Embed Size (px)
Citation preview

British Heart Journal, 1975, 37, 1277-1280.
Transmission of audible praecordial gallopsounds to right supraclavicular fossa'
George J. DiDonna, Robert A. O'Rourke,2 Kirk L. Peterson, and Joel S. KarlinerFrom the Cardiovascular Division, Department of Medicine, University of California at San Diego, U.S.A.
To evaluate the significance of audible gallop sounds in the right supraclavicular fossa we performed simul-taneous external heart sound recordings at 50 and 100 Hz at the left ventricular apex, left sternal border,and right supraclavicular fossa in 50 patients with audiblegallop sounds at the left ventricular apex. In eachpatient heart sounds were recorded with a simultaneous jugular phlebogram, apex cardiogram, and carotidpulse tracing. In 44 patients an apicalfourth heart sound coincident with the 'a' wave of the apex cardiogramwas recorded, and in 32 (73%) thefourth heart sound was audible and recordable in the right supraclavicularfossa. A left ventricular third heart sound, coincident with the rapid filling wave of the apex tracing, waspresent in 25 patients but was recorded in the right supraclavicular fossa in only 7 (28%). Intracardiacphonocardiography (high-fidelity catheter) was performed in six patients with left ventricular gallop soundsand in each instance arterial transmission of the third orfourth heart sound, or both, was present. Five addi-tional patients had a prominent low-frequency event recorded in the right supraclavicular fossa precedingthe peak of a prominent jugular venous 'a' wave, but only two had a soft parasternal fourth heart sound.Intracardiac phonocardiography in these five patients failed to reveal transmission of right ventricular gallopsounds to the superior vena cava.
We conclude that since left ventricular gallop sounds commonly are transmitted to the right supraclavicularfossa auscultation in this area is often helpful in their detection. In addition, a prominent jugular venous
'a' wave somotimes produces recordable presystolic vibrations that are occasionally audible as well.
Once the clinician has detected a gallop rhythmduring routine auscultation of the praecordium heis faced with the problem of deciding whether theseheart sounds emanate from the right or left ven-tricular chamber. A separate but related problemcommonly faced in clinical practice is the detectionof such gallop rhythm in patients with obesity orobstructive lung disease. Since it has been observedthat gallop sounds can often be heard with thestethoscope in the supraclavicular fossae (W. P.Harvey and A. DeLeon, 1969, personal communi-cation) we sought to determine the frequency withwhich this happens in respect of the right supracla-vicular fossa. In addition, we sought to ascertainwhether transmission of such sounds is specific forevents which originate in the left ventricle.
Received 24 March 1975.'Supported in part by USPHS Training Grant.'Teaching Scholar of the American Heart Association.
Patients and methods
A total of 60 patients were studied. Fifty had organicheart disease of left ventricular origin except for fivepatients with a physiological third heart sound. Tenpatients had organic cardiac disease involving only theright ventricle. In each patient praecordial gallop soundswere heard by more than one examiner. Auscultation inthe supraclavicular fossa was performed using the bellof the stethoscope, which was placed in the rightsupraclavicular fossa with the patient's head turnedslightly to the left. The examination was performned inheld expiration with the patient instructed to avoid aValsalva manoeuvre. Simultaneous phonocardiogramswere recorded at the cardiac apex, left stemal border,and right supraclavicular fossa at 50 and 100 Hz. Allrecordings were made with the patient lying supineduring held expiration using an Elema-ShonanderMingograph-75 with EMT-25b contact microphones.With each phonocardiogram a jugular phlebogram,apex cardiogram, and carotid pulse tracing were alsoobtained. Intracardiac phonocardiography was per-formed in 11 patients using a high-fidelity micromano-
copyright. on N
ovember 1, 2020 by guest. P
rotected byhttp://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.12.1277 on 1 Decem
ber 1975. Dow
nloaded from

