Embed Size (px)
Citation preview

C H A P T E R
9
Translational Neuroimaging for DrugDiscovery and Development inAutism Spectrum Disorders
Guidance from Clinical Imagingand Preclinical Research
Lori L. Badura 1, Michael D. Saxe 2, Celine Risterucci 3,Michael J. Brammer 4, Stephanie M. McTighe 5,
Robert H. Ring 6, Daniel G. Smith 6
1Percepts Ltd, 609 S Canterbury Road, Canterbury, CT 06331, USA2 Functional Neuroscience Research, F. Hoffmann-La Roche Ltd, Grenzacherstrasse 124,
CH-4070 Basel, Switzerland3CNS Biomarker & Pathophysiology, F. Hoffmann-La Roche Ltd, Grenzacherstrasse 124,
CH-4070 Basel, Switzerland4Centre for Neuroimaging Sciences, Institute of Psychiatry, Kings College, P089,
De Crespigny Park, London SE5 8AF, UK5Neuroscience Research Unit, Pfizer Global Research & Development, 700 Main Street,
Cambridge, MA 02139, USA6Autism Speaks, 1060 State Road, Princeton, NJ 08540, USA
T
h
1.0. Introduction 2
461.1. Autism Definition, Prevalence,and Treatment History 246
1.2. Translational Research Definition 2472.0. Clinical Imaging in AutismSpectrum Disorders 2
48245ranslational Neuroimaging
ttp://dx.doi.org/10.1016/B978-0-12-386945-6.00009-3
2.1. Emotional and Social Intelligence 25
02.2. Cognition and Memory 251 2.3. Default Networks 252 2.4. Novel Analysis Approaches 253 2.5. Application of Human Imagingin Autism Spectrum DisorderTranslational Research 254
� 2013 Elsevier Inc. All rights reserved.

9. TRANSLATIONAL NEUROIMAGING IN AUTISM SPECTRUM DISORDERS246
3.0. Preclinical Genetic Modelingof Autism Spectrum Disorders 2
563.1. Rare Variants UnderlyingSyndromic Autism SpectrumDisorders 256
3.1.1. FMR1 Models 2563.1.2. MECP2/Rett Syndrome
Models
2603.1.3. PTEN Models
2613.1.4. NLGN and NRXN
Models
2623.1.5. CNTNAP2 Gene
2643.1.6. SHANK Gene Models
2653.2. Mouse Models of 15q11e13Chromosomal Abnormalities 266
3.3. BTBR Mouse Models of CoreAutism Behavioral Symptoms 267
3.4. Application of Genetic Models inAutism Spectrum DisorderTranslational Research 268
4.0. Challenges and Approaches inTranslating from Bench to Patients 2
69SummaryThere is a profound unmet medical need for treatments that alleviate the core symptoms of autism spectrumdisorders (ASDs). Drug discovery and development for ASDs is complicated by the highly heterogeneousgenetics and behavioral phenotypes characteristic of ASDs, a poor understanding of ASD pathophysiology,and a lack of biomarkers. Translatable functional neuroimaging and electrophysiology techniques providea means to delineate neural circuits and pathophysiology underlying ASDs, and may improve the medica-tions development process by defining quantitative translational endpoints that align preclinical and clinicalarenas. There is a lack of functional imaging research on responses to potential therapeutics in ASD patientsand in animal models of ASD, but a rapidly growing body of research characterizing resting state and task-related neural circuit activation in ASD patients, and neurophysiology and behavioral phenotypes in ASDanimal models, is providing valuable insight for building a neurocircuitry-based translational strategy todefine patient populations and assess drug efficacy. The focus of this chapter is to review clinical neuro-imaging research in ASDs and research in preclinical ASD models with an eye toward identifying neuralcircuits for use in translational ASD drug development strategies.
1.0. INTRODUCTION
1.1. Autism Definition, Prevalence, and Treatment History
Autism is defined by the Diagnostic and Statistical Manual of Mental Disorders, 4th
Edition, Text Revision (DSM-IV-TR) by the core symptoms of qualitative impairment in recip-rocal social interaction, qualitative impairment in verbal and nonverbal communication, andrestricted repetitive and stereotyped patterns of behavior and interests. Many autism patientspresent with one or more adjunct symptoms, including intellectual disability and seizuredisorders. The term autism spectrum disorders (ASDs) is not formally defined, but iscommonly used to refer to classic autism, Asperger syndrome, and several monogenic neuro-developmental disorders with increased incidence of one or more core autism features,including Rett, fragile X, Angelman, and 22q13 deletion (also called Phelan-McDermid)syndromes. ASDs present clinically with great heterogeneity spanning two extremes,

1.0. INTRODUCTION 247
with children showing profound intellectual disability, dysmorphic features, congenital mal-formations, and robust repetitive and self-injurious behavior at one end, and patients withnormal IQ, mild social behavioral abnormalities, and no dysmorphic features at the otherend. Most patients fall into a broadly varying middle category with differing severities ofcore autism symptoms. There are no reliable genetic or physiological biomarkers of autismto further delineate idiopathic cases.
The Centers for Disease Control and Prevention estimate that 1 in 110 children in theUnited States have an ASD, and it is estimated to have an annual cost of more than $35billion.1 Increasing prevalence of diagnosis (1e2.6%) and the need for medical services acrossa normal life expectancy result in an extremely high financial and emotional burden, andunderscore the need for effective therapeutic interventions.2e8 The use of drugs for anxiety,depression, attention deficits and hyperactivity, impulsivity, seizures, sleep disruption andother psychiatric or neurological conditions, alone and in combination, is widespread inASD.9 None of these drugs treat the core symptoms of autism, nor are there any drugsapproved by the US Food and Drug Administration (FDA) for the treatment of the coresymptoms of autism. Two FDA-approved drugs for schizophrenia and bipolar depression,risperidone (Risperdal) and aripiprazole (Abilify), have been approved to treat a cluster ofadjunct autism symptoms referred to as irritability, but are plagued by adverse effectsincluding sedation, weight gain and metabolic disorders, and extrapyramidal symptoms.9
Thus, there is a profound unmet medical need in ASDs, and this review will highlight resultsfrom human functional neuroimaging studies in ASD and neurobiology research in geneticmodels of ASD, and how they converge as useful tools for forming translation research strat-egies for the development of ASD therapeutics.
1.2. Translational Research Definition
Translational research covers the breadth of activities that enable the efficient and effec-tive application of basic scientific findings into knowledge and studies that assess diseasesymptoms, progression, and therapeutic response in patient populations. Translationalapproaches span preclinical to clinical research, including animal models and experi-mental biology approaches in healthy humans that allow prediction of outcome inpatients. Central to this mission is the use of biomarkers and endpoints that enable theeffective testing of a proposed mechanism, selection of appropriate patients, and surro-gate measures of outcome in disease that increase the likelihood of detecting a relevantand robust signal. The discipline of translational medicine has become core to earlydrug development over the past decade, as scientists attempt to increase clinical successand facilitate target discovery through the generation of a more thorough understandingof disease-relevant targets and prediction of the impact on pathology in systems andcircuits.
Translational science is complicated by the difficulty in identifying biomarkers andendpoints that are measurable and relevant to disease in both preclinical models and inhumans. This is in large part due to the paucity of animal models that truly reflect humandisease, the lack of validated tools and methods that can be applied across species, andprohibitive costs associated with clinical experiments. For instance, ASDs are characterizedby distinct behavioral and cognitive dysfunctions that are not fully recapitulated in existing

9. TRANSLATIONAL NEUROIMAGING IN AUTISM SPECTRUM DISORDERS248
animal models. Furthermore, for those animal models in which there are sequelae potentiallyrelevant to outcome in patients, the biomarkers and assessment tools necessary to createtranslatable paradigms are not yet readily available. Human experimental biology para-digms can bridge this disconnect to some degree, by allowing for translation of basic neuralfunction between healthy animals and humans, and subsequent translation of neuralcircuitry during disease-relevant tasks from healthy volunteers to patients.
Functional imaging technologiesi (e.g. functional magnetic resonance imaging, fMRI; posi-tron emission tomography, PET; and single-photon emission computed tomography, SPECT)are tools of increasing value for application to translational science, as they enable the eval-uation of patterns of activation evoked by circuitry associated with functions that are analo-gous or homologous across species. In addition, the pharmacological signature ofmechanistic engagement is typically well preserved and detected with functional imaging,giving rise to potentially useful information about both on- and off-target actions of experi-mental drugs. In particular, fMRI provides enormous flexibility in the type of measures thatcan be obtained relevant to drug impact on brain function, including pharmacological MRI(PhMRI; direct effects of a drug on baseline hemodynamic signature), task-evoked MRI(changes in hemodynamic response to specific stimuli or behavioral tasks), and resting statefunctional connectivity (temporal correlations between specific brain regions in the absenceof any stimulus). Because PhMRI and resting state connectivity can often be assessed even inthe presence of anesthesia, these approaches are also amenable to use in animal models, thusproviding sensitive tools that can be used to assess drugetarget interactions across species.
2.0. CLINICAL IMAGING IN AUTISM SPECTRUM DISORDERS
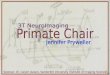
ASDs remain an entirely untapped area of investigation with regards to the application offunctional imaging for understanding the pharmacological action of drug intervention inpatient populations. While imaging has been increasingly used to probe the neurocircuitryand neural dysfunction underlying ASDs (Figure 9.1), these tools have not yet beenemployed in support of clinical drug development. Therefore, we will explore how imaginghas been applied to understand brain function in ASD patients, with a focus on the potentialfor use in drug development and translating from healthy volunteer clinical populations intopatients. In addition, we will review several genetic and nongenetic ASD animal modelsbecause of their critical role in elucidating mechanisms and brain circuits associated withASD risk genes and core behavioral symptoms (Figure 9.1), which will be vital for any trans-lational strategy.
There is considerable, but varying, evidence from structural MRI (sMRI) imaging studiesin ASD patients for whole brain and regionally specific volumetric abnormalities. The mostreplicated sMRI findings are volumetric increases in total brain, cerebellar hemispheres, and
iPlease refer to Wise in Chapter 1, Neuroimaging Modalities: Description, Comparisons, Strengths, and
Weaknesses; Brown in Chapter 2, Magnetic Resonance Imaging as a Tool for Modeling Drug Treatment of
Central Nervous System Disorders: Strengths and Weaknesses; and Schmidt et al. in Chapter 5, Positron
Emission Tomography in Alzheimer Disease: Diagnosis and Use as Biomarker Endpoints, in this volume for
detailed discussions of neuroimaging modalities.

Core symptoms: Social impairments Memory deficits Repetitive behaviors
A: Autistic patients vmPFCAmygdala
Fusiform gyrusOrbitofrontal cx (OFC)
Inferior frontal cxInferior occipital cx
Superior temporal sulcus
vmPFCCingulate cx
HippocampusAmygdala
Occipital cx Parietal cx
Anterior cingulate cx (ACC)Caudate putamen/Basal ganglia
Cerebellum
B: Animal models mPFCAmygdala
mPFCHippocampus
Amygdala
mPFCStriatum/Basal ganglia
A B
FIGURE 9.1 Brain circuits associated with autism spectrum disorder (ASD) pathophysiology: similarities in
human imaging and animal models of ASD. cx, cortex; inf, inferior; mPFC, medial prefrontal cortex; sup,superior; vmPFC, ventromedial prefrontal cortex.
2.0. CLINICAL IMAGING IN AUTISM SPECTRUM DISORDERS 249
the caudate nucleus, and reduced volumes in cortical thickness and corpus callosum.10e14
Similar abnormalities have been reported in animal models of ASD (discussed below), andindicate a clear role for translational imaging in further characterization of these brain abnor-malities. In addition, abnormal function and structure of frontotemporal and limbic networkswith social and pragmatic language deficits, of temporo-parieto-occipital networks withsyntactic-semantic language deficits, and of fronto-striato-cerebellar networks with repetitivebehaviors and restricted interests have been reported in autistic individuals.14,15 Over thepast two decades, functional imaging has been used in autistic populations to probe threebasic models of neural function:
(1) Emotional and social intelligence(2) Cognition and memory(3) Default (resting) networks.Each of these approaches has uncovered distinctive functional brain differences in ASD,
as compared to age- and gender-matched controls, including the identification of neuroana-tomical regions demonstrating consistent differences in activation levels under specific

9. TRANSLATIONAL NEUROIMAGING IN AUTISM SPECTRUM DISORDERS250
neurobehavioral tasks. These findings may be critical for customizing translational researchstrategies for ASD populations grouped by genetics or clinical presentation.
2.1. Emotional and Social Intelligence
Most functional imaging in ASDs has focused on emotional processing and indices ofsocial cognition because the core symptoms of autism include deficits in reciprocal socialinteraction and reduced empathy and emotional/social salience. The specific focus hasbeen on delineating circuitry underlying facial recognition and emotional salience (e.g. fusi-form cortical regions and the amygdaloid complex), in part because early studies identifieddeficits in the accurate perception of emotional content in facial expression.16e18 In high func-tioning autistic cases and individuals with Asperger syndrome, performance on a taskinvolving social intelligence (e.g. the Reading the Mind in the Eyes task aimed at identifyingmental or emotional state from the eyes of target face stimuli) during fMRI imaging revealeda distinct difference in the brain activation pattern within brain regions associated with socialintelligence, when compared to control subjects.19 In normal individuals, the emotion recog-nition task increased activation in the superior temporal gyrus and amygdala, with a lesserdegree of activation in some orbitofrontal cortical sites, whereas autistic or Asperger patientsshowed the highest amount of activation in the cortical and superior temporal regions, butnot within the amygdala or fusiform regions. The orbitofrontal cortex has previously beenidentified as a key site for accurately identifying emotional states, and the reported differ-ences in activation may underlie dysfunctional social emotional processing in ASDs.20
In addition, hypoactivity in response to happy versus neutral faces in a number of brainregions, including the fusiform region, is present in unaffected siblings of autistic patients,suggesting that patterns of neural function evoked by an emotional facial recognition taskmay be a sensitive index of risk and ASD endophenotype even in the absence of disease.21
The deficits in emotional recognition tasks shown by individuals with ASDs do notappear to be the result of reduced ability to visually process and recognize faces per se, asno deficits in performance are typically seen in response to control or nonemotional faces.22
Autism individuals also perform normally on gender recognition of faces, but show moreerrors when tasked to recognize faces according to emotional expression.17 This impairmentis associated with less activation in the inferior frontal and fusiform areas, suggesting thatemotion-specific processing is modulated by these regions. Likewise, there are no differ-ences in activation in major face-processing regions (i.e. fusiform areas and inferior occipitalgyrus) to neutral face stimuli.23 However, the same study revealed hypoactivity in a broaderdistributed network of regions associated with face processing, particularly those involvedwith the mirror neuron system (i.e. the amygdala, inferior frontal cortex, and superiortemporal sulcus). Significant hypoactivity in both the fusiform area and the amygdala hasalso been reported for exposure to dynamic emotional stimuli as compared with static facialimages in high-functioning autistics.24
Deficits in emotional recognition in ASD populations may not arise from an inability toattend to emotional stimuli appropriately, because ASD patients do not show deficits onbehavioral tests of emotional attention bias.25 Autism patients show performance equal tothat of controls in imitating or observing emotional faces, despite significant hypoactivityin the mirror neuron system of the inferior frontal gyrus.26 However, the cognitive strategies

