Embed Size (px)
Citation preview
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 1/59
TRANSFUSION REACTIONS AND TRANSFUSION REACTIONS AND THEIR MANAGEMENT THEIR MANAGEMENT
ByAIDA ALAUDIN

8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 2/59
30/11/2549 MD-3 /49 2
Transfusion Reaction is any unfavorable transfusion-related
event occurring in a patient during or aftertransfusion of blood components
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 3/59
30/11/2549 MD-3 /49 3
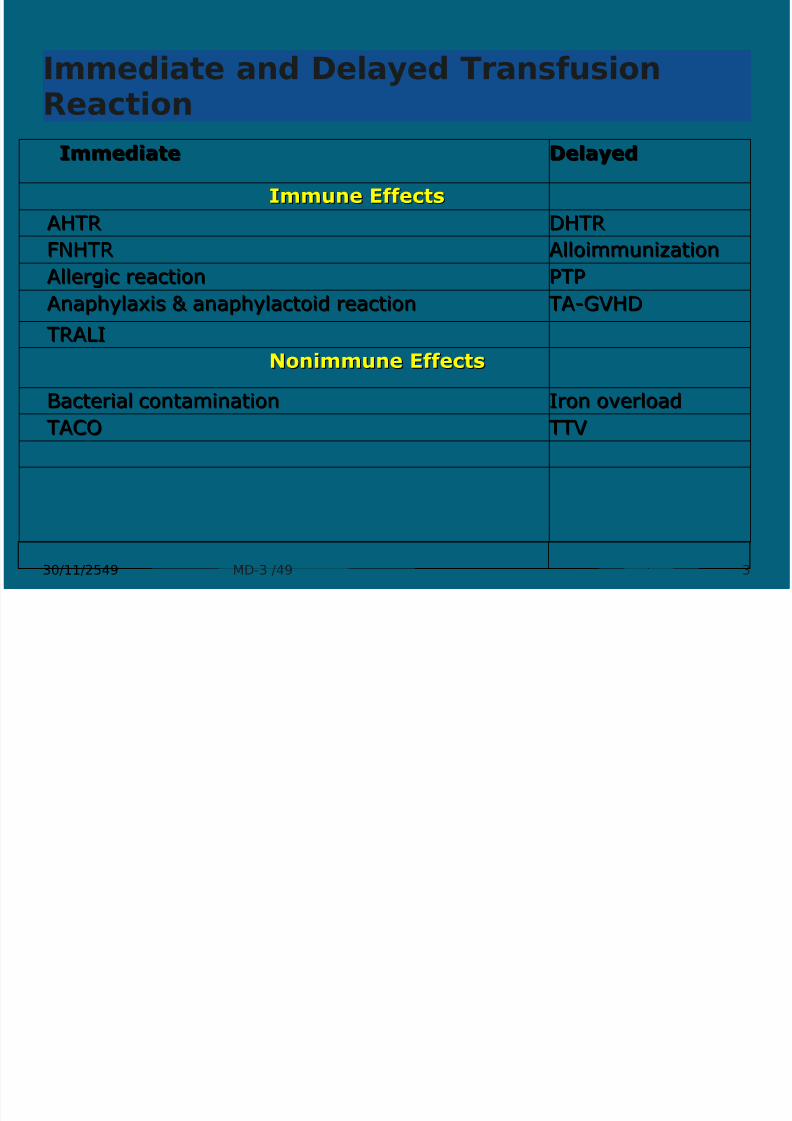
Immediate and Delayed TransfusionReaction
ImmediateImmediate DelayedDelayed
Immune EffectsImmune Effects
AHTRAHTR DHTRDHTR
FNHTRFNHTR AlloimmunizationAlloimmunization
Allergic reactionAllergic reaction PTPPTPAnaphylaxis & anaphylactoid reactionAnaphylaxis & anaphylactoid reaction TA-GVHDTA-GVHD
TRALITRALI
Nonimmune EffectsNonimmune Effects
Bacterial contaminationBacterial contamination Iron overloadIron overload
TACOTACO TTVTTV

8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 4/59
IMMUNE HAEMOLYTIC TRANSFUSIONREACTION
Defined as the destruction of red cells in therecipient of a transfusion caused by immunealloantibodies of red cells.

