Embed Size (px)
Citation preview

S
TR
JAM
Va
T
w
d
w
c
v
t
t
c
t
F
Tioasshfrr
act
FHm‡mas
M2
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 2 , N O . 9 , 2 0 0 9
© 2 0 0 9 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N I S S N 1 9 3 6 - 8 7 9 8 / 0 9 / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R I N C . D O I : 1 0 . 1 0 1 6 / j . j c i n . 2 0 0 9 . 0 7 . 0 0 5
TATE-OF-THE-ART PAPER
ranscatheter Aortic Valve Implantationeview of the Nature, Management, and Avoidance of Procedural Complications
ean-Bernard Masson, MD,* Jan Kovac, MD,† Gerhard Schuler, MD,‡ Jian Ye, MD,*nson Cheung, MD,* Samir Kapadia, MD,§ Murat E. Tuzcu, MD,§ Susheel Kodali, MD,�artin B. Leon, MD,� John G. Webb, MD*
ancouver, Canada; Leicester, United Kingdom; Leipzig, Germany; Cleveland, Ohio;nd New York, New York
ranscatheter aortic valve implantation (TAVI) is becoming a reality in the management of patients
ith severe aortic stenosis and high or prohibitive risk for standard surgical management. Current un-
erstanding of the potential adverse events associated with this procedure is limited. Risks associated
ith TAVI differ from those related to surgical valve replacement and include vascular injury; stroke;
ardiac injury such as heart block, coronary obstruction, and cardiac perforation; paravalvular leak; and
alve misplacement. The clinical experience of multiple centers experience with different valve implan-
ation systems and techniques was reviewed. Awareness of how complications occur might help in
heir avoidance, recognition, and management. Ultimately, improved understanding of the potential
omplications associated with TAVI might help improve outcomes and allow wider application of this
herapy. (J Am Coll Cardiol Intv 2009;2:811–20) © 2009 by the American College of Cardiology
oundation
TaOsEnshRpBiteds
A
Ato2
ranscatheter aortic valve implantation (TAVI)s increasingly recognized as a viable therapeuticption for patients with severe, symptomaticortic stenosis and high risk for conventionalurgery. Registries from multiple centers havehown TAVI can be accomplished in selectedigh-risk patients with outcomes that compareavorably with the outcome of standard valveeplacement as predicted by validated operativeisk assessment tools (1– 6).
Despite being less invasive than open-chestortic valve replacement, TAVI remains asso-iated with the potential for serious complica-ions. We review the potential complications of
rom the *Divisions of Cardiology and Cardiac Surgery, St. Paul’sospital, University of British Columbia, Vancouver, Canada; †Depart-ent of Cardiology, University Hospitals, Leicester, United Kingdom;
Department of Cardiology, Heart Center, Leipzig, Germany; §Depart-ent of Cardiovascular Medicine, Cleveland Clinic, Cleveland, Ohio;
nd the �Center for Interventional Vascular Therapy, Columbia Univer-ity Medical Center, New York, New York.
ianuscript received March 10, 2009; revised manuscript received July 2,
009, accepted July 27, 2009.
AVI and discuss their prevention, diagnosis,nd management.verview of procedure. Two TAVI systems have
een wide clinical application: the balloon-expandabledwards valve (Edwards Lifesciences, Irvine, Califor-ia), and the self-expandable CoreValve ReValvingystem (CoreValve, Irvine, California). Both systemsave been extensively described elsewhere (6–8).etrograde transarterial or antegrade transapical ap-roaches are currently used to access the aortic valve.alloon aortic valvuloplasty is performed before valve
nsertion to facilitate passage of the prosthesishrough the stenotic native valve. With the balloon-xpandable valve, ventricular burst pacing is used toecrease transvalvular flow and avoid expulsion of theystem toward the aorta upon deployment.
ccess and Delivery
rterial injury. The relatively large diameter ofhe delivery catheter has been a major limitationf transarterial TAVI. Early systems used 22- to5-F sheaths (outer diameter 9 to 10 mm), and
n the absence of adequate screening the inci-
dhEsrtdcwrt
msaacseatms
aNmlMep
rSstbpfocstdosvfic
flao
Aa
Lv
Tv
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 2 , N O . 9 , 2 0 0 9
S E P T E M B E R 2 0 0 9 : 8 1 1 – 2 0
Masson et al.
Transcatheter Aortic Valve Implantation
812
ence of arterial dissection and perforation was relativelyigh. Newer low-profile systems (e.g., CoreValve anddwards NovaFlex) are compatible with smaller 18-F
heaths (outer diameter approximately 7 mm). It iseasonable to assume that the risk of vascular complica-ions is reduced with the use of these lower-profileelivery systems. With technological advances, deliveryatheter and sheath size will likely decrease further,hich should be associated with further reductions in the
isk of vascular injury and less stringent criteria for aransarterial approach.
