Embed Size (px)
Citation preview

Transfusion Medicine in the NICU
Reese H Clark, MD
I do not have relevant financial relationships to disclose or conflicts of interest to resolve.
The off-label use of any drug will be identified, discussed and strongly discouraged.
Disclosure
What we believe to be true is not always trueWe love physiology and we can talk ourselves into trouble when we forget that everything, we do to critically ill neonates can have adverse consequences,- Prolonged high dose steroids (reduces inflammation but also impacts
growth)- Prolonged antibiotics (making sure infection is gone but changes the
microbiome)- Cisapride/Reglan (prokinetic but also rhythmagenic)
“If we respect truth, we must search for it by persistently searching for our errors..." Dr. Silverman
Background
Improved hemoglobin – more truck to carry oxygen to tissue. More oxygen content and improved oxygen delivery.Increased cardiac outputIncreased weight gain?Decreased apnea?
Reported benefits of transfusions

Complications associated with use of old blood- Increased potassium - Inflammation
Increased iron storesInfection from donorNEC?Increased morbidity?
Adverse impact


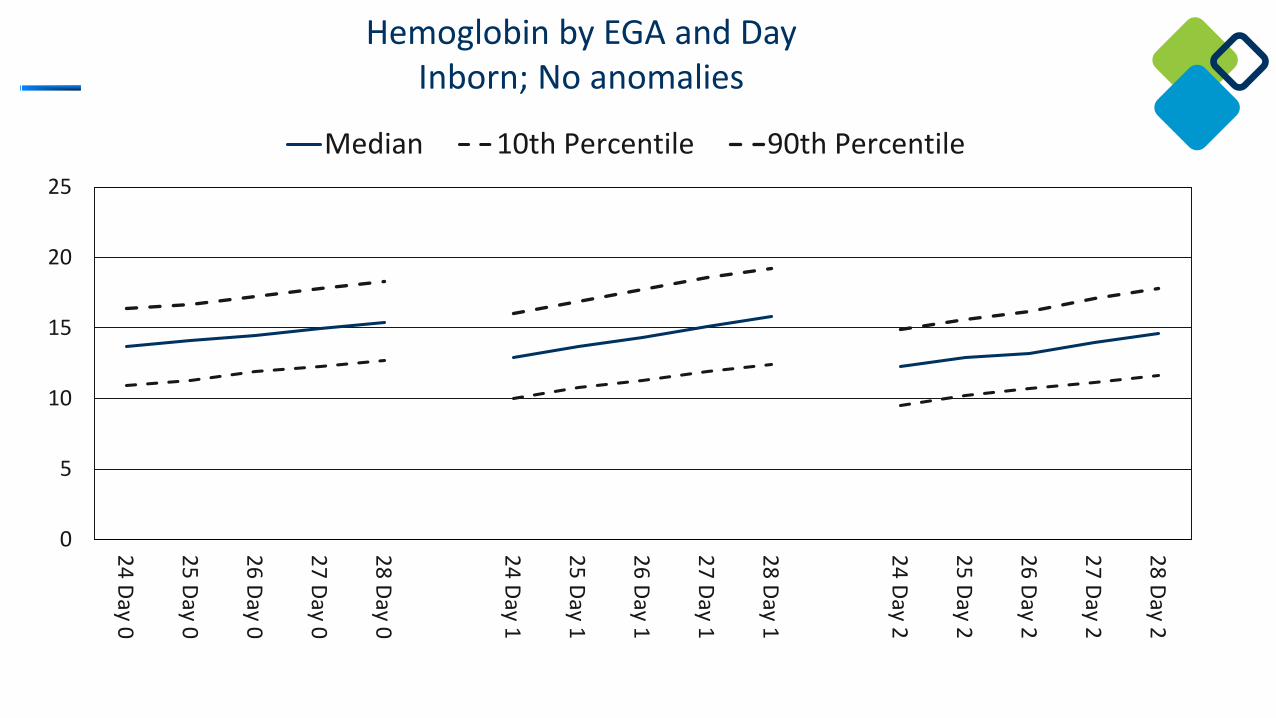
What is normal?
0
5
10
15
20
25
24 Day 0
25 Day 0
26 Day 0
27 Day 0
28 Day 0
24 Day 1
25 Day 1
26 Day 1
27 Day 1
28 Day 1
24 Day 2
25 Day 2
26 Day 2
27 Day 2
28 Day 2Median 10th Percentile 90th Percentile
Hemoglobin by EGA and DayInborn; No anomalies

