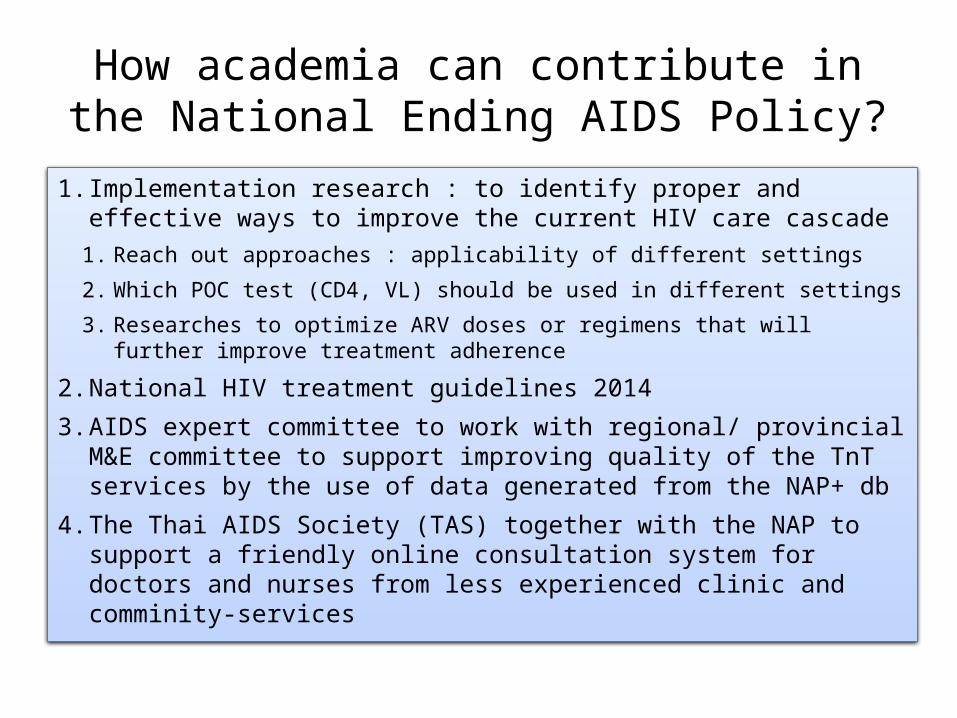
How academia can contribute in the National Ending AIDS Policy?
1. Implementation research : to identify proper and effective ways to improve the current HIV care cascade
1. Reach out approaches : applicability of different settings
2. Which POC test (CD4, VL) should be used in different settings
3. Researches to optimize ARV doses or regimens that will further improve treatment adherence
2. National HIV treatment guidelines 2014
3. AIDS expert committee to work with regional/ provincial M&E committee to support improving quality of the TnT services by the use of data generated from the NAP+ db
4. The Thai AIDS Society (TAS) together with the NAP to support a friendly online consultation system for doctors and nurses from less experienced clinic and comminity-services
