Embed Size (px)
Citation preview

TRAUMA AND SURGERYTRAUMA AND SURGERY IN THE PREGANANT IN THE PREGANANT PATIENTPATIENT
PRINCIPLES OF SURGERY-PRINCIPLES OF SURGERY-20092009NICHOLAS LEYLAND,BASc,MD,MHCM,FRCSCCHIEF OF OBSTETRICS AND GYNAECOLOGY, MEDICAL DIRECTOR OF THE WOMEN’S, CHILDREN’S AND FAMILY HEALTH PROGRAMST.JOSEPH’S HEALTH CENTRE,ASSOCIATE PROFESSOR OF OB/GYN,UNIVERSITY OF TORONTO

Surgery and Trauma in the Surgery and Trauma in the Pregnant PatientPregnant PatientLearning objectives:
1)TRAUMA IN PREGNANCY
2)THE ACUTE ABDOMEN IN PREGNANCY
3)CASES
5) UPDATE LEYLAND

Trauma in Pregnancy-Incidence:Trauma in Pregnancy-Incidence:
Maternal mortality rate
• 3.5%– Mortality rate is similar for
non-pregnant women
Fetal mortality rate
• 1% in minor trauma
• 15% in major trauma
• Overall fetal death rate from trauma = 1/30000 pregnancies
• Trauma occurs in 6-7% of pregnancies• 4.6-8.3% of Traumas are complicated by pregnancy

““THERAPEUTIC PARALYSIS”THERAPEUTIC PARALYSIS”

Maternal Physiology:Maternal Physiology:Surgical Implications:Surgical Implications:
• Cardiovascular Changes; CO ^ 50%,Blood Vol^ 50%• Maternal rbc ^ 30% ‘Dilutional Anaemia’• WBC ^ 12000, Labour 20,000• GI: Appendix (localization), Progesterone Decreased motility,^ alk
phosphatase, no change in Transaminases• Respiratory Changes: e.g. Decreased pCO2
General Management PrinciplesGeneral Management PrinciplesMaternal AssessmentMaternal Assessment
• Primary Survey– ABCs…Fetus
• Lateral Tilt– Supine position can cardiac output by 30%
– 15° tilt is appropriate
– Can decrease effect of CPR

General Management PrinciplesGeneral Management PrinciplesFetal AssessmentFetal Assessment
• Ultrasound– GA– Placentation/Abruption– Fetal viability– Extent of fetal trauma/demise– BPP?
• Celestone as indicated• Initiate FHM after patient is stabilized• Vaginal exam to rule out PROM

General Management PrinciplesGeneral Management PrinciplesMaternal AssessmentMaternal Assessment
• Rhogam:– Administer within 72 hrs– 10-30% of trauma have evidence of admixture– Betke-Kleihaurer test to determine quantity of
hemorrhages – 90% of hemorrhages are < 30 cc
• Anterior placed placentas have higher risk
General Management PrinciplesGeneral Management PrinciplesMaternal AssessmentMaternal Assessment
• Exploratory Laparotomy– usually necessary in penetrating trauma
– C/S may be required to attain adequate surgical exposure
• Tetanus– As usual
Imaging & RadiationImaging & Radiation
Harmful effects:1. Cell death and teratogenesis
– High doses of radiation before implantation is likely lethal
– In humans, high dose growth restriction, microcephaly, mental retardation
– Effects are greatest at 8-15 wks gestation– No proven effects before 8 wks or after 25 wks– Risks are not increased until radiation exposure = 5
rad

Fetal Radiation Exposure in typical trauma
Fetal Exposure
CXR (2 views) 0.02-0.07 mrad
Abdo XR (3 views) 100 mrad
CT Head/Chest <1 rad
CT Abdo 3.5 rad
Total 4.8 radACOG guidelines suggest that imaging is
safe when exposure is ≤ 5 rad
Imaging & RadiationImaging & Radiation

Blunt TraumaBlunt Trauma
• MVAs and abuse most common• Fetal death can follow direct blunt trauma or
maternal death– Specifically head trauma and ejection from vehicle
• Abdominal contents shifted in pregnancy– Retroperitoneal & splenic injury more frequent – GI injuries less frequent

