Embed Size (px)
Citation preview

Fax +41 61 306 12 34E-Mail [email protected]
Original Paper
Neuropsychobiology 2006;53:63–69 DOI: 10.1159/000091721
Treating Auditory Hallucinations by Transcranial Magnetic Stimulation: A Randomized Controlled Cross-Over Trial
Martin Jandl
a, b Juergen Steyer
a Martin Weber
a David E.J. Linden
c Johannes Rothmeier
a Konrad Maurer
b Wolfgang P. Kaschka
a
a Department of Psychiatry I, University of Ulm, Ulm , b
Department of Psychiatry and Psychotherapy, University of Frankfurt am Main, Frankfurt am Main , Germany; c
School of Psychology, University of Wales, Bangor , UK
after treatment start from rTMS over the left superior temporal gyrus as revealed by the decrease of AH scores compared to right-sided and sham procedures.
Copyright © 2006 S. Karger AG, Basel
Introduction
Up to 70% of schizophrenic patients suffer from verbal auditory hallucinations (AH) [1] and up to 30% of them are refractory to antipsychotic (AP) medication [2] . The presence of AH was found to be a predictor of poor prog-nosis in schizophrenia [3] . Facing this serious therapeutic problem, the quest for other treatment options seems to be justifi ed.
Members of our research group have succeeded in dis-playing a cerebral activation pattern of AH in a direct way for the fi rst time in 3 patients, using functional magnetic resonance imaging (fMRI) [4] . Corresponding activation patterns have been shown, at least partially, in further studies [5–9] . The main foci of activation (in right-hand-ed patients) were found in the left primary auditory cor-tex, as well as in higher auditory areas of the left poste-rior superior and middle temporal gyrus, activations dur-ing AH were also found in the left hippocampus, the frontal operculum and the amygdala [4] . Based on these fi ndings, it seems appropriate to apply repetitive transcra-
Key Words Hallucination � Schizophrenia � Repetitive transcranial magnetic stimulation
Abstract Background: In a previous functional magnetic reso-nance imaging study, the authors succeeded in demon-strating the activation of Heschl’s gyrus during auditory hallucinations (AH). Objectives: This study aims to treat AH specifi cally by repetitive transcranial magnetic stim-ulation (rTMS). Methods: 16 patients with AH were in-cluded in a randomized, cross-over, sham-controlled tri-al. 1 Hz rTMS was administered over the left and right temporo-parietal cortex and sham position, respectively, on 5 consecutive days; 900 stimuli each, strength 100% of motor threshold. Using the Psychotic Symptom Rat-ing Scales (PSYRATS), the hallucinations during the stimulation periods and 4-week follow-ups were quanti-fi ed. Electroencephalograms (EEG) were acquired be-fore and after each period. Results: Treatment responses were observed after left hemisphere rTMS only. The 5 patients who showed a response did so already after 2 days. However, group mean hallucination scores did not differ across treatment conditions. No signifi cant changes were found in EEG after rTMS. Conclusions: A subgroup of patients suffering from AH benefi ts soon
Received: June 7, 2005 Accepted after revision: November 20, 2005 Published online: February 23, 2006
Martin Jandl, MDDepartment of Psychiatry I, University of UlmWeingartshofer Strasse 2, DE–88214 Ravensburg (Germany)Tel. +49 751 7601 2810, Fax +49 751 7601 2224E-Mail [email protected]
© 2006 S. Karger AG, Basel0302–282X/06/0532–0063$23.50/0
Accessible online at:www.karger.com/nps

Jandl /Steyer /Weber /Linden /Rothmeier /Maurer /Kaschka
Neuropsychobiology 2006;53:63–69 64
nial magnetic stimulation (rTMS) to the temporal lobe of the dominant hemisphere in an attempt to disrupt AH. Most authors assume that low-frequency rTMS mainly has a suppressive effect on the affected cortex [10] , al-though the underlying mechanisms are not yet under-stood fundamentally.
The results of previous studies on the effects of rTMS on AH are inconsistent. Hoffman et al. [11, 12] reported marked improvements of symptoms in two studies. They also described improvement of up to 105 days during the follow-up period [12] . Whereas d’Alfonso et al. [13] as well as Poulet et al. [14] also reported signifi cant improve-ments, even during a 60-day follow-up period, both Mc-Intosh et al. [15] and Schoenfeldt-Lecuona et al. [16] failed to fi nd favorable effects. Previous trials also varied in the defi nition of responders [11, 12, 14, 16–18] . With these inconsistencies, the registration of the effects of rTMS on biological activity is an important addition to such trials. There are some indications that electroen-cephalographic (EEG) � -frequency band activity is in-creased in the left temporal lobe during AH [19, 20] .
In this randomized, three-armed, sham-controlled cross-over trial, we aimed to assess the effects of low-fre-quency rTMS over the posterior portion of the left supe-rior temporal gyrus (STG) in schizophrenic patients suf-fering from AH, especially the proportion of possible re-sponders. We expected an improvement in hallucination rating scores compared to baseline, as well as relative to both rTMS over the right hemisphere and sham stimula-tion. We also conducted the fi rst clinical trial of rTMS in AH that incorporated a biological measure, EEG. We as-sumed that there would be alterations in the different EEG frequency bands.
