Embed Size (px)
Citation preview

Research www.AJOG.org
OBSTETRICS
Transfusion ratios for postpartum hemodilutionalcoagulopathy: an in vitro thromboelastographic modelMichaela Kristina Farber, MD, MS; Neeti Sadana, MD; Richard Max Kaufman, MD; Xiaoxia Liu, BS;Bhavani Shankar Kodali, MD
OBJECTIVE: A 1:1:1 ratio of packed red blood cells (PRBC), fresh RESULTS: Maximum amplitude (MA) was lower compared to baseline
frozen plasma (FFP), and platelets (PLT) has been advocated fortrauma hemorrhage, but the effectiveness of this ratio for postpartumhemorrhage is unknown. We created an in vitro hemodilutional modelto investigate this strategy.STUDY DESIGN: Blood from 20 parturients at term was diluted 50%with 0.9% normal saline. Diluted samples were reconstituted with 1:1PRBC:FFP or 3:1 PRBC:FFP. In 10 samples, PLT were also added.Baseline, diluted, and reconstituted sample thromboelastographicvalues were compared.
From the Departments of Anesthesiology andPerioperative and Pain Medicine (Drs Farber andKodali and Ms Liu) and Pathology (Dr Kaufman),Brigham and Women’s Hospital, and theDepartment of Anesthesiology, Tufts UniversitySchool of Medicine (Dr Sadana), Boston, MA.
Received July 21, 2013; revised Oct. 28, 2013;accepted Nov. 18, 2013.
This research was supported by departmentalfunds from the Department of Anesthesiologyand Perioperative and Pain Medicine, Brighamand Women’s Hospital.
The authors report no conflict of interest.
Presented as a poster at the 42nd annualmeeting of the Society for ObstetricAnesthesiology and Perinatology, San Antonio,TX, May 12-16, 2010.
Reprints not available from the authors.
0002-9378/freeª 2014 Mosby, Inc. All rights reserved.http://dx.doi.org/10.1016/j.ajog.2013.11.029
For Editors’ Commentary,see Contents
values in both groups after 50% dilution with normal saline (P< .001)and remained lower than baseline despite reconstitution with 3:1:0 or1:1:0 PRBC:FFP:PLT (P < .0001) or 3:1:1 PRBC:FFP:PLT (P < .01).MA approached baseline (P ¼ not significant) in the samples with1:1:1 PRBC:FFP:PLT.
CONCLUSION: The addition of PLT to 1:1 PRBC:FFP optimized MA inthis in vitro hemodilutional model of postpartum hemorrhage.
Key words: dilutional coagulopathy, postpartum hemorrhage,thromboelastography, transfusion ratios
Cite this article as: Farber MK, Sadana N, Kaufman RM, et al. Transfusion ratios for postpartum hemodilutional coagulopathy: an in vitro thromboelastographic model.Am J Obstet Gynecol 2014;210:323.e1-7.
ostpartum hemorrhage (PPH) has
P been defined as blood loss>500mLwithin 24 hours of vaginal delivery,>1000 mL after cesarean delivery,1,2change in hematocrit of >10%, or needfor red blood cell transfusion.3-5 The
incidence of PPH is increasing in manyhigh-resource countries6-8; PPH in-creased from 2.3-2.9% (26%) in theUnited States from 1994 through 2006.8,9
Major obstetric hemorrhage, defined asblood loss of at least 2500 mL, trans-fusion of �5 U of blood, or transfusionof fresh frozen plasma (FFP), cryo-precipitate, or platelets (PLT), compli-cated 3.7 per 1000 births in the UnitedKingdom from 2005 through 2008.10,11
PPH remains a common and increasingsource of maternal morbidity and mor-tality worldwide, accounting for ap-proximately one-quarter of maternaldeaths per year.12
Transfusion recommendations formajor hemorrhage, defined as >10 U ofpacked red blood cells (PRBC) in 24hours, advocate more liberal use of FFPand PLT.13 An analysis of 246 soldierssuffering mass casualties in Iraq revealeda significant decrease in mortality whenlarge amounts of FFP were given,14 andtransfusion of 1:1:1 PRBC:FFP:PLT formassive trauma resuscitation improvedsurvival.15 Because obstetric hemor-rhage may be similar to trauma hemor-rhage in regards to rapid, unanticipated
APRIL 2014 Ameri
blood loss and risk of hemodilutionalcoagulopathy, some centers have em-pirically implemented transfusion pro-tocols for PPH that utilize a high FFPto PRBC ratio in addition to PLT trans-fusion.16 The use of point-of-care testingsuch as thromboelastography (TEG) forguiding hemostatic therapy during PPHhas also been advocated.17 The effec-tiveness of a 1:1:1 ratio of PRBC:FFP:PLTfor obstetric hemorrhage is unknown.