2.0. CLINICAL IMAGING IN AUTISM SPECTRUM DISORDERS 251
by which autistics make emotion-relevant judgments may involve different underlyingneural circuitry, with more dependence upon right hemisphere amygdala and ventromedialprefrontal cortical coupling. In contrast to other studies showing reduced fusiform activationfor autistics, another study revealed increased activity in fusiform brain regions in anemotional facial stimulus task in autistic and control groups.27 In autistic individuals, theactivation in this regionwas higher for familiar than stranger faces, and included recruitmentof the right hemispheric amygdala only for familiar stimuli. Therefore, the emotional salienceof the faces being judged may impact the attentional state of the participant in a way thatcould translate into differential neural activation that may, in turn, enhance recognition ofemotionally significant faces.
Some evidence indicates that there is not an inherent difference in ASD patients in theaccuracy of emotional identification, but rather a reduction in the speed with which suchjudgments are made.28 In a task where participants were asked to perform an emotion-match perceptual task, an emotion-label linguistic task, or a nonemotional control task, therewere no differences in the accuracy across any of the tasks between autistic and normalparticipants. In contrast, there was an increase in the reaction time for the emotion-matchcondition in autistics that was accompanied by decreased activation in the fusiformcortical regions, although with the expected reductions in fusiform activation for theautistic group. Thus, clinical studies aimed at characterizing the effects of pharmacolog-ical intervention on outcome in ASDs need to include carefully chosen experimental para-digms and must account for the expected linkage between behavioral and neural circuitryeffects.
2.2. Cognition and Memory
While there is a general consensus that ASDs are often associated with deficient executivecontrol, reports of cognition and memory dysfunction have been inconsistent and are likelyto depend on the task or cognitive strategy being investigated.29 In a battery of cognitivetasks, ASD patients showed significant deficits only in list learning and object recognition;performance on nonverbal tasks and digit span were normal.27 In a review of the literatureevaluating executive function in ASDs, response inhibition and set shifting were the mostconsistently reported deficits.30 Very few studies have coupled functional imaging withcognitive testing in ASDs. In a verbal learning task, autistic participants remembered fewerwords from a list than normal controls, and this finding was associated with decreasedmetabolism in anterior and posterior cingulate gyri.31 There were no differences in activationin the hippocampus or amygdala, suggesting that this specific cognitive deficit is not repre-sentative of a larger, overarching dysfunction in memory or emotion processing. Laterstudies suggest that memory dysfunction in ASD may be more related to the strategyemployed to complete the task than to an underlying deficit in generalized cognitive ability.For example, autistic subjects perform comparably to normal controls on an n-back memorytask, but neural activation patterns as assessed with fMRI are more representative ofa strategy employing visual processing (occipital and inferior temporal regions) ratherthan verbal coding.32 Similarly, in a task testing the ability to process sentences with highand low levels of imagery, autistic participants showed looser connectivity among cortical

9. TRANSLATIONAL NEUROIMAGING IN AUTISM SPECTRUM DISORDERS252
regions, and a stronger activation of occipital and parietal imagery-related neural regionsunder both task conditions, as compared to typically developing individuals.33
Another potentially fruitful area for investigating the linkage between cognition andpatterns of neural activation in ASDs is in the area of Self versus Other reflection. A numberof investigators have delineated regions of the brain specifically associated with the selfconcept and internal forms of attentional focus.34 Self-reflective cognitive processing iscentered in the ventromedial prefrontal cortex (VMPFC) and is indicated by higher activityin this region during self-referential thinking,35,36 and differences in activation levels havebeen seen for self-judgments of positive and negative words,37 indicating a fairly fine degreeof detection for emotionally valenced stimuli. Similarly, there is reduced activation in theVMPFC and anterior cingulate cortex of autistic participants during Self versus Other refer-ential judgments, as well as during rest,38 suggesting that dysfunction in these regionscontributes to reduced attention to self-referential information. Individuals with an ASDalso show deficits in deictic shifting (i.e. a slower response and less accuracy in personalpronoun reversals), associated with reduced connectivity between frontal (insular) andposterior (precuneus) connectivity.39 More recent evidence has shown that the lack of distinc-tion between self and other in autistic individuals is probably due to atypical processing inthe VMPFC and the cingulate cortex.40 Differences in activation patterns for autistic subjectswere seen only in those brain regions important for self-referential processing, and not forthose involving judgments of others. Such distinct patterns of neural response coupledwith behavioral expression may represent a hallmark of ASD and a potential critical func-tional endpoint for testing therapeutic efficacy. However, its use in translational strategieswould be challenging because analogous behaviors and cognitive processes are not testablein lower preclinical species.
2.3. Default Networks
Patterns of activity in default mode networks (DMN) are emerging as potential indica-tors of ASD phenotypes and etiologies, and may be useful platforms for testing therapeuticinterventions. fMRI and diffusion tensor imaging (DTI) suggest that volumetric abnormal-ities are associated with abnormal functional, structural connectivity, and synchronizationwithin fronto-temporo-limbic, temporo-parieto-occipital, and fronto-striato-cerebellarnetworks.14,15,41,42 Impaired activity and intrinsic connectivity in the DMN were reportedin multiple brain structures such as the medial prefrontal cortex, posterior cingulate cortex,or precuneus,14 and limited magnetic resonance spectroscopy (MRS) studies have reporteddecreased N-acetylaspartate (NAA) in the gray matter of ASD patients.10 While the volumeand overall organization of resting state networks are similar in ASD and control subjects,looser connectivity of anterioreposterior networks have been reported in ASD.43 Thedecreased functional connectivity between medial prefrontal-precuneus and other DMNsis correlated with the degree of deficit in social and communication skills.44 Furthermore,the VMPFC and cingulate cortex show reduced activity levels in autistic subjects comparedto controls even at rest,38 and decreased connectivity between insular cortical regions withsomatosensory cortex and amygdala are seen in autistic individuals during the restingstate.45 These default network systems may represent circuitry underlying self-introspectionand emotional regulation,46 and an opportunity to explore the impact of therapeutic

2.0. CLINICAL IMAGING IN AUTISM SPECTRUM DISORDERS 253
intervention in a task-independent manner. Indeed, Silani and colleagues47 reporteddecreased activity in insular regions for autistic participants during self-reflection andemotional introspection. The task-independent nature of these emotionally relevant activa-tion patterns makes default network systems highly interesting as probes of pharmacolog-ical effects in drug development, and could become increasingly important if associationswith social emotional and communication impairment are reliably demonstrated. Connec-tivity in the DMN and brain metabolites in homologous brain structures needs to be inves-tigated in animal models of ASDs in order to more precisely target specific brain structuresand identify mechanisms underlying ASDs, and to provide valuable translationalapproaches for drug development.
2.4. Novel Analysis Approaches
Since the early 1990s, fMRI has become a viable research tool for investigating multipleaspects of normal and abnormal human brain function in vivo,48 including the alterationsin ASDs described above. Most fMRI analysis has examined task-driven responses voxelby voxel, including the studies described above, and can tell us where significant responsestake place and how strong (or significant) they are. These methods may suffer from a lossof power by virtue of the way they perform multiple comparison corrections49 andbecause they explicitly ignore intervoxel interactions. However, they can give us informa-tion about which groups of brain regions respond to given tasks and how these responsescan be changed by experimental manipulation, and thus have considerable value in thedevelopment of animal models and the early phases of drug testing. They can tell uswhat networks of brain regions are abnormal in their responses in conditions such asASDs (and thus which systems should be targeted in animals) and whether drugresponses are compatible with central nervous system (CNS) penetrance and functionaleffects.
These methods have proved extremely useful, but have been criticized because findingscan differ considerably between groups due to arbitrary thresholding of maps50 and a lackof power to detect small effects with reliability.ii
This renders interpretation difficult unless sufficient data are available to permit goodmeta-analysis. In a drug development context, this can mean that it may be difficult to deter-mine whether a particular candidate drug has modulated a response of interest. A furtherproblem of task-driven fMRI is that a single task will often not engage all the brain areasthat may be of interest for a particular condition. In response, it has become very commonto perform fMRI studies where no task is donedso-called resting state fMRI51dwhichmainly uses independent component analysis (ICA) to identify brain regions displayingsimilar time-dependent changes in activity. Some of the findings obtained in ASDs usingthis approach have been listed above. They are contributing to our understanding of brainnetwork behavior in ASD and will be valuable for assessing how this can be modulatedby drug intervention.
iiPlease refer to Schmidt et al. in Chapter 5, Positron Emission Tomography in Alzheimer Disease: Diagnosis
and Use as Biomarker Endpoints, in this volume for further discussion regarding mapping neuroimages to
standard maps.

9. TRANSLATIONAL NEUROIMAGING IN AUTISM SPECTRUM DISORDERS254
Mass-univariate task-driven fMRI analysis and task-independent ICA-based resting stateanalysis are effective tools for identifying which groups of brain regions show altered func-tion in given conditions, and will be useful for assessing how these alterations are modulatedby drug administration. These methods have been almost exclusively used for multisubject(group) level inference, but there is currently a major shift toward personalized medicine,52
which requires accurate personalized patient profiles. An analytic development in fMRIthat may aid this move to an individual-level focus is the increased use of machine learningor multivariate pattern-recognition techniques. These are now being used extensively forsingle-subject class prediction (e.g. diagnostic category and responder and nonresponder).53
These methods operate by training a computer program to determine class boundaries ina group of individuals so that subsequently analyzed single-subject test data samples canbe located relative to the boundary (i.e. they can be allocated to a class). The main reasonthat these methods can be substantially more effective in a predictive role than the traditionalmethods described above is that they use data from many regions or even the whole brain(rather than a single voxel) to characterize the state of an individual subject, thus providingmuchmore power to achieve useful single-subject classification. Research papers on the anal-ysis of structural brain imaging data have demonstrated considerable initial promise forautomatic detection of autism in individuals.54
Another potentially important use of machine learning lies in the area of preclinical anal-ysis of drug effects. During drug development, a major area of interest is identifying the CNSsite of action of novel therapeutics. This can be a difficult problemwhen the exact time courseof the drug effect is unknown. Normal methods of fMRI analysis (which depend on usingaccurate models of response to predict cerebral responses, and hence to determine whichbrain regions are responding) are then precluded or, at best, will suffer severe reductionsin power. Machine learning-based parameter estimation offers considerable improvementsin results (e.g. greater signal-to-noise ratios) as much more data containing useful informa-tion are included in the estimation process. This, in turn, increases sensitivity of responsedetection, leading to better characterization of responding regions and more effective useof animal models in the translational research process.
2.5. Application of Human Imaging in Autism SpectrumDisorder Translational Research
A clinical neuroimaging model for translational drug development in ASD should includean activation paradigm (behavioral, cognitive, or resting state) that is applicable to bothhealthy volunteer and patient populations; have an impact on discrete neural regions of acti-vation that are highly replicable across sites and studies; and be sensitive to acute pharma-cologic intervention. Social cognition, emotional, and learning and memory tasks areamenable to coupling with functional neuroimaging in humans, are easily administered topatient populations, and activate discrete neural systems that have been characterized inASD and typically developing individuals. However, there may be unique complicationsfor using some of the more validated tasks, including the use of emotion recognition in faces,which may be affected by strategic bias in ASD patients who employ unique visual process-ing strategies. These strategies are largely subconscious, and there is no evidence that onestrategy is more advantageous for overall performance. Without cognitive remediation there

2.0. CLINICAL IMAGING IN AUTISM SPECTRUM DISORDERS 255
would be very little incentive for an ASD patient to switch their strategy for making judg-ments, even if a pharmacotherapy increased their facility to do so. Thus, one might not seea discernible change in the recruitment of neural function in underserved brain regions,although the magnitude of activity in those regions might be altered by drug treatment.The impact of cognitive remediation on recognition strategies employed by ASD patientsis poorly defined, and may yet prove to be a fruitful method for assessing the effects of ther-apeutic intervention in ASD drug development.
Considering the inherent difficulties in translating pharmacodynamic endpoints frompreclinical models into humans, resting state networks might also prove to be a sensitiveprobe for assessing drug effects across species. Default network activity would probablybe translatable from healthy volunteers to patients with a low impact of cognitive andemotional skill level and strategy, as participants could serve as their own controls. Forexample, assessment of circuitry activation with fMRI during passive speech stimulationhas revealed hypoactivity in the superior temporal gyrus of autistic individuals and mayserve as an early diagnostic tool or biomarker to select patients and measure functionalresponse to pharmacological interventions.55 Pharmacological effects on potentially endo-phenotypic systems could be detected in the absence of task-related activation patternsand might enable greater sensitivity in comparing regional activation effects, as well asproviding a simple paradigm to promote translation from preclinical models where taskperformance may not be feasible during the functional imaging process.
The use of healthy volunteers to assess translation of pharmacological signatures in brainregions known to be important in the etiology of ASDs could provide appropriate bridgingfor determining the mechanistic activity and potential relevance of drugs in development.Of note are findings of neural activation patterns in healthy men and women in responseto oxytocin, a hypothalamic neuropeptide of growing interest for therapeutic interventionin ASDs. Kirsch and colleagues56 were the first to demonstrate functional changes in brainregions relevant to processing fear and social cognition of healthy male volunteers adminis-tered with intranasal oxytocin, showing both decreased activation and decreased coupling ofrelevant emotional and autonomic brain circuits centered on the amygdala. Oxytocin waslater shown to have marked effects on brain functionality in healthy men as a function ofcooperative behavior,57 with increases in activity of the caudate and increased connectivitybetween the amygdala and anterior insular regions under conditions of reciprocated cooper-ation. Likewise, emotional salience, another potentially important area associated with socialimpairment in ASDs, can be affected by treatment with oxytocin. Activity within the amyg-dala was significantly reduced following intranasal oxytocin administration in nulliparoushealthy volunteer women in response to the emotionally salient stimulus of infant laughter,58
with increased connectivity between the amygdala and brain regions associated with posi-tive emotional valence, including the orbitofrontal cortex. These results demonstrate thatoxytocin acts within the amygdala and brain circuits important for social cognition andemotional salience, and suggest that oxytocin may decrease negative emotional arousal bydampening amygdala activity, while simultaneously increasing incentive salience byenhancing connectivity in reward-related brain regions. Overall, the growing body of humanefficacy and imaging research with oxytocin may represent a powerful translational neuro-imaging paradigm for assessing (and potentially predicting) the therapeutic efficacy of noveldrug therapies in ASD populations.

9. TRANSLATIONAL NEUROIMAGING IN AUTISM SPECTRUM DISORDERS256
3.0. PRECLINICAL GENETIC MODELINGOF AUTISM SPECTRUM DISORDERS
For an effective translational drug development strategy, behavioral or cognitive para-digms and insight into the most relevant neural circuits should extend from preclinicalresearch and subsequent studies in healthy volunteer populations. At best, preclinicalmodels are useful for identifying brain circuits and molecular mechanisms associated withdisease, and for predicting therapeutic pharmacodynamic activity in humans. To improvethe probability of meeting these aims, and thereby facilitate a predictive translationalresearch strategy, it is essential to use techniques for assessing neural circuitry in vivo thatspan across species (as rodent behavior alone has not proved reliable in developing novelmedications for CNS diseases). The technical feasibility of directly assessing neural activationpatterns in animals during a behavioral task is rapidly evolving, but there is a current paucityof task-related in vivo physiology and neuroimaging work in ASD models. In the absence ofrobust evidence for quantitative and drug-responsive neurophysiological studies, thegrowing body of research on the impact of ASD risk genes on neurophysiology and behav-ioral phenotype in mouse models serves as a starting point for identifying potential braincircuits that might be the focus of future in vivo functional activity studies. In the followingsection, we review several of the most extensively characterized genetic mouse models ofASDs and the commonly used BTBR mouse model of core behavioral symptoms of autism,with a focus on neurobiological and behavioral findings that point to brain circuits that mightbe useful in a translational research strategy.iii
These findings are summarized in Table 9.1.
3.1. Rare Variants Underlying Syndromic Autism Spectrum Disorders
3.1.1. FMR1 Models
Fragile X syndrome (FXS) is the most common inherited form of intellectual disability andprimarily affects males. It is also recognized as the leading single-gene cause of autism (2e6%of cases), as comorbidity is observed in 25e50% of FXS patients.59,60 Shared symptomsinclude the core autistic deficits in communication, social interaction, and repetitive behav-iors, as well as social avoidance and anxiety, lack of eye contact, ADHD, and seizures,61 butFXS is distinguished by additional clinical features such as craniofacial abnormalities andmacroorchidism. FXS results from a trinucleotide expansion (> 200 CGG repeats) in theFMR1 (fragile X mental retardation 1) gene that prevents expression of fragile X mental retar-dation protein (FMRP), and carriers of 50e200 repeats can exhibit autistic behaviors withoutintellectual disability.62
Identification of the FXS gene in 1991 led to the rapid generation of a mouse model of FXS[Fmr1 knockout (KO) mice], and additional mouse and rat models have followed.63e66 Fmr1KO mice exhibit physical, morphological, and functional abnormalities that are consistent
iiiFor further discussion of the use of neuroimaging and genetic rodent models of neuropsychiatric disorders,
please refer to Steckler and Salvadore in Chapter 7, Neuroimaging as a Translational Tool in Animal and
Human Models of Schizophrenia, in this volume.