Methods
Patients The patients were recruited from both the psychiatric wards and
the outpatient clinic. Inclusion criteria were: AH due to schizophre-nia or schizoaffective disorder for at least 1 year, resistance to treat-ment, defi ned as non-response to at least two attempts of adequate AP pharmacotherapy. The latter was defi ned as recommended dos-ages for at least 6–8 weeks with at least two APs, sequentially used, at least one of which had to be an atypical [21] .
16 patients (10 m, 6 f) were included and randomized, of which 14 (9 m, 5 f) completed the study. 14 were right-handed, 2 left-handed according to the Edinburgh Inventory [22] , and age ranged between 19 and 70 years (mean 36.3, SD 13.7). Mean du-ration of AH was 9.6 years (SD 8.3), 14 patients were diagnosed with paranoid schizophrenia, and 2 with schizoaffective disorder according to DSM-IV criteria [23] , as established by semistruc-tured psychiatric interviews. Patients were included after the pro-
tocol, especially the procedure of rTMS had been clearly ex-plained to them orally and in written form, and written informed consent had been obtained. All patients were informed that dis-continuing the trial would not infl uence their further treatment. The protocol has been approved by the Ethics Committee of the University Hospital of Ulm, in accordance with the last amend-ment of the 1964 Declaration of Helsinki of the World Medical Association. All patients were interviewed by a licensed psychol-ogist (J.S.) for their psychiatric and medical history, and were also carefully screened for their frequency of occurrence of AH. All patients reported AH involving comments and/or dialogues; moreover, 1 patient reported acoasms. Complete medical and neurological examinations were carried out. In structural neuro-imaging examinations (cranial computed tomography or cranial magnetic resonance imaging), no patient exhibited atrophic ce-rebral alterations, the determination of ‘lack of atrophy’ has been made by an experienced neuroradiologist. We did not assess the coil cortex distance, as, assuming no effect of atrophy, the poste-rior portion of the STG should be within the volume affected by TMS [24] . Reasons for exclusion were comorbidity of another apparent DSM-IV axis I disorder, a neurological disorder, pace-maker and other electronic devices, a history of head surgery or cerebral seizures. Dosages of APs and antidepressants (AD) were kept constant during the whole trial and the follow-up period, beginning 1 week before the trial. All patients were treated with oral APs. To a subset of 8 right-handed patients (5 m, 3 f), mean age 34.8 years (SD 16.5), mean duration of AH 5.1 years (SD 4.6), quantitative EEG recordings were available.
Patients’ Allocation and General Procedures After screening for inclusion criteria, the patients were random-
ized by tossing a dice (M.J.) and allocated to one of the three arms of the trial: rTMS over the left posterior portion of the STG, i.e. midway T3-P3 according to the extended ten-twenty system [25, 26] , rTMS over the right posterior portion of the STG, i.e. midway T4-P4, or sham stimulation. The patients were stimulated on 5 suc-cessive days between 9 and 11 a.m., followed by a 4-week follow-up period, including ratings after 1, 2 and 4 weeks. This was followed by randomized reallocation to one of the remaining two arms, which involved the same procedure, and fi nally the last remaining arm. So each patient passed through each stimulation (or sham) protocol.
Ratings For the assessment of AH, the auditory hallucination subscale
of the Psychotic Symptom Rating Scales (PSYRATS (AH)) [27] was administered after each stimulation and on the follow-up dates. This was the primary outcome measure, which assessed levels and characteristics of hallucinations by a multidimensional, 11-item, 5-point scale. This scale has been developed for monitoring dimen-sional changes during the therapeutic process, with the advantages of very good validity and interrater reliability. At days 1, 2, 5 and the follow-up dates the Scale for the Assessment of Positive Symp-toms (SAPS) was administered as well [28] . At days 1 and 5 we ap-plied the Scale for the Assessment of Negative Symptoms (SANS) [29] and the Beck Depression Inventory (BDI) [30, 31] to explore effects on negative and depressive symptoms.
The rater (J.S.) and all therapeutically involved clinicians and nursing staff were blinded to any group assignment of the patients. Only the two physicians performing the stimulations (M.W., M.J.)

Transcranial Magnetic Stimulation in Auditory Hallucinations
Neuropsychobiology 2006;53:63–69 65
were not blinded to the protocol. Their personal contacts to the patients were restricted to the minimum.
EEG Investigations 10-min resting EEG recordings were obtained before the fi rst
(day 1) and after the last (day 5) rTMS/sham session of each rTMS/sham period, within a time frame of 1 h. Before acquisition, all pa-tients were instructed in the same way to close their eyes and relax. They were seated in a comfortable chair in a half-supine position within a sound- and light-attenuated examination room. For acqui-sitions and recordings of the EEG signals, a Schwarzer Comlab 32 System (Schwarzer GmbH, Munich, Germany) was used. 21 Ag/AgCl scalp electrodes were positioned according to an extended ten-twenty system [25, 26] at Fp1, Fp2, Fpz, F7, F8, F3, F4, Fz, T3, T4, C3, C4, Cz, P3, P4, Pz, P7, P8, O1, O2, Oz (referenced to Cz). Both a horizontal and a vertical electro-oculogram were re-corded, as well as a one-channel electrocardiogram for artifact iden-tifi cation. Electrode impedances were kept below 5 k � . The digiti-zation rate was 250 Hz. High-pass cut-off was set at 0.53 Hz, low-pass cut-off at 70 Hz; no notch fi lter was used. The reliability of EEG recordings was regarded as suffi cient on the basis of group comparisons [32] .
