Embed Size (px)
Citation preview

For peer review only
Tranexamic Acid in Hip Fracture Patients: a protocol for a randomized, placebo controlled trial on the efficacy of
tranexamic acid in reducing blood loss in hip fracture patients
Journal: BMJ Open
Manuscript ID bmjopen-2015-010676
Article Type: Protocol
Date Submitted by the Author: 25-Nov-2015
Complete List of Authors: Gausden, Elizabeth; Hospital for Special Surgery, Orthopaedic Surgery Garner, Matthew; Hospital for Special Surgery, Orthopaedic Surgery Warner, Stephen; Hospital for Special Surgery, Orthopaedic Surgery Nellenstein, Andrew; Hospital for Special Surgery, Orthopaedic Surgery Tedore, Tiffany; Weill Cornell Medical College, Anesthesia Flores, Eva; Weill Cornell Medical College, Internal Medicine Lorich, Dean; Hospital for Special Surgery, Orthopaedic Surgery
<b>Primary Subject Heading</b>:
Surgery
Secondary Subject Heading: Evidence based practice, Haematology (incl blood transfusion)
Keywords: tranexamic acid, hip fracture, blood transfusion
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on 26 July 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010676 on 21 June 2016. D
ownloaded from

For peer review only
1
Tranexamic Acid in Hip Fracture patients: a 1
protocol for a randomized, placebo controlled trial 2
on the efficacy of tranexamic acid in reducing 3
blood loss in hip fracture patients 4
5
Elizabeth Gausden, MD; Matthew R. Garner, MD; Stephen J. Warner, MD, PhD; 6 Andrew Nellenstein, BS; Tiffany Tedore, MD; Eva Flores, MD; Dean G. Lorich, MD 7
8
9
10
Abstract 11
Introduction 12
There is a high incidence of blood transfusion following hip fractures in elderly 13
patients. Tranexamic acid (TXA) has proven efficacy in decreasing blood loss in 14
trauma patients as well as patients undergoing elective orthopaedic surgery. In 15
order to prove the efficacy of TXA, a randomized controlled trial will measure the 16
effect in a population of patients undergoing hip fracture surgery. 17
Methods 18
This is a double-blinded, randomized placebo-controlled trial. Patients admitted 19
through the emergency room diagnosed with an intertrochanteric or femoral neck 20
fracture will be eligible for enrollment and randomized to either treatment with 1 21
gram of intravenous TXA or intravenous saline at the time of skin incision. Patients 22
undergoing percutaneous intervention for non or minimally displaced femoral neck 23
fractures will not be eligible for enrollment. Postoperative transfusion rates will be 24
recorded and blood loss will be calculated from serial hematocrits. 25
Page 1 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
2
Ethics and dissemination 26
This protocol was approved by the Institutional Review Board (IRB) and is 27
registered with clinicaltrials.gov. The findings of the trial will be disseminated 28
through peer-reviewed journals and conference presentations. 29
30
Strengths and limitations of this study 31
• A prospective, randomized, placebo-controlled trial is the optimal study 32
design to address the question of efficacy of tranexamic acid (TXA) use in 33
patients with hip fractures 34
• The outcomes will be reported based on one-year follow-up, which is longer 35
follow-up than any other study examining tranexamic acid use in patients 36
with hip fractures. 37
• Findings will provide objective data from which clinicians can base future 38
guidelines regarding TXA administration 39
• Recruitment is slow as patients and health-care proxies are wary of enrolling 40
in a study in a trauma setting 41
42
Introduction 43
44
Hip fractures in the elderly remains a pressing public health issue in the United 45
States given the aging population. 1 Hip fractures are associated with numerous 46
adverse events and increased mortality up to one year after the event. 2-5 Elderly 47
patients sustaining hip fractures commonly lose more than one liter of blood and up 48
Page 2 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
3
to 60% will require a blood transfusion. 6 A meta-analysis of 20 studies found a 49
significantly increased risk of post-operative bacterial infection in patients who 50
receive an allogenic blood transfusion in the perioperative period. 7 In addition to 51
the increased risk of infection, patients who require blood transfusion following hip 52
fracture have an increased hospital length of stay. 8 Beyond the risk to the patient 53
from a blood transfusion, an allogenic blood transfusion in the United States was 54
recently estimated to increase costs by $1,731 per admission. 9 55
56
Numerous anti-fibrinolytics have been used to limit bleeding in orthopaedic surgery 57
and prevent the need for blood transfusion. 10-14 One of these anti-fibrinolytics, 58
tranexamic acid (TXA) is a synthetic derivative of the amino acid lysine and acts as a 59
competitive inhibitor in the activation of plasminogen to plasmin and therefore 60
prevents the degradation of fibrin. As a result of the CRASH-2 trial 15,16 that 61
demonstrated reduced mortality in trauma patients administered TXA the World 62
Health Organization (WHO) added it to the essential drugs list. Currently TXA is not 63
routinely used in patients with hip fractures in the United States, despite its 64
common use worldwide and proven efficacy in reducing blood loss. 65
66
Numerous studies have investigated the safety and efficacy of TXA in patients 67
undergoing elective orthopaedic surgery, including total joint replacement and 68
spine surgery. 17-22 The consensus from this literature is overwhelmingly in favor of 69
administration of TXA given the decrease in blood loss, transfusion rates, and cost. 70
23,24 Although several individual studies have found increased risk of 71
Page 3 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
4
thromboembolic events in groups receiving TXA, 25,26 larger studies and meta-72
analyses have uniformly found no increased risk of thrombosis. 27,28 73
74
Patients who suffer hip fractures frequently have multiple comorbidities making 75
them more susceptible to adverse events from blood loss. 19,20 The most common 76
comorbidities of individuals with hip fractures are congestive heart failure, chronic 77
pulmonary disease and diabetes. 1 Administering TXA to such patients has a 78
potential to offset blood loss, improve patient outcome and lower cost by decreasing 79
the rate of transfusions. 29,30 Five studies, all conducted outside the United States, 80
have reported results of using TXA in hip fracture surgery. 26,31-34 Sadeghi et al 32 81
randomized 67 hip fracture patients to receive either placebo injection or 82
intravenous tranexamic acid at the time of surgery. They found a significantly lower 83
volume of blood loss (652 ± 228 mL vs. 1108 ± 372 mL, P < 0.003) and shorter 84
hospital stays (4.3 ± 1.6 days vs. 5.8 ± 1.5 days, p< 0.05). Vijay et al. 34 also reported 85
significantly reduced transfusion rates in the TXA arm of their clinical trial. In a 86
retrospective cohort study, Lee et al 31 reported similar results, a transfusion rate 87
three times lower in patients who received TXA prior to hemiarthroplasty surgery. 88
In a separate randomized controlled trial that compared intravenous administration 89
of TXA to topical TXA administration as well as placebo in hip fracture patients 90
undergoing hemiarthroplasty, both of the TXA groups experienced less blood loss. 26 91
While this study found a significant reduction in blood loss and transfusion rates in 92
both TXA groups, they found a higher incidence of thromboembolic events in the 93
intravenous TXA group. 94
Page 4 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
5
Of the five studies investigating the use of TXA in hip fracture patients, four 95
were randomized controlled trials that were underpowered for detecting significant 96
differences in thromboembolic events (Table 1). 26,31-34 Furthermore, patients were 97
only followed perioperatively, and differences in six-month and one-year mortality 98
rates and late-onset complications were not assessed. 99
Use of Tranexamic Acid (TXA) in Patients with Hip Fractures
Country Design Hip fx ( IT or FNF)
TXA Regimen
DVT PPX Sample size
Blood loss (cc)
Transfuse Rate %
Thrombo-embolic Events
Lee 2015 31
UK Cohort Hemi-arthroplasy only
1 g bolus preop
Tinzaparin 84 cases/ 187 controls
- 6* 1
- 19 4
Emara 2014 26
Egypt RCT Hemi-arthroplasty only
10 mg/kg bolus, then 5 mg/kg/h infusion
Clexane 20 cases IV/ 20 cases topical/20 controls
640 5* 5
1100 32 0
Zufferey 2010 33
France RCT Hip fractures
15 mg/kg bolus preop and 3 h later
Fondaparinux x 35 days (mandatory ultrasound)
57 cases/ 53 controls
975 42 0
1178 60 0
Sadeghi and Mehr-Aein 2006 32
Iran RCT Hip fractures
15 mg/kg bolus preop
n/a
32 cases/ 35 controls
960 37 0
1484 57 0
Vijay 2013 34
India RCT Hip fractures
10 mg/kg bolus at surgery
N/a 45 cases/ 45 controls
39* 16 0
91* 40 0
100
In designing this study, we concluded that hip fracture patients are both likely to 101
experience significant blood loss and are susceptible to the adverse effects of blood 102
loss making them an ideal population to target for a randomized controlled trial of 103
the effects of perioperative TXA on blood loss. We hypothesize that administration 104
Page 5 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
6
of TXA will decrease blood loss in hip fracture patients and lower the rate of 105
allogenic blood transfusion. 106
107
108
109
Objective 110
To investigate the hypothesis that TXA will lower blood loss and transfusion rate in 111
patients with hip fractures. 112
113
Methods and analysis 114
115
Overview of trial design 116
We are conducting a single-center randomized control trial using a parallel two-arm 117
design to investigate whether tranexamic acid use perioperatively will decrease the 118
rate of transfusion in patients with hip fractures (Figure 1). Randomization will be 119
stratified by type of hip fracture, intertrochanteric and femoral neck fractures. The 120
surgical team, anesthesia team, and patients will be blinded to the assignment. Once 121
consent is obtained and a patient is enrolled, a 1:1 randomization system will be 122
employed by our institution’s investigational pharmacy to assign patients to receive 123
TXA or placebo. Patient enrollment will occur over approximately 2 years and 124
enrolled patients will be followed for 1 year postoperatively. Incidence of blood 125
transfusion, total calculated blood loss, transfusion, and acute adverse events 126
(transfusion reaction, cerebrovascular accident, myocardial infarction, pulmonary 127
Page 6 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
7
embolism, and surgical site infection) will be assessed in the perioperative period. 128
Patients will also be assessed at 2 week, 6 week, 3 month, 6 month and 12 month 129
follow-up for long-term adverse events as well as mortality rate. This trial is 130
registered (NCT01940536) and has received ethics approval from the Weill Cornell 131
Medical College Institutional Review Board (IRB# 1301013463). 132
133
134
Primary research question 135
In patients with hip fractures, does infusion of tranexamic acid at the time of 136
surgery result in lower rate of blood transfusion? 137
138
Secondary research question 139
In patients with hip fractures, does infusion of tranexamic acid at the time of 140
surgery result in: 141
1.) decreased blood loss? 142
2.) Shorter length of hospitalization? 143
3.) Any differences in occurrence of adverse events? 144
145
Hypothesis 146
As a primary outcome, there will be a decreased rate of blood transfusion in patients 147
who receive tranexamic acid intraoperatively and no significant increase in 148
frequency or severity of adverse events in comparison to patients who receive 149
Page 7 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
8
placebo. This study is powered to address the primary outcome of difference in 150
transfusion rates between the two study arms. 151
152
Setting and participants 153
Adult (over 18 years of age) patients presenting to a single tertiary care center with 154
a hip fracture. All patients with hip fractures at this institution are admitted to the 155
medical orthopaedic trauma service (MOTS). Prior to surgery, patients older than 156
75 years of age, or those with medical comorbidities will be cleared by the general 157
medical service prior to surgery. All potentially eligible patients will be screened 158
and documented as (1) eligible and included, (2) eligible and missed, or (3) 159
excluded. The study coordinator will obtain informed consent for participation in 160
the study using the approved IRB Informed Consent forms. 161
162
All patients will provide written informed consent and will understand that by 163
entering in the study they may receive placebo and not tranexamic acid. 164
Participation in the study is voluntary and their decision to participate will not 165
affect any other aspect of their care in case of refusal. Patients will have the right to 166
withdraw from the study at any point. 167
168
169
170
Inclusion criteria 171
Page 8 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
9
Patients admitted through the emergency room or transferred into our institution 172
and who meet the following criteria will be included in the study: 173
• Adults over the age of 18 174
• Intertrochanteric or femoral neck hip fracture 175
• Patients treated surgically with cephalomedullary nail or hemiarthroplasty 176
177
Exclusion criteria 178
Patient who meet any one or more of the following criteria will be excluded from the 179
study: 180
• Preoperative use of anticoagulant (Plavix, Warfarin, Lovenox) 181
• Documented allergy to tranexamic acid 182
• History of deep vein thrombosis or pulmonary embolus 183
• Hepatic dysfunction (AST/ALT > 60) 184
• Renal dysfunction (Cr >1.5 of GRR > 30) 185
• Active coronary artery disease (event in the past 12 months), history of 186
cerebrovascular accident (CVA) in the past 12 months, or presence of a drug-187
eluting stent 188
• Color blindness 189
• Leukemia or any active cancer 190
• Coagulopathy (INR> 1.4, PTT > 1.4x normal, Platelets < 100,000) 191
• Non-displaced femoral neck fractures treated percutaneously 192
193
Baseline 194
Page 9 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
10
Baseline assessment includes sex, birth date, height and weight, mechanism of 195
injury, time from injury to presentation to the emergency room, American Society of 196
Anesthesiologists (ASA) classification, Charlson Comorbidity Index, comorbidities 197
including diabetes, peripheral vascular disease, dementia, hypertension, and history 198
of smoking. The hemoglobin and hematocrit will be recorded at the time of 199
admission and on the morning of surgery, if applicable. 200
201
Blinding 202
After the patient consents and is enrolled in the study, the institution’s 203
investigational pharmacist will perform the randomization and assign the patient to 204
either receive TXA or placebo. Patients will be randomized in blocks of 20. The 205
packaging of the injections will be performed by the investigational pharmacy and 206
will be identical for both TXA and placebo. All clinicians, except for the pharmacist, 207
will remain blinded until the data is analyzed. 208
209
Intervention 210
The patients randomized to the treatment arm will receive 1 gram of intravenous 211
tranexamic acid infused at the time of surgical incision. Those assigned to the 212
placebo group will receive an infusion of saline at the time of surgical incision. 213
Patients with intertrochanteric hip fractures will be treated with a long, 214
intramedullary, cephalomedually implant with a trochanteric start point. Patients 215
with displaced femoral neck fractures will be treated with a cemented or non-216
Page 10 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
11
cemented hemiarthroplasty or total hip arthroplasty at the discretion of the treating 217
surgeon. 218
219
Blood transfusion criteria will remain consistent with hospital standards (Hb<8 220
g/dL or symptomatic anemia) as determined by an independent, blinded medical 221
team who will follow the patient throughout the hospital stay and number of blood 222
transfusions received will be documented upon patient discharge. Hematocrit and 223
hemoglobin will be recorded in all patients while they are in the hospital, for a 224
minimum of 2 days postoperatively. Further monitoring will be conducted based on 225
need as determined by the independent medical team. Estimated blood volume will 226
be calculated from these values and used to estimate blood loss (Appendix 1). 227
228
All patients will be permitted to weight-bear as tolerated post-operatively and deep 229
vein thrombosis (DVT) prophylaxis will be standardized. All enrolled patients will 230
receive subcutaneous heparin, 5000 units every 8 hours beginning upon admission 231
until 12 hours prior to surgery and restarting 6 hours after surgery. Calf mechanical 232
compression devices will also be utilized during the inpatient stay and will remain 233
on at all times with the exception of physical therapy sessions. Following discharge 234
from the hospital patients will be given aspirin 325 mg twice daily for DVT 235
prophylaxis for a total of 6 weeks. Diagnostic studies to assess for thromboembolic 236
events (i.e. DVT, pulmonary embolism, and stroke) will be ordered only if the 237
patient develops clinical signs or symptoms that justify their use. 238
Primary Outcome 239
Page 11 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
12
The primary outcome of the study will be the rate of blood transfusion in the 240
postoperative period until time of discharge. Patients will be monitored with serial 241
hemoglobin and hematocrit measurements and their vital signs will be recorded as 242
per the standard of care to determine the need for blood transfusion. 243
Secondary Outcome 244
The secondary study outcomes include the calculated blood loss (calculated based 245
on validated methods as outlined in Appendix 1), frequency of adverse events 246
(including transfusion reaction, myocardial infarction, deep vein thrombosis, 247
pulmonary embolus, cerebrovascular accident, re-operation, re-admission, 248
infection, and death) (Figure 1). 249
250
Sample size consideration 251
The transfusion rate amongst patients with hip fractures is between 19-60%. 26,31-34 252
The average reduction in transfusion rate in the previous 5 studies using TXA was 253
20%. 26,31-34 We plan to include 110 patients in each treatment arm for a total of 254
220 patients. This study design will achieve 81% power to detect a reduction in 255
blood transfusion from 40% in the placebo control group to 20% in the tranexamic 256
acid group using two-sided Fisher’s exact test with statistical significance set to 257
alpha equal to 0.05. 258
259
260
Data analysis plan 261
Descriptive analyses of the patient population will include reporting means (with 262
Page 12 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
13
standard deviations) for continuous variables and frequencies (with percentages) 263
for categorical or discrete variables. Following the descriptive analysis, a chi-square 264
analysis will be conducted to evaluate the superiority of tranexamic acid in reducing 265
the rate of transfusion versus the placebo control group. The analysis and reporting 266
of the results of the clinical outcomes will follow the CONSORT guidelines 267
(www.consort-statement.org). We will conduct a multiple logistic regression model 268
to determine if type of fracture (intertrochanteric or femoral neck), comorbidities, 269
Charlson comorbidity index, age, time to surgery, and mechanism of injury are 270
related to transfusion administration. Similarly we will conduct a multiple linear 271
regression model to determine if patient comorbidities, age, time to surgery, and 272
mechanism of injury are related to blood loss. We will also conduct subgroup 273
analyses to determine if the effect of TXA is modified by fracture type 274
(intertrochanteric or femoral neck). 275
Our a priori hypothesis, based on retrospective data, 6 is that patients with 276
intertrochanteric fractures incur more blood loss than femoral neck fractures and 277
will have a higher rate of transfusion. If these subgroup analyses are 278
underpowered, the subgroup data will be used to generate further hypotheses to be 279
tested in the future. All analyses will be performed using Stata 14.0 software (Stata 280
Corporation, College Station, TX, USA). 281
282
Data safety monitoring 283
Page 13 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
14
The data safety monitoring board (DSMB) has been established to monitor the trial 284
and renew the study biannually. This board is independent of the trial and free of 285
conflicts with any of the investigation team. 286
287
Discussion 288
There is clinical uncertainty and a lack of high-quality evidence regarding the use of 289
TXA in hip fracture patients. Despite its proven efficacy in elective orthopaedic 290
surgery, 20,35 the optimal dosing and timing of TXA administration is still debated. 36 291
Furthermore, the efficacy and side effect profile of TXA in patients with fractures 292
remains unclear. The immediate goal of this trial is to provide high-quality evidence 293
that can be used to develop clinical guidelines for use of TXA in patients with hip 294
fractures. 295
296
Patients undergoing total joint arthroplasty and elective spine surgery represent a 297
different population from patients who sustain hip fractures. A larger percentage of 298
hip fracture patients have significant medical comorbidities, and many have history 299
of cardiac disease. 1 While TXA has demonstrated safety and efficacy in patients 300
without significant cardiac disease undergoing elective surgery, there is still debate 301
if TXA will have the same effect in patients with significant comorbidities. 20,36,37 The 302
data investigating TXA in patients with comorbidities is limited, which has further 303
deterred clinicians from using TXA in patients with hip fractures. However, the 304
potential benefit of decreasing blood loss and decreasing the number of transfusions 305
following hip fracture surgery is overwhelming and will likely result in improved 306
Page 14 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
15
patient outcomes, shorter length of stay and lower cost. The study investigators 307
believe that the potential benefit of TXA in such patients outweighs the risk of TXA. 308
The majority of literature regarding TXA has confirmed its safety and squelched 309
concerns that its use will result in higher rates of thrombosis. 15,25,28,37,38 310
311
The literature to date regarding TXA and hip fractures (Table 1) is limited. Four out 312
of five studies identified a significant decrease in rate of transfusion in patients who 313
received TXA compared to those that did not. 26,31-34 The largest study, with a total 314
of 219 patients, was a cohort study with no randomization. 31 Furthermore, the 315
studies did not follow patients up to 1 year postoperatively, which is our intention. 316
The extended follow-up period allows for assessment of mortality at 12 months as 317
well as incidence of unanticipated adverse events following discharge from the 318
hospital. 319
320
Tranexamic acid has the potential to decrease transfusion rates by decreasing blood 321
loss in patients with hip fractures. Ultimately, this will decreased hospital length of 322
stay and improve outcomes in the hundreds of thousands of patients with hip 323
fractures every year. If the results prove the efficacy of TXA in hip fracture patients, 324
this study may change the standard of care across the United States for these 325
patients. 326
327
Funding 328
This work is supported by a Dr. Thomas Sculco grant. 329 330
Page 15 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
16
331
332
333
Appendix 334
Blood Loss Calculation:Patient’s Blood Volume (PBV) = (k1 x Height3
(m)) + (k2 x Weight (kg)) + k3 335
k1 = 0.3669, k2 = 0.03219, and k3 = 0.6041 for men k1 = 0.3561, k2=0.03308, and k3 = 0.1833 for 336 women 337
Multiplying the PBV by the hematocrit (Hct) gives the red blood cell (RBC) volume. As 338
such, a change in the RBC volume can be calculated from a change in the Hct level as 339
follows: 340
Pre-op RBC volume loss = PBV x (Admit Hct – Day of surgery Hct) Operative RBC volume loss = PBV x 341 (Day of surgery Hct – PACU Hct) 342