8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 5/59
30/11/2549 MD-3 /49 5
Acute Hemolytic TransfusionReaction
(Ab in recipient serum) + (Ag on RBC donor)
- Neuroendocrine responses
-Complement Activation
-Coagulation Activation
- Cytokines Effects
Acute hemolytic transfusion reaction
Pathophysiology
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 6/59
30/11/2549 MD-3 /49 6
Pathophysiology
Two mechanisms for RBCs destruction 1) Intravascular hemolysis
2) Extravascular hemolysis
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 7/5930/11/2549 MD-3 /49 7
Signs and Symptoms of
AHTRChills , feverHypotensionGeneralized bleeding
HemoglobinemiaHemoglobinuriaRenal failureDIC
Feelings of doom
Agitation
Facial flushing
Restlessness
Dyspnoea
Abdominal , chest orback pain
Pain along infusionvein
Nausea,vomiting
Diarrhoea
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 8/5930/11/2549 MD-3 /49 8
Acute Hemolytic Transfusion
Reactions
v -Acute onset within minutes or 1 2 hours
after transfuse incompatible blood
v -Most common cause is ABO incompatible
transfusion
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 9/59
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 10/5930/11/2549 MD-3 /49 10
Laboratory investigation for
AHTR10 ml of clotted blood labelled as post Tx sample 1 for
- repeat ABO and Rhesus grouping
- repeat compatibility test
- Ab screening and Direct Coomb’s Test
Send another sample 24 hours later and label as post Tx sample 2
Send FBC in EDTA tube
Send blood sample for biochemistry lab for
- serum electrolytes and renal profile
- serum bilirubin
Send blood for DIVC screening
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 11/5930/11/2549 MD-3 /49 11
Laboratory investigation for
AHTRUrine output should be monitored and presence of hemoglobinuria noted
ECG should be done to check for evidence of hyperkalemia
Urine should be sent to confirm presence of hemoglobinuria
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 12/59
30/11/2549 MD-3 /49 12
Treatment of AHTRDepends on
Amount of incompatible blood transfused
Specificity of the offending antibody Clinical severity of the reaction

8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 13/59
30/11/2549 MD-3 /49 13
TreatmentTreatment
u:Primary concerns
- vigorous treatment of hypotension
- promotion of renal blood flow
To prevent renal failure
Acute Hemolytic TransfusionReaction

8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 14/59
30/11/2549 MD-3 /49 14
Treatment of AHTR
Stop the transfusion immediately, inform bloodbank
IV line should be maintained with N/S infusion,initiall 20-30ml/kg to maintain SBP
Monitor vital signs and strict I/O chart(maintain urine output at 1-1.5ml/kg/hour
Maintain airway, give oxygen support if necessary
Administer IV Frusemide 1 mg/kg if urineoutput < 1ml/kg/hour
If patient is hypotensive, give inotrope IVdopamine 1 µg/kg/min

8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 15/59
30/11/2549 MD-3 /49 15
PreventionPrevention
upreventing or detecting errors in every phase of the transfusionpreventing or detecting errors in every phase of the transfusion
process :process :
usample acquisitionsample acquisition
uat all steps in laboratory testingat all steps in laboratory testinguat the time of issueat the time of issue
uat the time of transfusionat the time of transfusionuEnsuring that all clinical staff recognize signs and symptoms of Ensuring that all clinical staff recognize signs and symptoms of
acute reactionacute reaction
AHTR

8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 16/59
30/11/2549 MD-3 /49 16
Delayed Hemolytic TransfusionReaction
Most often the result of an anamnesticresponse (transfusion, pregnancy,transplantation )
Mild clinical signs and symptomsUnexpected or unexplained decreased in Hb or
Hct after transfusion should be investigate aspossible DHTR

8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 17/59
30/11/2549 MD-3 /49 17
Delayed Hemolytic Transfusion ReactionPathophysiology - 2 types of DHTR
1) secondary (anamnestic) response totransfused RBCs 3 – 7 day after Tx
2) primary alloimmunization longer - Extravascular hemolysis
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 18/59
30/11/2549 MD-3 /49 18
Delayed Hemolytic Transfusion Reaction
Signs & Symptoms
mild fever or fever with chill
mild anemia
mild to moderate jaundice
Uncommon hemoglobinemia,
Hemoglobinuria, shock, renal failure