TMS Procedure For rTMS, we used a Medtronic Dantec stimulator with a fi g-
ure-of-eight-coil (MagPro, MC-B 70, r = 5 cm, Medtronic GmbH Düsseldorf, Germany); the center of the coil was positioned over midway T3-P3 or T4-P4, respectively. Sham stimulation was car-ried out by taking the position of T3-P3 but with the coil tilted by 45°, with the edge of the coil positioned left occipitally. At the po-sition T3-P3 and T4-P4, the handle of the coil pointed upwards. As suggested by Hoffman et al. [11, 12, 17] , the corresponding cortical region could thus be reached with suffi cient accuracy. Af-ter the patients had been told to relax their hands, the motoric threshold (MT) was assessed. MT was defi ned by the lowest output strength of the stimulator producing a twitch of a right-hand mus-cle in at least 5 out of 10 stimuli, applied over the left primary mo-tor cortex. We used visual control of MT, which has been found to be equivalent to control by electromyography and which has been used in previous studies [12, 33] . RTMS stimulus strength was set at 100% MT strength. We used low stimulation frequency of 1 Hz, 1 train over 15 min, i.e. 900 stimuli per session. The safe-ty guidelines of the International Society of Transcranial Stimula-tion [34] were observed. To rule out infl uences of the rTMS on the hearing level, audiometry pre- and post-study in 5 patients was performed.
Analyses Data were analyzed on an intention-to-treat basis. Mean
PSYRATS (AH) scores were computed by stimulation time and condition. Mean PSYRATS (AH) baseline scores were compared to those of post-test endpoints for each stimulation time and condi-tion by calculating the differences between the two time points. A general linear model for repeated measurements of an analysis of variance (ANOVA) was used to test for a signifi cant interaction of the two factors of the experimental design, eight times (the fi ve post-stimulation and the three follow up scores) ! three conditions (left, right, sham), with the order of stimulation as a covariate. The same procedure was applied to the secondary outcome measures (SAPS, SANS and BDI scores). Partial response was defi ned as at
least 30% decrease, and response as at least 50% decrease of PSYRATS (AH) sum score, on at least 2 successive days. Response and partial response during the follow-up period were defi ned by the respective decreases on 2 successive days during that period or on the last day only. For statistical computation of the feature ‘re-sponse to stimulation’, the � 2 test with the factors response and stimulation condition has been used according to Pearson as well as Fisher’s exact test. t Tests have been performed for differences between responders and non-responders in the factors age, duration of AH, number of administered APs, number of ADs respectively and former alcohol or drug abuse. Offl ine preprocessing of the EEG data was performed by the Brain Vision Analyzer software (Brain Products GmbH, Munich, Germany). After fi ltering the raw data with high-pass 0.53 Hz and low-pass 30 Hz, the EEG was segment-ed to 2-second epochs. An experienced electroencephalographer examined all segments in the context of a semiautomatic artifact rejection program; the fi rst 25 artifact-free epochs of each acquisi-tion were retained. The EEG epochs were fi ltered to the following frequency bands by Fourier transformation: � /low � (1.5–6/s), � (6.5–8/s), � -1 (8.5–10/s), � -2 (10.5–12/s), � -1 (12.5–18/s), � -2 (18.5–21/s) and � -3 (21.5–30/s) [35] . For the assessment of rTMS effects on EEG, we performed ANOVA for each of the seven EEG frequency bands, applied to the main effects time (pre-, post-stim-ulation) and condition (stimulation site left, right, sham) as well as interaction (time ! condition), with the order of stimulation as a covariate. To provide evidence of group differences in EEG be-tween responders and non-responders, ANOVA were performed for each frequency band, with the factors group (response, non-re-sponse) ! condition and order of stimulation as a covariate.
Results
In 14 out of 16 patients included, rTMS sessions were conducted over the total trial period and pre- and post-treatment ratings were obtained. One patient dropped out because of changes in medical treatment, another one without giving reasons. EEG analyses were performed in 8 patients. One patient (No. 9) reported that he ‘heard’ the click noise of the stimulator coil at day 1 until day 3 of the treatment period for several hours after the stimu-lation, even at night, when he awoke from sleep. One pa-tient (No. 3) reported dull headaches irregularly after stimulation; medical treatment was not needed. No se-vere side effects were observed.
Primary Outcome Measure Whereas mean PSYRATS (AH) sum score did not re-
veal signifi cant changes compared to baseline under the three stimulation conditions ( table 1 ), signifi cant differ-ences in the feature ‘response to stimulation’ ( � 2 test of signifi cance for distribution of responders and non-re-sponders, p = 0.018, Fisher’s exact test, p = 0.036) were observed between the three conditions. Five complete or
Jandl /Steyer /Weber /Linden /Rothmeier /Maurer /Kaschka
Neuropsychobiology 2006;53:63–69 66
partial responders were identifi ed for left hemisphere stimulation during the stimulation period. Four of them showed a response also during follow-up. For right hemi-sphere stimulation, one partial responder was identifi ed during the stimulation period only (she was one of the partial responders to left hemisphere stimulation as well). No clinical responses were observed for sham stimula-tion. All of the partial or full responders already respond-ed on the second day of stimulation. Three of the fi ve responders or partial responders to left hemisphere stim-ulation revealed improvement during the follow-up mon-itoring, two responders changed to partial response dur-ing follow-up ( table 2 ). The number needed to treat (NNT) for a partial or full response during the stimulation period was 3.2. The NNT after 4 weeks’ follow-up was 8.0. We did not fi nd any specifi c pattern of predictive factors for either response or non-response ( table 3 ), not even with regard to the EEG frequency bands.