If a patient requires a pre-op or intraoperative transfusion, the calculation will be adjusted as 343 follows: 344
Pre-op RBC volume loss = [PBV x (Admit Hct – Day of surgery Hct)]+ (No. of Units Transfused x 345 0.285) / (Admit Hct – Day of surgery Hct) / 2)Operative RBC volume loss = [PBV x (Day of surgery 346 Hct – PACU Hct)] +)]+ (No. of Units Transfused x 0.285) / (Day of surgery Hct – Post-op Hct) / 2 347
348
349
350
351
352
Figure Legend 353
354
Figure 1: Study Design (TXA: tranexamic acid; PRBC: packed red blood cells) 355
356
Table 1: Previously reported outcomes of TXA in hip fracture patients. *drain 357 output. Thromboembolic events include only symptomatic thromboembolic events. 358 359
Page 16 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
17
Contributorship Statement: 360
Elizabeth B. Gausden: This author made substantial contributions to the design of 361 the work, planning of data analysis, drafting and revising of the protocol, final 362 approval of the version to be published and agrees to be accountable for all aspects 363 of the work in ensuring that questions related to the accuracy of the work. 364 Matthew R. Garner: This author made substantial contributions to conception of the 365 study and the design of the work, planning of data analysis, drafting and revising of 366 the protocol, final approval of the version to be published and agrees to be 367 accountable for all aspects of the work in ensuring that questions related to the 368 accuracy of the work. 369 Stephen Warner: This author made substantial contributions to the design of the 370 work, planning of data analysis, drafting and revising of the protocol, final approval 371 of the version to be published and agrees to be accountable for all aspects of the 372 work in ensuring that questions related to the accuracy of the work. 373 Andrew Nellenstein: This author made substantial contributions to the design of the 374 work, planning of data analysis, drafting and revising of the protocol, final approval 375 of the version to be published and agrees to be accountable for all aspects of the 376 work in ensuring that questions related to the accuracy of the work. 377 Tiffany Tedore: This author made substantial contributions to the design of the 378 work, planning of data analysis, drafting and revising of the protocol, final approval 379 of the version to be published and agrees to be accountable for all aspects of the 380 work in ensuring that questions related to the accuracy of the work. 381 Eva Flores: This author made substantial contributions to the design of the work, 382 planning of data analysis, drafting and revising of the protocol, final approval of the 383 version to be published and agrees to be accountable for all aspects of the work in 384 ensuring that questions related to the accuracy of the work. 385 Dean G. Lorich: This author made substantial contributions to the design of the 386 work, planning of data analysis, drafting and revising of the protocol, final approval 387 of the version to be published and agrees to be accountable for all aspects of the 388 work in ensuring that questions related to the accuracy of the work. 389
390
Competing Interests: 391
No, there are no competing interests 392
393
394
395
396
397
Page 17 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
18
References 398
1. Brauer CA, Coca-Perraillon M, Cutler DM, Rosen AB. Incidence and mortality of 399
hip fractures in the united states. JAMA. 2009;302(14):1573-1579. 400
2. Richmond J, Aharonoff GB, Zuckerman JD, Koval KJ. Mortality risk after hip 401
fracture. J Orthop Trauma. 2003;17(1):53-56. 402
3. Heyes GJ, Tucker A, Marley D, Foster A. Predictors for 1-year mortality following 403
hip fracture: A retrospective review of 465 consecutive patients. Eur J Trauma 404
Emerg Surg. 2015. 405
4. Shah MR, Aharonoff GB, Wolinsky P, Zuckerman JD, Koval KJ. Outcome after hip 406
fracture in individuals ninety years of age and older. J Orthop Trauma. 407
2001;15(1):34-39. 408
5. Sathiyakumar V, Greenberg SE, Molina CS, Thakore RV, Obremskey WT, Sethi MK. 409
Hip fractures are risky business: An analysis of the NSQIP data. Injury. 410
2015;46(4):703-708. 411
6. Foss NB, Kehlet H. Hidden blood loss after surgery for hip fracture. J Bone Joint 412
Surg Br. 2006;88(8):1053-1059. 413
7. Hill GE, Frawley WH, Griffith KE, Forestner JE, Minei JP. Allogeneic blood 414
transfusion increases the risk of postoperative bacterial infection: A meta-analysis. J 415
Trauma. 2003;54(5):908-914. 416
Page 18 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
19
8. Shokoohi A, Stanworth S, Mistry D, Lamb S, Staves J, Murphy MF. The risks of red 417
cell transfusion for hip fracture surgery in the elderly. Vox Sang. 2012;103(3):223-418
230. 419
9. Saleh A, Small T, Chandran Pillai AL, Schiltz NK, Klika AK, Barsoum WK. Allogenic 420
blood transfusion following total hip arthroplasty: Results from the nationwide 421
inpatient sample, 2000 to 2009. J Bone Joint Surg Am. 2014;96(18):e155. 422
10. Kagoma YK, Crowther MA, Douketis J, Bhandari M, Eikelboom J, Lim W. Use of 423
antifibrinolytic therapy to reduce transfusion in patients undergoing orthopedic 424
surgery: A systematic review of randomized trials. Thromb Res. 2009;123(5):687-425
696. 426
11. Eubanks JD. Antifibrinolytics in major orthopaedic surgery. J Am Acad Orthop 427
Surg. 2010;18(3):132-138. 428
12. Yuan C, Zhang H, He S. Efficacy and safety of using antifibrinolytic agents in spine 429
surgery: A meta-analysis. PLoS One. 2013;8(11):e82063. 430
13. Zufferey P, Merquiol F, Laporte S, et al. Do antifibrinolytics reduce allogeneic 431
blood transfusion in orthopedic surgery? Anesthesiology. 2006;105(5):1034-1046. 432
14. Tse EY, Cheung WY, Ng KF, Luk KD. Reducing perioperative blood loss and 433
allogeneic blood transfusion in patients undergoing major spine surgery. J Bone Joint 434
Surg Am. 2011;93(13):1268-1277. 435
Page 19 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
20
15. CRASH-2 trial collaborators, Shakur H, Roberts I, et al. Effects of tranexamic acid 436
on death, vascular occlusive events, and blood transfusion in trauma patients with 437
significant haemorrhage (CRASH-2): A randomised, placebo-controlled trial. Lancet. 438
2010;376(9734):23-32. 439
16. CRASH-2 collaborators, Roberts I, Shakur H, et al. The importance of early 440
treatment with tranexamic acid in bleeding trauma patients: An exploratory 441
analysis of the CRASH-2 randomised controlled trial. Lancet. 2011;377(9771):1096-442
101, 1101.e1-2. 443
17. Whiting DR, Gillette BP, Duncan C, Smith H, Pagnano MW, Sierra RJ. Preliminary 444
results suggest tranexamic acid is safe and effective in arthroplasty patients with 445
severe comorbidities. Clin Orthop Relat Res. 2014;472(1):66-72. 446
18. Cid J, Lozano M. Tranexamic acid reduces allogeneic red cell transfusions in 447
patients undergoing total knee arthroplasty: Results of a meta-analysis of 448
randomized controlled trials. Transfusion. 2005;45(8):1302-1307. 449
19. Lemay E, Guay J, Cote C, Roy A. Tranexamic acid reduces the need for allogenic 450
red blood cell transfusions in patients undergoing total hip replacement. Can J 451
Anaesth. 2004;51(1):31-37. 452
20. Poeran J, Rasul R, Suzuki S, et al. Tranexamic acid use and postoperative 453
outcomes in patients undergoing total hip or knee arthroplasty in the united states: 454
Retrospective analysis of effectiveness and safety. BMJ. 2014;349:g4829. 455
Page 20 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
21
21. Raksakietisak M, Sathitkarnmanee B, Srisaen P, et al. Two doses of tranexamic 456
acid reduce blood transfusion in complex spine surgery: A prospective randomized 457
study. Spine (Phila Pa 1976). 2015. 458
22. Wind TC, Barfield WR, Moskal JT. The effect of tranexamic acid on transfusion 459
rate in primary total hip arthroplasty. J Arthroplasty. 2014;29(2):387-389. 460
23. Tuttle JR, Ritterman SA, Cassidy DB, Anazonwu WA, Froehlich JA, Rubin LE. Cost 461
benefit analysis of topical tranexamic acid in primary total hip and knee 462
arthroplasty. J Arthroplasty. 2014;29(8):1512-1515. 463
24. Huang F, Wu D, Ma G, Yin Z, Wang Q. The use of tranexamic acid to reduce blood 464
loss and transfusion in major orthopedic surgery: A meta-analysis. J Surg Res. 465
2014;186(1):318-327. 466
25. Nishihara S, Hamada M. Does tranexamic acid alter the risk of thromboembolism 467
after total hip arthroplasty in the absence of routine chemical thromboprophylaxis? 468
Bone Joint J. 2015;97-B(4):458-462. 469
26. Emara WM, Moez KK, Elkhouly AH. Topical versus intravenous tranexamic acid 470
as a blood conservation intervention for reduction of post-operative bleeding in 471
hemiarthroplasty. Anesth Essays Res. 2014;8(1):48-53. 472
27. Duncan CM, Gillette BP, Jacob AK, Sierra RJ, Sanchez-Sotelo J, Smith HM. Venous 473
thromboembolism and mortality associated with tranexamic acid use during total 474
hip and knee arthroplasty. J Arthroplasty. 2015;30(2):272-276. 475
Page 21 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
22
28. Yang ZG, Chen WP, Wu LD. Effectiveness and safety of tranexamic acid in 476
reducing blood loss in total knee arthroplasty: A meta-analysis. J Bone Joint Surg Am. 477
2012;94(13):1153-1159. 478
29. Foss NB, Kristensen MT, Kehlet H. Anaemia impedes functional mobility after hip 479
fracture surgery. Age Ageing. 2008;37(2):173-178. 480
30. Lawrence VA, Silverstein JH, Cornell JE, Pederson T, Noveck H, Carson JL. Higher 481
hb level is associated with better early functional recovery after hip fracture repair. 482
Transfusion. 2003;43(12):1717-1722. 483
31. Lee C, Freeman R, Edmondson M, Rogers BA. The efficacy of tranexamic acid in 484
hip hemiarthroplasty surgery: An observational cohort study. Injury. 2015. 485
32. Sadeghi M MA. Does a single bolus dose of tranexamic acid reduce blood loss and 486
transfusion requirements during hip fracture surgery? A prospective randomized 487
double blind study in 67 patients. Acta Medica Iranica. 2007;45(6):437-442. 488
33. Zufferey PJ, Miquet M, Quenet S, et al. Tranexamic acid in hip fracture surgery: A 489
randomized controlled trial. Br J Anaesth. 2010;104(1):23-30. 490
34. Vijay BS, Bedi V, Mitra S, Das B. Role of tranexamic acid in reducing 491
postoperative blood loss and transfusion requirement in patients undergoing hip 492
and femoral surgeries. Saudi J Anaesth. 2013;7(1):29-32. 493
Page 22 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
23
35. Danninger T, Memtsoudis SG. Tranexamic acid and orthopedic surgery-the 494
search for the holy grail of blood conservation. Ann Transl Med. 2015;3(6):77-495
5839.2015.01.25. 496
36. Simmons J, Sikorski RA, Pittet JF. Tranexamic acid: From trauma to routine 497
perioperative use. Curr Opin Anaesthesiol. 2015;28(2):191-200. 498
37. Whiting DR, Gillette BP, Duncan C, Smith H, Pagnano MW, Sierra RJ. Preliminary 499
results suggest tranexamic acid is safe and effective in arthroplasty patients with 500
severe comorbidities. Clin Orthop Relat Res. 2014;472(1):66-72. 501
38. Gillette BP, DeSimone LJ, Trousdale RT, Pagnano MW, Sierra RJ. Low risk of 502
thromboembolic complications with tranexamic acid after primary total hip and 503
knee arthroplasty. Clin Orthop Relat Res. 2013;471(1):150-154. 504
505
Page 23 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
254x243mm (72 x 72 DPI)
Page 24 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
Tranexamic Acid in Hip Fracture patients: a protocol
for a randomized, placebo controlled trial on the
efficacy of tranexamic acid in reducing blood loss in
hip fracture patients
Elizabeth Gausden, MD; Matthew R. Garner, MD; Stephen J. Warner, MD, PhD; Andrew Nellenstein,
BS; Tiffany Tedore, MD; Eva Flores, MD; Dean G. Lorich, MD
Page 25 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
Tranexamic Acid in Hip Fracture Patients: a protocol for a randomized, placebo controlled trial on the efficacy of
tranexamic acid in reducing blood loss in hip fracture patients
Journal: BMJ Open
Manuscript ID bmjopen-2015-010676.R1
Article Type: Protocol
Date Submitted by the Author: 08-Feb-2016
Complete List of Authors: Gausden, Elizabeth; Hospital for Special Surgery, Orthopaedic Surgery Garner, Matthew; Hospital for Special Surgery, Orthopaedic Surgery Warner, Stephen; Hospital for Special Surgery, Orthopaedic Surgery Levack, Ashley; Hospital for Special Surgery, Orthopaedic Surgery Nellestein, Andrew; Weill Cornell Medical College, Anesthesia Tedore, Tiffany; Weill Cornell Medical College, Anesthesia Flores, Eva; Weill Cornell Medical College, Internal Medicine Lorich, Dean; Hospital for Special Surgery, Orthopaedic Surgery
<b>Primary Subject Heading</b>:
Surgery
Secondary Subject Heading: Evidence based practice, Haematology (incl blood transfusion)
Keywords: tranexamic acid, hip fracture, blood transfusion
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on 26 July 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010676 on 21 June 2016. D
ownloaded from

For peer review only
1
Title: Tranexamic Acid in Hip Fracture patients: a protocol for a randomized, placebo 1 controlled trial on the efficacy of tranexamic acid in reducing blood loss in hip fracture 2
patients 3 4 5
Please send all correspondences and requests for reprints to: 6 7 8 9 10
Elizabeth B. Gausden, MD 11 [email protected] 12
Hospital for Special Surgery 13 535 East 70
th Street 14
New York, NY 10021 15 Tel: 212 606 1057 16 Fax: 212 734 3833 17
18 Matthew R. Garner, MD 19
Hospital for Special Surgery 20 New York, NY USA 21
22 Stephen J. Warner, MD 23
Hospital for Special Surgery 24 New York, NY USA 25
26 Ashley Levack, MD 27
Hospital for Special Surgery 28 New York, NY USA 29
30 Andrew Nellestein, BS, MS 31
New York Presbyterian Hospital 32 New York, NY USA 33
34 Tiffany Tedore, MD 35
New York Presbyterian Hospital 36 New York, NY USA 37
38 Eva Flores, MD 39
New York Presbyterian Hospital 40 New York, NY USA 41
42 Dean G. Lorich, MD 43
New York Presbyterian Hospital 44 New York, NY USA 45
46
Page 1 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
2
Abstract 47
Introduction 48
There is a high incidence of blood transfusion following hip fractures in elderly 49
patients. Tranexamic acid (TXA) has proven efficacy in decreasing blood loss in 50
general trauma patients as well as patients undergoing elective orthopaedic surgery. 51
In order to prove the efficacy of TXA, a randomized controlled trial will measure the 52
effect in a population of patients undergoing hip fracture surgery. 53
Methods 54
This is a double-blinded, randomized placebo-controlled trial. Patients admitted 55
through the emergency room diagnosed with an intertrochanteric or femoral neck 56
fracture will be eligible for enrollment and randomized to either treatment with 1 57
gram of intravenous TXA or intravenous saline at the time of skin incision. Patients 58
undergoing percutaneous intervention for non or minimally displaced femoral neck 59
fractures will not be eligible for enrollment. Postoperative transfusion rates will be 60
recorded and blood loss will be calculated from serial hematocrits. 61
Ethics and dissemination 62
This protocol was approved by the Institutional Review Board (IRB) and is 63
registered with clinicaltrials.gov. The findings of the trial will be disseminated 64
through peer-reviewed journals and conference presentations. 65
66
Key Words: tranexamic acid, hip fracture, blood transfusion 67
68
Page 2 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
3
69
Strengths and limitations of this study 70
• A prospective, randomized, placebo-controlled trial is the optimal study 71
design to address the question of efficacy of tranexamic acid (TXA) use in 72
patients with hip fractures 73
• The outcomes will be reported based on one-year follow-up, which is longer 74
follow-up than any other study examining tranexamic acid use in patients 75
with hip fractures. 76
• Findings will provide objective data from which clinicians can base future 77
guidelines regarding TXA administration 78
• Recruitment is slow as patients and health-care proxies are wary of enrolling 79
in a study in a trauma setting 80
81
Introduction 82
83
Hip fractures in the elderly remains a pressing public health issue in the United 84
States given the aging population.1 Hip fractures are associated with numerous 85
adverse events and increased mortality up to one year after the event.2-5 The 86
hidden blood loss in hip fractures, in addition to intraoperative blood loss, may be as 87
high as 1500 cc. 6,7 The rate of blood transfusion in the perioperative period for hip 88
fracture patients is reported between 20-60%.8-11 Total blood loss, and thus rate of 89
transfusion, is greater for extracapsular hip fractures compared to intracapsular hip 90
fractures. 6 A meta-analysis of 20 studies found a significantly increased risk of post-91
Page 3 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
4
operative bacterial infection in patients who receive an allogenic blood transfusion 92
in the perioperative period.12 In addition to the increased risk of infection, patients 93
who require blood transfusion following hip fracture have an increased hospital 94
length of stay.13 Beyond the risk to the patient from a blood transfusion, an allogenic 95
blood transfusion in the United States was recently estimated to increase costs by 96
$1,731 per admission.14 97
98
Numerous anti-fibrinolytics have been used to limit bleeding in orthopaedic surgery 99
and prevent the need for blood transfusion.15-19 One of these anti-fibrinolytics, 100
tranexamic acid (TXA) is a synthetic derivative of the amino acid lysine and acts as a 101
competitive inhibitor in the activation of plasminogen to plasmin and therefore 102
prevents the degradation of fibrin. As a result of the CRASH-2 trial20,21 that 103
demonstrated reduced mortality in trauma patients administered TXA the World 104
Health Organization (WHO) added it to the essential drugs list. Currently TXA is not 105
routinely used in patients with hip fractures in the United States, despite its 106
common use worldwide and proven efficacy in reducing blood loss. 107
108
Numerous studies have investigated the safety and efficacy of TXA in patients 109
undergoing elective orthopaedic surgery, including total joint replacement and 110
spine surgery.22-27 The consensus from this literature is overwhelmingly in favor of 111
administration of TXA given the decrease in blood loss, transfusion rates, and 112
cost.28,29 Although several individual studies have found increased risk of 113
Page 4 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
5
thromboembolic events in groups receiving TXA,9,30 larger studies and meta-114
analyses have uniformly found no increased risk of thrombosis.31,32 115
116
Patients who suffer hip fractures frequently have multiple comorbidities making 117
them more susceptible to adverse events from blood loss. 19,20 The most common 118
comorbidities of individuals with hip fractures are congestive heart failure, chronic 119
pulmonary disease and diabetes.1 Administering TXA to such patients has a 120
potential to offset blood loss, improve patient outcome and lower cost by decreasing 121
the rate of transfusions.33,34 Five studies, all conducted outside the United States, 122
have reported results of using TXA in hip fracture surgery.8-11,35 Sadeghi et al8 123
randomized 67 hip fracture patients to receive either placebo injection or 124
intravenous tranexamic acid at the time of surgery. They found a significantly lower 125
volume of blood loss (652 ± 228 mL vs. 1108 ± 372 mL, P < 0.003) and shorter 126
hospital stays (4.3 ± 1.6 days vs. 5.8 ± 1.5 days, p< 0.05). Vijay et al.35 also reported 127
significantly reduced transfusion rates in the TXA arm of their clinical trial. In a 128
retrospective cohort study, Lee et al11 reported similar results, a transfusion rate 129
three times lower in patients who received TXA prior to hemiarthroplasty surgery. 130
In a separate randomized controlled trial that compared intravenous administration 131
of TXA to topical TXA administration as well as placebo in hip fracture patients 132
undergoing hemiarthroplasty, both of the TXA groups experienced less blood loss.9 133
While this study found a significant reduction in blood loss and transfusion rates in 134
both TXA groups, they found a higher incidence of thromboembolic events in the 135
intravenous TXA group. 136
Page 5 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
6
Of the five studies investigating the use of TXA in hip fracture patients, four 137
were randomized controlled trials that were underpowered for detecting significant 138
differences in thromboembolic events (Table 1).8-11,35 Furthermore, patients were 139
only followed perioperatively, and differences in six-month and one-year mortality 140
rates and late-onset complications were not assessed. 141
Use of Tranexamic Acid (TXA) in Patients with Hip Fractures
Country Design Hip fx ( IT or FNF)
TXA Regimen
DVT PPX Sample size
Blood loss (cc)
Transfuse Rate %
Thrombo-embolic Events
Lee 201511
UK Cohort Hemi-arthroplasy only
1 g bolus preop
Tinzaparin 84 cases/ 187 controls
- 6* 1
- 19 4
Emara 20149
Egypt RCT Hemi-arthroplasty only
10 mg/kg bolus, then 5 mg/kg/h infusion
Clexane 20 cases IV/ 20 cases topical/20 controls
640 5* 5
1100 32 0
Zufferey 201010
France RCT Hip fractures
15 mg/kg bolus preop and 3 h later
Fondaparinux x 35 days (mandatory ultrasound)
57 cases/ 53 controls
975 42 0
1178 60 0
Sadeghi and Mehr-Aein 20068
Iran RCT Hip fractures
15 mg/kg bolus preop
n/a
32 cases/ 35 controls
960 37 0
1484 57 0
Vijay 201335
India RCT Hip fractures
10 mg/kg bolus at surgery
N/a 45 cases/ 45 controls
39* 16 0
91* 40 0
142
In designing this study, we concluded that hip fracture patients are both likely to 143
experience significant blood loss and are susceptible to the adverse effects of blood 144
loss making them an ideal population to target for a randomized controlled trial of 145
the effects of perioperative TXA on blood loss. We hypothesize that administration 146
Page 6 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
7
of TXA will decrease blood loss in hip fracture patients and lower the rate of 147
allogenic blood transfusion. 148
149
150
151
Objective 152
To investigate the hypothesis that TXA will lower blood loss and transfusion rate in 153
patients with hip fractures. 154
155
Methods and analysis 156
157
Overview of trial design 158
We are conducting a single-center randomized control trial using a parallel two-arm 159
design to investigate whether tranexamic acid use perioperatively will decrease the 160
rate of transfusion in patients with hip fractures (Figure 1). Randomization will be 161
stratified by type of hip fracture(ie. intertrochanteric versus femoral neck fracture). 162
The surgical team, anesthesia team, and patients will be blinded to the assignment. 163
Once consent is obtained and a patient is enrolled, a 1:1 randomization system will 164
be employed by our institution’s investigational pharmacy to assign patients to 165
receive TXA or placebo. Patient enrollment will occur over approximately 2 years 166
and enrolled patients will be followed for 1 year postoperatively. Incidence of blood 167
transfusion, total calculated blood loss, transfusion, and acute adverse events 168
(transfusion reaction, cerebrovascular accident, myocardial infarction, pulmonary 169
Page 7 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
8
embolism, and surgical site infection) will be assessed in the perioperative period. 170
Patients will also be assessed at 2 week, 6 week, 3 month, 6 month and 12 month 171
follow-up for long-term adverse events as well as mortality rate. This trial is 172
registered (NCT01940536) and has received ethics approval from the Weill Cornell 173
Medical College Institutional Review Board (IRB# 1301013463). 174
175
176
Primary research question 177
In patients with hip fractures, does a single bolus of tranexamic acid at the time of 178
surgery result in lower rate of blood transfusion? 179
180
Secondary research question 181
In patients with hip fractures, does a single bolus of tranexamic acid at the time of 182
surgery result in: 183
1.) decreased calculated blood loss? 184
2.) Shorter length of hospitalization? 185
3.) Any differences in occurrence of adverse events? 186
187
Hypothesis 188
As a primary outcome, there will be a decreased rate of blood transfusion in patients 189
who receive tranexamic acid intraoperatively and no significant increase in 190