Blunt Trauma - ConsequencesBlunt Trauma - Consequences• Placental Abruption
– In up to 40% of severe blunt trauma– In up to 3% of minor blunt trauma– Contractions q10min = 20% risk of abruption– Abruption confers 50% fetal mortality
• Uterine rupture– Increases with force and gestation– Fetal death frequent here, but maternal death 10%
• Pelvic Fracture– Consider fetal skull fracture– MAST trousers contraindicated– If stable vaginal delivery still feasible
• Pre-Term Labour …

Blunt Trauma – Pre Term LabourBlunt Trauma – Pre Term Labour
Can PTL be predicted after blunt abdominal trauma?• 85 patients over 3 yrs with non-catastrophic trauma
Findings• Preterm Labour in 13 (15%)• Presence of Abdo pain or Contractions do not predict
PTL• Domestic abuse victims were more likely to have
repeated trauma
(Pak 1998)

MVAsMVAs
Frequency
• In USA, 2% of all live births have been exposed to a reported MVA
Seatbelts
• Up to 25% of pregnant drivers are unrestrained.
• Seatbelts positioned improperly cause a 3-4 fold increase in energy transmission through the uterus
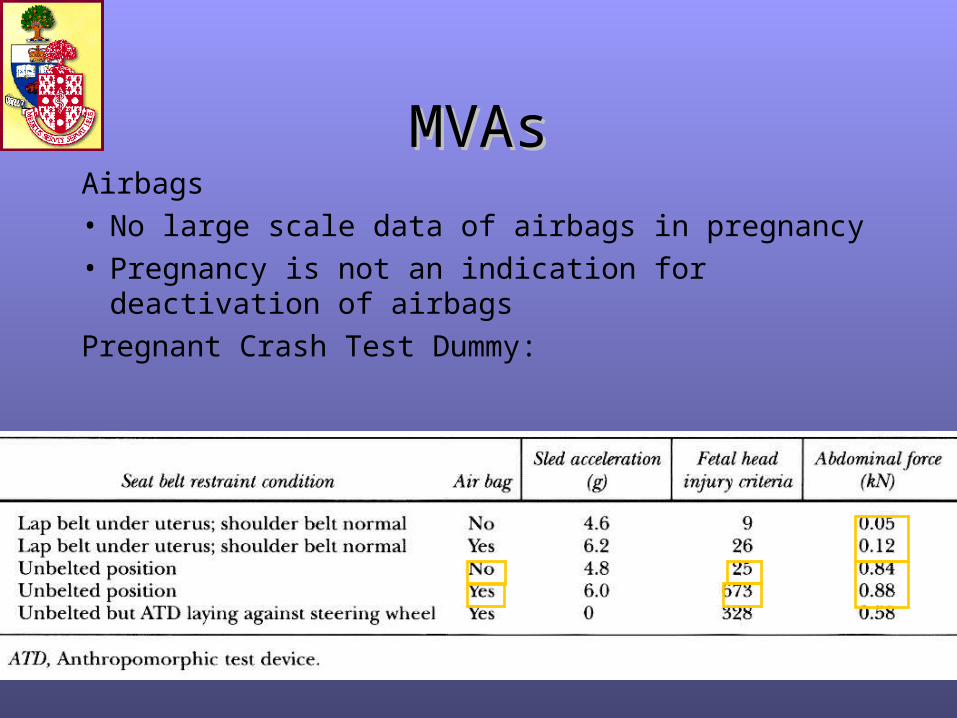
MVAsMVAsAirbags
• No large scale data of airbags in pregnancy
• Pregnancy is not an indication for deactivation of airbags
Pregnant Crash Test Dummy:
Penetrating TraumaPenetrating Trauma
• Uterus may serve to protect maternal organs– Visceral injury from penetrating trauma in pregnancy =
38% vs 90%– Of GSWs to abdomen, death in pregnancy is 1/3 rate of
non-pregnant– Fetal death rate: 71% of GSWs, 42% stabs
• Penetrating trauma is generally an indication for exploratory laparotomy
• Half the women had perinatal deaths due to either maternal shock, uteroplacental injury, or direct fetal injury.

A Unified ApproachA Unified Approach
Is there a need for a standardized protocol for obstetrical patients who experience trauma?
The low incidence of trauma during pregnancy leaves trauma teams at risk of ignoring steps that may prevent adverse outcomes. An organized approach of stabilizing the injured gravida and then initiating ultrasound and EFM in pregnancies beyond 24 wks will ensure the best outcome for the mother and her unborn child. It is now a requirement in Australia for a level 1 trauma centre to have a protocol detailing the management of pregnant patients after trauma.