Secondary Outcome Measures Under the three stimulation conditions, the SAPS,
SANS and BDI sum scores did not reveal signifi cant changes compared to the respective baseline. Neither there were main effects, interaction effects (time ! stim-ulation condition) nor sequence effects.
EEG Investigations ANOVA for interaction of the factors time (pre-post)
and condition (with the order of stimulation as a covari-ate) did not reveal signifi cant differences in EEG power of the analyzed frequency bands.
Discussion
Given that the results of previous studies on the ef-fects of rTMS on AH in schizophrenic patients have been inconsistent, our purpose was to assess the effects of rTMS on AH, especially with regard to the proportion of possible responders and the presence of factors that might predict response probability. Low-frequency rTMS over the posterior portion of the left STG should be compared with right STG as well as sham stimula-tion. As a biological secondary outcome measure, we additionally assessed potential effects on EEG frequen-cy bands.
The feature ‘response to rTMS’ differed signifi cantly between stimulation conditions. In a proportion of pa-tients (5 out of 16) suffering from AH, who had otherwise been resistant to treatment, a defi nite clinical effect, i.e. response or partial response, was only found during the left hemisphere stimulation periods. One patient showed partial response both during left and right hemisphere rTMS. No clinical improvement was found during the sham period. Improvement appeared already after the second stimulation. The effect was partially maintained beyond the end of the stimulation period (in 4 of the 5 responders). The NNT at the end of the left hemisphere stimulation week was 3.2, which is in the range normally observed for psychiatric treatment [36] .
Taking the whole group of patients into consideration, there was no signifi cant decrease in PSYRATS (AH) mean score during the rTMS as well as during the follow-up period, neither by left nor right hemisphere stimula-tion nor sham, compared to baseline.
In this trial, we assessed rTMS effects on AH with stimulation of both hemispheres. Although most neuro-psychological studies on AH implicate mainly the left hemisphere, the role of the right hemisphere should not be underestimated. In our previous fMRI study, one left-handed patient revealed a right temporal activation [4] , and other groups have reported right temporal activa-tion during AH as well [5, 6] . Lee et al. [37] found a de-crease of hallucination scores also after right hemisphere rTMS. It is also advantageous that rTMS over both hemispheres eases the problem of the inclusion of left-handed patients. However, the proportion of responders by right hemisphere stimulation was not signifi cant in the present study (1 out of 16). Contrary to the conclu-sion that only rTMS over the left hemisphere leads to a decrease in AH, it could be argued that possible delayed effects of rTMS over the right hemisphere could not be found simply because of our relatively short treatment
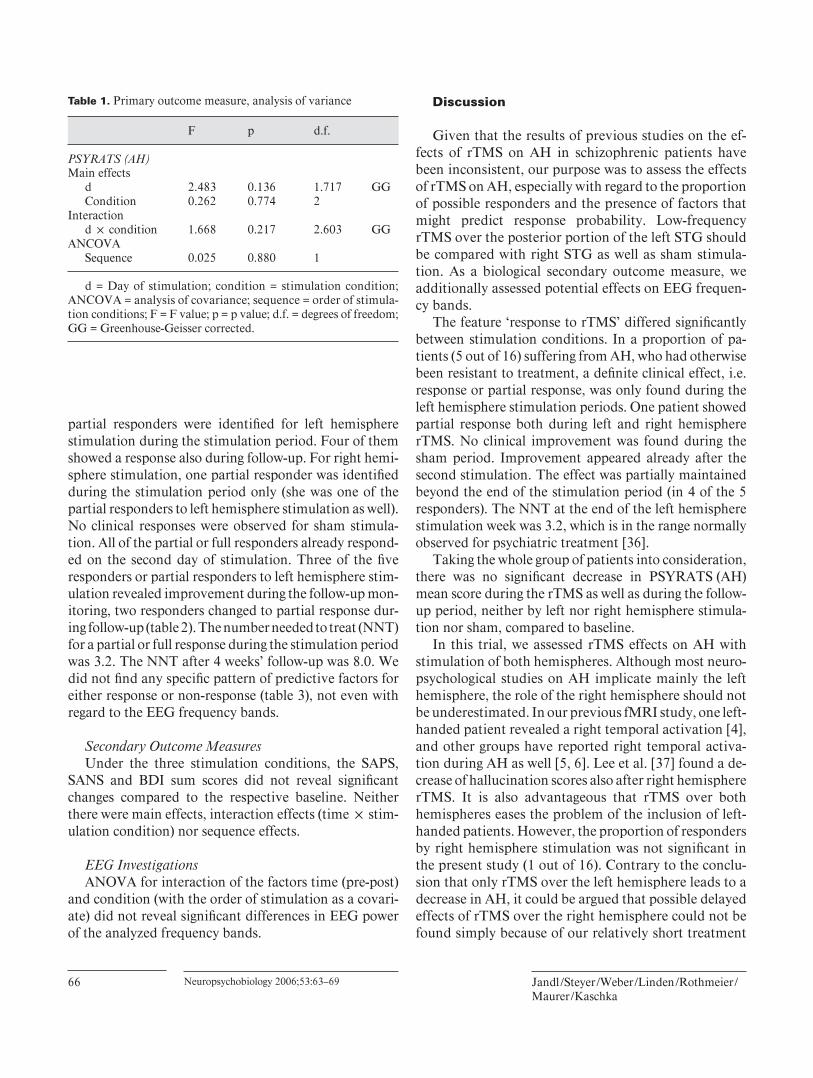
Table 1. Primary outcome measure, analysis of variance
F p d.f.
