Embed Size (px)
Citation preview

C H A P T E R
11
Translational NeuroimagingSubstance Abuse Disorders
Adam J. Schwarz 1, Martin H. Plawecki 2, DavidL. McKinzie 3, Conrad J. Wong 4
1Translational Medicine, Eli Lilly and Co., 839 S. Delaware Street,
Indianapolis, IN 46285, USA2Department of Psychiatry, Indiana University School of Medicine,
Goodman Hall. 355 W. 16th St., Suite 4800, Indianapolis, IN 46202, USA3Neuroscience Discovery Research, Eli Lilly and Co., 839 S. Delaware Street,
Indianapolis, IN 46285, USA4Early Phase Clinical DevelopmentdNeuroscience, Eli Lilly and Co.,
839 S. Delaware Street, Indianapolis, IN 46285, USA
T
h
1.0. Introduction 3
081.1. Models of Drug Dependence 309 1.2. Imaging the PhysiologicalSubstrates of Substance Abuse 310
2.0. Preclinical 3
112.1. Animal Models of SubstanceAbuse 311
2.2. Imaging in Animal Modelsof Drug Dependence 312
2.2.1. Studies in Naive Animals:Acute Effects of Abused
Substances on Brain
Function
3122.2.2. Functional Imaging of
Genetic Models
316307ranslational Neuroimaging
ttp://dx.doi.org/10.1016/B978-0-12-386945-6.00011-1
2.2.3. Effects of Chronic
Drug Exposure on
Brain Physiology and
Function
3172.2.4. Effects of Self-
Administration on
Functional Response to
Drug Challenge
3182.2.5. Dopamine Release and
Conditioned Place
Preference
3182.3. Summary of Preclinical Modelsand Imaging 319
3.0. Clinical-Experimental MedicineModels and Drug Studies 3
20� 2013 Elsevier Inc. All rights reserved.

11. TRANSLATIONAL NEUROIMAGING308
3.1. Human Experimental ModelsAvailable for SubstanceAbuse 32
0 3.1.1. Pharmacological Models 3203.2. Imaging Applied to ExperimentalModels, Disease State,and Pharmacotherapyin Humans 322
3.2.1. Effects of Chronic DrugExposure on Brain
Structure and
Neurochemistry
3223.2.2. Imaging Direct
Pharmacological Effects
on Neurochemistry
3233.2.3. Imaging Direct
Pharmacological Effects
on Resting Brain
Function
3243.2.4. Functional Responses to
Alcohol-Related
Olfactory and Gustatory
Cues
3253.2.5. Modulation of
Functional Responses to
Task-Based fMRI
Paradigms
3263.2.6. Functional Imaging
Studies of
Pharmacotherapy
3273.3. Summary 328
4.0. Translational Imaging of SubstanceAbuse Models for Drug Discoveryand Development 3
294.1. Drug Discovery 329 4.2. Clinical Development 330 4.3. Translation 331SummarySubstance abuse disorders represent a major source of morbidity and mortality throughout the world and aremost succinctly characterized as the recurrent use of a substance despite problems directly related to thatusage. Animal models offer the possibility of experimental constructs through which cardinal processesunderlying substance abusedacquisition of dependence, craving, withdrawal, and relapsedcan be under-stood. A key finding that has emerged from different functional imaging paradigms in both animals andhumans over a range of drugs of abuse is a core involvement of the mesolimbic dopamine reward system.Functional imaging studies have now demonstrated clear evidence of pharmacological effects on this circuitand potential neuronal substrates of genetic factors, a promising avenue for the identification and validationof drug targets. We review major findings in this field and discuss how imaging of substance abuse andexperimental models thereof might be more closely integrated into drug development.
1.0. INTRODUCTION
While the exact definition may change over time [Diagnostic and Statistical Manual ofMental Disorders, 4th Edition, Text Revision (DSM-IV-TR); DSM V, proposed revision],substance abuse disorders are succinctly characterized as the recurrent use of a substancedespite problems directly related to that usage. These problems may exist in any and allaspects of an individual’s lifedfrom social to physiological (tolerance and/or withdrawal)to neuropsychiatric. These problems, particularly when they include legal substances suchas alcohol and nicotine, are a major source of morbidity and mortality throughout theworld.1e5

1.0. INTRODUCTION 309
While many investigators seek to identify risk factors (e.g. genetics and life stress) leadingto the eventual development of a substance abuse disorder, repeated exposure to thesubstance is a prerequisite condition for a problematic pattern to develop. Consequently,most experimental models, whether human or animal, require the subject to have thesubstance of interest administered and its physiological, behavioral, and subjective effectsmonitored.
1.1. Models of Drug Dependence
Key features of drug dependence:
(1) The development of drug tolerance;(2) Awithdrawal syndrome when drug consumption is ceased or substantially reduced
abruptly;(3) Relapse, typically as a result of exposure to stress or drug-associated cues that lead to
reexposure to the drug.
However, not all people exposed to drugs with high propensity for abuse show similarhigh intake patterns and the development of dependence, suggesting the presence of stronggenetic influences on the predisposition to drug dependence. For example, a familial historyof alcoholism doubles the chance of an individual becoming alcohol dependent.6
Importantly, drugs abused by humans are also preferentially self-administered bya diverse range of species.7 This strong cross-species homology enables environmental andgenetic determinants, as well as combinations of these two aspects, to be modeled in therodent with a high degree of control over experimental parameters defining the acquisitionof dependence, withdrawal, and reinstatement. The development of dependence can bemodeled preclinically through repeated exposure (forced or self-administered) methodo-logies and the influence of genetics (e.g. selected breeding lines or transgenic manipulations)can be superimposed upon these models to reflect geneeenvironment interactions uponfactors mediating addiction processes (i.e. drug taking, dependence, withdrawal, andrelapse).8 Animal models offer the possibility of studying components of addiction undergreater experimental control, free from confounds such as variable prior history of substanceuse or abuse and comorbidities that inevitably exist in the human disorder itself. On the otherhand, the potential sensitivity of behavioral, biochemical, and imaging readouts to specificsof the model (e.g. strain) can undermine the generalizability of findings.
In turn, human experimental medicine methods have been developed that allow the studyof drug administration (and in particular self-administration) under controlled conditions inthe laboratory, allowing some aspects (e.g. controlled administration schedule) of the preclin-ical models to be paralleled; however, ethical considerations limit the applicability of suchmodels in healthy subjects. Depending on the model and the amount of consumptioninvolved, studies of licit and illicit substances of abuse can be performed in subjects alreadyusing the substance. Differential exposure patterns (e.g. social drinkers, alcoholics, or light orheavy smokers) and familial history or genetic risk can be studied. In order to probe thecentral pharmacology underlying the effects of abused substances (and the treatmentthereof), neuroimaging studies can be performed both in experimental models and directlyin the target population.

11. TRANSLATIONAL NEUROIMAGING310
In this chapter, we provide an overview of these models and review the neuroimagingmethods that have been brought to bear on them. We also address the actual and potentialutility of these imaging approaches in both discovery and development of medicines tocombat substance abuse. Although we concentrate on alcohol and nicotine addiction, find-ings and commonalities of other abused substances are discussed where appropriate, withmechanisms that may be efficacious across many drugs of abuse,9 consistent with action ata core, common biological feature of abused substances.10
Alcohol abuse and dependence remains a significant health problem in the world.Approximately 30% of the adult US population meet diagnostic criteria for an alcohol usedisorder in their lifetime and 8.5% have met the criteria within the past 12months.11 In theEuropean Union, an estimated 3.4% of individuals older than 15 years satisfy the diagnosticcriteria for alcohol dependence in the past 12 months.2 In the United States, alcohol-relatedconditions were estimated to cost $184.6 billion in 1998, the most recent year with availabledata,12 and were associated with nearly 40% of automobile fatalities13 and contributed tosignificant medical disabilities.11 Similarly, alcohol use disorders cost 48.9 per 100,000disability-adjusted life years in Europe and are the first and third highest single causes ofmorbidity and mortality for men and women, respectively.2 Despite the enormity of thisproblem, only approximately one-quarter of those diagnosed with alcohol dependencereceive treatment in the USA.11
1.2. Imaging the Physiological Substrates of Substance Abuse
A range of neuroimaging methods have been used to characterize models of substanceabuse and probe the effects of pharmacological intervention. These approaches are typicallycategorized in one of three ways:
• Characterization of basal brain characteristics. In this approach, the imagingexperiment assays the effect of repeated drug exposure on measures of restingbrain parameters in the absence of any applied stimulus or additional experimentalprobe.
• Acute pharmacological challenge. This approach uses acute drug challenge as anexperimental probe to drive the signal changes of interest. This can be applied inanimals and humans to characterize the effect of a compound of interest per se.The compound could be an abused substance, a putative treatment, or a combinationof both.
• Response to a behavioral task or stimulus. In preclinical experiments, this approachrequires a conscious, behaving animal and so is not applicable to magnetic resonanceimaging (MRI)-based methods.i
However, nuclear medicine approaches enable the use of ligands such as 2-deoxyglucose(2-DG) or 18F-fluorodeoxyglucose positron emission tomography (FDG-PET) to measure
iAlthough imaging methods using conscious animals are not usually performed, such methods are being
developed. Nevertheless, it is important to point out that the behavioral repertoire of the animal within
a scanner is necessarily limited. Please refer to Ferris et al. in Chapter 3, Small Animal Imaging as a Tool for
Modeling Central Nervous System Disorders: Strengths and Weaknesses, in this volume.

2.0. PRECLINICAL 311
glucose uptake, or 11C-raclopride PET to measure dopamine (DA) D2 receptor binding, cor-responding to accumulated tracer uptake over the time window of the behavioral paradigm(see above).ii In clinical studies, this is usually probed by functional MRI (fMRI) methods,using scanner-compatible tasks.
2.0. PRECLINICAL
2.1. Animal Models of Substance Abuse
There is no true animal model of alcohol or drug addiction that recapitulates the fullspectrum of characteristics that define the clinical condition. Thus, preclinicalapproaches toward advancing our knowledge of mechanisms that mediate the reinforc-ing properties of abused substances have implicitly and explicitly attempted to modelspecific endophenotypes associated with substance abuse disorders. For instance, whilemost animal models have been based on self-administration procedures, others haveexamined neuroadaptive changes following acute or chronic forced substance adminis-tration. Measurement endpoints are varied and designed to elucidate specific pheno-types of interest that relate to core symptoms of clinical addiction disorders. Forexample, to study processes involved in drug dependence, forced administration proce-dures (e.g. ethanol vapor inhalation, subcutaneous nicotine or morphine pellets, orchronic daily cocaine injections) are most commonly employed. The advantage of forcedadministration procedures is that drug exposuredparticularly peak drug levelsdisbetter controlled than can be achieved under chronic, voluntary self-administrationparadigms. In other instances, the objective might be to explore mechanisms underlyingdrug relapse where the subject’s response to drug or associated cues is measuredfollowing an abstinence period from drug taking. The measures could be behavioral(e.g. self-administration) or neurochemical/metabolic [e.g. dopamine efflux in thenucleus accumbens (NAcc) or neuronal activation], but reflect the organism’s responsenot necessarily to the drug itself, but rather to stimuli associated with drugavailability.
The influence of genetics is a factor commonly integrated with environmental manipula-tions. Genetic animal models of addiction disorders can be classified within three generalcategories:
(1) Selectively bred lines for a particular phenotype;(2) Specific targeted or spurious gene mutations or deletions that have concomitant (and
sometimes unexpected) effects upon addiction-related physiology;(3) Inbred lines on an undefined genetic composition that exhibit an addiction-like
phenotype.
iiPlease refer to Wise in Chapter 1, Neuroimaging Modalities: Description, Comparisons, Strengths and
Weaknesses; and Brown in Chapter 2, Magnetic Resonance Imaging as a Tool for Modeling Drug Treatment
of Central Nervous System Disorders: Strengths and Weaknesses, in this volume for detailed discussions of
neuroimaging modalities.

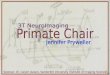
FIGURE 11.1 Endophenotypes and methodologies commonly used in preclinical addiction para-
digms. Autonomic refers to methods that measure cardiovascular and body temperature parameters, for example.CPA, conditioned place aversion; CPP, conditioned place preference; ICSS, intracranial self-stimulation; LMA,locomotor activity; RR, rotor-rod; SA, self-administration; TA, taste aversion.
11. TRANSLATIONAL NEUROIMAGING312
Many studies have used these genetic approaches to dissect the components of drugaddiction. Figure 11.1 highlights common endophenotypes studied in addiction paradigms,as well as the methods used. It is important to point out that a single methodology, such asself-administration, can be conducted under a multitude of variables. For instance, self-administration can involve free-choice drinking (continuous or scheduled access) or invokeoperant paradigms using different schedules of reinforcement (e.g. progressive ratio to assessthe motivational properties of the drug under study). Moreover, self-administration can beadapted to assess tolerance and drug withdrawal effects, and is commonly used to inferpropensity for drug relapse when extinguished operant responding is reinstated followingexposure to the drug or associated cues. Finally, the involvement of specific genes is oftenevaluated directly (e.g. specific receptor knockout mouse) or indirectly (e.g. using a ratline selectively bred for high alcohol drinking behavior).
2.2. Imaging in Animal Models of Drug Dependence
2.2.1. Studies in Naive Animals: Acute Effects of Abused Substances on BrainFunction
Many preclinical functional imaging studies of abused drugs have been mechanistic innature, seeking to map the acute central nervous system (CNS) effects of the substance itselfin naive animals, primarily rodents. Coupled with behavioral profiling, this approach has

2.0. PRECLINICAL 313
facilitated elucidation of the neuroanatomical substrates of drug actions. This careful charac-terization of acute drug response has served as a template for exploring neuroadaptiveprocesses involved in drug dependence, withdrawal, and relapse.
2.2.1.1. ALCOHOL
A range of 2-DG experiments have characterized patterns of brain metabolism changesthat parallel behavioral observations of excitatory effects at lower doses and in the ascendingblood alcohol level (BAL) phase and more depressive effects at higher doses and in thedescending BAL phase. Early studies examined relatively high doses (> 0.8 g/kg) and thelatter phase of the BAL curve and found monotonic dose-dependent local cerebral glucoseutilization (LCGU) reductions in brain structures, including the auditory and visualsystems.14,15 Lower range of doses (< 1.0 g/kg) in the early BAL phase revealed a biphasicdose response consistent with the behavioral profile outlined above.16 At a dose of0.25 g/kg, corresponding to a peak BAL of 20mg/dL at 10min, increases in LCGU localizedto mesocorticolimbic and nigrostriatal regions were observed; at an intermediate dose of0.5 g/kg this positive response was weaker, and at 1.0 g/kg decreased LCGU was observedin brain regions resembling those within the auditory/visual circuits identified as showingdecreased LCGU in the previous studies.16
Oral or intragastric routes of administration include the effects of gastric alcohol metabo-lism and more realistic pharmacokinetic profiles. A study with intragastric administrationat doses of 0.25, 1.0, and 2.0 g/kg with 2-DG administered just 3 min after ethanol, thuscapturing the ascending and plateau parts of the BAL curve, found increased LCGU in themesocorticolimbic system.17 The higher doses evidenced attenuated LCGU increases. More-over, the dopamine receptor antagonist, flupenthixol, was found to block the LCGU increasesinduced by 0.25 g/kg intragastric ethanol, consistent with a role for dopamine underlying thefunctional activation at low doses.18 The effects of flupenthixol were less clear at the higherdoses, however, implying a more complex central pharmacology in the higher dose range.Finally, a time-resolved study demonstrated that LCGU was increased in the basal gangliaimmediately following an intragastric dose of 0.8 g/kg ethanol, whereas at a later time point(45 min) decreased LCGU was observed.
Following these experiments, pharmacological MRI (phMRI) studies of alcohol challengein rodents have been performed. A subcutaneous dose of 0.6 g/kg ethanol induced wide-spread blood oxygenation level dependent (BOLD) signal decreases in the rat brain.19,20
Interestingly, these decreases were substantially attenuated by acute pretreatment with theAMPA receptor potentiator, LY404187, a compound that also reversed behavioral effects ofhigher, intoxicating doses of ethanol (1e2 g/kg).20 Moreover, a parallel experiment using2-DG in conscious animals revealed consistent effects: decreased LCGU induced by acute2.0 g/kg ethanol and reversal of these decreases in rats pretreated with LY404187.20
2.2.1.2. NICOTINE
A number of studies in the rat have characterized the effects of acute nicotine challengeon central measures of glucose metabolism (2-DG), early gene expression (c-Fos), and hemo-dynamic response (phMRI) in the rat over a range of doses and routes of administ-ration (Table 11.1). Overall, nicotine results in localized functional increases in all of theseimaging parameters, although dose dependence appears to be a function of brain region.