8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 19/59
30/11/2549 MD-3 /49 19
Delayed Hemolytic Transfusion ReactionTherapy and Prevention - Goal of therapy is prevention - Treat severe complication if necessary - Alert to history of sensitization (previous transfusion, Pregnancy,
transplantation)
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 20/59
30/11/2549 MD-3 /49 20
Febrile Nonhemolytic TransfusionReaction
( FNHTR) Definition
Temperature increase of more or equal to1oC associated with transfusion, with nomedical explanation other than bloodtransfusion
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 21/59
30/11/2549 MD-3 /49 21
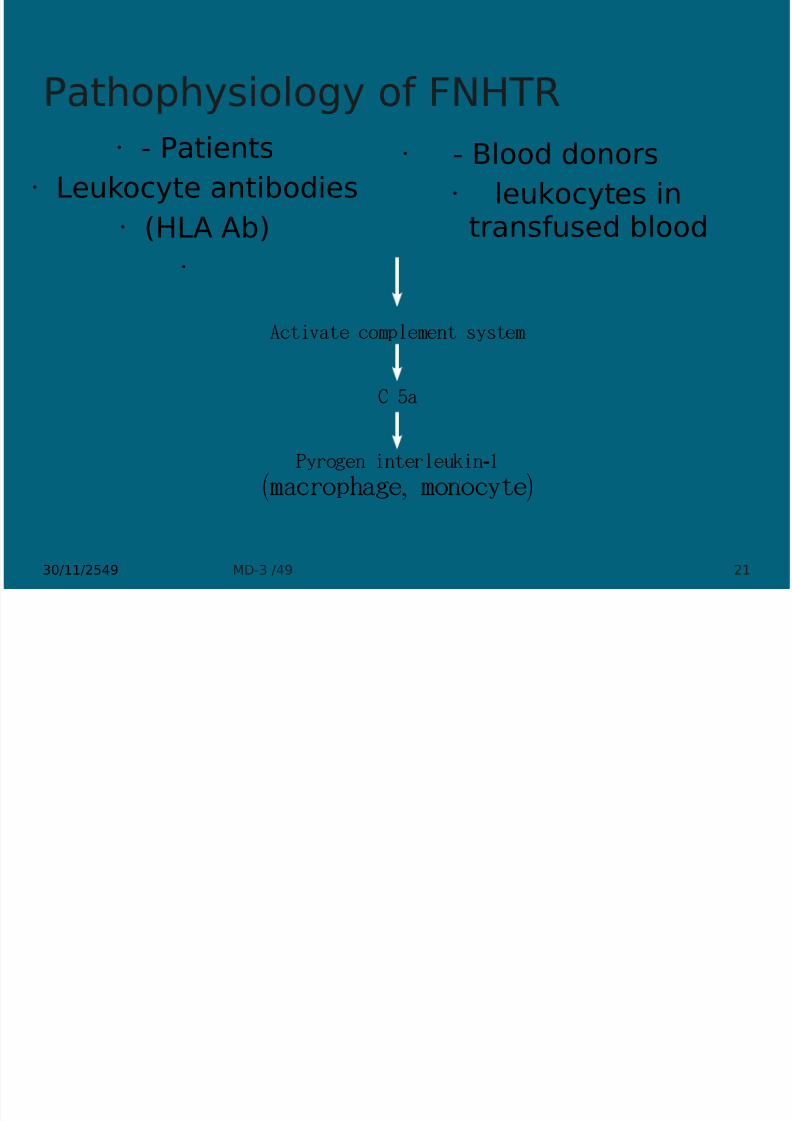
Pathophysiology of FNHTR - Patients
Leukocyte antibodies (HLA Ab)
- Blood donors leukocytes intransfused blood
Activate complement system
C 5a
-Pyrogen interleukin 1
( , )macrophage monocyte
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 22/59
30/11/2549 MD-3 /49 22
Febrile Nonhemolytic Transfusion
ReactionSigns & Symptoms
Fever with or without chills
most symptoms are mild
severe reaction :- headache,hypotension, cyanosis,tachycardia, tachypnea, dyspnea,
cough
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 23/59
30/11/2549 MD-3 /49 23
Febrile Nonhemolytic Reaction Febrile Nonhemolytic Reaction
Diagnosis of FNHTR is by exclusion of other causes of transfusionDiagnosis of FNHTR is by exclusion of other causes of transfusionreactio as fever could be due to acute hemolytic transfusionreactio as fever could be due to acute hemolytic transfusionreaction or by bacterially contaminated blood.reaction or by bacterially contaminated blood.
TreatmentTreatmentu
discontinued blood transfusion if the patient has severe reactiondiscontinued blood transfusion if the patient has severe reactionuAntipyretic for feverAntipyretic for feveruIf patient has experienced 2 or more FNHTR, tryIf patient has experienced 2 or more FNHTR, try
- paracetamol orally I hour before transfusion- paracetamol orally I hour before transfusion
- slow transfusion and keep the patient warm- slow transfusion and keep the patient warmu
PreventionPreventionuusing leucocyte- depleted blood componentsusing leucocyte- depleted blood components
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 24/59
30/11/2549 MD-3 /49 24
Allergic Transfusion Reactions
Probably the most frequent kind of reactionPathophysiology
Allergen – Reagin (IgE,IgG) Complex
attach mast cell (degranulation)
histamine/leukotrienes
Allergic reactions (urticaria)
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 25/59
30/11/2549 MD-3 /49 25
Allergic Transfusion Reactions
Signs & Symptoms - Urticaria (circumscribed areas of cutaneousedema and
itching) - severe reactions are rare
Therapy & Prevention - Stop transfusion temporarily while administering
antihistamine (Chlorpheniramine) by slow IV, transfusion can be continued if urticariais the only symptom. But if patientdevelops
extensive
urticariaor a confluent total body rash, it would be necessaryto
stop the transfusion, even if symptoms have responded to treatment. - For patients who have had severe or frequent minor urticaria
following transfusion, administering oral antihistamine 30 mins before