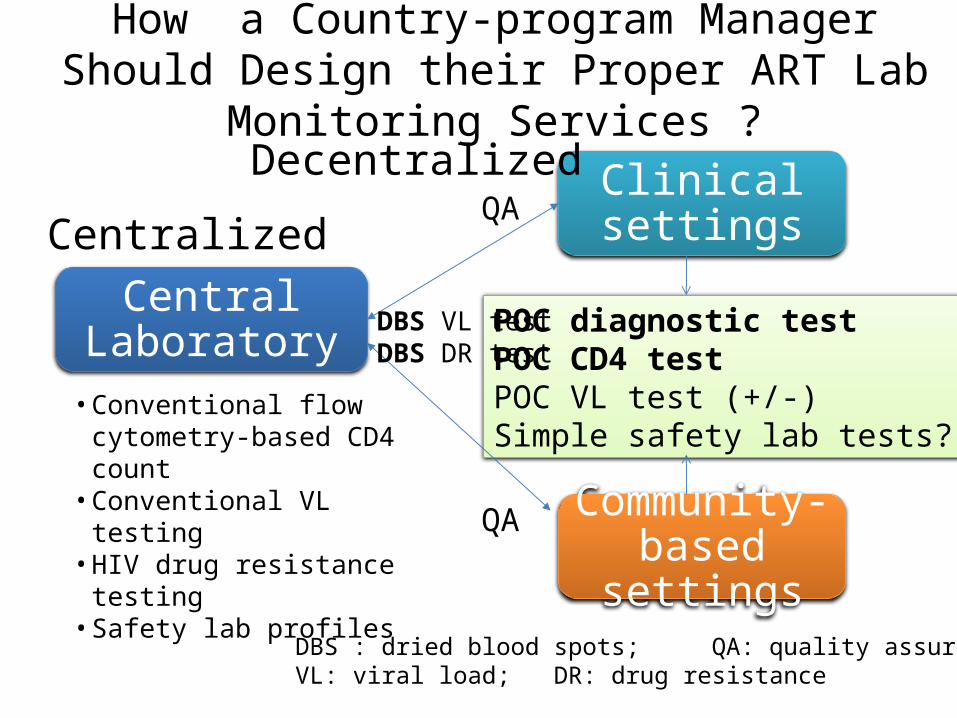
How a Country-program Manager Should Design their Proper ART Lab Monitoring Services ?
Central Laboratory
Clinical settings
Community-based settings
• Conventional flow cytometry-based CD4 count
• Conventional VL testing• HIV drug resistance testing• Safety lab profiles
POC diagnostic testPOC CD4 testPOC VL test (+/-)Simple safety lab tests?
DBS VL testDBS DR test
QA
QA
DBS : dried blood spots; QA: quality assuranceVL: viral load; DR: drug resistance
Centralized
Decentralized
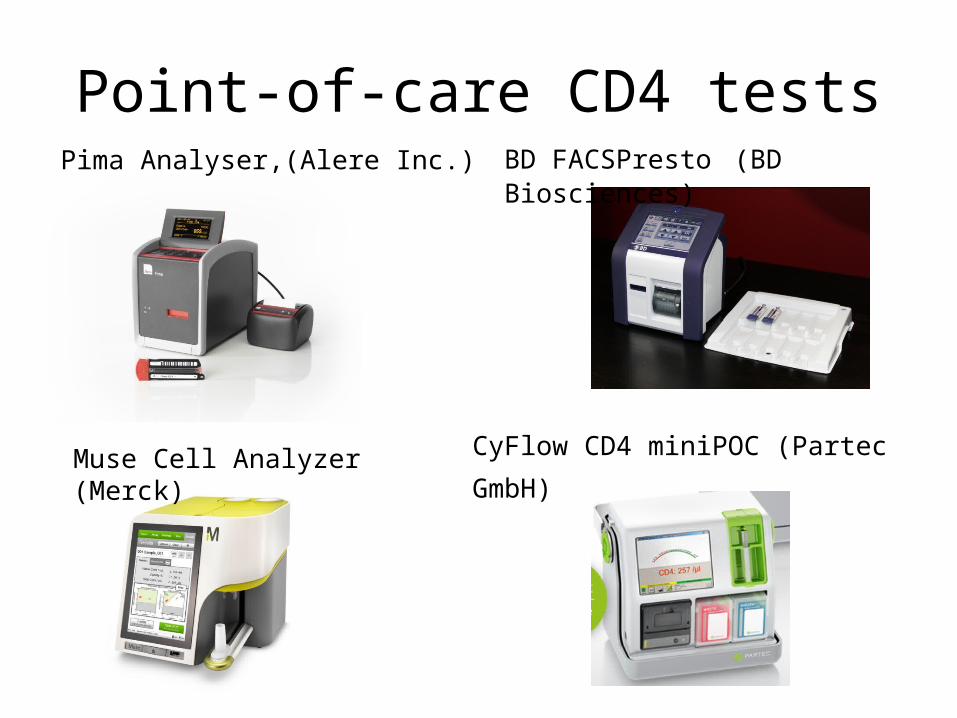
Point-of-care CD4 testsPima Analyser,(Alere Inc.) BD FACSPresto (BD Biosciences)
Muse Cell Analyzer (Merck) CyFlow CD4 miniPOC (Partec
GmbH)