0
10
20
30
40
50
60
24 Day 0
25 Day 0
26 Day 0
27 Day 0
28 Day 0
24 Day 1
25 Day 1
26 Day 1
27 Day 1
28 Day 1
24 Day 2
25 Day 2
26 Day 2
27 Day 2
28 Day 2Median 10th Percentile 90th Percentile
Hematocrit by EGA and DayInborn; No anomalies
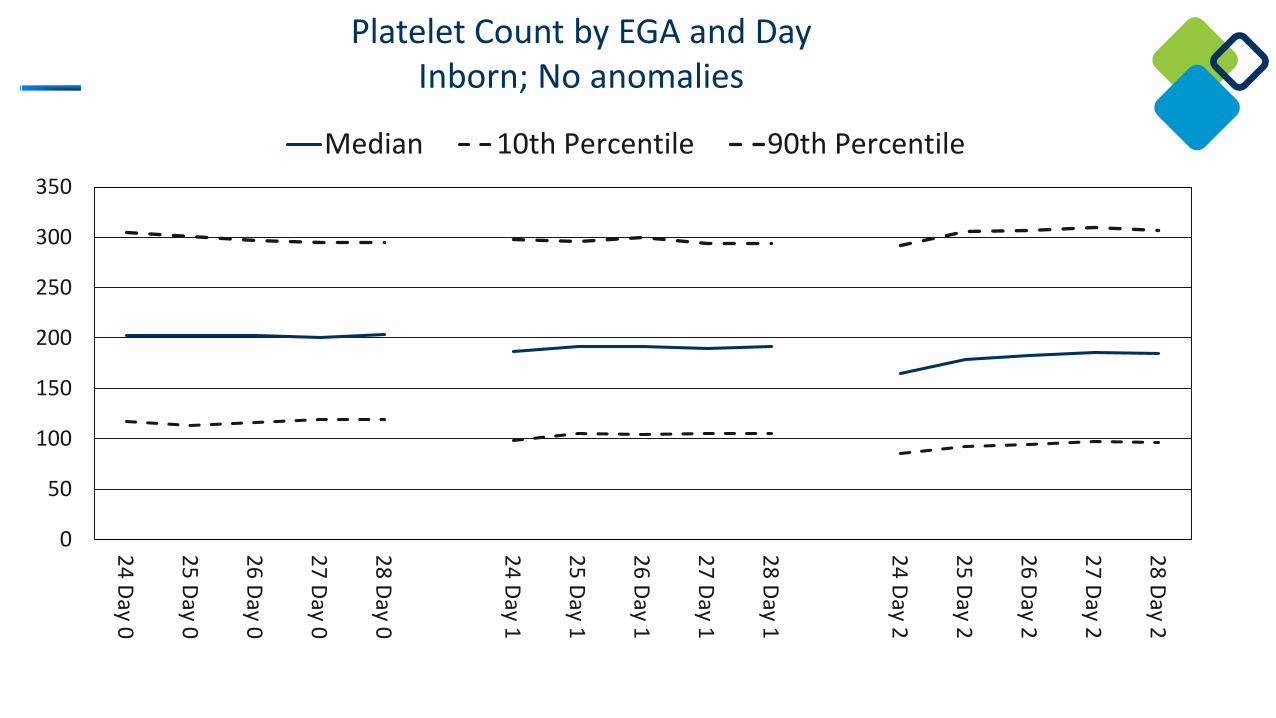
0
50
100
150
200
250
300
350
24 Day 0
25 Day 0
26 Day 0
27 Day 0
28 Day 0
24 Day 1
25 Day 1
26 Day 1
27 Day 1
28 Day 1
24 Day 2
25 Day 2
26 Day 2
27 Day 2
28 Day 2Median 10th Percentile 90th Percentile
Platelet Count by EGA and DayInborn; No anomalies
When do premature infants need a blood transfusion?
