Embed Size (px)
Citation preview

Full Terms & Conditions of access and use can be found athttp://www.tandfonline.com/action/journalInformation?journalCode=ijmh20
Journal of Mental Health
ISSN: 0963-8237 (Print) 1360-0567 (Online) Journal homepage: http://www.tandfonline.com/loi/ijmh20
Training and post-disaster interventions forthe psychological impacts on disaster-exposedemployees: a systematic review
Samantha K. Brooks, Rebecca Dunn, Richard Amlôt, Neil Greenberg & G.James Rubin
To cite this article: Samantha K. Brooks, Rebecca Dunn, Richard Amlôt, Neil Greenberg& G. James Rubin (2018): Training and post-disaster interventions for the psychologicalimpacts on disaster-exposed employees: a systematic review, Journal of Mental Health, DOI:10.1080/09638237.2018.1437610
To link to this article: https://doi.org/10.1080/09638237.2018.1437610
Published online: 15 Feb 2018.
Submit your article to this journal
View related articles
View Crossmark data

http://tandfonline.com/ijmhISSN: 0963-8237 (print), 1360-0567 (electronic)
J Ment Health, Early Online: 1–25� 2018 Informa UK Limited, trading as Taylor & Francis Group. DOI: 10.1080/09638237.2018.1437610
REVIEW ARTICLE
Training and post-disaster interventions for the psychological impactson disaster-exposed employees: a systematic review
Samantha K. Brooks1 , Rebecca Dunn1, Richard Amlot2 , Neil Greenberg1* , and G. James Rubin1*
1Department of Psychological Medicine, King’s College London, London, UK, and 2Emergency Response Department Science and Technology,
Health Protection Directorate, Public Health England, Salisbury, UK
Abstract
Background: When organisations are exposed to traumatic situations, such as disasters, oftenstaff are not prepared for the potential psychological impact which can negatively affect theirwellbeing.Aims: To conduct a systematic review of the literature on psychological interventions aimed atimproving staff wellbeing during or after disasters.Method: Four electronic literature databases were searched. Reference lists of relevant articleswere hand-searched.Results: Fifteen articles were included. Five studies suggested that pre-disaster skills trainingand disaster education can improve employee confidence. Ten studies on post-disasterinterventions revealed mixed findings on the effectiveness of psychological debriefing andlimited evidence for cognitive behavioural therapy, psychoeducation and meditation.Conclusions: Pre-disaster training and education can improve employees’ confidence in theirability to cope with disasters. The routine use of post-disaster psychological debriefings is notsupported; further research is needed to determine if debriefing interventions could be usefulin some circumstances. Further research is needed to provide more evidence on the potentialpositive effects of cognitive behavioural therapy, psychoeducation and meditation. Moreexperimental studies on psychological disaster interventions are needed.
Keywords
Disasters, interventions, wellbeing, work
History
Received 3 August 2017Revised 15 November 2017Accepted 18 January 2018Published online 13 February 2018
Introduction
Disasters and traumatic events are occurring more often
across the world (Guha-Sapir et al., 2013), with earthquakes,
hurricanes, floods, explosions and terrorist attacks affecting
increasingly large numbers of people. Many people who are
exposed to trauma are exposed as part of an occupational
group: for example a commercial organisation targeted by
terrorists or healthcare workers who assist with the emergency
response.
There has been much research on the prevalence of
psychological disorders – such as post-traumatic stress
disorder (PTSD), depression, anxiety, and alcohol misuse –
in employees following disaster exposure. For example a
review by Strohmeier & Scholte (2015) revealed high levels
of trauma-related psychological problems in humanitarian
workers, and research has demonstrated a risk of mental
health problems in frequently trauma-exposed employees,
such as fire-fighters (Chang et al., 2005) and police (West
et al., 2008). A number of recent reviews exploring organ-
isational responses to disasters (Brooks et al., 2015, 2016,
2017) have identified factors affecting the development of
psychological disorders in occupational groups, suggesting
that the extent of traumatic exposure, lack of social support,
lack of preparedness and greater impact of the disaster on
one’s personal and professional life may all be associated with
poor psychological outcomes. These factors appear to be
important in determining wellbeing regardless of occupation –
the same factors were identified in a study of rescue workers,
who are involved in disaster recovery as part of their role
(Brooks et al., 2015), and in other occupational groups who
would not expect to be exposed to trauma (Brooks et al.,
2017).
While the prevalence of psychological problems post-
disaster and factors affecting psychological wellbeing after a
traumatic incident have been explored, there is less evidence
regarding how to support trauma-exposed staff, and what kind
of interventions might be successful in reducing the distress
experienced during and after disasters.
Groups who are routinely exposed to traumatic situations
as part of their everyday work – such as rescue workers, the
military and emergency services personnel – are likely to have
some employee support systems in place and to be prepared to
support their staff or colleagues after being exposed to
trauma. For example a recent article (Dunn et al., 2015)
suggested that preparatory mental health briefings at the start
*These authors contributed equally to this work.
