Embed Size (px)
Citation preview

www.jecgonline.com
Journal of Electrocard
Transient pathologic Q waves in a case of apical ballooning
Pablo Robles, MD,4 Jose Julio Jimenez, MD, Isabel Monedero, MD, Ana Isabel Huelmos, MDDepartament of Cardiology, Fundacion Hospital Alcorcon, Madrid, Spain
Received 5 November 2006
Presentation
A 73-year-old woman with known mild systemic
hypertension was admitted to our hospital because of a 2-
hour history of chest pain. As a remarkable fact, her
husband had died that day. Physical examination showed a
normal blood pressure (130/60 mm Hg) and a heart rate of
100 beats per minute. Hematologic values and serum
creatinine levels were normal. Sodium and potassium serum
levels were also within normal limits. Initial serum creatine
kinase (CK) level was slightly increased (220 U/L; reference
range, 24-170 U/L), with a troponin I level of 11.8 lg/mL
(normal values up to 0.4 lg/mL). Chest x-ray was
unremarkable. The first electrocardiogram (EKG) was
performed when the patient still had chest pain and showed
Q waves and ST elevation in all the precordial leads and
leads I, II, and aVL (Fig. 1). Simultaneously, 2-dimensional
echocardiography was carried out showing apical akinesis
and mild ventricular dysfunction accompanied by ventric-
ular dilatation. With the diagnosis of extensive acute
anterior myocardial infarction (AMI), an urgent coronarog-
raphy was undertaken to perform a primary angioplasty, but
the coronary angiogram revealed a normal coronary tree.
Left ventriculogram demonstrated extensive apical akinesis
with hypercontractility of the basal segments (Fig. 2). An
ejection fraction of 0.35 was calculated. Peak CK and
troponin I serum levels were 2005 U/L and 31 lg/mL,
respectively. An EKG performed 5 days later showed deep
negative T waves in precordial leads, but Q waves could not
be observed (Fig. 3). Three weeks after admission, a 2-
dimensional echocardiography showed normal ventricular
function with no regional motion abnormalities. An almost-
normal EKG was obtained with absence of Q waves and
ST-T abnormalities (Fig. 4).
Diagnosis
The presence of pathologic Q waves in EKG is
traditionally considered as evidence of established AMI.
0022-0736/$ – see front matter D 2007 Elsevier Inc. All rights reserved.
doi:10.1016/j.jelectrocard.2007.02.003
4 Corresponding author. Pablo Robles, MD, Unidad de Cardiologıa,
Avda Budapest n8 1 28922, Alcorcon 28922, Madrid, Spain. Tel.: +34 91
6817330; fax: +34 916817330.
E-mail addresses: [email protected], [email protected]
Abnormal Q waves are one of the most reliable markers of
myocardial necrosis. Pathologic and experimental studies
also support this assertion.
Although their disappearance on a long-term basis has
been well described in 5% to 25% of heart attacks and, more
often than not, in inferior AMI, their disappearance for brief
periods is an infrequent entity. Profound ischemia may not
result in necrosis but may cause myocardial stunning that
can induce transient cell damage and, as a consequence, a
loss of electrical forces.
We describe the case of a patient with suspected AMI
who developed transient pathologic Q waves. The exact
mechanism for regression or disappearance of abnormal
Q waves remains uncertain. Transient EKG changes
resembling AMI with Q waves and ST-segment elevation
have been reported in a variety of clinical situations in
which evidence for myocardial necrosis was not apparent.
Such EKG changes resolved to normal within minutes or
days. Few reports showed cases in which exercise testing
induced a painless reversible EKG abnormality identical to
acute anterior AMI, and subsequent angiography revealed a
severe stenosis in the proximal left coronary artery.1
In recent years, patients have been reported to have a
clinical picture that resembles AMI before some stressful
condition but have normal coronary arteries and a takot-
subo-shaped left ventricle on ventriculography or echocar-
diography. This type of stress cardiomyopathy is known as
bapical ballooningQ (AB)2 or btakotsubo cardiomyopathy,Q3
and it has been reported more frequently in Japan.