8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 26/59
30/11/2549 MD-3 /49 26
Anaphylactic and Anaphylactoid
reactions Anaphylaxis is a rare but life threatening
complication.
Pathophysiology- IgE antibody to IgA in donor plasma (anti-IgA antibodies)
- immediate generalized hypersensitivityreaction due to activity of IgE antibodies or thepresence of anti Ig-A in patients with congenitaldeficiency of IgA

8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 27/59
30/11/2549 MD-3 /49 27
Anaphylactic and Anaphylactoid
reactionsSigns & Symptoms - Anaphylactic generalized flushing,
coughing, dyspnea, nausea, vomiting,
bronchospasm, chest pain, hypotension,abdominal cramps, diarrhea, arrythmias,hypotension, syncope, sndit can progress toloss of consciousness, shock, and rarely
death. - Anaphylactoid (less severe) urticaria,
periorbital swelling, dyspnea, orperilaryngeal edema
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 28/59
30/11/2549 MD-3 /49 28
Anaphylactic and Anaphylactoidreactions
Therapy and PreventionStop transfusion
Keep IV line open with 0.9% saline
Maintain airway and give oxygen, neb Salbutamol
can also be given
Medication :-
- IM epinephrine then repeat every 10 minsaccording to
blood pressure and pulse rate until improvementoccurs
- slow IV of antihistamine
Wash RBCs and blood components
Transfuse IgA deficiency blood
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 29/59
30/11/2549 MD-3 /49 29
Transfusion-related Acute Lung Injury (TRALI)
Acute and severe type of transfusion reaction that can be fatal
Pathophysiology Leukocyte Ab in donor react with pt. leukocytes
Activate complements
Adherence of granulocytes to pulmonaryendothelium with release of proteolytic enzymes &
toxic O2
metabolites
Endothelial damage
Interstitial edema and fluid in alveoli
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 30/59
30/11/2549 MD-3 /49 30
Transfusion-related Acute Lung Injury
(TRALI)
Symptoms and signs
Fever
Non-productive coughHypotension
Tachypnea
Dyspnea
Diffuse pulmonary infiltration on X-rays
Clinical of noncardiogenic pumonary edema - within 4hours of transfusion
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 31/59
30/11/2549 MD-3 /49 31
Transfusion-related Acute Lung
Injury (TRALI)Therapy and Prevention
Manage in ICU setting as oxygen therapy andassissted ventilation are often required
Adequate respiratory and hemodynamic supportivetreatmentCorticosteroids might be helpfulIf antibodies are present, the blood center should
be notified so that the donor will be permanently
deferred from future donations.Patients who develop TRALI are unlikely to have
another reaction because it is most often donorspecific.
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 32/59
30/11/2549 MD-3 /49 32
Transfusion-associated Circulatory
Overload (TACO)Patients at significant risk
Children
Elderly patientsChronic anemia
Cardiac disease
Thalassemia major or Sickle cell disease
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 33/59
30/11/2549 MD-3 /49 33
Pathophysiology
Volume overload
Congestive heart failure
Pulmonary edema
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 34/59
30/11/2549 MD-3 /49 34
Symptoms and Signs
Dyspnea
CoughingCyanosis
Orthopnea
Chest discomfort
Headache
RestlessnessTachycardia
Systolic hypertensionincrease > 50
mm.Hg