TABLE 9.1 Neurobiological and Behavioral Characteristics of Mouse Models of Autism Spectrum Disorder Genetics andCore Behavioral Symptoms
Model Neuroanatomical changes Behaviors relevant to core autism symptoms Additional deficits
Neurophysiology
aberrations
Potential
targets
Finding Region Social Repetitive Communication Finding Region
FMR1 KO Increased
dendrite density
CTX Strain-
dependent
deficits
Impaired HPC-
depend. memory,
seizures, PPI deficit,
hyperactivity, anxiety
Hyperexcitability,
Impaired Ltp
Increased LTD
Decreased LTP
Increased LTD
CX
HPC
AMYG
CRB
mGluR1/5,
GABAB
PTEN
cond. KO
(forebra in)
General
neuronal
hypertrophy
Whole brain Decreased
interaction,
impaired
recognition
Macrocephaly,
seizures,
impaired spatial
memory,
hyperactivity,
anxiety, PPI deficit
Hyperexctability HPC mTOR, S6K
MeCP2 KO Reduced
volume
and brain
weight
Whole brain Model-
dependent
deficits
Forepaw
rubbing,
hindlimb
clasping (model-
dependent)
Model-
dependent
deficits
Tremors, seizures,
motor
dysfunction,
breathing
abnormalities,
learning and
memory deficits
Decreased
LTP, reduced
EPSC
size
CX,
HPC
BDNF,
5-HT, GABA,
MECP2
NLGN4 KO Reduced
volume
CRB,
brainstem
Decreased
interaction,
impaired
recognition
Decreased
USVs (adults)
NLGN3 KO Reduced
volume
Whole brain Impaired
recognition
Decreased
USVs (adults)
Impaired
olfaction,
hyperactivity
NLGN3 R451C
mutant
Decreased
interacting
(strain-
dependent)
Decreased
USVs (pups)
Reduced
acoustic startle
Increased
inhibition
Increased
excitation,
Enhanced LTP
CX
HPC
NRXN 1
alpha KO
Increased self-
grooming
Increased
startle, reduced PPI
Reduced
excitation
HPC
CNTNAP2 KO Neuronal
migration
defects, Inhib.
interneuron loss
CTX Decreased
interaction
Increased self-
grooming and
perseveration
Decreased
USVs (pups)
Seizures, sensory
hypersensitivity,
hyperactivity
Abnormal
neuronal
synchrony
CX D2, 5-HT2C/2A
(Continued)
3.0.PRECLIN
ICALGENETIC
MODELIN
GOFAUTISM
SPECTRUM
DISORDERS
257

TABLE 9.1 Neurobiological and Behavioral Characteristics of Mouse Models of Autism Spectrum Disorder Genetics andCore Behavioral Symptomsdcont’d
Model Neuroanatomical changes Behaviors relevant to core autism symptoms Additional deficits
Neurophysiology
aberrations
Potential
targets
Finding Region Social Repetitive Communication Finding Region
Shank3 KO Increased
volume
Caudate Decreased
interaction
Increased self-
grooming,
stereotyped
object
exploration
Decreased
USVs (adults)
Anxiety ,
self-injury,
memory
impairment
Reduced
excitation
and LTP
HPC,
Striatum
mGluR5
Shank3 C-term.
deletion
Context-specific
abnormalities
Increased
latency to
vocalize (adults)
Increased
aggression
Reduced LTD HPC, CX mGluR5
Chrom 15q 11 -
13 paternal
dup
Decreased
approach
Increased
USVs (pups)
Reversal learning
impairment,
decreased
exploratory
activity, increased
freezing in fear
conditioning
5-HT2C/
2Areceptors
UBE3a CNV
(3x normal
expression)
Decreased
approach
Increased self-
grooming
Decreased USVs
(adults)
Decreased EPSC,
mEPSC amplitude
and frequency,
postsynaptic
excitability,
probability of
glutamate release,
and glutamate in
synaptic cleft
CX Glutamatergic
system
BTBR Agenesis of the
corpus
callosum,
reduced adult
neurogenesis
Corpus
callosum,
dentate
gyrus
Decreased
approach,
interaction,
decreased
juvenile play,
impaired social
transmission of
food preference
Increased self-
grooming,
increased bar
biting, rigid
object
exploration
Decreased USVs
(adults and
pups)
Learning
and memory
deficits
mGluR5,
GABAA, 5-HT
AMYG, amygdala; chrom, chromosome; CNV, copy number variation; cond., conditional; CRB, cerebellum; CX, cortex; dup, duplication; EPSC, excitatory postsynaptic
current; Fmr1, fragile X mental retardation 1; HPC, hippocampus; KO, knockout; LTD, long-term depression; LTP, long-term potentiation; Mecp2, methyl CpG binding protein 2;
Nlgn3, neuroligin 3; Nlgn4, neuroligin 4; Nrxn1a, neurexin-1a; PPI, prepulse inhibition; PTEN, phosphatase and tensin homolog; Shank3, SH3 and multiple ankyrin repeat domains 3;
Ube3a, ubiquitin protein ligase E3A; USV, ultrasonic vocalizations.
9.TRANSLATIO
NALNEUROIM
AGIN
GIN
AUTISM
SPECTRUM
DISORDERS
258

3.0. PRECLINICAL GENETIC MODELING OF AUTISM SPECTRUM DISORDERS 259
with FXS symptoms, including increased density of long and immature dendritic spines incortical neurons and enlarged testicles.67e70 However, in contrast to the moderate to severeintellectual disability and autistic behaviors observed in FXS patients, the behavioral deficitsin Fmr1 KO mice are comparatively mild and highly variable. Impairments in spatialmemory paradigms such as the Morris water maze have been reported, primarily duringreversal learning,66,71 and may indicate a deficit in cognitive flexibility that relates to theautistic feature of insistence on sameness or adherence to a learned routine.72 Deficits havealso been observed in other memory tests that require intact hippocampal function, suggest-ing the hippocampus may be particularly affected by loss of FMRP.73e77
Behavioral abnormalities in Fmr1 KO mice are also consistent with a subset of autisticsymptoms, including increased repetitive behaviors, hyperactivity, attention deficits, impul-sivity, and resistance to change.74,78e80 Among the most common findings are altered sensi-tivities to sensory stimuli (e.g. audiogenic seizure, pain responses, and startle) that may relateto seizures and self-injurious behaviors in autism and FXS.74,81e84 Both increases anddecreases in social interactions and anxiety-like behaviors have been reported in Fmr1 KOmice,21,79,80,85e89 but may be confounded by increased exploratory activity and hyperac-tivity.66,74,79,90 The lack of consistent behavioral deficits in Fmr1 KO mice could be due tothe fact that the effects of Fmr1 deletion are highly influenced by genetic background.21,73
Some autistic behaviors are only observed in a single strain, and in some cases differentstrains show opposite phenotypes. A second factor is the possibility of compensation forloss of FMRP by functionally redundant proteins, such as the paralogues FXR1P andFXR2P, which may compensate to a lesser extent in humans.74 Indeed, a study found thatcrossing Fmr1 KO mice with null mutants for the Fxr2 gene exaggerated several behavioraldeficits, suggesting partial overlap in function.83
Despite these caveats, disease-relevant behavioral deficits in Fmr1 KO mice suggest thatthere may be similar dysfunctions in brain structures that mediate learning and memory,sensory modalities, and emotional responses. Circuit defects in Fmr1 KO mice includesynaptic plasticity within the cerebellum, hippocampus, amygdala, and cortex, and suggestalterations in both excitatory and inhibitory neurotransmitter systems. Studies have repeat-edly found increased long-term depression (LTD) in the hippocampus and cerebellum thatdepends on activation of group1 metabotropic glutamate receptors (mGluR1 andmGluR5).
91e96 In contrast, long-term potentiation (LTP) was reduced in the amygdala,75,97
anterior cingulate, and somatosensory cortex, and hyperexcitability was found in bothsomatosensory and barrel cortices, which suggests a widespread loss of feedback inhibitionin the neocortex of Fmr1 KO mice.75,98,99 These electrophysiological changes may beexplained, in part, by alterations in the expression or composition of receptors for glutamateand g-aminobutyric acid (GABA), and decreased expression of GABAA and GABAB recep-tors (for review see100), as well as GluR1, have been observed in Fmr1 KO mice. Alterationsin these receptors are thought to shift the balance between the activity of excitatory and inhib-itory neurotransmission, andmay directly contribute to symptoms of FXS and autism such asseizure and cognitive impairment.98,99,101,102
While many of the electrophysiological and protein expression changes observed in Fmr1KO mice have not been confirmed in humans, they do highlight specific circuits and neuro-transmitter systems as potential sites for therapeutic intervention. Based on preclinical obser-vations such as those described above, two leading theories have emerged regarding the

9. TRANSLATIONAL NEUROIMAGING IN AUTISM SPECTRUM DISORDERS260
effective treatment of symptoms of FXS and autism by targeting mGlu and GABA receptors(for review see100,103). mGluR5 receptor antagonists have been shown to reverse autism-related behaviors such as seizures, hyperactivity, and anxiety in Fmr1 KO mice, and prom-ising results were reported in a small clinical trial with an mGluR5 antagonist in FXSpatients.104e106 Similarly, a GABAB receptor agonist was found to reduce seizures in Fmr1KO mice, and trials are currently ongoing for treatment of ASDs with the GABAB agonist,R-baclofen.107 In addition to these targets, alternative therapies such as lithium have beenshown in preclinical studies to normalize hyperactivity, social interaction, and learning defi-cits in Fmr1 KO mice.108
Together, these studies show that Fmr1 KO mice exhibit behavioral abnormalities acrossa range of domains that correspond to some of the core and comorbid features of autism,but the degree of impairment is highly dependent on the background strain and themethod of interrogation. Their value as a translational tool for studying defects insynaptic transmission that could underlie aspects of ASDs has been demonstrated, inpart, by the identification of several molecular targets for putative therapeutic interven-tions currently in the clinic. It is anticipated that future brain imaging studies in Fmr1KO mice may reveal additional circuit defects or novel biomarkers that can be directlyassessed in autistic patients.
3.1.2. MECP2/Rett Syndrome Models
Mutations in the X-linked geneMECP2 (methyl CpG binding protein 2) cause Rett syndrome,a progressive pervasive developmental disorder primarily affecting girls.109 Rett syndromepatients develop normally through 6e18months of age, after which patients show a period ofprecipitous regression, losing skills inmanyareas such as social interaction and communication.The syndrome is characterized by repetitive movements such as hand clasping or wringing,motor dysfunction, intellectual disability, breathing problems, and autism symptoms.110e113
Several mouse models of Rett syndrome have been created and include KO,114e116 trunca-tions,117,118 and overexpressing mice.119 Deletion models have been extensively reviewedelsewhere;110,111 they recapitulate features of Rett syndrome, including hindlimb clasping,tremors, seizures, motor dysfunction, breathing abnormalities and/or learning and memorydeficits (social abnormalities118,120 andeffects oncommunicationare less consistent121,122).Over-expression can bemanifested as symptoms similar to the loss of functionmutations in humans,and has been shown to cause related behavioral deficits in rodents,123 suggesting that preciseregulation ofMECP2 is necessary for normal neuronal function.
Studies using cell-type and temporally specific disruption ofMecp2 have been used to assessthe underlying neurobiological mechanisms associated with specific behavioral symptoms,110
and may point to target regions for imaging in patients for translational research purposes. Amodel lackingMecp2 only in GABAergic interneurons120 has a similar phenotype to that of theconstitutive KO, whereas forebrain interneuron-specific KO abolishes breathing abnormalitiesbut retains other Rett-like symptoms. Neurons in cortical layers 2 and 3 and the striatumshowed a 50% reduction in intracellular GABA and reduced expression of Gad1 and Gad2(glutamate decarboxylase 1 and 2) transcripts, resulting in decreased mini inhibitory post-synaptic current amplitude and charge. These findings implicate GABAergic dysfunction inthe forebrain in Mecp2-related repetitive movement disorders, and in the hindbrain inbreathing abnormalities. Consistent with these findings, treatment with NO-711 (a GABA

3.0. PRECLINICAL GENETIC MODELING OF AUTISM SPECTRUM DISORDERS 261
reuptake blocker) has a beneficial effect on breathing difficulties inMecp2KOmice,124 andmaypoint to the use of GABA receptor PET imaging within brain regions regulating breathing andcharacterization of breathing phenotype as endpoints in a drug development translationalresearch strategy in some Rett syndrome patients. In contrast, a translational experimentalmedicine approach targeting repetitive behaviors might focus on forebrain regions and,in addition to GABAergic neurons, to glutamatergic corticostriatal circuits implicated by otherautism risk genes.125
There are also potential roles for BDNF (brain-derivedneurotrophic factor) ,126 norepineph-rine,127 and serotonin in Rett syndrome symptoms that have been reviewed elsewhere,110,123
which upon further validation may implicate additional brain circuits to drive a translationalimaging strategy. Perhapsmost importantly, reactivation ofMecp2 in the adult animal is suffi-cient to reverse some deficits and improve survival,128 and critically shows that Mecp2 hasa key function in mature neurons and that rescue in the developed state is possible.112 Anexperimentalmedicine approach to restoreMECP2expression in adultRett syndromepatientsand to reliably evaluate functional impact is desperately needed.
3.1.3. PTEN Models
PTEN (phosphatase and tensin homolog) is a lipid phosphatase and tumor suppressor genethat is most commonly associated with a broad range of cancers, but has also been implicatedin variants of autism in which patients have pronounced macrocephaly, and in syndromicautism associated with Bannayan-Riley-Ruvalcaba and Proteus syndromes, and Cowdendisease.129e134 Although a causal association of PTEN in nonsyndromic autism has notbeen firmly established, mouse models of PTEN have been used to understand pathogenicfeatures that may contribute to the development of autism, and to test putative drug thera-pies for autistic symptoms.
Homozygous deletion of Pten in mice results in embryonic lethality, whereas heterozy-gotes show deficits in social behaviors (females only)135 and an increased incidence ofcancer.136e138 Because the incidence of cancer was not increased in the brain, mice weregenerated to delete Pten selectively from the brain; these mice exhibited features found inpatients with PTEN mutations, such as seizures and brain hypertrophy.139 Interestingly,many of the symptoms of PTEN-associated ASDs were also observed when Ptenwas deletedonly frommature neurons in the cortex and hippocampus.140 These conditional PtenKOmice(cPten KO) showed decreased social interactions and recognition, learning and memoryimpairments, hyperactivity, seizures, prepulse inhibition deficits, and increased anxiety-like behaviors and startle responses. Macrocephaly was also observed, and appeared to bedue to general neuronal hypertrophy, as evidenced by increased soma and axon size, thickerdendrites with denser spines, and larger projection fields. The seizures and dendritic spinechanges in these mice suggest increased excitatory transmission, and a shift toward increasedexcitation was observed following short hairpin (sh)RNA-mediated knockdown of Pten inthe hippocampus.141 Together, these data demonstrate that deletion of Pten from corticaland hippocampal neurons is sufficient to produce several ASD-related behaviors, andsuggest that one or both of these regions may be critical substrates for similar deficits inautistic patients.
PTEN is part of a molecular signaling pathway that includes additional molecules associ-ated with ASD such as NF1 (neurofibromytosis type 1) and TSC2 (tuberous sclerosis complex