Correspondence: Samantha K. Brooks Department of PsychologicalMedicine, King’s College London, London, UK. E-mail:[email protected]

of their role, monitoring of employees’ wellbeing and
informal support, such as trauma risk management (TRiM;
Greenberg et al., 2008) or psychological first aid (PFA;
Pekevski, 2012) could enable staff to better support their
colleagues. However, as Dunn et al. noted, there has been
little evidence on how to best support trauma-exposed
employees, and it is unclear how many organisations apply
evidence to their practice. Often some form of psychological
debriefing, or ‘‘Critical Incident Stress Debriefing’’
(Mitchell, 1983), occurs. This differs from the structured
debriefing often offered in workplaces which typically take
the form of ‘‘after action reviews’’ and review performance
rather than wellbeing, in that psychological debriefing is
designed specifically to prevent the development of post-
traumatic stress and similar symptoms, is conducted by
mental health professionals, and offers a structured approach
for employees to discuss their emotions (Mitchell, 1983).
There has been mixed evidence on the effectiveness of this
kind of intervention, with research suggesting that debriefing
is unhelpful and can even have negative consequences
(Wessely et al., 2000). This has led the National Institute
for Health and Care Excellence (NICE) to suggest that
individual debriefing sessions focusing on the trauma experi-
ence should not be part of routine practice (NICE, 2005).
The aim of this article was to review the evidence on
effective interventions to support employees during or after
traumatic incident such as a disaster. We explored: (1) Can
pre-disaster training equip employees with better coping skills
if a disaster were to occur? (2) What kinds of post-disaster
interventions have been evaluated? (3) To what extent do pre-
disaster and post-disaster interventions protect the wellbeing
of employees and promote resilience?
Method
Search strategy
This study forms part of a wider review on the psychological
impact of disasters on employees (Brooks et al., 2015, 2016,
2017): our previous publications emerging from this review
focus on the factors affecting the psychological wellbeing of
disaster-exposed employees, and the data on interventions has
until now not been reviewed. One large, broad search was
used to locate articles for each strand of the study. This
combined three smaller searches. Search 1 included psycho-
logical terms, such as ‘‘wellbeing’’ and ‘‘PTSD’’. Search 2
included terms relating to extreme events, and was informed
by the emergency events database (Centre for Research on the
Epidemiology of Disasters, 2009). Search 3 included terms
relating to occupational groups, such as ‘‘employees’’ and
‘‘organisation’’. The full search strategy can be seen in
Appendix I.
One author (SKB) ran the searches on MEDLINE�,
Embase, PsycINFO� and Web of Science. Resulting citations
were downloaded to EndNote� software version X7
(EndNote, Philadelphia, PA), where duplicate items were
immediately removed. SKB then evaluated titles for relevance
and removed any clearly not relevant to the review. Next, two
authors (SKB, RD) used the inclusion criteria to screen
abstracts of the remaining citations and then finally to screen
full texts. Reference lists of all remaining articles were then
hand-searched for any additional, relevant studies: if our
included articles contained any citations which appeared to be
relevant and had not been found through our search, we
looked up these papers and assessed their relevance by
abstract and then by full-text.
Inclusion criteria
Articles were eligible for inclusion if they:
� Were written in English.
� Were published in peer-reviewed journals.
� Included employed participants (any occupational group;
any group of people that work together within a
hierarchical system to achieve some sense of group aim).
� Involved a ‘‘disaster’’ or potential disaster – we took an
inclusive approach to the definition of ‘‘disaster’’ and
largely relied on authors’ own assessment of whether to
categorise the incident in this way or not.
� Involved any form of psychological intervention designed
to help employees in any occupational group cope either
during or after a disaster.
� Was published post-1984 (30 years before the start of our
study in 2014 – reducing the risk of including research
conducted before post-traumatic stress disorder was
introduced as a diagnostic category in the DSM-III-R
(American Psychiatric Association, 1980)).
Data extraction and synthesis
We designed spreadsheets with the following headings: first
author; publication year; country of study; disaster; primary
aim; design; occupation of participants; participant demo-
graphics; details of intervention; outcomes measured; instru-
ments used; key results; conclusions; and limitations. These
data were extracted by two authors (SKB, RD) from all
studies which remained after the full-text screening.
During the data extraction, it became clear that due to the
varying types of interventions, instruments used and out-
comes measured, meta-analysis would not be possible.
Instead, we extracted all relevant outcomes, grouped articles
into pre-disaster and post-disaster interventions, and grouped
articles with similar outcomes together where possible.