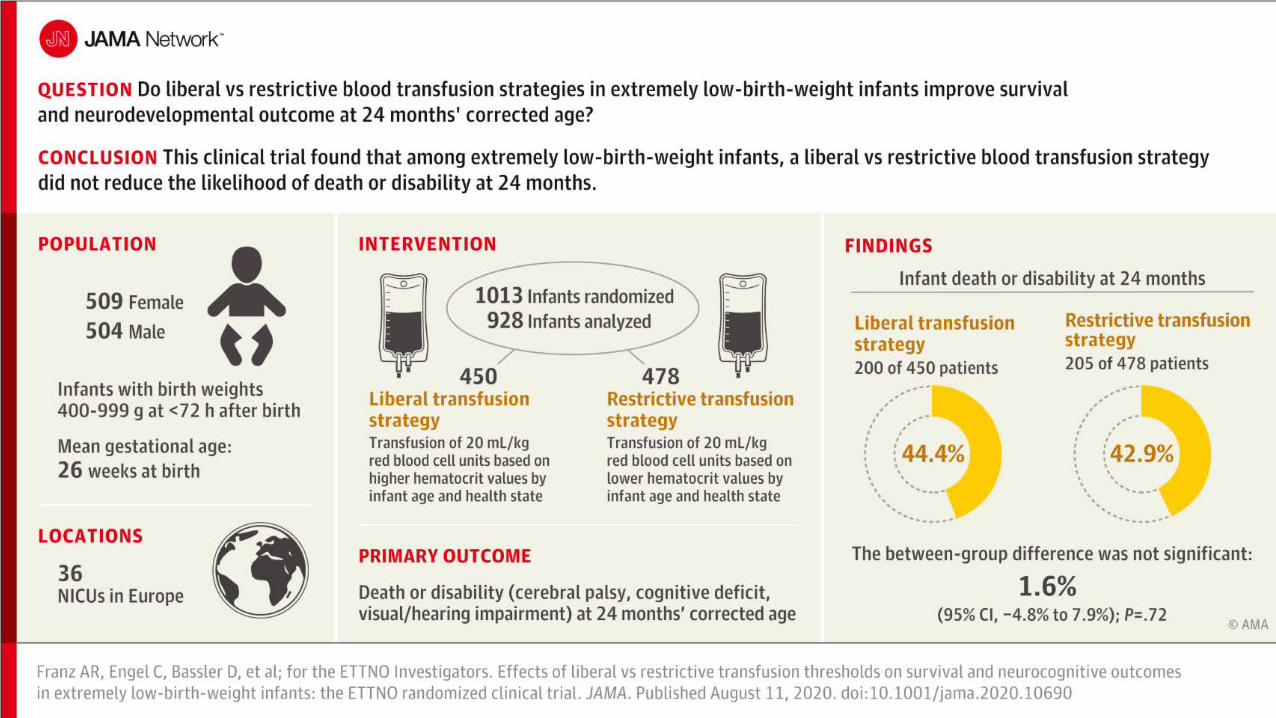
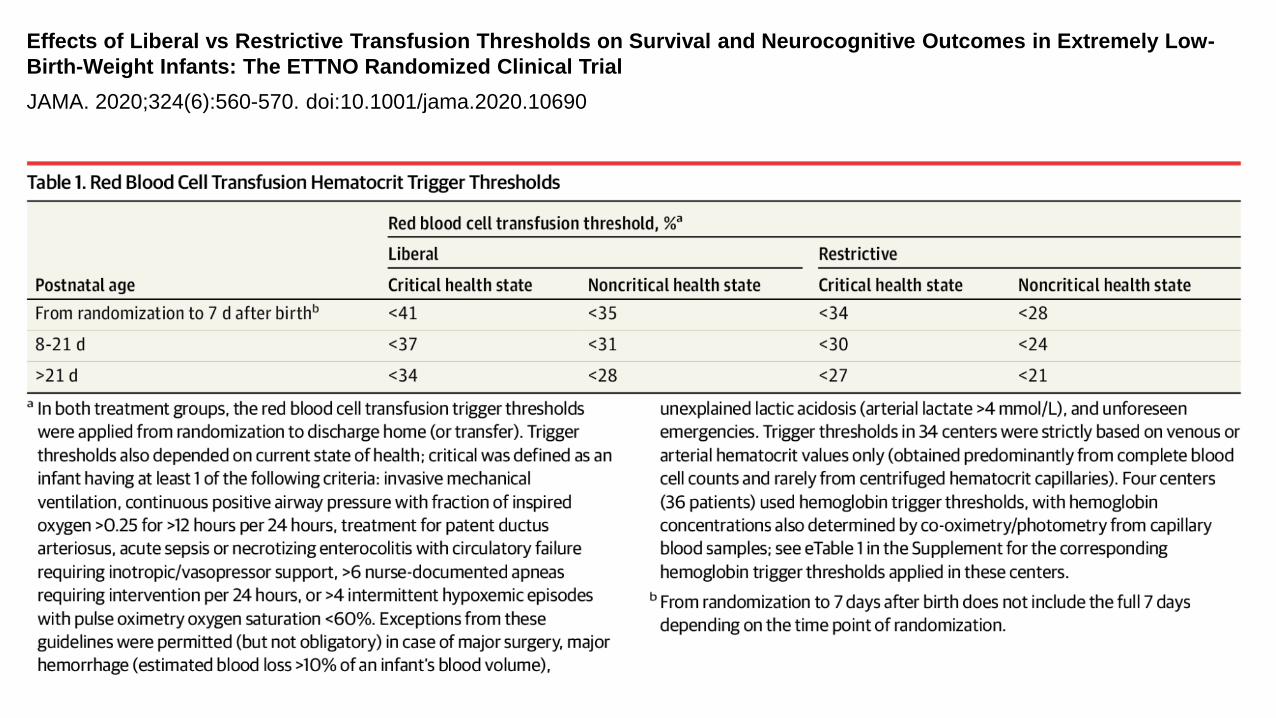
Effects of Liberal vs Restrictive Transfusion Thresholds on Survival and Neurocognitive Outcomes in Extremely Low-Birth-Weight Infants: The ETTNO Randomized Clinical TrialJAMA. 2020;324(6):560-570. doi:10.1001/jama.2020.10690
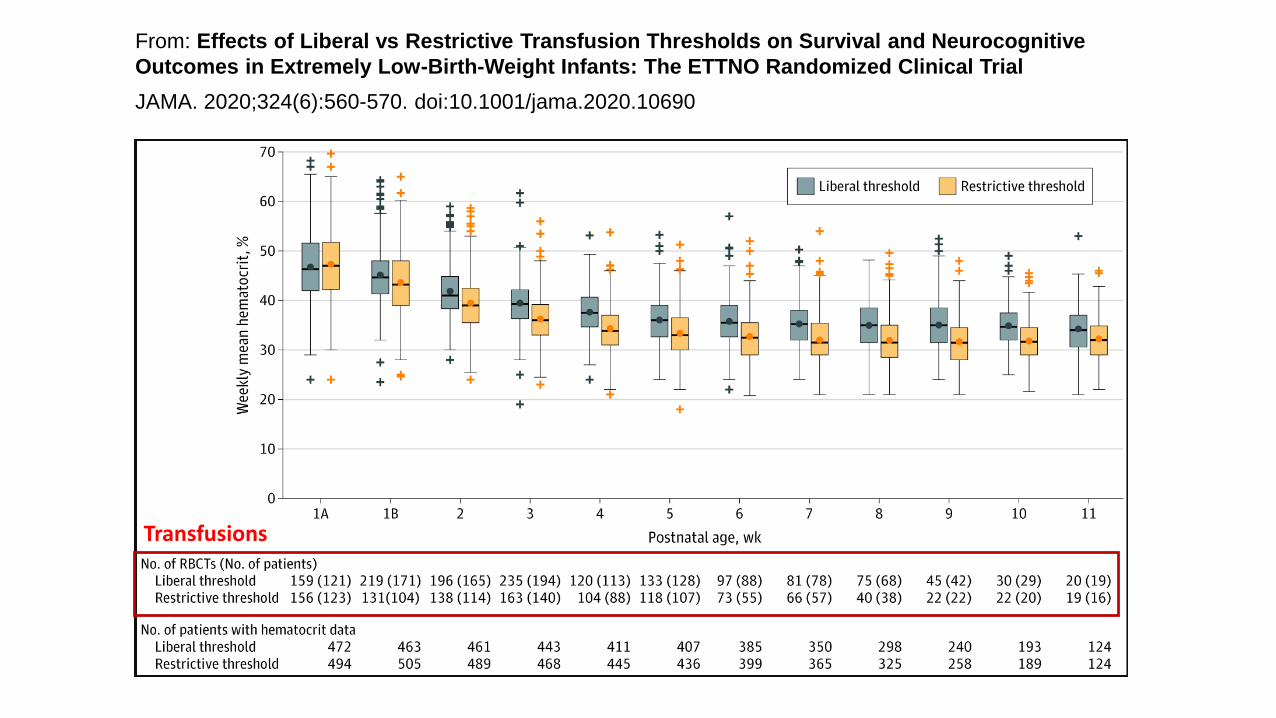
From: Effects of Liberal vs Restrictive Transfusion Thresholds on Survival and Neurocognitive Outcomes in Extremely Low-Birth-Weight Infants: The ETTNO Randomized Clinical TrialJAMA. 2020;324(6):560-570. doi:10.1001/jama.2020.10690
Transfusions