We designed an in vitro model ofobstetric hemodilutional coagulopathyusing TEG to study the efficacy of a 1:1PRBC:FFP transfusion ratio comparedto the traditional 3:1 PRBC:FFP ratio.The effect of adding PLT in vitro to either1:1 or 3:1 PRBC:FFP samples was alsoevaluated.
MATERIALS AND METHODS
After institutional review board approvalandwritten informed consent, 20 healthyparturients aged 18-40 years with un-complicated pregnancies at term gesta-tion (37-41 weeks) presenting in earlylabor were recruited. Exclusion criteriaincluded a history of hypertension, pre-eclampsia, gestational diabetes, diabe-tes mellitus, preexisting coagulopathy,history of deep vein thrombosis or
can Journal of Obstetrics & Gynecology 323.e1

Research Obstetrics www.AJOG.org
pulmonary embolism, or use of medi-cations that enhanced or impairedcoagulation. Women in active labor orwho were receiving intravenous fluid,oxytocin, prostaglandin therapy, orepidural analgesia at the time of consentand blood draw were also excluded. Asingle blood sample was collected fromparticipants within an hour of consent, atleast 3 hours prior to delivery. No pa-tients enrolled in this study experiencedPPH coincidental to study participation.
Two sets of 10 subjects were recruitedto participate in this study (groups 1and 2). Blood was obtained for completeblood cell count and TEG studies atthe time of venipuncture and insertionof an 18-gauge intravenous catheter. Thefirst 2 mL of blood was discarded toavoid tissue contamination, then venousblood was collected into 4 citratedVacutainers (BectonDickinson, FranklinLakes, NJ), each with a maximum ca-pacity of 2.7 mL of blood and containing0.5 mL 0.109 molar, 3.2% sodium
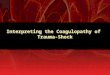
FIGURE 1Thromboelastography sample cup de
Pin attached to torsion wire is suspended in cup co
rate of 4.45 degrees every 10 seconds (4�45’). Aselectrical transducer to signal that is recorded by c
Reprinted with permission from Wolters Kluwer Health.
323.e2 American Journal of Obstetrics & Gynecol
citrate. Citrated blood from each Vacu-tainer from a single patient was pooled toeliminate variability in citrate concen-tration between samples.Three physicians (M.K.F., N.S., and
B.S.K.) trained to perform TEG pro-cessed all samples. Two Haemoscopedual-channel TEG analyzers (model5000; Haemoscope Corp, Niles, IL) with4 channels and disposable plastic cupsand pins were used for this study. Ana-lyzers were calibrated daily for qualitycontrol as per manufacturer guidelines.For analysis using TEG, 1 mL of wholeblood was added to a vial of standardizedkaolin for clot activation. After mixing bygentle inversion, 340 mL kaolin-activatedwhole blood was immediately added to aTEG analyzer cup prewarmed to 37�Cand containing 20 mL of 0.2 mol/L cal-cium chloride for citrate reversal.TEG is a real-time monitor of whole
blood coagulation that measures visco-elastic changes in the blood duringnormal and abnormal clot formation
sign
ntaining whole blood (0.36 mL); cup oscillates at
clot starts to form, torsion on pin is converted by
omputer over time.
ogy APRIL 2014
and fibrinolysis (Figure 1).18 TEG dem-onstrates initial fibrin formation, clotformation rate, clot strengthening, andeventual clot lysis (Figure 2). StandardTEG parameters were analyzed in termsof reaction (R) time (minutes), K time(minutes), a angle (degrees), andmaximum amplitude (MA; mm). R timeis the period of time from when blood isplaced in the TEG until initial fibrinformation, detected as 2 mm in ampli-tude above baseline on the TEG tracing.The R time (normal range, 4e8 mi-nutes) represents clotting factor functionand is prolonged by anticoagulants andshortened in hypercoagulable conditions.The K time is measured from R timeuntil a standardized level of clot firmness(20 mm amplitude on the TEG tracing;normal range, 1e4 minutes) is achieved,and represents speed of clot strength-ening. K time is shortened by an increasedfibrinogen level, to a lesser extent by PLTfunction, and is prolonged by anticoagu-lants. The a angle measures the slope ofthe TEG tracing from R time to K timeand inversely correlates with K time, witha larger a angle reflecting enhanced fibrindeposition and strength (normal range,47e74 degrees). The MA reflects overallclot strength determined by fibrin andPLT function, with a normal range of 55-73mmamplitude on theTEG tracing.18,19
For each patient in group 1, 4 sampleswere created from the citrated pooledwhole blood sample as follows: (1) con-trol: 1 mL whole blood; (2) hemodiluted:8 mL whole blood þ 8 mL 0.9% normalsaline; (3) 1:1:0 PRBC:FFP:PLT: reconsti-tution of diluted sample with PRBC, FFP,and PLT in a ratio of 1:1:0 (4 mL dilutedbloodþ 2mL PRBCþ 2mL FFP; no PLTadded); and (4) 3:1:0 PRBC:FFP:PLT:reconstitution of diluted sample withPRBC, FFP, and PLT in a ratio of 3:1:0(4 mL diluted blood þ 3 mL PRBC þ1 mL FFP; no PLT added).