PSYRATS (AH)Main effects
d 2.483 0.136 1.717 GGCondition 0.262 0.774 2
Interactiond ! condition 1.668 0.217 2.603 GG
ANCOVASequence 0.025 0.880 1
d = Day of stimulation; condition = stimulation condition; ANCOVA = analysis of covariance; sequence = order of stimula-tion conditions; F = F value; p = p value; d.f. = degrees of freedom; GG = Greenhouse-Geisser corrected.
Transcranial Magnetic Stimulation in Auditory Hallucinations
Neuropsychobiology 2006;53:63–69 67
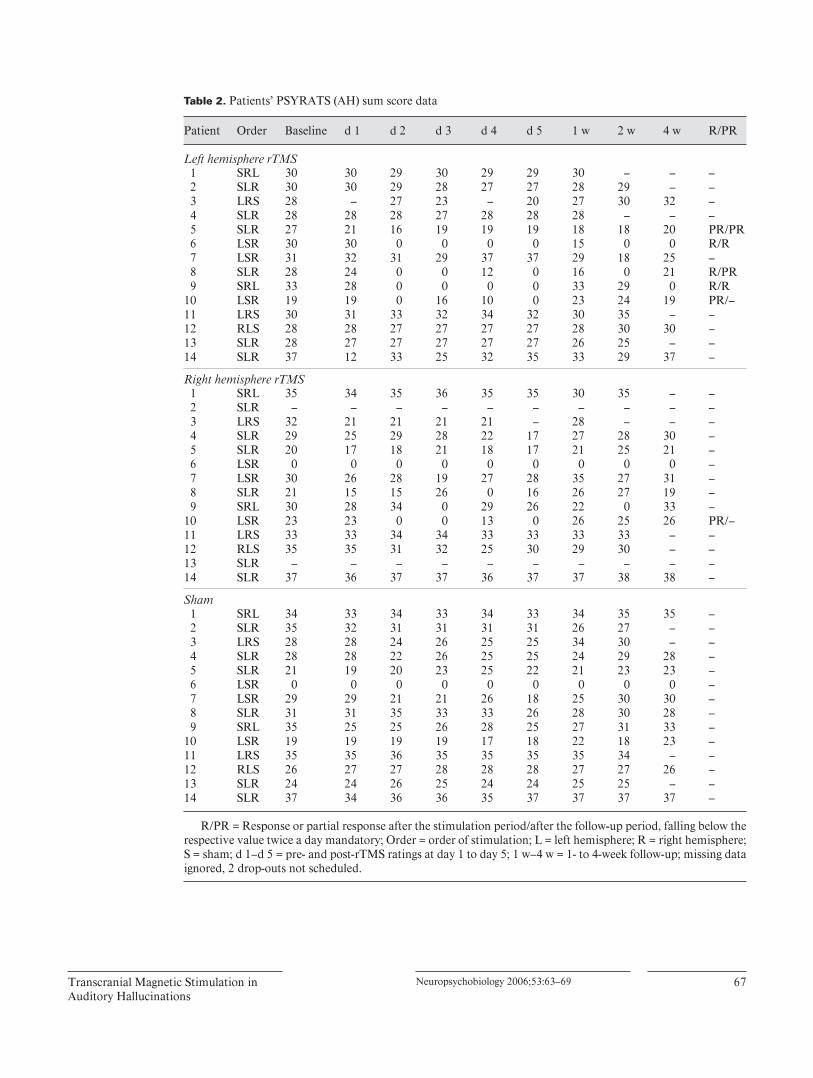
Table 2. Patients’ PSYRATS (AH) sum score data
Patient Order Baseline d 1 d 2 d 3 d 4 d 5 1 w 2 w 4 w R/PR
Left hemisphere rTMS1 SRL 30 30 29 30 29 29 30 – – –2 SLR 30 30 29 28 27 27 28 29 – –3 LRS 28 – 27 23 – 20 27 30 32 –
4 SLR 28 28 28 27 28 28 28 – – – 5 SLR 27 21 16 19 19 19 18 18 20 PR/PR 6 LSR 30 30 0 0 0 0 15 0 0 R/R 7 LSR 31 32 31 29 37 37 29 18 25 – 8 SLR 28 24 0 0 12 0 16 0 21 R/PR 9 SRL 33 28 0 0 0 0 33 29 0 R/R10 LSR 19 19 0 16 10 0 23 24 19 PR/–11 LRS 30 31 33 32 34 32 30 35 – –12 RLS 28 28 27 27 27 27 28 30 30 –13 SLR 28 27 27 27 27 27 26 25 – –14 SLR 37 12 33 25 32 35 33 29 37 –
Right hemisphere rTMS 1 SRL 35 34 35 36 35 35 30 35 – – 2 SLR – – – – – – – – – – 3 LRS 32 21 21 21 21 – 28 – – – 4 SLR 29 25 29 28 22 17 27 28 30 – 5 SLR 20 17 18 21 18 17 21 25 21 – 6 LSR 0 0 0 0 0 0 0 0 0 – 7 LSR 30 26 28 19 27 28 35 27 31 – 8 SLR 21 15 15 26 0 16 26 27 19 – 9 SRL 30 28 34 0 29 26 22 0 33 –10 LSR 23 23 0 0 13 0 26 25 26 PR/–11 LRS 33 33 34 34 33 33 33 33 – –12 RLS 35 35 31 32 25 30 29 30 – –13 SLR – – – – – – – – – –14 SLR 37 36 37 37 36 37 37 38 38 –
Sham 1 SRL 34 33 34 33 34 33 34 35 35 – 2 SLR 35 32 31 31 31 31 26 27 – – 3 LRS 28 28 24 26 25 25 34 30 – – 4 SLR 28 28 22 26 25 25 24 29 28 – 5 SLR 21 19 20 23 25 22 21 23 23 – 6 LSR 0 0 0 0 0 0 0 0 0 – 7 LSR 29 29 21 21 26 18 25 30 30 – 8 SLR 31 31 35 33 33 26 28 30 28 – 9 SRL 35 25 25 26 28 25 27 31 33 –10 LSR 19 19 19 19 17 18 22 18 23 –11 LRS 35 35 36 35 35 35 35 34 – –12 RLS 26 27 27 28 28 28 27 27 26 –13 SLR 24 24 26 25 24 24 25 25 – –14 SLR 37 34 36 36 35 37 37 37 37 –
R/PR = Response or partial response after the stimulation period/after the follow-up period, falling below the respective value twice a day mandatory; Order = order of stimulation; L = left hemisphere; R = right hemisphere; S = sham; d 1–d 5 = pre- and post-rTMS ratings at day 1 to day 5; 1 w–4 w = 1- to 4-week follow-up; missing data ignored, 2 drop-outs not scheduled.

Jandl /Steyer /Weber /Linden /Rothmeier /Maurer /Kaschka
Neuropsychobiology 2006;53:63–69 68
duration. This explanation is unlikely, however, because the onset of clinical effects of rTMS, where present, was immediate.
Aside from the direct effects on AH in the responders, we saw no relevant psychometrically ascertainable effects of rTMS. It is also important to mention that no severe side effects were reported.
Contrary to our hypothesis, a clear-cut neurophysio-logic correlate of the rTMS effects on AH, especially a decrease in higher frequency bands in the brain areas im-plicated in the generation of AH, could not be identifi ed by our method of quantitative EEG. The mean changes in brain electrical activation patterns after both rTMS and sham did not reach signifi cance level. It is probably too early to judge the potential use of quantitative EEG for the monitoring of rTMS treatment effects on the basis of this rather small sample, but we would advocate the further use of this non-invasive monitoring technique in larger samples.