Kirpalani H et al. NICHD Neonatal Research Network. Higher or Lower Hemoglobin Transfusion Thresholds for Preterm Infants. N Engl J Med. 2020 Dec 31;383(27):2639-2651. doi: 10.1056/NEJMoa2020248. PMID: 33382931; PMCID: PMC8487591.
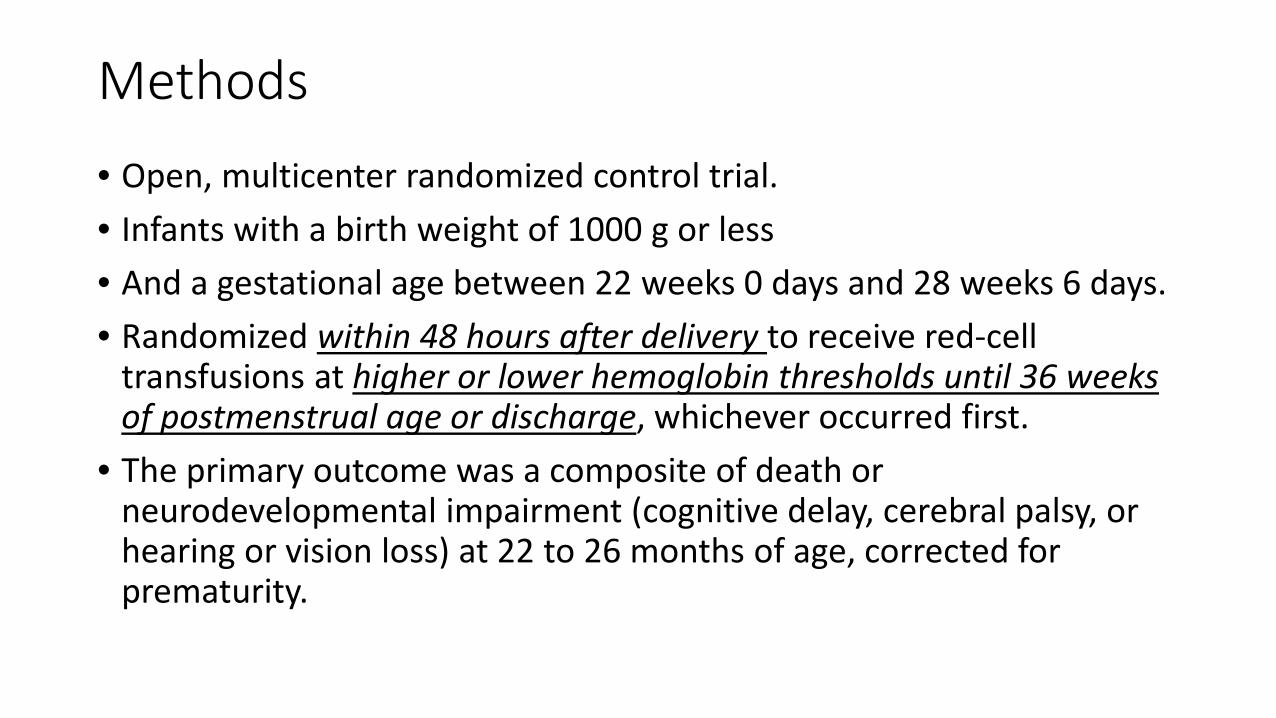
Methods• Open, multicenter randomized control trial.• Infants with a birth weight of 1000 g or less• And a gestational age between 22 weeks 0 days and 28 weeks 6 days.• Randomized within 48 hours after delivery to receive red-cell
transfusions at higher or lower hemoglobin thresholds until 36 weeks of postmenstrual age or discharge, whichever occurred first.
• The primary outcome was a composite of death or neurodevelopmental impairment (cognitive delay, cerebral palsy, or hearing or vision loss) at 22 to 26 months of age, corrected for prematurity.
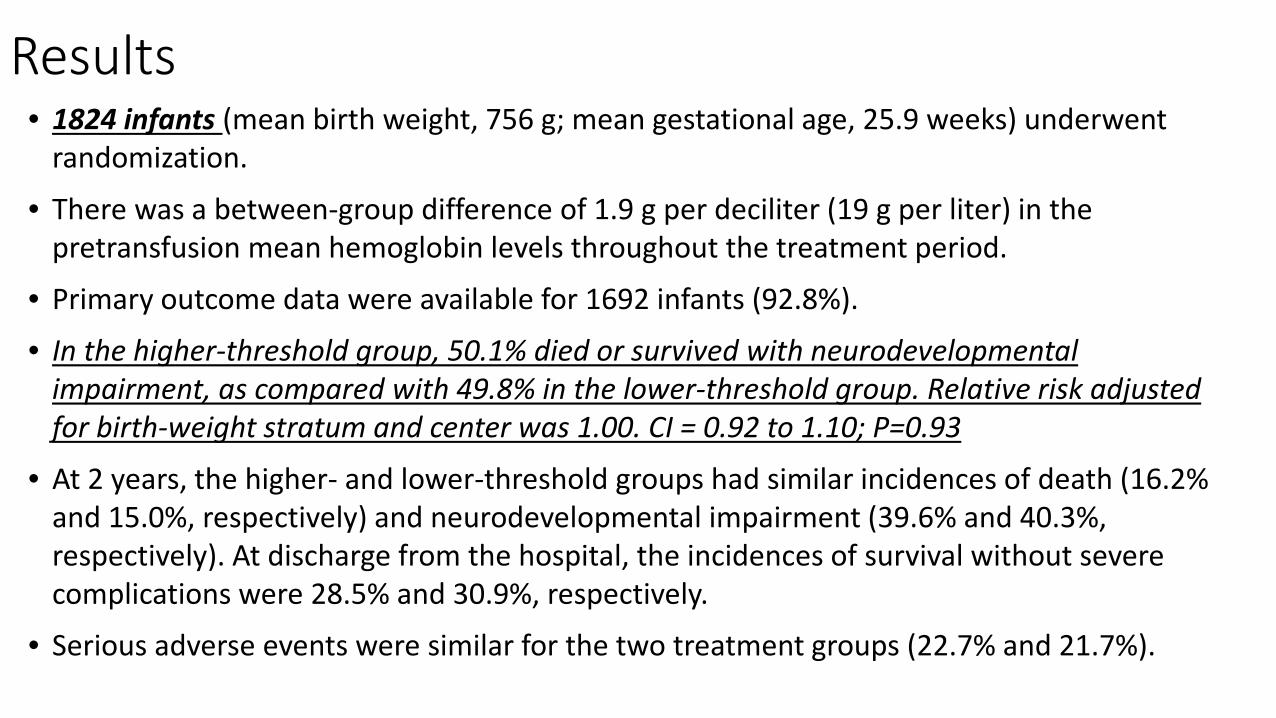
Results• 1824 infants (mean birth weight, 756 g; mean gestational age, 25.9 weeks) underwent
randomization.
• There was a between-group difference of 1.9 g per deciliter (19 g per liter) in the pretransfusion mean hemoglobin levels throughout the treatment period.
• Primary outcome data were available for 1692 infants (92.8%).
• In the higher-threshold group, 50.1% died or survived with neurodevelopmental impairment, as compared with 49.8% in the lower-threshold group. Relative risk adjusted for birth-weight stratum and center was 1.00. CI = 0.92 to 1.10; P=0.93
• At 2 years, the higher- and lower-threshold groups had similar incidences of death (16.2% and 15.0%, respectively) and neurodevelopmental impairment (39.6% and 40.3%, respectively). At discharge from the hospital, the incidences of survival without severe complications were 28.5% and 30.9%, respectively.
• Serious adverse events were similar for the two treatment groups (22.7% and 21.7%).