frequency or severity of adverse events in comparison to patients who receive 191
Page 8 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
9
placebo. This study is powered to address the primary outcome of difference in 192
transfusion rates between the two study arms. 193
194
Setting and participants 195
Adult (over 18 years of age) patients presenting to a single tertiary care center with 196
an acute hip fracture. All patients with hip fractures at this institution are admitted 197
to the medical orthopaedic trauma service (MOTS). Prior to surgery, patients older 198
than 75 years of age, or those with medical comorbidities will be optimized by the 199
general medical service prior to surgery. All potentially eligible patients will be 200
screened and documented as (1) eligible and included, (2) eligible and missed, or 201
(3) excluded. The study coordinator will obtain informed consent for participation 202
in the study using the approved IRB Informed Consent forms. 203
204
All patients will provide written informed consent and will understand that by 205
entering in the study they may receive placebo or tranexamic acid. Participation in 206
the study is voluntary and their decision to participate will not affect any other 207
aspect of their care in case of refusal. Patients will have the right to withdraw from 208
the study at any point. 209
210
211
212
213
214
Page 9 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
10
Inclusion criteria 215
Patients admitted through the emergency room or transferred into our institution 216
and who meet the following criteria will be included in the study: 217
• Adults over the age of 18 218
• Acute intertrochanteric or femoral neck hip fracture 219
• Patients treated surgically with cephalomedullary nail, hemiarthroplasty, or 220
total hip arthroplasty (THA) 221
Exclusion criteria 222
Patient who meet any one or more of the following criteria will be excluded from the 223
study: 224
• Preoperative use of anticoagulant (clopidogrel, enoxaparin, warfarin, 225
argatroban, rivaroxaban, fondaparinux) 226
• Documented allergy to tranexamic acid 227
• History of deep vein thrombosis or pulmonary embolus 228
• Hepatic dysfunction (AST/ALT > 60) 229
• Renal dysfunction (Cr >1.5 of GRR > 30) 230
• Active coronary artery disease (event in the past 12 months), history of 231
cerebrovascular accident (CVA) in the past 12 months, or presence of a drug-232
eluting stent 233
• Color blindness 234
• Leukemia or any active cancer 235
• Coagulopathy (INR> 1.4, PTT > 1.4x normal, Platelets < 50,000) 236
• Non-displaced femoral neck fractures treated percutaneously 237
Page 10 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
11
238
Baseline 239
Baseline assessment includes sex, birth date, height and weight, mechanism of 240
injury, time from injury to presentation to the emergency room, American Society of 241
Anesthesiologists (ASA) classification, Charlson Comorbidity Index, comorbidities 242
including diabetes, cardiovascular disease, pulmonary disease, peripheral vascular 243
disease, dementia, hypertension, and history of smoking. The hemoglobin and 244
hematocrit will be recorded at the time of admission and on the morning of surgery. 245
246
Blinding 247
After the patient consents and is enrolled in the study, the patients will be stratified 248
based on type of hip fracture, intracapsular or extracapsular. The institution’s 249
investigational pharmacist will perform the randomization following the 250
stratification by fracture type and assign the patient to either receive TXA or 251
placebo. Patients will be randomized in blocks of 20. The packaging of the 252
injections will be performed by the investigational pharmacy and will be identical 253
for both TXA and placebo. All clinicians, except for the pharmacist, and the patients 254
will remain blinded until the data is analyzed. 255
256
Intervention 257
The patients randomized to the treatment arm will receive 1 gram of intravenous 258
tranexamic acid mixed in 100 cc of saline bolused at the time of surgical incision. 259
Page 11 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
12
Those assigned to the placebo group will receive an equivalent volume bolus of 260
saline at the time of surgical incision. 261
Patients with intertrochanteric hip fractures will be treated with a long, 262
intramedullary hip screw implant with a trochanteric start point. Patients with 263
displaced femoral neck fractures will be treated with a cemented or non-cemented 264
hemiarthroplasty or total hip arthroplasty at the discretion of the treating surgeon. 265
All surgeries will be supervised by the attending surgeon with the assistance of 266
orthopaedic residents. The surgical technique as well as the anesthetic technique, 267
regional versus general anesthesia, will be recorded and assessed in the final 268
analysis. The time from injury to surgery will also be recorded and included in the 269
analysis. 270
271
Blood transfusion criteria will remain consistent with hospital standards (Hb<8 272
g/dL or symptomatic anemia) as determined by an independent, blinded medical 273
team who will follow the patient throughout the hospital stay and number of blood 274
transfusions received will be documented upon patient discharge. Hematocrit and 275
hemoglobin will be recorded daily in all patients while they are in the hospital. 276
Further monitoring will be conducted based on need as determined by the 277
independent medical team. Estimated blood volume will be calculated from these 278
values and used to estimate blood loss (Appendix 1).36 279
280
All patients will be permitted to weight-bear as tolerated post-operatively and deep 281
vein thrombosis (DVT) prophylaxis will be standardized. All enrolled patients will 282
Page 12 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
13
receive subcutaneous heparin, 5000 units every 8 hours beginning upon admission 283
until 12 hours prior to surgery and restarting 6 hours after surgery. Calf mechanical 284
compression devices will also be utilized during the inpatient stay and will remain 285
on at all times with the exception of physical therapy sessions. Following discharge 286
from the hospital patients will be given aspirin 325 mg twice daily for DVT 287
prophylaxis for a total of 6 weeks. Diagnostic studies to assess for thromboembolic 288
events (i.e. DVT, pulmonary embolism, and stroke) will be ordered only if the 289
patient develops clinical signs or symptoms that justify their use. 290
Primary Outcome 291
The primary outcome of the study will be the rate of blood transfusion in the 292
postoperative period until time of discharge. Patients will be monitored with serial 293
hemoglobin and hematocrit measurements and their vital signs will be recorded as 294
per the standard of care to determine the need for blood transfusion. Only 295
intraoperative and postoperative blood transfusions will be considered for the primary 296
outcome measure as the drug will be administered at the time of surgical incision. 297
Therefore, we anticipate TXA in this study only modifying the rate of intraoperative or 298
postoperative transfusion, not pre-operative transfusion.. 299
300
Secondary Outcome 301
The secondary study outcomes include the calculated blood loss (calculated based 302
on validated methods as outlined in Appendix 1), frequency of adverse events 303
(including transfusion reaction, myocardial infarction, symptomatic deep vein 304
Page 13 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
14
thrombosis, pulmonary embolus, cerebrovascular accident, re-operation, re-305
admission, infection, and death) (Figure 1). 306
307
For the study purposes, a transfusion reaction will be defined as any constellation of 308
symptoms during a blood transfusion that necessitate discontinuation of the 309
transfusion. 310
Myocardial infarction will be defined as a cardiologist diagnosis of myocardial 311
infarction in combination with electrocardiogram changes, echocardiogram 312
changes, or creatine kinase MB or troponin changes. A pulmonary embolism must 313
be confirmed by pulmonary angiography, computed tomographic (CT) scan of the 314
chest, echocardiographic visualization or visualization of thrombus at autopsy. A 315
symptomatic deep vein thrombosis must be confirmed by venography, CT scan, 316
magnetic resonance imaging, or pathologic evidence at autopsy. A cerebrovascular 317
accident must be diagnosed by a neurologist and will be defined as an embolic, 318
thrombotic or hemorrhagic vascular accident or stroke with motor, sensory, or 319
cognitive dysfunction that persists for longer than 24 hours.37 320
A surgical site infection (SSI) will be defined as either superficial or deep infections. 321
Superficial SSI involves only skin or subcutaneous tissue while a deep SSI extends 322
deep to the fascial and muscle layers. Reoperation is defined as any return to the 323
operating room for a procedure related to the fractured hip. 324
325
326
Sample size consideration 327
Page 14 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
15
The transfusion rate amongst patients with hip fractures is between 6-60%.8-11,35 328
Our institutional transfusion rate was calculated based on a random sample of 60 329
patients and was 65% for extracapsular hip fractures and 35% for intracapsular hip 330
fractures, for an overall transfusion rate of 49%. The average reduction in 331
transfusion rate in the previous 5 studies using TXA was 20%.8-11,35 We plan to 332
include a total of 338 patients, 146 intracapsular hip fractures and 192 333
extracapsular hip fractures. This study design will achieve 81% power to detect a 334
reduction in blood transfusion from 65% in the placebo control group to 45% in the 335
tranexamic acid group with statistical significance set to alpha equal to 0.05 for the 336
extracapsular hip fracture group. Similarly the study will achieve 81% power to 337
detect a reduction in blood transfusion from 35% in the placebo control group to 338
15% in the tranexamic acid group with statistical significance set to alpha equal to 339
0.05 for the intracapsular hip fracture group. 340
341
342
Data analysis plan 343
Descriptive analyses of the patient population will include reporting means (with 344
standard deviations) for continuous variables and frequencies (with percentages) 345
for categorical or discrete variables. Following the descriptive analysis, a chi-square 346
analysis will be conducted to evaluate the superiority of tranexamic acid in reducing 347
the rate of transfusion versus the placebo control group. The analysis and reporting 348
of the results of the clinical outcomes will follow the CONSORT guidelines 349
(www.consort-statement.org). We will conduct a multiple logistic regression model 350
Page 15 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
16
to determine if type of fracture (intertrochanteric or femoral neck), comorbidities, 351
Charlson comorbidity index, age, time to surgery, and mechanism of injury are 352
related to transfusion administration. Similarly we will conduct a multiple linear 353
regression model to determine if patient comorbidities, age, time to surgery, and 354
mechanism of injury are related to blood loss. We will also conduct subgroup 355
analyses to determine if the effect of TXA is modified by fracture type 356
(intertrochanteric or femoral neck). 357
Our a priori hypothesis, based on retrospective data,6 is that patients with 358
intertrochanteric fractures incur more blood loss than femoral neck fractures and 359
will have a higher rate of transfusion. If these subgroup analyses are 360
underpowered, the subgroup data will be used to generate further hypotheses to be 361
tested in the future. All analyses will be performed using Stata 14.0 software (Stata 362
Corporation, College Station, TX, USA). 363
364
Data safety monitoring 365
The data safety monitoring board (DSMB) has been established to monitor the trial 366
and renew the study biannually. This board is independent of the trial and free of 367
conflicts with any of the investigation team. 368
369
Discussion 370
There is clinical uncertainty and a lack of high-quality evidence regarding the use of 371
TXA in hip fracture patients. Despite its proven efficacy in elective orthopaedic 372
surgery,25,38 the optimal dosing and timing of TXA administration is still debated.39 373
Page 16 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
17
Furthermore, the efficacy and side effect profile of TXA in patients with fractures 374
remains unclear. The immediate goal of this trial is to provide high-quality evidence 375
that can be used to develop clinical guidelines for use of TXA in patients with hip 376
fractures. 377
378
Patients undergoing elective total joint arthroplasty and elective spine surgery 379
represent a different population from patients who sustain hip fractures. A larger 380
percentage of hip fracture patients have significant medical comorbidities, and 381
many have history of cardiac disease.1 While TXA has demonstrated safety and 382
efficacy in patients without significant cardiac disease undergoing elective surgery, 383
there is still debate if TXA will have the same effect in patients with significant 384
comorbidities.25,39,40 The data investigating TXA in patients with comorbidities is 385
limited, which has further deterred clinicians from using TXA in patients with hip 386
fractures. However, the potential benefit of decreasing blood loss and decreasing 387
the number of transfusions following hip fracture surgery is overwhelming and will 388
likely result in improved patient outcomes, shorter length of stay and lower cost. 389
The study investigators believe that the potential benefit of TXA in such patients 390
outweighs the risk of TXA. The majority of literature regarding TXA has confirmed 391
its safety and squelched concerns that its use will result in higher rates of 392
thrombosis.20,30,32,40,41 393
394
The literature to date regarding TXA and hip fractures (Table 1) is limited. Four out 395
of five studies identified a significant decrease in rate of transfusion in patients who 396
Page 17 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
18
received TXA compared to those that did not.8-11,35 The largest study, with a total of 397
219 patients, was a cohort study with no randomization.11 While they found a 398
significant decrease in blood transfusion rate, the study design limits the 399
interpretation of the results secondary to the potential biases of surgeon and patient 400
preference. Several excluded all patients with preoperative anemia, which limits the 401
generalizability of their findings.8,9 None of the randomized trials provided a 402
detailed analysis of total number of patients excluded from the study at each stage. 403
While the early results from these studies are promising, the overall validity cannot 404
be confirmed without this information. Similarly, there has yet to be a large study to 405
perform a complete subanalysis to determine the efficacy of TXA amongst both 406
intracapsular and extracapsular hip fracture patients. Furthermore, the studies did 407
not follow patients up to 1 year postoperatively, which is our intention. The 408
extended follow-up period allows for assessment of mortality at 12 months as well 409
as incidence of unanticipated adverse events following discharge from the hospital. 410
The most novel characteristic of this study in comparison to the other studies is that 411
it is powered to detect a significant difference in blood transfusion rates in both 412
intracapsular and extracapsular hip fractures. As the hidden blood loss experienced 413
by hip fracture patients is distinct between these two patterns of hip fractures,6 it is 414
important to demonstrate efficacy in both groups independently. 415
416
Tranexamic acid has the potential to decrease transfusion rates by decreasing blood 417
loss in patients with hip fractures. Ultimately, this will decreased hospital length of 418
stay and improve outcomes in the hundreds of thousands of patients with hip 419
Page 18 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
19
fractures every year. If the results prove the efficacy of TXA in hip fracture patients, 420
this study may change the standard of care across the United States for these 421
patients. 422
423
Funding 424
This work is supported by a Dr. Thomas Sculco grant and a Dr. Joseph M. Lane grant. 425 426
Word Count 427
3,690 words 428
429
Data Sharing 430
This article presents the study design; data being collected during the research will 431
become available as the study begins. 432
433
Competing Interest 434
None of the authors has any potential financial conflict of interest related to this 435
manuscript 436
437
Contributorship 438
Elizabeth B. Gausden: This author revised the study from its original form 439
and condensed the application of the tranexamic acid to one dose in the 440
operating room in order to facilitate the flow of the project. This author 441
made substantial contributions to the planning of data analysis, drafting 442
and revising of the protocol, final approval of the version to be published 443
Page 19 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
20
and agrees to be accountable for all aspects of the work in ensuring that 444
questions related to the accuracy of the work. 445
446
Matthew R. Garner: This author conceived of the study and designed the 447
first draft of the protocol. He was awarded the Thomas P. Sculco 448
Research Grant and the Joseph M. Lane Research Grant for his proposal of 449
the project. He made substantial contributions to the drafting and 450
revising of the protocol, final approval of the version to be published and 451
agrees to be accountable for all aspects of the work in ensuring that 452
questions related to the accuracy of the work. 453
454
455
Stephen Warner: This author made substantial contributions to the 456
design of the work, planning of data analysis, drafting and revising of the 457
protocol, final approval of the version to be published and agrees to be 458
accountable for all aspects of the work in ensuring that questions related 459
to the accuracy of the work. 460
461
Ashley Levack: This author made substantial contributions to the study 462
design, modifications of the study to conform to guidelines and for 463
logistics. She will also be involved in patient recruitment, data collection 464
and analysis. This author made substantial contributions to the design of 465
the work, planning of data analysis, drafting and revising of the protocol, 466
Page 20 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
21
final approval of the version to be published and agrees to be accountable 467
for all aspects of the work in ensuring that questions related to the 468
accuracy of the work. 469
470
Andrew Nellestein: This is a research assistant who facilitated IRB 471
submissions and amendments. He is also coordinating the enrollment of 472
patients in the study and working with the orthopaedic trauma team 473
during the process of drug administration. This author made substantial 474
contributions to the design of the work, planning of data analysis, drafting 475
and revising of the protocol, final approval of the version to be published 476
and agrees to be accountable for all aspects of the work in ensuring that 477
questions related to the accuracy of the work. 478
479
Tiffany Tedore: Dr. Tedore is the main anesthesiologist who will be 480
orchestrating the anesthesiologists who administer the drug prior to skin 481
incision. This author made substantial contributions to the design of the 482
work, planning of data analysis, drafting and revising of the protocol, final 483
approval of the version to be published and agrees to be accountable for 484
all aspects of the work in ensuring that questions related to the accuracy 485
of the work. 486
487
Eva Flores: Dr, Flores is the head of the Medical Orthopaedic Trauma 488
Service (MOTS) who organizes the medical attendings who manage the 489
Page 21 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
22
patients following surgery. This author made substantial contributions to 490
the design of the work, planning of data analysis, drafting and revising of 491
the protocol, final approval of the version to be published and agrees to 492
be accountable for all aspects of the work in ensuring that questions 493
related to the accuracy of the work. 494
495
Dean G. Lorich: Dr. Lorich is the chief of the orthopaedic trauma service 496
at NYP. This author made substantial contributions to the design of the 497
work, planning of data analysis, drafting and revising of the protocol, final 498
approval of the version to be published and agrees to be accountable for 499
all aspects of the work in ensuring that questions related to the accuracy 500
of the work. 501
502
503
504
505 506 507
Page 22 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
23
References 508 509 510
1. Brauer CA, Coca-Perraillon M, Cutler DM, Rosen AB. Incidence and mortality of hip 511
fractures in the united states. JAMA. 2009;302(14):1573-1579. 512
2. Richmond J, Aharonoff GB, Zuckerman JD, Koval KJ. Mortality risk after hip 513
fracture. J Orthop Trauma. 2003;17(1):53-56. 514
3. Heyes GJ, Tucker A, Marley D, Foster A. Predictors for 1-year mortality following 515
hip fracture: A retrospective review of 465 consecutive patients. Eur J Trauma 516
Emerg Surg. 2015. 517
4. Shah MR, Aharonoff GB, Wolinsky P, Zuckerman JD, Koval KJ. Outcome after hip 518
fracture in individuals ninety years of age and older. J Orthop Trauma. 519
2001;15(1):34-39. 520
5. Sathiyakumar V, Greenberg SE, Molina CS, Thakore RV, Obremskey WT, Sethi MK. 521
Hip fractures are risky business: An analysis of the NSQIP data. Injury. 522
2015;46(4):703-708. 523
6. Foss NB, Kehlet H. Hidden blood loss after surgery for hip fracture. J Bone Joint 524
Surg Br. 2006;88(8):1053-1059. 525
7. Smith GH, Tsang J, Molyneux SG, White TO. The hidden blood loss after hip 526
fracture. Injury. 2011;42(2):133-135. 527
Page 23 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
24
8. Sadeghi M MA. Does a single bolus dose of tranexamic acid reduce blood loss and 528
transfusion requirements during hip fracture surgery? A prospective randomized 529
double blind study in 67 patients. Acta Medica Iranica. 2007;45(6):437-442. 530
9. Emara WM, Moez KK, Elkhouly AH. Topical versus intravenous tranexamic acid as 531
a blood conservation intervention for reduction of post-operative bleeding in 532
hemiarthroplasty. Anesth Essays Res. 2014;8(1):48-53. 533
10. Zufferey PJ, Miquet M, Quenet S, et al. Tranexamic acid in hip fracture surgery: A 534
randomized controlled trial. Br J Anaesth. 2010;104(1):23-30. 535
11. Lee C, Freeman R, Edmondson M, Rogers BA. The efficacy of tranexamic acid in 536
hip hemiarthroplasty surgery: An observational cohort study. Injury. 537
2015;46(10):1978-1982. 538
12. Hill GE, Frawley WH, Griffith KE, Forestner JE, Minei JP. Allogeneic blood 539
transfusion increases the risk of postoperative bacterial infection: A meta-analysis. J 540
Trauma. 2003;54(5):908-914. 541
13. Shokoohi A, Stanworth S, Mistry D, Lamb S, Staves J, Murphy MF. The risks of red 542
cell transfusion for hip fracture surgery in the elderly. Vox Sang. 2012;103(3):223-543
230. 544
14. Saleh A, Small T, Chandran Pillai AL, Schiltz NK, Klika AK, Barsoum WK. Allogenic 545
blood transfusion following total hip arthroplasty: Results from the nationwide 546
inpatient sample, 2000 to 2009. J Bone Joint Surg Am. 2014;96(18):e155. 547
Page 24 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from
For peer review only
25
15. Kagoma YK, Crowther MA, Douketis J, Bhandari M, Eikelboom J, Lim W. Use of 548
antifibrinolytic therapy to reduce transfusion in patients undergoing orthopedic 549
surgery: A systematic review of randomized trials. Thromb Res. 2009;123(5):687-550
696. 551
16. Eubanks JD. Antifibrinolytics in major orthopaedic surgery. J Am Acad Orthop 552
Surg. 2010;18(3):132-138. 553
17. Yuan C, Zhang H, He S. Efficacy and safety of using antifibrinolytic agents in spine 554
surgery: A meta-analysis. PLoS One. 2013;8(11):e82063. 555
18. Zufferey P, Merquiol F, Laporte S, et al. Do antifibrinolytics reduce allogeneic 556
blood transfusion in orthopedic surgery? Anesthesiology. 2006;105(5):1034-1046. 557
19. Tse EY, Cheung WY, Ng KF, Luk KD. Reducing perioperative blood loss and 558