Quality appraisal
This study used a quality appraisal tool developed for a
previous review (Brooks et al., 2015) which had been
informed by existing quality appraisal tools (Drummond &
Jefferson, 1996; EPHPP, 2009; National Institute for Health,
2014). This tool assessed quality in three areas – study design,
data collection and methodology and analysis and interpret-
ation of results. The appraisal tool can be seen in Appendix II.
Results
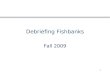
The initial search yielded 18 005 studies. One hundred and
seventy of these were relevant to the overall set of reviews on
the psychological impact of disasters on occupational groups,
and 15 were relevant for inclusion in this review. Details of
screening can be seen in Figure 1.
Seven studies were longitudinal, seven were cross-
sectional and one was a randomised controlled trial.
2 S. K. Brooks et al. J Ment Health, Early Online: 1–25

The disasters explored in the literature included earthquakes
(n¼ 3), the 11 September terrorist attacks in New York
(n¼ 3), potential pandemics (n¼ 2), hurricanes (n¼ 2) and
terrorism in general, a simulated submarine disaster, a rail
crash, a bank robbery and a bombing (each n¼ 1). A
summary of the characteristics of articles included in this
review is presented in Table 1, and more detailed description
of each study’s intervention is presented in Table 2.
Overall quality was mixed (see Figure 2). Studies typically
scored highly for design. Scores for data collection and
methodology were more mixed, with several articles not using
standardised measures and having participation rates of less
than 50%. Analysis and interpretation of results tended to be
the weakest areas; many did not use statistical tests or
consider confounding variables.
One-third of the relevant articles involved employees who
had not yet experienced a disaster and evaluated pre-disaster
training interventions designed to improve confidence and
ability to cope should an incident occur, while the remaining
two-third looked at interventions to improve wellbeing after a
disaster had occurred.
Pre-disaster
Summary of studies
Five studies involved pre-disaster interventions aimed at
improving preparedness and ability to cope with disasters. Of
these, two involved Canadian hospital workers preparing for a
potential influenza epidemic (Aiello et al., 2011; Maunder
et al., 2010), one involved Norwegian Navy sailors participat-
ing in a simulated submarine disaster (Eid et al., 2004), one
involved occupational health workers preparing for terrorist
attacks in the USA (Gershon et al., 2004) and one involved
Records iden�fied through database searching
n = 17,999
Addi�onal records iden�fied through hand searching
n = 6
Total records found n = 18,005
Duplicates removed n = 6183
Titles screened n = 11,822
Abstracts screened n = 3655
Studies relevant for this review n = 15
Full-text ar�cles assessed for eligibility
n = 571
Studies relevant for broader set of reviews
n = 170
Excluded a�er �tle screening n = 8167
Excluded a�er abstract screening n = 3084
Excluded a�er full-text screening
n = 401
Relevant for other reviews but not interven�on-
related n = 155
Figure 1. Screening process.
DOI: 10.1080/09638237.2018.1437610 Psychological disaster interventions 3

Tab
le1
.S
um
mar
yo
fp
aper
s.
Stu
dy
Co
un
try
Dis
aste
rD
esig
nP
arti
cip
ants
(n)
Ro
leo
fp
arti
cip
ants
Inte
rven
tio
nO
utc
om
esas
sess
edR
esu
lts
Aie
llo
etal
.(2
01
1)
Can
ada
Po
ten
tial
infl
u-
enza
pan
dem
icP
rean
dp
ost
-tra
inin
gsu
rvey
s1
25
0H
osp
ital
staf
fT
rain
ing
sess
ion
on
wh
atto
exp
ect
and
how
toco
pe.
Co
nfi
den
cein
abil
ity
tod
eal
wit
hp
an-
dem
icp
re-t
rain
-in
gan
db
elie
fth
ato
ne
wil
lb
eab
leto
cop
ed
uri
ng
ap
and
emic
po
st-
trai
nin
g;
asse
ssed
via
stu
dy-s
pec
ific
surv
ey.
On
ly3
4.9
%fe
ltco
nfi
den
tin
bei
ng
able
tod
eal
wit
hth
ep
and
emic
pre
-tr
ain
ing
;7
6.1
%fe
ltb
ette
rab
leto
cop
eas
are
sult
of
the
sess
ion
.8
7.5
%fo
un
dth
ese
ssio
n‘‘
use
ful’
’;9
1.3
%fo
un
dit
‘‘h
elp
ful
and
info
rmat
ive’
’an
d6
9.7
%fe
ltth
eyw
ere
pre
par
edfo
ra
pan
dem
icfo
l-lo
win
gth
ese
ssio
nB
osc
arin
oet
al.
(20
05
)U
SA
11
Sep
tem
ber
20
01
terr
ori
stat
tack
s.
Lo
ng
itu
din
al–
bas
elin
ed
ata
coll
ecte
d1
3–
15
mo
nth
sp
ost
-dis
aste
ran
dfo
llow
-up
dat
aco
llec
ted
24
mo
nth
sp
ost
-dis
aste
r.