8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 35/59
30/11/2549 MD-3 /49 35
Therapy & PreventionRapid reduction of hypervolemia
Respiratory and cardiac supportOxygen therapy
Diuretic
Therapeutic phlebotomy
- Use appropiate transfusion rate - Use appropiate blood components
T h e ra p y
Pre v e n tioPre v e n tio
nn
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 36/59
30/11/2549 MD-3 /49 36
Metabolic ReactionCitrate toxicity
Hyperkalemia
Hypothermia
Coagulopathy in massive transfusion
Air embolism
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 37/59
30/11/2549 MD-3 /49 37
Transfusion-associated Graft-versus-Host Disease ( TA-GVHD)
Patient at risk q Bone marrow
transplantationqChemotherapy
q Radiation treatment
qNewborn
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 38/59
30/11/2549 MD-3 /49 38
Transfusion-associated Graft-versus-Host
Disease ( TA-GVHD) Pathophysiology
Infusion of Immunocompetent Cells (Lymphocyte)
Patient at risk
proliferation of donor T lymphocytes
attack against patient tissue
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 39/59
30/11/2549 MD-3 /49 39
Graft-versus-Host ReactionSigns & Symptoms
§ ~Onset 3 to 30 days after transfusion§ –Clinical significant pancytopenia
§ ,Other effects include fever elevated
,liver enzymes
,copious watery diarrhea erythematousskin erythroderma
and desquamation
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 40/59
30/11/2549 MD-3 /49 40
Graft-versus-Host Reaction
Therapy :- , , ,Drugs corticosteroids methotrexate azathioprine:- , , ,Drugs corticosteroids methotrexate azathioprine
antithymocyte globulin antithymocyte globulin
But no adequate therapy But no adequate therapy
PreventionPrevention
( - )Irradiation of Blood Components 25 30 Gy( - )Irradiation of Blood Components 25 30 Gy
avoid potential fatalities avoid potential fatalities
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 41/59
30/11/2549 MD-3 /49 41
Iron overload~1 unit of PRCs has 250 mg of Iron
/Removed by body 1 mg day
accumulate iron Hemosiderosis
iron accumulate in tissue
Hemochromatosis
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 42/59
30/11/2549 MD-3 /49 42
Posttransfusion HemosiderosisAffected organ :- heart, liver, endocrine glands
Signs & Symptoms - muscle weakness, fatigue, weight loss, mild
jaundice, anemia, mild diabetes, and cardiacarrhythmia
Therapy Iron – chelating agentPrevention transfuse with young RBCs
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 43/59
30/11/2549 MD-3 /49 43
AlloimmunizationResult from prior exposure to donor bloodcomponents
Significant complication even small amount
of bloodAdverse effects may include
difficulty in finding compatible blood
transfusion reactionplatelet refractoriness
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 44/59
30/11/2549 MD-3 /49 44
AlloimmunizationPathophysiology
1st exposure moderate
production IgM and IgGantibody by foreign antigens
2nd exposure rapid
production of large amount of IgG
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 45/59
30/11/2549 MD-3 /49 45
AlloimmunizationSigns & Symptoms
mild slight fever and Hb
severe platelet refractorinesswith bleeding
Therapy & Prevention
depends on type and severity
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 46/59
30/11/2549 MD-3 /49 46
Posttransfusion PurpuraRare complication
Rapid onset of thrombocytopenia as a result of anamnestic production of platelet
alloantibodyUsually occurs in multiparous woman
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 47/59
30/11/2549 MD-3 /49 47
Posttransfusion PurpuraPathophysiology
Platelet Ab (anti-PLA1
) attach platelet
surface destruction by RES
Signs & Symptoms
Purpura and thrombocytopenia
occur
~ 1 – 2 weeks after transfusion
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 48/59
30/11/2549 MD-3 /49 48
Posttransfusion PurpuraTherapy and Prevention
Get expert advise from the
Transfusion MedicineDepartment
Corticosteroids combined withhigh dose of IVIg
Exchange transfusion
Plasmapheresis
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 49/59
30/11/2549 MD-3 /49 49
Bacterial contamination
reactionCause gram –ve, gram +ve bacteria most frequent – Yersinia enterocolitica
Pathophysiology
Bacteria growing in cold temperature
Produced endotoxin