In all, 1mLof each of these samples wasanalyzed using TEG within 30 minutes ofcollection. A PLT count and hematocritwere measured from the control andreconstituted samples by our institution’shematology laboratory (Sysmex XE 5000;Sysmex Corp, Hyogo, Japan).
The blood utilized for reconstitutionwas obtained from the institution’s

FIGURE 2Thromboelastography tracing parameters
Standard TEG parameters were analyzed, including reaction (R) time (minutes), K time (minutes; not
shown), a angle (degrees), and maximum amplitude (MA; mm).
TEG, thromboelastography.
Reprinted with permission from Wolters Kluwer Health.
TABLE 1Maternal demographic andobstetric dataDemographic n [ 20
Age, y 32 (6)
Weight, kg 85 (17)
Gestational age, wk 39.3 (1.1)
Parity 0 (0e4)
Ethnicity
Non-HispanicCaucasian
12 (60)
Hispanic 6 (30)
African American 1 (5)
Asian American 1 (5)
Age, weight, and gestational age are presented as mean(SD); parity is presented as median (range); ethnicity ispresented as n (%).
Farber. An in vitro thromboelastographic model forpostpartum hemodilutional coagulopathy. Am JObstet Gynecol 2014.
www.AJOG.org Obstetrics Research
blood bank. The PRBC (type O, anti-body negative) was stored at 4�C andused within 2 weeks of expiration. TheFFP (type O) was stored at e20�C. TheFFP was thawed and utilized within2 hours for this study.
In group 2, the same methodologywas used to obtain the baseline, diluted,and reconstituted samples, with theaddition of PLT to the reconstitutedsamples. PLT were added in a volumeof 1.2 mL to the reconstituted samples.The amount of PLT added was pre-determined to approximate a PLT countof 100,000/mm�3 based on pilot testingof PLT dilutions and resulting laboratorymeasurements. PLT aliquots were ob-tained by apheresis from healthy donorsand were provided by our institution’sblood bank. Reconstituted samples willbe referred to as follows: group 1,PRBC:FFP:PLT ¼ 1:1:0 and 3:1:0; group2, PRBC:FFP:PLT ¼ 1:1:1 and 3:1:1.
Statistical analysis of TEG and labo-ratory data was performed using soft-ware (SAS, version 9.3; SAS Institute,Cary, NC). Repeated measures analysisof variance with a mixed model ap-proach was used to analyze outcomes.Bonferroni adjusted pairwise compari-sons (to control for familywise errorrate) was performed to examine the ef-fect of different tests on TEG parameters.P < .05 was used to indicate statisticalsignificance. All analyses were 2-tailed.
A power calculation based on thecomparison of MA between the 2 groupsfor 1:1:0 and 3:1:0 was performed. Thecriterion for significance (a) was set at.05. The test was 2-tailed. With the pro-posed sample size of 10 and 10 for the 2groups, the study would have a power of99% to yield a statistically significantresult. This computation assumes that themean difference between MA is 12 mmand the commonwithin-group SD is 2.85mm. A 12-mm decrease in MA for thepower calculationwas based on a study inwhich this degree of reduction inMAwasassociated with significant bleeding aftercardiac surgery.20 Furthermore, a 12-mmdecrease in MA (20-25% decrease) willresult in MA values below normal rangeof MA in healthy pregnant subjects atterm gestation (66.7e70.3 mm).21 Asample size of 10 per group was based
on a previous in vitro hemodilutionalrotational thromboelastometry (ROTEM)study in which 8 patient samples wereused to demonstrate significantly im-paired hemostasis after 60% dilutionwith normal saline 0.9%.22
RESULTS
Demographic and obstetric data arepresented in Table 1. Results of TEGanalysis are shown in Table 2 for group 1and group 2.