16
81
Par
tici
pan
tsd
ivid
edin
tog
rou
ps
–n
ow
ork
site
sess
ion
atte
nd
ed(n¼
15
01
);o
ne
sess
ion
atte
nd
ed(n¼
82
);2
–3
sess
ion
sat
ten
ded
(n¼
68
)an
d4þ
sess
ion
sat
ten
ded
(n¼
30
).
Var
iou
sB
rief
emp
loyer
-pro
-v
ided
wo
rksi
tecr
isis
inte
rven
tio
ns.
Alc
oh
ol
abu
seas
sess
edb
yst
ud
y-s
pec
ific
qu
esti
on
san
dG
AG
Ecr
iter
ia;
sub
clin
ical
/par
tial
PT
SD
asse
ssed
by
mo
dif
ied
ver
sio
no
fP
TS
Dse
ctio
no
fN
IMH
-DIS
and
WH
Od
iag
-n
ost
icin
terv
iew
;d
epre
ssio
nas
sess
edb
yS
CID
’sd
epre
s-si
on
scal
e;p
sy-
chia
tric
syn
-d
rom
es(a
nx
iety
,so
mat
isat
ion
and
glo
bal
sever
ity
)as
sess
edb
yB
rief
Sy
mp
tom
Inven
tory
-18
.T
reat
men
tg
rou
ps
wer
eas
ked
tow
hat
exte
nt
ses-
sio
ns
hel
ped
them
dea
lw
ith
po
st-
dis
aste
rem
o-
tio
nal
pro
ble
ms
21
.2%
rep
ort
edth
ein
terv
enti
on
hel
ped
alo
t;2
2.8
%sa
idit
hel
ped
som
e;3
3.7
%sa
idit
hel
ped
ali
ttle
and
22
.4%
fou
nd
itn
ot
atal
lh
elp
ful.
Bet
wee
n1
and
3se
ssio
ns
app
eare
dto
be
effe
ctiv
ein
pro
tect
ing
wo
rk-
ers
fro
mb
inge
dri
nk
ing
(OR¼
0.2
6,
p5
0.0
5)
and
alco
ho
ld
epen
d-
ence
(OR¼
0.0
9,
p5
0.0
5).
2–
3se
ssio
ns
wer
ep
rote
ctiv
efo
rP
TS
D(O
R¼
0.3
6,
p5
0.0
5),
dep
res-
sio
n(O
R¼
0.2
3,
p5
0.0
5),
som
a-ti
sati
on
(OR¼
0.3
6,
p5
0.0
5),
anx
iety
(co
nti
nu
ed)
4 S. K. Brooks et al. J Ment Health, Early Online: 1–25

Stu
dy
Co
un
try
Dis
aste
rD
esig
nP
arti
cip
ants
(n)
Ro
leo
fp
arti
cip
ants
Inte
rven
tio
nO
utc
om
esas
sess
edR
esu
lts
usi
ng
ast
ud
y-
spec
ific
scal
e.(O
R¼
0.1
7,
p5
0.0
1)
and
glo
bal
sever
ity
(OR¼
0.3
0,
p5
0.0
5)
Bo
scar
ino
etal
.(2
00
6)
US
A1
1S
epte
mb
er2
00
1te
rro
rist
atta
cks
Lo
ng
itu
din
al–
bas
elin
ed
ata
coll
ecte
d1
3–
15
mo
nth
sp
ost
-dis
aste
ran
dfo
llow
-up
dat
aco
llec
ted
24
mo
nth
sp
ost
-dis
aste
r.
11
21
Var
iou
sB
rief
emp
loyer
-pro
-v
ided
wo
rksi
tecr
isis
inte
rven
tio
ns.
As
above
Un
adju
sted
ou
t-co
mes
wer
egen
-er
ally
bet
ter
for
inte
rven
tio
ns
case
sfo
ral
lo
ut-
com
esw
ith
exce
pti
on
of
PT
SD
.A
fter
1:5
mat
chin
g,
wo
rk-
ers
wit
hem
plo
yer
inte
rven
tio
ns
had
less
sever
eP
TS
Dsy
mp
tom
s(�
0.8
)b
ut
no
dif
fere
nce
was
fou
nd
inP
TS
Dp
reval
ence
inp
ast
yea
r.P
rop
ensi
tysc
ore
resu
lts
bas
edo
n1
:5m
atch
ing
-in
terv
enti
on
wo
rker
sh
adb
ette
ro
utc
om
esat
foll
ow
-up
for
dep
ress
ion
(�2
.7%
,p5
0.0
5)
and
alco
ho
ld
epen
den
ce(�
4.8
%,
p5
0.0
1)
inp
ast
yea
ran
dre
du
ced
PT
SD
(�0
.8,
p5
0.0
5),
dep
ress
ion
and
anx
iety
sym
p-
tom
s(�
1.7
,p5
0.0
5)
inp
ast
mo
nth
Dif
ede
etal
.(2
00
7)
US
A1
1S
epte
mb
er2
00
1te
rro
rist
atta
cks
Ran
do
mis
edco
ntr
oll
edtr
ial
21
(7in
CB
Tin
terv
en-
tio
ng
rou
p,
14
intr
eatm
ent
asu
sual
(TA
U)
gro
up
).