TABLE 11.1 Summary of Doses Examined in Imaging Studies of the Acute CNS Response to Nicotine inthe Rat
Modality Reference Route Dose (mg/kg free base)
2-DG London et al., 1985220 IV e e e e e e e e e 11.75 e
London et al., 198821,22 SC e e 0.1 0.3 e e e 11.0 e e e
Pontieri et al., 199627 IV 0.05 e e e e e e e e e e
c-Fos Ren and Sagar, 199224 IV (1h) e e e e e 0.5 e 11.0 e e 22.0
Matta et al., 199323 IV 0.05 e 0.1 e e e e e e e e
Pang et al., 199326 SC e e 0.1 e e e 0.8 11.0 11.4 e e
Sharp et al., 199325 IP e e e e e 0.5 e 11.0 e e 22.0
Kiba et al., 199326 SC e e e e e e e 11.0 e e e
Mathieu-Kia et al.,199830
SC e e e e 0.35 e e e e e e
phMRI (rCBV) Gozzi et al., 200629 IV e e e e 0.35 e e e e e e
Choi et al., 200628 IP e 0.07 e e e e e e e e e
2-DG, deoxyglucose; c-Fos, proto-oncogene c-Fos; IP, intraperitoneal; IV, intravenous; phMRI, pharmacological MRI rCBV, relative
cerebral blood volume; SC, subcutaneous.
11. TRANSLATIONAL NEUROIMAGING314
Early work identified stronger LCGU increases at 0.3 mg/kg than to 1.0 or 0.1 mg/kg.21,22
Dose-dependent increases in c-Fos immunoreactivity were noted in midbrain and subcor-tical structures,23e25 with 0.4 mg/kg determined to be sufficient for maximum c-Fos expres-sion in midbrain regions, and cortical structures being less extensively reported.26 In theanterior cingulate cortex, a dose-dependent increase in c-Fos expression was found betweenintravenous doses of 0.05 and 0.1 mg/kg,23 whereas these increases were observed toplateau at higher intraperitoneal doses of 0.5e2.0 mg/kg.25 In contrast, stronger, dose-dependent increases in the piriform cortex were observed at relatively high doses of1.0e2.0 mg/kg nicotine.25 A 2-DG study using a low dose (0.05 mg/kg), chosen as it wasshown to be behaviorally active in self-administration paradigms, found a differentialincrease in both LCGU and dopamine (measured by microdialysis) in the shell versus thecore of the Nacc.27 Later studies mapped the central response to acute nicotine challengeacross the whole brain more systematically using both c-Fos and phMRI techniques, demon-strating a strong correspondence in neuroanatomical pattern of response at 0.07 and0.35mg/kg;28e30 the strongest increases were observed in medial prefrontal and anteriorcingulate cortices, orbitofrontal cortex, NAcc, habenula, and anterior thalamic nuclei, aswell as in ventrolateral structures, including the amygdala, piriform cortex, and subiculum.The activated cortical structures are those with strongest dopaminergic innervation.
2.2.1.3. OTHER DRUGS
Acute challenge with both cocaine and d-amphetamine induces widespread increases infunctional imaging measures in the naive rat brain. The neuroanatomical distributionincludes particularly strong responses in many cortical regions as well as in subcortical

2.0. PRECLINICAL 315
structures (e.g. the NAcc) related to the mesolimbic dopaminergic system and relevant to thereinforcing properties of drugs of abuse. MRI studies using phMRI-like acquisition schemessensitive to BOLD,31,32 relative cerebral blood volume (rCBV),33e37 relative cerebral bloodflow (rCBF),38,39 cerebral metabolic rate of oxygen (CMRO2)
38 and manganese uptake40 allyield positive response patterns consistent with those observed in autoradiography studiesmeasuring rCBF41,42 and LCGU.42e47 In the case of d-amphetamine, functional connectivityanalyses have been applied to resolve the mesolimbic dopamine projections from the ventraltegmental area (VTA) to the ventral striatum and medial prefrontal cortex from the relativelynonselective univariate response pattern.48 These findings confirm the functional engage-ment of this key dopaminergic reward pathway in the response to amphetamine measuredusing these techniques.
2-DG studies exploring the doseeresponse relationship have found similar patternsfor both drugs, namely a more focal response, primarily involving the mesolimbic system,at low doses (approximately 0.2e0.5 mg/kg) with more widespread patterns, involvingthe nigrostriatal and extrapyramidal cortical regions, becoming significant at higherdoses, consistent with the dose-dependent onset of drug-induced locomotor activity andstereotypy.43,49 PhMRI doseeresponse studies have revealed negative rCBV responses inthe dorsal and ventral striatum at 0.25mg/kg, but not at higher doses up to 3mg/kg,at which the widespread positive response observed in other studies was observed, withthe most significant effects in the NAcc, caudate putamen, and insula cortex.50 These bivalentresponses were hypothesized to be due to differential affinities of dopamine for the presy-naptic D2/D3 autoreceptors (dominant at low doses) and excitatory postsynaptic D1/D5receptors (dominant at higher doses).
2.2.1.3.1. SPECIES-DEPENDENT VALENCE OF THE RESPONSE TO ACUTE COCAINE CHAL-
LENGE While the rat has been the most widely used preclinical species in imaging studiesof this type, the translatability of these experiments is contingent upon their consistencyacross species. Whereas positive metabolic and hemodynamic responses are reliablyobserved in the rat, experiments with both 2-DG and phMRI have shown that acute cocainechallenge induces negative response in both mice44,51 and nonhuman primates;52,53 in bothspecies, signal decreases in ventral and dorsal striatum and prefrontal cortical regionswere prominent. Mandeville and coworkers53 hypothesize that this difference in functionalresponse valence may be due to different relative densities of postsynaptic dopamine D1(excitatory) versus D2 (inhibitory) receptors, with D1:D2 ratios of approximately three inthe rat and closer to unity in mice, primates, and humans. Interestingly, phMRI responsesto cocaine in humans are mixed, with both positive and negative BOLD signal changes beingreported (see Section 3.0).
Applied to preclinical drug discovery, the rCBV response to amphetamine has also beenshown to be a useful imaging model to probe modulation by novel dopaminergiccompounds targeted at treating drug dependence. A substantial body of evidence frompreclinical drug-dependence behavioral models demonstrates the potential utility of selec-tive antagonism of the dopamine D3 receptor in the treatment of substance abuse.9 The DAD3 receptor has a focal distribution that overlaps the mesolimbic DA pathway and includesa high density in the NAcc.9 A series of imaging experiments in the rat demonstrated thatacute pretreatment with three different selective D3 antagonist molecules, from different

11. TRANSLATIONAL NEUROIMAGING316
chemical classes, consistently potentiated the rCBV response to d-amphetamine challengein the NAcc.37,54,55 This included an independent replication of the effect with one of thecompounds, the widely used tool compound, SB277011A,37,54 which was also shown todisrupt functional connectivity in the mesolimbic dopamine pathways.54 Consistent withthis body of work, an independent study found that the D2 antagonist, eticlopride, dose-dependently potentiated the rCBV response to d-amphetamine in the NAcc, in contrast tothe attenuation of the amphetamine-induced changes induced by the D2 agonistquinpirole.56
PhMRI studies of heroin in the rat have revealed that a 0.1 mg/kg intravenous chal-lenge elicits a mixture of both positive (sensorimotor cortex) and negative (prefrontalcortex and subcortical structures, including thalamus, hippocampus, and NAcc) BOLDresponses.57e59 These CNS signals were blocked by naloxone58,60 and suppressed bygamma-vinyl-g-aminobutyric acid (gamma-vinyl-GABA; a GABA transaminase inhi-bitor),58 consistent with the m-type opioid action of heroin and a downstream effect onGABA neurotransmission as part of the pharmacological action.
2.2.2. Functional Imaging of Genetic Models
2.2.2.1. ALCOHOL
Several 2-DG experiments have sought to elucidate the functional imaging correlates ofselectively bred rat models of alcoholism, specifically rats bred for high alcohol drinking(HAD) versus low alcohol drinking (LAD) behavior and alcohol-preferring (P) versus non-preferring (NP) rats (see Section 2.1). Interestingly, the functional CNS profiles of these twomodels are different in terms of both basal metabolism and evoked responses to an acutealcohol challenge. Whereas no significant difference was found in basal LCGU betweenHAD and LAD rats,61 P rats evidenced increased basal LCGU relative to both NP ratsand wild-type controls in brain regions involved in the mesolimbic dopamine pathway.62
In terms of response to acute alcohol doses, widespread reductions in LCGU were observedfollowing acute intraperitoneal doses of both 0.25 g/kg and 1.0 g/kg ethanol in LAD but notHAD rats.63 In contrast, an identical dosing paradigm resulted in stronger decreases inLCGU in P relative to NP rats,64 including regions involved in the mesolimbic system.This systematic and consistently executed set of studies, along with other neurobiologicalevidence,65 highlights the fact that markedly different functional and neurobiological effectscan underpin a similar behavioral phenotype (voluntary consumption of intoxicating levelsof alcohol).iii
2.2.2.2. NICOTINE
In the mouse, a phMRI study found relatively widespread BOLD increases in wild-typemice in response to 1mg/kg nicotine infusion, with strongest responses in frontal brainregions; whereas these responses were not present in high-affinity b2-containing neuronalacetylcholine receptor (b2*nAChR) knockout mice, implying that the central functional
iiiSee Steckler and Salvadore in Chapter 7, Neuroimaging as a Translational Tool in Animal and Human
Models of Schizophrenia, in this volume for further discussion on the application of imaging techniques to
help validate animal models of CNS disorders.

2.0. PRECLINICAL 317
response is dependent on b2* receptors.66 This is consistent with the observation that an a4b2
nicotinic receptor agonist elicited similar rCBV changes to nicotine in the rat.29
2.2.3. Effects of Chronic Drug Exposure on Brain Physiology and Function
2.2.3.1. ALCOHOL
The effects of chronic alcohol exposure on basal brain neurochemistry as detected bymagnetic resonance spectroscopy (MRS) appear complex. Increases in choline-containingmetabolites (Cho) have been observed in both the thalamus and basal ganglia after 16 and24week exposure67,68 along with decreases in the thalamus after 44 weeks.68 Interestingly,MRS analysis of ex vivo samples from one of these studies showed that the increasesat 16 weeks were driven primarily by increased phosphocholine, whereas decreases at40 weeks were driven largely by decreased glycerophosphocholine.68 Increases in Cho andglutamateþ glutamine (Glx) in the basal ganglia after 16 and 24weeks were monotonicallyrelated to BALs; however, other metaboliteetime profiles showed nonlinear behavior.67
These two studies are largely consistent but also indicate a complex set of underlying changesand the importance of parameters such as exposure duration on the direction of change.
Longitudinal structural MRI studies of brain volume in P rats over approximately 1 yearshowed continued growth of many brain structures both with and without free exposure toalcohol.69,70 Both studies investigated two independent cohorts of the P rats, but littleevidence of gross brain damage following chronic alcohol exposure was found, apart froma reduction in the corpus callosum. This stands in contrast to the widespread brain tissueshrinkage due to chronic alcohol exposure observed in humans (see Section 3.0).
Two early studies demonstrated substantially increased central blood flow and CMRO2 inacute alcohol withdrawal.71,72 These observations were consistent despite different adminis-tration schedules, i.e. 3e4 days intubation to severe intoxication71 versus 3 weeks ad libi-tum,72 although both studies measured the hemodynamic parameters at similar times aftercessation of alcohol (12 and 14e20 h respectively). A 2-DG study found similar increasesin LCGU at 16e24 h withdrawal following 4 days intoxication by intubation.73 However,these studies performed the imaging examinations under immobilization or anesthesia.A later 2-DG study using minimally restrained, conscious animals found the opposite effect;namely, reduced LCGU in cortical and limbic regions in acute (12e18 h) but not extended(14 days) withdrawal following 11 weekly episodes comprising 2-day intragastric ethanoladministration sufficient to cause severe intoxication.74 These studies highlight the potentialconfounding effects of anesthesia or invasive immobilization on functional readouts.
2.2.3.2. NICOTINE
Effects of passive chronic exposure to nicotine on the subsequent response to an acutenicotine challenge have been inconsistent, but were obtained using different paradigmsand dosing regimens. Experiments with constant infusion using implanted minipumps75
and thrice daily injections of 0.35mg/kg30 yielded functional sensitizationdincreasedresponses to nicotine challenge in many brain regions measured using 2-DG and c-Fosexpression, respectively. The potentiation was particularly pronounced in the latter experi-ment. However, another 2-DG experiment using twice-daily injections of 1mg/kg detectedfunctional tolerancedreduced responses to nicotine challengeddespite behavioral