Baseline and hemodiluted samplecomparisonFifty percent hemodilution of samples ingroups 1 and 2 significantly decreasedMA (reflecting a decrease in clot strength)compared to baseline MA (Table 2)(group 1: 68.7-57.5 mm; P < .0001; group2: 67.5-59.3 mm; P ¼ .0015). BaselineMA values in group 1 were not signifi-cantly different from baseline MA values
APRIL 2014 American Journal of Obstetrics & Gynecology 323.e3

TABLE 2Thromboelastographic and hematologic results
Group
Sample description
Baseline 50% dilution 3:1:0a 1:1:0b
Group 1: no added platelets
R time, min 6.1 (1.2) 5.9 (1.2) 5.7 (1.5) 5.1 (1.4)c
K time, min 1.4 (0.2) 1.8 (0.3) 2.9 (1.1)d 2.4 (0.8)d
a angle, degrees 67.7 (6.9) 64.3 (3.6) 54.0 (8.9)d 60.1 (7.3)d
MA, mm 68.7 (5.8) 57.5 (4.2)d 49.3 (5.0)d 51.0 (4.2)d
Hct, % 34.5 (2.1) e 27.7 (3.1)c 22.7 (2.4)c
Plt, 1000 mL�1 237 (60) e 61 (19)d 68 (16)d
Group 2: platelets added to3:1 and 1:1 samples
R time, min 5.8 (1.3) 6.0 (0.7) 5.1 (1.0) 4.8 (0.6)c
K time, min 1.4 (0.3) 1.6 (0.3) 1.2 (0.2)d,e 1.1 (0.2)d,e
a angle, degrees 65.8 (8.2) 66.7 (3.6) 70.8 (4.1)e 72.6 (6.1)d,e
MA, mm 67.5 (4.8) 59.3 (4.2)c 61.2 (2.7)c,e 63.2 (2.5)e
Hct, % 34.5 (2.9) e 24.0 (1.8)c 20.1 (2.6)c
Plt, 1000 mL�1 256 (65) e 189 (34)e 202 (52)e
Data presented as mean (SD).
a angle, clot formation rate; Hct, hematocrit; K, clot formation; MA, maximum amplitude; Plt, platelet count; R, reaction.
a 3 packed red blood cells:1 packed red blood cells:0 platelets; b 1 packed red blood cells:1 fresh frozen plasma:1 platelets;c P < .01 compared to baseline; d P < .001 compared to baseline; e P < .001 compared to values in group 1.
Farber. An in vitro thromboelastographic model for postpartum hemodilutional coagulopathy. Am J ObstetGynecol 2014.
Research Obstetrics www.AJOG.org
in group 2, and dilutedMAvalues in bothgroups were also similar (P ¼ .541 and.363, respectively). Hemodilution had noeffect on R time (time to initial clot for-mation), K time, or a angle (speed ofclot formation). Of note, hematocritand PLT count were not performed inhemodiluted samples for comparison tobaseline values.
Effect of reconstitution on R time:time to initial clot formationR time, time to initial clot formation,was not significantly longer in dilutedsamples compared to baseline samplesin groups 1 or 2 (P ¼ .691 and .372,respectively). R time decreased signifi-cantly in both samples reconstituted with1:1:0 and 1:1:1 (P ¼ .002, P ¼ .002).
Effect of reconstitution on K time anda angle: rate of clot formationK time, reflecting rate of clot forma-tion, was prolonged in the samplesreconstituted without PLT (1:1:0 and
323.e4 American Journal of Obstetrics & Gynecol
3:1:0) compared to baseline samples. Incontrast, K time decreased in the samplesreconstituted with PLT (1:1:1, 3:1:1) andwas significantly shorter compared to therespective reconstituted samples withoutPLT (1:1:0 and 3:1:0). This demonstratesa faster rate of clot formation in thesamples reconstituted with PLT.In group 1, a angle in both 1:1:0 and
3:1:0 PRBC:FFP:PLT decreased furtherfrom diluted samples and was sig-nificantly lower than baseline a angle(P < .001 and P < .001, respectively). Ingroup 2, reconstitution with both 1:1:1and 3:1:1 PRBC:FFP:PLT increased the aangle (P ¼ .003 and P ¼ .030, respec-tively). Along with a decrease in K time,the increase in a angle is consistent witha faster rate of clot formation in thesamples reconstituted with PLT.
Effect of reconstitution on PLT andMA: clot strengthIn group 1, the PLT count was signifi-cantly lower in both the 1:1:0 and the
ogy APRIL 2014
3:1:0 combinations compared to baselinePLT count (P < .001 and P < .001,respectively). In group 2, the PLT countincreased toward baseline values in bothreconstituted samples.