Angiography and multislice computed tomography are theain imaging modalities used to assess the presence and
everity of ilio-femoral disease and determine the feasibility ofn arterial approach. Minimal lumen diameter as well as themount and distribution of atheroma, tortuosity, and calcifi-ation will determine the risk for vascular injury related toheath insertion. Ideally the minimal lumen diameter shouldxceed the diameter of the delivery system. However, in thebsence of extensive calcification, bulky atheroma, or severeortuosity, short segments of relatively compliant artery 1 to 2m smaller in diameter than the intended sheath can often be
afely cannulated.Dissection or perforation of
the ilio-femoral arteries mightoccur in the presence of exces-sively traumatic sheath inser-tion (Fig. 1A). Dissection ofthe ascending or descendingaorta can similarly occur due tocatheter trauma (Fig. 2) or as
Figure 1. Vascular Injury
(A) Dissection of the right iliac artery. (B) Occlusion balloon (Occlusion Cathete
bbreviationsnd Acronyms
V � leftentricle/ventricular
AVI � transcatheter aorticalve implantation
Balloon Catheter, Cook Medical, Inc., Bloomington, Indiana) inflated in the left iliac a
n unpredictable complication of aortic valvuloplasty (1).onocclusive retrograde arterial dissection will com-only heal once antegrade flow is restored; therefore
imited dissections are often best managed conservatively.ore extensive arterial dissection can be managed with
ndovascular stenting although on occasion surgical re-air might be necessary.Vascular perforation leading to retroperitoneal hemor-
hage is a more dramatic potential complication of TAVI.uccessful management requires a high level of suspicion,hould sudden, unexplained hypotension appear. Whenhe large arterial sheath is occlusive, perforation mightecome evident only after sheath removal. Volume ex-ansion and angiographic assessment should be per-ormed without delay. Immediate reinsertion of thecclusive sheath over a guidewire or placement of a highlyompliant occlusion balloon proximal to the area ofuspected perforation typically provides rapid and rela-ively reliable control of bleeding (9), allowing time forefinitive management (Figs. 1B and 1C). Covered stentsr percutaneous endografts might be adequate, althoughurgical repair might be necessary. After uncomplicatedascular closure, ilio-femoral angiography performedrom the contralateral femoral access site allows rapiddentification and, if necessary, management of vascularomplications.
An unusual presentation peculiar to a large, occlusiveemoral sheath is a tendency for the sheath and endothe-ium to adhere. Sheath withdrawal is met with resistancend possible complete arterial avulsion and sudden hem-rrhage (Fig. 3). The risk of ilio-femoral adherence and
ton Scientific, Natick, Massachusetts). (C) Occlusion balloon (Coda Occlusion
r, Bos rtery.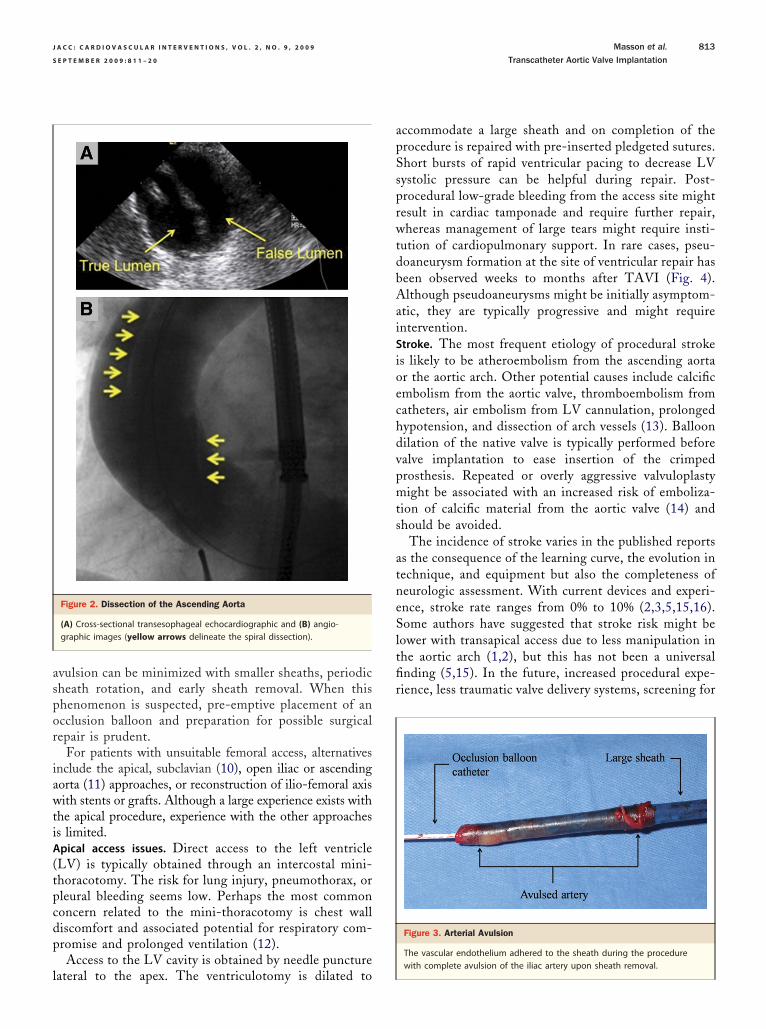
aspor
iawtiA(tpcdp
l
apSsprwtdbAaiSioechdvpmts
atneSltfir
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 2 , N O . 9 , 2 0 0 9 Masson et al.