POC HIV VL in the pipeline (2012)

How National AIDS Program (NAP+) Database Helping Us?

Thailand NAP Retention and Death RatesWorsening among non-ART populations
Retention rate Death0
20
40
60
80
10087
2.4
31
16.5
ARTNon-ART
% o
f pati
ents
N= 237,000
N= 88,000
Data as of mid of 2013
Lessen Learnt from Bangkok AIDS Committee (BAC) How NAP data-Driven Model can help to
Improve HIV Care Quality?
BAC Strategies to Improve the hospital Performances on HIV Care in Bangkok
• BAC has meeting q 3-4 months to review and monitor the key indicators of each hospital
• Any hospitals with a defined “red alert” indicator especially on low % VL control will be arrange for a supervision visit
• Each year, the best performed hospitals by “the targeted criteria : >75% of patients had VL tested and with >75% have VL <50 c/ml” will be awarded during the annual meeting

Proportion Patients with VL<50 c/mlBangkok Only (sites with>100 patients)
Overall VL<50 = 71%
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 180
10
20
30
40
50
60
70
80
90
100
7987
8177 78 78
% of Patients
National AIDS Program (NAP), Thailand. As of October 9, 2008
N= 124 N= 182 376
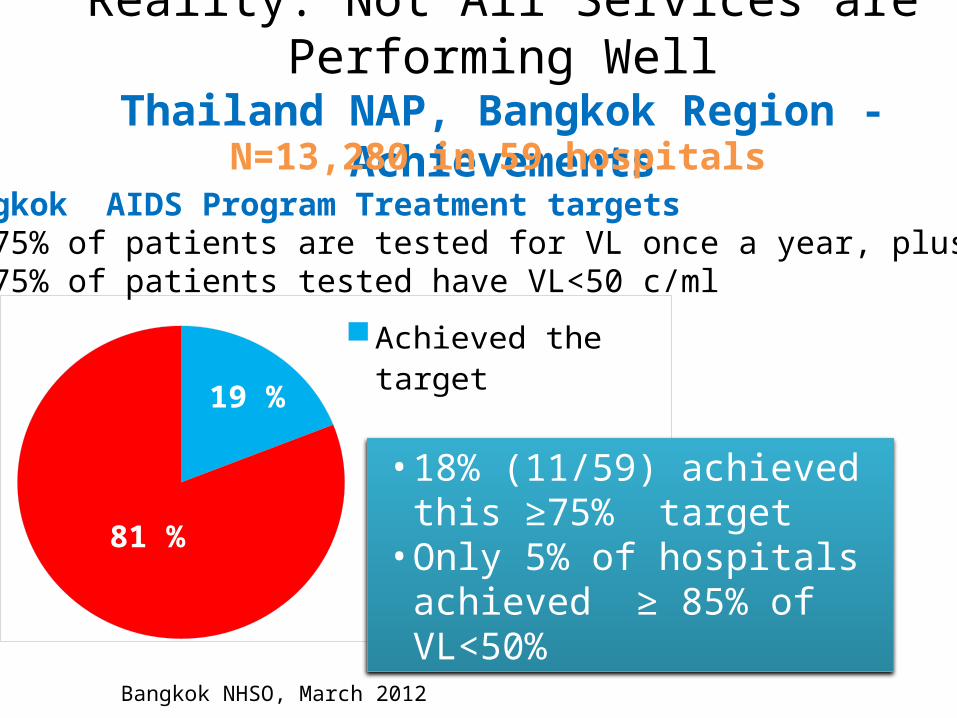
Reality: Not All Services are Performing WellThailand NAP, Bangkok Region -Achievements
19 %
81 %
Achieved the target
Below the target
Bangkok AIDS Program Treatment targets1. ≥75% of patients are tested for VL once a year, plus2. ≥75% of patients tested have VL<50 c/ml
• 18% (11/59) achieved this ≥75% target
• Only 5% of hospitals achieved ≥ 85% of VL<50%
Bangkok NHSO, March 2012
N=13,280 in 59 hospitals

Latest performance of hospitals in Bangkok
• Overall % patients with VL tested was >75%• And the latest overall % with undetectable VL
was >80%• There were however a few hospitals that still
require site visit and further support

When to start ART by guidelinesGuidelines CD4 Note
U.S. DHHS 2014 All When the patient is ready and committed to treatment
WHO 2013 <500 Regardless of CD4 for specific settings and the patient is ready and committed
Thai 2014 All When the patient is ready and committed to treatment