In group 1,MA remained significantlylower than baseline MA despite recon-stitution with either a 1:1:0 or 3:1:0 ratio(Table 2) (P < .0001 and P < .0001,respectively). MA was lower in the sam-ples reconstituted with either 1:1:0 or3:1:0 compared to diluted MA as well(P < .0001 and P < .0001, respectively).With the addition of PLT (group 2), MAincreased significantly in the 1:1:1 sam-ples compared to diluted samples (from59.3-63.2 mm, Table 2) (P ¼ .043),approaching baseline MA (P ¼ not sig-nificant from baseline). In 3:1:1 samples,the increase in MA (from 59.3-61.2) isnot statistically significant in compari-son to diluted samples (P ¼ .307) andMA in this group remained significantlylower than baseline MA (P < .0001).
Although there was no significant dif-ference betweenTEG variables in baselineor diluted samples in groups 1 and 2, thea angle and MA of group 2 samplesreconstituted with 1:1:1 or 3:1:1 weresignificantly higher than correspondingvalues in group 1, 1:1:0 and 3:1:0 (P <.0025 and P < .001, respectively). Inaddition, K times in the reconstitutedsamples of group 2 were significantlylower than respective K times in group 1(P ¼ .0003).
COMMENT
Emerging transfusion protocols for mas-sive hemorrhage after trauma recom-mend 1:1:1 PRBC:FFP:PLT.13-15 Patientswho received higher ratios of PLT:PRBCafter trauma and massive hemorrhagehad decreased blood loss, improved sur-vival, and decreased ventilator days.15
The optimal ratio of blood componentsfor massive PPH has not been deter-mined. The obstetric patient is pro-foundly different from a nonpregnantpatient; marked plasma volume expan-sion with a lesser increase in hemoglobinleads to a hemodilutional anemia atbaseline. Incidental thrombocytopeniaoccurs in 7.6% of women in the thirdtrimester of gestation and is attributedto expansion of maternal plasma volume

www.AJOG.org Obstetrics Research
as well as PLT consumption in the ute-roplacental unit.23 Many procoagulantfactors increase in pregnancy, whileanticoagulant factors such as proteins Cand S decrease. Hypofibrinolysis occursdue to increased plasminogen activatorinhibitor. Based on these differences,it is prudent to determine whetherPRBC:FFP:PLTratios optimal for traumahemorrhage are applicable to the man-agement of PPH. Our study suggests thatthe coagulation defects created by thehemodilution of blood from pregnantpatients at term can best be correctedtoward baseline values with PRBC andFFP in the ratio of 1:1 and the addition ofPLT.
Hemodilution 50% by volume withcrystalloid solution significantly decreasedMA, reflecting decreased clot strengthdetermined largely by PLT and to a lesserextent by fibrinogen activity. None ofthe other TEG parameters analyzed,including R time (time to initial clot for-mation; determined largely by procoagu-lant factor activity), K time, or a angle(rate of clot strengthening, both deter-mined largely by fibrinogen effectiveness)were altered by hemodilution in thismodel, suggesting that 50% crystalloiddilution of blood from pregnant patientsat term gestation does not decreaseclotting factors or fibrinogen levels suf-ficiently enough to alter these TEG var-iables. This is in contrast to previousin vitro models unrelated to pregnancywhere fibrinogen was the first factor tobecome critically low.22,24,25 The differ-ence may be due to pregnancy-inducedincreases in the baseline fibrinogenlevels (100%) and other clotting factors(20-100%) in this study compared tostudies in nonpregnant patients.26,27
Fibrinogen is a prerequisite for clotformation and is the first hemostaticcomponent that declines followingtrauma and hemodilution in nonpreg-nant subjects.28,29 A decrease in MAwith no impact on a angle or K timesuggests that pregnant women may bemore vulnerable to decreased PLT con-centration than from decreased clottingfactors and fibrinogen when hemodilu-tion occurs. This inference is furtherstrengthened by the TEG results inreconstituted samples in our study.