Figure 2. Separation of Hemoglobin Levels betweenTreatment Groups.
Hemoglobin levels in the higher-threshold and lower-threshold groups were recorded before enrollment and until 36 weeks of postmenstrual age. Values are means and 95% confidence intervals (indicated by 𝙸𝙸 bars), adjusted for infant as a random effect. Hemoglobin tests were performed at clinical discretion and were not dictated by protocol.
Panel A shows the hemoglobin levels that prompted a red-cell transfusion.
Panel B shows all hemoglobin levels that were measured in the two groups during the treatment period.


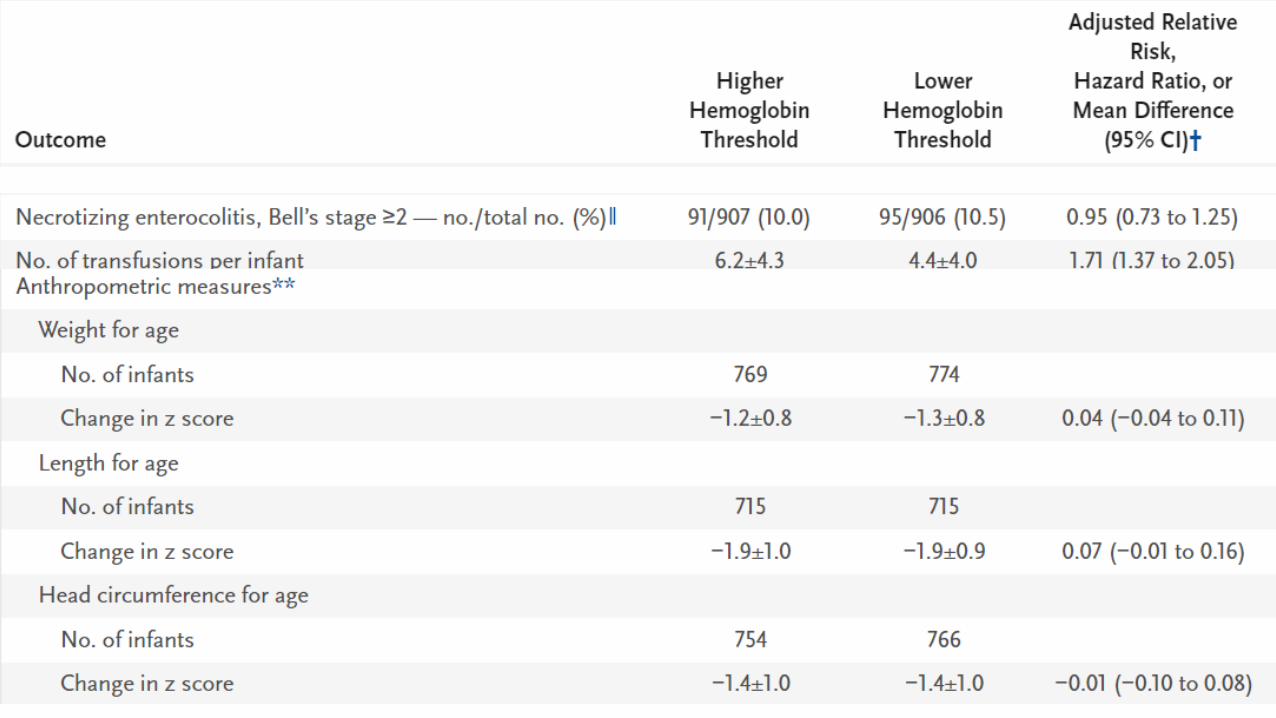


Secondary outcomes• Some observational studies have shown an association between transfusions and
necrotizing enterocolitis, but observational data have been inconsistent, and this finding has not been supported by available data from randomized trials.
• One prospective study showed that necrotizing enterocolitis was not associated with transfusion and was more likely to occur when nadir hemoglobin levels decreased to below 8 g per deciliter (80 g per liter) before transfusion. (Patel et al)
• Studies have suggested that the risks of hypoxemia and apnea of prematurity are increased among infants who do not receive transfusions. Postmenstrual age at the last use of caffeine therapy was used as a proxy for apnea, and the results were similar in the two threshold groups.
• Discrepancies between associations shown in observational studies and our findings underscore the pitfalls of observational studies.
Are transfusions associate with poor outcomes?

Vu PT et al. Transfusions and neurodevelopmental outcomes in extremely low gestation neonates enrolled in the PENUT Trial: a randomized clinical trial [published online ahead of print, 2021 Jan 11]. Pediatr Res. 2021;1-8.
Post hoc analysis of 936 infants 24-0/6 to 27-6/7 weeks’ enrolled in the PENUT Trial. Six hundred and twenty-eight (315 placebo, 313 Epo) survived and were assessed at 2 years.Evaluated associations between BSID-III scores and the number and volume of pRBCtransfusions.Each transfusion was associated with a decrease in mean cognitive score of 0.96 (95% CI of [−1.34, −0.57]), a decrease in mean motor score of 1.51 (−1.91, −1.12), and a decrease in mean language score of 1.10 (−1.54, −0.66). Significant negative associations between BSID-III score and transfusion volume and donor exposure were observed in the placebo group but not in the Epo group.Transfusions in ELGANs were associated with worse outcomes. We speculate that strategies to minimize the need for transfusions may improve outcomes.