9. TRANSLATIONAL NEUROIMAGING IN AUTISM SPECTRUM DISORDERS262
2; for review see142). A central molecule in this pathway is the serine/threonine-protein kinasemTOR (mammalian target of rapamycin), a downstream effector of PTEN that can be inhibitedby the drug rapamycin. Rapamycin (sirolimus, Rapamune) is used to treat certain cancers, andhas also been proposed as a putative treatment for ASDs associated with altered mTORsignaling. Preclinical studies in cPten KO mice support this idea, as treatment for 1e2weekswas found to reduce seizures, and longer treatments (4e6weeks) reduced macrocephaly andnormalized deficits in social interaction and anxiety-like behaviors.143,144 Importantly, theseeffects were observed even when administration began in juvenile or adult animals; thus,mTOR inhibitors may be an effective treatment strategy for autistic patients with defects inPTEN or related mTOR pathway genes.
Since the early 2000s, genetic association studies have identified defects in a multitude ofgenes that increase risk for ASD, but each is associated with only a small percentage of cases.Despite this genetic heterogeneity, the functions of various risk genes appear to converge ona few key pathways and processes, suggesting that ASDs may result from common mecha-nisms. One of the leading mechanisms involves synaptic dysfunction resulting from defectsin synapse formation, specification, maturation, and regulation. Several ASD-associatedgenes encode proteins that localize to presynaptic or postsynaptic sites, and serve as struc-tural bridges across the synaptic cleft or as scaffolding proteins that tether neurotransmitterrelease or receptor complexes to the cytoskeleton.145,146 In the next section we will focus ondiscussing key animal models of autism that involve synaptic proteins, and exhibit behav-ioral deficits that are similar to symptoms of autism.
3.1.4. NLGN and NRXN Models
Among the first synaptic proteins to be associated with ASD are those belonging to theNLGN (neuroligin) and NRXN (neurexin) gene families. These are cell adhesion moleculesthat support synaptic structure and function throughout the brain, and may thus contributeto maintaining a critical balance between excitatory and inhibitory activity.147,148 Neuroliginsinteract with neurexins anchored to presynaptic membranes and with a number of postsyn-aptic scaffolding proteins, and mutations in genes that encode several of these postsynapticproteins have also been linked to ASDs.145,146
There are four neuroligin genes in mammals and a fifth that is specific to humans,145 andASD-associated mutations in neuroligins 3 and 4 prompted the creation of some of the firstmouse models specifically for autism.149 Deletion of Nlgn4 in mice (NLGN4 KO) results inbehavioral abnormalities related to at least two core domains of autism, including a decreasein social interactions and recognition,150 reduced aggression in a resident intruder paradigm,and abnormal vocal responses in males during exposure to a female in estrus.150 MRI volu-metric studies showed an overall reduction of brain size, particularly in the cerebellum andbrainstem, but this was not associated with broad behavioral impairments as these mice werenormal in standard tests of locomotor activity, anxiety-like behavior, sensory functions, andlearning and memory.
The function of NLGN3 (neuroligin-3) has been examined using two different strategies:one that eliminates expression (NLGN3 KO mice) and another that introduces a rare muta-tion found in humans with ASDs that alters a single amino acid (Nlgn3R451C). Similar toNLGN4 KO mice, deletion of NLGN3 caused a reduction in brain volume as measured byMRI,151 and both KO and mutant mice152 exhibit deficits in vocal communication. Abnormal

3.0. PRECLINICAL GENETIC MODELING OF AUTISM SPECTRUM DISORDERS 263
social behaviors, however, appear to be subtle in KO mice and controversial in mutant mice.For example, NLGN3 KO mice showed normal levels of social interaction, but had a specificimpairment in social recognition that may be due to reduced olfactory function (smell iscrucial for identification in mice). Social behaviors in NLGN3R451C mutants are more difficultto interpret: one study showed a subtle reduction in social interactions,153 whereas a laterstudy reported normal social interaction but impaired recognition.154 Moreover, a secondline of NLGN3R451C mutants was examined in a thorough test battery that included testsfor core autism behaviors, as well as tests for memory, anxiety, sensory modalities, locomotoractivity, and resistance to change.152 Although both male and female mice were examined atseveral ages, they were surprisingly normal in almost all measures. Together, these studiessuggest that both NLGN3 and NLGN4 influence communication behaviors in mice thatmay be relevant to autism, whereas social behaviors are more clearly impacted by deletionof Nlgn4. NLGN3 may also play a unique role in hippocampal function, as improved perfor-mance in the Morris water maze was found in Nlgn3 KO mice and in one of the Nlgn3R451C
mutant lines,153 but not the other.152
It has been suggested that Nlgn3R451C mutants exhibit a more severe phenotype than doNlgn3 KO mice, owing to a gain of function that impacts synaptic transmission. Indeed,increased dendritic branching, elevated NR2B (glutamate/NMDA receptor subunit ε2)expression, and enhanced excitatory transmission were found in the hippocampus of bothNlgn3R451C mutant lines, but not in Nlgn3 KO mice.154 Interestingly, mutants also showeda significant increase in gephyrin and GABA, and stronger inhibitory synapses in the somato-sensory cortex. While it is unknown whether humans with this mutation exhibit similarchanges, the fact that a single defective gene can have opposite effects on neurotransmissionin different brain regions has broader implications for putative drug therapies. For example,the excessive inhibition in the cortex of Nlgn3R451C mice suggests a strategy aimed atreducing inhibitory neurotransmission, but this could exacerbate the increased excitatorydrive in the hippocampus. In the extreme case, a drug that corrects one behavioral deficitmay worsen another. Although attempts to normalize deficits in Nlgn3R451C mice withdrug treatments have not yet been reported, they appear to be a suitable preclinical modelin which to test this theory.
Defects in neurexin genes have been found in several genetic studies and further supportsynaptic dysfunction as a common mechanism underlying ASD.155e165 There are three neu-rexin genes in mammals and each drives expression of an a and b neurexin isoform viadistinct promoters, but alternative splicing may result in thousands of different protein iso-forms.166 In general, neurexins promote synapse formation and stability through trans-synaptic interaction with neuroligins, and specific neurexineneuroligin isoform bindingmay help to specify postsynaptic differentiation. Disruption of these interactions maycontribute to autism by causing a shift in the balance between excitatory and inhibitorysignaling.167,168
Both the a and b forms of neurexin-1 have been implicated in ASD, but the strongest asso-ciation thus far is with neurexin-1a, encoded byNRXN1. To determine if deletion ofNrxn1 inmice produced behavioral changes relevant to autism, KO mice were examined in fourdifferent tests of social interaction, but no abnormalities were observed.169 However,impaired nest building in the home cage suggested alterations in dopaminergic functionthat could be relevant to social deficits in autism.170 In addition, Nrxn1 KO mice exhibited

9. TRANSLATIONAL NEUROIMAGING IN AUTISM SPECTRUM DISORDERS264
a marked increase in self-grooming behaviors, which could indicate a change in corticostria-tal circuit activity, and may relate to ritualistic or stereotyped behavioral patterns in autism.
As with Nlgn3R451C mice, deletion of Nrxn1 produced alterations in synaptic transmissionin the hippocampal CA1 region, but in this case excitatory transmission was reduced in bothsingle-cell and field recordings, and was independent of changes in inhibitory transmissionor receptor levels.169 Surprisingly, Nrxn1 KO mice were normal in the Morris water maze,suggesting that reduced neurotransmission in the hippocampus did not significantly affectspatial memory. These mice were also normal in tests for anxiety and hyperactivity, butshowed improved motor learning in the rotarod test, as well as a small increase in acousticstartle responses and a large decrease in prepulse inhibition, which indicate deficits in senso-rimotor gating. Because similar behaviors were observed in Nlgn3R451C mice,152 synapticinteractions between neurexin and neuroligin may be particularly important for motorlearning and sensorimotor gating.
Overall, these studies indicate that deletion ormutation of neuroligin andneurexin genes inmice can produce behavioral changes that are analogous to core features of ASDs. The robustimpairment of social behaviors and vocal responses in Nlgn4 KO mice suggests similar genefunctions in mice and humans, and supports the validity of these mice as a model of autism.The utility of models that involve NLGN3 and neurexin-1a is less clear, owing both to themilder phenotype ofNlgn3 andNrxn1KOmice in tests for core autistic features, and conflict-ing reports regarding behavioral deficits in different Nlgn3R451C mutants. However, thechanges in synaptic transmission observed in Nlgn3R451C mice provide important insightsregarding the role of NLGN3 in synaptic function, and suggest specific neurotransmittersystems that could be targeted by novel therapies for some forms of ASD.
3.1.5. CNTNAP2 Gene
Mutations in the CNTNAP2 (contactin associated protein-like 2) gene are associated withautism and cortical dysplasia-focal epilepsy syndrome (CDFE), a rare ASD variant thatproduces severe impairments, including seizures, intellectual disability, language impair-ments, and autism symptoms.171e176 The protein encoded by CNTNAP2 is involved inneuroneglia interactions and clustering of potassium channels on myelinated axons, butmay play an additional role in neuronal migration during brain development.176,177 Consis-tent with these findings, Cntnap2 KO mice exhibit migration defects in cortical projectionneurons that resemble defects in CDFE patients.178 In addition, behavioral characterizationof Cntnap2 KO mice revealed numerous autism-like traits, as well as deficits observed inseveral other mouse models of autism. One of the most striking impairments was the induc-tion of seizures in adult animals upon routine handling, and may be related to a significantloss of paraventricular thalamic nucleus (anterior)-positive interneurons in multiple brainregions.178
Cntnap2 KO mice exhibit spatial learning and memory deficits specifically in the reversalphase of theMorris water maze, improved performance in the rotarod test, hyperactivity, andincreased sensitivity to sensory stimuli. With respect to core autistic behaviors, Cntnap2 KOmice exhibit an increase in perseverative alternations in the T-maze and abnormally repeti-tive self-grooming behavior. Abnormal social behaviors were observed in both juvenileand adult mice, and vocal communication was reduced in pups throughout early postnataldevelopment. The authors attempted to reverse behavioral deficits in Cntnap2 KO mice with

3.0. PRECLINICAL GENETIC MODELING OF AUTISM SPECTRUM DISORDERS 265
risperidone, an antipsychotic used to treat irritability in autistic patients. Although social andcommunication deficits were not reported to be altered by risperidone, treatment for7e10 days normalized repetitive grooming and perseverative behaviors, nest-buildingimpairments, and hyperactivity.
Electrophysiological studies in these mice have not yet been reported, but the reduction ofinhibitory interneurons and incidence of seizures suggest that additional deficits could benormalized by drugs that enhance GABAergic neurotransmission or attenuate glutamatergicsignaling. One logical experimental medicine approach in cortical dysplasiaefocal epilepsyand autism patients with CNTNAP2mutations may include focusing on patients with a well-characterized seizure phenotype, and the use of quantifiable electrophysiological and behav-ioral endpoints, rather than functional neuroimaging, to assess therapeutic response totreatment.
3.1.6. SHANK Gene Models
The SHANK (SH3 and multiple ankyrin repeat domains) gene family encodes three homolo-gous proteins (Shanks 1e3) that localize to dendrites of glutamatergic synapses throughoutthe brain, and serve as scaffolding proteins in the postsynaptic density.179 Multiple studiesindicate that mutations in Shank2 and Shank3 are associated with rare variants of ASD,including chromosome 22q13 deletion syndrome, and it has been hypothesized that defectsin Shank proteins contribute to ASDs by altering synaptic stability and maturation duringneuronal development.157,179e184 Studies thus far have not implicated the SHANK1 gene inautism, and the effects of deletion in mice are largely consistent with this inter-pretation.185e187 In contrast, several groups have independently created Shank3 mutantmice and each line exhibits some degree of behavioral abnormality that is reminiscent ofautistic deficits.
Heterozygous deletion of the ankyrin repeat domain of Shank3 resulted in a reductionof reciprocal social interactions and fewer vocalizations during free exploration tests, butnormal levels of interest for a caged conspecific or unfamiliar social odors.188 A reductionof GluR1 immunoreactivity in the hippocampus and impaired dendritic spine remodelingindicated defects in glutamatergic transmission and synaptic plasticity. Accordingly,these mice exhibited a decrease in the amplitude of miniature excitatory postsynapticcurrents (mEPSCs) and reduced LTP in the CA1 region, but no significant effect onLTD. In a separate mouse line, heterozygous deletion of the C-terminal region of Shank3found in autistic patients189 nearly eliminated protein from cortical synapses, and reducedexpression of the NR1 subunit of the NMDA receptor. These mice showed deficits inNMDA-dependent plasticity in the cortex and hippocampus, and increased mGluR-dependent LTD analogous to observations in Fmr1 KO mice. Behavioral tests revealeddelayed vocalizations and a slight reduction of social interaction that was confoundedby a pronounced increase in aggressive attacks. Surprisingly, these mice spent moretime investigating an enclosed male stimulus mouse. Thus, in comparison to other Shank3mutant mice the C-terminal deletion mutants have a distinct phenotype with unclear rele-vance to autism.
In general, mice with homozygous Shank3 mutations exhibit a more severe phenotypeand deficits that resemble multiple autistic traits. In one study, mutant mice showed notonly a lack of social interaction but also evidence for social aversion or anxiety125 and

9. TRANSLATIONAL NEUROIMAGING IN AUTISM SPECTRUM DISORDERS266
additional behaviors relevant to autism. These included seizures, increased self-grooming,and self-injurious behaviors that manifest as skin lesions in about one-third of the mice andwere even more pronounced in mating females. The excessive grooming suggested defectsin corticostriatal function, and analysis of this region revealed increased spine density onmedium spiny neurons, and a reduction in postsynaptic density proteins and glutamatereceptor subunits that corresponded to reduced glutamatergic activity in corticostriatalsynapses. Interestingly, there was also a significant enlargement of the caudate, as measuredby MRI, that has similarly been found in autistic patients.190 Mice with homozygous dele-tion of the Shank3 ankyrin repeat domain also exhibited multiple autism-related behaviorsthat included reduced social interaction, changes in the number and complexity of vocali-zations, and increased repetitive behaviors such as increased self-grooming and stereotypedexploration of a novel object in the home cage.191 Similar to other Shank3 mutants, thesemice had reduced levels of several postsynaptic density proteins and AMPA receptorsubunits, morphological changes in dendritic spines, and altered synaptic plasticity (LTP)in the hippocampus, and were impaired in several tests of hippocampal-dependentmemory.
In summary, evidence from four different Shank3 mutants supports a role for this proteinin each of the core behaviors that characterize autism. It is often the case that animal modelsrequire a more extreme genotypic insult to express a disease-like phenotype, and for disor-ders like autism that impact complex behaviors this may also be due to limitations in thesensitivity of standard behavioral assays to detect subtle impairments. In this context, it isnotable that the range and severity of deficits is generally greater in homozygous mutants.While this limits the construct validity of homozygous mutants that do not accurately modelhaploinsufficiency in humans, these mice exhibit synaptic defects in the cortex, hippo-campus, and striatum that could be useful in designing and evaluating novel treatmentsfor ASDs. Moreover, one Shank3 mutant showed a volumetric change in the caudate thatwas also observed in autistic patients, and could therefore be used as a translational measureto bridge the gap between preclinical and clinical studies.
3.2. Mouse Models of 15q11e13 Chromosomal Abnormalities
Duplications and deletions of chromosome 15q11e13 are among the most commonlyobserved mutations associated with ASDs, and are present in approximately 1e3% ofpatients.192 Mutations in individual genes within the 15q11e13 region cause distinct neu-rodevelopmental disorders, including Angelman syndrome [deletion of the maternallyimprinted UBE3A (ubiquitin protein ligase E3A) gene] 193 and Prader-Willi syndrome(paternal UBE3A deletions).194 The first mouse model of a 15q11e13 disorder was gener-ated by duplicating a syntenic region on mouse chromosome 7.195 Gene expression anal-ysis of mice with maternal and paternal duplications (matDup, patDup) showed theexpected doubling of maternally imprinted Ube3a or paternally imprinted genes [e.g.Ndn (necdin) and Snrpn (small nuclear ribonucleoprotein polypeptide N)], respectively, anda 1.5-fold increase in biallelic genes [e.g. Gabra5, Gabrb3, and Gabrg3 (a5, b3, and g3subunits of the GABA A receptor), and Herc2 (HECT and RLD domain containing E3 ubiquitinprotein ligase 2)]. Curiously, matDup mice seemed to show an unexpected increase in Ndnexpression.