allogeneic blood transfusion in patients undergoing major spine surgery. J Bone Joint 559
Surg Am. 2011;93(13):1268-1277. 560
20. CRASH-2 trial collaborators, Shakur H, Roberts I, et al. Effects of tranexamic acid 561
on death, vascular occlusive events, and blood transfusion in trauma patients with 562
significant haemorrhage (CRASH-2): A randomised, placebo-controlled trial. Lancet. 563
2010;376(9734):23-32. 564
21. CRASH-2 collaborators, Roberts I, Shakur H, et al. The importance of early 565
treatment with tranexamic acid in bleeding trauma patients: An exploratory 566
Page 25 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
26
analysis of the CRASH-2 randomised controlled trial. Lancet. 2011;377(9771):1096-567
101, 1101.e1-2. 568
22. Whiting DR, Gillette BP, Duncan C, Smith H, Pagnano MW, Sierra RJ. Preliminary 569
results suggest tranexamic acid is safe and effective in arthroplasty patients with 570
severe comorbidities. Clin Orthop Relat Res. 2014;472(1):66-72. 571
23. Cid J, Lozano M. Tranexamic acid reduces allogeneic red cell transfusions in 572
patients undergoing total knee arthroplasty: Results of a meta-analysis of 573
randomized controlled trials. Transfusion. 2005;45(8):1302-1307. 574
24. Lemay E, Guay J, Cote C, Roy A. Tranexamic acid reduces the need for allogenic 575
red blood cell transfusions in patients undergoing total hip replacement. Can J 576
Anaesth. 2004;51(1):31-37. 577
25. Poeran J, Rasul R, Suzuki S, et al. Tranexamic acid use and postoperative 578
outcomes in patients undergoing total hip or knee arthroplasty in the united states: 579
Retrospective analysis of effectiveness and safety. BMJ. 2014;349:g4829. 580
26. Raksakietisak M, Sathitkarnmanee B, Srisaen P, et al. Two doses of tranexamic 581
acid reduce blood transfusion in complex spine surgery: A prospective randomized 582
study. Spine (Phila Pa 1976). 2015. 583
27. Wind TC, Barfield WR, Moskal JT. The effect of tranexamic acid on transfusion 584
rate in primary total hip arthroplasty. J Arthroplasty. 2014;29(2):387-389. 585
Page 26 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
27
28. Tuttle JR, Ritterman SA, Cassidy DB, Anazonwu WA, Froehlich JA, Rubin LE. Cost 586
benefit analysis of topical tranexamic acid in primary total hip and knee 587
arthroplasty. J Arthroplasty. 2014;29(8):1512-1515. 588
29. Huang F, Wu D, Ma G, Yin Z, Wang Q. The use of tranexamic acid to reduce blood 589
loss and transfusion in major orthopedic surgery: A meta-analysis. J Surg Res. 590
2014;186(1):318-327. 591
30. Nishihara S, Hamada M. Does tranexamic acid alter the risk of thromboembolism 592
after total hip arthroplasty in the absence of routine chemical thromboprophylaxis? 593
Bone Joint J. 2015;97-B(4):458-462. 594
31. Duncan CM, Gillette BP, Jacob AK, Sierra RJ, Sanchez-Sotelo J, Smith HM. Venous 595
thromboembolism and mortality associated with tranexamic acid use during total 596
hip and knee arthroplasty. J Arthroplasty. 2015;30(2):272-276. 597
32. Yang ZG, Chen WP, Wu LD. Effectiveness and safety of tranexamic acid in 598
reducing blood loss in total knee arthroplasty: A meta-analysis. J Bone Joint Surg Am. 599
2012;94(13):1153-1159. 600
33. Foss NB, Kristensen MT, Kehlet H. Anaemia impedes functional mobility after hip 601
fracture surgery. Age Ageing. 2008;37(2):173-178. 602
34. Lawrence VA, Silverstein JH, Cornell JE, Pederson T, Noveck H, Carson JL. Higher 603
hb level is associated with better early functional recovery after hip fracture repair. 604
Transfusion. 2003;43(12):1717-1722. 605
Page 27 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
28
35. Vijay BS, Bedi V, Mitra S, Das B. Role of tranexamic acid in reducing 606
postoperative blood loss and transfusion requirement in patients undergoing hip 607
and femoral surgeries. Saudi J Anaesth. 2013;7(1):29-32. 608
36. George DA, Sarraf KM, Nwaboku H. Single perioperative dose of tranexamic acid 609
in primary hip and knee arthroplasty. Eur J Orthop Surg Traumatol. 2015;25(1):129-610
133. 611
37. Basques BA, Toy JO, Bohl DD, Golinvaux NS, Grauer JN. General compared with 612
spinal anesthesia for total hip arthroplasty. J Bone Joint Surg Am. 2015;97(6):455-613
461. 614
38. Danninger T, Memtsoudis SG. Tranexamic acid and orthopedic surgery-the 615
search for the holy grail of blood conservation. Ann Transl Med. 2015;3(6):77-616
5839.2015.01.25. 617
39. Simmons J, Sikorski RA, Pittet JF. Tranexamic acid: From trauma to routine 618
perioperative use. Curr Opin Anaesthesiol. 2015;28(2):191-200. 619
40. Whiting DR, Gillette BP, Duncan C, Smith H, Pagnano MW, Sierra RJ. Preliminary 620
results suggest tranexamic acid is safe and effective in arthroplasty patients with 621
severe comorbidities. Clin Orthop Relat Res. 2014;472(1):66-72. 622
41. Gillette BP, DeSimone LJ, Trousdale RT, Pagnano MW, Sierra RJ. Low risk of 623
thromboembolic complications with tranexamic acid after primary total hip and 624
knee arthroplasty. Clin Orthop Relat Res. 2013;471(1):150-154. 625
Page 28 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
29
626
627
Page 29 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
30
Figure Legend 628
629
Figure 1: Study Design (TXA: tranexamic acid; PRBC: packed red blood cells) 630
631
Table 1: Previously reported outcomes of TXA in hip fracture patients. *drain 632 output. Thromboembolic events include only symptomatic thromboembolic events. 633 634
Page 30 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
Figure 1: Study Design (TXA: tranexamic acid; PRBC: packed red blood cells)
254x243mm (72 x 72 DPI)
Page 31 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
Appendix
Blood Loss Calculation:Patient’s Blood Volume (PBV) = (k1 x Height3
(m)) + (k2 x Weight (kg)) + k3
k1 = 0.3669, k2 = 0.03219, and k3 = 0.6041 for men k1 = 0.3561, k2=0.03308, and k3 = 0.1833 for
women
Multiplying the PBV by the hematocrit (Hct) gives the red blood cell (RBC) volume. As
such, a change in the RBC volume can be calculated from a change in the Hct level as
follows:
Pre-op RBC volume loss = PBV x (Admit Hct – Day of surgery Hct)
Operative RBC volume loss = PBV x (Day of surgery Hct – PACU Hct)
Post-operative RBC volume loss= PBX x (PACU Hct – Hct POD#x)If a patient requires a pre-op or
intraoperative transfusion, the calculation will be adjusted as follows:
Pre-op RBC volume loss = [PBV x (Admit Hct – Day of surgery Hct)]+ (No. of Units Transfused x
0.285) / (Admit Hct – Day of surgery Hct) / 2)
Operative RBC volume loss = [PBV x (Day of surgery Hct – PACU Hct)] +)]+ (No. of Units Transfused x
0.285) / (Day of surgery Hct – Post-op Hct) / 2
Page 32 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
1
Spirit Checklist 1.) Title
Tranexamic Acid in Hip Fracture patients: a protocol for a randomized, placebo controlled trial on the efficacy of tranexamic acid in reducing blood loss in hip fracture patients
2.) Trial Registration
a.) Registry set
“The Effect of Tranexamic Acid on Transfusion Rates in Intertrochanteric Hip Fractures” Registered August 2014 clinicaltrials.gov: NCT01940536 13083
b.) Data set
Data Category Information
Primary registry and trial identifying number
Clinicaltrials.gov NCT01940536
Date of registration in primary registry
August 2014
Secondary identifying numbers
13083
Source of monetary support
Thomas Sculco Grant Joseph Lane Grant
Primary sponsor Thomas P. Sculco Research Grant
Secondary sponsor Joseph M. Lane Research Grant
Contact for public queries
Elizabeth Gausden, MD; [email protected]
Contact for scientific queries
Elizabeth Gausden, MD; [email protected]
Public Title Tranexamic Acid in Hip Fracture patients
Scientific title Tranexamic Acid in Hip Fracture patients: a protocol for a
randomized, placebo controlled trial on the efficacy of
tranexamic acid in reducing blood loss in hip fracture
patients
Countries of recruitment
United States
Page 33 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
2
Health condition(s) studied
Blood loss after hip fracture and hip fracture surgery
Intervention Use of intravenous tranexamic acid at the time of hip fracture surgery versus placebo (intravenous 0.9% saline)
Key inclusion and exclusion criteria
Inclusion
• Adults over the age of 18
• Intertrochanteric or femoral neck hip fracture
• Patients treated surgically with cephalomedullary nail or hemiarthroplasty
Exclusion
• Preoperative use of anticoagulant (Plavix, Warfarin, Lovenox)
• Documented allergy to tranexamic acid
• History of deep vein thrombosis or pulmonary embolus
• Hepatic dysfunction (AST/ALT > 60)
• Renal dysfunction (Cr >1.5 of GRR > 30)
• Active coronary artery disease (event in the past 12 months), history of cerebrovascular accident (CVA) in the past 12 months, or presence of a drug-eluting stent
• Color blindness
• Leukemia or any active cancer
• Coagulopathy (INR> 1.4, PTT > 1.4x normal, Platelets < 100,000)
• Non-displaced femoral neck fractures treated percutaneously
Study type Interventional Allocation: randomized Intervention model: parallel assignment Masking: Double blinded Primary purpose: preventing blood loss in hip fractures Phase III
Date of first enrollment
Pending
Target sample size 338
Primary outcome (s)
Transfusion of packed red blood cells (PRBC) following hip fracture surgery
Secondary outcome(s)
Calculated blood loss following surgery Adverse events (including transfusion reaction, myocardial infarction, deep vein thrombosis, pulmonary embolus, cerebrovascular accident, re-operation, re-admission, infection, and death)
Page 34 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
3
3.) Protocol version
The protocol has been modified from the original version listed on clinicaltrials.gov. The 2 changes reflect the inclusion of intracapsular hip fractures to be treated with arthroplasty as well as a revised power analysis and target study size.
4.) Funding
The funding for this study is coming from two grants, one from Dr. Joseph Lane and one from Dr. Thomas Sculco.
5.) Roles and Responsibilities
a.) Contributorship
Elizabeth B. Gausden: This author revised the study from its original form and condensed the application of the tranexamic acid to one dose in the operating room in order to facilitate the flow of the project. This author made substantial contributions to the planning of data analysis, drafting and revising of the protocol, final approval of the version to be published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy of the work. Matthew R. Garner: This author conceived of the study and designed the first draft of the protocol. He was awarded the Thomas P. Sculco Research Grant and the Joseph M. Lane Research Grant for his proposal of the project. He made substantial contributions to the drafting and revising of the protocol, final approval of the version to be published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy of the work. Ashley Levack: This author made substantial contributions to the study design, modifications of the study to conform to guidelines and for logistics. She will also be involved in patient recruitment, data collection and analysis. This author made substantial contributions to the design of the work, planning of data analysis, drafting and revising of the protocol, final approval of the version to be published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy of the work. Stephen Warner: This author made substantial contributions to the design of the work, planning of data analysis, drafting and revising of the protocol, final approval of the version to be published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy of the work.
Page 35 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
4
Andrew Nellestein: This is a research assistant who facilitated IRB submissions and amendments. He is also coordinating the enrollment of patients in the study and working with the orthopaedic trauma team during the process of drug administration. This author made substantial contributions to the design of the work, planning of data analysis, drafting and revising of the protocol, final approval of the version to be published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy of the work. Tiffany Tedore: Dr. Tedore is the main anesthesiologist who will be orchestrating the anesthesiologists who administer the drug prior to skin incision. This author made substantial contributions to the design of the work, planning of data analysis, drafting and revising of the protocol, final approval of the version to be published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy of the work. Eva Flores: Dr, Flores is the head of the Medical Orthopaedic Trauma Service (MOTS) who organizes the medical attendings who manage the patients following surgery. This author made substantial contributions to the design of the work, planning of data analysis, drafting and revising of the protocol, final approval of the version to be published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy of the work. Dean G. Lorich: Dr. Lorich is the chief of the orthopaedic trauma service at NYP. This author made substantial contributions to the design of the work, planning of data analysis, drafting and revising of the protocol, final approval of the version to be published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy of the work.
b.) Sponsor contact information
“Trial sponsor: Dr. Thomas P. Sculco Research Grant
Sponsor’s reference:
Contact name: Karla Felix
Address: 535 E. 70th St.
Telephone: 212 774 2717
Email: [email protected]
“Trial sponsor: Dr. Joseph M. Lane Research Grant
Sponsor’s reference:
Contact name: Karla Felix
Address: 535 E. 70th St.
Telephone: 212 774 2717
Page 36 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
5
Email: [email protected]
c.) Sponsor and funder:
This funder has no role in the design of the study and will not have any role during its execution, analyses, interpretation of the data, or decision to submit results. d.) Committees
As this is a single institution study, there is no steering committee other than the authors listed above. 6.) Background and rationale
a.) Background and rationale:
Hip fractures in the elderly remains a pressing public health issue in the United States given the aging population. 1 Hip fractures are associated with numerous adverse events and increased mortality up to one year after the event. 2-5 Elderly patients sustaining hip fractures commonly lose more than one liter of blood and up to 60% will require a blood transfusion. 6 A meta-analysis of 20 studies found a significantly increased risk of post-operative bacterial infection in patients who receive an allogenic blood transfusion in the perioperative period. 7 In addition to the increased risk of infection, patients who require blood transfusion following hip fracture have an increased hospital length of stay. 8 Beyond the risk to the patient from a blood transfusion, an allogenic blood transfusion in the United States was recently estimated to increase costs by $1,731 per admission. 9 Numerous anti-fibrinolytics have been used to limit bleeding in orthopaedic surgery and prevent the need for blood transfusion. 10-14 One of these anti-fibrinolytics, tranexamic acid (TXA) is a synthetic derivative of the amino acid lysine and acts as a competitive inhibitor in the activation of plasminogen to plasmin and therefore prevents the degradation of fibrin. As a result of the CRASH-2 trial15,16 that demonstrated reduced mortality in trauma patients administered TXA the World Health Organization (WHO) added it to the essential drugs list. Currently TXA is not routinely used in patients with hip fractures in the United States, despite its common use worldwide and proven efficacy in reducing blood loss. Numerous studies have investigated the safety and efficacy of TXA in patients undergoing elective orthopaedic surgery, including total joint replacement and spine surgery. 17-22 The consensus from this literature is overwhelmingly in favor of administration of TXA given the decrease in blood loss, transfusion rates, and cost. 23,24 Although few individual studies have found increased risk of thromboembolic events in groups
Page 37 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
6
receiving TXA, 25,26 larger studies and meta-analyses have uniformly found no increased risk of thrombosis.27,28 Patients who suffer hip fractures frequently have multiple comorbidities making them more susceptible to adverse events from blood loss. 19,20 The most common comorbidities of individuals with hip fractures are congestive heart failure, chronic pulmonary disease and diabetes. 1 Administering TXA to such patients has a potential to offset blood loss, improve patient outcome and lower cost by decreasing the rate of transfusions. 29,30 Five studies, all conducted outside the United States, have reported results of using TXA in hip fracture surgery. 26,31-33 Sadeghi et al34 randomized 67 hip fracture patients to receive either placebo injection or intravenous tranexamic acid at the time of surgery. They found a significantly lower volume of blood loss (652 ± 228 mL vs. 1108 ± 372 mL, P < 0.003) and shorter hospital stays (4.3 ± 1.6 days vs. 5.8 ± 1.5 days, p< 0.05). Vijay et al. 33 also reported significantly reduced transfusion rates in the TXA arm of their clinical trial. In a retrospective cohort study, Lee et al31 reported similar results, a transfusion rate three times lower in patients who received TXA prior to hemiarthroplasty surgery. In a separate randomized controlled trial that compared intravenous administration of TXA to topical TXA administration as well as placebo in hip fracture patients undergoing hemiarthroplasty, both of the TXA groups experienced less blood loss. 26 While this study found a significant reduction in blood loss and transfusion rates in both TXA groups, they found a higher incidence of thromboembolic events in the intravenous TXA group. Of the five studies investigating the use of TXA in hip fracture patients, four were randomized controlled trials that were underpowered for detecting significant differences in thromboembolic events (Table 1). Furthermore, patients were only followed perioperatively, and differences in six-month and one-year mortality rates and late-onset complications were not assessed.
In designing this study, we concluded that hip fracture patients are both likely to experience significant blood loss and are susceptible to the adverse effects of blood loss making them an ideal population to target for a randomized controlled trial of the effects of perioperative TXA on blood loss.
b.) Choice of comparators
The choice of intravenous saline as a control in this study is to replicate the standard of care at this time in the United States, which is no drug intervention for preventing blood loss in hip fracture surgery.
Page 38 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
7
7.) Objective
Hypothesis: We hypothesize that administration of TXA will decrease blood loss in hip fracture patients and lower the rate of allogenic blood transfusion.
Objective
To investigate the hypothesis that TXA will lower blood loss and transfusion rate in patients with hip fractures.
8.) Trial Design
This trial is designed as a stratified randomized, placebo-controlled, surgeon and patient blinded single-institution trial with four parallel groups and a primary endpoint of blood transfusion in the immediate postoperative hospitalization following hip fracture surgery. Randomization will be performed as block randomization with 1:1 allocation for both the intracapsular and the extracapsular hip fracture groups. 9.) Study Setting
Adult (over 18 years of age) patients presenting to a single urban tertiary care
center in with a hip fracture. All patients with hip fractures at this institution are admitted to the medical orthopaedic trauma service (MOTS) after presenting through the emergency room. 10.) Eligibility criteria
Inclusion criteria
Patients admitted through the emergency room or transferred into our institution and who meet the following criteria will be included in the study:
• Adults over the age of 18
• Intertrochanteric or femoral neck hip fracture
• Patients treated surgically with cephalomedullary nail or hemiarthroplasty
Exclusion criteria
Patient who meet any one or more of the following criteria will be excluded from the study:
• Preoperative use of anticoagulant (clopidogrel, enoxaparin, warfarin, argatroban, rivaroxaban, fondaparinux)
• Documented allergy to tranexamic acid
• History of deep vein thrombosis or pulmonary embolus
• Hepatic dysfunction (AST/ALT > 60)
Page 39 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
8
• Renal dysfunction (Cr >1.5 of GRR > 30)
• Active coronary artery disease (event in the past 12 months), history of cerebrovascular accident (CVA) in the past 12 months, or presence of a drug-eluting stent
• Color blindness
• Leukemia or any active cancer
• Coagulopathy (INR> 1.4, PTT > 1.4x normal, Platelets < 100,000)
• Non-displaced femoral neck fractures treated percutaneously 11.) Interventions
a.) Interventions
The patients randomized to the treatment arm will receive 1 gram of intravenous tranexamic acid infused at the time of surgical incision. Those assigned to the placebo group will receive an infusion of saline at the time of surgical incision. Patients with intertrochanteric hip fractures will be treated with a long, intramedullary hip screw implant with a trochanteric start point. Patients with displaced femoral neck fractures will be treated with a cemented or non-cemented hemiarthroplasty or total hip arthroplasty at the discretion of the treating surgeon. Blood transfusion criteria will remain consistent with hospital standards (Hb<8 g/dL or symptomatic anemia) as determined by an independent, blinded medical team who will follow the patient throughout the hospital stay and number of blood transfusions received will be documented upon patient discharge. Hematocrit and hemoglobin will be recorded in all patients while they are in the hospital, for a minimum of 2 days postoperatively. Further monitoring will be conducted based on need as determined by the independent medical team. Estimated blood volume will be calculated from these values and used to estimate blood loss (Appendix 1 All patients will be permitted to weight-bear as tolerated post-operatively and deep vein thrombosis (DVT) prophylaxis will be standardized. All enrolled patients will receive subcutaneous heparin, 5000 units every 8 hours beginning upon admission until 12 hours prior to surgery and restarting 6 hours after surgery. Calf mechanical compression devices will also be utilized during the inpatient stay and will remain on at all times with the exception of physical therapy sessions. Following discharge from the hospital patients will be given aspirin 325 mg twice daily for DVT prophylaxis for a total of 6 weeks. Diagnostic studies to assess for thromboembolic events (i.e. DVT, pulmonary embolism, and stroke) will be ordered only if the patient develops clinical signs or symptoms that justify their use.
Page 40 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
9
b.) Modifications
As the administration of TXA or placebo will occur at one time point in the operating room at the time of skin incision, there will be no criteria for modifying or discontinuing the treatment allocation following surgery. If a patient becomes unstable, experiences a sudden change in vital signs, drop in blood pressure or increase in heart rate, during the admission of the drug, the drug will be discontinued at that time. The patient will still be analyzed on an intention-to-treat basis. c.) Adherence
We do not anticipate adherence as an issue since the administration of the intervention will be performed by the anesthesiologist at the time of skin incision. d.) Concomitant care
No concomitant interventions will be permitted during the trial.
12.) Outcomes
Primary Outcome
The primary outcome of the study will be the rate of blood transfusion in the postoperative period until time of discharge. Patients will be monitored with serial hemoglobin and hematocrit measurements and their vital signs will be recorded as per the standard of care to determine the need for blood transfusion. Secondary Outcome
The secondary study outcomes include the calculated blood loss (calculated based on validated methods as outlined in Appendix 1), frequency of adverse events (including transfusion reaction, myocardial infarction, deep vein thrombosis, pulmonary embolus, cerebrovascular accident, re-operation, re-admission, infection, and death).