What to start in Resource-limited settings?
NtRTI orNRTI
Cytidine Analog
NNRTI or Boosted PIs
+ +TDFABCAZT
d4T
3TCFTC
Three drug combination in Naïve Patients2 Nucleoside RT Inhibitors + NNRTI or Boosted PIs
EFVRPVNVP
+ +
AlternativeLPV/rATV/rThai Guidelines 2014

What have we learned from 10 years analyses of
the TreatAsia Adult HIV Observational Database (TAHOD)
TAHOD nerwork. The 20th IAC, Melbourne, Australia: WEPE070

10 Years of TreatAsia Adult CohortN=6521; 21 centers in 12 countries in Asia
CD4 baseline increased from 93 (before 2005) to 134 cells/mm3 in 2010-2013
TAHOD nerwork. The 20th IAC, Melbourne, Australia: WEPE070

Factors associated with viral suppression N = 4735 patients Multivariate (associated with VL<400)
OR 95% CI p-value Year of ART initiation <0.001
2003-2005 1 2006-2009 1.76 (1.45-2.15) <0.0012010-2013 3.04 (2.33-3.97) <0.001
Age at ART initiation 0.001<=30 1 41-50 1.35 (1.07-1.71) 0.01151+ 1.57 (1.14-2.17) 0.006
Time from ART initiation (years) <0.001
0.0-0.5 1 0.5-1.0 2.14 (1.82-2.52) <0.0012.5-3.0 3.12 (2.52-3.88) <0.001

TreatAsia: TAHOD 10 yrs results
N = 4735 patients Multivariate (associated with VL<400) OR 95% CI p-value
Baseline viral Load (copies/mL)
<100000 1 >=100000 0.74 (0.60-0.91) 0.004
Baseline CD4 (cells/uL)
<=50 1 201+ 1.49 (1.18-1.89) 0.001
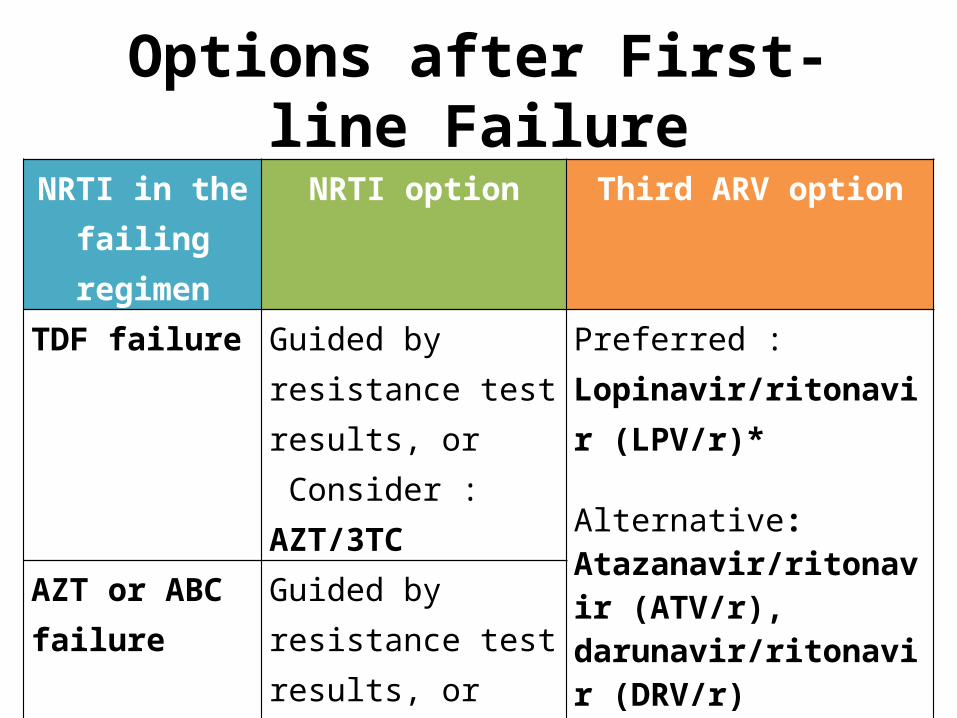
Options after First-line FailureNRTI in the
failing regimenNRTI option Third ARV option
TDF failure Guided by resistance test results, or Consider : AZT/3TC
Preferred : Lopinavir/ritonavir (LPV/r)*
Alternative: Atazanavir/ritonavir (ATV/r), darunavir/ritonavir (DRV/r)
AZT or ABC failure
Guided by resistance test results, orConsider :TDF/FTC or TDF/3TC