1278 DiDonna, O'Rourke, Peterson, and Karliner
meter tipped catheter'. Six of these patients had gallopsounds originating in the left ventricle, while fivepatients exhibited right ventricular gallop sounds.
50-
O.
4-E- 2 5-
z
0
S3 atopex
Apical S3ImcJIKC
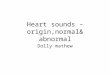
FIG. 1 Incidence of radiation of praecordial gallopsounds to right supraclavicular fossa (SCF). S3=third heart sound. S4-=fourth heart sound.
Results
An apical fourth heart sound was audible in 44patients. In 32 (73%) of these patients it was re-corded in the right supraclavicular fossa (Fig. 1).In each instance the fourth heart sound was coinci-dent with the 'a' wave of the simultaneously re-corded apex cardiogram (Fig. 2). Twenty-eightpatients had an apical third heart sound coincidentwith the rapid filling wave of the apex cardiogram.Only seven (28%) of these were recorded in the rightsupraclavicular fossa. In six patients gallop soundswhich were recorded in the left ventricle displayeddiscrete arterial transmission (Fig. 3).An additional group of five patients who had
evidence of right ventricular disease also werestudied by external phonocardiography. Two ofthese patients had primary pulmonary hypertension,one had chronic obstructive lung disease, one had anatrial septal defect (pulmonary to systemic flowratio of 3:1), and one had pulmonary stenosis.Each patient exhibited a prominent but low-frequency sound in the neck which preceded thepeak of a prominent jugular 'a' wave (Fig. 4) and intwo of these patients a presystolic sound wasrecordable at the left sternal border. In one otherpatient the 'v' wave of the jugular venous pulse was
Cardiomyopothy
RiqhtSCF-
,j.
5~~~I
...~~~~~~~~~~~ ~ ~~~~~ ~ ~ ~~ ~ ~ ~ ~~~~~~~~~~~~~~~~~~.............: \ACG
FIG. 2 Typical example of transmission of an apical fourth heart sound(S4) to the right supraclavicular fossa (SCF). The S4 is coincident with the'a' wave of the simultaneously recorded apex cardiogram (ACG).
Millar Instruments, Houston, Texas.
ECG
copyright. on N
ovember 1, 2020 by guest. P
rotected byhttp://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.12.1277 on 1 Decem
ber 1975. Dow
nloaded from

Audible praecordial gallop sounds to right supraclavicular fossa 1279
associated with an apparent third heart sound buta third heart sound was not recorded at the lowerleft sternal border. In an additional group of fivepatients with right ventricular disease intracardiacphonocardiograms demonstrated either a rightventricular third or fourth heart sound in each.These gallop sounds, however, could not be re-corded in the superior vena cava.
Discussion
Auscultation in the supraclavicular and carotidregions is usually performed to detect carotid orsubclavian bruits, cervical venous hums, or to tracethe transmission of praecordial systolic murmurs.In the past little attention has been directed towardsthe appreciation of either the normal heart soundsor gallop sounds in these areas. Others haveobserved that gallop sounds can often be heard withthe stethoscope in the supraclavicular fossae (W. P.Harvey and A. DeLeon, 1969, personal communica-tion). Groedel and Miller (1944) were among thefirst to use modern methods to study the heartsounds over the great vessels of the neck. In each oftheir 24 cases the first and second heart sounds wererecorded over the jugular and carotid regions. Inone of their patients the heart sounds, includingboth third and a fourth heart sound, were recordedmore easily over the neck vessels than over thecardiac apex. The authors emphasized that soundsand murmurs originating in the heart are trans-mitted in the direction of the flow of blood alongthe walls of the great vessels. They concluded,however, that the arteries did not seem importantfor the transmission of the heart sounds andmurmurs with the exception of the audible eventsat the aortic valve region.Our results show that left ventricular gallop
sounds, especially the fourth sound, are often trans-mitted to the right supraclavicular fossa. Lessfrequently a third sound gallop can be recorded inthe same region. Recordings were made over theright supraclavicular fossa since we found it difficultto obtain adequate recordings over the carotidvessels. It is our contention that these sounds,which are generated in the high pressure leftventricular chamber, are propagated antegradely bymeans of transverse vibrations along the walls ofthe great arteries, as has been reported experi-mentally by Farber and Purvis (1963). Not onlymay these sounds be recorded after a variable butshort delay in the right supraclavicular fossa butwhen the bell of the stethoscope is placed lightlyover the right supraclavicular fossa such gallopsounds are often easily audible. Why the third heartsound should be transmitted so much less frequently
is not clear, but this phenomenon may be related tothe active nature of fourth heart sound production-that is, to atrial contraction-compared with theessentially passive nature of third heart soundproduction. Whether the presumably greaterkinetic energy imparted by the former accounts forthis difference must remain speculative.During the course ofour studies it became evident
that it was possible also in patients with rightventricular dysfunction to record apparently promi-
Cardiomyopathy
LV preurem(Millar) S4 ;Ic
V
A
Aorta
.111--j II1% -I
=
Subclaviin
!;'+'~, *_, 4 7'0''0;
FIG. 3 Arterial transmission of a fourth heartsound (S4) recorded by Millar high-fidelity micro-manometer-tip catheter. The S4 is coincident with theCa' wave of the left ventricular pressure pulse.In this instance the third heart sound (S3) is nottransmitted to the arteries. ICP=intracardiacphonocardiogram.
copyright. on N
ovember 1, 2020 by guest. P
rotected byhttp://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.12.1277 on 1 Decem
ber 1975. Dow
nloaded from