This is a controlled trial which could not confi rm the improvement in AH mean score unlike Hoffman’s [11, 12] and Poulet’s studies [14] . Their very optimistic fol-low-up data could not be replicated, except for a subgroup of patients. The difference in the method of quantifi ca-tion of AH may be one underlying cause of this discrep-ancy. The fact that the PSYRATS (AH) has relatively few intermediate frequency scoring levels might be one of the reasons for the differences in the outcome of Hoffman’s and our study [R.E. Hoffman, pers. commun.]. But it must also be taken into account that in Hoffman et al.’s [12] parallel controlled study, stimulation lasted 4 days longer and, though interrupted by a 3-day break, includ-ed a total of 7,920 stimuli – 3,420 more than in our trial. Poulet et al. [14] stimulated during 5 days twice a day, administering overall 10,000 stimuli. Their markedly
better outcome could then be due to the total number of stimuli. Another important difference to most of these studies is that we used a cross-over method rather than a parallel controlled trial. The latter does not meet the prob-lem of carryover effects when active treatment is followed by sham. Authors of rTMS studies on AH all use about the same stimulation site, midway between T3 and P3. This seems reasonable according to our fi ndings from pre-vious fMRI trials, especially regarding the coactivation of auditory association areas [4] and in view of the fact that the primary auditory cortex itself is probably not ac-cessible by TMS.
The primary limitation of the study is the relatively small sample size; another problem of rTMS studies re-sides in the limited possibilities for placebo control. Al-though our patients could not differentiate between ac-tive treatment and sham period, and there was no se-quence effect on the outcome, all sham strategies are mere compromises. We are also aware of the problem of a short pre-study period. Yet the long overall duration of the cross-over trial did not seem to allow additionally keeping medication constant for up to 4 or 6 weeks. Otherwise the drop-out rate could have increased substantially. Further-more, our understanding of the cerebral activation pat-terns involved in AH and the way in which TMS might alter them still seems to be rather patchy. At least the con-siderable advances in neuroimaging [4, 38, 39] inspire confi dence that the stimulation site of our and previous rTMS studies (over posterior STG) was chosen appropri-ately. The lack of clinical improvement in many studies amongst others might have resulted from insuffi cient stimulation intensity or duration of the treatment period. The positive outcome of Hoffman’s study [12] published 2003 and Poulet’s trial [14] would support this. Longer and larger parallel randomized controlled trials, extend-ing over several weeks, thus seem desirable. In the ab-sence of any clear-cut benefi ts of right hemisphere stimu-lation in the present study, we would recommend to re-strict further studies to a dominant hemisphere treatment group and a placebo group, in order to maximize sample size.