Standard doses of boosted protease inhibitors (bPIs) associated with a high exposure in Asian
LPV/r ATV/r0
20
40
60
80
100
120
140
90
41
128
7270
42
Caucasians Std dose
Asian Std Dose
Asian low dose (30% reduction)
Ritonavir-boosted Protease Inhibitor
Med
ian
AUC
(mg*
h/L)
van der Lugt J, and Avinhingsanon A. Asian Biomedicine Feb 2009

2010 2011 2012 2013 20140
500
1000
1500
2000
2500
3000
330450
1460
2200
2460
Cost
Sav
ing
(mill
ion
Baht
)Cost Saving When Using a Lower Dose
Atazanavir : from 300 to 200 mg5 year savings = ≥6900 million Baht
to treat 5000 cases with a 5% cases increased/yr
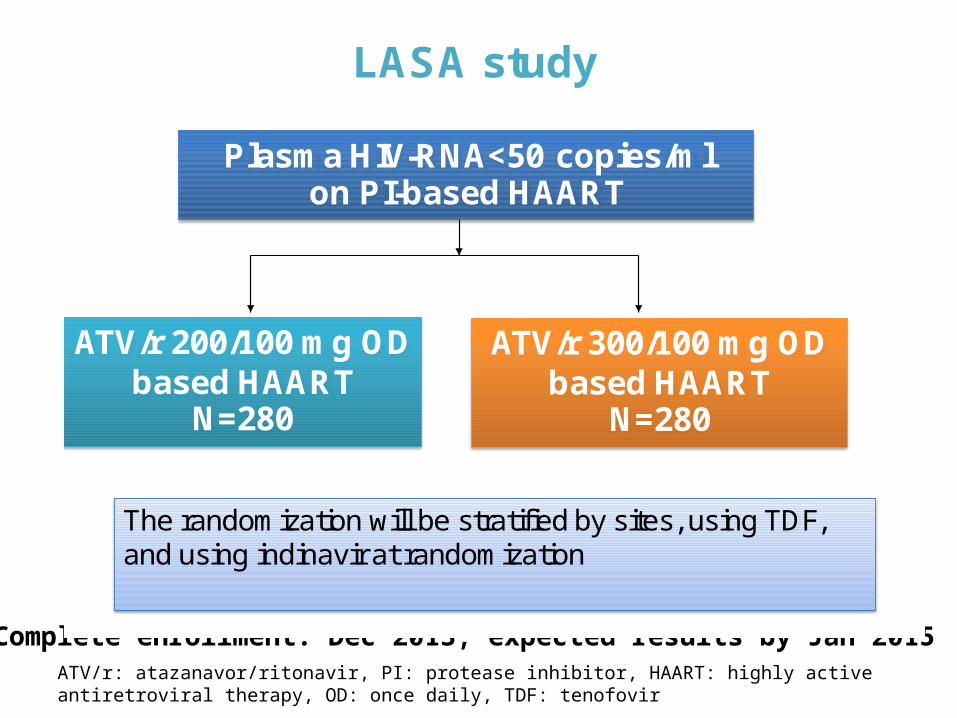
ATV/r: atazanavor/ritonavir, PI: protease inhibitor, HAART: highly active antiretroviral therapy, OD: once daily, TDF: tenofovir
LASA study
Plasma HIV-RNA<50 copies/ml on PI-based HAART
ATV/r 200/100 mg ODbased HAART
N=280
ATV/r 300/100 mg ODbased HAART
N=280
The randomization will be stratified by sites, using TDF, and using indinavir at randomization
Complete enrollment: Dec 2013, expected results by Jan 2015
Recruit Test Treat Retain
WHO 2013 Guidelines Implementation
HIV testing
CD4Viral load
Safety Comorbidity
Diagnosis Efficacy SafetyLab testmonitoring
RTTR






![18.10 [Kiat-kiat Seputar Harddisk]](https://img.dokumen.tips/doc/110x75/55cf8e01550346703b8d89a0/1810-kiat-kiat-seputar-harddisk.jpg)




