Dis
aste
rw
ork
ers
Inte
rven
tio
ng
rou
p:
12
wee
kly
sess
ion
so
fco
g-
nit
ive
beh
avio
ura
lth
erap
y.T
AU
gro
up
:M
enta
l
PT
SD
,d
epre
ssio
n,
alco
ho
lp
rob
lem
san
dvar
iou
scl
in-
ical
dis
ord
ers;
mea
s-u
res
incl
ud
ed
An
AN
OV
Aex
am-
inin
gp
re/p
ost
chan
ges
inC
AP
Ssc
ore
sfo
un
da
sig
nif
ican
tm
ain
effe
cto
fti
me
(F
(co
nti
nu
ed)
DOI: 10.1080/09638237.2018.1437610 Psychological disaster interventions 5

Tab
le1
.C
on
tin
ued
Stu
dy
Co
un
try
Dis
aste
rD
esig
nP
arti
cip
ants
(n)
Ro
leo
fp
arti
cip
ants
Inte
rven
tio
nO
utc
om
esas
sess
edR
esu
lts
hea
lth
trea
tmen
tco
mm
on
lyav
ail-
able
afte
ra
trau
-m
atic
even
t;p
arti
cip
ants
wer
eg
iven
resu
lts
of
thei
rP
TS
Dev
alu
atio
nan
dre
ferr
edb
ack
too
ccu
pat
ion
alh
ealt
hfo
ras
sist
-an
cew
ith
ob
tain
-in
gtr
eatm
ent
thro
ug
hco
mm
u-
nit
yp
rov
ider
s(t
ho
ug
hn
on
eto
ok
this
up
).
clin
icia
n-a
dm
inis
-te
red
PT
SD
Sca
le,
stru
ctu
red
clin
ical
inte
rvie
wfo
rD
SM
-IV
Ax
isI
dis
ord
ers,
life
stre
sso
rch
eck
list
-re
vis
ed,
PT
SD
chec
kli
st,
bec
kd
epre
ssio
nin
ven
-to
ry,
SC
L-9
0-R
,M
ich
igan
alco
ho
lsc
reen
ing
test
,so
cial
adju
stm
ent
scal
ean
dli
feev
ents
scal
e.
(1,
19
)¼
9.6
90
,p5
0.0
1);
asi
g-
nif
ican
tm
ain
effe
cto
fG
rou
p(F
(1,
19
)¼
6.3
17
,p5
0.0
5);
and
asi
gn
ific
ant
tim
eX
Gro
up
inte
ract
ion
(F(1
,1
9)¼
6.5
47
,p5
0.0
5).
Sig
nif
ican
td
ecre
ase
inC
AP
Ssc
ore
sfo
rC
BT
gro
up
com
par
edto
TA
Ug
rou
p(F¼
4.1
,p5
0.0
1).
No
ne
intr
eatm
ent
con
di-
tio
nin
crea
sed
inC
AP
Ssc
ore
bu
t2
1%
inT
AU
gro
up
did
incr
ease
.A
nA
NO
VA
exam
in-
ing
pre
/po
stch
anges
inB
DI
sco
res
fou
nd
atr
end
for
ati
me
XG
rou
pin
tera
ctio
n(F
(1,
16
)¼
3.4
57
,p5
0.0
81
)w
ith
no
sig
nif
ican
tm
ain
effe
cts.
An
AN
OV
Aex
amin
-in
gp
re/p
ost
chan
ges
inS
CL
-9
0G
SI
sco
res
fou
nd
atr
end
for
ati
me
XG
rou
pin
tera
ctio
n,
F(1
,1
8)¼
3.0
74
,p5
0.0
97
,an
da
sig
nif
ican
tm
ain
effe
cto
fG
rou
p,
F(1
,1
8)¼
7.0
62
,p5
0.0
16
,b
ut
no
(co
nti
nu
ed)
6 S. K. Brooks et al. J Ment Health, Early Online: 1–25

Stu
dy
Co
un
try
Dis
aste
rD
esig
nP
arti
cip
ants
(n)
Ro
leo
fp
arti
cip
ants
Inte
rven
tio
nO
utc
om
esas
sess
edR
esu
lts
sig
nif
ican
tm
ain
effe
cto
fti
me.
No
sig
nif
ican
td
iffe
r-en
ces
inal
coh
ol
sco
res.