11. TRANSLATIONAL NEUROIMAGING318
sensitization.76 The concentration and time profile during the chronic exposure phase wouldprobably be different in each of these experiments, although it is interesting that the twomostsimilar paradigms (repeated injections rather than constant infusion) yielded oppositeeffects.
2.2.4. Effects of Self-Administration on Functional Response to Drug Challenge
2.2.4.1. NICOTINE
The effects of a formal nicotine self-administration schedule on basal c-Fos expression, incomparison to saline administering and sham control groups, included increased expressionin many brain regions also activated in the response to acute nicotine challenge,28e30
including the prefrontal, anterior cingulate, and piriform cortices, the shell of the NAcc,the lateral geniculate nucleus, the medial terminal nucleus, and the superior colliculi.77
2.2.4.2. OTHER DRUGS
The effects of cocaine self-administration on basal brain function have been shown toevolve with the duration of exposure to the drug in both rodents78 and primates.79 In bothrats and rhesus monkeys, the initial stages of self-administration (5 days) are associatedwith focal LCGU decreases in the NAcc, whereas longer periods of self-administration (30or 100 days) result in more widespread metabolic decreases, involving dorsal as well asventral striatum. These findings are consistent with an increased behavioral impact on senso-rimotor and cognitive domains with increased drug exposure, in addition to the motivationalbehaviors associated with the ventral striatum.79
Consistent effects of withdrawal following cocaine self-administration on basal brainfunction have also been observed in several studies. Both 2-DG80 and rCBV-phMRI81
studies of withdrawal following cocaine self-administration observed widespread reduc-tions in basal LCGU and rCBV, respectively, with these decreases becoming morepronounced over 6e72 h withdrawal80 and persisting to 10 days.81 Moreover, LCGU valuesin many brain regions negatively correlated with the amount of cocaine consumed in thelast binge.80
Effects of cocaine self-administration and withdrawal on pharmacologically evokedphMRI responses are divergent. Both a blunted dopaminergic functional response in thecaudate putamen after 10 days withdrawal (as measured using the evoked response tod-amphetamine challenge)81 and a potentiated response to cocaine challenge administeredafter 28 days withdrawal82 have been reported. These differences may reflect the differentpharmacological challenge (reinstatement) or the differing time of withdrawal, but remainto be elucidated. In contrast, the BOLD phMRI responses to acute heroin challenge havebeen found to be attenuated after both 24 h59 and 10e12 days57 withdrawal following heroinself-administration.
2.2.5. Dopamine Release and Conditioned Place Preference
Preclinical PETexperiments allow brainmetabolism (e.g. using 18F-FDG) or dopamine flux(e.g. using 11C-raclopride) to be mapped in situ in direct analogues to human PET studies.Methods to determine the temporal profile of neurotransmitter release have also been devel-oped83 and shown to detect alcohol-induced dopamine release in the rat striatum, a findingconsistent with clinical observations.84

2.0. PRECLINICAL 319
Moreover, PETexperiments can also be designed in which tracer uptake is accumulated inthe awake, behaving state can be subsequently read out in vivo while the animal is anesthe-tized in the scanner.85 This opens the way to combining imaging interrogations of metabo-lism85 or dopamine flux86 with a behavioral episode. In this way, the effect of cocaineversus saline conditioned place preference on striatal dopamine release was elucidatedusing 11C-raclopride PET when rats were subsequently placed in each of the pairedchambers.87 This revealed decreased raclopride bindingdreflecting environmental cue-induced increases in dopamine releasedin the ventral striatum in the cocaine-paired versusthe saline-paired chamber. Moreover, the degree of binding strongly correlated acrossanimals with their behavioral preference score.
2.3. Summary of Preclinical Models and Imaging
Animal models offer the possibility of well-controlled experimental constructs bywhich cardinal processes underlying substance abusedacquisition of dependence,craving, withdrawal, and relapsedcan be dissected. A key finding that has emergedfrom the functional imaging data over a range of drugs of abuse is a core involvementof the mesolimbic dopamine reward system, including the medial prefrontal cortex,NAcc, and VTA. Strong evidence now implicates this system in all aspects of preclinicalmodels of drug dependence, from acute drug response to the effects of chronic exposure,withdrawal, and cueedrug associations. The ability to image ventral striatal function andits modulation provides a potentially powerful translational tooldPET-based methodo-logies to measure dopamine flux are more convergent across species than functionalmeasures, which have used different paradigms in rodents than are typically employedin humans (see Section 3.0).
Imaging studies have also revealed some limitations to the extent that preclinicalmodels mimic the physiological changes observed in the human disorder (e.g. divergentbrain neurochemical and structural profiles in alcohol dependence) as well as functionalvariability between models with very similar behavioral phenotypes. The dose-dependencyof functional effects observed in imaging studies generally matches the behavioralprofiles, both illuminating the neural substrates underlying these different behaviors(e.g. self-administration versus locomotor activity or stereotypy) and underscoring theimportance of looking for treatment effects at a relevant dose.
The initial application of preclinical imaging in the context of drug discovery mostlyfocused on acute challenge models as mechanistic tools to probe the modulatory effectsof potential treatments. This approach has delivered important mechanistic insights intothe mechanism of action of developmental therapeuticsdfor example, the potentiation ofdopamine-driven response in the NAcc by DA D3 receptor antagonists, a finding thatdovetails with the blunted dopamine response observed in the ventral striatum of humanaddicts (see Section 3.0). However, increasing emphasis has been placed on using imagingto further our understanding of the neurobiological underpinnings of the cardinal aspectsof drug addiction as embodied in behavioral models, especially the effects of drug self-administration, withdrawal, and reinstatement, and the effects of potential treatmentsthereon. From a translational perspective, it is important to match the preclinical experimentto the techniques likely to be most tractable in human studies. The increasing availability of

11. TRANSLATIONAL NEUROIMAGING320
imaging techniques (or surrogates88) that enable studies in conscious, behaving animalsprovides substantial promise in this regard.
3.0. CLINICAL-EXPERIMENTAL MEDICINE MODELSAND DRUG STUDIES
3.1. Human Experimental Models Available for Substance Abuse
3.1.1. Pharmacological Models
Various experimentalmodelshavebeenestablished toaddress thephenotypic characteristicsof substance abuse disorders in humans. Generally, experiments have a goal of characterizingthe pharmacological or behavioral effect of a particular substance with or without coadminis-tration of a potential therapeutic drug. Current human experimental models for substanceabuse disorders lack a true pharmacological model per se (i.e. a compound that when adminis-tered produces symptoms analogous to the disorder being studied), as the self-administrationof a specific substance despite its consequences is a cardinal feature of the disease process.
3.1.1.1. HUMAN LABORATORY MODELS
Human laboratory models of self-administration have been implemented for many drugsof abuse.reviewed in 89 For ethical reasons, the population for such studies is almost alwaysdrawn from current users of the drug who are not seeking treatment, thus limiting the abilityto generalize to those who are. Self-administration directly models drug-taking behavior andtherefore has strong face validity. Alcohol studies may employ a free-access paradigm withminimal response requirement (e.g. a simple button push). These experiments, however, maynot be specific to wanting (i.e. craving), and may be better correlated with drug liking.90 Thoseexperiments that seek to translate animal models of motivated behavior typically employoperant responding paradigms with a fixed or progressive ratio, and possibly a choicebetween the drug and an alternative reinforcer (e.g. money). These assays require eitherconstant or increasing response requirements for successive drug exposures. In the case ofprogressive ratio paradigms where the subject must work harder to obtain the drug overthe course of the experiment, the work is hypothesized to represent motivation or wantingthe drug, and is thought to better represent the extent to which a subject will go to obtaina drug.90 These methodologies provide perspective on some behavioral properties ofa drug while sacrificing a constant exposure. The frequency of drug availability is modeledon the administration habits and target drug exposure levels for the particular drugdforexample, cocaine self-administration typically employs a binge model,91 whereas theschedule of smoking marijuana would be controlled differently.92
The use of the ideal clinical population, those meeting diagnostic criteria for a substanceabuse disorder, is complex from an experimental point of view. By definition, substance-dependent individuals have suffered ongoing consequences from the drug which likelyinclude the following:
(1) Significant time spent using or recovering from the drug, which potentially limits theiravailability and interest in experiments that occur on a fixed schedule;

3.0. CLINICAL-EXPERIMENTAL MEDICINE MODELS AND DRUG STUDIES 321
(2) Social or legal consequences that may impair travel to/from appointments andwillingness of others to facilitate their participation;
(3) Physiological tolerance or dependence, which may preclude drug administration at aneffective dosage or prevent compliance with short periods of abstinence;
(4) Medical illness ranging from infectious disease, malnutrition or organ failure, which maydrastically alter or eliminate safety margins during exposure.
Any of these complications or their combination may preclude an individual from anexperiment, and as a group may limit their utility as a population of interest. Furthermore,many individuals with a substance abuse disorder suffer from a coexisting psychiatric diag-nosis, i.e. a pathological anxiety or affective condition, which also limits their role in manyinvestigational paradigms.93 For ethical reasons, humanmodels of relapse, in which the para-digm would require administration of an abused drug to a recovered patient, are notpossible; such experimental designs can only be modeled in animals.
The effects of potential therapeutics on self-administration in the laboratory setting maybe more predictive of clinical efficacy than effects on ancillary subjective responses, such ascraving. In the case of cocaine, several putative treatments have elicited changes in subjec-tive effects but not on self-administration per se, consistent with the fact that no treatment(out of more than 60) tested in clinical trials has proven efficacious at treating cocainedependence.89
Behavioral pharmacology models have also been developed for smoking in which admin-istration is controlled (e.g. by specified schedules of cigarette puffs) and exposure to nicotineand toxins and effects on other physiological variables can be studied in a controlledsetting.94 However, these models have been primarily employed to study the effects of ciga-rette replacements (e.g. electronic cigarettes) on exposure to nicotine and toxicants rather thanthe mechanisms underlying nicotine dependence.
3.1.1.2. ALCOHOL CHALLENGE PARADIGMS
Generally, alcohol challenge paradigms take two formsdexperimentally controlledexposures versus subject-determined or self-administration. Experimentally controlledexposures aim to reduce the variability in breath, blood, or brain alcohol concentration acrosssubjectsda design, if adequately performed, that enables a direct comparison of the depen-dent variables of interest. Classically, this is accomplished by oral self-administration withtarget alcohol concentrations calculated based upon body weight or total body water.95e100
Alternatively, intravenous alcohol administration has been used to avoid the significantvariability in pharmacokinetic profiles achieved through oral dosing,101,102 although thisroute of administration is more artificial and may not capture key sensory and behavioralattributes intrinsic to the disorder.101,103e111
Alcohol self-administration paradigms have two general areas of potential utility: pheno-typing traits that define the disorder112e114 and pharmaceutical evaluation and/or develop-ment of new addiction treatments.115e122 Most human alcohol self-administrationexperiments have employed a free-access design, but investigators have also begun toexamine the properties of progressive-work designs.121,123e126 While the majority of theseexperiments have relied upon oral alcohol administration, the use of intravenous deliveryhas now also expanded into self-administration.114,127

11. TRANSLATIONAL NEUROIMAGING322
3.1.1.3. MODELS BASED ON BEHAVIORAL PHENOTYPE
Various strategies of population selection have been adopted for the study of alcohol abuseand dependence, ranging from alcohol-dependent individuals per se128e131 to more specificpopulations based upon their overall level or pattern of alcohol consumption, e.g. heavy,moderate, or binge social drinkers.97,98,117,132e135 Alternatively, subjects may be characterizedbased upon other risk factors, including subjective response to alcohol, specifically, behavior-ally high versus low alcohol responders,136e139 with low responses to the aversive effects ofalcohol being the risk factor for alcohol dependence. In a similar way, studies of nicotinedependence select or stratify subjects based on smoking history and current use.
3.1.1.4. GENETIC AND FAMILY HISTORY MODELS
Investigations of the effects of familial risk and specific genetic variation provide a comple-ment to population selection based on a behavioral phenotype.iv
In the case of alcohol, for example, some investigators have examined subjects based upontheir familial history of alcoholism.103,105,106,114,139e141 This mechanism, most directly compa-rable to the selectively bred alcohol-preferring rats in the animal literature (see Section 2.0),assumes that the underlying difference between the groups is attributable to currentlyunknowndand possibly heterogeneousdgenetic influences. Unfortunately, in the humansubject it is difficult, if not impossible, to isolate the impact of environmental learning andmodeling; a factor that can be partially addressed by twin studies.142e145
Other studies have focused on identified genetic factors to predict response to a parti-cular intervention based on a specific polymorphism. More specifically, investigators haveexamined variance associated with genes encoding the m-type opioid receptor(OPRM1),146e149 the a2 subunit of the GABA receptor (GABRA2),110,134,144,150 and alcoholdehydrogenase.104,151,152 Taken together, human alcohol challenges have begun to explorea wide range of possibilities through careful selection of study population and experi-mental design. However, as any one genetic polymorphism (or gene) is unlikely to accountfor significant variance in explaining the development of alcoholism, this approach can beuseful for studying particular disease pathways.
3.2. Imaging Applied to Experimental Models, Disease State,and Pharmacotherapy in Humans
3.2.1. Effects of Chronic Drug Exposure on Brain Structure and Neurochemistry
3.2.1.1. ALCOHOL
A large number of studies have elucidated the effects of chronic alcohol exposure on thestructure and neurochemistry of the human brain.reviewed in 153 Computed tomography (CT)studies from the 1970s through to more recent MR morphometry studies have shown thatexcessive alcohol intake leads to widespread reductions in brain volumedboth gray andwhite matter, and particularly in the frontal lobesdthat can nevertheless be partially
ivFor further discussion on structural neuroimaging phenotypes and behavioral disorders with a genetic basis,
see Tost et al. in Chapter 6, Rethinking the Contribution of Neuroimaging to Translation in Schizophrenia,
in this volume.