13.) Participation timeline
Page 41 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
10
Figure 1: Study Design (TXA: tranexamic acid; PRBC: packed red blood cells) 14.) Sample size consideration
The transfusion rate amongst patients with hip fractures is between 6-60%.8-11,35
Our institutional transfusion rate was calculated based on a random sample of 60
patients and was 65% for extracapsular hip fractures and 35% for intracapsular hip
fractures, and an overall transfusion rate of 49%. The average reduction in
transfusion rate in the previous 5 studies using TXA was 20%.8-11,35 We plan to
include a total of 338 patients, 146 intracapsular hip fractures and 192
Page 42 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
11
extracapsular hip fractures. This study design will achieve 81% power to detect a
reduction in blood transfusion from 65% in the placebo control group to 45% in the
tranexamic acid group with statistical significance set to alpha equal to 0.05 for the
extracapsular hip fracture group. Similarly the study will achieve 81% power to
detect a reduction in blood transfusion from 35% in the placebo control group to
15% in the tranexamic acid group with statistical significance set to alpha equal to
0.05 for the intracapsular hip fracture group.
15.) Recruitment
Adult (over 18 years of age) patients presenting to a single tertiary care center with a hip fracture. All patients with hip fractures at this institution are admitted to the medical orthopaedic trauma service (MOTS). Prior to surgery, patients older than 75 years of age, or those with medical comorbidities will be optimized by the general medical service prior to surgery. All potentially eligible patients will be screened and documented as (1) eligible and included, (2) eligible and missed, or (3) excluded. The study coordinator will obtain informed consent for participation in the study using the approved IRB Informed Consent forms. All patients will provide written informed consent and will understand that by entering in the study they may receive placebo and not tranexamic acid. Participation in the study is voluntary and their decision to participate will not affect any other aspect of their care in case of refusal. Patients will have the right to withdraw from the study at any point. 16.) Allocation
a.)Sequence generation
After the patient consents and is enrolled in the study, the institution’s investigational pharmacist will assign the patient to either receive TXA or placebo via computer generated randomization. Patients will be randomized in blocks of b.)Concealment
The packaging of the injections will be performed by the investigational pharmacy and will be identical for both TXA and placebo. All clinicians, except for the pharmacist, will remain blinded until the data is analyzed.
Page 43 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
12
c.)Implementation
After the patient consents and is enrolled in the study, the institution’s investigational pharmacist will perform the randomization and assign the patient to either receive TXA or placebo. Patients will be randomized in blocks of 20. The packaging of the injections will be performed by the investigational pharmacy and will be identical for both TXA and placebo. All clinicians, except for the pharmacist, will remain blinded until the data is analyzed. 17.) Blinding
a.) Masking
The patient, the surgeon, the anesthesiologist and the hospitalist will all be blinded to the assignment of intervention. Therefore, the decision to transfuse a patient will be made independent of the intervention. b.)Emergency unblinding
Unblinding of intervention assignment will only be allowed in exceptional circumstances if knowlegde of treatment is crucial to further management of the patient. An example of this is if a patient becomes unstable during drug administration in the operating room. The allocation will not be disclosed to the surgeon or the patient or other study personnel who are not directly treating the patient at that time. All code breaks will be reported and documented. 18.) Methods
a.) Data collection methods
Baseline assessment includes sex, birth date, height and weight, mechanism of injury, time from injury to presentation to the emergency room, American Society of Anesthesiologists (ASA) classification, Charlson Comorbidity Index, comorbidities including diabetes, peripheral vascular disease, dementia, hypertension, and history of smoking. The hemoglobin and hematocrit will be recorded at the time of admission and on the morning of surgery, if applicable. Blood transfusion criteria will remain consistent with hospital standards (Hb<8 g/dL or symptomatic anemia) as determined by an independent, blinded medical team who will follow the patient throughout the hospital stay and number of blood transfusions received will be documented upon patient discharge. Hematocrit and hemoglobin will be recorded in all patients while they are in the hospital, for a minimum of 2 days postoperatively. Further monitoring will be conducted based on need as determined by the independent medical team. Estimated blood volume will be calculated from these values and used to estimate blood loss. After discharge, patients will undergo routine follow-up at 2wk, 6wk, 3mo, 6mo and 1 yr after surgery. Each will be questioned regarding possible adverse events that may have occurred since their previous visit. Further, electronic inpatient records
Page 44 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
13
will be reviewed at the 1 year follow-up appointment to determine if any undocumented adverse events may have occurred and patients will also be called at that time if they fail to attend their 1 year follow-up appointment. 19.) Data Management
All data will be entered electronically into a Microsoft Excel database that will be password protected on an institutional computer. Any identifying health information will be removed or, if needed, coded when data is summarized in a spreadsheet format for statistical analysis purposes. 20.) Statistical Analysis
a.) Outcomes
Descriptive analyses of the patient population will include reporting means (with standard deviations) for continuous variables and frequencies (with percentages) for categorical or discrete variables. Following the descriptive analysis, a chi-square analysis will be conducted to evaluate the superiority of tranexamic acid in reducing the rate of transfusion versus the placebo control group. The analysis and reporting of the results of the clinical outcomes will follow the CONSORT guidelines (www.consort-statement.org). We will conduct a multiple logistic regression model to determine if type of fracture (intertrochanteric or femoral neck), comorbidities, Charlson comorbidity index, age, time to surgery, and mechanism of injury are related to transfusion administration. Similarly we will conduct a multiple linear regression model to determine if patient comorbidities, age, time to surgery, and mechanism of injury are related to blood loss. We will also conduct subgroup analyses to determine if the effect of TXA is modified by fracture type (intertrochanteric or femoral neck). All analyses will be performed using Stata 14.0 software (Stata Corporation, College Station, TX, USA). b.)Additional analyses Our a priori hypothesis, based on retrospective data, 6 is that patients with intertrochanteric fractures incur more blood loss than femoral neck fractures and will have a higher rate of transfusion. If these subgroup analyses are underpowered, the subgroup data will be used to generate further hypotheses to be tested in the future.
c.)Analysis population and missing data
Not applicable- as there will largely be no compliance breakdowns given that the intervention is a one-time administration of a drug during a surgical procedure. Should a patient consent and be enrolled in the trial and decide to unenroll prior to drug administration they will not be taken into account for the analysis.
Page 45 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
14
In the event of missing data, ie missing hemoglobin levels postoperatively, we do not plan on using an imputing method but rather analyzing only the data collected given that these missing data points will likely be randomly arranged throughout the study. 21.) Methods: Monitoring
a.)Formal Committee
The data safety monitoring board (DSMB) has been established to monitor the trial and renew the study biannually. This board is independent of the trial and free of conflicts with any of the investigation team. b.)Interim analysis
Data will be analyzed every six months throughout the study by the study investigators.
22.) Harms
The secondary outcomes of this study including adverse outcomes and events. These events will be monitored for after the subject has provided consent and has been enrolled in the study. If a subject experiences an adverse event after the informed consent document is signed (entry) but the subject has not yet received the intervention in the operating room, the event will be reported as not related to study drug. Adverse events during hospitalization will be recorded and patients will be asked about adverse events during their follow-up appointments. Adverse events will be reported to the DSMB as well.
23.) Auditing
The data safety monitoring board (DSMB) has been established to monitor the trial and renew the study biannually. This board is independent of the trial and free of conflicts with any of the investigation team.
24.) Research ethics approval
The protocol and site specific consent forms have been approved by our institutional review board (IRB) with respect to scientific content and compliance with applicable research and human subjects regulations.
25.) Protocol amendments
Page 46 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
15
See attached.
26.) Consent or assent
a.) Consent
Informed consent will be obtained by research associated personnel at the time of patient presentation. Written consent will be obtained from the patient when possible, or from the health care proxy if the patient is unable to consent for themselves.
Each patient will be provided the written informed consent form to read and will have the opportunity to ask any questions related to the research protocol/methods to the researcher obtaining consent.
b.)Ancillary studies
not applicable
27.) Confidentiality
Data is only recorded electronicallyand will be kept in the Principal Investigator’s locked office on a password-protected computer. Only research personnel will have access to electronic files kept in the PIs locked office, and only research personnel will know the password needed to access research files. Patients will be numbered sequentially on the data collection sheet. Numbers will be associated with names and medical records, which will be stored in a separate file by the research coordinator.
28.) Declaration of interests
None of the authors of the study or study personnel have any financial relationships
related to the nature of the study.
29.) Access to data
n/a – single institution study
30.) Ancillary and post-trial care
n/a- this is a privately funded study with no study-specific insurance policy.
31.) Dissemination policy
a.) trial results
Page 47 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
16
The results from the trial will be reviewed by the authors and following editing from each member a manuscript will be prepared for publication in a peer reviewed journal. b.)authorship
The authors currently listed will be included as authors on the final manuscript submitted for publication according to their maintained involvement. New authors will be required by meet guidelines for authorship as stated previously. c.)Reproducible research
n/a
32.) Informed consent material
see attached
33.) Biological specimens
n/a
References
1. Brauer CA, Coca-Perraillon M, Cutler DM, Rosen AB. Incidence and mortality of hip
fractures in the united states. JAMA. 2009;302(14):1573-1579.
2. Richmond J, Aharonoff GB, Zuckerman JD, Koval KJ. Mortality risk after hip
fracture. J Orthop Trauma. 2003;17(1):53-56.
3. Heyes GJ, Tucker A, Marley D, Foster A. Predictors for 1-year mortality following
hip fracture: A retrospective review of 465 consecutive patients. Eur J Trauma
Emerg Surg. 2015.
Page 48 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
17
4. Shah MR, Aharonoff GB, Wolinsky P, Zuckerman JD, Koval KJ. Outcome after hip
fracture in individuals ninety years of age and older. J Orthop Trauma.
2001;15(1):34-39.
5. Sathiyakumar V, Greenberg SE, Molina CS, Thakore RV, Obremskey WT, Sethi MK.
Hip fractures are risky business: An analysis of the NSQIP data. Injury.
2015;46(4):703-708.
6. Foss NB, Kehlet H. Hidden blood loss after surgery for hip fracture. J Bone Joint
Surg Br. 2006;88(8):1053-1059.
7. Hill GE, Frawley WH, Griffith KE, Forestner JE, Minei JP. Allogeneic blood
transfusion increases the risk of postoperative bacterial infection: A meta-analysis. J
Trauma. 2003;54(5):908-914.
8. Shokoohi A, Stanworth S, Mistry D, Lamb S, Staves J, Murphy MF. The risks of red
cell transfusion for hip fracture surgery in the elderly. Vox Sang. 2012;103(3):223-
230.
9. Saleh A, Small T, Chandran Pillai AL, Schiltz NK, Klika AK, Barsoum WK. Allogenic
blood transfusion following total hip arthroplasty: Results from the nationwide
inpatient sample, 2000 to 2009. J Bone Joint Surg Am. 2014;96(18):e155.
10. Kagoma YK, Crowther MA, Douketis J, Bhandari M, Eikelboom J, Lim W. Use of
antifibrinolytic therapy to reduce transfusion in patients undergoing orthopedic
Page 49 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
18
surgery: A systematic review of randomized trials. Thromb Res. 2009;123(5):687-
696.
11. Eubanks JD. Antifibrinolytics in major orthopaedic surgery. J Am Acad Orthop
Surg. 2010;18(3):132-138.
12. Yuan C, Zhang H, He S. Efficacy and safety of using antifibrinolytic agents in spine
surgery: A meta-analysis. PLoS One. 2013;8(11):e82063.
13. Zufferey P, Merquiol F, Laporte S, et al. Do antifibrinolytics reduce allogeneic
blood transfusion in orthopedic surgery? Anesthesiology. 2006;105(5):1034-1046.
14. Tse EY, Cheung WY, Ng KF, Luk KD. Reducing perioperative blood loss and
allogeneic blood transfusion in patients undergoing major spine surgery. J Bone Joint
Surg Am. 2011;93(13):1268-1277.
15. CRASH-2 trial collaborators, Shakur H, Roberts I, et al. Effects of tranexamic acid
on death, vascular occlusive events, and blood transfusion in trauma patients with
significant haemorrhage (CRASH-2): A randomised, placebo-controlled trial. Lancet.
2010;376(9734):23-32.
16. CRASH-2 collaborators, Roberts I, Shakur H, et al. The importance of early
treatment with tranexamic acid in bleeding trauma patients: An exploratory
analysis of the CRASH-2 randomised controlled trial. Lancet. 2011;377(9771):1096-
101, 1101.e1-2.
Page 50 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
19
17. Whiting DR, Gillette BP, Duncan C, Smith H, Pagnano MW, Sierra RJ. Preliminary
results suggest tranexamic acid is safe and effective in arthroplasty patients with
severe comorbidities. Clin Orthop Relat Res. 2014;472(1):66-72.
18. Cid J, Lozano M. Tranexamic acid reduces allogeneic red cell transfusions in
patients undergoing total knee arthroplasty: Results of a meta-analysis of
randomized controlled trials. Transfusion. 2005;45(8):1302-1307.
19. Lemay E, Guay J, Cote C, Roy A. Tranexamic acid reduces the need for allogenic
red blood cell transfusions in patients undergoing total hip replacement. Can J
Anaesth. 2004;51(1):31-37.
20. Poeran J, Rasul R, Suzuki S, et al. Tranexamic acid use and postoperative
outcomes in patients undergoing total hip or knee arthroplasty in the united states:
Retrospective analysis of effectiveness and safety. BMJ. 2014;349:g4829.
21. Raksakietisak M, Sathitkarnmanee B, Srisaen P, et al. Two doses of tranexamic
acid reduce blood transfusion in complex spine surgery: A prospective randomized
study. Spine (Phila Pa 1976). 2015.
22. Wind TC, Barfield WR, Moskal JT. The effect of tranexamic acid on transfusion
rate in primary total hip arthroplasty. J Arthroplasty. 2014;29(2):387-389.
23. Tuttle JR, Ritterman SA, Cassidy DB, Anazonwu WA, Froehlich JA, Rubin LE. Cost
benefit analysis of topical tranexamic acid in primary total hip and knee
arthroplasty. J Arthroplasty. 2014;29(8):1512-1515.
Page 51 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
20
24. Huang F, Wu D, Ma G, Yin Z, Wang Q. The use of tranexamic acid to reduce blood
loss and transfusion in major orthopedic surgery: A meta-analysis. J Surg Res.
2014;186(1):318-327.
25. Nishihara S, Hamada M. Does tranexamic acid alter the risk of thromboembolism
after total hip arthroplasty in the absence of routine chemical thromboprophylaxis?
Bone Joint J. 2015;97-B(4):458-462.
26. Emara WM, Moez KK, Elkhouly AH. Topical versus intravenous tranexamic acid
as a blood conservation intervention for reduction of post-operative bleeding in
hemiarthroplasty. Anesth Essays Res. 2014;8(1):48-53.
27. Duncan CM, Gillette BP, Jacob AK, Sierra RJ, Sanchez-Sotelo J, Smith HM. Venous
thromboembolism and mortality associated with tranexamic acid use during total
hip and knee arthroplasty. J Arthroplasty. 2015;30(2):272-276.
28. Yang ZG, Chen WP, Wu LD. Effectiveness and safety of tranexamic acid in
reducing blood loss in total knee arthroplasty: A meta-analysis. J Bone Joint Surg Am.
2012;94(13):1153-1159.
29. Foss NB, Kristensen MT, Kehlet H. Anaemia impedes functional mobility after hip
fracture surgery. Age Ageing. 2008;37(2):173-178.
30. Lawrence VA, Silverstein JH, Cornell JE, Pederson T, Noveck H, Carson JL. Higher
hb level is associated with better early functional recovery after hip fracture repair.
Transfusion. 2003;43(12):1717-1722.
Page 52 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
21
31. Lee C, Freeman R, Edmondson M, Rogers BA. The efficacy of tranexamic acid in
hip hemiarthroplasty surgery: An observational cohort study. Injury.
2015;46(10):1978-1982.
32. Zufferey PJ, Miquet M, Quenet S, et al. Tranexamic acid in hip fracture surgery: A
randomized controlled trial. Br J Anaesth. 2010;104(1):23-30.
33. Vijay BS, Bedi V, Mitra S, Das B. Role of tranexamic acid in reducing
postoperative blood loss and transfusion requirement in patients undergoing hip
and femoral surgeries. Saudi J Anaesth. 2013;7(1):29-32.
34. Sadeghi M MA. Does a single bolus dose of tranexamic acid reduce blood loss and
transfusion requirements during hip fracture surgery? A prospective randomized
double blind study in 67 patients. Acta Medica Iranica. 2007;45(6):437-442.
Appendix
Blood Loss Calculation:Patient’s Blood Volume (PBV) = (k1 x Height3
(m)) + (k2 x Weight (kg)) + k3
k1 = 0.3669, k2 = 0.03219, and k3 = 0.6041 for men k1 = 0.3561, k2=0.03308, and k3 = 0.1833 for women
Multiplying the PBV by the hematocrit (Hct) gives the red blood cell (RBC) volume. As
such, a change in the RBC volume can be calculated from a change in the Hct level as
follows:
Pre-op RBC volume loss = PBV x (Admit Hct – Day of surgery Hct) Operative RBC volume loss = PBV x (Day of surgery Hct – PACU Hct)
If a patient requires a pre-op or intraoperative transfusion, the calculation will be adjusted as follows:
Pre-op RBC volume loss = [PBV x (Admit Hct – Day of surgery Hct)]+ (No. of Units Transfused x
0.285) / (Admit Hct – Day of surgery Hct) / 2)Operative RBC volume loss = [PBV x (Day of surgery
Page 53 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
22
Hct – PACU Hct)] +)]+ (No. of Units Transfused x 0.285) / (Day of surgery Hct – Post-op Hct) / 2
Page 54 of 54
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
Tranexamic Acid in Hip Fracture Patients: a protocol for a randomized, placebo controlled trial on the efficacy of
tranexamic acid in reducing blood loss in hip fracture patients
Journal: BMJ Open
Manuscript ID bmjopen-2015-010676.R2
Article Type: Protocol
Date Submitted by the Author: 29-Mar-2016
Complete List of Authors: Gausden, Elizabeth; Hospital for Special Surgery, Orthopaedic Surgery Garner, Matthew; Hospital for Special Surgery, Orthopaedic Surgery Warner, Stephen; Hospital for Special Surgery, Orthopaedic Surgery Levack, Ashley; Hospital for Special Surgery, Orthopaedic Surgery Nellestein, Andrew; Weill Cornell Medical College, Anesthesia Tedore, Tiffany; Weill Cornell Medical College, Anesthesia Flores, Eva; Weill Cornell Medical College, Internal Medicine Lorich, Dean; Hospital for Special Surgery, Orthopaedic Surgery
<b>Primary Subject Heading</b>:
Surgery
Secondary Subject Heading: Evidence based practice, Haematology (incl blood transfusion), Surgery
Keywords: tranexamic acid, hip fracture, blood transfusion
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on 26 July 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010676 on 21 June 2016. D
ownloaded from

For peer review only
1
Tranexamic Acid in Hip Fracture patients: a protocol for a randomized, placebo controlled trial on the efficacy of tranexamic acid in reducing
blood loss in hip fracture patients
Elizabeth Bishop Gausden, MD*1 [email protected]
Phone: (646) 350-9897 Fax: 212.606.1477
Matthew R. Garner, MD2 [email protected]
Stephen J. Warner, MD, PhD1
Ashley Levack, MD, MAS1 [email protected]
Andrew Nellestein, BS, MS3 [email protected]
Tiffany Tedore, MD4
Eva Flores, MD5 [email protected]
Dean G. Lorich, MD3
1 Hospital for Special Surgery Department of Orthopaedics
535 E. 70th Street New York, NY 10021
2 Harborview Medical Center Department of Orthopaedics
325 9th Ave. Seattle, WA 98104
3 New York Presbyterian Hospital
Department of Orthopaedic Trauma 525 E. 68th St
New York, NY 10065
4 New York Presbyterian Hospital Department of Anesthesiology
525 E. 68th St New York, NY 10065
5 New York Presbyterian Hospital Department of Internal Medicine
525 E. 68th St New York, NY 10065
*corresponding author word count: 3,415 Keywords: tranexamic acid, hip fracture, blood transfusion
Page 1 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from
For peer review only
2
Abstract
Introduction
There is a high incidence of blood transfusion following hip fractures in elderly
patients. Tranexamic acid (TXA) has proven efficacy in decreasing blood loss in
general trauma patients as well as patients undergoing elective orthopaedic surgery.
A randomized controlled trial will measure the effect of TXA in a population of
patients undergoing hip fracture surgery.
Methods
This is a double-blinded, randomized placebo-controlled trial. Patients admitted
through the emergency room that are diagnosed with an intertrochanteric or
femoral neck fracture will be eligible for enrollment and randomized to either
treatment with 1 gram of intravenous TXA or intravenous saline at the time of skin
incision. Patients undergoing percutaneous intervention for non-displaced or
minimally displaced femoral neck fractures will not be eligible for enrollment.
Postoperative transfusion rates will be recorded and blood loss will be calculated
from serial hematocrits.
Ethics and dissemination
This protocol was approved by the Institutional Review Board (IRB) and is
registered with clinicaltrials.gov. The findings of the trial will be disseminated
through peer-reviewed journals and conference presentations.
Page 2 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
3
Strengths and limitations of this study
• A prospective, randomized, placebo-controlled trial is the optimal study
design to address the question of efficacy of tranexamic acid (TXA) use in
patients with hip fractures
• The outcomes will be reported based on one-year follow-up, which is longer
follow-up than any other study examining tranexamic acid use in patients
with hip fractures.
• Findings will provide objective data from which clinicians can base future
guidelines regarding TXA administration.
• Recruitment is slow as patients and health-care proxies are wary of enrolling
in a study in a trauma setting.
Page 3 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
4
Introduction
Hip fractures in the elderly remain a pressing public health issue in the United
States given the aging population.1 Hip fractures are associated with numerous
adverse events and increased mortality up to one year after the event.2-5 Hidden
blood loss in hip fractures, in addition to intraoperative blood loss, may be as high
as 1,500 cc. 6,7 The rate of blood transfusion in the perioperative period for hip
fracture patients is reported between 20-60%.8-11 Total blood loss, and thus rate of
transfusion, is greater for extracapsular hip fractures compared to intracapsular hip
fractures.6 A meta-analysis of 20 studies found a significantly increased risk of post-
operative bacterial infection in patients who receive an allogenic blood transfusion
in the perioperative period.12 In addition to the increased risk of infection, patients
who require blood transfusion following hip fracture have an increased hospital
length of stay.13 Furthermore, an allogenic blood transfusion in the United States
was recently estimated to increase costs by $1,731 per admission.14
Numerous anti-fibrinolytics have been used to limit bleeding in orthopaedic surgery
and prevent the need for blood transfusion.15-19 One of these anti-fibrinolytics,
tranexamic acid (TXA), is a synthetic derivative of the amino acid lysine and acts as a
competitive inhibitor in the activation of plasminogen to plasmin, therefore
preventing the degradation of fibrin. As a result of the CRASH-2 trial,20,21 which
demonstrated reduced mortality in trauma patients who received TXA, the World
Health Organization (WHO) added TXA to the essential drugs list. Currently TXA is
Page 4 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
5
not routinely used in patients with hip fractures in the United States, despite its
common use worldwide and proven efficacy in reducing blood loss in other
populations.