3.0. PRECLINICAL GENETIC MODELING OF AUTISM SPECTRUM DISORDERS 267
MatDup mice did not have a measurable phenotype in a variety of tests related to coreautism symptoms, including social approach, communication, and reversal learning(behavioral inflexibility). In contrast, patDup mice exhibited deficits in social approach,a decreased number of ultrasonic vocalizations, and reversal learning deficits. Thesemice also exhibit a decrease in exploratory behavior, and increased freezing in a fear-conditioning task.196 It is unclear why the patDup mice, and not the matDup mice, wouldhave a more robust ASD phenotype when maternal aberrations and paternal deletions areassociated with ASD in humans with much greater prevalence than are paternalduplications.
Dysfunction in brain serotonin (5-HT) systems may underlie the patDup mouse pheno-type. The duplicated region contains a small nucleolar RNA (snoRNA; MBII52) that isinvolved in post-transcriptional modification of the 5-HT2C receptor, 5-HTR2C. PatDupmice showed a duplication of this snoRNA, increased RNA editing ratio of 5-HTR2C, andan increased calcium response to 5-HT2C agonism.195 The mice also show reduced levelsof 5-HT in a number of brain areas, including the olfactory bulb and midbrain.196 Furtherwork should elucidate whether modulation of the serotonin system can ameliorate deficitsin this model.
A second model of 15q11e13 abnormalities expresses duplications or triplications ofUbe3a,197 and was created to test the role of increased copies of maternally imprintedUbe3a in ASDs associated with 15q11e13. The effects of Ube3a overexpression were genedosage-dependent (i.e. severe in triplication and mild in duplication mice) on tests ofsocial behavior and communication (i.e. ultrasonic vocalizations), and included repetitivebehaviors in triplication mice. The mild social phenotype and effects on ultrasonic vocal-izations in mice with targeted duplication of maternal Ube3a, or duplication of the15q11e13 region containing Ube3a, appear to be consistent across laboratories.195,197
Taken together, the effects of maternal Ube3a mutations argue for an important role inmouse neurodevelopment, consistent with the human condition, and begin to makea case for the translational value of Ube3a mouse models. The glutamatergic systemwas implicated, as mice showed a lower probability of glutamate release, lower levelsof glutamate in the synaptic cleft, and reduced postsynaptic excitability. Therefore,increasing synaptic glutamatergic action may be beneficial in ASDs associated withUBE3A overexpression.
3.3. BTBR Mouse Models of Core Autism Behavioral Symptoms
BTBR Tþtf/J is an inbred mouse strain that has a behavioral phenotype with face validityfor the core behavioral symptoms of autism. BTBR mice show impairment in several socialbehavior tasks, abnormalities in vocalizations in response to social stimuli, repetitivegrooming behavior and aberrant learning and memory.198,199 The social behavioral differ-ences in BTBR mice are robust, having been shown in several different tests,199e202 andappear to be specific to tests of preference and direct interaction with other mice. BTBRmice show normal performance in social novelty and social recognition tasks, indicatinga preserved capacity for social information processing and memory.199,200 The neurobiolog-ical substrates of social behaviors include hypothalamic neuropeptide systems like oxytocinand vasopressin,203 and need to be further defined in BTBR mice using novel physiology

9. TRANSLATIONAL NEUROIMAGING IN AUTISM SPECTRUM DISORDERS268
approaches,204 with the ultimate aim of assessing their predictive validity and developinga translational imaging strategy, including fMRI coupled with social emotional tasks, inASD patients.205
The most commonly reported repetitive behavior in BTBR mice is a significant increase inself-grooming behavior.200e202,206 In addition to self-grooming, BTBR mice are reported toshow increased and repetitive bar-biting behavior, and a more rigid pattern of explorationof objects in a spontaneous object exploration task.207 Increased self-grooming behavior isa phenotype found in some genetic mouse models of ASDs (as described above), and hasbeen linked to dysfunction in glutamatergic corticostriatal neuronal circuitry.125 Moreover,mGluR5 negative allosteric modulators suppress excessive grooming behavior in BTBRmice, further implicating excessive glutamatergic signaling as a key source of aberrant repet-itive behaviors.208 BTBR mice may be a valuable component of a translational medicinestrategy centered on mGluR5 quantification via PET imaging and repetitive behaviors linkedto activation of corticostriatal circuitry.
BTBR mice have a spontaneous deletion of the Disc1 (disrupted in schizophrenia 1) geneand malformation of the corpus callosum209 and hippocampal commissure,210 which isreflective of white matter commissure pathophysiology associated with ASDs,13,211e216
and may underlie dysfunction in hippocampus-dependent behavioral tasks.199,200 The roleof the spontaneous deletion in Disc1217,218 and callosal pathology is unclear, but is beingactively explored.210 Genetics and neurophysiology research on brain circuits associatedwith core autism symptoms will determine the utility of BTBR mice as an animal model ofASD, and its value within a translational research strategy for drug development.
3.4. Application of Genetic Models in Autism Spectrum Disorder TranslationalResearch
Altering genes associated with autism in mice recapitulates some behavioraldeficits found in patients with mutations in the same genes, but is not an exact approachbecause of species differences in circuits mediating analogous behaviors, the function ofparticular genes, variation in precise mutations, and functional redundancy with other genesor compensatorymechanisms. An additional level of complexity is derived from the fact that,in some cases, siblings and carriers that share the same genetic anomaly have been diagnosedwith clinically distinct psychiatric disorders or no behavioral deficits that qualify asautistic.219 Indeed, this is consistent with the idea that many of the genes associated withautism are insufficient to cause the disorder, and that ASD is only evident when combinato-rial factors are present (the multigene or multihit hypothesis).iv
Therefore, to realize the value of animal models fully in understanding the neurobiologicalorigins of ASDs and developing effective pharmacotherapies, behavioral endpoints are notsufficient and must be combined with other preclinical measures, such as electrophysiolog-ical recordings and functional imaging that are amenable to direct translation into experi-mental medicine studies in humans.
ivFor further discussion on the multi-hit hypothesis of complex disorders, please refer to Steckler and
Salvadore in Chapter 7, Neuroimaging as a Translational Tool in Animal and Human Models of Schizo-
phrenia, in this volume.

4.0. CHALLENGES AND APPROACHES IN TRANSLATING FROM BENCH TO PATIENTS 269
4.0. CHALLENGES AND APPROACHES INTRANSLATING FROM BENCH TO PATIENTS
Current pharmacological approaches for the treatment of ASDs include on-label use oftwo antipsychotic drugs for the treatment of a cluster of symptoms referred to as irritabilityin autism, and off-label use of drugs that have limited efficacy in ameliorating associatedbehavioral symptoms, including antidepressants for the treatment of anxiety and depressionsymptoms, as well as stimulants for hyperactivity, impulsivity and inattention, and antiepi-leptics for seizures. However, as ASD pathophysiology is heterogeneous and mostlyunknown, no medication is available that addresses the core symptoms of ASD and signifi-cantly improves long-term outcome.
Given the highly heterogenous nature of ASD etiologies and symptoms, and the lack ofunderstanding around the biological basis for ASD, transitioning drugs from preclinical toclinical phases is a major challenge. The better the underlying neurobiology is understood,the easier it may be to identify novel molecular drug targets and develop medications. Anexample is FXS, where prominent theories implicating metabotropic glutamate receptorsand GABA receptors have emerged from an understanding of the genetic and neurobiolog-ical pathophysiology.100,220 It is proposed that the transition between bench and bedside can beimproved by using cross-species assays that measure the same aspect of pathophysiology inthe animal model as in the human, such as neuroimaging technologies (e.g. fMRI, sMRI, andMRS). Neuroimaging findings in animal models of ASD combined with clinical imagingoutcomes could yield a more precise and mechanistic understanding of the pathophysiologyof ASD by defining key brain structures and circuits underlying ASD-related deficits. Thesespecific brain circuits might then be mined for novel drug targets in preclinical geneticmodels of ASD, and monitored in patients to identify endophenotypes or responses thatcould be useful as drug efficacy outcome measures. Perhaps the best outcomes of using bidi-rectional translational approaches would be to support patient stratification with quantita-tive physiology measures rather than behavioral phenotyping alone, and to providetreatment-sensitive responses to help determine drug efficacy, identify appropriate dosingregimens, and differentiation across treatment classes.
Even if not yet shown for ASDs, translational imaging tools have demonstrated greatvalue for drug research and development in other CNS therapeutic areas. One example isschizophrenia, where imaging studies have been applied to both humans and animalmodels.v
It has been suggested that dysfunctions in corticalelimbicethalamic circuits in pharmaco-logical animal models of schizophrenia [i.e. acute administration of uncompetitive NMDAreceptor (NMDAR) in rodents] are reminiscent of neuroimaging findings in schizophrenicpatients and in healthy individuals treated with NMDAR antagonists that evokepsychosis-like symptoms.221e227 In addition, efforts have been made to discriminatepsychotic patients from healthy individuals, and subclassification of individual schizo-phrenia types using different approaches, including machine learning-based pattern
vPlease refer to Steckler and Salvadore in Chapter 7, Neuroimaging as a Translational Tool in Animal and
Human Models of Schizophrenia, in this volume for further discussion of the use of neuroimaging tools in
translational drug discovery and development for the understanding and treatment of schizophrenia.

9. TRANSLATIONAL NEUROIMAGING IN AUTISM SPECTRUM DISORDERS270
classification methods on MRI data.228e230 Findings from these studies indicate that complexpatterns of brain abnormality can be detected in early stages of psychotic illness, which hascritical implications for early identification and intervention in individuals at a high risk ofdeveloping psychosis/schizophrenia. Finally, efficacy of antipsychotics, including poor treat-ment response, has been monitored in both animals and humans.223,231e239 These findingssuggest that antipsychotics can modulate the imbalance in frontal cortexestriatalethalamiccircuitry described in animal models of schizophrenia and in schizophrenic patients, andhighlight the potential of imaging in detecting the influence of dosage and duration ofantipsychotic treatments. In conclusion, imaging findings in CNS disorders such asschizophrenia support the value of using preclinical and clinical imaging tools for drugdiscovery, and are likely to be useful in defining a path forward for drug developmentfor ASD.
Developing and validating an appropriate functional neuroimaging paradigm that allowspredictive translation of pharmacodynamic activity from animal models to humans mustaddress several specific experimental questions. First, which models (transgenic, behavioral,or developmental) recapitulate behaviors relevant to ASDs? Second, what is the fMRI signa-ture (task-evoked, relative activity, or resting state connectivity) of those models? Third, howdo we define comparable regions of interest (ROIs) in preclinical and clinical samples?Fourth, does the activity of the circuit alter in response to pharmacological interventionand is it similar across species or clinical models? As reviewed in the preceding sections,novel rodent models are emerging that may provide a basis for effective translation ofpreclinical data into human experimental medicine models. Several transgenic modelsappear to recapitulate specific domains of ASD dysfunction andmake it possible to capitalizeon genes and neural circuits relevant to ASDs. The biggest challenge to designing a transla-tional neuroimaging paradigm arises from the absence of functional imaging data in ASDpreclinical models. As such, the choice of which models to invest in remains largely specu-lative and prospective in terms of delineating the best methods for predicting drug responseand building platforms of drug intervention in ASD patients.
References
1. Ganz M. The Costs of Autism. In: Moldin SO RJ, editor. Understanding autism: from basic neuroscience to
treatment. Boca Raton: Taylor and Francis Group; Fla 2006.2. Baron-Cohen S, Scott FJ, Allison C, et al. Prevalence of autism-spectrum conditions: UK school-based pop-
ulation study. Br J Psychiatry Jun 2009;194(6):500e9.3. Blenner S, Reddy A, Augustyn M. Diagnosis and management of autism in childhood. Bmj 2011;343:d6238.4. Fombonne E. Epidemiology of pervasive developmental disorders. Pediatr Res Jun 2009;65(6):591e8.5. Kim YS, Leventhal BL, Koh YJ, Fombonne E, Laska E, Lim EC, et al. Prevalence of autism spectrum disorders
in a total population sample. Am J Psychiatry Sep 2011;168(9):904e12.6. Kogan MD, Blumberg SJ, Schieve LA, Boyle CA, Perrin JM, Ghandour RM, et al. Prevalence of parent-reported
diagnosis of autism spectrum disorder among children in the US, 2007. Pediatrics Nov 2009;124(5):1395e403.7. Lord C. Epidemiology: How common is autism? Nature Jun 9 2011;474(7350):166e8.8. Pinto-Martin JA, Levy SE, Feldman JF, Lorenz JM, Paneth N, Whitaker AH. Prevalence of autism spectrum
disorder in adolescents born weighing <2000 grams. Pediatrics Nov 2011;128(5):883e91.9. McPheeters ML, Warren Z, Sathe N, Bruzek JL, Krishnaswami S, Jerome RN, et al. A systematic review of
medical treatments for children with autism spectrum disorders. Pediatrics May 2011;127(5):e1312e21.10. Anagnostou E, Taylor MJ. Review of neuroimaging in autism spectrum disorders: what have we learned and
where we go from here. Mol Autism 2011;2(1):4.

REFERENCES 271
11. Hrdlicka M. Structural neuroimaging in autism. Neuro Endocrinol Lett Jun 2008;29(3):281e6.12. Nickl-Jockschat T, Habel U, Maria Michel T, Manning J, Laird AR, Fox PT, et al. Brain structure anomalies in
autism spectrum disorder-a meta-analysis of VBM studies using anatomic likelihood estimation. Hum BrainMapp Jun 20 2011.
13. Paul LK, Brown WS, Adolphs R, Tyszka JM, Richards LJ, Mukherjee P, et al. Agenesis of the corpus callosum:genetic, developmental and functional aspects of connectivity. Nat Rev Neurosci Apr 2007;8(4):287e99.
14. Pina-Camacho L, Villero S, Fraguas D, Boada L, Janssen J, Navas-Sanchez FJ, et al. Autism Spectrum Disorder:Does Neuroimaging Support the DSM-5 Proposal for a Symptom Dyad? A Systematic Review of FunctionalMagnetic Resonance Imaging and Diffusion Tensor Imaging Studies. J Autism Dev Disord Sep 20 2011.
15. Wass S. Distortions and disconnections: disrupted brain connectivity in autism. Brain Cogn Feb 2011;75(1):18e28.
16. Adolphs R, Sears L, Piven J. Abnormal processing of social information from faces in autism. J Cogn Neurosci
Feb 15 2001;13(2):232e40.17. Hall GB, Szechtman H, Nahmias C. Enhanced salience and emotion recognition in Autism: a PET study. Am J
Psychiatry Aug 2003;160(8):1439e41.18. Weeks SJ, Hobson RP. The salience of facial expression for autistic children. J Child Psychol Psychiatry Jan
1987;28(1):137e51.19. Baron-Cohen S, Ring HA, Wheelwright S, Bullmore ET, Brammer MJ, Simmons A, et al. Social intelligence in
the normal and autistic brain: an fMRI study. Eur J Neurosci Jun 1999;11(6):1891e8.20. Baron-Cohen S, Ring H, Moriarty J, Schmitz B, Costa D, Ell P. Recognition of mental state terms. Clinical
findings in children with autism and a functional neuroimaging study of normal adults. Br J Psychiatry Nov1994;165(5):640e9.
21. Spencer CM, Alekseyenko O, Hamilton SM, Thomas AM, Serysheva E, Yuva-Paylor LA. Modifying behavioralphenotypes in Fmr1KO mice: genetic background differences reveal autistic-like responses. Autism Research
2011;4(1):40e56.22. Ashwin C, Chapman E, Colle L, Baron-Cohen S. Impaired recognition of negative basic emotions in autism:
a test of the amygdala theory. Soc Neurosci 2006;1(3e4):349e63.23. Hadjikhani N, Joseph RM, Snyder J, Tager-Flusberg H. Abnormal activation of the social brain during face
perception in autism. Hum Brain Mapp May 2007;28(5):441e9.24. Pelphrey KA, Morris JP, McCarthy G, Labar KS. Perception of dynamic changes in facial affect and identity in
autism. Soc Cogn Affect Neurosci Jun 2007;2(2):140e9.25. Monk CS, Weng SJ, Wiggins JL, Kurapati N, Louro HM, Carrasco M, et al. Neural circuitry of emotional face
processing in autism spectrum disorders. J Psychiatry Neurosci Mar 2010;35(2):105e14.26. Dapretto M, Davies MS, Pfeifer JH, Scott AA, Sigman M, Bookheimer SY, et al. Understanding emotions in
others: mirror neuron dysfunction in children with autism spectrum disorders. Nat Neurosci Jan 2006;9(1):28e30.
27. Pierce K, Haist F, Sedaghat F, Courchesne E. The brain response to personally familiar faces in autism: findingsof fusiform activity and beyond. Brain Dec 2004;127(Pt 12):2703e16.
28. Piggot J, Kwon H, Mobbs D, Blasey C, Lotspeich L, Menon V, et al. Emotional attribution in high-functioningindividuals with autistic spectrum disorder: a functional imaging study. J Am Acad Child Adolesc Psychiatry Apr2004;43(4):473e80.
29. Harms MB, Martin A, Wallace GL. Facial emotion recognition in autism spectrum disorders: a review ofbehavioral and neuroimaging studies. Neuropsychol Rev Sep 2010;20(3):290e322.
30. Sanders J, Johnson KA, Garavan H, Gill M, Gallagher L. A review of neuropsychological and neuroimagingresearch in autistic spectrum disorders: Attention, inhibition and cognitive flexibility. Res Autism Spectrum
Disorders 2008;2:1e16.31. Haznedar MM, BuchsbaumMS, Wei TC, Hof PR, Cartwright C, Bienstock CA, et al. Limbic circuitry in patients
with autism spectrum disorders studied with positron emission tomography and magnetic resonance imaging.Am J Psychiatry Dec 2000;157(12):1994e2001.
32. Koshino H, Carpenter PA, Minshew NJ, Cherkassky VL, Keller TA, Just MA. Functional connectivity in anfMRI working memory task in high-functioning autism. Neuroimage Feb 1 2005;24(3):810e21.
33. Kana RK, Keller TA, Cherkassky VL, Minshew NJ, Just MA. Sentence comprehension in autism: thinking inpictures with decreased functional connectivity. Brain Sep 2006;129(Pt 9):2484e93.