We present a case of AB with transient abnormal Q
waves (TAQ). Transient abnormal Q waves are defined as
abnormal Q waves that disappear within days. They are
most often seen in patients with ischemic heart disease but
are also described in other cardiac and noncardiac
conditions summarized in Table 1. Brief episodes of
myocardial ischemia give rise to reversible biochemical
and ultrastructural myocardial changes resulting in transient
EKG changes and provide an accepted theory for the
pathogenesis of TAQ. Investigations have shown that the
occurrence of exercise-induced TAQ may be a symptom of
ischemic heart disease.4
The etiology and clinical features of this form of
reversible left ventricular dysfunction remain unclear.
iology 40 (2007) 489–492

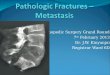
Fig. 1. Electrocardiogram 2 hours after admission. A QS pattern in leads V1 through V4 and ST elevation in leads I, aVL, and V2 through V6 were noted.
P. Robles et al. / Journal of Electrocardiology 40 (2007) 489–492490
Although provocative vasospasm has been confirmed in
some cases, multivessel epicardial spasm seems unlikely
because the abnormalities in contractility affect multiple
vascular territories. An alternative mechanism is microvas-
cular spasm. Abnormal coronary flow in the absence of
obstructive disease has recently been reported in patients
with stress-related myocardial dysfunction. Others have
demonstrated reduced coronary flow reserve and regional
defects on cardiac metaiodobenzylguanidine-enhanced im-
aging in such patients, suggesting the presence of sympa-
thetically mediated microcirculatory dysfunction.5
Some authors have demonstrated this kind of myocardial
ischemia without significant stenosis in an epicardial artery.
Management
The presence of Q waves in cases of AB were rarely
commented on in the literature. When this parameter was
Fig. 2. Left ventriculogram in systole showing extensive midventricul
analyzed, abnormal Q waves were present in between 20%
and 30% of patients.6
These abnormalities typically resolved in a few days
with restoration of normal R wave progression as in our
case. Also, the prolonged ST-segment elevation and
negative T waves observed in our patient have been related
to a severely dysfunctional but viable myocardium.
Furthermore, the persistent negative T waves have been
associated with denervation of the sympathetic nerve in
the jeopardized myocardium. Patients with AB compared
with those with AMI usually show asynergy in more
extensive areas and lower peak CK serum levels. Likewise,
patients with AB have a more rapid clinical and echocar-
diographic improvement.
The differentiation between patients with AB and those
with anterior acute AMI is difficult. Apical ballooning is an
acute cardiac syndrome that closely mimics ST-segment
elevation AMI leading to emergency thrombolysis or
coronary angiography in many patients. Previously pub-
ar and apical akinesis with hypercontractility of basal segments.

Fig. 3. Electrocardiogram 5 days later showed disappearance of Q waves, partial resolution of ST elevation, and development of giant negative Twaves in leads
with previous Q waves.
P. Robles et al. / Journal of Electrocardiology 40 (2007) 489–492 491
lished studies have tested the proposition that clinical and
EKG features may reliably differentiate AB from an acute
anterior AMI secondary to occlusion of the left anterior
descending coronary artery.7 Patients presenting with the
AB syndrome are usually postmenopausal women who
present with ischemiclike chest discomfort, ST-segment
elevation, small cardiac biomarker elevation, and charac-
teristic midventricular and apical wall motion abnormalities
in the absence of obstructive epicardial coronary disease.
Patients with AB develop symptoms proximate to an acute
emotional stress. The patients with AB have similar EKG
Fig. 4. Electrocardiogram 20 days later revealed a
findings to patients with anterior AMI infarct but with less
prominent ST-segment elevation in the anterior precordial
EKG leads. The clinical predictive value of the clinical and
EKG features in an individual patient was not sufficient to
reliably exclude AMI. The only reliable way to prospec-
tively distinguish AB from anterior AMI is coronary
angiography to document the absence or presence of
obstructive epicardial coronary atherothrombosis and left
ventriculography or echocardiography to demonstrate
the characteristic apical and midventricular wall motion
abnormalities.8
bsence of Q waves and ST-T abnormalities.

Table 1
Causes of transient Q waves
Extracardiac pathologies
Subarachnoid hemorrhage
Pancreatitis
Bronchial asthma
Phosphoric intoxication
Pulmonary embolism
Spontaneous pneumothorax
Ischemic heart disease
Treadmill tests
Angina crisis in Prinzmetal angina
Early reperfusion in acute coronary syndromes
Other cardiac disease
Myocarditis
Unknown mechanism
Apical ballooning syndrome
Technical problems
Electrode misplacement
P. Robles et al. / Journal of Electrocardiology 40 (2007) 489–492492
There is not a specific treatment for this entity. Some
authors recommend avoiding the use of pressor agents and
b-agonists because of the significant catecholamine release
observed in patients with AB.