S E P T E M B E R 2 0 0 9 : 8 1 1 – 2 0 Transcatheter Aortic Valve Implantation
813
vulsion can be minimized with smaller sheaths, periodicheath rotation, and early sheath removal. When thishenomenon is suspected, pre-emptive placement of ancclusion balloon and preparation for possible surgicalepair is prudent.
For patients with unsuitable femoral access, alternativesnclude the apical, subclavian (10), open iliac or ascendingorta (11) approaches, or reconstruction of ilio-femoral axisith stents or grafts. Although a large experience exists with
he apical procedure, experience with the other approachess limited.pical access issues. Direct access to the left ventricleLV) is typically obtained through an intercostal mini-horacotomy. The risk for lung injury, pneumothorax, orleural bleeding seems low. Perhaps the most commononcern related to the mini-thoracotomy is chest walliscomfort and associated potential for respiratory com-romise and prolonged ventilation (12).Access to the LV cavity is obtained by needle puncture
Figure 2. Dissection of the Ascending Aorta
(A) Cross-sectional transesophageal echocardiographic and (B) angio-graphic images (yellow arrows delineate the spiral dissection).
ateral to the apex. The ventriculotomy is dilated to
ccommodate a large sheath and on completion of therocedure is repaired with pre-inserted pledgeted sutures.hort bursts of rapid ventricular pacing to decrease LVystolic pressure can be helpful during repair. Post-rocedural low-grade bleeding from the access site mightesult in cardiac tamponade and require further repair,hereas management of large tears might require insti-
ution of cardiopulmonary support. In rare cases, pseu-oaneurysm formation at the site of ventricular repair haseen observed weeks to months after TAVI (Fig. 4).lthough pseudoaneurysms might be initially asymptom-
tic, they are typically progressive and might requirentervention.troke. The most frequent etiology of procedural strokes likely to be atheroembolism from the ascending aortar the aortic arch. Other potential causes include calcificmbolism from the aortic valve, thromboembolism fromatheters, air embolism from LV cannulation, prolongedypotension, and dissection of arch vessels (13). Balloonilation of the native valve is typically performed beforealve implantation to ease insertion of the crimpedrosthesis. Repeated or overly aggressive valvuloplastyight be associated with an increased risk of emboliza-
ion of calcific material from the aortic valve (14) andhould be avoided.
The incidence of stroke varies in the published reportss the consequence of the learning curve, the evolution inechnique, and equipment but also the completeness ofeurologic assessment. With current devices and experi-nce, stroke rate ranges from 0% to 10% (2,3,5,15,16).ome authors have suggested that stroke risk might be
ower with transapical access due to less manipulation inhe aortic arch (1,2), but this has not been a universalnding (5,15). In the future, increased procedural expe-ience, less traumatic valve delivery systems, screening for
Figure 3. Arterial Avulsion
The vascular endothelium adhered to the sheath during the procedure
with complete avulsion of the iliac artery upon sheath removal.
tdoa
tota
P
Iwueaa
ietamoobrafib
aorta; LV � left ventricle; PA � pseudoaneurysm.
ent across it.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 2 , N O . 9 , 2 0 0 9
S E P T E M B E R 2 0 0 9 : 8 1 1 – 2 0
Masson et al.
Transcatheter Aortic Valve Implantation
814
hick aortic atheroma, and possibly embolic protectionevices currently under development might lower the riskf stroke. Procedural anticoagulation to reach a targetctivated clotting time over 250 s is generally suggested.
The longer-term thromboembolic risk associated withranscatheter valves is currently unknown. Empiric dualral antiplatelet therapy is generally recommended for 3o 6 months, followed by long-term daily low-dosespirin.
ositioning and Deployment
mproper positioning. An ideal transcatheter aortic prosthesisould restrain the native leaflets and relieve stenosis withoutnnecessary contact with the surrounding structures. A valvextending excessively into the ventricle or the aorta might bessociated with adverse events such as mitral insufficiency,rrhythmias or aortic injury.