There was no significant improvementin MA after reconstitution with 3:1:0 or1:1:0 PRBC:FFP:PLT; the efficacy of the1:1 PRBC:FFP ratio occurred only afterPLT were added. This in vitro modelsuggests that PLT contribution may beas vital as liberal plasma for restoring clotstrength after hemodilution during PPH.A significantly higher a angle and
shorter K time in the 1:1:1 PRBC:FFP:PLTsamples was observed, representing en-hanced kinetics of clot formation. Alphaangle and K time are reciprocally relatedand reflect fibrinogen-PLT interactionduring clot formation. Alpha angle is anindirect measure of fibrinogen, andfaster clot strengthening kinetics medi-ated by enhanced fibrinogen and PLTinteractions are reflected by a larger aangle and a shorter K time. The mostsuperior clot strengthening kinetics inthis in vitro study, reflected by a larger aangle and shorter K time, were seen inthe reconstituted samples with 1:1:1PRBC:FFP:PLT. The addition of PLTimproved clot strength (MA) in both1:1:1 and 3:1:1 samples (61.2 vs 63.2), abetween-group difference that is likelyto have no clinical relevance. However,the addition of PLT in the 1:1:1 samplesalso enhanced the rate of clot strength-ening, yielding a shorter K time andlarger a angle. Taken together, the TEGresults of 1:1 samples with PLT reflectsuperior global coagulation comparedto other samples.To our knowledge, this is the first
study to evaluate the effects of trans-fusion ratios using an in vitro obstetrichemodilutional model. The findings ofour study suggest superiority of a 1:1ratio of PRBC: FFP over a 3:1 PRBC:FFPratio and the potential benefit of PLT inthis setting. In our in vitro model, a PLTcount of 50,000/mm�3 was found to beinadequate despite a 1:1 PRBC:FFP ratioof blood products added to the dilutedsample. The significance of PLT in PPHhas been suggested in vivo: womenwith a PLT count of <100,000/mm3 orfibrinogen concentration of <2.9 g/L�1
during labor had an increased incidenceof PPH (odds ratio, 19.7).30 Althoughour study cannot define the minimumPLT count needed for optimal coagula-tion, the range of PLT counts in
APRIL 2014 Ameri
the 1:1:1 PRBC:FFP:PLT ranged from112,000e255,000/mm�3. Further eval-uation of PLT count and qualitativeanalysis of clot strength using TEG dur-ing in vivo PPH may define the optimalthreshold for PLT transfusion in PPH. Aretrospective evaluation of severe PPHutilizing high FFP:PRBC transfusionratios showed lower odds for requiringinterventional procedures compared tohigher PRBC:FFP ratios.31 The impactthat PLT may have had on the study re-sults cannot be defined due to theretrospective nature of the study andchanging transfusion protocols over thestudy duration.31
We utilized TEG in our study, al-though investigators have historicallyrelied on prothrombin time, activatedpartial thromboplastin time, PLT count,and fibrinogen levels to guide transfusiontherapy. Unlike TEG, prothrombin time,activated partial thromboplastin time,PLT count, andfibrinogen levels are statictests of coagulation that do not reveal thequalitative effect that PLT have on globalhemostasis. TEG and ROTEM can facil-itate resuscitation in trauma patients byproviding a global, dynamic assessmentof coagulation during severe hemor-rhage,32 and are increasingly advocatedfor the identification andmanagement ofhypocoagulability and hyperfibrinolysisthat can occur inmajor trauma.33-35 TEGand ROTEM point-of-care tests offer thepotential of rapid diagnosis and correc-tion of coagulopathic bleeding duringPPH.17 Based on the finding that earlyfibrinolysis in the setting of PPH isassociated with subsequent severe hem-orrhage,36 a randomized trial using fi-brinogen concentrate and hemostaticresponse using TEG monitoring duringPPH is currently underway.37 Standardreference ranges for TEG at term gesta-tion and a transfusion algorithm thatincorporates TEG values to guide trans-fusion has been published,38 furtherfacilitating the use of TEG for PPHmanagement.
A major limitation of this study is thatit is an in vitro model. The purpose ofour design was to mimic the knownhypercoagulable state of pregnancy andthe early stages of PPH when crystalloidresuscitation begins and blood product
can Journal of Obstetrics & Gynecology 323.e5

Research Obstetrics www.AJOG.org
transfusion is anticipated. We recognizethat this model cannot replicate tem-perature and pH change, hypocalcemia,and other humoral or systemic effectsthat occur during PPH in vivo. In addi-tion, it is not possible to recreate thecapillary endothelium in vitro, thus itseffect on coagulation cannot be evalu-ated by TEG. Nevertheless, TEG hasbeen successfully used to study the ef-fects of amniotic fluid, magnesium,oxytocin, and estrogen on coagulation inthe pregnant population.39-42 Furtherin vivo studies to determine the role ofPLT in PPH are needed.