Is there variability in practice?

Patel RM et al. Variation in Neonatal Transfusion Practice. J Pediatr. 2021 Aug;235:92-99.e4. doi: 10.1016/j.jpeds.2021.04.002. Epub 2021 Apr 7. PMID: 33836184
Retrospective cohort study using data from 7 geographically diverse US academic and community hospitals that participated in the National Heart Lung and Blood Institute Recipient Epidemiology and Donor Evaluation Study-III (REDS-III) from 2013 to 2016. 60 243 infants were evaluated. The incidence of any transfusion differed by gestational age (P < .0001), with 80% (95% CI 76%-84%) transfused at <27 weeks of gestation (n = 329) and 0.5% (95% CI 0.5%-0.6%) transfused at ≥37 weeks of gestation (n = 53 919). The median pretransfusion hemoglobin was 11.2 g/dL (10th-90th percentile 8.8-14.1) for the entire cohort, ranging from 10.5 g/dL (8.8-12.3) for infants born extremely preterm at <27 weeks of gestation to 13.0 g/dL (10.5-15.5) for infants born at term.The median pretransfusion platelet count (×109/L) was 71 (10th-90th percentile 26-135) for the entire cohort, and was >45 for all gestational age groups examined. The median pretransfusion international normalized ratio for the entire cohort was 1.7 (10th-90th percentile 1.2-2.8).A large proportion of neonatal transfusions in the US were administered at thresholds greater than supported by the best-available evidence and highlight an opportunity for improved patient blood management.
Is the sex or age of a blood donor associated with morbidity or mortality in very low-birth-weight infants receiving blood transfusion?
Patel RM et al. Association of Blood Donor Sex and Age With Outcomes in Very Low-Birth-Weight Infants Receiving Blood Transfusion. JAMA Netw Open. 2021 Sep 1;4(9):e2123942. doi: 10.1001/jamanetworkopen.2021.23942. PMID: 34477851