Prosthesis embolization immediately after deployments generally the result of a gross error in positioning orjection of the device by an effective ventricular contrac-ion during deployment (Fig. 5). Embolization to theorta is well-tolerated so long as coaxial wire position isaintained, preventing the valve from flipping over to
bstruct antegrade flow. Typically the valve can be snaredr repositioned with a partially inflated valvuloplastyalloon into a stable position in the aorta. A TAVIeattempt is often successful, although an alternativepproach might be advisable when the reason for initialailure cannot be addressed (17). Embolization to the LVs far less likely, but in such cases surgical removal mighte the only option (18). The ability to recapture and
osition. (B) The prosthesis is secured in the aorta with no detectable gradi-
Figure 4. Apical Pseudoaneurysm
(A) Pseudoaneurysm arising from the left ventricular apex apparent severalweeks after a transapical procedure. The black arrow indicates the valvedstent. (B) Pseudoaneurysm formation after a local wound infection. Ao �
Figure 5. Embolization
(A) The embolized balloon-expandable valve orientation is maintained by the wire p

raaCithctpfcpcfi(ans
hypotension episode.
leaflet (not the stent itself) seemed to obstruct the ostium.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 2 , N O . 9 , 2 0 0 9 Masson et al.
S E P T E M B E R 2 0 0 9 : 8 1 1 – 2 0 Transcatheter Aortic Valve Implantation
815
eposition a valve after deployment would clearly bedvantageous, and such prostheses might become avail-ble in the upcoming years (19).oronary obstruction. Coronary obstruction might occurf an obstructive portion of the valve frame (Fig. 6A) orhe sealing cuff is placed directly over a coronary ostium;owever, this is exceedingly rare. The presence of openells over a coronary ostium is well-tolerated, but al-hough percutaneous coronary interventions have beenerformed after valve implantation (20), it is likely thatrame struts will prevent or complicate selective coronaryannulation. Of more concern is the possibility of dis-lacing an unusually bulky, calcified native leaflet over aoronary ostium (Fig. 7) (7). Although this might beatal, some cases have been successfully managed bymmediate percutaneous angioplasty or bypass surgery2). The risk of coronary occlusion is low but difficult tossess and most likely depends on the bulkiness of theative leaflets, height of the coronary ostia, and dimen-ions of the sinus of Valsalva. Echocardiography, aortog-
the ostium. (B) Successful percutaneous intervention restored left coronaryn (arrows) are approximated after valve implantation. (D) At autopsy, the
Figure 6. Coronary Obstruction and Frame Deformation
(A) Normal flow in the left coronary artery despite the presence of a stentstrut at the left main coronary ostium. (B) Oval shape of the transcathetervalve, possibly the result of chest compressions received during a transient
Figure 7. Left Main Obstruction
(A) Left main coronary artery occlusion resulting from a bulky leaflet displaced overflow. (C) In a second patient, calcifications from the native aortic leaflet and left mai

ruaptoolMtacmtnantmlemd
Rc
etmrblmo(Pidrmctms
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 2 , N O . 9 , 2 0 0 9
S E P T E M B E R 2 0 0 9 : 8 1 1 – 2 0
Masson et al.
Transcatheter Aortic Valve Implantation
816
aphy, and multislice computed tomography have beensed to assess these relationships (21). On occasionortography during aortic valvuloplasty might help clarifyotential concerns. At this time no definite criteria existo exclude patients on the basis of the risk for coronarybstruction, but some have suggested that the coronarystia should be minimally located 14 mm away from theeaflets insertion.itral valve injury. Mitral valve injury was first reported in
he setting of the transvenous, transseptal approach to theortic valve (22). With this approach the delivery systemrosses the mitral valve with the potential for temporaryitral incompetence (23) or abrasion and laceration of
he anterior mitral leaflet (24). Although this approach iso longer used, mitral injury might still occur. With thentegrade apical approach, a wire can be passed under-eath a mitral chordae. Advancing a large catheter overhis wire might result in temporary distortion of theitral valve apparatus or avulsion of a mitral chordae,
eading to acute mitral regurgitation. Resistance to cath-ter advancement through the ventricle or transientitral regurgitation assessed by transesophageal echocar-
Figure 8. Delayed Mitral Valve Injury
(A) The stent (double arrow) is in contact with the anterior mitral leaflet. Prosthe mitral leaflet at the point of contact (single arrow). (B) Ensuing severe misecondary to chordeal rupture created (D) severe mitral regurgitation several moutflow tract.
iography should alert the operator to this possibility. g
ewiring or use of a balloon flotation catheter might beonsidered to avoid subchordal passage.