3.0. CLINICAL-EXPERIMENTAL MEDICINE MODELS AND DRUG STUDIES 323
reversed following sustained abstinence.154e160 Diffusion imaging studies have alsorevealed disruptions in white matter microstructure owing to chronic alcohol exposure.161,162
MRS studies have revealed similar findings with respect to brain metabolites such asN-acetylaspartate (NAA), Cho, and GABA; namely, reduced levels in alcohol-dependentsubjects that can be reversed upon abstinence.153
3.2.1.2. NICOTINE
Chronic nicotine exposure through smoking has also been shown to lead to measur-able effects on brain structure and function.reviewed in 163 Structural MRI studies haverevealed decreased gray matter volume in smokers compared with nonsmokers, althoughthere is some heterogeneity across studies in the regions affected. Atrophy in thetemporal lobes is one of the more consistent findings, and is supported by a studycomparing effects of alcohol and smoking on brain structure, in which smoking heavydrinkers evidenced increased temporal lobe atrophy relative to nonsmoking heavydrinkers;164 effects of both smoking and alcohol on brain atrophy were greater than thosedue to alcohol alone. Similarly, MRS studies revealed combined effects of both smokingand alcohol that are worse than either drug alone, especially in terms of reduced NAAand Cho in the frontal lobes and cerebellum;163 effects of smoking, independent ofalcohol consumption, include reduced NAA and Cho in the midbrain and an inversecorrelation between NAA in the thalamus and cigarette consumption.165 Reduced NAAhas also been reported in the hippocampus of smokers.166
3.2.2. Imaging Direct Pharmacological Effects on Neurochemistry
3.2.2.1. ACUTE DRUG EFFECTS ON DOPAMINE FLUX
There is convergent evidence across many abused substances, including alcohol, amphet-amine, cocaine, cannabis, andnicotine, that acute administration leads to increasedDA releasein the midbrain and ventral striatumdkey nodes in the mesolimbic reward system.84,167e170
Moreover, the rewarding effects and hence abuse potential of these substances havebeen hypothesized to be positively correlated with rapid striatal DA efflux.10 With chronicdrug taking, however, neuroadaptations occur; for instance, blunted DA responses areobserved in addicts compared with healthy controls,171 suggesting compensatory mecha-nisms that may relate to dependence and withdrawal symptoms. However, above andbeyond any direct pharmacological effects, many consider midbrain and ventral striatal DAtransmission to have substantial cognitive and psychological components, such as thoserelating to drug wanting172 or expectations about impending drug delivery.173
3.2.2.2. EFFECTS OF CHRONIC DRUG EXPOSURE ON DOPAMINE NEUROTRANSMISSION
A number of PET and single-photon emission computed tomography (or SPECT) studieshave demonstrated the key role of impaired striatal dopamine neurotransmission in drugdependence and behavioral responses to abused substances.174 In addicts, reduced dopa-mine tone has been measured in both alcoholics175 and cocaine users,176 and increased stria-tal D2 and D3 receptor availability has been observed in nicotine-dependent subjects.177
These changes do not normalize quickly in abstinence.177,178 In contrast, drug-inducedchanges in dopamine transporter (DAT) density and speed of normalization upon abstinence

11. TRANSLATIONAL NEUROIMAGING324
are more variable across drugs of abuse, and hence less likely to be related to a commonmechanistic relationship to addiction.v,179
Other factors may mediate the effects on dopamine receptor binding in the striatum, suchas gender,96 cognitive state,180 or genetic factors underlying the biology of addiction.For example, an OPRM1 polymorphism was strongly associated with striatal dopaminerelease in response to alcohol in both social drinkers and humanized mouse lines.146
3.2.3. Imaging Direct Pharmacological Effects on Resting Brain Function
3.2.3.1. ALCOHOL
Pharmacological imaging paradigms to detect a direct compound effect on some measureof basal brain activity (e.g. metabolism, perfusion, or BOLD signal) provide a potential trans-lational model to examine the functional substrates of abused drugs and modulatory effectsof putative treatments for drug dependence. Studies have elucidated the effects of a pharma-cokinetically controlled exposure of alcohol (intravenously clamped at 0.6 g/L) on restingbrain perfusion,181 BOLD functional connectivity,182 and neurochemistry111 in socialdrinkers. At steady state exposure, alcohol increased central perfusion in the precentralgyrus, occipital pole, bilateral hippocampus, and posterior cingulate cortex181 and alteredconnectivity between the posterior cingulate cortex and sensorimotor network.182 TheMRS study revealed alcohol-induced reductions in both GABA and NAA in the occipitalcortex, suggesting acute modulation of GABAergic neurotransmission and accompanyingeffects on neuronal viability.111
3.2.3.2. NICOTINE
An early phMRI study examined BOLD response to intravenous nicotine, observing dose-dependent (0.75, 1.50, and 2.25mg/70 kg) BOLD increases in the ventral striatum, anteriorcingulate, amygdala, and prefrontal cortex of active smokers;183 a similar set of brain regionswas identified as underlying the response to other abused substances. Dose-dependentincreases in subjective parameters including rush, high, and drug liking were also observed,and correlated strongly with the rapid time course of the BOLD signal changes.
3.2.3.3. OTHER DRUGS
Several human phMRI studies have examined the direct effects of cocaine infusion onBOLD contrast in habitual cocaine users. In one of the earliest studies, a double-blind cross-over experimental design was used to determine the effects of an intravenous cocaine bolusin comparison to saline.184 The high temporal resolution of fMRI allowed the temporalsequence of brain activity to be correlated with changes in subjective ratings followingcocaine infusion; brain regions with early but transient BOLD responses correlated withsubjectively rated feelings of rush, whereas more sustained responses in the ventral striatum(positive BOLD signal changes) and amygdala (negative BOLD signal changes) correlatedwith craving.184 However, later nonblinded phMRI studies of acute cocaine challenge also
vSee also Nutt and Nestor in Chapter 10, Neuroimaging as a Biomarker for the Diagnosis, Progression, and
Treatment of Substance Abuse Disorders, in this volume for further discussion of common mechanisms
of addictive behaviors.

3.0. CLINICAL-EXPERIMENTAL MEDICINE MODELS AND DRUG STUDIES 325
observed a mixture of positive and negative BOLD responses in a largely congruent set ofbrain structures, but with negative rather than positive BOLD signal changes in the ventralstriatum185,186da finding that was postulated,185 but found not,186 to be due to expectationon the part of the participants. The reason for the differential valence in the ventral striatalBOLD responses thus remains to be explained, although it could be a result of the differentdoses (0.6 mg/kg versus 0.29mg/kg) employed in the two studies.
A BOLD phMRI study of a single acute dose of intravenous morphine in healthy volun-teers revealed a mixture of responses comprising a pattern of signal increases in rewardcircuitry similar to other abused drugs and a pattern of cortical decreases analogous toother sedative drugs.187 Interestingly, the valence of these responses is opposite to thatobserved in response to heroin infusion in the rat (see Section 2.0). The effects of pharma-cokinetically controlled steady state (80 nmol/L) morphine on resting perfusion181 andfunctional connectivity182 have also been evaluated, showing increased perfusion in theanterior cingulate and insular cortices and the cerebellum and extensive alterations in func-tional connectivity.
3.2.4. Functional Responses to Alcohol-Related Olfactory and Gustatory Cues
Experimental designs have been developed to dissociate systemic alcohol exposure fromthe gustatory and olfactory cues associated with the drinking experience. The direct brainresponses to gustatory or olfactory alcohol stimuli per se can be elucidated by means of para-digms in which subjects are exposed to tastes or odors during an fMRI scanning session. Bothgustatory188 and olfactory189 alcohol cues have been shown to directly increase the BOLDresponse in the mesocorticolimbic system in comparison to appetitive control stimuli inheavy drinkers. The response to olfactory alcohol-related cues was also found to be potenti-ated in this population by a 50mg% BAL achieved using an intravenous clamp,127,190 andinversely correlated with antisocial trait density.191
In a human implementation of a conditioned stimulus (CS) paradigm, visual non-alcohol-related cues were subliminally related to presence (þ) or absence (�) of intravenouslyclamped alcoholdand hence the subjective effects of intoxicationdand then tested usingfMRI in the absence (but purported possibility) of intravenous alcohol the following day.This experiment revealed a negative BOLD response to CSþ stimuli in the medial prefrontalcortex (mPFC), reflecting negative prediction error.192
3.2.4.1. GENETIC EFFECTS
The olfactory cue paradigm has also demonstrated measurable functional effects of familyhistory of alcoholismdthe strongest risk factor for development of alcohol dependencedonreward processing in relation to alcohol cues. It was found that the presence of intravenouslyinfused and clamped 50mg% alcohol had differential effects on the mPFC response to olfac-tory alcohol cues dependent on the familial history of heavy drinkers;193 under placebo infu-sion, a significant response to olfactory alcohol (versus comparator odors) was present infamily-history-positive, but not family-history-negative subjects. In contrast, the presenceof intravenous alcohol reversed this pattern, with the mPFC response attenuated infamily-history-positive but enhanced in family-history-negative subjects.
Specific genetic variants have also been associated with differential functional brainresponses to alcohol cues. Homozygotes for the putative risk (A) allele of the rs279871

11. TRANSLATIONAL NEUROIMAGING326
SNP in the GABRA2 gene evidenced increased BOLD responses to olfactory alcohol cues inthe mPFC, but decreased responses in the VTA.134 C carriers of the rs2023239 SNP on thecannabinoid receptor CB1-encoding gene CNR1 also evidenced an increased BOLD responseto gustatory alcohol cues in the mesolimbic system, including the VTA, ventral striatum, andventromedial/orbitofrontal cortices; this genotype-dependent effect that was paralleled byan increased subjective reward and positive affect after drinking.194 These fMRI responseswere also correlated with urge to consume and alcohol use ratings in the C allele carriers.A copy-number variation at 22q13.1 was identified as being associated with alcohol depen-dence and functional brain responses to gustatory cues; specifically, the response in the pre-cuneus was determined to mediate the association between a 22-kilobase pair homozygousdeletion at this locus and severity of alcohol dependence.195
3.2.5. Modulation of Functional Responses to Task-Based fMRI Paradigms
The vast majority of imaging studies of substance abuse in humans have attempted toelucidate neural mechanisms underlying aspects of the disorder using more conventionaltask-based fMRI paradigms.vi
One common approach has been to use visual representations of drug-related cues, moti-vated by the fact that drug taking, and relapse to drug taking after a period of abstinence, isoften triggered by the presence of visual or other cues associated with the drug. fMRI studiesof visual cue reactivity have elucidated neural substrates of cue-induced brain function inaddicts relative to controls and functional correlates of associated behaviors (e.g. craving,drug taking, or relapse). Convergent evidence across a number of studies has identifiedcommon substrates of significant BOLD response to drug-related cues across a wide varietyof abused substances.196,197 These notably include the ventral striatum, a key node of themesolimbic reward system that is activated by drug-related cues in a variety of populations.
The reward system has also been widely studied using paradigms not overtly drug-related (e.g. the monetary incentive delay task).198,199 The emotional/stress axis has beenprobed using affectivedusually visualdcues [e.g. images of different emotional valence,such as the international affective picture series (IAPS),200,201 or implicit facial affect para-digms,202] and other studies have examined impulsivity.203 fMRI studies of nicotine in partic-ular have also examined higher cognitive processes due to the interest in the nicotinic systemon cognition per se.201 Modulation of the central responses to such paradigms by a number ofexperimental conditions can be investigateddfor example, dependent versus comparatorpopulations, genotype, genetic risk, behavioral risk, or exposure to the abused drug duringthe experiment.
For alcohol in particular, a range of populations have been studied; often, social drinkersrather than teetotalers are used as a control arm to compare with alcoholics, whereas otherstudies have examined heavy drinkers or nondependent individuals with a family associa-tion with alcoholism, or different genetic groups of a similar drinking profile. Moreover,experiments using a controlled alcohol exposure (sufficient to elicit subjective effects) have
viPlease refer to Nutt and Nestor in Chapter 10, Neuroimaging as a Biomarker for the Diagnosis, Progression,
and Treatment of Substance Abuse Disorders, in this volume for further discussions on neuroimaging of
human addiction, including substance abuse.

3.0. CLINICAL-EXPERIMENTAL MEDICINE MODELS AND DRUG STUDIES 327
been combined with task-based functional imaging readouts,137,203,204 analogous to thegustatory or olfactory cue designs discussed above.
There is a burgeoning literature on genetic modulation of task-based fMRI responses. Forexample, variants encoding D2 and D4 DA receptors (DRD2 and DRD4) and the GABAreceptor subunit a2 (GABRA2) have been associated with differential brain activityrelated to impulsiveness in subjects with alcohol abuse disorders and familial risk of alco-holism;205,206 and genetic variants associated with the a4 and a5 subunits of the nAChR,CHRNA4, and CHRNA5, have been reported to modulate brain activity in response to atten-tion and smoking cues.207,208 Such studies have taken as their point of departure genes that arebiologically associated with the substance and its action on the brain, or those behaviorally orclinically associated with dependence. Replication and convergence of the dependence ofbrain functional responses on specific genetic variants will be of great value in understandingpredisposition to substance abuse and offer potential avenues for tailored therapies.
3.2.6. Functional Imaging Studies of Pharmacotherapy
For application to drug development, an imaging method must be sensitive to pharmaco-logical manipulation and sufficiently well characterized and reproducible that the outcomecan be interpreted with confidence. An important aspect of this characterization is the avail-ability of data with comparator drugs that can demonstrate pharmacological sensitivity andallow benchmarking of new compounds.
3.2.6.1. ALCOHOL
A number of studies have demonstrated the sensitivity of fMRI paradigms to pharmaco-logical modulation. In particular, several studies demonstrated pharmacological reversal ofexaggerated BOLD fMRI responses to visual alcohol cues in alcoholic subjects. In a study ofabstinent alcoholics, a single acute 400mg dose of the D2/D3 antagonist amisulpride normal-ized predosing differences between the alcoholic group and controls, although subjectivecraving was not reduced.209Another study examined the combination of 50mg dailydoses of the opioid antagonist naltrexone (Revia) and twice-daily 0.25mg doses of the5-hydroxytryptamine 3A (5-HT3A) receptor antagonist ondansetron (Zofran) over 7 days innontreatment-seeking alcoholics; both drugs reduced the visual cue-induced activation inthe ventral striatum but the combination reduced the response more than either drugalone.210 In that study, subjective craving was also reduced by the pharmacological treat-ment. This finding with naltrexone is consistent with its effects on the drinking patterns ofalcoholics in a clinical laboratory setting.129 In a separate study from the same group, aripi-prazole (Abilify; a partial dopaminergic agonist, acting on both postsynaptic D2 receptorsand presynaptic autoreceptors, as well as acting as a partial agonist at 5-HT1A receptorsand an antagonist at 5-HT2A receptors) was dosed up to 15mg over 14 days.211 The cue-induced response in the ventral striatum was attenuated in subjects dosed with aripiprazolecompared with placebo; moreover, the ventral striatal response in the aripiprazole groupcorrelated with the number of heavy drinking days, thus reinforcing the relationshipbetween this functional brain response and behavior. These findings are convergentwith clinical laboratory studies of aripiprazole showing reduced euphoric and stimulatingeffects of alcohol as well as alcohol consumption.212,213 Both of these last two imagingstudies210,211employed a priming sip of alcohol before the visual cue paradigm.