In conclusion, our in vitro model ofhemodilution at term gestation suggeststhat a 1:1 ratio of PRBC:FFP providesoptimal clot strength in the presence ofPLT. Prospective randomized trials areneeded to analyze the benefit of a 1:1:1ratio of PRBC:FFP:PLT for resuscitationof massive PPH, and to define theoptimal PLT count in this setting. Thetransfusion of blood components is notwithout risk; high ratios of FFP and PLTto PRBC do not necessarily lower mor-tality in all transfused patients.43 The useof point-of-care hemostatic testing suchas TEG to guide transfusion for obstetrichemorrhage may optimize the ratio ofproducts administered. -
REFERENCES
1. Berg CJ, Atrash HK, Koonin LM, Tucker M.Pregnancy-related mortality in the UnitedStates, 1987-1990. Obstet Gynecol 1996;88:161-7.2. McClure JH, Cooper GM, Clutton-Brock TH;Center for Maternal and Child Enquiries. Savingmothers’ lives: reviewing maternal deaths tomake motherhood safer: 2006-8: a review. Br JAnaesth 2011;107:127-32.3. Arulkumaran S,Mavrides E, PenneyGC, et al.Prevention and management of postpartumhemorrhage. Royal College of Obstetricians andGynaecologists Green-top Guideline no. 52, May2009. Minor revision Nov 2009 and April 2011.4. Combs CA, Murphy EL, Laros RK Jr. Factorsassociated with postpartum hemorrhage withvaginal birth. Obstet Gynecol 1991;77:69-76.5. Combs CA, Murphy EL, Laros RK Jr. Factorsassociated with hemorrhage in cesarean de-liveries. Obstet Gynecol 1991;77:77-82.6. Cameron CA, Roberts CL, Olive EC, Ford JB,Fischer WE. Trends in postpartum hemorrhage.Aust N Z J Public Health 2006;30:151-6.7. Knight M, Callaghan WM, Berg C, et al.Trends in postpartum hemorrhage in high
323.e6 American Journal of Obstetrics & Gynecol
resource countries: a review and recommen-dations from the international postpartum hem-orrhage collaborative group. BMC PregnancyChildbirth 2009;9:55.8. Bateman BT, Berman MF, Riley L, Leffert L.The epidemiology of post partum hemorrhage ina large, nationwide sample of deliveries. AnesthAnalg 2010;110:1368-73.9. Callaghan WM, Kuklina EV, Berg CJ. Trendsin postpartum hemorrhage: United States,1994-2006. Am J Obstet Gynecol 2010;202:353-5.10. Cantwell R, Clutton-Brock T, Cooper G,Dawson A, Drife J, Garrod D, et al. Savingmothers’ lives: reviewing maternal deaths tomakemotherhood safer: 2006-2008. The eighthreport of the confidential enquiries into maternaldeaths in the United Kingdom. BJOG2011;118(Suppl):1-203.11. Brace V, Kernaghan D, Penney G. Learningfrom adverse clinical outcomes: major obstetrichemorrhage in Scotland, 2003-05. BJOG2007;114:1388-96.12. Department of Reproductive Health andResearch, WHO. WHO recommendations for theprevention and treatment of postpartum hemor-rhage.Geneva:WordHealthOrganization; 2012:3.13. Fries D, Innerhofer D, Shobersberger W.Time for changing coagulation management intrauma-related massive bleeding. Curr OpinAnesthesiol 2009;22:267-7.14. BorgmanMA, Spinella PC, Perkins JG, et al.The ratio of blood products transfused affectsmortality in patients receiving massive trans-fusions at a combat support hospital. J Trauma2007;63:805-13.15. Holcomb JB, Zarzabal LA, Michalek JE,et al. Increased platelet: RBC ratios are associ-ated with improved survival after massivetransfusion. J Trauma 2011;71(Suppl):S318-28.16. Burtelow M, Riley E, Druzin M, Fontaine M,Viele M, Goodnough LT. How we treat: man-agement of life-threatening primary postpartumhemorrhage with a standardized massivetransfusion protocol. Transfusion 2007;47:1564-72.17. Solomon C, Collis RE, Collins PW. Hemo-static monitoring during postpartum hemor-rhage and implications for management. Br JAnaesth 2012;109:851-63.18. Srinivasa V, Gilbertson LI, Bhavani-Shankar K. Thromboelastography: where is itand where is it heading? Int Anesthesiol Clin2001;39:35-49.19. Butwick A, Ting V, Ralls LA, Harter S,Riley E. The association between thromboelas-tographic parameters and total estimated bloodloss in patients undergoing elective cesareandelivery. Anesth Analg 2011;112:1041-7.20. Welsby IJ, Jiao K, Ortel TL, et al. Thekaolin-activated Thromboelastograph predictsbleeding after cardiac surgery. J CardiothoracVasc Anesth 2006;20:531-5.21. Karlsson O, Sporrong T, Hillarp A,Jeppsson A, Hellgren M. Prospective longitudi-nal study of thromboelastography and standardhemostatic laboratory tests in healthy women