The ventricular end of a transcatheter prosthesis can bexpected to contact the anterior mitral curtain. A pros-hesis extending too far into the LV might interfere withovement of the mitral leaflet and cause acute mitral
egurgitation. Surgical removal of such prosthesis mighte necessary, although this seems exceedingly rare. Theong-term effects of lesser degrees of prosthesis-anterior
itral leaflet contact are unknown, but isolated instancesf late mitral valve injury have been documented (25)Fig. 8).aravalvular regurgitation. Minor paravalvular regurgitation
s ubiquitous with current transcatheter valves, but the inci-ence of moderate or severe paravalvular leaks was greatlyeduced by the routine insertion of prostheses larger than theeasured annulus diameter. Initial reports suggested signifi-
ant paravalvular leak in many patients after implantation ofhe first-generation balloon-expandable TAVI (22,23), butore recent publications report infrequent cases of moderate or
evere paravalvular regurgitation with both systems (3–5).Mild and even moderate degrees of paravalvular regur-
valve endocarditis 1 year after implantation associated with perforation ofgurgitation. (C) In a second patient, prolapse of the anterior mitral leaflets after the procedure. Ao � aorta; LA � left atrium; LVOT � left ventricular
thetictral reonth
itation seem well-tolerated, and clinically significant
hmqislutcecpltprvAaSsEalaobsvaacLrV
acCprratLmpTrHtiat
.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 2 , N O . 9 , 2 0 0 9 Masson et al.
S E P T E M B E R 2 0 0 9 : 8 1 1 – 2 0 Transcatheter Aortic Valve Implantation
817
emolysis has not been observed to date (26). However,oderately severe or severe paravalvular, albeit infre-
uent, is likely to be hemodynamically significant. Thenitial sign is typically an unexpectedly low aortic dia-tolic pressure. Rising ventricular filling pressure mightead to myocardial ischemia, ventricular dysfunction, andltimately shock. The diagnosis is confirmed with aor-ography or, more reliably, echocardiography. Most likelyauses are incorrect positioning, undersizing, or under-xpansion. Balloon re-expansion might be helpful inases of incomplete expansion, whereas a second overlap-ing prosthesis might be the most effective solution for
eaks caused by malposition (Fig. 9). Exclusion of pa-ients with an annulus larger than the largest availablerosthesis is prudent to avoid significant paravalvularegurgitation. TAVI in stenotic, congenitally bicuspidalves is possible, but experience is limited.nnular and root rupture. Rupture of the aortic annulus israre complication of aortic balloon valvuloplasty (27).
imilarly, rare cases of annular or root rupture withubsequent hemodynamic collapse occurred with TAVI.xcessive balloon dilation, aggressive valve oversizing,
nd extensive annular calcification might increase theikelihood of this uncommon complication. When thennulus and/or subannular tissues are markedly calcifiedr when the root is unusually small, it seems prudent toe less aggressive with balloon dilation and valve over-izing. Unexplained hypotension after balloon dilation oralve expansion should prompt echocardiographic orngiographic assessment of the LV outflow tract andortic root. A tear created at the level of the valve inflowan result in either ventricular septal defect (Fig. 10) orV to left atrial shunt (Fig. 11), whereas aortic root
upture will likely cause massive bleeding and tamponade.
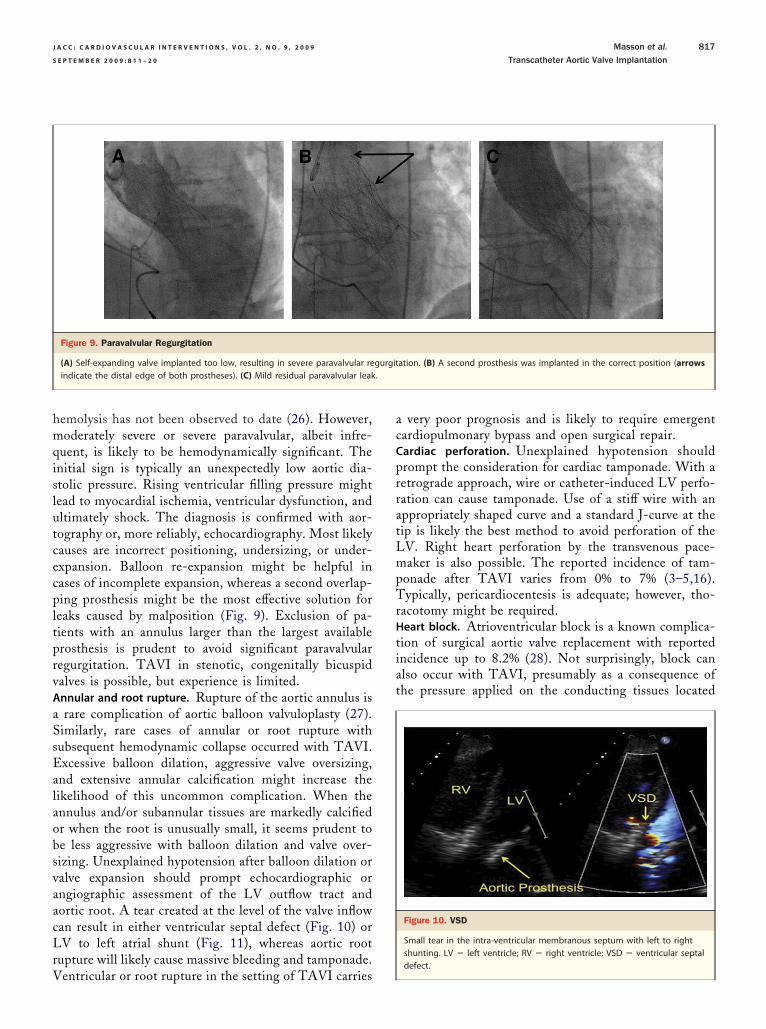
Figure 9. Paravalvular Regurgitation
(A) Self-expanding valve implanted too low, resulting in severe paravalvular reindicate the distal edge of both prostheses). (C) Mild residual paravalvular leak
entricular or root rupture in the setting of TAVI carries
very poor prognosis and is likely to require emergentardiopulmonary bypass and open surgical repair.ardiac perforation. Unexplained hypotension shouldrompt the consideration for cardiac tamponade. With aetrograde approach, wire or catheter-induced LV perfo-ation can cause tamponade. Use of a stiff wire with anppropriately shaped curve and a standard J-curve at theip is likely the best method to avoid perforation of theV. Right heart perforation by the transvenous pace-aker is also possible. The reported incidence of tam-