11. TRANSLATIONAL NEUROIMAGING328
Novel compounds in development have also begun to be assessed using imaging tech-niques. The neurokinin-1 (NK-1) receptor antagonist LY686017 (3weeks of daily 50mgdosing) was tested in high trait anxiety alcoholic inpatients using a visual fMRI paradigmcomprising positive and negative emotional valence visual cues (IAPS).200 Compared toplacebo, treatment with LY686017 biased the BOLD responses to the emotional stimulitoward a positive effectdresponses to negative emotional stimuli were blunted in the infe-rior frontal gyrus and responses to positive emotional stimuli were augmented in the ventralstriatum. These observations are consistent with both the theoretical action of this compoundand a body of experimental data in both rodent and human models on its effect on anxietyand stress responses.200
3.2.6.2. NICOTINE
A series of studies examined the effect of the a4b2 nicotinic acetylcholine receptor partialagonist varenicline, which is approved in the USA for smoking cessation (Chantix), ondifferent axes of brain function in smokers. In a perfusion fMRI study of central reactivityto smoking cues in nontreatment-seeking smokers, 3 weeks treatment with varenicline(titrated to a dose of 1mg twice daily), in comparison to placebo, resulted in strong reversalof the positive response in the medial orbitofrontal cortex and a suppression of the responsein the ventral striatum.214 A separate study examined the effect on workingmemory functionand brain activation in smokers under short-term abstinence. Subjects underwent a 2-weektreatment with varenicline (titrated to a dose of 1mg twice daily) or placebo and remainedabstinent from smoking for the last 3 days. Subjects in the varenicline group showedincreased BOLD responses, especially to the more difficult (3-back) condition, than thoseon placebo in medial and lateral prefrontal regions activated by the working memorytask.215 Moreover, subjects with high dependence ratings had significantly reduced correctresponse times. A third study examined the modulatory effect of varenicline on affectivestimuli provided by a facial emotion-matching task. Here, a 2-week treatment with vareni-cline (titrated to a dose of 1mg twice daily) resulted in altered BOLD responses in the medialprefrontal cortex, middle temporal gyrus, occipital cortex, and thalamus, with attenuation ofthe response in the amygdala revealed in a region-of-interest (ROI)-level analysis.202
3.3. Summary
Since clinical studies of substance abuse invariably involve a population of drug users,most work has involved (implicitly or explicitly) a characterization of the disease state per se.Imaging studies have revealed that chronic exposure to both alcohol and nicotine leads toreduced gray matter volumes and neurochemical abnormalitiesdincluding reduced levelsof the neuronal viability marker, NAAdin drug users relative to controls. Moreover, thecombined effects of these two drugs are greater than the effects of either substance alone.
FMRI studies have revealed strong convergent evidence of the involvement of the meso-limbic reward system. A consistent finding across many abused substances is that visualdrug-related cues evoke increased functional responses in addicts, relative to controls, inkey brain regions including the ventral striatum andmedial orbitofrontal/prefrontal cortices.Likewise, olfactory and gustatory alcohol cues activate similar brain regions in alcoholics,responses that are potentiated in the presence of significant blood alcohol exposure. Studies

4.0. TRANSLATIONAL IMAGING OF SUBSTANCE ABUSE MODELS 329
of the direct pharmacological effects of abused substances (e.g. phMRI) have been less widelyemployed in humans than in animals. PhMRI studies of cocaine and nicotine have revealedeffects of intravenous drug challenge in the ventral striatum among other brain regions;many of these responses correlated with subjective responses to the drug. However, thevalence of the ventral striatal BOLD response to cocaine was inconsistent across studiesand this observation remains to be fully elucidated.
PET studies have also revealed consistent, rapid increases in dopamine flux in the ventralstriatum following administration of many abused substances. This fast temporal pharmaco-dynamic effect has been linked to the subjective rewarding effects of the drug and henceabuse potential. However, chronic drug exposure in addicted individuals has been consis-tently associated with attenuated dopamine release (relative to controls) in the ventral stria-tum in response to a dopaminergic stimulus. These two common features of abusedsubstances have underscored the central importance of the mesolimbic dopamine systemin addictive disorders.
The relationship of functional differences to specific subpopulations, genotypes, and riskfactors has also begun to be elucidated and holds promise for addressing more specifichypotheses in the clinical laboratory setting. Genotype-specific effects offer potential imaginggenetics models, but data on replication and convergence (or not) of the functional effectsrelating to addiction216 will be of great value in confirming the relationships between alteredreceptor biology and functional roles underlying the clinical manifestations.
A number of task-based fMRI studies have demonstrated effects of actual and potentialtherapeutics for drug dependence on particular axes of brain function, in particular, butnot limited to, the response to visual cues associated with the drug. While these provide clearpharmacodynamic evidence for compound effects on particular brain circuits relevant tobehaviors underlying drug taking and relapse, they represent tests of biological hypothesesof central drug action rather than predictors of clinical efficacy. Indeed, the fMRI studies ofvarenicline were all performed after US Food and Drug Administration approval for thetreatment of smoking cessation in order to understand how the agent is acting, rather thanduring drug development in order to predict its efficacy ahead of pivotal clinical trials.The extent to which such imaging models can be used to predict clinical response remainsto be demonstrated. Effective translation of effects observed in imaging studies to clinicalefficacy may be increased by identifying the target patient population that shows effects inimaging studies, thereby matching the biological action of the compound.
4.0. TRANSLATIONAL IMAGING OF SUBSTANCE ABUSE MODELSFOR DRUG DISCOVERY AND DEVELOPMENT
4.1. Drug Discovery
In drug development, molecules are typically identified as candidate therapeutics basedon a package of chemical and biological optimization involving preclinical species. Thesearch for novel compounds is usually driven by target validationda biological rationalelinking the molecular target or perturbed system (or both) to the clinical pathology. In thiscontext, there are several potential roles for imaging related to substance abuse. First, from

11. TRANSLATIONAL NEUROIMAGING330
a disease-understanding perspective, imaging studies can reveal or confirm neurobiologicalmechanisms related to addiction and link brain regions, circuits, or neurotransmitter abnor-malities to behavior and the pathological processes underlying substance abuse. Thesestudies may be in animal models, experimental medicine models, or clinical populations.Second, pharmacodynamic, physiological or functional imaging methods can be directlyapplied in preclinical drug discovery to determine the extent to which biological parametersin the preclinical model match those in the humanmodels and/or in the disease state in orderto develop an understanding about a particular mechanism of action and to assess the effectof putative candidate therapeutics on the imaging readout.
4.2. Clinical Development
Once a candidate molecule is committed to initial testing in humans, the emphasis tends toshift to the development of that particular compound and to answering key questions rele-vant to its immediate development. Across psychiatric disorders, the most establishedimaging approach is to employ PET scanning to profile how an appropriate radiotracer (ifavailable) is displaced by the drug candidate in vivo. This can confirm brain penetrationand target engagement, and inform dose selection for subsequent trials.217,218 Physiologicalor functional imaging methodsdsuch as those discussed in this chapterdcan also be appliedin early-phase clinical trials to interrogate the biological effects of developmental compoundson the CNS and potentially inform dose selection. Rather than reflecting target engagementat the molecular level, such methods can probe pharmacological effects on relevant physi-ology or brain functiondeither pharmacodynamically as proof of mechanism or by modifica-tion of an abnormal parameter related to the disease state. In order to obtain reliableinformation about the compound at hand, the imaging assay itself needs to have stable acqui-sition and analysis parameters and be well characterized in terms of its stability, reproduc-ibility, and sensitivity to relevant pharmacological effects. A sound understanding of thevariability of the responses of interest, and hence appropriate powering of the study, iscritical.219
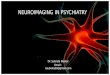
Figure 11.2 illustrates schematically the relationship between imaging studies and thedrug development process. Studies in humans can inform preclinical models and diseaseunderstanding as well as yielding potential imaging biomarkers for application in clinicaldrug development. The bulk of the published literature on imaging methods applied tosubstance abuse could be considered as comprising studies that inform our understandingof the disease state and potential treatments. However, an increasing number of pharmaco-logical interventions are being assessed using imaging methodsdin particular fMRIdthusbuilding confidence that fMRI studies of novel compounds could be used to confirm hypoth-eses regarding the central effects of a particular compound and inform the selection of anappropriate dose for (and possibly design of) proof-of-concept or efficacy trials. The para-digm and clinical population should match the hypothesized action of the compound, asexemplified in the aforementioned study using the NK-1 antagonist in which an emotionalstressor was used as the fMRI probe in a population enriched for anxiety. While a positiveresult in an imaging study can inform subsequent development and increase confidence inthe compound for substance abuse indications, caution should be exercised regardingpredictability of clinical efficacy from a pharmacodynamic endpoint.

FIGURE 11.2 Imaging within a typical drug discovery and development paradigm involves the characteriza-tion and application (to compound selection, optimization and understanding) of imaging measures in animalmodels, followed by the possible use of well-characterized imaging biomarkers to assess physiological effects of thedrug candidate in clinical development.
4.0. TRANSLATIONAL IMAGING OF SUBSTANCE ABUSE MODELS 331
4.3. Translation
While in vivo imaging provides many opportunities for translation between preclinicaland clinical studies, it is important that the imaging techniques align. PET studies of dopa-minergic abnormalities in the striatum are an excellent example where the same techniquecan be applied to successfully measure the same physiological phenomenon in humansand behaving animals. For functional imaging, in contrast, most clinical studies haveemployed task-based paradigms, whereas immobilization and anesthesia constraints inanimals have led to pharmacological challenge paradigms becoming dominant. Theincreasing availability of techniques that allow functional imaging readouts (or analoguesthereof) in conscious, behaving animals, and the increasing use of phMRI paradigms inhumans both offer promising routes to narrow this gap. In general, imaging paradigms forwhich the effects beingmeasured are relatively robust to realistic variants in the experimental

11. TRANSLATIONAL NEUROIMAGING332
construct (e.g. small differences in challenge dose, anesthetic level, strain, or genetic back-ground) are of particular value.
Substance abuse and dependence reflect heterogeneous effects of genes and environment.Factors underlying this complex interaction are beginning to be disentangled using imaginggenetics approaches that offer much promise for the identification and validation of drugtargets, especially when combined in a translational context with imaging experiments intransgenic rodent models.
References
1. Nutt DJ, King LA, Phillips LD. Drug harms in the UK: a multicriteria decision analysis. Lancet2010;376(9752):1558e65.
2. Wittchen HU, Jacobi F, Rehm J, Gustavsson A, Svensson M, Jonsson B, et al. The size and burden ofmental disorders and other disorders of the brain in Europe 2010. Eur Neuropsychopharmacol
2011;21(9):655e79.3. Policy OoNDC. The economic costs of drug abuse in the United States, 1992e2002. Vol. Publication No. 207303.
Washington, D.C: Executive Office of the President; 2004.4. Rehm J, Mathers C, Popova S, Thavorncharoensap M, Teerawattananon Y, Patra J, et al. Global burden of
disease and injury and economic cost attributable to alcohol use and alcohol-use disorders. Lancet
2009;373(9682):2223e33.5. Degenhardt L, Hall W. Extent of illicit drug use and dependence, and their contribution to the global burden of
disease. Lancet 2012;379(9810):55e70.6. Nurnberger Jr JI, Wiegand R, Bucholz K, O’Connor S, Meyer ET, Reich T, et al. A family study of alcohol
dependence: coaggregation of multiple disorders in relatives of alcohol-dependent probands. Arch Gen
Psychiatry 2004;61(12):1246e56.7. Griffiths RR, Bigelow GE, Henningfield JE. Similarities in animal and human drug taking behavior. In:
Mello NK, editor. Advances in substance abuse. Greenwich, CT: JAI Press; 1980.8. Crabbe JC. Genetic contributions to addiction. Annu Rev Psychol 2002;53:435e62.9. Heidbreder CA, Newman AH. Current perspectives on selective dopamine D(3) receptor antagonists as
pharmacotherapeutics for addictions and related disorders. Ann N Y Acad Sci 2010;1187:4e34.10. Volkow ND, Fowler JS, Wang GJ, Swanson JM, Telang F. Dopamine in drug abuse and addiction: results of
imaging studies and treatment implications. Arch Neurol 2007;64(11):1575e9.11. Hasin DS, Stinson FS, Ogburn E, Grant BF. Prevalence, correlates, disability, and comorbidity of DSM-IV
alcohol abuse and dependence in the United States: results from the National Epidemiologic Survey onAlcohol and Related Conditions. Archives of General Psychiatry 2007;64(7):830e42.
12. Harwood H. Updating Estimates of the Economic Costs of Alcohol Abuse in the United States: Estimates,Update, Methods and Data. In: Report prepared by the Lewin Group for the National Institute on Alcohol Abuse andAlcoholism; 2000.
13. Yi H, Chen CM, Williams GD. Alcohol epidemiologic data system, in surveillance report. Bethseda, MD:National Institute on Alcohol Abuse and Alcoholism, Division of Epidemiology and Prevention Research;2006.
14. Eckardt MJ, Campbell GA, Marietta CA, Majchrowicz E, Weight FF. Acute ethanol administration selectivelyalters localized cerebral glucose metabolism. Brain Res 1988;444(1):53e8.
15. Grunwald F, Schrock H, Biersack HJ, Kuschinsky W. Changes in local cerebral glucose utilization in the awakerat during acute and chronic administration of ethanol. J Nucl Med 1993;34(5):793e8.
16. Williams-Hemby L, Porrino LJ. Low and moderate doses of ethanol produce distinct patterns of cerebralmetabolic changes in rats. Alcohol Clin Exp Res 1994;18(4):982e8.
17. Williams-Hemby L, Porrino LJ. I Functional consequences of intragastrically administered ethanol in rats asmeasured by the 2-[14C]deoxyglucose method. Alcohol Clin Exp Res 1997;21(9):1573e80.
18. Yoshimoto K, McBride WJ, Lumeng L, Li TK. Alcohol stimulates the release of dopamine and serotonin in thenucleus accumbens. Alcohol 1992;9(1):17e22.

REFERENCES 333
19. Jones N, O’Neill MJ, Tricklebank M, Libri V, Williams SC. Examining the neural targets of the AMPA receptorpotentiator LY404187 in the rat brain using pharmacological magnetic resonance imaging. Psychopharmacology
(Berl) 2005;180(4):743e51.20. Jones N, Messenger MJ, O’Neill MJ, Oldershaw A, Gilmour G, Simmons RM, et al. AMPA receptor potenti-
ation can prevent ethanol-induced intoxication. Neuropsychopharmacology 2008;33(7):1713e23.21. London ED, Connolly RJ, Szikszay M, Wamsley JK, Dam M. Effects of nicotine on local cerebral glucose
utilization in the rat. J Neurosci 1988;8(10):3920e8.22. London ED, Dam M, Fanelli RJ. Nicotine enhances cerebral glucose utilization in central components of the rat
visual system. Brain Res Bull 1988;20(3):381e5.23. Matta SG, Foster CA, Sharp BM. Nicotine stimulates the expression of cFos protein in the parvocellular par-
aventricular nucleus and brainstem catecholaminergic regions. Endocrinology 1993;132(5):2149e56.24. Ren T, Sagar SM. Induction of c-fos immunostaining in the rat brain after the systemic administration of
nicotine. Brain Res Bull 1992;29(5):589e97.25. Sharp BM, Beyer HS, McAllen KM, Hart D, Matta SG. Induction and Desensitization of the c-Fos mRNA
Response to Nicotine in Rat Brain. Mol Cell Neurosci 1993;4(2):199e208.26. Pang Y, Kiba H, Jayaraman A. Acute nicotine injections induce c-fos mostly in non-dopaminergic neurons of
the midbrain of the rat. Brain Res Mol 1993;20(1e2):162e70.27. Pontieri FE, Tanda G, Orzi F, Di Chiara G. Effects of nicotine on the nucleus accumbens and similarity to those
of addictive drugs. Nature 1996;382(6588):255e7.28. Choi JK, Mandeville JB, Chen YI, Kim YR, Jenkins BG. High resolution spatial mapping of nicotine action using
pharmacologic magnetic resonance imaging. Synapse 2006;60(2):152e7.29. Gozzi A, Schwarz A, Reese T, Bertani S, Crestan V, Bifone A. Region-specific effects of nicotine on brain
activity: a pharmacological MRI study in the drug-naive rat. Neuropsychopharmacology 2006;31(8):1690e703.30. Mathieu-Kia AM, Pages C, Besson MJ. Inducibility of c-Fos protein in visuo-motor system and limbic struc-
tures after acute and repeated administration of nicotine in the rat. Synapse 1998;29(4):343e54.31. Febo M, Segarra AC, Nair G, Schmidt K, Duong TQ, Ferris CF. The neural consequences of repeated cocaine
exposure revealed by functional MRI in awake rats. Neuropsychopharmacology 2005;30(5):936e43.32. Luo F, Wu G, Li Z, Li SJ. Characterization of effects of mean arterial blood pressure induced by cocaine and
cocaine methiodide on BOLD signals in rat brain. Magn Reson Med 2003;49(2):264e70.33. Marota JJ, Mandeville JB, Weisskoff RM, Moskowitz MA, Rosen BR, Kosofsky BE. Cocaine activation
discriminates dopaminergic projections by temporal response: an fMRI study in Rat. Neuroimage
2000;11(1):13e23.34. Schwarz AJ, Reese T, Gozzi A, Bifone A. Functional MRI using intravascular contrast agents: detrending of the
relative cerebrovascular (rCBV) time course. Magn Reson Imaging 2003;21(10):1191e200.35. Schwarz AJ, Zocchi A, Reese T, Gozzi A, Garzotti M, Varnier G, et al. Concurrent pharmacological MRI and in
situ microdialysis of cocaine reveal a complex relationship between the central hemodynamic response andlocal dopamine concentratio. Neuroimage 2004;23(1):296e304.
36. Chen YC, Galpern WR, Brownell AL, Matthews RT, Bogdanov M, Isacson O, et al. Detection of dopaminergicneurotransmitter activity using pharmacologic MRI: correlation with PET, microdialysis, and behavioral data.Magn Reson Med 1997;38(3):389e98.
37. Schwarz A, Gozzi A, Reese T, Bertani S, Crestan V, Hagan J, et al. elective dopamine D(3) receptor antagonistSB-277011-A potentiates phMRI response to acute amphetamine challenge in the rat brain. Synapse
2004;54(1):1e10.38. Schmidt KF, Febo M, Shen Q, Luo F, Sicard KM, Ferris CF, et al. Hemodynamic and metabolic changes induced
by cocaine in anesthetized rat observed with multimodal functional MRI. Psychopharmacology (Berl)
2006;185(4):479e86.39. Silva AC, Zhang W, Williams DS, Koretsky AP. Multi-slice MRI of rat brain perfusion during amphetamine
stimulation using arterial spin labeling. Magn Reson Med 1995;33(2):209e14.40. Lu H, Xi ZX, Gitajn L, Rea W, Yang Y, Stein EA. Cocaine-induced brain activation detected by
dynamic manganese-enhanced magnetic resonance imaging (MEMRI). Proc Natl Acad Sci U S A 2007;104(7):2489e94.
41. Stein EA, Fuller SA. Selective effects of cocaine on regional cerebral blood flow in the rat. J Pharmacol Exp Ther1992;262(1):327e34.