Eid
etal
.(2
00
4)
No
rway
Sim
ula
ted
sub
mar
ine
dis
aste
r
Ex
per
imen
tal
stu
dy;
surv
eys
con
du
cted
pre
-tra
inin
gan
dat
the
end
of
the
6-d
trai
nin
g.
18
Sai
lors
Dis
aste
rsi
mu
lati
on
exer
cise
Per
son
alit
yh
ard
i-n
ess
asse
ssed
by
sho
rtfo
rmo
fth
ed
isp
osi
tio
nal
resi
lien
cysc
ale;
cop
ing
style
asse
ssed
by
Co
pin
gS
tyle
Qu
esti
on
nai
re;
PT
SD
asse
ssed
by
Imp
act
Of
Even
tS
cale
and
PT
SS
-1
0;
qu
alit
yo
fli
feas
sess
edb
yG
HQ
-12
.
On
asc
ale
of
1–
5,
med
ian
sco
reo
f5
for
wh
eth
ersi
mi-
lar
exer
cise
ssh
ou
ldb
eh
eld
on
are
gu
lar
bas
is;
med
ian
of
4/5
for
the
exer
cise
rein
-fo
rcin
gth
eir
con
-fi
den
cein
thei
rjo
bs.
Mea
sure
so
nIE
S,
PT
SS
-10
or
GH
Q-1
2n
ever
exce
ed’’
low
sym
pto
m,
sam
eas
usu
al’’
du
rin
gth
eex
erci
se.
QO
Lm
easu
red
by
GH
Qsi
gn
ifi-
can
tly
incr
ease
dover
tim
e[F
(6,
14
)¼
4.0
,p5
0.0
1].
Str
ess
sym
pto
ms
mea
-su
red
by
IES
sig
-n
ific
antl
yd
ecre
ased
over
tim
e[F
(6,
14
)¼
2.7
6,
p5
0.0
5].
Per
son
alit
yh
ard
i-n
ess
was
neg
a-ti
vel
yas
soci
ated
wit
hIE
Sto
tal
(r¼�
0.5
2,
p5
0.0
5),
IES
intr
usi
on
(r¼�
0.4
7,
p5
0.0
5)
and
IES
avo
idan
ce(r¼�
0.4
7,
p5
0.0
5)
wh
ile
avo
idan
ceco
pin
g
(co
nti
nu
ed)
DOI: 10.1080/09638237.2018.1437610 Psychological disaster interventions 7

Tab
le1
.C
on
tin
ued
Stu
dy
Co
un
try
Dis
aste
rD
esig
nP
arti
cip
ants
(n)
Ro
leo
fp
arti
cip
ants
Inte
rven
tio
nO
utc
om
esas
sess
edR
esu
lts
was
po
siti
vel
yas
soci
ated
wit
hG
HQ
-12
ind
icat
-in
gre
du
ced
QO
L(r¼
0.5
3,
p5
0.0
5).
Ger
sho
net
al.
(20
04
)U
SA
Ter
rori
smin
gen
eral
Cro
ss-s
ecti
on
al8
4O
ccu
pat
ion
alh
ealt
hw
ork
ers
Ter
rori
smed
uca
-ti
on
alw
ork
pla
cep
rog
ram
me
Co
nfi
den
cein
clin
-ic
alsk
ills
;p
erce
pti
on
of
wo
rksi
tere
adi-
nes
s;m
oti
vat
ion
totr
eat
terr
ori
smv
icti
ms;
mo
tiv-
atio
nto
rece
ive
smal
lpox
vac
cin
e–
all
mea
sure
dby
stu
dy-s
pec
ific
qu
esti
on
nai
re.
Incr
ease
dco
nfi
-d
ence
inp
rote
ct-
ing
self
-wh
ilst
cari
ng
for
vic
tim
so
fb
iote
rro
rism
(59
.7%
)an
dch
emic
alte
rro
r-is
mex
po
sure
(59
.7%
);re
cog
-n
isin
gsy
mp
tom
so
fte
rro
rism
exp
osu
re(8
1.7
%)
and
trea
tin
gv
ic-
tim
so
fch
emic
alex
po
sure
(69
.5%
)K
enar
dy
etal
.(1
99
6)
Au
stra
lia
Ear
thqu
ake
Lo
ng
itu
din
al(�
27
,5
0,
86
and
11
4w
eek
sp
ost
-dis
aste
r)
19
5(6
2d
ebri
efed
and
13
3n
ot
deb
rief
ed)
Em
ergen
cyse
rvic
esan
dd
isas
ter
wo
rker
sG
rou
pst
ress
deb
rief
ing
How
stre
ssfu
lth
eyfo
un
dth
ed
isas
ter,
asse
ssed
by
stu
dy-s
pec
ific
scal
e;p
sych
o-
log
ical
mo
rbid
ity
asse
ssed
by
Imp
act
of
Even
tssc
ale
and
GH
Q-
12
.