onade after TAVI varies from 0% to 7% (3–5,16).ypically, pericardiocentesis is adequate; however, tho-
acotomy might be required.eart block. Atrioventricular block is a known complica-
ion of surgical aortic valve replacement with reportedncidence up to 8.2% (28). Not surprisingly, block canlso occur with TAVI, presumably as a consequence ofhe pressure applied on the conducting tissues located
ation. (B) A second prosthesis was implanted in the correct position (arrows
Figure 10. VSD
Small tear in the intra-ventricular membranous septum with left to rightshunting. LV � left ventricle; RV � right ventricle; VSD � ventricular septal
gurgit
defect.

stbprehnfor
larp(
O
Abpt
caqplrnChLTmcsstwitqai
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 2 , N O . 9 , 2 0 0 9
S E P T E M B E R 2 0 0 9 : 8 1 1 – 2 0
Masson et al.
Transcatheter Aortic Valve Implantation
818
ubendocardially in the LV outflow tract and interven-ricular septum. In initial reports of TAVI-induced heartlock with the 2 currently used systems, permanentacemaker implantation rate was 7% (29) and 18% (30),espectively. Early experience suggests that prosthesesxtending farther in the ventricle are associated with aigher incidence of conduction abnormalities, most likelyew-onset left bundle branch block (30). Potential riskactors also include aggressive oversizing and the presencef pre-existing infranodal conduction anomalies such asight bundle branch block or second-degree heart block.
Heart block typically manifests immediately after valvu-oplasty or valve implantation. Consequently, placement oftemporary pacemaker is desirable during the procedure. In
are cases heart block has appeared days after the procedure;ost-procedural monitoring for 48 h has been suggested30,31).
ther Complications
rrhythmia. Atrial fibrillation or ventricular ectopy mighte precipitated by cardiac manipulation and is oftenoorly tolerated in the setting of aortic stenosis. Reposi-
Figure 11. Annulus Rupture
(A) Pre-implantation significant mitral regurgitation (MR) and severe calcificatiotion, a tear (arrows) is visible at the ventricular edge of the stent, connectingatrial shunt. (D) Autopsy proven tear of the anterior mitral curtain.
ioning the ventricular wire is often all that is necessary in c
ases of frequent ventricular ectopy. Sustained ventricularrrhythmias might occur spontaneously or as a conse-uence of rapid pacing but generally are responsive torompt defibrillation; preparatory placement of defibril-
ator pads is advisable. Timely management of tachyar-hythmias is important to help prevent adverse hemody-amic consequences.ardiogenic shock. Patients with severe aortic stenosis oftenave little myocardial reserve, particularly in the presence ofV dysfunction, hypertrophy, or coronary artery disease.achycardia of any cause, including burst pacing, should beinimized, and hypotension should be avoided. Whatever the
ause, hypotension or tachycardia might initiate a downwardpiral of ischemia and myocardial dysfunction, leading tohock. Vasopressor agents (phenylephrine or norepinephrine)o maintain adequate perfusion pressure are often helpful (32),hereas agents with a more pronounced chronotropic or
notropic effect should be avoided when possible. Rarely,emporary femoral cardiopulmonary support might be re-uired, although most often relief of aortic stenosis is associ-ted with prompt improvement of the LV function andmprovement of hemodynamic status can be expected. Should
he aortic annulus and subvalvular tissues. (B and C) After valve implanta-ft ventricular outflow tract and left atrium, with large left ventricular to left
n of tthe le
hest compressions be required, post-resuscitation evaluation

ocArahfesamcSmditcss
C
Spnpit
RPC
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 2 , N O . 9 , 2 0 0 9 Masson et al.