11. TRANSLATIONAL NEUROIMAGING334
42. Thomas Jr WL, Cooke ES, Hammer Jr RP. Cocaine-induced sensitization of metabolic activity in extrapyra-midal circuits involves prior dopamine D1-like receptor stimulation. J Pharmacol Exp Ther 1996;278(1):347e53.
43. Porrino LJ, Domer FR, Crane AM, Sokoloff L. Selective alterations in cerebral metabolism within the meso-corticolimbic dopaminergic system produced by acute cocaine administration in rats. Neuropsychopharmacology
1988;1(2):109e18.44. Zocchi A, Conti G, Orzi F. Differential effects of cocaine on local cerebral glucose utilization in the mouse and
in the rat. Neurosci Lett 2001;306(3):177e80.45. Orzi F, Dow-Edwards D, Jehle J, Kennedy C, Sokoloff L. Comparative effects of acute and chronic adminis-
tration of amphetamine on local cerebral glucose utilization in the conscious rat. J Cereb Blood Flow Metab
1983;3(2):154e60.46. Wechsler LR, Savaki HE, Sokoloff L. Effects of d- and 1-amphetamine on local cerebral glucose utilization in
the conscious rat. J Neurochem 1979;32(1):15e22.47. Engber TM, Dennis SA, Jones BE, Miller MS, Contreras PC. Brain regional substrates for the actions of the
novel wake-promoting agent modafinil in the rat: comparison with amphetamine. Neuroscience1998;87(4):905e11.
48. Schwarz AJ, Gozzi A, Reese T, Bifone A. In vivo mapping of functional connectivity in neurotransmittersystems using pharmacological MRI. Neuroimage 2007;34(4):1627e36.
49. Porrino LJ, Lucignani G, Dow-Edwards D, Sokoloff L. Correlation of dose-dependent effects of acuteamphetamine administration on behavior and local cerebral metabolism in rats. Brain Res
1984;307(1e2):311e20.50. Ren J, Xu H, Choi JK, Jenkins BG, Chen YI. Dopaminergic response to graded dopamine concentration elicited
by four amphetamine doses. Synapse 2009;63(9):764e72.51. Perles-Barbacaru TA, Procissi D, Demyanenko AV, Jacobs RE. Quantitative pharmacologic MRI in mice. NMR
Biomed Apr 2012;25(4):498e505.52. Lyons D, Friedman DP, Nader MA, Porrino LJ. Cocaine alters cerebral metabolism within the ventral striatum
and limbic cortex of monkeys. J Neurosci 1996;16(3):1230e8.53. Mandeville JB, Choi JK, Jarraya B, Rosen BR, Jenkins BG, Vanduffel W. FMRI of cocaine self-administration in
macaques reveals functional inhibition of basal ganglia. Neuropsychopharmacology 2011;36(6):1187e98.54. Schwarz AJ, Gozzi A, Reese T, Heidbreder CA, Bifone A. Pharmacological modulation of functional connec-
tivity: the correlation structure underlying the phMRI response to d-amphetamine modified by selectivedopamine D3 receptor antagonist SB277011A. Magn Reson Imaging 2007;25(6):811e20.
55. Micheli F, Bonanomi G, Blaney FE, Braggio S, Capelli AM, Checchia A, et al. 1,2,4-triazol-3-yl-thiopropyl-tetrahydrobenzazepines: a series of potent and selective dopamine D(3) receptor antagonists. J Med Chem2007;50(21):5076e89.
56. Chen YC, Choi JK, Andersen SL, Rosen BR, Jenkins BG. Mapping dopamine D2/D3 receptor function usingpharmacological magnetic resonance imaging. Psychopharmacology (Berl) 2005;180(4):705e15.
57. Luo F, Xi ZX, Wu G, Liu C, Gardner EL, Li SJ. Attenuation of brain response to heroin correlates with thereinstatement of heroin-seeking in rats by fMRI. Neuroimage 2004;22(3):1328e35.
58. Xi ZX, Wu G, Stein EA, Li SJ. GABAergic mechanisms of heroin-induced brain activation assessed withfunctional MRI. Magn Reson Med 2002;48(5):838e43.
59. Xi ZX, Wu G, Stein EA, Li S. J, Opiate tolerance by heroin self-administration: an fMRI study in rat.Magn Reson
Med 2004;52(1):108e14.60. Xu H, Li SJ, Bodurka J, Zhao X, Xi ZX, Stein EA. Heroin-induced neuronal activation in rat brain assessed by
functional MRI. Neuroreport 2000;11(5):1085e92.61. Learn JE, Smith DG, McBride WJ, Lumeng L, Li TK. Local cerebral glucose utilization rates in alcohol-naive
high-alcohol-drinking (HAD) and low-alcohol-drinking (LAD) rats. Alcohol Clin Exp Res 2001;25(4):517e23.62. Smith DG, Learn JE, McBride WJ, Lumeng L, Li TK, Murphy JM. Alcohol-naive alcohol-preferring (P) rats
exhibit higher local cerebral glucose utilization than alcohol-nonpreferring (NP) and Wistar rats. Alcohol ClinExp Res 2001;25(9):1309e16.
63. Learn JE, Smith DG, McBride WJ, Lumeng L, Li TK. Ethanol effects on local cerebral glucose utilization inhigh-alcohol-drinking and low-alcohol-drinking rats. Alcohol 2003;29(1):1e9.
64. Strother WN, McBride WJ, Lumeng L, Li TK. Effects of acute administration of ethanol on cerebral glucoseutilization in adult alcohol-preferring and alcohol-nonpreferring rats. Alcohol 2005;35(2):119e28.

REFERENCES 335
65. Murphy JM, Stewart RB, Bell RL, Badia-Elder NE, Carr LG, McBride WJ, et al. Phenotypic and genotypiccharacterization of the Indiana University rat lines selectively bred for high and low alcohol preference. BehavGenet 2002;32(5):363e88.
66. Suarez SV, Amadon A, Giacomini E, Wiklund A, Changeux JP, Le Bihan D, et al. Brain activation by short-termnicotine exposure in anesthetized wild-type and beta2-nicotinic receptors knockout mice: a BOLD fMRI study.Psychopharmacology (Berl) 2009;202(4):599e610.
67. Zahr NM, Mayer D, Vinco S, Orduna J, Luong R, Sullivan EV, et al. In vivo evidence for alcohol-inducedneurochemical changes in rat brain without protracted withdrawal, pronounced thiamine deficiency, or severeliver damage. Neuropsychopharmacology 2009;34(6):1427e42.
68. Lee H, Holburn GH, Price RR. Proton MR spectroscopic studies of chronic alcohol exposure on the rat brain.J Magn Reson Imaging 2003;18(2):147e51.
69. Sullivan EV, Adalsteinsson E, Sood R, Mayer D, Bell R, McBride W, et al. Longitudinal brain magnetic reso-nance imaging study of the alcohol-preferring rat. Part I: adult brain growth. Alcohol Clin Exp Res
2006;30(7):1234e47.70. Pfefferbaum A, Adalsteinsson E, Sood R, Mayer D, Bell R, McBride W, et al. Longitudinal brain magnetic
resonance imaging study of the alcohol-preferring rat. Part II: effects of voluntary chronic alcohol consump-tion. Alcohol Clin Exp Res 2006;30(7):1248e61.
71. Hemmingsen R, Barry DI, Hertz MM, Klinken L. Cerebral blood flow and oxygen consumption during ethanolwithdrawal in the rat. Brain Res 1979;173(2):259e69.
72. Newman LM, Hoffman WE, Miletich DJ, Albrecht RF. Regional blood flow and cerebral metabolic changesduring alcohol withdrawal and following midazolam therapy. Anesthesiology 1985;63(4):395e400.
73. Campbell GA, Eckardt MJ, Majchrowicz E, Marietta CA, Weight FF. Ethanol-withdrawal syndrome associatedwith both general and localized increases in glucose uptake in rat brain. Brain Res 1982;237(2):517e22.
74. Clemmesen L, Ingvar M, Hemmingsen R, Bolwig TG. Local cerebral glucose consumption during ethanolwithdrawal in the rat: effects of single and multiple episodes and previous convulsive seizures. Brain Res
1988;453(1e2):204e14.75. Grunwald F, Schrock H, Theilen H, Biber A, Kuschinsky W. Local cerebral glucose utilization of the awake rat
during chronic administration of nicotine. Brain Res 1988;456(2):350e6.76. London ED, Fanelli RJ, Kimes AS, Moses R. L, Effects of chronic nicotine on cerebral glucose utilization in the
rat. Brain Res 1990;520(1e2):208e14.77. Pagliusi SR, Tessari M, DeVevey S, Chiamulera C, Pich EM. The reinforcing properties of nicotine are asso-
ciated with a specific patterning of c-fos expression in the rat brain. Eur J Neurosci 1996;8(11):2247e56.78. Macey DJ, Rice WN, Freedland CS, Whitlow CT, Porrino LJ. Patterns of functional activity associated with
cocaine self-administration in the rat change over time. Psychopharmacology (Berl) 2004;172(4):384e92.79. Porrino LJ, Lyons D, Smith HR, Daunais JB, Nader MA. Cocaine self-administration produces a progressive
involvement of limbic, association, and sensorimotor striatal domains. J Neurosci 2004;24(14):3554e62.80. Hammer Jr RP, Pires WS, Markou A, Koob GF. Withdrawal following cocaine self-administration decreases
regional cerebral metabolic rate in critical brain reward regions. Synapse 1993;14(1):73e80.81. Gozzi A, Tessari M, Dacome L, Agosta F, Lepore S, Lanzoni A, et al. Neuroimaging evidence of altered fronto-
cortical and striatal function after prolonged cocaine self-administration in the rat. Neuropsychopharmacology2011;36(12):2431e40.
82. Chen YI, Famous K, Xu H, Choi JK, Mandeville JB, Schmidt HD, et al. Cocaine self-administration leads toalterations in temporal responses to cocaine challenge in limbic and motor circuitry. Eur J Neurosci
2011;34(5):800e15.83. Morris ED, Yoder KK, Wang C, Normandin MD, Zheng QH, Mock B, et al. ntPET: a new application of PET
imaging for characterizing the kinetics of endogenous neurotransmitter release. Mol Imaging 2005;4(4):473e89.
84. Boileau I, Assaad JM, Pihl RO, Benkelfat C, Leyton M, Diksic M, et al. Alcohol promotes dopamine release inthe human nucleus accumbens. Synapse 2003;49(4):226e31.
85. Schiffer WK, Mirrione MM, Dewey SL. Optimizing experimental protocols for quantitative behavioral imagingwith 18F-FDG in rodents. J Nucl Med 2007;48(2):277e87.
86. Patel VD, Lee DE, Alexoff DL, Dewey SL, Schiffer WK. Imaging dopamine release with Positron EmissionTomography (PET) and (11)C-raclopride in freely moving animals. Neuroimage 2008;41(3):1051e66.