9. TRANSLATIONAL NEUROIMAGING IN AUTISM SPECTRUM DISORDERS272
34. Lieberman MD. Social cognitive neuroscience: a review of core processes. Annu Rev Psychol 2007;58:259e89.
35. D’Argembeau A, Collette F, Van der Linden M, Laureys S, Del Fiore G, Degueldre C, et al. Self-referentialreflective activity and its relationship with rest: a PET study. Neuroimage Apr 1 2005;25(2):616e24.
36. Ochsner KN, Beer JS, Robertson ER, Cooper JC, Gabrieli JD, Kihsltrom JF, et al. The neural correlates of directand reflected self-knowledge. Neuroimage Dec 2005;28(4):797e814.
37. Fossati P, Hevenor SJ, Graham SJ, Grady C, Keightley ML, Craik F, et al. In search of the emotional self: an fMRIstudy using positive and negative emotional words. Am J Psychiatry Nov 2003;160(11):1938e45.
38. Kennedy DP, Courchesne E. Functional abnormalities of the default network during self- and other-reflectionin autism. Soc Cogn Affect Neurosci Jun 2008;3(2):177e90.
39. Mizuno A, Liu Y, Williams DL, Keller TA, Minshew NJ, Just MA. The neural basis of deictic shifting inlinguistic perspective-taking in high-functioning autism. Brain Aug 2011;134(Pt 8):2422e35.
40. Lombardo MV, Chakrabarti B, Bullmore ET, Sadek SA, Pasco G, Wheelwright SJ, et al. Atypical neural self-representation in autism. Brain Feb 2010;133(Pt 2):611e24.
41. Haznedar MM, Buchsbaum MS, Hazlett EA, LiCalzi EM, Cartwright C, Hollander E. Volumetric analysis andthree-dimensional glucose metabolic mapping of the striatum and thalamus in patients with autism spectrumdisorders. Am J Psychiatry Jul 2006;163(7):1252e63.
42. Verhoeven JS, De Cock P, Lagae L, Sunaert S. Neuroimaging of autism. Neuroradiology Jan 2010;52(1):3e14.43. Cherkassky VL, Kana RK, Keller TA, Just MA. Functional connectivity in a baseline resting-state network in
autism. Neuroreport Nov 6 2006;17(16):1687e90.44. Assaf M, Jagannathan K, Calhoun VD, Miller L, Stevens MC, Sahl R, et al. Abnormal functional connectivity of
default mode sub-networks in autism spectrum disorder patients. Neuroimage Oct 15 2010;53(1):247e56.45. Ebisch SJ, Gallese V, Willems RM, Mantini D, Groen WB, Romani GL, et al. Altered intrinsic functional
connectivity of anterior and posterior insula regions in high-functioning participants with autism spectrumdisorder. Hum Brain Mapp Jul 2011;32(7):1013e28.
46. Broyd SJ, Demanuele C, Debener S, Helps SK, James CJ, Sonuga-Barke EJ. Default-mode brain dysfunction inmental disorders: a systematic review. Neurosci Biobehav Rev Mar 2009;33(3):279e96.
47. Silani G, Bird G, Brindley R, Singer T, Frith C, Frith U. Levels of emotional awareness and autism: an fMRIstudy. Soc Neurosci 2008;3(2):97e112.
48. Ogawa S, Tank DW, Menon R, Ellermann JM, Kim SG, Merkle H, et al. Intrinsic signal changes accompanyingsensory stimulation: functional brain mapping with magnetic resonance imaging. Proc Natl Acad Sci U S A Jul 11992;89(13):5951e5.
49. Nichols T, Hayasaka S. Controlling the familywise error rate in functional neuroimaging: a comparativereview. Stat Methods Med Res Oct 2003;12(5):419e46.
50. Wise RG, Preston C. What is the value of human FMRI in CNS drug development? Drug Discov Today Nov2010;15(21e22):973e80.
51. Biswal B, Yetkin FZ, Haughton VM, Hyde JS. Functional connectivity in the motor cortex of resting humanbrain using echo-planar MRI. Magn Reson Med Oct 1995;34(4):537e41.
52. Brammer M. The role of neuroimaging in diagnosis and personalized medicinedcurrent position and likelyfuture directions. Dialogues Clin Neurosci 2009;11(4):389e96.
53. O’Toole AJ, Jiang F, Abdi H, Penard N, Dunlop JP, Parent MA. Theoretical, statistical, and practical perspec-tives on pattern-based classification approaches to the analysis of functional neuroimaging data. J Cogn
Neurosci Nov 2007;19(11):1735e52.54. Ecker C, Marquand A, Mourao-Miranda J, Johnston P, Daly EM, Brammer MJ, et al. Describing the brain in
autism in five dimensionsdmagnetic resonance imaging-assisted diagnosis of autism spectrum disorder usinga multiparameter classification approach. J Neurosci Aug 11 2010;30(32):10612e23.
55. Lai G, Schneider HD, Schwarzenberger JC, Hirsch J. Speech stimulation during functional MR imaging asa potential indicator of autism. Radiology Aug 2011;260(2):521e30.
56. Kirsch P, Esslinger C, Chen Q, Mier D, Lis S, Siddhanti S, et al. Oxytocin modulates neural circuitry for socialcognition and fear in humans. J Neurosci Dec 7 2005;25(49):11489e93.
57. Rilling JK, Demarco AC, Hackett PD, Thompson R, Ditzen B, Patel R, et al. Effects of intranasal oxytocin andvasopressin on cooperative behavior and associated brain activity in men. Psychoneuroendocrinology Apr2011;37(4):447e61.

REFERENCES 273
58. Riem MM, van Ijzendoorn MH, Tops M, Boksem MA, Rombouts SA, Bakermans-Kranenburg MJ. NoLaughing Matter: Intranasal Oxytocin Administration Changes Functional Brain Connectivity during Expo-sure to Infant Laughter. Neuropsychopharmacology Apr 2011;37(5):1257e66.
59. Hatton DD, Sideris J, Skinner M, Mankowski J, Bailey Jr DB, Roberts J. Autism behavior in children with fragileX syndrome: prevalence, stability, and the impact of FMRP. Am J Med Genet A Sep 1 2006;140A(17):1804e13.
60. Hagerman RJ. Lessons from fragile X regarding neurobiology, autism, and neurodegeneration. J Dev Behav
Pediatr Feb 2006;27(1):63e74.61. Wang LW, Berry-Kravis E, Hagerman RJ, Fragile X. Leading the way for targeted treatments in autism. Neu-
rotherapeutics Jul 2010;7(3):264e74.62. Hagerman PJ, Hagerman RJ. The fragile-X premutation: a maturing perspective. Am J Hum Genet May
2004;74(5):805e16.63. Verkerk AJ, Pieretti M, Sutcliffe JS, Fu YH, Kuhl DP, Pizzuti A, et al. Identification of a gene (FMR-1) containing
a CGG repeat coincident with a breakpoint cluster region exhibiting length variation in fragile X syndrome.Cell May 31 1991;65(5):905e14.
64. Pieretti M, Zhang FP, Fu YH, Warren ST, Oostra BA, Caskey CT, et al. Absence of expression of the FMR-1 genein fragile X syndrome. Cell Aug 23 1991;66(4):817e22.
65. Mientjes EJ, Nieuwenhuizen I, Kirkpatrick L, Zu T, Hoogeveen-Westerveld M, Severijnen L, et al. Thegeneration of a conditional Fmr1 knock out mouse model to study Fmrp function in vivo. Neurobiol Dis Mar2006;21(3):549e55.
66. Consortium TD- BFX. Fmr1 knockout mice: a model to study fragile X mental retardation. The Dutch-BelgianFragile X Consortium. Cell Jul 15 1994;78(1):23e33.
67. Comery TA, Harris JB, Willems PJ, Oostra BA, Irwin SA, Weiler IJ, et al. Abnormal dendritic spines in fragile Xknockout mice: maturation and pruning deficits. Proc Natl Acad Sci U S A May 13 1997;94(10):5401e4.
68. Irwin SA, Galvez R, Greenough WT. Dendritic spine structural anomalies in fragile-X mental retardationsyndrome. Cereb Cortex Oct 2000;10(10):1038e44.
69. Nimchinsky EA, Oberlander AM, Svoboda K. Abnormal development of dendritic spines in FMR1 knock-outmice. J Neurosci Jul 15 2001;21(14):5139e46.
70. Kooy RF, D’Hooge R, Reyniers E, Bakker CE, Nagels G, De Boulle K, et al. Transgenic mouse model for thefragile X syndrome. Am J Med Genet Aug 9 1996;64(2):241e5.
71. D’Hooge R, Nagels G, Franck F, Bakker CE, Reyniers E, Storm K, et al. Mildly impaired water maze perfor-mance in male Fmr1 knockout mice. Neuroscience Jan 1997;76(2):367e76.
72. Silverman JL, Yang M, Lord C, Crawley JN. Behavioural phenotyping assays for mouse models of autism. Nat
Rev Neurosci Jul 2010;11(7):490e502.73. Paradee W, Melikian HE, Rasmussen DL, Kenneson A, Conn PJ, Warren ST. Fragile X mouse: strain effects of
knockout phenotype and evidence suggesting deficient amygdala function. Neuroscience 1999;94(1):185e92.74. Yan QJ, Asafo-Adjei PK, Arnold HM, Brown RE, Bauchwitz RP. A phenotypic and molecular characterization
of the fmr1-tm1Cgr fragile X mouse. Genes Brain Behav Dec 2004;3(6):337e59.75. Zhao MG. Deficits in Trace Fear Memory and Long-Term Potentiation in a Mouse Model for Fragile X
Syndrome. Journal of Neuroscience 2005;25(32):7385e92.76. Mineur YS, Sluyter F, de Wit S, Oostra BA, Crusio WE. Behavioral and neuroanatomical characterization of the
Fmr1 knockout mouse. Hippocampus 2002;12(1):39e46.77. Ventura R, Pascucci T, Catania MV, Musumeci SA, Puglisi-Allegra S. Object recognition impairment in Fmr1
knockout mice is reversed by amphetamine: involvement of dopamine in the medial prefrontal cortex. BehavPharmacol Sep 2004;15(5e6):433e42.
78. Moon J, Beaudin AE, Verosky S, Driscoll LL, Weiskopf M, Levitsky DA, et al. Attentional dysfunction,impulsivity, and resistance to change in a mouse model of fragile X syndrome. Behavioral Neuroscience
2006;120(6):1367e79.79. Spencer CM, Alekseyenko O, Serysheva E, Yuva-Paylor LA, Paylor R. Altered anxiety-related and social
behaviors in the Fmr1 knockout mouse model of fragile X syndrome. Genes, Brain and Behavior 2005;4(7):420e30.
80. Pietropaolo S, Guilleminot A, Martin B, D’Amato FR, Crusio WE. Genetic-background modulation of core andvariable autistic-like symptoms in Fmr1 knock-out mice. PLoS ONE 2011;6(2):e17073.

9. TRANSLATIONAL NEUROIMAGING IN AUTISM SPECTRUM DISORDERS274
81. Chen L, Toth M. Fragile X mice develop sensory hyperreactivity to auditory stimuli. Neuroscience 2001;103(4):1043e50.
82. Nielsen DM, Derber WJ, McClellan DA, Crnic LS. Alterations in the auditory startle response in Fmr1 targetedmutant mouse models of fragile X syndrome. Brain Res Feb 8 2002;927(1):8e17.
83. Spencer CM. Exaggerated behavioral phenotypes in Fmr1/Fxr2 double knockout mice reveal afunctiona genetic interaction between Fragile X-related proteins. Human Molecular Genetics 2006;15(12):1984e94.
84. Price TJ, Rashid MH, Millecamps M, Sanoja R, Entrena JM, Cervero F. Decreased nociceptive sensitization inmice lacking the fragile X mental retardation protein: role of mGluR1/5 and mTOR. J Neurosci Dec 192007;27(51):13958e67.
85. Moy SS, Nadler JJ, Young NB, Nonneman RJ, Grossman AW, Murphy DL, et al. Social approach in geneticallyengineered mouse lines relevant to autism. Genes Brain and Behavior 2009;8(2):129e42.
86. Dahlhaus R, El-Husseini A. Altered neuroligin expression is involved in social deficits in a mouse model of thefragile X syndrome. Behavioural Brain Research 2010;208(1):96e105.
87. McNaughton CH, Moon J, Strawderman MS, Maclean KN, Evans J, Strupp BJ. Evidence for social anxiety andimpaired social cognition in a mouse model of fragile X syndrome. Behavioral Neuroscience 2008;122(2):293e300.
88. Mineur YS, Huynh LX, Crusio WE. Social behavior deficits in the Fmr1 mutant mouse. Behavioural BrainResearch 2006;168(1):172e5.
89. Mines MA, Yuskaitis CJ, King MK, Beurel E, Jope RS. GSK3 influences social preference and anxiety-relatedbehaviors during social interaction in a mouse model of fragile X syndrome and autism. PLoS ONE 2010;5(3):e9706.
90. Peier AM, McIlwain KL, Kenneson A, Warren ST, Paylor R, Nelson DL. (Over)correction of FMR1 deficiencywith YAC transgenics: behavioral and physical features. Hum Mol Genet May 1 2000;9(8):1145e59.
91. Hou L, Antion MD, Hu D, Spencer CM, Paylor R, Klann E, et al. Dynamic Translational of Fragile X MentalRetardation Protein Controls mGluR-Dependent Long-Term Depression. Neuron 2006;51(4):441e54.
92. Huber KM. Altered synaptic plasticity in a mouse model of fragile X mental retardation. Proceedings of theNational Academy of Sciences 2002;99(11):7746e50.
93. Koekkoek SKE, Yamaguchi K, Milojkovic BA, Dortland BR, Ruigrok TJ, Maex R, et al. Deletion of FMR1 inPurkinje Cells Enhances Parallel Fiber LTD, Enlarges Spines, and Attenuates Cerebellar Eyelid Conditioning inFragile X Syndrome. Neuron 2005;47(3):339e52.
94. Nosyreva ED. Metabotropic Receptor-Dependent Long-Term Depression Persists in the Absence of ProteinSynthesis in the Mouse Model of Fragile X Syndrome. Journal of Neurophysiology 2006;95(5):3291e5.
95. Sharma A, Hoeffer CA, Takayasu Y, Miyawaki T, McBride SM, Klann E, et al. Dysregulation of mTORSignaling in Fragile X Syndrome. Journal of Neuroscience 2010;30(2):694e702.
96. Zhang J, Hou L, Klann E, Nelson DL. Altered Hippocampal Synaptic Plasticity in the Fmr1 Gene FamilyKnockout Mouse Models. Journal of Neurophysiology 2009;101(5):2572e80.
97. Suvrathan A, Hoeffer CA, Wong H, Klann E, Chattarji S. Characterization and reversal of synaptic defects inthe amygdala in a mouse model of fragile X syndrome. Proceedings of the National Academy of Sciences
2010;107(25):11591e6.98. Gibson JR, Bartley AF, Hays SA, Huber KM. Imbalance of Neocortical Excitation and Inhibition and Altered
UP States Reflect Network Hyperexcitability in the Mouse Model of Fragile X Syndrome. Journal of
Neurophysiology 2008;100(5):2615e26.99. Li Reduced Cortical Synaptic Plasticity J, Expression GluR1. Associated with Fragile X Mental Retardation
Protein Deficiency. Molecular and Cellular Neuroscience 2002;19(2):138e51.100. Paluszkiewicz SM, Martin BS, Huntsman MM. Fragile X Syndrome: The GABAergic System and Circuit
Dysfunction. Developmental Neuroscience 2011;33(5):349e64.101. El Idrissi A, Ding X-H, Scalia J, Trenkner E, Brown WT, Dobkin C. Decreased GABAA receptor expression in
the seizure-prone fragile X mouse. Neuroscience Letters 2005;377(3):141e6.102. Pacey LKK, Tharmalingam S, Hampson DR. Subchronic Administration and Combination Metabotropic
Glutamate and GABAB Receptor Drug Therapy in Fragile X Syndrome. Journal of Pharmacology and Experi-
mental Therapeutics 2011;338(3):897e905.103. Bear MF, Huber KM, Warren ST. The mGluR theory of fragile X mental retardation. Trends in Neurosciences
2004;27(7):370e7.