Numerous studies have investigated the safety and efficacy of TXA in patients
undergoing elective orthopaedic surgery, including total joint replacement and
spine surgery.22-27 The consensus from this literature is overwhelmingly in favor of
administration of TXA given the decrease in blood loss, transfusion rates, and
cost.28,29 Although several individual studies have found increased risk of
thromboembolic events in groups receiving TXA,9,30 larger studies and meta-
analyses have uniformly found no increased risk of thrombosis.31,32
Patients who suffer hip fractures frequently have multiple comorbidities making
them more susceptible to adverse events from blood loss. 19,20 The most common
comorbidities of individuals with hip fractures are congestive heart failure, chronic
pulmonary disease and diabetes.1 Administering TXA to such patients has a
potential to offset blood loss, improve patient outcomes and lower cost of care by
decreasing the rate of transfusions.33,34 Five studies, all conducted outside the
United States, have previously reported results of using TXA in hip fracture
surgery.8-11,35 Sadeghi et al8 randomized 67 hip fracture patients to receive either
placebo injection or intravenous tranexamic acid at the time of surgery. They found
a significantly lower volume of blood loss (652 ± 228 mL vs. 1108 ± 372 mL, P <
0.003) and shorter hospital stays (4.3 ± 1.6 days vs. 5.8 ± 1.5 days, p< 0.05). Vijay et
Page 5 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
6
al.35 also reported significantly reduced transfusion rates in the TXA arm of their
clinical trial. In a retrospective cohort study, Lee et al11 similarly reported a
transfusion rate three times lower in patients who received TXA prior to
hemiarthroplasty. In a separate randomized controlled trial that compared
intravenous administration of TXA to topical TXA administration as well as placebo
in hip fracture patients undergoing hemiarthroplasty, both of the TXA groups
experienced less blood loss.9
In designing this study, we concluded that hip fracture patients are both likely to
experience significant blood loss and are susceptible to the adverse effects of blood
loss making them an ideal population to target for a randomized controlled trial of
the effects of perioperative TXA on blood loss. We hypothesize that administration
of TXA will decrease blood loss in hip fracture patients and lower the rate of
allogenic blood transfusion.
Objective
To investigate the hypothesis that TXA will lower blood loss and transfusion rate in
patients with hip fractures.
Methods and analysis
Overview of trial design
We are conducting a single-center randomized controlled trial using a parallel two-
arm design to investigate whether peri-operative tranexamic acid use will decrease
Page 6 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
7
the rate of transfusion in patients with hip fractures (Figure 1). Randomization will
be stratified by type of hip fracture (ie. intertrochanteric versus femoral neck
fracture). The surgical team, anesthesia team, and patients will be blinded to the
assignment. Once consent is obtained and a patient is enrolled, a 1:1 randomization
system will be employed by our institution’s investigational pharmacy to assign
patients to receive TXA or placebo. Patient enrollment will occur over
approximately 2 years and enrolled patients will be followed for 1 year
postoperatively. Incidence of blood transfusion, total calculated blood loss, and
acute adverse events (transfusion reaction, cerebrovascular accident, myocardial
infarction, pulmonary embolism, symptomatic deep vein thrombosis, surgical site
infection, and death) will be assessed in the perioperative period. Patients will also
be assessed at 2 weeks, 6 weeks, 3 months, 6 months and 12 months post-
operatively to capture long-term adverse events as well as determine mortality rate.
This trial is registered (NCT01940536) and has received ethical approval from the
Weill Cornell Medical College Institutional Review Board (IRB# 1301013463).
Primary research question
In patients with hip fractures, does a single bolus of tranexamic acid at the time of
surgery result in a lower rate of blood transfusion?
Secondary research question
In patients with hip fractures, does a single bolus of tranexamic acid at the time of
surgery result in:
Page 7 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
8
1.) decreased calculated blood loss?
2.) shorter length of hospitalization?
3.) differences in occurrence of adverse events?
Hypothesis
As a primary outcome, there will be a decreased rate of blood transfusion in patients
who receive tranexamic acid intraoperatively and no significant increase in
frequency or severity of adverse events in comparison to patients who receive
placebo. This study is powered to address the primary outcome of difference in
transfusion rates between the two study arms for both intracapsular and
extracapsular hip fractures.
Setting and participants
Adult patients (over 18 years of age) presenting to a single tertiary care center with
an acute hip fracture will be screened for eligibility. All patients with hip fractures
at this institution are admitted to the medical orthopaedic trauma service (MOTS).
Prior to surgery, patients older than 75 years of age, or those with medical
comorbidities will be optimized by the general medical service prior to surgery. All
potentially eligible patients will be screened and documented as (1) eligible and
included, (2) eligible and missed, or (3) excluded. The study coordinator will obtain
informed consent for participation in the study using the approved IRB Informed
Consent forms.
Page 8 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
9
All patients will provide written informed consent and will understand that by
entering in the study they may receive either placebo or tranexamic acid.
Participation in the study is voluntary and their decision to participate will not
affect any other aspect of their care in case of refusal. Patients will have the right to
withdraw from the study at any point.
Inclusion criteria
Patients admitted through the emergency department or transferred to our
institution who meet the following criteria will be included in the study:
• Adults over the age of 18
• Acute intertrochanteric or femoral neck hip fracture
• Patients treated surgically with cephalomedullary nail, hemiarthroplasty, or
total hip arthroplasty (THA)
Exclusion criteria
Patient who meet any one or more of the following criteria will be excluded from the
study:
• Use of any anticoagulant at the time of admission (for example, vitamin K
antagonists, anti-thrombin agents, antiplatelet agents, or factor IIa & Xa
inhibitors)
• Documented allergy to tranexamic acid
• History of deep vein thrombosis or pulmonary embolus
• Hepatic dysfunction (AST/ALT > 60)
• Renal dysfunction (Cr >1.5 of GRR > 30)
Page 9 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
10
• Active coronary artery disease (event in the past 12 months)
• History of cerebrovascular accident (CVA) in the past 12 months
• Presence of a drug-eluting stent
• Color blindness
• Leukemia or any active cancer
• Coagulopathy based on admission laboratory values (INR> 1.4, PTT > 1.4x
normal, Platelets < 50,000)
• Non-displaced femoral neck fractures treated percutaneously
Baseline
Baseline assessment includes sex; birth date; height and weight; mechanism of
injury; time from injury to presentation to our institution; American Society of
Anesthesiologists (ASA) classification; Charlson Comorbidity Index; and
comorbidities including diabetes, cardiovascular disease, pulmonary disease,
peripheral vascular disease, dementia, hypertension, and history of smoking. The
hemoglobin and hematocrit will be recorded at the time of admission and on the
morning of surgery.
Blinding
After consent and enrollment in the study, patients will be stratified based on type
of hip fracture (intracapsular or extracapsular). Following stratification by fracture
type, the institution’s investigational pharmacist will perform the randomization
and assign the patient to either receive TXA or placebo. Patients will be
Page 10 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
11
randomized in blocks of 20. The packaging of the injections will be performed by
the investigational pharmacy and will be identical for both TXA and placebo. All
patients and clinicians, with the exception of the pharmacist, will remain blinded
until the data is analyzed.
Intervention
The patients randomized to the treatment arm will receive 1 gram of intravenous
tranexamic acid mixed in 100 cc of saline, bolused at the time of surgical incision.
Those assigned to the placebo group will receive an equivalent volume bolus of
saline at the time of surgical incision.
Patients with intertrochanteric hip fractures will be treated with a long
intramedullary hip screw implant with a trochanteric start point. Patients with
displaced femoral neck fractures will be treated with a cemented or non-cemented
hemiarthroplasty or total hip arthroplasty at the discretion of the treating surgeon.
All surgeries will be supervised by the attending surgeon with the assistance of
orthopaedic residents. The surgical technique as well as the anesthetic technique
(regional versus general anesthesia) will be recorded and assessed in the final
analysis. The time from injury to surgery will also be recorded and included in the
analysis.
Blood transfusion criteria will remain consistent with hospital standards (Hb<8
g/dL or symptomatic anemia) as determined by an independent, blinded medical
team who will follow the patient throughout the hospital stay. Number of blood
Page 11 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
12
transfusions received will be documented upon patient discharge. Hematocrit and
hemoglobin will be recorded daily for all patients while they remain in the hospital.
Further monitoring will be conducted based on need as determined by the
independent medical team. Estimated blood volume will be calculated using
baseline height, weight and gender and the laboaratory values will be used to
calculate estimated blood loss post-operatively (Appendix 1).36
All patients will be permitted to weight-bear as tolerated post-operatively and deep
vein thrombosis (DVT) prophylaxis will be standardized. All enrolled patients will
receive subcutaneous heparin, 5000 units every 8 hours beginning upon admission
until 12 hours prior to surgery and restarting 6 hours after surgery. Calf mechanical
compression devices will also be utilized during the inpatient stay and will remain
on at all times with the exception of physical therapy sessions. Following discharge
from the hospital patients will be given aspirin 325 mg twice daily for DVT
prophylaxis for a total of 6 weeks. Diagnostic studies to assess for thromboembolic
events (i.e. DVT, pulmonary embolism, and stroke) will be ordered only if the
patient develops clinical signs or symptoms that justify their use.
Primary Outcome
The primary outcome of the study will be the rate of blood transfusion from the
time of surgery until discharge. Patients will be monitored with serial hemoglobin
and hematocrit measurements and their vital signs will be recorded as per the
standard of care to determine the need for blood transfusion. Only intraoperative and
postoperative blood transfusions will be considered for the primary outcome measure as
Page 12 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
13
the drug will be administered at the time of surgical incision. Therefore, we anticipate that
TXA administration in this study will only modify the rate of intraoperative or postoperative
transfusion, and have no effect on the rate of pre-operative transfusion in this population.
Secondary Outcome
The secondary study outcomes include the calculated blood loss (calculated based
on validated methods as outlined in Appendix 1), frequency of adverse events
(including transfusion reaction, myocardial infarction, symptomatic deep vein
thrombosis, pulmonary embolus, cerebrovascular accident, re-operation, re-
admission, infection, and death) (Figure 1).
For the study purposes, a transfusion reaction will be defined as any constellation of
symptoms during a blood transfusion that necessitate discontinuation of the
transfusion.
Myocardial infarction will be defined as a cardiologist diagnosis of myocardial
infarction based on a combination of electrocardiogram changes, echocardiogram
changes, or creatine kinase MB or troponin changes. A pulmonary embolism must
be confirmed by pulmonary angiography, computed tomographic (CT) scan of the
chest, echocardiographic visualization or visualization of thrombus at autopsy. A
symptomatic deep vein thrombosis must be confirmed by venography, CT scan,
magnetic resonance imaging, or pathologic evidence at autopsy. A cerebrovascular
accident must be diagnosed by a neurologist and will be defined as an embolic,
thrombotic or hemorrhagic vascular accident or stroke with motor, sensory, or
cognitive dysfunction that persists for longer than 24 hours.37
Page 13 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
14
A surgical site infection (SSI) will be defined as either superficial or deep infection.
Superficial SSI involves only skin or subcutaneous tissue while a deep SSI extends
deep to the fascial and muscle layers. Reoperation is defined as any return to the
operating room for a procedure related to the fractured hip.
Sample size consideration
The transfusion rate amongst patients with hip fractures is between 6-60%.8-11,35
Our institutional transfusion rate was calculated based on a random sample of 60
patients and was 65% for extracapsular hip fractures and 35% for intracapsular hip
fractures, for an overall transfusion rate of 49%. The average reduction in
transfusion rate in the previous 5 studies using TXA was 20%.8-11,35 We plan to
include a total of 338 patients (146 intracapsular hip fractures and 192
extracapsular hip fractures). This study design will achieve 81% power to detect a
reduction in blood transfusion from 65% in the placebo control group to 45% in the
tranexamic acid group with statistical significance set to alpha equal to 0.05 for the
extracapsular hip fracture group. Similarly the study will achieve 81% power to
detect a reduction in blood transfusion from 35% in the placebo control group to
15% in the tranexamic acid group with statistical significance set to alpha equal to
0.05 for the intracapsular hip fracture group.
Data analysis plan
Descriptive analyses of the patient population will include reporting means (with
standard deviations) for continuous variables and frequencies (with percentages)
for categorical or discrete variables. A chi-square analysis will be conducted to
Page 14 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
15
evaluate the superiority of tranexamic acid in reducing the rate of transfusion in the
TXA group versus the placebo control group. The analysis and reporting of the
results of the clinical outcomes will follow the CONSORT guidelines (www.consort-
statement.org). We will conduct a multiple logistic regression model to determine if
type of fracture (intertrochanteric or femoral neck), comorbidities, Charlson
comorbidity index, age, time to surgery, and mechanism of injury are related to
transfusion administration. Similarly we will conduct a multiple linear regression
model to determine which variables are related to blood loss. We will also conduct
subgroup analyses to determine if the effect of TXA is modified by fracture type
(intertrochanteric or femoral neck).
Our a priori hypothesis, based on retrospective data,6 is that patients with
intertrochanteric fractures incur more blood loss than femoral neck fractures and
will have a higher rate of transfusion. If these subgroup analyses are
underpowered, the subgroup data will be used to generate further hypotheses to be
tested in the future. All analyses will be performed using Stata 14.0 software (Stata
Corporation, College Station, TX, USA).
Data safety monitoring
The data safety monitoring board (DSMB) has been established to monitor the trial
safety and renew the study biannually. This board is independent of the trial and
free of conflicts with any of the investigation team.
Page 15 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
16
Discussion
There is clinical uncertainty and a lack of high-quality evidence regarding the use of
TXA in hip fracture patients. Despite its proven efficacy in elective orthopaedic
surgery,25,38 the optimal dosing and timing of TXA administration is still debated.39
Furthermore, the efficacy and side effect profile of TXA in patients with fractures
remains unclear. The immediate goal of this trial is to provide high-quality evidence
that can be used to develop clinical guidelines for use of TXA in patients with hip
fractures.
Patients undergoing elective total joint arthroplasty and elective spine surgery
represent a different population from patients who sustain hip fractures. A larger
percentage of hip fracture patients have significant medical comorbidities, and
many have history of cardiac disease.1 While TXA has demonstrated safety and
efficacy in patients without significant cardiac disease undergoing elective surgery,
there is still debate if TXA will have the same effect in patients with significant
comorbidities.25,39,40 The data investigating TXA in patients with comorbidities is
limited, which has further deterred clinicians from using TXA in patients with hip
fractures. However, the potential benefit of decreasing blood loss and decreasing
the number of transfusions following hip fracture surgery is overwhelming and will
likely result in improved patient outcomes, shorter length of stay and lower cost.
The study investigators believe that the potential benefit of TXA in such patients
outweighs the risk of TXA. The majority of literature regarding TXA has confirmed
Page 16 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
17
its safety and squelched concerns that its use will result in higher rates of
thrombosis.20,30,32,40,41
Of the five studies investigating the use of TXA in hip fracture patients, four were
randomized controlled trials that were underpowered for detecting significant
differences in thromboembolic events (Table 1).8-11,35 Furthermore, patients were
only followed perioperatively, and differences in six-month and one-year mortality
rates and late-onset complications were not assessed.
Use of Tranexamic Acid (TXA) in Patients with Hip Fractures
Country Design Hip fx ( IT or FNF)
TXA Regimen
DVT PPX Sample size
Blood loss (cc)
Transfuse Rate %
Thrombo-embolic Events
Lee 201511
UK Cohort Hemi-arthroplasy only
1 g bolus preop
Tinzaparin 84 cases/ 187 controls
- 6* 1
- 19 4
Emara 20149
Egypt RCT Hemi-arthroplasty only
10 mg/kg bolus, then 5 mg/kg/h infusion
Clexane 20 cases IV/ 20 cases topical/20 controls
640 5* 5
1100 32 0
Zufferey 201010
France RCT Hip fractures
15 mg/kg bolus preop and 3 h later
Fondaparinux x 35 days (mandatory ultrasound)
57 cases/ 53 controls
975 42 0
1178 60 0
Sadeghi and Mehr-Aein 20068
Iran RCT Hip fractures
15 mg/kg bolus preop
n/a
32 cases/ 35 controls
960 37 0
1484 57 0
Vijay 201335
India RCT Hip fractures
10 mg/kg bolus at surgery
N/a 45 cases/ 45 controls
39* 16 0
91* 40 0
Four out of five studies identified a significant decrease in rate of transfusion in
patients who received TXA compared to those that did not.8-11,35 The largest study,
Page 17 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
18
with a total of 219 patients, was a cohort study with no randomization.11 While they
found a significant decrease in blood transfusion rate, the study design limits the
interpretation of the results secondary to the potential biases of surgeon and patient
preference. Several studies excluded all patients with preoperative anemia, which
limits the generalizability of their findings.8,9 None of the randomized trials
provided a detailed analysis of total number of patients excluded from the study at
each stage. While the early results from these studies are promising, the overall
validity cannot be confirmed without this information. Similarly, there has yet to be
a large study to perform a complete subgroup analysis to determine the efficacy of
TXA amongst both intracapsular and extracapsular hip fracture patients.
Furthermore, the studies did not follow patients up to 1 year postoperatively, which
is our intention. The extended follow-up period allows for assessment of mortality
at 12 months as well as incidence of unanticipated adverse events following
discharge from the hospital. The most novel characteristic of this study in
comparison to the other studies is that it is powered to detect a significant
difference in blood transfusion rates in both intracapsular and extracapsular hip
fractures. As the hidden blood loss experienced by hip fracture patients is distinct
between these two patterns of hip fractures,6 it is important to demonstrate efficacy
in both groups independently.
Tranexamic acid has the potential to decrease transfusion rates by decreasing blood
loss in patients with hip fractures. Ultimately, this will decreased hospital length of
stay and improve outcomes in the hundreds of thousands of patients with hip
Page 18 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
19
fractures every year. If the results prove the efficacy of TXA in hip fracture patients,
this study may change the standard of care across the United States for these
patients.
Page 19 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
20
Funding
This work is supported by a Dr. Thomas Sculco grant and a Dr. Joseph M. Lane grant.
Contributor Statement
Elizabeth B. Gausden: This author revised the study from its original form and condensed the application of the tranexamic acid to one dose in the operating room in order to facilitate the flow of the project. This author made substantial contributions to the planning of data analysis, drafting and revising of the protocol, final approval of the version to be published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy of the work. Matthew R. Garner: This author conceived of the study and designed the first draft of the protocol. He was awarded the Thomas P. Sculco Research Grant and the Joseph M. Lane Research Grant for his proposal of the project. He made substantial contributions to the drafting and revising of the protocol, final approval of the version to be published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy of the work. Ashley Levack: This author made substantial contributions to the study design, modifications of the study to conform to guidelines and for logistics. She will also be involved in patient recruitment, data collection and analysis. This author made substantial contributions to the design of the work, planning of data analysis, drafting and revising of the protocol, final approval of the version to be published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy of the work. Stephen Warner: This author made substantial contributions to the design of the work, planning of data analysis, drafting and revising of the protocol, final approval of the version to be published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy of the work. Andrew Nellestein: This is a research assistant who facilitated IRB submissions and amendments. He is also coordinating the enrollment of patients in the study and working with the orthopaedic trauma team during the process of drug administration. This author made substantial contributions to the design of the work, planning of data analysis, drafting and revising of the protocol, final approval of the version to be published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy of the work.
Page 20 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
21
Tiffany Tedore: Dr. Tedore is the main anesthesiologist who will be orchestrating the anesthesiologists who administer the drug prior to skin incision. This author made substantial contributions to the design of the work, planning of data analysis, drafting and revising of the protocol, final approval of the version to be published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy of the work. Eva Flores: Dr, Flores is the head of the Medical Orthopaedic Trauma Service (MOTS) who organizes the medical attendings who manage the patients following surgery. This author made substantial contributions to the design of the work, planning of data analysis, drafting and revising of the protocol, final approval of the version to be published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy of the work. Dean G. Lorich: Dr. Lorich is the chief of the orthopaedic trauma service at NYP. This author made substantial contributions to the design of the work, planning of data analysis, drafting and revising of the protocol, final approval of the version to be published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy of the work.
Competing Interest None of the authors have any disclosures pertaining to this research.
Page 21 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
22
Figure Legend
Figure 1: Study Design (TXA: tranexamic acid; PRBC: packed red blood cells)
Table 1: Previously reported outcomes of TXA in hip fracture patients. *drain output. Thromboembolic events include only symptomatic thromboembolic events.
Page 22 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
23
References
1. Brauer CA, Coca-Perraillon M, Cutler DM, Rosen AB. Incidence and mortality of hip
fractures in the united states. JAMA. 2009;302(14):1573-1579.
2. Richmond J, Aharonoff GB, Zuckerman JD, Koval KJ. Mortality risk after hip
fracture. J Orthop Trauma. 2003;17(1):53-56.
3. Heyes GJ, Tucker A, Marley D, Foster A. Predictors for 1-year mortality following
hip fracture: A retrospective review of 465 consecutive patients. Eur J Trauma
Emerg Surg. 2015.
4. Shah MR, Aharonoff GB, Wolinsky P, Zuckerman JD, Koval KJ. Outcome after hip
fracture in individuals ninety years of age and older. J Orthop Trauma.
2001;15(1):34-39.
5. Sathiyakumar V, Greenberg SE, Molina CS, Thakore RV, Obremskey WT, Sethi MK.
Hip fractures are risky business: An analysis of the NSQIP data. Injury.
2015;46(4):703-708.
6. Foss NB, Kehlet H. Hidden blood loss after surgery for hip fracture. J Bone Joint
Surg Br. 2006;88(8):1053-1059.
7. Smith GH, Tsang J, Molyneux SG, White TO. The hidden blood loss after hip
fracture. Injury. 2011;42(2):133-135.