181 infants evaluated. Mean (SD) birth weight 919 (253) g and mean (SD) EGA 27.0 (2.2) weeks.56 infants (31%) received RBC transfusion from exclusively female donors. The mean (SD) donor age was 46.6 (13.7) years. Infants receiving red blood cell transfusion from female donors had a lower risk of death or serious morbidity compared with those who received transfusion from male donors.The primary outcome (death or significant morbidity) incidence was 21% (12 of 56 infants) among infants receiving RBCs from exclusively female donors, compared with 45% (56 of 125 infants) among those receiving RBCs from exclusively male donors. For the typical infant, who received a median (interquartile range) of 2 (1-3) transfusions, RBC transfusion from exclusively female donors, compared with male donors, was associated with a lower risk of the primary outcome (relative risk, 0.29; 95% CI, 0.16-0.54).
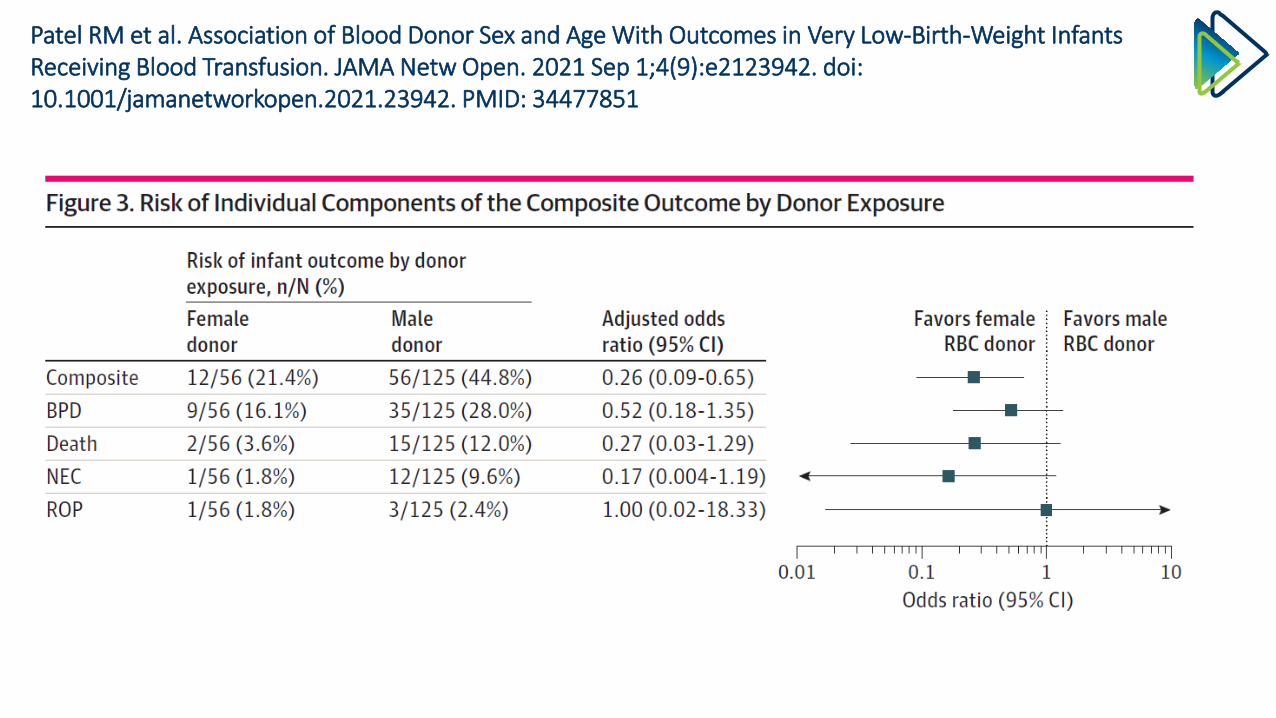
Patel RM et al. Association of Blood Donor Sex and Age With Outcomes in Very Low-Birth-Weight Infants Receiving Blood Transfusion. JAMA Netw Open. 2021 Sep 1;4(9):e2123942. doi: 10.1001/jamanetworkopen.2021.23942. PMID: 34477851
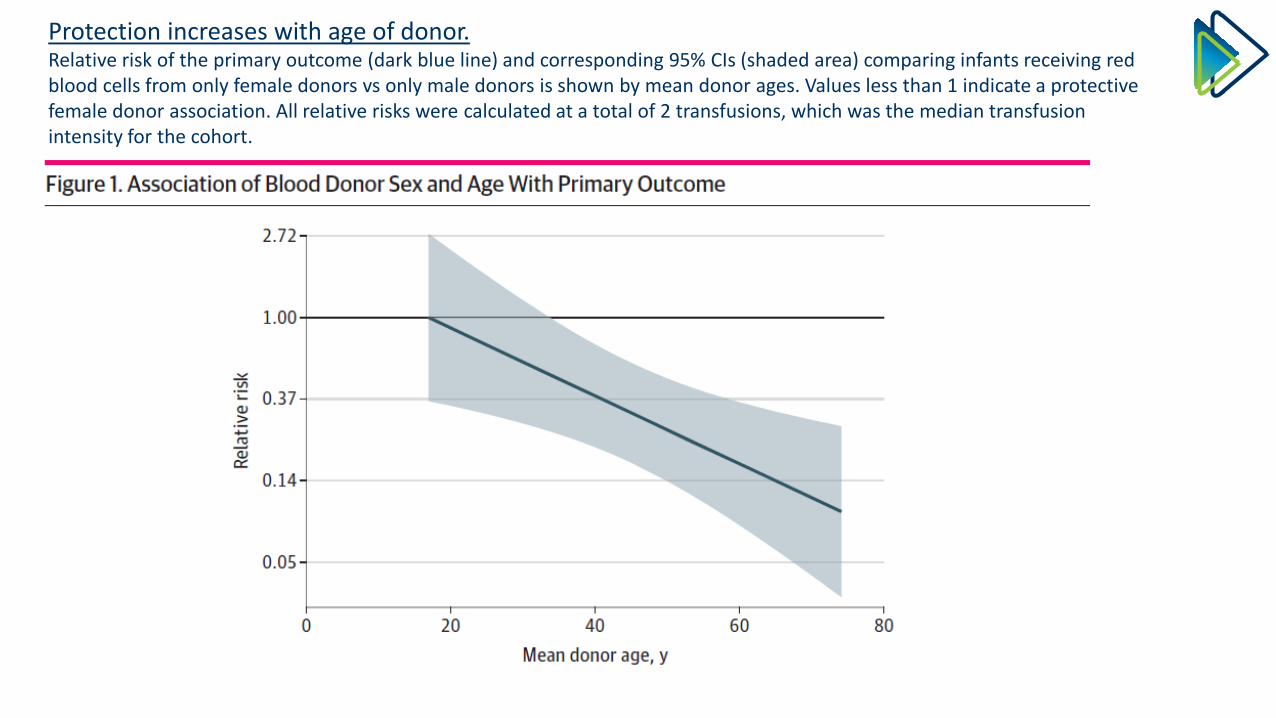
Protection increases with age of donor.Relative risk of the primary outcome (dark blue line) and corresponding 95% CIs (shaded area) comparing infants receiving redblood cells from only female donors vs only male donors is shown by mean donor ages. Values less than 1 indicate a protectivefemale donor association. All relative risks were calculated at a total of 2 transfusions, which was the median transfusion intensity for the cohort.
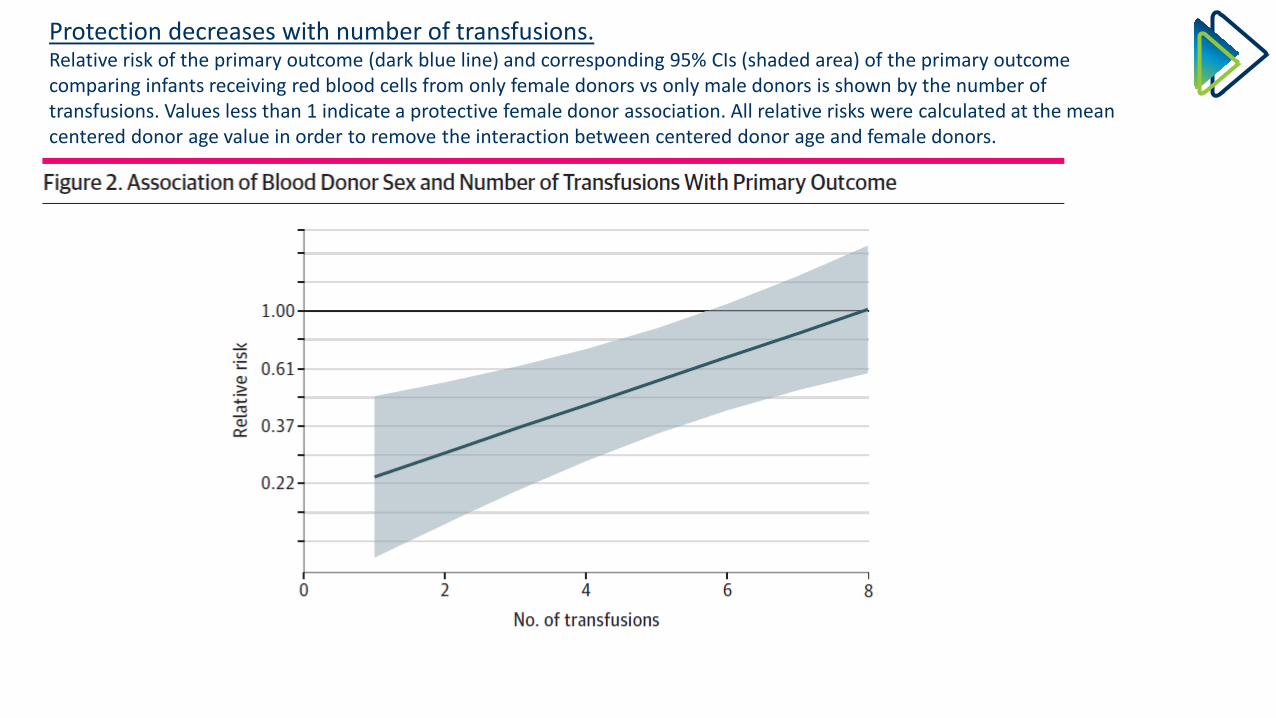
Protection decreases with number of transfusions.Relative risk of the primary outcome (dark blue line) and corresponding 95% CIs (shaded area) of the primary outcome comparing infants receiving red blood cells from only female donors vs only male donors is shown by the number of transfusions. Values less than 1 indicate a protective female donor association. All relative risks were calculated at the mean centered donor age value in order to remove the interaction between centered donor age and female donors.