ogy APRIL 2014
during normal pregnancy. Anesth Analg2012;115:890-8.22. De Lorenzo C, Calatzis A, Welsch U,Heindl B. Fibrinogen concentrate reverses dilu-tional coagulopathy induced in vitro by saline butnot by hydroxyethyl starch 6%. Anesth Analg2006;102:1194-200.23. Burrows RF, Kelton JG. Thrombocyto-penia at delivery: a prospective survey of 6715deliveries. Am J Obstet Gynecol 1990;162:731-4.24. Fries D, Innerhofer P, Reif C, et al. The effectof fibrinogen substitution on reversal of dilutionalcoagulopathy: an in vitro model. Anesth Analg2006;102:347-51.25. Haas T, Fries D, Velik-Salchner C, Reif C,Klingler A, Innerhofer P. The in vitro effects offibrinogen concentrate, factor XIII and freshfrozen plasma on impaired clot formation after60% dilution. Anesth Analg 2008;106:1360-5.26. Hui C, Lili M, Libin C, et al. Changes incoagulation and hemodynamics during preg-nancy: a prospective longitudinal study of 58cases. Arch Gynecol Obstet 2012;285:1231-6.27. Stirling Y, Woolf L, North WR,Seghatchian MJ, Meade TW. Hemostasis innormal pregnancy. Thromb Haemost 1984;52:176-82.28. Hiipala ST, Myllyla GJ, Vahtera EM. Hemo-static factors and replacement of major bloodloss with plasma-poor red cell concentrates.Anesth Analg 1995;81:360-5.29. Singbartl K, Innerhofer P, Radvan J, et al.Hemostasis and hemodilution: a quantitativemathematical guide for clinical practice. AnesthAnalg 2003;96:929-35.30. Simon L, Santi TM, Sacquin P, Hamza J.Pre-anesthetic assessment of coagulationabnormalities in obstetric patients: usefulness,timing, and clinical implications. Br J Anaesth1997;78:678-83.31. Pasquier P, Gayat E, Rackelboom T, et al.An observational study of the fresh frozenplasma: red blood cell ratio in postpartumhemorrhage. Anesth Analg 2013;116:155-61.32. Cushing M, Shaz BH. Blood transfusion intrauma patients: unresolved questions. MinervaAnestesiol 2011;77:349-59.33. Johansson PI, Stensballe J, Vindelov N,Perner A, Espersen K. Thomboelastographyand thromboelastometry in assessing coagul-opathy in trauma. Scand J Trauma ResuscEmerg Med 2009;17:45-52.34. Kashuk JL, Moore EE, Wohlauer M, et al.Initial experiences with point-of-care rapid throm-belastography for management of life-threateningpost-injury. Transfusion 2012;52:23-33.35. Johansson PI, Ostrowski SR, Secher NH.Management of major blood loss: an update.Acta Anaesthesiol Scand 2010;54:1039-49.36. Charbit B, Mandelbrot L, Samain E, et al;PPH Study Group. The decrease of fibrinogen isan early predictor of the severity of postpartumhemorrhage. J ThrombHaemost 2007;5:266-73.37. Wikkelsoe AJ, Afshari A, Stensballe J, et al.The FIB-PPH trial: fibrinogen concentrate asinitial treatment for postpartum hemorrhage:

www.AJOG.org Obstetrics Research
study protocol for a randomized controlled trial.Trials 2012;13:110.38. Hill JS, Devenie G, Powell M. Point-of-caretesting of coagulation and fibrinolytic statusduring postpartum hemorrhage: developing athromboelastography�-guided transfusion algo-rithm. Anaesth Intensive Care 2012;40:1007-15.39. Harnett MJ, Hepner DL, Datta S, Kodali BS.Effect of amniotic fluid on coagulation andplatelet function in pregnancy: an evaluation
using thromboelastography. Anaesthesia 2005;60:1068-72.40. Harnett MJ, Datta S, Bhavani-Shankar K.The effect of magnesium on coagulation inparturients with preeclampsia. Anesth Analg2001;92:1257-60.41. Butwick A, Harter S. An in vitro investigationof the coagulation effects of exogenous oxytocinusing thromboelastography in healthy parturi-ents. Anesth Analg 2011;113:323-6.
APRIL 2014 Ameri
42. Harnett MJ, Bhavani-Shankar K, Datta S,Tsen LC. In vitro fertilization-induced alterationsin coagulation and fibrinolysis as measured bythromboelastography. Anesth Analg 2002;95:1063-6.43. Sambasivan CN, Kunio NR, Nair PV, et al;Trauma Outcomes Group. High ratios of plasmaand platelets to packed red blood cells do notaffect mortality in nonmassively transfused pa-tients. J Trauma 2011;71:S329-36.
can Journal of Obstetrics & Gynecology 323.e7