REFERENCES 275
104. Thomas AM, Bui N, Graham D, Perkins JR, Yuva-Paylor LA, Paylor R. Genetic reduction of group 1 metab-otropic glutamate receptors alters select behaviors in a mouse model for fragile X syndrome. Behavioural BrainResearch 2011;223(2):310e21.
105. Yan QJ, Rammal M, Tranfaglia M, Bauchwitz RP. Suppression of two major Fragile X Syndrome mouse modelphenotypes by the mGluR5 antagonist MPEP. Neuropharmacology 2005;49(7):1053e66.
106. Jacquemont S, Curie A, des Portes V, Torrioli MG, Berry-Kravis E, Hagerman RJ, et al. Epigenetic modificationof the FMR1 gene in fragile X syndrome is associated with differential response to the mGluR5 antagonistAFQ056. Sci Transl Med Jan 5 2011;3(64):64.
107. Pacey LKK, Heximer SP, Hampson DR. Increased GABAB Receptor-Mediated Signaling Reducesthe Susceptibility of Fragile X Knockout Mice to Audiogenic Seizures. Molecular Pharmacology 2009;76(1):18e24.
108. Liu Z-H, Chuang D-M, Smith CB. Lithium ameliorates phenotypic deficits in a mouse model of fragile Xsyndrome. The International Journal of Neuropsychopharmacology 2010;14(05):618e30.
109. Amir RE, Van den Veyver IB, Wan M, Tran CQ, Francke U, Zoghbi HY. Rett syndrome is caused by mutationsin X-linked MECP2, encoding methyl-CpG-binding protein 2. Nat Genet Oct 1999;23(2):185e8.
110. Chahrour M, Zoghbi HY. The story of Rett syndrome: from clinic to neurobiology. Neuron Nov 8 2007;56(3):422e37.
111. Ricceri L, De Filippis B, Laviola G. Mouse models of Rett syndrome: from behavioural phenotyping topreclinical evaluation of new therapeutic approaches. Behav Pharmacol Sep 2008;19(5e6):501e17.
112. Guy J, Cheval H, Selfridge J, Bird A. The role of MeCP2 in the brain. Annu Rev Cell Dev Biol Nov 102011;27:631e52.
113. Percy AK. Rett syndrome: exploring the autism link. Arch Neurol Aug 2007;68(8):985e9.114. Chen RZ, Akbarian S, Tudor M, Jaenisch R. Deficiency of methyl-CpG binding protein-2 in CNS neurons
results in a Rett-like phenotype in mice. Nat Genet Mar 2001;27(3):327e31.115. Guy J, Hendrich B, Holmes M, Martin JE, Bird A. A mouse Mecp2-null mutation causes neurological symp-
toms that mimic Rett syndrome. Nat Genet Mar 2001;27(3):322e6.116. Pelka GJ, Watson CM, Christodoulou J, Tam PP. Distinct expression profiles of Mecp2 transcripts with
different lengths of 3’UTR in the brain and visceral organs during mouse development. Genomics Apr2005;85(4):441e52.
117. Lawson-Yuen A, Liu D, Han L, Jiang ZI, Tsai GE, Basu AC, et al. Ube3a mRNA and protein expression are notdecreased in Mecp2R168X mutant mice. Brain Res Nov 14 2007;1180:1e6.
118. Shahbazian M, Young J, Yuva-Paylor L, Spencer C, Antalffy B, Noebels J, et al. Mice with truncated MeCP2recapitulate many Rett syndrome features and display hyperacetylation of histone H3. Neuron Jul 182002;35(2):243e54.
119. Collins AL, Levenson JM, Vilaythong AP, et al. Mild overexpression of MeCP2 causes a progressive neuro-logical disorder in mice. Hum Mol Genet Nov 1 2004;13(21):2679e89.
120. Chao HT, Chen H, Samaco RC, et al. Dysfunction in GABA signalling mediates autism-like stereotypies andRett syndrome phenotypes. Nature Nov 11 2010;468(7321):263e9.
121. De Filippis B, Ricceri L, Laviola G. Early postnatal behavioral changes in the Mecp2e308 truncation mousemodel of Rett syndrome. Genes Brain Behav Mar 1 2010;9(2):213e23.
122. Picker JD, Yang R, Ricceri L, Berger-Sweeney J. An altered neonatal behavioral phenotype in Mecp2 mutantmice. Neuroreport Apr 3 2006;17(5):541e4.
123. Samaco RC, Neul JL. Complexities of Rett syndrome and MeCP2. J Neurosci Jun 1 2011;31(22):7951e9.124. Abdala AP, Dutschmann M, Bissonnette JM, Paton JF. Correction of respiratory disorders in a mouse model of
Rett syndrome. Proc Natl Acad Sci U S A Oct 19 2010;107(42):18208e13.125. Peca J, Feliciano C, Ting JT, et al. Shank3 mutant mice display autistic-like behaviours and striatal dysfunction.
Nature 2011;472(7344):437e42.126. Chang Q, Khare G, Dani V, Nelson S, Jaenisch R. The disease progression of Mecp2 mutant mice is affected by
the level of BDNF expression. Neuron Feb 2 2006;49(3):341e8.127. Roux JC, Dura E, Moncla A, Mancini J, Villard L. Treatment with desipramine improves breathing and survival
in a mouse model for Rett syndrome. Eur J Neurosci Apr 2007;25(7):1915e22.128. Guy J, Gan J, Selfridge J, Cobb S, Bird A. Reversal of neurological defects in a mouse model of Rett syndrome.
Science Feb 23 2007;315(5815):1143e7.

9. TRANSLATIONAL NEUROIMAGING IN AUTISM SPECTRUM DISORDERS276
129. Butler MG, Dasouki MJ, Zhou XP, Talebizadeh Z, Brown M, Takahashi TN, et al. Subset of individuals withautism spectrum disorders and extreme macrocephaly associated with germline PTEN tumour suppressorgene mutations. J Med Genet Apr 2005;42(4):318e21.
130. Goffin A, Hoefsloot LH, Bosgoed E, Swillen A, Fryns JP. PTEN mutation in a family with Cowden syndromeand autism. Am J Med Genet Aug 8 2001;105(6):521e4.
131. Herman GE, Butter E, Enrile B, Pastore M, Prior TW, Sommer A. Increasing knowledge of PTEN germline muta-tions: Two additional patients with autism and macrocephaly. Am J Med Genet AMar 15 2007;143(6):589e93.
132. Orrico A, Galli L, Buoni S, Orsi A, Vonella G, Sorrentino V. Novel PTEN mutations in neurodevelopmentaldisorders and macrocephaly. Clin Genet Feb 2009;75(2):195e8.
133. Rodriguez-Escudero I, Oliver MD, Andres-Pons A, Molina M, Cid VJ, Pulido R. A comprehensive functionalanalysis of PTEN mutations: implications in tumor- and autism-related syndromes. Hum Mol Genet Nov 12011;20(21):4132e42.
134. Varga EA, Pastore M, Prior T, Herman GE, McBride KL. The prevalence of PTEN mutations in a clinicalpediatric cohort with autism spectrum disorders, developmental delay, and macrocephaly. Genet Med Feb2009;11(2):111e7.
135. Page DT, Kuti OJ, Prestia C, Sur M. Haploinsufficiency for Pten and Serotonin transporter cooperativelyinfluences brain size and social behavior. Proceedings of the National Academy of Sciences 2009;106(6):1989e94.
136. Di Cristofano A, Pesce B, Cordon-Cardo C, Pandolfi PP. Pten is essential for embryonic development andtumour suppression. Nat Genet Aug 1998;19(4):348e55.
137. Stambolic V, Tsao MS, Macpherson D, Suzuki A, Chapman WB, Mak TW. High incidence of breast andendometrial neoplasia resembling human Cowden syndrome in ptenþ/- mice. Cancer Res Jul 1 2000;60(13):3605e11.
138. Suzuki A, de la Pompa JL, Stambolic V, Elia AJ, Sasaki T, del Barco Barrantes I, et al. High cancer susceptibilityand embryonic lethality associated with mutation of the PTEN tumor suppressor gene in mice. Curr Biol Oct 221998;8(21):1169e78.
139. Backman SA, Stambolic V, Suzuki A, Haight J, Elia A, Pretorius J, et al. Nature Genetics 2001;29(4):396e403.140. Kwon C-H, Luikart BW, Powell CM, Zhou J, Matheny SA, Zhang W, et al. in Mice. Neuron 2006;50(3):377e88.141. Luikart BW, Schnell E, Washburn EK, Bensen AL, Tovar KR, Westbrook GL. Pten knockdown in vivo increases
excitatory drive onto dentate granule cells. J Neurosci Mar 16 2011;31(11):4345e54.142. Ehninger D, Silva AJ. Rapamycin for treating Tuberous sclerosis and Autism spectrum disorders. Trends in
Molecular Medicine 2011;17(2):78e87.143. Zhou J, Blundell J, Ogawa S, Kwon CH, Zhang W, Sinton C, et al. Pharmacological Inhibition of mTORC1
Suppresses Anatomical, Cellular, and Behavioral Abnormalities in Neural-Specific Pten Knock-Out Mice.Journal of Neuroscience 2009;29(6):1773e83.
144. Sunnen CN, Brewster AL, Lugo JN, Vanegas F, Turcios E, Mukhi S, et al. Inhibition of the mammalian target ofrapamycin blocks epilepsy progression in NS-Pten conditional knockout mice. Epilepsia 2011;52(11):2065e75.
145. Sudhof TC. Neuroligins and neurexins link synaptic function to cognitive disease. Nature 2008;455(7215):903e11.
146. Buxbaum JD. Multiple rare variants in the etiology of autism spectrum disorders. Dialogues Clin Neurosci
2009;11(1):35e43.147. Levinson JN, El-Husseini A. Building excitatory and inhibitory synapses: balancing neuroligin partnerships.
Neuron Oct 20 2005;48(2):171e4.148. Rubenstein JL, Merzenich MM. Model of autism: increased ratio of excitation/inhibition in key neural systems.
Genes Brain Behav Oct 2003;2(5):255e67.149. Jamain S, Quach H, Betancur C, Rastam M, Colineaux C, Gillberg IC, et al. Paris Autism Research International
Sibpair Study. Mutations of the X-linked genes encoding neuroligins NLGN3 and NLGN4 are associated withautism. Nature Genetics 2003;34(1):27e9.
150. Jamain S, Radyushkin K, Hammerschmidt K, Granon S, Boretius S, Varoqueaux F, et al. Reduced socialinteraction and ultrasonic communication in a mouse model of monogenic heritable autism. Proceedings of theNational Academy of Sciences 2008;105(5):1710e5.
151. Radyushkin K, Hammerschmidt K, Boretius S, Varoqueaux F, El-Kordi A, Ronnenberg A, et al. Neuroligin-3-deficient mice: model of a monogenic heritable form of autism with an olfactory deficit. Genes Brain andBehavior 2009;8(4):416e25.

REFERENCES 277
152. Chadman KK, Gong S, Scattoni ML, Boltuck SE, Gandhy SU, Heintz N, et al. Minimal aberrant behavioralphenotypes of neuroligin-3 R451C knockin mice. Autism Research 2008;1(3):147e58.
153. Tabuchi K, Blundell J, Etherton MR, Hammer RE, Liu X, Powell CM, et al. A Neuroligin-3 Mutation Implicatedin Autism Increases Inhibitory Synaptic Transmission in Mice. Science 2007;318(5847):71e6.
154. Etherton M, Foldy C, Sharma M, Tabuchi K, Liu X, Shamloo M, et al. Autism-linked neuroligin-3 R451Cmutation differentially alters hippocampal and cortical synaptic function. Proceedings of the National Academy of
Sciences 2011;108(33):13764e9.155. Pardo CA, Eberhart CG. The Neurobiology of Autism. Brain Pathology 2007;17(4):434e47.156. Kim H-G, Kishikawa S, Higgins AW, Seong IS, Donovan DJ, Shen Y, et al. Disruption of Neurexin 1 Associated
with Autism Spectrum Disorder. The American Journal of Human Genetics 2008;82(1):199e207.157. Marshall CR, Noor A, Vincent JB, Lionel AC, Feuk L, Skaug J, et al. Structural Variation of Chromosomes in
Autism Spectrum Disorder. The American Journal of Human Genetics 2008;82(2):477e88.158. Feng J, Schroer R, Yan J, Li W, Skinner C, Schwartz CE, et al. High frequency of neurexin 1beta signal peptide
structural variants in patients with autism. Neurosci Lett Nov 27 2006;409(1):10e3.159. Glessner JT, Wang K, Cai G, Korvatska O, Kim CE, Wood S, et al. Autism genome-wide copy number variation
reveals ubiquitin and neuronal genes. Nature May 28 2009;459(7246):569e73.160. Kirov G, Gumus D, Chen W, Norton N, Georgieva L, Sari M, et al. Comparative genome hybridization
suggests a role for NRXN1 and APBA2 in schizophrenia. Hum Mol Genet Feb 1 2008;17(3):458e65.161. Morrow EM, Yoo SY, Flavell SW, Kim TK, Lin Y, Hill RS, et al. Identifying autism loci and genes by tracing
recent shared ancestry. Science Jul 11 2008;321(5886):218e23.162. Sebat J, Lakshmi B, Malhotra D, Troge J, Lese-Martin C, Walsh T, et al. Strong association of de novo copy
number mutations with autism. Science Apr 20 2007;316(5823):445e9.163. Szatmari P, Paterson AD, Zwaigenbaum L, Roberts W, Brian J, Liu XQ, et al. Mapping autism risk loci using
genetic linkage and chromosomal rearrangements. Nat Genet Mar 2007;39(3):319e28.164. Yan J, Noltner K, Feng J, Li W, Schroer R, Skinner C, et al. Neurexin 1alpha structural variants associated with
autism. Neurosci Lett Jun 27 2008;438(3):368e70.165. Zweier C, de Jong EK, Zweier M, Orrico A, Ousager LB, Collins AL, et al. CNTNAP2 and NRXN1 are mutated
in autosomal-recessive Pitt-Hopkins-like mental retardation and determine the level of a common synapticprotein in Drosophila. Am J Hum Genet Nov 2009;85(5):655e66.
166. Ullrich B, Ushkaryov YA, Sudhof TC. Cartography of neurexins: more than 1000 isoforms generated byalternative splicing and expressed in distinct subsets of neurons. Neuron Mar 1995;14(3):497e507.
167. Graf ER, Zhang X, Jin SX, Linhoff MW, Craig AM. Neurexins induce differentiation of GABA and glutamatepostsynaptic specializations via neuroligins. Cell Dec 29 2004;119(7):1013e26.
168. Prange O, Wong TP, Gerrow K, Wang YT, El-Husseini A. A balance between excitatory and inhibitory synapsesis controlled by PSD-95 and neuroligin. Proc Natl Acad Sci U S A Sep 21 2004;101(38):13915e20.
169. Etherton MR, Blaiss CA, Powell CM, Sudhof TC. Mouse neurexin-1 deletion causes correlated electrophysi-ological and behavioral changes consistent with cognitive impairments. Proceedings of the National Academy ofSciences 2009;106(42):17998e8003.
170. Szczypka MS, Kwok K, Brot MD, Marck BT, Matsumoto AM, Donahue BA, et al. Dopamine production in thecaudate putamen restores feeding in dopamine-deficient mice. Neuron Jun 2001;30(3):819e28.
171. Arking DE, Cutler DJ, Brune CW, Teslovich TM, West K, Ikeda M, et al. A Common Genetic Variant in theNeurexin Superfamily Member CNTNAP2 Increases Familial Risk of Autism. The American Journal of Human
Genetics 2008;82(1):160e4.172. Scott-Van Zeeland AA, Abrahams BS, Alvarez-Retuerto AI, Sonnenblick LI, Rudie JD, Ghahremani D, et al.
Altered Functional Connectivity in Frontal Lobe Circuits Is Associated with Variation in the Autism Risk GeneCNTNAP2. Science Translational Medicine 2010;2(56):56ra80e56ra80.
173. Alarcon M, Abrahams BS, Stone JL, Duvall JA, Perederiy JV, Bomar JM, et al. Linkage, association, and gene-ex-pression analyses identify CNTNAP2 as an autism-susceptibility gene. Am J Hum Genet Jan 2008;82(1):150e9.
174. Bakkaloglu B, O’Roak BJ, Louvi A, Gupta AR, Abelson JF, Morgan TM, et al. Molecular cytogenetic analysisand resequencing of contactin associated protein-like 2 in autism spectrum disorders. Am J Hum Genet Jan2008;82(1):165e73.
175. Rossi E, Verri AP, Patricelli MG, Destefani V, Ricca I, Vetro A, et al. A 12Mb deletion at 7q33-q35 associatedwith autism spectrum disorders and primary amenorrhea. Eur J Med Genet Nov-Dec 2008;51(6):631e8.