11. TRANSLATIONAL NEUROIMAGING336
87. Schiffer WK, Liebling CN, Reiszel C, Hooker JM, Brodie JD, Dewey SL. Cue-induced dopamine releasepredicts cocaine preference: positron emission tomography studies in freely moving rodents. J Neurosci
2009;29(19):6176e85.88. Lowry JP, Griffin K, McHugh SB, Lowe AS, TricklebankM, Sibson NR. Real-time electrochemical monitoring of
brain tissue oxygen: a surrogate for functional magnetic resonance imaging in rodents. Neuroimage
2010;52(2):549e55.89. Haney M. Self-administration of cocaine, cannabis and heroin in the human laboratory: benefits and pitfalls.
Addict Biol 2009;14(1):9e21.90. Czachowski CL, Samson HH. Ethanol- and sucrose-reinforced appetitive and consummatory responding in
HAD1, HAD2, and P rats. Alcohol Clin Exp Res 2002;26(11):1653e61.91. Vosburg SK, Haney M, Rubin E, Foltin RW. Using a novel alternative to drug choice in a human laboratory
model of a cocaine binge: a game of chance. Drug Alcohol Depend 2010;110(1e2):144e50.92. Foltin RW, Fischman MW, Pedroso JJ, Pearlson GD. Marijuana and cocaine interactions in humans: cardio-
vascular consequences. Pharmacol Biochem Behav 1987;28(4):459e64.93. Swendsen J, Conway KP, Degenhardt L, Glantz M, Jin R, Merikangas KR, et al. Mental disorders as risk factors
for substance use, abuse and dependence: results from the 10-year follow-up of the National ComorbiditySurvey. Addiction 2010;105(6):1117e28.
94. Vansickel AR, Cobb CO, Weaver MF, Eissenberg TE. A clinical laboratory model for evaluating the acute effectsof electronic “ cigarettes”: nicotine delivery profile and cardiovascular and subjective effects. Cancer Epidemiol
Biomarkers Prev 2010;19(8):1945e53.95. Penetar DM, Maclean RR, McNeil JF, Lukas SE. Kudzu extract treatment does not increase the intoxicating
effects of acute alcohol in human volunteers. Alcohol Clin Exp Res 2011;35(4):726e34.96. Urban NB, Kegeles LS, Slifstein M, Xu X, Martinez D, Sakr E, et al. Sex differences in striatal dopamine release
in young adults after oral alcohol challenge: a positron emission tomography imaging study with [(1)(1)C]raclopride. Biol Psychiatry 2010;68(8):689e96.
97. King AC, Byars JA. Alcohol-induced performance impairment in heavy episodic and light social drinkers.J Stud Alcohol 2004;65(1):27e36.
98. King AC, de Wit H, McNamara PJ, Cao D. Rewarding, stimulant, and sedative alcohol responses and rela-tionship to future binge drinking. Arch Gen Psychiatry 2011;68(4):389e99.
99. Ray LA, Hutchison KE, MacKillop J, Miranda Jr R, Audette A, Swift R, et al. Effects of naltrexone during thedescending limb of the blood alcohol curve. Am J Addict 2008;17(4):257e64.
100. Drobes DJ, Anton RF, Thomas SE, Voronin K. A clinical laboratory paradigm for evaluatingmedication effects on alcohol consumption: naltrexone and nalmefene. Neuropsychopharmacology2003;28(4):755e64.
101. Ramchandani VA, Plawecki M, Li TK, O’Connor S. Intravenous ethanol infusions can mimic the time course ofbreath alcohol concentrations following oral alcohol administration in healthy volunteers. Alcohol Clin Exp Res
2009;33(5):938e44.102. Friel PN, Baer JS, Logan BK. Variability of ethanol absorption and breath concentrations during a large-scale
alcohol administration study. Alcohol Clin Exp Res 1995;19(4):1055e60.103. Ramchandani VA, Flury L, Morzorati SL, Kareken D, Blekher T, Foroud T, et al. Recent drinking history:
association with family history of alcoholism and the acute response to alcohol during a 60 mg% clamp. J StudAlcohol 2002;63(6):734e44.
104. Neumark YD, Friedlander Y, Durst R, Leitersdorf E, Jaffe D, Ramchandani VA, et al. Alcohol dehydrogenasepolymorphisms influence alcohol-elimination rates in a male Jewish population. Alcohol Clin Exp Res2004;28(1):10e4.
105. Morzorati SL, Ramchandani VA, Flury L, Li TK, O’Connor S. Self-reported subjective perception of intoxicationreflects family history of alcoholism when breath alcohol levels are constant. Alcohol Clin Exp Res
2002;26(8):1299e306.106. Blekher T, Ramchandani VA, Flury L, Foroud T, Kareken D, Yee RD, et al. Saccadic eye movements are
associated with a family history of alcoholism at baseline and after exposure to alcohol. Alcohol Clin Exp Res
2002;26(10):1568e73.107. Ramchandani VA, Bolane J, Li TK, O’Connor S. A physiologically-based pharmacokinetic (PBPK) model for
alcohol facilitates rapid BrAC clamping. Alcohol Clin Exp Res 1999;23(4):617e23.

REFERENCES 337
108. Ramchandani VA, O’Connor S, Blekher T, Kareken D, Morzorati S, Nurnberger Jr J, et al. A preliminary studyof acute responses to clamped alcohol concentration and family history of alcoholism. Alcohol Clin Exp Res
1999;23(8):1320e30.109. O’Connor S, Ramchandani VA, Li TK. PBPK modeling as a basis for achieving a steady BrAC of 60 þ/- 5 mg%
within ten minutes. Alcohol Clin Exp Res 2000;24(4):426e7.110. Roh S, Matsushita S, Hara S, Maesato H, Matsui T, Suzuki G, et al. Role of GABRA2 in moderating subjective
responses to alcohol. Alcohol Clin Exp Res 2011;35(3):400e7.111. Gomez R, Behar KL, Watzl J, Weinzimer SA, Gulanski B, Sanacora G, et al. Intravenous Ethanol Infusion
Decreases Human Cortical gamma-Aminobutyric Acid and N-Acetylaspartate as Measured with ProtonMagnetic Resonance Spectroscopy at 4 Tesla. Biol Psychiatry 2012;71(3):239e46.
112. de Wit H, McCracken SG. Ethanol self-administration in males with and without an alcoholic first-degreerelative. Alcohol Clin Exp Res 1990;14(1):63e70.
113. Petrakis IL, Buonopane A, O’Malley S, Cermik O, Trevisan L, Boutros NN, et al. The effect of tryptophandepletion on alcohol self-administration in non-treatment-seeking alcoholic individuals. Alcohol Clin Exp Res2002;26(7):969e75.
114. Zimmermann US, Mick I, Laucht M, Vitvitskiy V, Plawecki MH, Mann KF, et al. Offspring of parents with analcohol use disorder prefer higher levels of brain alcohol exposure in experiments involving computer-assistedself-infusion of ethanol (CASE). Psychopharmacology (Berl) 2009;202(4):689e97.
115. McKee SA, Harrison EL, O’Malley SS, Krishnan-Sarin S, Shi J, Tetrault JM, et al. Varenicline reduces alcoholself-administration in heavy-drinking smokers. Biol Psychiatry 2009;66(2):185e90.
116. Sarid-Segal O, Knapp CM, Burch W, Richardson MA, Bahtia S, DeQuattro K, et al. The anticonvulsant zoni-samide reduces ethanol self-administration by risky drinkers. Am J Drug Alcohol Abuse 2009;35(5):316e9.
117. George DT, Herion DW, Jones CL, Phillips MJ, Hersh J, Hill D, et al. Rimonabant (SR141716) has no effect onalcohol self-administration or endocrine measures in nontreatment-seeking heavy alcohol drinkers. Psycho-pharmacology (Berl) 2010;208(1):37e44.
118. Davidson D, Palfai T, Bird C, Swift R. Effects of naltrexone on alcohol self-administration in heavy drinkers.Alcohol Clin Exp Res 1999;23(2):195e203.
119. O’Malley SS, Krishnan-Sarin S, Farren C, Sinha R, Kreek MJ. Naltrexone decreases craving and alcohol self-administration in alcohol-dependent subjects and activates the hypothalamo-pituitary-adrenocortical axis.Psychopharmacology (Berl) 2002;160(1):19e29.
120. McKee SA, O’Malley SS, Shi J, Mase T, Krishnan-Sarin S. Effect of transdermal nicotine replacement on alcoholresponses and alcohol self-administration. Psychopharmacology (Berl) 2008;196(2):189e200.
121. Setiawan E, Pihl RO, Cox SM, Gianoulakis C, Palmour RM, Benkelfat C, et al. The effect of naltrexone onalcohol’s stimulant properties and self-administration behavior in social drinkers: influence of gender andgenotype. Alcohol Clin Exp Res 2011;35(6):1134e41.
122. Zimmermann US, O’Connor S, Ramchandani VA. Modeling Alcohol Self-Administration in the HumanLaboratory. Curr Top Behav Neurosci 2011 [Epub ahead of print].
123. Spiga R, Macenski MJ, Meisch RA, Roache JD. Human ethanol self-administration. I: The interaction betweenresponse requirement and ethanol dose. Behav Pharmacol 1997;8(1):91e100.
124. Perkins KA, Fonte C, Grobe JE. Sex differences in the acute effects of cigarette smoking on the reinforcing valueof alcohol. Behav Pharmacol 2000;11(1):63e70.
125. Barrett SP, Pihl RO, Benkelfat C, Brunelle C, Young SN, Leyton M. Nicotine increases alcohol self-adminis-tration in non-dependent male smokers. Drug Alcohol Depend 2006;81(2):197e204.
126. Barrett SP, Tichauer M, Leyton M, Pihl RO. The role of dopamine in alcohol self-administration in humans:individual differences. Eur Neuropsychopharmacol 2008;18(6):439e47.
127. Zimmermann US, Mick I, Vitvitskyi V, Plawecki MH, Mann KF, O’Connor S. Development and pilot validationof computer-assisted self-infusion of ethanol (CASE): a new method to study alcohol self-administration inhumans. Alcohol Clin Exp Res 2008;32(7):1321e8.
128. Drobes DJ, Anton RF. Drinking in alcoholics following an alcohol challenge research protocol. J Stud Alcohol
2000;61(2):220e4.129. Drobes DJ, Anton RF, Thomas SE, Voronin K. Effects of naltrexone and nalmefene on subjective response to
alcohol among non-treatment-seeking alcoholics and social drinkers. Alcohol Clin Exp Res 2004;28(9):1362e70.

11. TRANSLATIONAL NEUROIMAGING338
130. Modell JG, Glaser FB, Mountz JM. The ethics and safety of alcohol administration in the experimental setting toindividuals who have chronic, severe alcohol problems. Alcohol 1993;28(2):189e97.
131. Sinha R, Krishnan-Sarin S, Farren C, O’Malley S. Naturalistic follow-up of drinking behavior followingparticipation in an alcohol administration study. J Subst Abuse Treat 1999;17(1e2):159e62.
132. Brumback T, Cao D, King A. Effects of alcohol on psychomotor performance and perceived impairment inheavy binge social drinkers. Drug Alcohol Depend 2007;91(1):10e7.
133. Miranda Jr R, MacKillop J, Monti PM, Rohsenow DJ, Tidey J, Gwaltney C, et al. Effects of topiramate on urge todrink and the subjective effects of alcohol: a preliminary laboratory study. Alcohol Clin Exp Res
2008;32(3):489e97.134. Kareken DA, Liang T, Wetherill L, Dzemidzic M, Bragulat V, Cox C, et al. A polymorphism in GABRA2 is
associated with the medial frontal response to alcohol cues in an fMRI study. Alcohol Clin Exp Res2010;34(12):2169e78.
135. King A, Munisamy G, de Wit H, Lin S. Attenuated cortisol response to alcohol in heavy social drinkers. Int JPsychophysiol 2006;59(3):203e9.
136. Schuckit MA. Low level of response to alcohol as a predictor of future alcoholism. Am J Psychiatry
1994;151(2):184e9.137. Trim RS, Simmons AN, Tolentino NJ, Hall SA, Matthews SC, Robinson SK, et al. Acute ethanol effects on brain
activation in low- and high-level responders to alcohol. Alcohol Clin Exp Res 2010;34(7):1162e70.138. Wilhelmsen KC, Schuckit M, Smith TL, Lee JV, Segall SK, Feiler HS, et al. The search for genes related to a low-
level response to alcohol determined by alcohol challenges. Alcohol Clin Exp Res 2003;27(7):1041e7.139. Schuckit MA. Subjective responses to alcohol in sons of alcoholics and control subjects. Arch Gen Psychiatry
1984;41(9):879e84.140. Zimmermann US, Buchmann AF, Spring C, Uhr M, Holsboer F, Wittchen HU. Ethanol administration dampens
the prolactin response to psychosocial stress exposure in sons of alcohol-dependent fathers. Psychoneur-
oendocrinology 2009;34(7):996e1003.141. Mick I, Spring K, Uhr M, Zimmermann US. Alcohol administration attenuates hypothalamic-pituitary-adrenal
(HPA) activity in healthy men at low genetic risk for alcoholism, but not in high-risk subjects. Addict Biol 2012[Epub ahead of print].
142. Grant JD, Heath AC, Madden PA, Bucholz KK, Whitfield JB, Martin NG. An assessment of the genetic rela-tionship between alcohol metabolism and alcoholism risk in Australian twins of European ancestry. BehavGenet 1999;29(6):463e72.
143. Heath AC, Madden PA, Bucholz KK, Dinwiddie SH, Slutske WS, Bierut LJ, et al. Genetic differences in alcoholsensitivity and the inheritance of alcoholism risk. Psychol Med 1999;29(5):1069e81.
144. Lind PA, MacGregor S, Montgomery GW, Heath AC, Martin NG, Whitfield JB. Effects of GABRA2 variation onphysiological, psychomotor and subjective responses in the alcohol challenge twin study. Twin Res Hum Genet
2008;11(2):174e82.145. Heath AC, Martin NG. Genetic differences in psychomotor performance decrement after alcohol: a multivar-
iate analysis. J Stud Alcohol 1992;53(3):262e71.146. Ramchandani VA, Umhau J, Pavon FJ, Ruiz-Velasco V, Margas W, Sun H, et al. A genetic determinant of the
striatal dopamine response to alcohol in men. Mol Psychiatry 2011;16(8):809e17.147. Ray LA, Hutchison KE. Effects of naltrexone on alcohol sensitivity and genetic moderators of medication
response: a double-blind placebo-controlled study. Arch Gen Psychiatry 2007;64(9):1069e77.148. Ray LA, Hutchison KE, Ashenhurst JR, Morrow AL. Naltrexone selectively elevates GABAergic neuroactive
steroid levels in heavy drinkers with the Asp40 allele of the OPRM1 gene: a pilot investigation. Alcohol Clin ExpRes 2010;34(8):1479e87.
149. Arias AJ, Armeli S, Gelernter J, Covault J, Kallio A, Karhuvaara S, et al. Effects of opioid receptorgene variation on targeted nalmefene treatment in heavy drinkers. Alcohol Clin Exp Res 2008;32(7):1159e66.
150. Pierucci-Lagha A, Covault J, Feinn R, Nellissery M, Hernandez-Avila C, Oncken C, et al. GABRA2 allelesmoderate the subjective effects of alcohol, which are attenuated by finasteride. Neuropsychopharmacology
2005;30(6):1193e203.151. McCarthy DM, Pedersen SL, Lobos EA, Todd RD, Wall TL. ADH1B*3 and response to alcohol in African-
Americans. Alcohol Clin Exp Res 2010;34(7):1274e81.