Our results also point to another important question for further investigations. In our sample of schizophrenia patients with medication-resistant AH, those who re-sponded to rTMS did so already during the fi rst 2 days. Further trials are needed to confi rm the temporal pattern of rTMS treatment response. If confi rmed, it could allow clinicians to identify non-responders early and thus avoid unnecessary TMS sessions. Finally, efforts should con-tinue to establish criteria for a likely rTMS response in
Table 3. Predictive factors for response
Mean R (SD)
Mean NR (SD)
p
Age, years 33.8 (9.9) 37.5 (14.9) 0.60Duration of auditory hallucinations, years 8.6 (8.6) 9.5 (7.9) 0.87Number of antipsychotics 1.8 (0.8) 1.5 (0.5) 0.35Number of antidepressants 0.8 (0.4) 0.7 (0.4) 0.74History of alcohol or drug abuse 0.6 (0.5) 0.3 (0.4) 0.29
R = Responders; NR = non-responders.

Transcranial Magnetic Stimulation in Auditory Hallucinations
Neuropsychobiology 2006;53:63–69 69
schizophrenia patients with AH, possibly based on a com-bination of biological and psychological markers. This would enable clinicians to focus rTMS therapy on those who are most likely to benefi t.
Acknowledgements
The authors would like to thank Dr. David Prvulovic and Dr. Jonas Obleser for their kind support.
References
1 Sartorius N, Shapiro R, Jablonsky A: The in-ternational pilot study of schizophrenia. Schizophr Bull 1974; 1: 21–35.
2 Shergill SS, Murray RM, McGuire PK: Audi-tory hallucinations: a review of psychological treatment. Schizophr Res 1998; 32: 137–150.
3 Jablonsky A: Schizophrenia: the epidemiologi-cal horizon; in Hirsch SR, Weinberger DR (eds): Schizophrenia. Oxford, Blackwell Sci-ence, 1995, pp 206–256.
4 Dierks T, Linden DEJ, Jandl M, Formisano E, Goebel R, Lanfermann H, Singer W: Activa-tion of Heschl’s gyrus during auditory halluci-nations. Neuron 1999; 22: 615–621.
5 Lennox BR, Park SB, Jones PB, Morris PG, Park G: Spatial and temporal mapping of neu-ral activity associated with auditory hallucina-tions. Lancet 1999; 353: 644.
6 Lennox BR, Park SB, Medley I, Morris PG, Jones PB: The functional anatomy of auditory hallucinations in schizophrenia. Psychiatry Res 2000; 100: 13–20.
7 Shergill SS, Bullmore E, Simmons A, Murray R, McGuire P: Functional anatomy of audi-tory verbal imagery in schizophrenic patients with auditory hallucinations. Am J Psychiatry 2000; 157: 1691–1693.
8 Shergill SS, Cameron LA, Brammer MJ, Wil-liams SC, Murray RM, McGuire PK: Modality specifi c neural correlates of auditory and so-matic hallucinations. J Neurol Neurosurg Psy-chiatry 2001; 71: 688–690.
9 Bentaleb LA, Beauregard M, Liddle P, Stip E: Cerebral activity associated with auditory ver-bal hallucinations: a functional magnetic reso-nance imaging case study. J Psychiatry Neuro-sci 2002; 27: 110–115.
10 Sack AT, Linden DE: Combining transcranial magnetic stimulation and functional imaging in cognitive brain research: possibilities and limitations. Brain Res Brain Res Rev 2003; 43:
41–56. 11 Hoffman RE, Boutros NN, Hu S, Berman RM,
Krystal JH, Charney DS: Transcranial magnet-ic stimulation and auditory hallucinations in schizophrenia. Lancet 2000; 355: 1073–1075.
12 Hoffman RE, Hawkins KA, Gueorguieva R, Boutros NN, Rashid F, Carroll K, Krystal JH: Transcranial magnetic stimulation of left tem-poro-parietal cortex and medication-resistant auditory hallucinations. Arch Gen Psychiatry 2003; 60: 49–56.
13 D’Alfonso AAL, Aleman A, Kessels RPC, Schouten EA, Postma A, van der Linden JA, Cahn W, Greene Y, de Haan EHF, Kahn RS: Transcranial magnetic stimulation of left audi-tory cortex in patients with schizophrenia: ef-fects on hallucinations and neurocognition. J Neuropsychiatry Clin Neurosci 2002; 14: 77–79.
14 Poulet E, Brunelin J, Bediou B, Bation R, Forgeard L, Dalery J, d’Amato T, Saoud M: Slow transcranial magnetic stimulation can rapidly reduce resistant auditory hallucina-tions in schizophrenia. Biol Psychiatry 2005;
57: 188–191. 15 McIntosh AM, Semple D, Tasker K, Harrison
LK, Owens DGC, Johnstone EC, Ebmeier KP: Transcranial magnetic stimulation for audito-ry hallucinations in schizophrenia. Psychiatry Res 2004; 127: 9–17.