ThrombocytopeniaWhat is the Threshold for Treatment?
What We Believe to be True is Not Always True

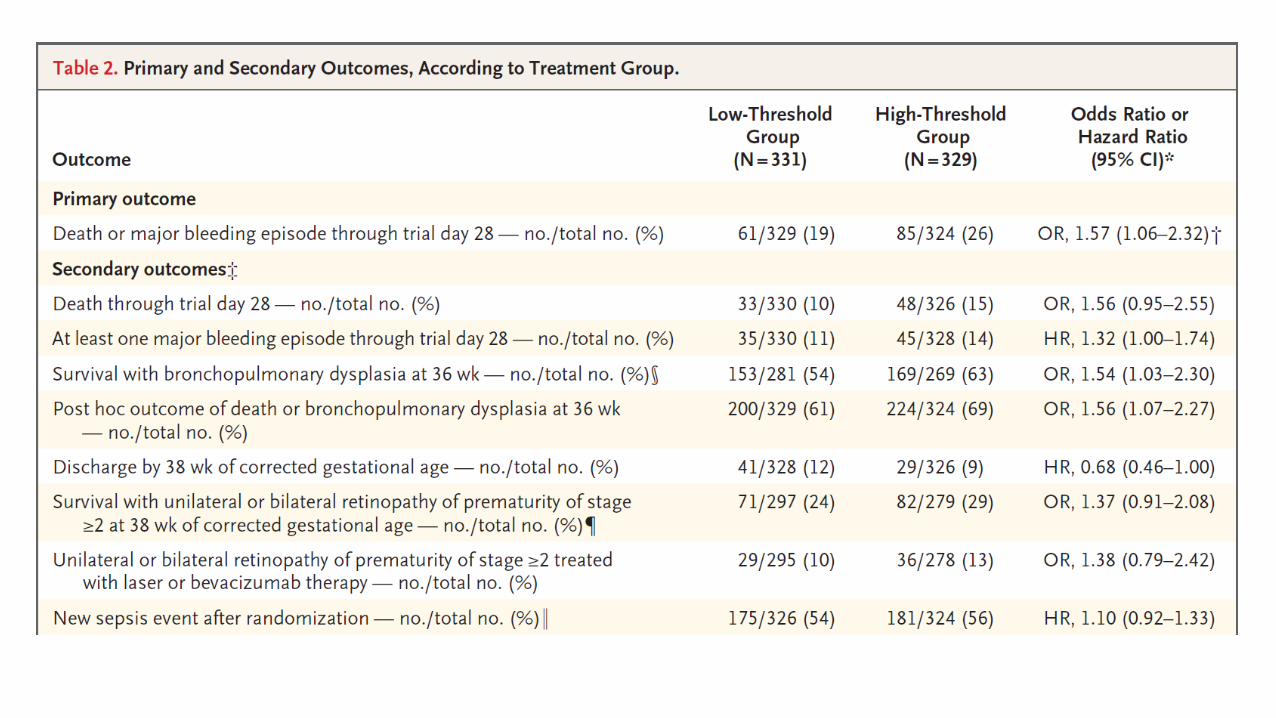
Randomized Trial of Platelet-Transfusion Thresholds in Neonates.
• Infants born at less than 34 weeks of gestation in whom severe thrombocytopenia developed were randomly assigned to receive a platelet transfusion at platelet-count thresholds of 50,000 per cubic millimeter (high-threshold group) or 25,000 per cubic millimeter (low-threshold group).
• The primary outcome was death or new major bleeding within 28 days after randomization.
• A total of 660 infants (median birth weight, 740 g; and median gestational age, 26.6 weeks) underwent randomization.
• In the high-threshold group, 90% of the infants (296 of 328 infants) received at least one platelet transfusion, as compared with 53% (177 of 331 infants) in the low-threshold group. A new major bleeding episode or death occurred in 26% of the infants (85 of 324) in the high-threshold group and in 19% (61 of 329) in the low-threshold group (odds ratio, 1.57; 1.06 to 2.32; P=0.02).
Curley A et al. N Engl J Med 2019;380(3):242-251

Major bleeding episode or death occurred MORE often in infants who were in the high threshold group and got more platelets.• Intracranial hemorrhage (leading to neurosurgical intervention or
radiologic imaging showing midline shift)• Intraventricular hemorrhage filling 50% or more of the cerebral
ventricle.• Pulmonary hemorrhage (fresh bleeding through an endotracheal tube
with increased ventilatory requirements)• Frank rectal bleeding• Severe bleeding (fatal bleeding, life-threatening bleeding associated
with shock, or bleeding requiring fluid boluses or red-cell transfusion).
Curley A et al. N Engl J Med 2019;380(3):242-251

Conclusions
• More is not better• Consistency in approach is important• Managing blood loss is as important as it deciding who needs
blood• Rather than defining new policies, carefully reviewing the
clinical trials and adopting the strategies used in clinical studies will lead to consistency and better outcomes.

Effects of Liberal vs Restrictive Transfusion Thresholds on Survival and Neurocognitive Outcomes in Extremely Low-Birth-Weight Infants: The ETTNO Randomized Clinical TrialJAMA. 2020;324(6):560-570. doi:10.1001/jama.2020.10690






