REFERENCES 339
152. Duranceaux NC, Schuckit MA, Eng MY, Robinson SK, Carr LG, Wall TL. Associations of variations in alcoholdehydrogenase genes with the level of response to alcohol in non-Asians. Alcohol Clin Exp Res
2006;30(9):1470e8.153. Buhler M, Mann K. Alcohol and the human brain: a systematic review of different neuroimaging methods.
Alcohol Clin Exp Res 2011;35(10):1771e93.154. Carlen PL, Wortzman G, Holgate RC, Wilkinson DA, Rankin JC. Reversible cerebral atrophy in recently
abstinent chronic alcoholics measured by computed tomography scans. Science 1978;200(4345):1076e8.155. Carlen PL, Wilkinson DA, Holgate R, Wortzman G. Computed tomography scans of alcoholics: cerebral
atrophy? Science 1979;204(4398):1238.156. Carlen PL, Wilkinson DA, Wortzman G, Holgate R. Partially reversible cerebral atrophy and functional
improvement in recently abstinent alcoholics. Can J Neurol Sci 1984;11(4):441e6.157. Gotze P, Kuhne D, Hansen J, Knipp HP. [Brain atrophy in chronic alcoholism. Clinical and computer tomo-
graphic study]. Arch Psychiatr Nervenkr 1978;226(2):137e56.158. Hommer D, Momenan R, Kaiser E, Rawlings R. Evidence for a gender-related effect of alcoholism on brain
volumes. Am J Psychiatry 2001;158(2):198e204.159. Fein G, Di Sclafani V, Cardenas VA, Goldmann H, Tolou-Shams M, Meyerhoff DJ. Cortical gray matter loss in
treatment-naive alcohol dependent individuals. Alcohol Clin Exp Res 2002;26(4):558e64.160. Pfefferbaum A, Sullivan EV, Rosenbloom MJ, Mathalon DH, Lim KO. A controlled study of cortical gray
matter and ventricular changes in alcoholic men over a 5-year interval. Arch Gen Psychiatry 1998;55(10):905e12.
161. Pfefferbaum A, Adalsteinsson E, Sullivan EV. Dysmorphology and microstructural degradation of the corpuscallosum: Interaction of age and alcoholism. Neurobiol Aging 2006;27(7):994e1009.
162. Pfefferbaum A, Rosenbloom M, Rohlfing T, Sullivan EV. Degradation of association and projection whitematter systems in alcoholism detected with quantitative fiber tracking. Biol Psychiatry 2009;65(8):680e90.
163. Azizian A, Monterosso J, O’Neill J, London ED. Magnetic resonance imaging studies of cigarette smoking.Handb Exp Pharmacol 2009;192:113e43.
164. Durazzo TC, Rothlind JC, Cardenas VA, Studholme C, Weiner MW, Meyerhoff DJ. Chronic cigarette smokingand heavy drinking in human immunodeficiency virus: consequences for neurocognition and brainmorphology. Alcohol 2007;41(7):489e501.
165. Durazzo TC, Gazdzinski S, Banys P, Meyerhoff DJ. Cigarette smoking exacerbates chronic alcohol-inducedbrain damage: a preliminary metabolite imaging study. Alcohol Clin Exp Res 2004;28(12):1849e60.
166. Gallinat J, Lang UE, Jacobsen LK, Bajbouj M, Kalus P, von Haebler D, et al. Abnormal hippocampal neuro-chemistry in smokers: evidence from proton magnetic resonance spectroscopy at 3 T. J Clin Psychopharmacol2007;27(1):80e4.
167. Volkow ND, Wang GJ, Fowler JS, Logan J, Gatley SJ, Wong C, et al. Reinforcing effects of psychostimulants inhumans are associated with increases in brain dopamine and occupancy of D(2) receptors. J Pharmacol Exp Ther
1999;291(1):409e15.168. Drevets WC, Gautier C, Price JC, Kupfer DJ, Kinahan PE, Grace AA, et al. Amphetamine-induced dopamine
release in human ventral striatum correlates with euphoria. Biol Psychiatry 2001;49(2):81e96.169. Brody AL, Mandelkern MA, Olmstead RE, Allen-Martinez Z, Scheibal D, Abrams AL, et al. Ventral striatal
dopamine release in response to smoking a regular vs a denicotinized cigarette. Neuropsychopharmacology
2009;34(2):282e9.170. Bossong MG, van Berckel BN, Boellaard R, Zuurman L, Schuit RC, et al. Delta 9-tetrahydrocannabinol induces
dopamine release in the human striatum. Neuropsychopharmacology 2009;34(3):759e66.171. Volkow ND, Wang GJ, Fowler JS, Tomasi D, Telang F. Addiction: beyond dopamine reward circuitry. Proc Natl
Acad Sci U S A 2011;108(37):15037e42.172. Berridge KC, Robinson TE, Aldridge JW. Dissecting components of reward: ‘liking’, ‘wanting’, and learning.
Curr Opin Pharmacol 2009;9(1):65e73.173. Schultz W. Behavioral dopamine signals. Trends Neurosci 2007;30(5):203e10.174. Volkow ND, Fowler JS, Wang GJ, Baler R, Telang F. Imaging dopamine’s role in drug abuse and addiction.
Neuropharmacology 2009;56(Suppl. 1):3e8.175. Martinez D, Gil R, Slifstein M, Hwang DR, Huang Y, Perez A, et al. Alcohol dependence is associated with
blunted dopamine transmission in the ventral striatum. Biol Psychiatry 2005;58(10):779e86.

11. TRANSLATIONAL NEUROIMAGING340
176. Martinez D, Narendran R, Foltin RW, Slifstein M, Hwang DR, Broft A, et al. Amphetamine-induced dopaminerelease: markedly blunted in cocaine dependence and predictive of the choice to self-administer cocaine. Am J
Psychiatry 2007;164(4):622e9.177. Fehr C, Yakushev I, Hohmann N, Buchholz HG, Landvogt C, Deckers H, et al. Association of low striatal
dopamine d2 receptor availability with nicotine dependence similar to that seen with other drugs of abuse.Am J Psychiatry 2008;165(4):507e14.
178. Volkow ND, Fowler JS. Addiction, a disease of compulsion and drive: involvement of the orbitofrontal cortex.Cereb Cortex 2000;10(3):318e25.
179. Volkow ND, Fowler JS, Wang GJ, Swanson JM. Dopamine in drug abuse and addiction: results from imagingstudies and treatment implications. Mol Psychiatry 2004;9(6):557e69.
180. Yoder KK, Kareken DA, Morris ED. What were they thinking? Cognitive states may influence [11C]raclopridebinding potential in the striatum. Neurosci Lett 2008;430(1):38e42.
181. Khalili-Mahani N, van Osch MJ, Baerends E, Soeter RP, de Kam M, et al. Pseudocontinuous arterial spinlabeling reveals dissociable effects of morphine and alcohol on regional cerebral blood flow. J Cereb Blood FlowMetab 2011;31(5):1321e33.
182. Khalili-Mahani N, Zoethout RM, Beckmann CF, Baerends E, de KamML, et al. Effects of morphine and alcoholon functional brain connectivity during “resting state”: A placebo-controlled crossover study in healthy youngmen. Hum Brain Mapp May 2012;33(5):1003e18.
183. Stein EA, Pankiewicz J, Harsch HH, Cho JK, Fuller SA, Hoffmann RG, et al. Nicotine-induced limbic corticalactivation in the human brain: a functional MRI study. Am J Psychiatry 1998;155(8):1009e15.
184. Breiter HC, Gollub RL, Weisskoff RM, Kennedy DN, Makris N, Berke JD, et al. Acute effects of cocaine onhuman brain activity and emotion. Neuron 1997;19(3):591e611.
185. Kufahl PR, Li Z, Risinger RC, Rainey CJ, Wu G, Bloom AS, et al. Neural responses to acute cocaine admin-istration in the human brain detected by fMRI. Neuroimage 2005;28(4):904e14.
186. Kufahl P, Li Z, Risinger R, Rainey C, Piacentine L, Wu G, et al. Expectation modulates human brain responsesto acute cocaine: a functional magnetic resonance imaging study. Biol Psychiatry 2008;63(2):222e30.
187. Becerra L, Harter K, Gonzalez RG, Borsook D. Functional magnetic resonance imaging measures of the effectsof morphine on central nervous system circuitry in opioid-naive healthy volunteers. Anesth Analg
2006;103(1):208e16. table of contents.188. Filbey FM, Claus E, Audette AR, Niculescu M, Banich MT, Tanabe J, et al. Exposure to the taste of alcohol
elicits activation of the mesocorticolimbic neurocircuitry. Neuropsychopharmacology 2008;33(6):1391e401.189. Kareken DA, Claus ED, Sabri M, Dzemidzic M, Kosobud AE, Radnovich AJ, et al. Alcohol-related olfactory
cues activate the nucleus accumbens and ventral tegmental area in high-risk drinkers: preliminary findings.Alcohol Clin Exp Res 2004;28(4):550e7.
190. Bragulat V, Dzemidzic M, Talavage T, Davidson D, O’Connor SJ, Kareken DA. Alcohol sensitizes cerebralresponses to the odors of alcoholic drinks: an fMRI study. Alcohol Clin Exp Res 2008;32(7):1124e34.
191. Oberlin BG, Dzemidzic M, Bragulat V, Lehigh CA, Talavage T, O’Connor SJ, et al. Limbic responses to rewardcues correlate with antisocial trait density in heavy drinkers. Neuroimage 2011;60(1):644e52.
192. Kareken DA, Grahame N, Dzemidzic M, Walker MJ, Lehigh CA, O’Connor SJ. fMRI of the brain’s response tostimuli experimentally paired with alcohol intoxication. Psychopharmacology (Berl) Apr 2012;220(4):787e97.
193. Kareken DA, Bragulat V, Dzemidzic M, Cox C, Talavage T, Davidson D, et al. Family history of alcoholismmediates the frontal response to alcoholic drink odors and alcohol in at-risk drinkers. Neuroimage
2010;50(1):267e76.194. Hutchison KE, Haughey H, Niculescu M, Schacht J, Kaiser A, Stitzel J, et al. The incentive salience of alcohol:
translating the effects of genetic variant in CNR1. Arch Gen Psychiatry 2008;65(7):841e50.195. Liu J, Calhoun VD, Chen J, Claus ED, Hutchison KE. Effect of homozygous deletions at 22q13.1 on alcohol
dependence severity and cue-elicited BOLD response in the precuneus. Addict Biol; 2011 [Epub ahead of print].196. Kuhn S, Gallinat J. Common biology of craving across legal and illegal drugsda quantitative meta-analysis of
cue-reactivity brain response. Eur J Neurosci 2011;33(7):1318e26.197. Chase HW, Eickhoff SB, Laird AR, Hogarth L. The neural basis of drug stimulus processing and craving: an
activation likelihood estimation meta-analysis. Biol Psychiatry 2011;70(8):785e93.198. Wrase J, Schlagenhauf F, Kienast T, Wustenberg T, Bermpohl F, Kahnt T, et al. Dysfunction of reward pro-
cessing correlates with alcohol craving in detoxified alcoholics. Neuroimage 2007;35(2):787e94.

REFERENCES 341
199. Hommer DW, Bjork JM, Gilman JM. Imaging brain response to reward in addictive disorders. Ann N YAcad Sci
2011;1216:50e61.200. George DT, Gilman J, Hersh J, Thorsell A, Herion D, Geyer C, et al. Neurokinin 1 receptor antagonism as
a possible therapy for alcoholism. Science 2008;319(5869):1536e9.201. Newhouse PA, Potter AS, Dumas JA, Thiel CM. Functional brain imaging of nicotinic effects on higher
cognitive processes. Biochem Pharmacol 2011;82(8):943e51.202. Loughead J, Ray R, Wileyto EP, Ruparel K, O’Donnell GP, Senecal N, et al. Brain activity and emotional
processing in smokers treated with varenicline. Addict Biol 2011 [Epub ahead of print].203. Schuckit MA, Tapert S, Matthews SC, Paulus MP, Tolentino NJ, Smith TL, et al. FMRI differences between
subjects with low and high responses to alcohol during a stop signal task. Alcohol Clin Exp Res
2012;36(1):130e40.204. Gilman JM, Ramchandani VA, Davis MB, Bjork JM, Hommer DW. Why we like to drink: a functional magnetic
resonance imaging study of the rewarding and anxiolytic effects of alcohol. J Neurosci 2008;28(18):4583e91.205. Filbey FM, Claus ED, Morgan M, Forester GR, Hutchison K. Dopaminergic genes modulate response inhibition
in alcohol abusing adults. Addict Biol 2011 [Epub ahead of print].206. Villafuerte S, Heitzeg MM, Foley S, Wendy Yau WY, Majczenko K, et al. Impulsiveness and insula activation
during reward anticipation are associated with genetic variants in GABRA2 in a family sample enriched foralcoholism. Mol Psychiatry May 2012;17(5):511e9.
207. Winterer G, Musso F, Konrad A, Vucurevic G, Stoeter P, Sander T, et al. Association of attentional networkfunction with exon 5 variations of the CHRNA4 gene. Hum Mol Genet 2007;16(18):2165e74.
208. Janes AC, Smoller JW, David SP, Frederick BD, Haddad S, Basu A, et al. Association between CHRNA5 geneticvariation at rs16969968 and brain reactivity to smoking images in nicotine dependent women. Drug AlcoholDepend 2012;120(1e3):7e13.
209. Hermann D, Smolka MN, Wrase J, Klein S, Nikitopoulos J, Georgi A, et al. Blockade of cue-induced brainactivation of abstinent alcoholics by a single administration of amisulpride as measured with fMRI. AlcoholClin Exp Res 2006;30(8):1349e54.
210. Myrick H, Anton RF, Li X, Henderson S, Randall PK, Voronin K. Effect of naltrexone and ondansetron onalcohol cue-induced activation of the ventral striatum in alcohol-dependent people. Arch Gen Psychiatry
2008;65(4):466e75.211. Myrick H, Li X, Randall PK, Henderson S, Voronin K, Anton R. F, The effect of aripiprazole on cue-induced
brain activation and drinking parameters in alcoholics. J Clin Psychopharmacol 2010;30(4):365e72.212. Kranzler HR, Covault J, Pierucci-Lagha A, Chan G, Douglas K, Arias AJ, et al. Effects of aripiprazole on
subjective and physiological responses to alcohol. Alcohol Clin Exp Res 2008;32(4):573e9.213. Voronin K, Randall P, Myrick H, Anton R. Aripiprazole effects on alcohol consumption and subjective reports
in a clinical laboratory paradigmdpossible influence of self-control. Alcohol Clin Exp Res 2008;32(11):1954e61.214. Franklin T, Wang Z, Suh JJ, Hazan R, Cruz J, Li Y, et al. Effects of varenicline on smoking cue-triggered neural
and craving responses. Arch Gen Psychiatry 2011;68(5):516e26.215. Loughead J, Ray R, Wileyto EP, Ruparel K, Sanborn P, Siegel S, et al. Effects of the alpha4beta2 partial agonist
varenicline on brain activity and working memory in abstinent smokers. Biol Psychiatry 2010;67(8):715e21.216. Mier D, Kirsch P, Meyer-Lindenberg A. Neural substrates of pleiotropic action of genetic variation in COMT:
a meta-analysis. Mol Psychiatry 2010;15(9):918e27.217. Tauscher J, Schwarz AJ. Imaging biomarkers in drug development: case studies. In: Littman BH, Krishna R,
editors. Translational medicine and drug discovery. Cambridge: University Press; 2011. p. 222e64.218. Cole PE, Schwarz AJ, Schmidt ME. Applications of imaging biomarkers in the early clinical development of
central nervous system therapeutics. Clinical Pharmacology and Therapeutics Feb 2012;91(2):315e20.219. Schwarz AJ, Becerra L, Upadhyay J, Anderson J, Baumgartner R, Coimbra A, et al. A procedural framework for
good imaging practice in pharmacological fMRI studies applied to drug development #2: protocol optimi-zation and best practices. Drug Discov Today 2011;16(15e16):671e82.
220. London ED, Connolly RJ, Szikszay M, Wamsley J. K, Distribution of cerebral metabolic effects of nicotine in therat. Eur J Pharmacol 1985;110(3):391e2.