Page 23 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
24
8. Sadeghi M MA. Does a single bolus dose of tranexamic acid reduce blood loss and
transfusion requirements during hip fracture surgery? A prospective randomized
double blind study in 67 patients. Acta Medica Iranica. 2007;45(6):437-442.
9. Emara WM, Moez KK, Elkhouly AH. Topical versus intravenous tranexamic acid as
a blood conservation intervention for reduction of post-operative bleeding in
hemiarthroplasty. Anesth Essays Res. 2014;8(1):48-53.
10. Zufferey PJ, Miquet M, Quenet S, et al. Tranexamic acid in hip fracture surgery: A
randomized controlled trial. Br J Anaesth. 2010;104(1):23-30.
11. Lee C, Freeman R, Edmondson M, Rogers BA. The efficacy of tranexamic acid in
hip hemiarthroplasty surgery: An observational cohort study. Injury.
2015;46(10):1978-1982.
12. Hill GE, Frawley WH, Griffith KE, Forestner JE, Minei JP. Allogeneic blood
transfusion increases the risk of postoperative bacterial infection: A meta-analysis. J
Trauma. 2003;54(5):908-914.
13. Shokoohi A, Stanworth S, Mistry D, Lamb S, Staves J, Murphy MF. The risks of red
cell transfusion for hip fracture surgery in the elderly. Vox Sang. 2012;103(3):223-
230.
14. Saleh A, Small T, Chandran Pillai AL, Schiltz NK, Klika AK, Barsoum WK. Allogenic
blood transfusion following total hip arthroplasty: Results from the nationwide
inpatient sample, 2000 to 2009. J Bone Joint Surg Am. 2014;96(18):e155.
Page 24 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
25
15. Kagoma YK, Crowther MA, Douketis J, Bhandari M, Eikelboom J, Lim W. Use of
antifibrinolytic therapy to reduce transfusion in patients undergoing orthopedic
surgery: A systematic review of randomized trials. Thromb Res. 2009;123(5):687-
696.
16. Eubanks JD. Antifibrinolytics in major orthopaedic surgery. J Am Acad Orthop
Surg. 2010;18(3):132-138.
17. Yuan C, Zhang H, He S. Efficacy and safety of using antifibrinolytic agents in spine
surgery: A meta-analysis. PLoS One. 2013;8(11):e82063.
18. Zufferey P, Merquiol F, Laporte S, et al. Do antifibrinolytics reduce allogeneic
blood transfusion in orthopedic surgery? Anesthesiology. 2006;105(5):1034-1046.
19. Tse EY, Cheung WY, Ng KF, Luk KD. Reducing perioperative blood loss and
allogeneic blood transfusion in patients undergoing major spine surgery. J Bone Joint
Surg Am. 2011;93(13):1268-1277.
20. CRASH-2 trial collaborators, Shakur H, Roberts I, et al. Effects of tranexamic acid
on death, vascular occlusive events, and blood transfusion in trauma patients with
significant haemorrhage (CRASH-2): A randomised, placebo-controlled trial. Lancet.
2010;376(9734):23-32.
21. CRASH-2 collaborators, Roberts I, Shakur H, et al. The importance of early
treatment with tranexamic acid in bleeding trauma patients: An exploratory
Page 25 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
26
analysis of the CRASH-2 randomised controlled trial. Lancet. 2011;377(9771):1096-
101, 1101.e1-2.
22. Whiting DR, Gillette BP, Duncan C, Smith H, Pagnano MW, Sierra RJ. Preliminary
results suggest tranexamic acid is safe and effective in arthroplasty patients with
severe comorbidities. Clin Orthop Relat Res. 2014;472(1):66-72.
23. Cid J, Lozano M. Tranexamic acid reduces allogeneic red cell transfusions in
patients undergoing total knee arthroplasty: Results of a meta-analysis of
randomized controlled trials. Transfusion. 2005;45(8):1302-1307.
24. Lemay E, Guay J, Cote C, Roy A. Tranexamic acid reduces the need for allogenic
red blood cell transfusions in patients undergoing total hip replacement. Can J
Anaesth. 2004;51(1):31-37.
25. Poeran J, Rasul R, Suzuki S, et al. Tranexamic acid use and postoperative
outcomes in patients undergoing total hip or knee arthroplasty in the united states:
Retrospective analysis of effectiveness and safety. BMJ. 2014;349:g4829.
26. Raksakietisak M, Sathitkarnmanee B, Srisaen P, et al. Two doses of tranexamic
acid reduce blood transfusion in complex spine surgery: A prospective randomized
study. Spine (Phila Pa 1976). 2015.
27. Wind TC, Barfield WR, Moskal JT. The effect of tranexamic acid on transfusion
rate in primary total hip arthroplasty. J Arthroplasty. 2014;29(2):387-389.
Page 26 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
27
28. Tuttle JR, Ritterman SA, Cassidy DB, Anazonwu WA, Froehlich JA, Rubin LE. Cost
benefit analysis of topical tranexamic acid in primary total hip and knee
arthroplasty. J Arthroplasty. 2014;29(8):1512-1515.
29. Huang F, Wu D, Ma G, Yin Z, Wang Q. The use of tranexamic acid to reduce blood
loss and transfusion in major orthopedic surgery: A meta-analysis. J Surg Res.
2014;186(1):318-327.
30. Nishihara S, Hamada M. Does tranexamic acid alter the risk of thromboembolism
after total hip arthroplasty in the absence of routine chemical thromboprophylaxis?
Bone Joint J. 2015;97-B(4):458-462.
31. Duncan CM, Gillette BP, Jacob AK, Sierra RJ, Sanchez-Sotelo J, Smith HM. Venous
thromboembolism and mortality associated with tranexamic acid use during total
hip and knee arthroplasty. J Arthroplasty. 2015;30(2):272-276.
32. Yang ZG, Chen WP, Wu LD. Effectiveness and safety of tranexamic acid in
reducing blood loss in total knee arthroplasty: A meta-analysis. J Bone Joint Surg Am.
2012;94(13):1153-1159.
33. Foss NB, Kristensen MT, Kehlet H. Anaemia impedes functional mobility after hip
fracture surgery. Age Ageing. 2008;37(2):173-178.
34. Lawrence VA, Silverstein JH, Cornell JE, Pederson T, Noveck H, Carson JL. Higher
hb level is associated with better early functional recovery after hip fracture repair.
Transfusion. 2003;43(12):1717-1722.
Page 27 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
28
35. Vijay BS, Bedi V, Mitra S, Das B. Role of tranexamic acid in reducing
postoperative blood loss and transfusion requirement in patients undergoing hip
and femoral surgeries. Saudi J Anaesth. 2013;7(1):29-32.
36. George DA, Sarraf KM, Nwaboku H. Single perioperative dose of tranexamic acid
in primary hip and knee arthroplasty. Eur J Orthop Surg Traumatol. 2015;25(1):129-
133.
37. Basques BA, Toy JO, Bohl DD, Golinvaux NS, Grauer JN. General compared with
spinal anesthesia for total hip arthroplasty. J Bone Joint Surg Am. 2015;97(6):455-
461.
38. Danninger T, Memtsoudis SG. Tranexamic acid and orthopedic surgery-the
search for the holy grail of blood conservation. Ann Transl Med. 2015;3(6):77-
5839.2015.01.25.
39. Simmons J, Sikorski RA, Pittet JF. Tranexamic acid: From trauma to routine
perioperative use. Curr Opin Anaesthesiol. 2015;28(2):191-200.
40. Whiting DR, Gillette BP, Duncan C, Smith H, Pagnano MW, Sierra RJ. Preliminary
results suggest tranexamic acid is safe and effective in arthroplasty patients with
severe comorbidities. Clin Orthop Relat Res. 2014;472(1):66-72.
41. Gillette BP, DeSimone LJ, Trousdale RT, Pagnano MW, Sierra RJ. Low risk of
thromboembolic complications with tranexamic acid after primary total hip and
knee arthroplasty. Clin Orthop Relat Res. 2013;471(1):150-154.
Page 28 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
29
Page 29 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from
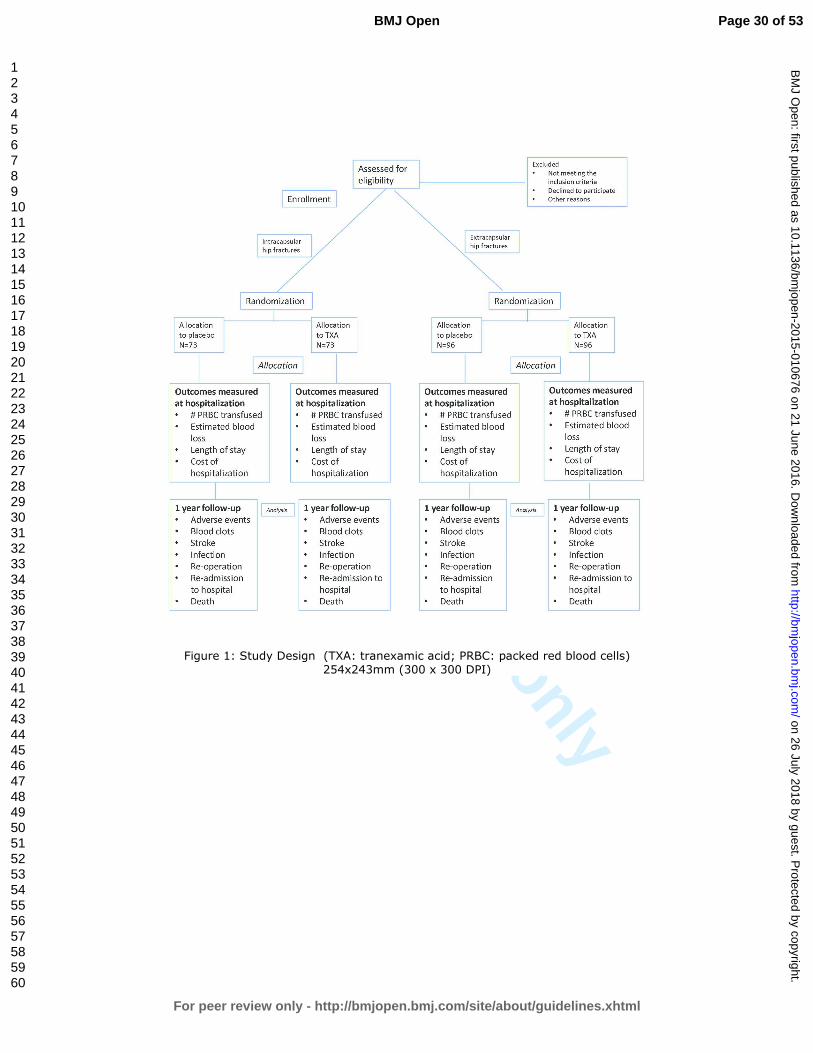
For peer review only
Figure 1: Study Design (TXA: tranexamic acid; PRBC: packed red blood cells)
254x243mm (300 x 300 DPI)
Page 30 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
Appendix
Blood Loss Calculation:Patient’s Blood Volume (PBV) = (k1 x Height3 (m)) + (k2 x Weight (kg)) + k3
k1 = 0.3669, k2 = 0.03219, and k3 = 0.6041 for men k1 = 0.3561, k2=0.03308, and k3 = 0.1833 for women
Multiplying the PBV by the hematocrit (Hct) gives the red blood cell (RBC) volume. As
such, a change in the RBC volume can be calculated from a change in the Hct level as
follows:
Pre-‐op RBC volume loss = PBV x (Admit Hct – Day of surgery Hct)
Operative RBC volume loss = PBV x (Day of surgery Hct – PACU Hct)
Post-‐operative RBC volume loss= PBX x (PACU Hct – Hct POD#x)If a patient requires a pre-‐op or intraoperative transfusion, the calculation will be adjusted as follows:
Pre-‐op RBC volume loss = [PBV x (Admit Hct – Day of surgery Hct)]+ (No. of Units Transfused x 0.285) / (Admit Hct – Day of surgery Hct) / 2)
Operative RBC volume loss = [PBV x (Day of surgery Hct – PACU Hct)] +)]+ (No. of Units Transfused x 0.285) / (Day of surgery Hct – Post-‐op Hct) / 2
Page 31 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
1
Spirit Checklist 1.) Title
Tranexamic Acid in Hip Fracture patients: a protocol for a randomized, placebo controlled trial on the efficacy of tranexamic acid in reducing blood loss in hip fracture patients
2.) Trial Registration
a.) Registry set “The Effect of Tranexamic Acid on Transfusion Rates in Intertrochanteric Hip Fractures” Registered August 2014 clinicaltrials.gov: NCT01940536 13083
b.) Data set
Data Category Information Primary registry and trial identifying number
Clinicaltrials.gov NCT01940536
Date of registration in primary registry
August 2014
Secondary identifying numbers
13083
Source of monetary support
Thomas Sculco Grant Joseph Lane Grant
Primary sponsor Thomas P. Sculco Research Grant Secondary sponsor Joseph M. Lane Research Grant Contact for public queries
Elizabeth Gausden, MD; [email protected]
Contact for scientific queries
Elizabeth Gausden, MD; [email protected]
Public Title Tranexamic Acid in Hip Fracture patients Scientific title Tranexamic Acid in Hip Fracture patients: a protocol for a
randomized, placebo controlled trial on the efficacy of tranexamic acid in reducing blood loss in hip fracture patients
Countries of recruitment
United States
Page 32 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
2
Health condition(s) studied
Blood loss after hip fracture and hip fracture surgery
Intervention Use of intravenous tranexamic acid at the time of hip fracture surgery versus placebo (intravenous 0.9% saline)
Key inclusion and exclusion criteria
Inclusion Adults over the age of 18 Intertrochanteric or femoral neck hip fracture Patients treated surgically with cephalomedullary
nail or hemiarthroplasty Exclusion
Preoperative use of anticoagulant (Plavix, Warfarin, Lovenox)
Documented allergy to tranexamic acid History of deep vein thrombosis or pulmonary
embolus Hepatic dysfunction (AST/ALT > 60) Renal dysfunction (Cr >1.5 of GRR > 30) Active coronary artery disease (event in the past 12
months), history of cerebrovascular accident (CVA) in the past 12 months, or presence of a drug-eluting stent
Color blindness Leukemia or any active cancer Coagulopathy (INR> 1.4, PTT > 1.4x normal,
Platelets < 100,000) Non-displaced femoral neck fractures treated
percutaneously
Study type Interventional Allocation: randomized Intervention model: parallel assignment Masking: Double blinded Primary purpose: preventing blood loss in hip fractures Phase III
Date of first enrollment
Pending
Target sample size 338 Primary outcome (s)
Transfusion of packed red blood cells (PRBC) following hip fracture surgery
Secondary outcome(s)
Calculated blood loss following surgery Adverse events (including transfusion reaction, myocardial infarction, deep vein thrombosis, pulmonary embolus, cerebrovascular accident, re-operation, re-admission, infection, and death)
Page 33 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
3
3.) Protocol version
The protocol has been modified from the original version listed on clinicaltrials.gov. The 2 changes reflect the inclusion of intracapsular hip fractures to be treated with arthroplasty as well as a revised power analysis and target study size.
4.) Funding The funding for this study is coming from two grants, one from Dr. Joseph Lane and one from Dr. Thomas Sculco.
5.) Roles and Responsibilities a.) Contributorship
Elizabeth B. Gausden: This author revised the study from its original form and condensed the application of the tranexamic acid to one dose in the operating room in order to facilitate the flow of the project. This author made substantial contributions to the planning of data analysis, drafting and revising of the protocol, final approval of the version to be published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy of the work. Matthew R. Garner: This author conceived of the study and designed the first draft of the protocol. He was awarded the Thomas P. Sculco Research Grant and the Joseph M. Lane Research Grant for his proposal of the project. He made substantial contributions to the drafting and revising of the protocol, final approval of the version to be published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy of the work. Ashley Levack: This author made substantial contributions to the study design, modifications of the study to conform to guidelines and for logistics. She will also be involved in patient recruitment, data collection and analysis. This author made substantial contributions to the design of the work, planning of data analysis, drafting and revising of the protocol, final approval of the version to be published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy of the work. Stephen Warner: This author made substantial contributions to the design of the work, planning of data analysis, drafting and revising of the protocol, final approval of the version to be published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy of the work.
Page 34 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
4
Andrew Nellestein: This is a research assistant who facilitated IRB submissions and amendments. He is also coordinating the enrollment of patients in the study and working with the orthopaedic trauma team during the process of drug administration. This author made substantial contributions to the design of the work, planning of data analysis, drafting and revising of the protocol, final approval of the version to be published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy of the work. Tiffany Tedore: Dr. Tedore is the main anesthesiologist who will be orchestrating the anesthesiologists who administer the drug prior to skin incision. This author made substantial contributions to the design of the work, planning of data analysis, drafting and revising of the protocol, final approval of the version to be published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy of the work. Eva Flores: Dr, Flores is the head of the Medical Orthopaedic Trauma Service (MOTS) who organizes the medical attendings who manage the patients following surgery. This author made substantial contributions to the design of the work, planning of data analysis, drafting and revising of the protocol, final approval of the version to be published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy of the work. Dean G. Lorich: Dr. Lorich is the chief of the orthopaedic trauma service at NYP. This author made substantial contributions to the design of the work, planning of data analysis, drafting and revising of the protocol, final approval of the version to be published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy of the work.
b.) Sponsor contact information “Trial sponsor: Dr. Thomas P. Sculco Research Grant Sponsor’s reference: Contact name: Karla Felix Address: 535 E. 70th St. Telephone: 212 774 2717 Email: [email protected] “Trial sponsor: Dr. Joseph M. Lane Research Grant Sponsor’s reference: Contact name: Karla Felix Address: 535 E. 70th St. Telephone: 212 774 2717
Page 35 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
5
Email: [email protected] c.) Sponsor and funder: This funder has no role in the design of the study and will not have any role during its execution, analyses, interpretation of the data, or decision to submit results. d.) Committees As this is a single institution study, there is no steering committee other than the authors listed above. 6.) Background and rationale (page 3-6)
a.) Background and rationale: Hip fractures in the elderly remains a pressing public health issue in the United States given the aging population. 1 Hip fractures are associated with numerous adverse events and increased mortality up to one year after the event. 2-5 Elderly patients sustaining hip fractures commonly lose more than one liter of blood and up to 60% will require a blood transfusion. 6 A meta-analysis of 20 studies found a significantly increased risk of post-operative bacterial infection in patients who receive an allogenic blood transfusion in the perioperative period. 7 In addition to the increased risk of infection, patients who require blood transfusion following hip fracture have an increased hospital length of stay. 8 Beyond the risk to the patient from a blood transfusion, an allogenic blood transfusion in the United States was recently estimated to increase costs by $1,731 per admission. 9 Numerous anti-fibrinolytics have been used to limit bleeding in orthopaedic surgery and prevent the need for blood transfusion. 10-14 One of these anti-fibrinolytics, tranexamic acid (TXA) is a synthetic derivative of the amino acid lysine and acts as a competitive inhibitor in the activation of plasminogen to plasmin and therefore prevents the degradation of fibrin. As a result of the CRASH-2 trial15,16 that demonstrated reduced mortality in trauma patients administered TXA the World Health Organization (WHO) added it to the essential drugs list. Currently TXA is not routinely used in patients with hip fractures in the United States, despite its common use worldwide and proven efficacy in reducing blood loss. Numerous studies have investigated the safety and efficacy of TXA in patients undergoing elective orthopaedic surgery, including total joint replacement and spine surgery. 17-22 The consensus from this literature is overwhelmingly in favor of administration of TXA given the decrease in blood loss, transfusion rates, and cost. 23,24 Although few individual studies have found increased risk of thromboembolic events in groups
Page 36 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
6
receiving TXA, 25,26 larger studies and meta-analyses have uniformly found no increased risk of thrombosis.27,28 Patients who suffer hip fractures frequently have multiple comorbidities making them more susceptible to adverse events from blood loss. 19,20 The most common comorbidities of individuals with hip fractures are congestive heart failure, chronic pulmonary disease and diabetes. 1 Administering TXA to such patients has a potential to offset blood loss, improve patient outcome and lower cost by decreasing the rate of transfusions. 29,30 Five studies, all conducted outside the United States, have reported results of using TXA in hip fracture surgery. 26,31-33 Sadeghi et al34 randomized 67 hip fracture patients to receive either placebo injection or intravenous tranexamic acid at the time of surgery. They found a significantly lower volume of blood loss (652 ± 228 mL vs. 1108 ± 372 mL, P < 0.003) and shorter hospital stays (4.3 ± 1.6 days vs. 5.8 ± 1.5 days, p< 0.05). Vijay et al. 33 also reported significantly reduced transfusion rates in the TXA arm of their clinical trial. In a retrospective cohort study, Lee et al31 reported similar results, a transfusion rate three times lower in patients who received TXA prior to hemiarthroplasty surgery. In a separate randomized controlled trial that compared intravenous administration of TXA to topical TXA administration as well as placebo in hip fracture patients undergoing hemiarthroplasty, both of the TXA groups experienced less blood loss. 26 While this study found a significant reduction in blood loss and transfusion rates in both TXA groups, they found a higher incidence of thromboembolic events in the intravenous TXA group. Of the five studies investigating the use of TXA in hip fracture patients, four were randomized controlled trials that were underpowered for detecting significant differences in thromboembolic events (Table 1). Furthermore, patients were only followed perioperatively, and differences in six-month and one-year mortality rates and late-onset complications were not assessed.
In designing this study, we concluded that hip fracture patients are both likely to experience significant blood loss and are susceptible to the adverse effects of blood loss making them an ideal population to target for a randomized controlled trial of the effects of perioperative TXA on blood loss.
b.) Choice of comparators The choice of intravenous saline as a control in this study is to replicate the standard of care at this time in the United States, which is no drug intervention for preventing blood loss in hip fracture surgery.
Page 37 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
7
7.) Objective (line 158-160)
Hypothesis: We hypothesize that administration of TXA will decrease blood loss in hip fracture patients and lower the rate of allogenic blood transfusion.
Objective To investigate the hypothesis that TXA will lower blood loss and transfusion rate in patients with hip fractures.