S E P T E M B E R 2 0 0 9 : 8 1 1 – 2 0 Transcatheter Aortic Valve Implantation
819
f the stent position and expansion (Fig. 6B) might beonsidered.cute renal failure. Aortic stenosis is often associated withenal dysfunction due to renal pathology, medications,nd low cardiac output. Angiographic contrast injection,ypotension, and atheroembolism might contribute tourther reduction of the glomerular filtration rate. How-ver, improved renal perfusion after relief of aortictenosis has a salutary effect on renal function, andlthough severe renal dysfunction and dialysis require-ent might occur, improvement in renal function is most
ommon.tructural valve failure. Acute valve failure has been docu-ented very rarely. Potential causes include manufacturing
efects, leaflet damage during crimping or implantation andnadequate closing pressure due to abnormal flow charac-eristics. If structural valve failure is suspected to be theause for significant valvular regurgitation, implantation of aecond valve within the failed valve has been shown to be auccessful strategy (1).
onclusions
ymptomatic aortic stenosis is associated with a dismalrognosis. Any intervention designed to relieve aortic ste-osis carries both the potential for benefit and risk. Im-roved understanding of these potential risks will likelymprove the safety and widen the potential application ofranscatheter aortic valve replacement.
eprint requests and correspondence: Dr. John G. Webb, St.aul’s Hospital, 1081 Burrard Street, Vancouver, BC V6Z 1Y6,anada. E-mail: [email protected].
EFERENCES
1. Svensson LG, Dewey T, Kapadia S, et al. United States feasibilitystudy of transcatheter insertion of a stented aortic valve by the leftventricular apex. Ann Thorac Surg 2008;86:46–55.
2. Walther T, Falk V, Kempfert J, et al. Transapical minimally invasiveaortic valve implantation; the initial 50 patients. Eur J CardiothoracSurg 2008;33:983–8.
3. Grube E, Schuler G, Buellesfeld L, et al. Percutaneous aortic valvereplacement for severe aortic stenosis in high-risk patients using thesecond- and current third-generation self-expanding CoreValve pros-thesis: device success and 30-day clinical outcome. J Am Coll Cardiol2007;50:69–76.
4. Webb JG, Pasupati S, Humphries K, et al. Percutaneous transarterialaortic valve replacement in selected high-risk patients with aorticstenosis. Circulation 2007;116:755–63.
5. Walther T, Simon P, Dewey T, et al. Transapical minimally invasiveaortic valve implantation: multicenter experience. Circulation 2007;116:I240–5.
6. Ye J, Cheung A, Lichtenstein SV, et al. Transapical aortic valveimplantation in humans. J Thorac Cardiovasc Surg 2006;131:1194–6.
7. Webb JG, Chandavimol M, Thompson CR, et al. Percutaneous aorticvalve implantation retrograde from the femoral artery. Circulation2006;113:842–50.
8. Grube E, Laborde JC, Gerckens U, et al. Percutaneous implantation ofthe CoreValve self-expanding valve prosthesis in high-risk patients
with aortic valve disease: the Siegburg First-In-Man study. Circulation2006;114:1616–24.
9. Masson J-B, Al Bugami S, Webb JG. Endovascular balloon occlusionfor catheter-induced large artery perforation in the catheterizationlaboratory. Catheter Cardiovasc Interv 2009;73:514–8.
0. Ruge H, Lange R, Bleiziffer S, et al. First successful aortic valveimplantation with the CoreValve ReValving System via right subcla-vian artery access: a case report. Heart Surg Forum 2008;11:E323–4.
1. Bauernschmitt R, Schreiber C, Bleiziffer S, et al. Transcatheter aorticvalve implantation through the ascending aorta: an alternative optionfor no-access patients. Heart Surg Forum 2009;12:E63–4.
2. Walther T, Falk V, Borger MA, et al. Minimally invasive transapicalbeating heart aortic valve implantation—proof of concept. Eur J Car-diothorac Surg 2007;31:9–15.
3. Berry C, Cartier R, Bonan R. Fatal ischemic stroke related to nonpermissive peripheral artery access for percutaneous aortic valve re-placement. Catheter Cardiovasc Interv 2007;69:56–63.