1280 DiDonna, O'Rourke, Peterson, and Karliner
10 Pulmonory hypertension
ECG_ b.
Right __ ¢ 4 fw12SCF'
2nd leftt.4
JVP's
FIG. 4 Prominent presystolic 'sound' is recorded in right supraclavicularfossa (SCF) in patient with primary pulmonary hypertension. Vibrationbegins before the peak of a prominent jugular venous "a' wave. Aprominent S4 is not seen at second left intercostal space (ICS). Probably theprominent jugular venous 'a' wave is responsible for vibration recorded in theSCF. Note wide splitting of second heart sound. JVP=jugular venous pulse.
nent third and fourth heart sounds in the rightsupraclavicular fossa. However, these easily re-
cordable events were less commonly audible in theright supraclavicular fossa, possibly because of theirlower frequency (less than 50 Hz). Audible soundscorresponding to recordable events in the neck werenot present upon praecordial auscultation, nor
could they be recorded along the left sternal border.We contend that prominent jugular venous pulsa-tions may lead to the recording, and at times to theauscultation, of these vibrations. A similar explana-tion for the occurrence of presystolic clicks recordedover the jugular venous pulsation in patients withtricuspid regurgitation has been offered by Abinader(1973). By contrast, when right ventricular gallopsounds were recorded within that chamber trans-mission to the superior vena cava could not bedemonstrated. This observation is consistent withthe hypothesis that arterial sounds are transmittedthrough vessel walls. Presumably the arterial wall ismore conducive to such sound transmission than arethin-walled veins.The diagnostic and prognostic importance of prae-
cordial gallop sounds is well known. Both third and
fourth heart sounds can be difficult to hear for avariety of reasons. The observation that the leftventricular fourth sound and, less frequently, theleft ventricular third sound are transmitted to thesupraclavicular fossae increases the likelihood thatthey will be more frequently recognized in patientsin whom routine praecordial auscultation is difficult,such as commonly occurs in patients with obesity orhyperinflation of the lungs.
References
Abinader, E. G. (1973). Systolic venous reflux sounds.American Heart J'ournal, 85, 452.
Farber, J. J., and Purvis, J. H. (1963). Conduction of cardio-vascular sound along arteries. Circulation Research, 12,308.
Groedel, F. M., and Miller, M. (1944). Studies on theacoustic phenomena over the vessels of the neck in thehealthy and the diseased heart. Experimental Medicineand Surgery, 2, 193.
Requests for reprints to Dr. Joel S. Karliner, UniversityHospital, 225 W. Dickinson Street, San Diego, Cali-fornia 92103, U.S.A.
copyright. on N
ovember 1, 2020 by guest. P
rotected byhttp://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.12.1277 on 1 Decem
ber 1975. Dow
nloaded from



![Research Article ...downloads.hindawi.com/journals/abi/2012/327269.pdf · while pathological heart sounds, such as heart murmurs, are high-frequency, noise-like sounds [6]. Heart](https://img.dokumen.tips/doc/110x75/5fd0e4c6f4f6f44dac3dda1b/research-article-while-pathological-heart-sounds-such-as-heart-murmurs-are.jpg)