8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 50/59
30/11/2549 MD-3 /49 50
Symptoms & SignsAcute onset within ~ 30 min after
transfusion
Dryness and flushing skin
Fever, hypotension, shaking chills, muscle
pain, vomitting, abdominal cramps, bloody
diarrhea, hemoglobinuria, shock, renalfailure, and DIC.
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 51/59
30/11/2549 MD-3 /49 51
Therapy & PreventionBroad – spectrum antibiotics
Symptomatic treatmentPrevention
ØPhlebotomy and blood components preparation &processing , thawing by sterile technique.
Therapy
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 52/59
30/11/2549 MD-3 /49 52
Transfusion – Transmitted DiseasesViral Infections
Hepatitis Viruses :- HBV, HCV
Retroviruses :- HIVHerpesviruses :- CMV, EBV
Parvovirus :- Human B19 parvovirus
Prion :- infectious particle of CJD
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 53/59
30/11/2549 MD-3 /49 53
Transfusion – Transmitted DiseasesBacterial Infection
Gram negative and positive
SyphilisLyme disease (Borrellosis)
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 54/59
30/11/2549 MD-3 /49 54
Transfusion – Transmitted DiseasesParasitic Infections
Malaria
Chagas disease
Toxoplasmosis
Leishmaniasis
S l i l T ti
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 55/59
30/11/2549 MD-3 /49 55
Serological Testingfor Infectious markers
HIV – Ag
Anti – HIV
HBsAgAnti – HCV
Test for syphilis
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 56/59
30/11/2549 MD-3 /49 56
Steps to take when a transfusion
reaction occursStop the transfusion immediately
Leave the needle in the vein and begin infusingnormal saline
Obtain vital signs
Begin O2
if pulmonary symptoms are
prominent
Carry out PE : lung, heart, skin, signs of abnormal bleeding
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 57/59
30/11/2549 MD-3 /49 57
Steps to take when a transfusion
reaction occursObtain a new blood sample for repeat RBCcompatibility test and inspection forhemolysis
Obtain a urine sample if the patient canvoid
Obtain a chest x-ray if pulmonary symptomare prominent
Make a preliminary assesment of thesituation
Begin definitive treatment
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 58/59
30/11/2549 MD-3 /49 58
- -Non Immune Mediated Hemolysis- -Non Immune Mediated Hemolysis
CausesCausesuPhysical or chemical destruction of Physical or chemical destruction of
blood: freezing, heating, hemolyticblood: freezing, heating, hemolytic
drugdrugusolution added to bloodsolution added to bloodu
Bacterial contaminationBacterial contaminationTreatmentTreatment
–depends on the causesdepends on the causesumild reaction supportive treatmentmild reaction supportive treatmentusevere reaction intensive treatmentsevere reaction intensive treatment
8/7/2019 TRANSFUSION REACTIONS AND THEIR MANAGEMENT
http://slidepdf.com/reader/full/transfusion-reactions-and-their-management 59/59
Thank you