4. Isner J. Acute catastrophic complications of balloon aortic valvulo-plasty. The Mansfield Scientific Aortic Valvuloplasty Registry Inverti-gators. J Am Coll Cardiol 1991;17:1436–44.
5. Webb JG, Altwegg L, Boone RH, et al. Transcatheter aortic valvereplacement: impact on clinical and valve-related outcomes. Circulation2009;119:3009–16.
6. Cribier A, Eltchaninoff H, Tron C, et al. Treatment of calcific aorticstenosis with the percutaneous heart valve: mid-term follow-up fromthe initial feasibility studies: the French experience. J Am Coll Cardiol2006;47:1214–23.
7. Al Ali AM, Altwegg L, Horlick EM, et al. Prevention and manage-ment of transcatheter balloon-expandable aortic valve malposition.Catheter Cardiovasc Interv 2008;72:573–8.
8. Tuzcu ME. Transcatheter aortic valve replacement malposition andembolization: innovation brings solutions also new challenges. CatheterCardiovasc Interv 2008;72:579–80.
9. Buellesfeld L, Gerckens U, Grube E. Percutaneous implantation of thefirst repositionable aortic valve prosthesis in a patient with severe aorticstenosis. Catheter Cardiovasc Interv 2008;71:579–84.
0. Geist V, Sherif MA, Khattab AA. Successful percutaneous coronaryintervention after implantation of a CoreValve percutaneous aorticvalve. Catheter Cardiovasc Interv 2009;73:61–7.
1. Lu TL, Huber CH, Rizzo E, Dehmeshki J, von Segesser LK, QanadliSD. Ascending aorta measurements as assessed by ECG-gated multi-detector computed tomography: a pilot study to establish normativevalues for transcatheter therapies. Eur Radiol 2009;19:664–9.
2. Cribier A, Eltchaninoff H, Tron C, et al. Early experience withpercutaneous transcatheter implantation of heart valve prosthesis forthe treatment of end-stage inoperable patients with calcific aorticstenosis. J Am Coll Cardiol 2004;43:698–703.
3. Cribier A, Eltchaninoff H, Bash A, et al. Percutaneous transcatheterimplantation of an aortic valve prosthesis for calcific aortic stenosis: firsthuman case description. Circulation 2002;106:3006–8.
4. Hanzel GS, Harrity PJ, Schreiber TL, O’Neill WW. Retrogradepercutaneous aortic valve implantation for critical aortic stenosis.Catheter Cardiovasc Interv 2005;64:322–6.
5. Wong DR, Boone RH, Thompson CR, et al. Mitral valve injury lateafter transcatheter aortic valve implantation. J Thorac Cardiovasc Surg2009l;137:1547–9.
6. Murphy CJ, Pasupati S, Webb JG. Hemolysis after transcatheterballoon-expandable aortic valve insertion. Can J Cardiol 2007;23:260.
7. Hayes SN, Holmes DR Jr., Nishimura RA, Reeder GS. Palliativepercutaneous aortic balloon valvuloplasty before noncardiac operations andinvasive diagnostic procedures. Mayo Clin Proc 1989;64:753–7.
8. Dawkins S, Hobson AR, Kalra PR, Tang ATM, Monro JL, DawkinsKD. Permanent pacemaker implantation after isolated aortic valvereplacement: incidence, indications, and predictors. Ann Thorac Surg2008;85:108–12.
9. Sinhal A, Altwegg L, Pasupati S, et al. Atrioventricular block aftertranscatheter balloon expandable aortic valve implantation. J Am Coll
Cardiol Intv 2008;1:305–9.
3
3
3
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 2 , N O . 9 , 2 0 0 9
S E P T E M B E R 2 0 0 9 : 8 1 1 – 2 0
Masson et al.
Transcatheter Aortic Valve Implantation
820
0. Piazza N, Onuma Y, Jesserun E, et al. Early and persistent intraven-tricular conduction abnormalities and requirements for pacemakingafter percutaneous replacement of the aortic valve. J Am Coll CardiolIntv 2008;1:310–6.
1. Vahanian A, Alfieri O, Al-Attar N, et al. Transcatheter valve implanta-tion for patients with aortic stenosis: a position statement from theEuropean Association of Cardio-Thoracic Surgery (EACTS) and the
European Society of Cardiology (ESC), in collaboration with the Euro- Kpean Association of Percutaneous Cardiovascular Interventions (EAPCI).Eur Heart J 2008;29:1463–70.
2. Fassl J, Walther T, Groesdonk HV, et al. Anesthesia management fortransapical transcatheter aortic valve implantation: a case series. J Car-diothorac Vasc Anesth 2009;23:286–91.
ey Words: aortic valve � catheter � complication.





