A Unified ApproachA Unified Approach
Issues to consider• Delayed monitoring during primary survey and imaging
– Average time to clear c-spine estimated at 36 minutes
• Access to FHR monitor in ER may not be available– Estimated that 15% of ERs in USA have this
• Other activities in resuscitation room may preclude continuous access to FH, or hinder ability to hear it
• Patients transferred to labour floor for ongoing monitoring may not receive optimal management of non-obstetrical issues– Eg. Soft tissue injury, Physiotherapy, occupational therapy, etc.

TRAUMA IN PREGNANCY- TRAUMA IN PREGNANCY- Key Points:Key Points:
• Trauma occurs in 6-7% of pregnancies• Physiologic changes of pregnancy may confuse the
picture• ABCs should not be abandoned in managing a pregnant
trauma patient• Consider Rhogam, Celestone, PROM, and initial FH
monitoring• Education regarding proper use of seatbelts in pregnancy is
paramount• Consideration of a standardized trauma protocol or record
for obstetrical use may be warranted.

TRAUMA IN PREGNANCY-TRAUMA IN PREGNANCY- Key Points: Key Points:
• Investigations ….LEYLAND’S AXIOM… “IF AN INVESTIGATION IS INDICATED DO IT”
• Fetal viability….24 weeks• Fetal monitoring….OBS/PERINATOLOGY• Transfer to regional center ONLY after
maternal stabilization
TRAUMA IN PREGNANCY:TRAUMA IN PREGNANCY:Head TraumaHead Trauma
• Dead Mother = Dead Fetus

CaseCase
• ID: 21 y/o G1 P0 @ 18/40
• HPI:– Sudden onset of colicky right sided pain– Anorexia– No BM x 3 days, emesis x 1– Warmth x 2 days– No dysuria, no gross hematuria, no PV bleeding

CaseCase
• O/E:– BP: 110/55; HR: 110 regular; RR: 18; Temp:
37.9– Abdo: uterine height of 20 cm, tender over right
side of abdomen w/ rebound– V/E: N

CaseCase
• DDx:– Appendicitis
– UTI
– Renal calculi
– Cholecystitis
– Ovarian cyst / torsion
– Ligamentous pain
– Cecal diverticulitis
– Acute iliitis

CaseCase
• Investigations?• Labs:
– Hb 130, WBC 14, Plt 350– Lytes, Cr, liver tests all normal– Urine R&M – trace protein, no leuks, no bacteria, trace
blood
• Imaging:– Fetal U/S – BPP 8/8– RLQ U/S - compressible blind-ended tubular structure
w/ a maximal diameter of 9 mm, wall thickened to 5 mm
Appendicitis - BackgroundAppendicitis - Background
• Of the most common causes of the acute abdo
• Peaks in 2nd and 3rd decades of life, M>F• Anatomy:
– Lies in the RLQ of the abdomen– Exceptions:
• Malrotation (LUQ)• Pregnancy (RLQ-RUQ)
EpidemiologyEpidemiology
• Incidence – 0.05-0.07%
• Perforation – 20-55% (versus 4-19% in general population)
• Fetal mortality – 1.5-9% w/o perf (up to 36% w/ perf)
• Overall correct diagnosis 50-86%

ClinicalClinical
• Symptoms non-specific initially• Initially dull, poorly localized periumbilical
pain• Localizes to McBurney’s point• Nausea/vomiting• Low grade fever ~38 (if rupture, fever
higher)• Eventually +/- peritoneal signs

Labs/ImagingLabs/Imaging
• Labs: elevated WBC, no abnormalities that indicated an alternate dx (liver functions, B-HCG, etc)
• CT: 95% spec and sens
• U/S: 81% spec, 86% sens

ManagementManagement
• Surgical• Preop
– Hydration– Abx prophylaxis
• Non-perfed: cefazolin 1 g IV, metronidazole 500 mg IV• Perfed: ceftriaxone 1 g IV, metronidazole 500 mg IV
• Delaying intervention for >24 hrs, risks perfs• Risk of preg comps (SA or prematurity) w/
laparotomy decrease with gestational age• May do laparotomy or laparoscopy

G.I. DISEASE IN PREGNANCY:G.I. DISEASE IN PREGNANCY:APPENDICITISAPPENDICITIS
• Fetal Mortality and Maternal Morbidity rates are directly correlated to the delay in diagnosis and treatment******