No
corr
elat
ion
bet
wee
nn
um
ber
of
deb
rief
ing
ses-
sio
ns
and
per
-ce
ived
hel
pfu
l-n
ess.
No
sig
nif
ican
tfi
nd
-in
gs
inre
lati
on
tod
ebri
efin
gh
elp
-fu
lnes
sfo
rth
eIE
So
rG
HQ
-12
.D
ebri
efin
gw
asre
po
rted
tob
e‘‘
ver
y’’
or
‘‘ex
trem
ely
’’h
elp
ful
by
34
%o
fp
arti
cip
ants
,‘‘
som
ewh
at’’
hel
pfu
lby
46
%an
d‘‘
no
tat
all’
’h
elp
ful
by
20
%.
Th
ose
wh
ow
ere
deb
rief
edre
po
rted
sig
nif
i-ca
ntl
yh
igh
erover
all
GH
Q-1
2sc
ore
s.O
ver
all,
(co
nti
nu
ed)
8 S. K. Brooks et al. J Ment Health, Early Online: 1–25

Stu
dy
Co
un
try
Dis
aste
rD
esig
nP
arti
cip
ants
(n)
Ro
leo
fp
arti
cip
ants
Inte
rven
tio
nO
utc
om
esas
sess
edR
esu
lts
sub
ject
sin
the
deb
rief
edg
rou
psh
ow
edle
ssim
pro
vem
ent
insy
mp
tom
sth
anth
ose
wh
ow
ere
no
td
ebri
efed
and
this
was
tru
efo
rb
oth
the
IES
(Mea
nst
and
ar-
dis
edch
ang
ein
dex
:�
0.3
1–
0.5
6v
)an
dth
eG
HQ
-12
(Mea
nst
and
ard
ised
chan
ge
ind
ex:
0.1
0–
0.2
8).
Lev
elo
fh
elp
erst
ress
was
un
rela
ted
tod
ebri
efin
gei
ther
over
all
or
inre
la-
tio
nto
chan
ge
over
tim
e.T
her
ew
ere
sig
nif
ican
tm
ain
effe
cts
for
hel
per
stre
sso
nb
oth
the
IES
(F(1
,1
90
)¼
6.7
8,
p5
0.0
1)
and
the
GH
Q-1
2(F
(1,
19
0)¼
8.6
9,
p5
0.0
1)
con
-fi
rmin
gth
efa
ctth
atth
ose
rep
ort
-in
gg
reat
erh
elp
erst
ress
had
hig
her
level
so
fm
ea-
sure
dp
sych
op
ath
olo
gy
Mau
nd
eret
al.
(20
10
)C
anad
aP
ote
nti
alin
flu
-en
zap
and
emic
A‘‘
do
se-f
ind
ing
’’st
ud
yco
mp
ared
pre
-po
stch
anges
inth
ree
dif
-fe
ren
td
ura
tio
ns
of
trai
nin
g.
15
8H
osp
ital
wo
rker
sC
om
pu
ter-
assi
sted
‘‘P
and
emic
Str
ess
Vac
cin
e’’
trai
nin
gco
urs
e.P
arti
cip
ants
ran
-d
om
lyas
sig
ned
tosh
ort
cou
rse
(7se
ssio
ns,
Co
nfi
den
cein
trai
n-
ing
and
sup
po
rt;
per
ceiv
edef
fi-
cacy
toad
apt
top
and
emic
con
di-
tio
ns;
inte
rper
-so
nal
pro
ble
ms;
cop
ing
via
Sig
nif
ican
tim
pro
ve-
men
tsfr
om
the
star
tto
the
end
of
the
cou
rse
inp
and
emic
self
-ef
fica
cy,
con
fi-
den
cein
trai
nin
gan
dsu
pp
ort
and
(co
nti
nu
ed)
DOI: 10.1080/09638237.2018.1437610 Psychological disaster interventions 9

Tab
le1
.C
on
tin
ued
Stu
dy
Co
un
try
Dis
aste
rD
esig
nP
arti
cip
ants
(n)
Ro
leo
fp
arti
cip
ants
Inte
rven
tio
nO
utc
om
esas
sess
edR
esu
lts
med
ian
11
1m
in);
med
ium
cou
rse
(12
sess
ion
s,1
58
min
);o
rlo
ng
cou
rse
(17
ses-
sio
ns,
22
3m
in).
pro
ble
m-s
olv
ing
,se
ekin
gsu
pp
ort
or
esca
pe-
avo
id-
ance
.N
ine-
item
SA
RS
scal
ead
apte
dfo
rin
flu
-en
za;
Of
24
-ite
mP
and
emic
Sel
f-E
ffic
acy
Sca
led
eriv
edfo
rth
isst
ud
y;
IIP
-32
;w
ays
of
cop
ing
inven
tory
.
inte
rper
son
alp
rob
lem
s.D
imen
sio
ns
of
inte
rper
son
alp
rob
lem
sw
hic
him
pro
ved
incl
ud
edp
rob
-le
ms
wit
hb
ein
gso
cial
lyin
hib
ited
,n
on
-ass
erti
ve,
over
lyac
com
mo
-d
atin
g,
self
-sa
crif
icin
gan
din
tru
sive/
nee
dy.