9. TRANSLATIONAL NEUROIMAGING IN AUTISM SPECTRUM DISORDERS278
176. Strauss KA, Puffenberger EG, Huentelman MJ, Gottlieb S, Dobrin SE, Parod JM, et al. Recessive symptomaticfocal epilepsy and mutant contactin-associated protein-like 2. N Engl J Med Mar 30 2006;354(13):1370e7.
177. Poliak S, Gollan L, Martinez R, Custer A, Einheber S, Salzer JL, et al. Caspr2, a new member of the neurexinsuperfamily, is localized at the juxtaparanodes of myelinated axons and associates with Kþ channels. Neuron
Dec 1999;24(4):1037e47.178. Penagarikano O, Abrahams BS, Herman EI, Winden KD, Gdalyahu A, Dong H, et al. Absence of CNTNAP2
Leads to Epilepsy, Neuronal Migration Abnormalities, and Core Autism-Related Deficits. Cell 2011;147(1):235e46.
179. Grabrucker AM, Schmeisser MJ, Schoen M, Boeckers TM. Postsynaptic ProSAP/Shank scaffolds in the cross-hair of synaptopathies. Trends in Cell Biology 2011;21(10):594e603.
180. Berkel S, Marshall CR, Weiss B, Howe J, Roeth R, Moog U, et al. Mutations in the SHANK2 synaptic scaffoldinggene in autism spectrum disorder and mental retardation. Nature Genetics 2010;42(6):489e91.
181. Bourgeron T. A synaptic trek to autism. Current Opinion in Neurobiology 2009;19(2):231e4.182. Durand CM, Betancur C, Boeckers TM, Bockmann J, Chaste P, Fauchereau F, et al. Mutations in the gene
encoding the synaptic scaffolding protein SHANK3 are associated with autism spectrum disorders. Nature
Genetics 2006;39(1):25e7.183. Gauthier J, Spiegelman D, Piton A, Lafreniere RG, Laurent S, St-Onge J, et al. Novel de novo SHANK3
mutation in autistic patients. American Journal of Medical Genetics Part B: Neuropsychiatric Genetics 2009;150B(3):421e4.
184. Moessner R, Marshall CR, Sutcliffe JS, Skaug J, Pinto D, Vincent J, et al. Contribution of SHANK3 Mutations toAutism Spectrum Disorder. The American Journal of Human Genetics 2007;81(6):1289e97.
185. Silverman JL, Turner SM, Barkan CL, Tolu SS, Saxena R, Hung AY, et al. Sociability and motor functions inShank1 mutant mice. Brain Research 2011;1380:120e37.
186. Wohr M, Roullet FI, Hung AY, Sheng M, Crawley JN. Communication impairments in mice lacking Shank1:reduced levels of ultrasonic vocalizations and scent marking behavior. PLoS ONE 2011;6(6):e20631.
187. Hung AY, Futai K, Sala C, Valtschanoff JG, Ryu J, Woodworth MA, et al. Smaller Dendritic Spines, WeakerSynaptic Transmission, but Enhanced Spatial Learning in Mice Lacking Shank1. Journal of Neuroscience
2008;28(7):1697e708.188. Bozdagi O, Sakurai T, Papapetrou D, Wang X, Dickstein DL, Takahashi N, et al. Haploinsufficiency of the
autism-associated Shank3 gene leads to deficits in synaptic function, social interaction, and social communi-cation. Mol Autism 2010;1(1):15.
189. Bangash MA, Park JM, Melnikova T, Wang D, Jeon SK, Lee D, et al. Enhanced Polyubiquitination of Shank3and NMDA Receptor in a Mouse Model of Autism. Cell 2011;145(5):758e72.
190. Sears LL, Vest C, Mohamed S, Bailey J, Ranson BJ, Piven J. An MRI study of the basal ganglia in autism. ProgNeuropsychopharmacol Biol Psychiatry May 1999;23(4):613e24.
191. Wang X, McCoy PA, Rodriguiz RM, Pan Y, Je HS, Roberts AC, et al. Synaptic dysfunction and abnormalbehaviors in mice lacking major isoforms of Shank3. Human Molecular Genetics 2011;20(15):3093e108.
192. Hogart A, Wu D, LaSalle JM, Schanen NC. The comorbidity of autism with the genomic disorders of chro-mosome 15q11.2-q13. Neurobiol Dis May 2010;38(2):181e91.
193. Chamberlain SJ, Lalande M. Angelman syndrome, a genomic imprinting disorder of the brain. J Neurosci Jul 282010;30(30):9958e63.
194. Nicholls RD, Knepper JL. Genome organization, function, and imprinting in Prader-Willi and Angelmansyndromes. Annu Rev Genomics Hum Genet 2001;2:153e75.
195. Nakatani J, Tamada K, Hatanaka F, Ise S, Ohta H, Inoue K, et al. Abnormal behavior in a chromosome-engineered mouse model for human 15q11e13 duplication seen in autism. Cell Jun 26 2009;137(7):1235e46.
196. Tamada K, Tomonaga S, Hatanaka F, et al. Decreased exploratory activity in a mouse model of 15q duplicationsyndrome; implications for disturbance of serotonin signaling. PLoS One 2010;5(12):e15126.
197. Smith SE, Zhou YD, Zhang G, Jin Z, Stoppel DC, Anderson MP. Increased gene dosage of Ube3a results in autismtraits and decreased glutamate synaptic transmission in mice. Sci Transl Med Oct 5 2011;3(103). 103ra197.
198. Moy SS, Nadler JJ, Young NB, Nonneman RJ, Segall SK, Andrade GM, et al. Social approach and repetitivebehavior in eleven inbred mouse strains. Behav Brain Res Aug 5 2008;191(1):118e29.
199. Moy SS, Nadler JJ, Young NB, Perez A, Holloway LP, Barbaro RP, et al. Mouse behavioral tasks relevant toautism: phenotypes of 10 inbred strains. Behav Brain Res Jan 10 2007;176(1):4e20.

REFERENCES 279
200. McFarlane HG, Kusek GK, Yang M, Phoenix JL, Bolivar VJ, Crawley JN. Autism-like behavioral phenotypes inBTBR Tþtf/J mice. Genes Brain Behav Mar 2008;7(2):152e63.
201. Pobbe RL, Pearson BL, Defensor EB, Bolivar VJ, Blanchard DC, Blanchard RJ. Expression of social behaviors ofC57BL/6J versus BTBR inbred mouse strains in the visible burrow system. Behav Brain Res Dec 252010;214(2):443e9.
202. Yang M, Scattoni ML, Zhodzishsky V, Chen T, Caldwell H, Young WS, et al. Social approach behaviors aresimilar on conventional versus reverse lighting cycles, and in replications across cohorts, in BTBR Tþ tf/J,C57BL/6J, and vasopressin receptor 1B mutant mice. Front Behav Neurosci 2007;1:1.
203. Insel TR. The challenge of translation in social neuroscience: a review of oxytocin, vasopressin, and affiliativebehavior. Neuron Mar 25 2010;65(6):768e79.
204. Yizhar O, Fenno LE, Prigge M, Schneider F, Davidson TJ, O’Shea DJ, et al. Neocortical excitation/inhibitionbalance in information processing and social dysfunction. Nature Sep 8 2011;477(7363):171e8.
205. McPartland JC, Coffman M, Pelphrey KA. Recent advances in understanding the neural bases of autismspectrum disorder. Curr Opin Pediatr Dec 2011;23(6):628e32.
206. Yang M, Zhodzishsky V, Crawley JN. Social deficits in BTBR Tþtf/J mice are unchanged by cross-fosteringwith C57BL/6J mothers. Int J Dev Neurosci Dec 2007;25(8):515e21.
207. Pearson BL, Pobbe RL, Defensor EB, Oasay L, Bolivar VJ, Blanchard DC, et al. Motor and cognitive stereotypiesin the BTBR Tþtf/J mouse model of autism. Genes Brain Behav Mar 2011;10(2):228e35.
208. Silverman JL, Tolu SS, Barkan CL, Crawley JN. Repetitive self-grooming behavior in the BTBR mouse model ofautism is blocked by the mGluR5 antagonist MPEP. Neuropsychopharmacology Mar 2010;35(4):976e89.
209. Wahlsten D, Metten P, Crabbe JC. Survey of 21 inbred mouse strains in two laboratories reveals that BTBR T/þtf/tf has severely reduced hippocampal commissure and absent corpus callosum. Brain Res May 2 2003;971(1):47e54.
210. Bothe GWM, Solanki MN, Du W, Kusek GK, Auerbach RC, Manley K, et al. Genetic investigations of corpuscallosum abnormalities in Btbr tþ tf/j mice. Society for Neuroscience Washington D.C; 2011.
211. Badaruddin DH, Andrews GL, Bolte S, Schilmoeller KJ, Schilmoeller G, Paul LK, et al. Social and behavioralproblems of children with agenesis of the corpus callosum. Child Psychiatry Hum Dev Dec 2007;38(4):287e302.
212. Vidal CN, Nicolson R, DeVito TJ, Hayashi KM, Geaga JA, Drost DJ, et al. Mapping corpus callosum deficits inautism: an index of aberrant cortical connectivity. Biol Psychiatry Aug 1 2006;60(3):218e25.
213. Hardan AY, Minshew NJ, Keshavan MS. Corpus callosum size in autism. Neurology Oct 10 2000;55(7):1033e6.214. Hardan AY, Pabalan M, Gupta N, Bansal R, Melhem NM, Fedorov S, et al. Corpus callosum volume in children
with autism. Psychiatry Res Oct 30 2009;174(1):57e61.215. Frazier TW, Hardan AY. A meta-analysis of the corpus callosum in autism. Biol Psychiatry Nov 15 2009;66(10):
935e41.216. Paul LK. Developmental malformation of the corpus callosum: a review of typical callosal development and
examples of developmental disorders with callosal involvement. J Neurodev Disord Mar 2011;3(1):3e27.217. Clapcote SJ, Roder JC. Deletion polymorphism of Disc1 is common to all 129 mouse substrains: implications
for gene-targeting studies of brain function. Genetics Aug 2006;173(4):2407e10.218. Koike H, Arguello PA, Kvajo M, Karayiorgou M, Gogos JA. Disc1 is mutated in the 129S6/SvEv strain and
modulates working memory in mice. Proc Natl Acad Sci U S A Mar 7 2006;103(10):3693e7.219. State MW, Levitt P. The conundrums of understanding genetic risks for autism spectrum disorders. Nat
Neurosci 2011;14(12):1499e506.220. Rooms L, Kooy RF. Advances in understanding fragile X syndrome and related disorders. Curr Opin Pediatr
Dec 2011;23(6):601e6.221. Deakin JF, Lees J, McKie S, Hallak JE, Williams SR, Dursun SM. Glutamate and the neural basis of the
subjective effects of ketamine: a pharmaco-magnetic resonance imaging study. Arch Gen Psychiatry Feb2008;65(2):154e64.
222. Gaisler-Salomon I, Schobel SA, Small SA, Rayport S. How high-resolution basal-state functional imaging canguide the development of new pharmacotherapies for schizophrenia. Schizophr Bull Nov 2009;35(6):1037e44.
223. Gozzi A, Large CH, Schwarz A, Bertani S, Crestan V, Bifone A. Differential effects of antipsychotic and gluta-matergic agents on the phMRI response to phencyclidine. Neuropsychopharmacology Jun 2008;33(7):1690e703.
224. Littlewood CL, Jones N, O’Neill MJ, Mitchell SN, Tricklebank M, Williams SC. Mapping the central effects ofketamine in the rat using pharmacological MRI. Psychopharmacology (Berl) May 2006;186(1):64e81.

9. TRANSLATIONAL NEUROIMAGING IN AUTISM SPECTRUM DISORDERS280
225. Musso F, Brinkmeyer J, Ecker D, London MK, Thieme G, Warbrick T, et al. Ketamine effects on brainfunctiondsimultaneous fMRI/EEG during a visual oddball task. Neuroimage Sep 15 2011;58(2):508e25.
226. Risterucci C, Jeanneau K, Schoppenthau S, Bielser T, Kunnecke B, von Kienlin M, et al. Functional magneticresonance imaging reveals similar brain activity changes in two different animal models of schizophrenia.Psychopharmacology (Berl) Aug 2005;180(4):724e34.
227. Stone JM. Imaging the glutamate system in humans: relevance to drug discovery for schizophrenia. Curr PharmDes 2009;15(22):2594e602.
228. Kim DI, Sui J, Rachakonda S, White T, Manoach DS, Clark VP, et al. Identification of imaging biomarkers inschizophrenia: a coefficient-constrained independent component analysis of the mind multi-site schizophreniastudy. Neuroinformatics Dec 2010;8(4):213e29.
229. Pantelis C, Yucel M, Bora E, Fornito A, Testa R, Brewer WJ, et al. Neurobiological markers of illness onset inpsychosis and schizophrenia: The search for a moving target. Neuropsychol Rev Sep 2009;19(3):385e98.
230. Sun D, van Erp TG, Thompson PM, Bearden CE, Daley M, Kushan L, et al. Elucidating a magnetic resonanceimaging-based neuroanatomic biomarker for psychosis: classification analysis using probabilistic brain atlasand machine learning algorithms. Biol Psychiatry Dec 1 2009;66(11):1055e60.
231. Ertugrul A, Volkan-Salanci B, Basar K, Karli Oguz K, Demir B, Ergun EL, et al. The effect of clozapine onregional cerebral blood flow and brain metabolite ratios in schizophrenia: relationship with treatmentresponse. Psychiatry Res Nov 30 2009;174(2):121e9.
232. Hagino H, Tabuchi E, Kurachi M, Saitoh O, Sun Y, Kondoh T, et al. Effects of D2 dopamine receptor agonistand antagonist on brain activity in the rat assessed by functional magnetic resonance imaging. Brain Res Dec 71998;813(2):367e73.
233. Ho BC, Andreasen NC, Ziebell S, Pierson R, Magnotta V. Long-term antipsychotic treatment and brainvolumes: a longitudinal study of first-episode schizophrenia. Arch Gen Psychiatry Feb 2011;68(2):128e37.
234. Nordquist RE, Risterucci C, Moreau JL, von Kienlin M, Kunnecke B, Maco M, et al. Effects of aripiprazole/OPC-14597 on motor activity, pharmacological models of psychosis, and brain activity in rats. Neuropharma-
cology Feb 2008;54(2):405e16.235. Puri BK. Brain tissue changes and antipsychotic medication. Expert Rev Neurother Jul 2011;11(7):943e6.236. Roder CH, Hoogendam JM, van der Veen FM. FMRI, antipsychotics and schizophrenia. Influence of different
antipsychotics on BOLD-signal. Curr Pharm Des 2010;16(18):2012e25.237. Sambataro F, Blasi G, Fazio L, Caforio G, Taurisano P, Romano R, et al. Treatment with olanzapine is associated
with modulation of the default mode network in patients with Schizophrenia. Neuropsychopharmacology Mar2010;35(4):904e12.
238. Szulc A, Galinska B, Tarasow E, Waszkiewicz N, Konarzewska B, Poplawska R, et al. Proton magnetic reso-nance spectroscopy study of brain metabolite changes after antipsychotic treatment. Pharmacopsychiatry Jun2011;44(4):148e57.
239. van Veelen NM, Vink M, Ramsey NF, van Buuren M, Hoogendam JM, Kahn RS. Prefrontal lobe dysfunctionpredicts treatment response in medication-naive first-episode schizophrenia. Schizophr Res Jul 2011;129(2e3):156e62.

![Enhanced Visual Functioning in Autism: An ALE ... - BrainMap · ces [Caron et al., 2006; Soulie`res et al., 2009]. Several neuroimaging studies have revealed stronger task-related](https://img.dokumen.tips/doc/110x75/5e0a1d1055ca481301152340/enhanced-visual-functioning-in-autism-an-ale-ces-caron-et-al-2006-soulieres.jpg)