Acute cholecystitis - BackgroundAcute cholecystitis - Background
• A syndrome with:– RUQ pain– Fever– Leukocytosis– Assoc w/ GB inflammation usually due to
gallstone (in preg – 90%)

EpidemiologyEpidemiology
• Incidence of <0.1% in pregnancy
• Maternal mortality 0-1%– 15% with pancreatitis
• Fetal mortality 10-20%– 60% with pancreatitis

ClinicalClinical
• RUQ/epigastric pain, steady and severe >4-6 hours
• Nausea/vomiting, anorexia• Fatty food ingestion exacerbates pain 1
hour after intake• Ill looking, tachycardic, febrile, lie still,
peritoneal signs, +ve Murphy’s sign (inspiratory arrest) +/- jaundice

PathophysiologyPathophysiology
• Pregnancy predisposes to accumulation of GB stones by:– Increasing viscosity of bile– Increasing the number of micelles on which
cholesterol crystals precipitate– Relaxing the GB leading to stasis
• Increased risk of cholelithiasis stays for up to 5 years postpartum

Labs/ImagingLabs/Imaging
• Labs:– Elevated WBC w/ left shift– Elevated bili and ALP, +/- high AST/ALT/amylase
• U/S:– Cholelithiasis– Wall thickening >4.5 mm– Sonographic Murphy’s sign– Dilation of GB– Sens 88%, spec 80%
• HIDA scan – Sens 97%, spec 90%

ManagementManagement
• IV hydration• Analgesia
– Demerol preferred over morphine (morphine may produce spasm of sphincter of Oddi)
• NPO• Abx
– Metronidazole 500 mg IV q8h– Ceftriaxone 1 g IV q24h

ManagementManagement
• Surgery is safest to perform during TM2• Laparoscopic cholecystectomy has been
performed during pregnancy but safety is uncertain
• Patients w/ choledocholithiasis or pancreatitis can be mx w/ ERCP w/ sphincterotomy
• If preg and have gallstones but asymptomatic – no surgery
• Pre-preg if have symptoms consistent w/ gallstones consider cholecystectomy
G.I. DISEASE IN PREGNANCY:G.I. DISEASE IN PREGNANCY:BOWEL OBSTRUCTIONBOWEL OBSTRUCTION
• Morbidity and Mortality related to the delay in diagnosis*
• Previous Surgery and Adhesions--3d TM
• Volvulus, Hernia, Intussusception
• Signs and Symptoms =
• Diagnosis Serial Assessments and Serial AXRs
• Management?

CASE 2CASE 2
• “THE MOOSE STORY”

CASE 2CASE 2
• “THE MOOSE STORY”
• NOW IN THE NEUROSURGICAL ICU
• CONSULTS OBS RE CT, ANGIOGRAPHY
• CONSIDERATION OF TERMINATION?

CASE 2CASE 2
• “THE MOOSE STORY”
• THE HAPPY ENDING……….
CASE 3CASE 3
• 30 YR OLD WOMAN AT 24 WEEKS GESTATION MVA HIT FROM BEHIND
• HAD SEAT BELT ON, NO HEAD INJURY• O/E VSS, BRUISED AND TENDER
ABDOMEN• FETAL HEART TONES HEARD• WHAT ARE THE ISSUES HERE?
CASE 3CASE 3
• MATERNAL CONSIDERATIONS FIRST!
• FETUS SECONDARY
• MONITORING IF FETUS VIABLE
• FETAL MATERNAL TRANSFUSION
BETKE-KLEIHAUER
• SURGICAL DELIVERY IF FETAL DISTRESS AND MOTHER IS STABLE

SURGERY IN THE SURGERY IN THE PREGNANT PATIENTPREGNANT PATIENT
Learning objectives:
1)TRAUMA IN PREGNANCY
2)THE ACUTE ABDOMEN IN PREGNANCY
3)CASES
THANKS!
SURGERY IN THE SURGERY IN THE PREGNANT PATIENTPREGNANT PATIENT
• AVOID “THERAPEUTIC PARALYSIS”• IF AN INVESTIGATION IS INDICATED
FOR DIAGNOSIS ---DO IT!• NEVER COMPROMIZE THE MATERNAL
CARE FOR THE SAKE OF THE FETUS!• THERE ARE VERY FEW DRUGS OR
INVESTIGATIVE TESTS WHICH CAUSE SERIOUS FETAL DAMAGE





