8.) Trial Design (line 164-181) This trial is designed as a stratified randomized, placebo-controlled, surgeon and patient blinded single-institution trial with four parallel groups and a primary endpoint of blood transfusion in the immediate postoperative hospitalization following hip fracture surgery. Randomization will be performed as block randomization with 1:1 allocation for both the intracapsular and the extracapsular hip fracture groups. 9.) Study Setting (line 204-205) Adult (over 18 years of age) patients presenting to a single urban tertiary care center in with a hip fracture. All patients with hip fractures at this institution are admitted to the medical orthopaedic trauma service (MOTS) after presenting through the emergency room. 10.) Eligibility criteria (line 222-246)
Inclusion criteria Patients admitted through the emergency room or transferred into our institution and who meet the following criteria will be included in the study:
Adults over the age of 18 Intertrochanteric or femoral neck hip fracture Patients treated surgically with cephalomedullary nail or hemiarthroplasty
Exclusion criteria Patient who meet any one or more of the following criteria will be excluded from the study:
Preoperative use of anticoagulant (clopidogrel, enoxaparin, warfarin, argatroban, rivaroxaban, fondaparinux)
Documented allergy to tranexamic acid History of deep vein thrombosis or pulmonary embolus Hepatic dysfunction (AST/ALT > 60)
Page 38 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
8
Renal dysfunction (Cr >1.5 of GRR > 30) Active coronary artery disease (event in the past 12 months), history of
cerebrovascular accident (CVA) in the past 12 months, or presence of a drug-eluting stent
Color blindness Leukemia or any active cancer Coagulopathy (INR> 1.4, PTT > 1.4x normal, Platelets < 100,000) Non-displaced femoral neck fractures treated percutaneously
11.) Interventions (line 267-301)
a.) Interventions The patients randomized to the treatment arm will receive 1 gram of intravenous tranexamic acid infused at the time of surgical incision. Those assigned to the placebo group will receive an infusion of saline at the time of surgical incision. Patients with intertrochanteric hip fractures will be treated with a long, intramedullary hip screw implant with a trochanteric start point. Patients with displaced femoral neck fractures will be treated with a cemented or non-cemented hemiarthroplasty or total hip arthroplasty at the discretion of the treating surgeon. Blood transfusion criteria will remain consistent with hospital standards (Hb<8 g/dL or symptomatic anemia) as determined by an independent, blinded medical team who will follow the patient throughout the hospital stay and number of blood transfusions received will be documented upon patient discharge. Hematocrit and hemoglobin will be recorded in all patients while they are in the hospital, for a minimum of 2 days postoperatively. Further monitoring will be conducted based on need as determined by the independent medical team. Estimated blood volume will be calculated from these values and used to estimate blood loss (Appendix 1 All patients will be permitted to weight-bear as tolerated post-operatively and deep vein thrombosis (DVT) prophylaxis will be standardized. All enrolled patients will receive subcutaneous heparin, 5000 units every 8 hours beginning upon admission until 12 hours prior to surgery and restarting 6 hours after surgery. Calf mechanical compression devices will also be utilized during the inpatient stay and will remain on at all times with the exception of physical therapy sessions. Following discharge from the hospital patients will be given aspirin 325 mg twice daily for DVT prophylaxis for a total of 6 weeks. Diagnostic studies to assess for thromboembolic events (i.e. DVT, pulmonary embolism, and stroke) will be ordered only if the patient develops clinical signs or symptoms that justify their use.
Page 39 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
9
b.) Modifications As the administration of TXA or placebo will occur at one time point in the operating room at the time of skin incision, there will be no criteria for modifying or discontinuing the treatment allocation following surgery. If a patient becomes unstable, experiences a sudden change in vital signs, drop in blood pressure or increase in heart rate, during the admission of the drug, the drug will be discontinued at that time. The patient will still be analyzed on an intention-to-treat basis. c.) Adherence We do not anticipate adherence as an issue since the administration of the intervention will be performed by the anesthesiologist at the time of skin incision. d.) Concomitant care No concomitant interventions will be permitted during the trial.
12.) Outcomes (line 241-275) Primary Outcome The primary outcome of the study will be the rate of blood transfusion in the postoperative period until time of discharge. Patients will be monitored with serial hemoglobin and hematocrit measurements and their vital signs will be recorded as per the standard of care to determine the need for blood transfusion. Secondary Outcome The secondary study outcomes include the calculated blood loss (calculated based on validated methods as outlined in Appendix 1), frequency of adverse events (including transfusion reaction, myocardial infarction, deep vein thrombosis, pulmonary embolus, cerebrovascular accident, re-operation, re-admission, infection, and death).
13.) Participation timeline (Figure 1)
Page 40 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
10
Figure 1: Study Design (TXA: tranexamic acid; PRBC: packed red blood cells) 14.) Sample size consideration (line 335-348) The transfusion rate amongst patients with hip fractures is between 6-60%.8-11,35
Our institutional transfusion rate was calculated based on a random sample of 60
patients and was 65% for extracapsular hip fractures and 35% for intracapsular hip
fractures, and an overall transfusion rate of 49%. The average reduction in
transfusion rate in the previous 5 studies using TXA was 20%.8-11,35 We plan to
include a total of 338 patients, 146 intracapsular hip fractures and 192
Page 41 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
11
extracapsular hip fractures. This study design will achieve 81% power to detect a
reduction in blood transfusion from 65% in the placebo control group to 45% in the
tranexamic acid group with statistical significance set to alpha equal to 0.05 for the
extracapsular hip fracture group. Similarly the study will achieve 81% power to
detect a reduction in blood transfusion from 35% in the placebo control group to
15% in the tranexamic acid group with statistical significance set to alpha equal to
0.05 for the intracapsular hip fracture group.
15.) Recruitment (line 203-218) Adult (over 18 years of age) patients presenting to a single tertiary care center with a hip fracture. All patients with hip fractures at this institution are admitted to the medical orthopaedic trauma service (MOTS). Prior to surgery, patients older than 75 years of age, or those with medical comorbidities will be optimized by the general medical service prior to surgery. All potentially eligible patients will be screened and documented as (1) eligible and included, (2) eligible and missed, or (3) excluded. The study coordinator will obtain informed consent for participation in the study using the approved IRB Informed Consent forms. All patients will provide written informed consent and will understand that by entering in the study they may receive placebo and not tranexamic acid. Participation in the study is voluntary and their decision to participate will not affect any other aspect of their care in case of refusal. Patients will have the right to withdraw from the study at any point. 16.) Allocation (lines 257-265) a.)Sequence generation
After the patient consents and is enrolled in the study, the institution’s investigational pharmacist will assign the patient to either receive TXA or placebo via computer generated randomization. Patients will be randomized in blocks of 20. b.)Concealment The packaging of the injections will be performed by the investigational pharmacy and will be identical for both TXA and placebo. All clinicians, except for the pharmacist, will remain blinded until the data is analyzed.
Page 42 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
12
c.)Implementation After the patient consents and is enrolled in the study, the institution’s investigational pharmacist will perform the randomization and assign the patient to either receive TXA or placebo. Patients will be randomized in blocks of 20. The packaging of the injections will be performed by the investigational pharmacy and will be identical for both TXA and placebo. All clinicians, except for the pharmacist, will remain blinded until the data is analyzed. 17.) Blinding (lines 257-265) a.) Masking The patient, the surgeon, the anesthesiologist and the hospitalist will all be blinded to the assignment of intervention. Therefore, the decision to transfuse a patient will be made independent of the intervention. b.)Emergency unblinding Unblinding of intervention assignment will only be allowed in exceptional circumstances if knowlegde of treatment is crucial to further management of the patient. An example of this is if a patient becomes unstable during drug administration in the operating room. The allocation will not be disclosed to the surgeon or the patient or other study personnel who are not directly treating the patient at that time. All code breaks will be reported and documented. 18.) Methods (line 248-255) a.) Data collection methods Baseline assessment includes sex, birth date, height and weight, mechanism of injury, time from injury to presentation to the emergency room, American Society of Anesthesiologists (ASA) classification, Charlson Comorbidity Index, comorbidities including diabetes, peripheral vascular disease, dementia, hypertension, and history of smoking. The hemoglobin and hematocrit will be recorded at the time of admission and on the morning of surgery, if applicable. Blood transfusion criteria will remain consistent with hospital standards (Hb<8 g/dL or symptomatic anemia) as determined by an independent, blinded medical team who will follow the patient throughout the hospital stay and number of blood transfusions received will be documented upon patient discharge. Hematocrit and hemoglobin will be recorded in all patients while they are in the hospital, for a minimum of 2 days postoperatively. Further monitoring will be conducted based on need as determined by the independent medical team. Estimated blood volume will be calculated from these values and used to estimate blood loss. After discharge, patients will undergo routine follow-up at 2wk, 6wk, 3mo, 6mo and 1 yr after surgery. Each will be questioned regarding possible adverse events that
Page 43 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
13
may have occurred since their previous visit. Further, electronic inpatient records will be reviewed at the 1 year follow-up appointment to determine if any undocumented adverse events may have occurred and patients will also be called at that time if they fail to attend their 1 year follow-up appointment. 19.) Data Management All data will be entered electronically into a Microsoft Excel database that will be password protected on an institutional computer. Any identifying health information will be removed or, if needed, coded when data is summarized in a spreadsheet format for statistical analysis purposes. 20.) Statistical Analysis (lines 351-370) a.) Outcomes Descriptive analyses of the patient population will include reporting means (with standard deviations) for continuous variables and frequencies (with percentages) for categorical or discrete variables. Following the descriptive analysis, a chi-square analysis will be conducted to evaluate the superiority of tranexamic acid in reducing the rate of transfusion versus the placebo control group. The analysis and reporting of the results of the clinical outcomes will follow the CONSORT guidelines (www.consort-statement.org). We will conduct a multiple logistic regression model to determine if type of fracture (intertrochanteric or femoral neck), comorbidities, Charlson comorbidity index, age, time to surgery, and mechanism of injury are related to transfusion administration. Similarly we will conduct a multiple linear regression model to determine if patient comorbidities, age, time to surgery, and mechanism of injury are related to blood loss. We will also conduct subgroup analyses to determine if the effect of TXA is modified by fracture type (intertrochanteric or femoral neck). All analyses will be performed using Stata 14.0 software (Stata Corporation, College Station, TX, USA). b.)Additional analyses Our a priori hypothesis, based on retrospective data, 6 is that patients with intertrochanteric fractures incur more blood loss than femoral neck fractures and will have a higher rate of transfusion. If these subgroup analyses are underpowered, the subgroup data will be used to generate further hypotheses to be tested in the future.
c.)Analysis population and missing data
Not applicable- as there will largely be no compliance breakdowns given that the intervention is a one-time administration of a drug during a surgical procedure.
Page 44 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
14
Should a patient consent and be enrolled in the trial and decide to unenroll prior to drug administration they will not be taken into account for the analysis. In the event of missing data, ie missing hemoglobin levels postoperatively, we do not plan on using an imputing method but rather analyzing only the data collected given that these missing data points will likely be randomly arranged throughout the study. 21.) Methods: Monitoring (lines 372-375) a.)Formal Committee The data safety monitoring board (DSMB) has been established to monitor the trial and renew the study biannually. This board is independent of the trial and free of conflicts with any of the investigation team. b.)Interim analysis Data will be analyzed every six months throughout the study by the study investigators.
22.) Harms (lines 312-334)
The secondary outcomes of this study including adverse outcomes and events. These events will be monitored for after the subject has provided consent and has been enrolled in the study. If a subject experiences an adverse event after the informed consent document is signed (entry) but the subject has not yet received the intervention in the operating room, the event will be reported as not related to study drug. Adverse events during hospitalization will be recorded and patients will be asked about adverse events during their follow-up appointments. Adverse events will be reported to the DSMB as well.
23.) Auditing (lines 372-375)
The data safety monitoring board (DSMB) has been established to monitor the trial and renew the study biannually. This board is independent of the trial and free of conflicts with any of the investigation team.
24.) Research ethics approval (lines 77-80)
The protocol and site specific consent forms have been approved by our institutional review board (IRB) with respect to scientific content and compliance with applicable research and human subjects regulations.
Page 45 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
15
25.) Protocol amendments
See attached.
26.) Consent or assent (lines 214-218)
a.) Consent
Informed consent will be obtained by research associated personnel at the time of patient presentation. Written consent will be obtained from the patient when possible, or from the health care proxy if the patient is unable to consent for themselves.
Each patient will be provided the written informed consent form to read and will have the opportunity to ask any questions related to the research protocol/methods to the researcher obtaining consent.
b.)Ancillary studies
not applicable
27.) Confidentiality
Data is only recorded electronically and will be kept in the Principal Investigator’s locked office on a password-protected computer. Only research personnel will have access to electronic files kept in the PIs locked office, and only research personnel will know the password needed to access research files. Patients will be numbered sequentially on the data collection sheet. Numbers will be associated with names and medical records, which will be stored in a separate file by the research coordinator.
28.) Declaration of interests
None of the authors of the study or study personnel have any financial relationships
related to the nature of the study.
29.) Access to data
n/a – single institution study
30.) Ancillary and post-trial care (lines 436)
n/a- this is a privately funded study with no study-specific insurance policy.
Page 46 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
16
31.) Dissemination policy
a.) Trial results
The results from the trial will be reviewed by the authors and following editing from each member a manuscript will be prepared for publication in a peer reviewed journal. b.)Authorship
The authors currently listed will be included as authors on the final manuscript submitted for publication according to their maintained involvement. New authors will be required by meet guidelines for authorship as stated previously. c.)Reproducible research
n/a
32.) Informed consent material
see attached
33.) Biological specimens
n/a
References
1. Brauer CA, Coca-Perraillon M, Cutler DM, Rosen AB. Incidence and mortality of hip
fractures in the united states. JAMA. 2009;302(14):1573-1579.
2. Richmond J, Aharonoff GB, Zuckerman JD, Koval KJ. Mortality risk after hip
fracture. J Orthop Trauma. 2003;17(1):53-56.
3. Heyes GJ, Tucker A, Marley D, Foster A. Predictors for 1-year mortality following
hip fracture: A retrospective review of 465 consecutive patients. Eur J Trauma
Emerg Surg. 2015.
Page 47 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
17
4. Shah MR, Aharonoff GB, Wolinsky P, Zuckerman JD, Koval KJ. Outcome after hip
fracture in individuals ninety years of age and older. J Orthop Trauma.
2001;15(1):34-39.
5. Sathiyakumar V, Greenberg SE, Molina CS, Thakore RV, Obremskey WT, Sethi MK.
Hip fractures are risky business: An analysis of the NSQIP data. Injury.
2015;46(4):703-708.
6. Foss NB, Kehlet H. Hidden blood loss after surgery for hip fracture. J Bone Joint
Surg Br. 2006;88(8):1053-1059.
7. Hill GE, Frawley WH, Griffith KE, Forestner JE, Minei JP. Allogeneic blood
transfusion increases the risk of postoperative bacterial infection: A meta-analysis. J
Trauma. 2003;54(5):908-914.
8. Shokoohi A, Stanworth S, Mistry D, Lamb S, Staves J, Murphy MF. The risks of red
cell transfusion for hip fracture surgery in the elderly. Vox Sang. 2012;103(3):223-
230.
9. Saleh A, Small T, Chandran Pillai AL, Schiltz NK, Klika AK, Barsoum WK. Allogenic
blood transfusion following total hip arthroplasty: Results from the nationwide
inpatient sample, 2000 to 2009. J Bone Joint Surg Am. 2014;96(18):e155.
10. Kagoma YK, Crowther MA, Douketis J, Bhandari M, Eikelboom J, Lim W. Use of
antifibrinolytic therapy to reduce transfusion in patients undergoing orthopedic
Page 48 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
18
surgery: A systematic review of randomized trials. Thromb Res. 2009;123(5):687-
696.
11. Eubanks JD. Antifibrinolytics in major orthopaedic surgery. J Am Acad Orthop
Surg. 2010;18(3):132-138.
12. Yuan C, Zhang H, He S. Efficacy and safety of using antifibrinolytic agents in spine
surgery: A meta-analysis. PLoS One. 2013;8(11):e82063.
13. Zufferey P, Merquiol F, Laporte S, et al. Do antifibrinolytics reduce allogeneic
blood transfusion in orthopedic surgery? Anesthesiology. 2006;105(5):1034-1046.
14. Tse EY, Cheung WY, Ng KF, Luk KD. Reducing perioperative blood loss and
allogeneic blood transfusion in patients undergoing major spine surgery. J Bone Joint
Surg Am. 2011;93(13):1268-1277.
15. CRASH-2 trial collaborators, Shakur H, Roberts I, et al. Effects of tranexamic acid
on death, vascular occlusive events, and blood transfusion in trauma patients with
significant haemorrhage (CRASH-2): A randomised, placebo-controlled trial. Lancet.
2010;376(9734):23-32.
16. CRASH-2 collaborators, Roberts I, Shakur H, et al. The importance of early
treatment with tranexamic acid in bleeding trauma patients: An exploratory
analysis of the CRASH-2 randomised controlled trial. Lancet. 2011;377(9771):1096-
101, 1101.e1-2.
Page 49 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
19
17. Whiting DR, Gillette BP, Duncan C, Smith H, Pagnano MW, Sierra RJ. Preliminary
results suggest tranexamic acid is safe and effective in arthroplasty patients with
severe comorbidities. Clin Orthop Relat Res. 2014;472(1):66-72.
18. Cid J, Lozano M. Tranexamic acid reduces allogeneic red cell transfusions in
patients undergoing total knee arthroplasty: Results of a meta-analysis of
randomized controlled trials. Transfusion. 2005;45(8):1302-1307.
19. Lemay E, Guay J, Cote C, Roy A. Tranexamic acid reduces the need for allogenic
red blood cell transfusions in patients undergoing total hip replacement. Can J
Anaesth. 2004;51(1):31-37.
20. Poeran J, Rasul R, Suzuki S, et al. Tranexamic acid use and postoperative
outcomes in patients undergoing total hip or knee arthroplasty in the united states:
Retrospective analysis of effectiveness and safety. BMJ. 2014;349:g4829.
21. Raksakietisak M, Sathitkarnmanee B, Srisaen P, et al. Two doses of tranexamic
acid reduce blood transfusion in complex spine surgery: A prospective randomized
study. Spine (Phila Pa 1976). 2015.
22. Wind TC, Barfield WR, Moskal JT. The effect of tranexamic acid on transfusion
rate in primary total hip arthroplasty. J Arthroplasty. 2014;29(2):387-389.
23. Tuttle JR, Ritterman SA, Cassidy DB, Anazonwu WA, Froehlich JA, Rubin LE. Cost
benefit analysis of topical tranexamic acid in primary total hip and knee
arthroplasty. J Arthroplasty. 2014;29(8):1512-1515.
Page 50 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
20
24. Huang F, Wu D, Ma G, Yin Z, Wang Q. The use of tranexamic acid to reduce blood
loss and transfusion in major orthopedic surgery: A meta-analysis. J Surg Res.
2014;186(1):318-327.
25. Nishihara S, Hamada M. Does tranexamic acid alter the risk of thromboembolism
after total hip arthroplasty in the absence of routine chemical thromboprophylaxis?
Bone Joint J. 2015;97-B(4):458-462.
26. Emara WM, Moez KK, Elkhouly AH. Topical versus intravenous tranexamic acid
as a blood conservation intervention for reduction of post-operative bleeding in
hemiarthroplasty. Anesth Essays Res. 2014;8(1):48-53.
27. Duncan CM, Gillette BP, Jacob AK, Sierra RJ, Sanchez-Sotelo J, Smith HM. Venous
thromboembolism and mortality associated with tranexamic acid use during total
hip and knee arthroplasty. J Arthroplasty. 2015;30(2):272-276.
28. Yang ZG, Chen WP, Wu LD. Effectiveness and safety of tranexamic acid in
reducing blood loss in total knee arthroplasty: A meta-analysis. J Bone Joint Surg Am.
2012;94(13):1153-1159.
29. Foss NB, Kristensen MT, Kehlet H. Anaemia impedes functional mobility after hip
fracture surgery. Age Ageing. 2008;37(2):173-178.
30. Lawrence VA, Silverstein JH, Cornell JE, Pederson T, Noveck H, Carson JL. Higher
hb level is associated with better early functional recovery after hip fracture repair.
Transfusion. 2003;43(12):1717-1722.
Page 51 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
21
31. Lee C, Freeman R, Edmondson M, Rogers BA. The efficacy of tranexamic acid in
hip hemiarthroplasty surgery: An observational cohort study. Injury.
2015;46(10):1978-1982.
32. Zufferey PJ, Miquet M, Quenet S, et al. Tranexamic acid in hip fracture surgery: A
randomized controlled trial. Br J Anaesth. 2010;104(1):23-30.
33. Vijay BS, Bedi V, Mitra S, Das B. Role of tranexamic acid in reducing
postoperative blood loss and transfusion requirement in patients undergoing hip
and femoral surgeries. Saudi J Anaesth. 2013;7(1):29-32.
34. Sadeghi M MA. Does a single bolus dose of tranexamic acid reduce blood loss and
transfusion requirements during hip fracture surgery? A prospective randomized
double blind study in 67 patients. Acta Medica Iranica. 2007;45(6):437-442.
Appendix
Blood Loss Calculation:Patient’s Blood Volume (PBV) = (k1 x Height3
(m)) + (k2 x Weight (kg)) + k3
k1 = 0.3669, k2 = 0.03219, and k3 = 0.6041 for men k1 = 0.3561, k2=0.03308, and k3 = 0.1833 for women
Multiplying the PBV by the hematocrit (Hct) gives the red blood cell (RBC) volume. As
such, a change in the RBC volume can be calculated from a change in the Hct level as
follows:
Pre-op RBC volume loss = PBV x (Admit Hct – Day of surgery Hct) Operative RBC volume loss = PBV x (Day of surgery Hct – PACU Hct)
If a patient requires a pre-op or intraoperative transfusion, the calculation will be adjusted as follows:
Pre-op RBC volume loss = [PBV x (Admit Hct – Day of surgery Hct)]+ (No. of Units Transfused x 0.285) / (Admit Hct – Day of surgery Hct) / 2)Operative RBC volume loss = [PBV x (Day of surgery
Page 52 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from

For peer review only
22
Hct – PACU Hct)] +)]+ (No. of Units Transfused x 0.285) / (Day of surgery Hct – Post-op Hct) / 2
Page 53 of 53
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 26 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010676 on 21 June 2016. Dow
nloaded from





