16 Schoenfeldt-Lecuona C, Groen G, Walter H, Buechler N, Wunderlich A, Spitzer M, Herwig U: Stereotaxic rTMS for the treatment of audi-tory hallucinations in schizophrenia. Neurore-port 2004; 15: 1669–1673.
17 Hoffman RE, Boutros NN, Berman RM, Roessler E, Belger A, Krystal JH, Charney DS: Transcranial magnetic stimulation of left tem-poro-parietal cortex in three patients reporting hallucinated ‘voices’. Biol Psychiatry 1999; 46:
130–132. 18 Franck N, Poulet E, Terra JL, Dalery J,
d’Amato T: Left temporo-parietal transcranial magnetic stimulation in treatment-resistant schizophrenia with verbal hallucinations. Psy-chiatry Res 2002; 120: 107–109.
19 Mueller T, Dierks T, Fritze J, Maurer K: Func-tional brain imaging (mapping of EEG) in rela-tion to psychopathologic changes in schizo-phrenia. Psychiatry Res 1989; 29: 419–420.
20 Ropohl A, Sperling W, Elstner S, Tomandl B, Reulbach U, Kaltenhauser M, Kornhuber J, Maihofner C: Cortical activity associated with auditory hallucinations. Neuroreport 2004; 15:
523–526. 21 National Institute for Clinical Excellence: Full
guidance on the use of newer (atypical) antipsy-chotic drugs for the treatment of schizophre-nia. Technology Appraisal Guidance No 43, London 2002 (www.nice.org.uk).
22 Oldfi eld RC: The assessment and analysis of handedness: the Edinburgh Inventory. Neuro-psychologia 1971; 9: 97–113.
23 American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, ed 4. Washington, American Psychiatric Press, 1994.
24 Bohning DE: Introduction and overview of TMS physics; in George MS, Belmaker RH (eds): Transcranial Magnetic Stimulation in Neuropsychiatry. Washington, American Psy-chiatric Press, 2000, pp 13–44.
25 Jasper HH: The ten-twenty electrode system of the International Federation. Electroencepha-logr Clin Neurophysiol 1958; 10: 371–375.
26 American Encephalographic Society: Guide-lines for standard electrode position nomencla-ture. J Clin Neurophysiol 1991; 8: 200–222.
27 Haddock G, McCarron J, Tarrier N, Faragher EB: Scales to measure dimensions of hallucina-tions and delusions: the Psychotic Symptom Rating Scales (PSYRATS). Psychol Med 1999;
29: 879–889. 28 Andreasen NC: Scale for the Assessment of
Positive Symptoms (SAPS). Iowa City, Uni-versity of Iowa, 1984.
29 Andreasen NC: The Scale for the Assessment of Negative Symptoms (SANS): conceptual and theoretical foundations. Br J Psychiatry 1989(suppl 7):49–58.
30 Beck AT: Depression Inventory. Philadelphia, Center for Cognitive Therapy, 1978.
31 Hautzinger M, Bailer M, Worall H, Keller F: Das Beck-Depressions-Inventar (BDI). Bern, Huber, 1992.
32 Burgess AP, Gruzelier J: Individual reliability of amplitude distribution in topographical mapping of EEG. Electroencephalogr Clin Neurophysiol 1993; 86: 219–223.
33 Pridmore S, Fernandes Filho JA, Nahas Z, Liberatos C, George MS: Motor threshold in transcranial magnetic stimulation: a compari-son of a neurophysiological method and a vi-sualization of movement method. J ECT 1998;
14: 25–27. 34 Wassermann E: Risk and safety of repetitive
transcranial magnetic stimulation: report and suggested guidelines from the International Workshop on the Safety of Repetitive Tran-scranial Magnetic Stimulation, June 5–7, 1996. Electroencephalogr Clin Neurophysiol 1998; 108: 1–16.
35 Kubicki S, Herrmann WM, Fichte K, Freund G: Refl ections on the topics: EEG frequency bands and regulation of vigilance. Pharmaco-psychiatry 1979; 12: 237–245.
36 Nadeem Z, McIntosh A, Lawrie S: Schizophre-nia. Clin Evid 2005; 1–30.
37 Lee SH, Kim W, Chung WC, Jung KH, Bakh WM, Jun TY, Kim KS, George MS, Chae JH: A double blind study showing that two weeks of daily repetitive TMS over the left or right temporoparietal cortex reduces symptoms in patients with schizophrenia who are having treatment-refractory auditory hallucinations. Neurosci Lett 2005; 376: 122–181.
38 Silbersweig DA, Stern E, Frith C, Cahill C, Holmes A, Grootoonk S, Seaward J, McKenna P, Chua SE, Schnorr L, Jones T, Frackowiak RSJ: A functional neuroanatomy of hallucina-tions in schizophrenia. Nature 1995; 378: 176–179.
39 Hubl D, Koenig T, Strik W, Federspiel A, Kreis R, Boesch C, Maier SE, Schroth G, Lovblad K, Dierks T: Pathways that make voices: white matter changes in auditory hallucinations. Arch Gen Psychiatry 2004; 61: 658–668.



