Articles Appearing
Acquisition
What is inside the electrocardiograph?—Richard Gregg, MSEE;
MSEE; Karen Giuliano, PhD
Clinical diagnosis
Referral of patients with ST-elevation acute myocardial infarctio
teletransmission of 12-lead electrocardiogram—Martin Sillesen;
Freddy Lippert; Peter Clemmensen, MD
Mini-Symposium on ECG Waveform Ch
e-pub: Relation between P-wave dispersion and left ventricular geo
Mustafar Gur, MD; Remzi Yilmaz, MD; Recep Demirbag, MD; S
P-wave duration and dispersion in patients with coronary slow
Infarction frame count—Sait M. Dogan; Metin Gursurer; Must
e-pub: P-wave and QRS complex measurements in patients un
Madias, MD; Asma Yazidi, MD; Mohammed Bennani, MD; Ah
Tahiri, MD
Letter to the Editor: Interatrial block: a prevalent widely neglecte
David Spodick, MD
High prevalence of widened P waves among pediatric patien
Ariyarajah, MD; Debra O’Brien, CRT; Sirin Apiyasawat, MD; Dan
Relation of admission QRS duration with development of angiog
infarction treated with primary percutaneous interventions—O
MD; Hatice Selcuk, MD; Omer Alyan, MD; Tolga Aksu, MD; F
MD; Ahmet Demir, MD; Yucel Balbay, MD; Erdogan Ilkay, M
R-wave amplitude response to myocardial ischemia in hyper
Yoshiki Akakabe, MD; Michiyo Yamano, MD; Shigeyuki M
Kuribayashi, MD, PhD; Hiroki Sugihara, MD, PhD
References
1. West JN, Bennett MR, Pentecost BL. Association of transient abnormal
Q-waves during exercise testing with a stenosis of the main stem of the
left coronary artery. Int J Cardiol 1991;31:102.
2. Korlakunta HL, Thambidorai SK, Denney SD, Khan IA. Transient left
ventricular apical ballooning: a novel heart syndrome. Int J Cardiol
2005;102:351.
3. Akashi YJ, Nakazawa K, Sakakibara M, Miyake F, Musha H, Sasaka K.
123I-MIBG myocardial scintigraphy in patients with btakotsuboQcardiomyopathy. J Nucl Med 2004;45:1121.
4. Godballe C, Hoeck HC, Sorensen JA. Transient abnormal Q-waves.
Ugeskr Laeger 1990;152:92.
5. Wittstein IS, Thiemann DR, Lima JA, et al. Neurohumoral features of
myocardial stunning due to sudden emotional stress. N Engl J Med
2005;352:539.
6. Donohue D, Movahed MR. Clinical characteristics, demographics and
prognosis of transient left ventricular apical ballooning syndrome. Heart
Fail Rev 2005;10:311.
7. Inoue M, Shimizu M, Ino H, et al. Differentiation between patients with
takotsubo cardiomyopathy and those with anterior acute myocardial
infarction. Circ J 2005;69:89.
8. Bybee KA, Motiei A, Syed I, et al. Electrocardiography cannot reliably
differentiate transient left ventricular apical ballooning syndrome from
anterior ST-segment elevation myocardial infarction. J Electrocardiol
2001;40:38, e1.
in Next Issue
Sophia Zhou, PhD; James Lindauer, MD; Eric Helfenbein,
n directly to the catheterization suite based on prehospital
Maria Sejersten; Soren Strange; Soren Loumann Nielsen;
anges in Common Clinical Syndromes
metric patterns in newly diagnosed essential hypertension—
elahattin Akyol, MD; Halil Altiparmak, MD
flow and its relationship with Thrombolysis in Myocardial
afa Aydin; Ezgi Kalaycioglu; Fatih Cam
dergoing hemodialysis—Abbdenasser Drighil, MD; John
med Bennis, MD; Beenyouness Ramdan, MD; Azzeddine
d and portenous abnormality—Vignendra Ariyarajah, MD;
ts in two separate hospitals—Ray Loo, MD; Vignendra
iel Silbert, MD; Stephen Katz, MD; David Spodick, MD, DSc
raphic no-reflow in acute ST-segment elevation myocardial
rhan Maden, MD; Fehmi Kacmaz, MD; Mehmet Selcuk,
atma Metin, MD; Omac Tufekcioglu, MD; Ramazan Atak,
D
trophic cardiomyopathy—Tatsuya Kawasaki, MD, PhD;
iki, MD, PhD; Tadaaki Kamitani, MD, PhD; Toshiro