Co
pin
gw
ith
stre
ssu
sin
gp
rob
-le
m-s
olv
ing
,se
ekin
gsu
pp
ort
fro
mo
ther
so
res
cap
e-av
oid
ance
did
no
tch
ange
over
the
cou
rse
over
all:
how
ever
,fo
rth
ose
no
tre
po
rtin
gp
rob
-le
m-s
olv
ing
and
seek
ing
sup
po
rt,
ther
ew
ere
pre
-p
ost
imp
rove-
men
ts.
Am
on
gth
ose
un
der
-uti
-li
sin
gp
rob
lem
-so
lvin
gat
T1
ther
ew
asa
sig
-n
ific
ant
pre
-po
stin
crea
se(9
5%
CI
of
dif
fere
nce
0.2
–0
.4,
p5
0.0
01
).A
mo
ng
tho
seu
nd
er-u
tili
sin
gse
ekin
gsu
pp
ort
,th
ere
was
agai
nan
incr
ease
(95
%C
Io
fd
iffe
ren
ce0
.1–
0.3
,p¼
0.0
03
).A
mo
ng
tho
sew
ho
rep
ort
edan
yu
se
(co
nti
nu
ed)
10 S. K. Brooks et al. J Ment Health, Early Online: 1–25

Stu
dy
Co
un
try
Dis
aste
rD
esig
nP
arti
cip
ants
(n)
Ro
leo
fp
arti
cip
ants
Inte
rven
tio
nO
utc
om
esas
sess
edR
esu
lts
of
esca
pe-
avo
id-
ance
atT
1,
ther
ew
asa
dec
reas
ein
this
typ
eo
fco
pin
g(9
5%
CI
of
dif
fere
nce
�0
.1–
0.0
,p¼
0.0
1).
Eac
hco
urs
ele
ng
thre
sult
edin
imp
roved
self
-ef
fica
cyan
dco
n-
fid
ence
intr
ain
-in
gan
dsu
pp
ort
.T
he
med
ium
-le
ng
thco
urs
eap
pea
red
tob
eo
pti
mal
.M
ille
r-B
urk
eet
al.
(19
99
)U
SA
Ban
kro
bb
erie
sC
ross
-sec
tio
nal
14
1B
ank
emp
loyee
sC
riti
cal
inci
den
tst
ress
deb
rief
ing
.W
ork
pro
du
ctiv
ity,
stre
ss,
physi
cal
hea
lth
,w
ork
rela
-ti
on
ship
s,p
er-
son
alre
lati
on
-sh
ips,
des
ire
tokee
pw
ork
ing
,d
ays
off
wo
rk;
psy
cho
log
ical
hea
lth
sym
pto
ms
–su
rvey
des
ign
edfo
rth
est
ud
y.
Of
47
%at
ten
ded
afo
rmal
lyp
re-
sen
ted
CIS
Dse
s-si
on
;al
mo
st8
of
10
bel
ieved
itto
be
hel
pfu
l(t
hes
era
tin
gs
wer
en
ot
asso
ciat
edw
ith
asp
ects
of
the
rob
ber
yco
nte
xt)
.7
7%
also
rate
din
terv
enti
on
sw
ith
co-w
ork
ers
assu
cces
sfu
l;6
4%
inte
rven
tio
ns
wit
hsu
per
vis
ors
;5
4%
wit
hfa
mil
y/
frie
nd
san
d4
8%
wit
hover
all
wo
rken
vir
on
men
t.O
f2
0%
con
sid
ered
over
all
wo
rken
vir
on
men
tto
hav
em
ade
thei
rre
cover
yw
ors
e.O
f1
1%
rep
ort
edth
atqu
esti
on
sfr
om
cust
om
ers,
po
lice
and
med
ia
(co
nti
nu
ed)
DOI: 10.1080/09638237.2018.1437610 Psychological disaster interventions 11

Tab
le1
.C
on
tin
ued
Stu
dy
Co
un
try
Dis
aste
rD
esig
nP
arti
cip
ants
(n)
Ro
leo
fp
arti
cip
ants
Inte
rven
tio
nO
utc
om
esas
sess
edR
esu
lts
wer
eo
bst
acle
sto
reco
ver
yN
ort
het
al.
(20
02
)U
SA
Ok
lah
om
aC
ity
bo
mb
ing
Cro
ss-s
ecti
on
al1
81
Fir
e-fi
gh
ters
wh
ose
rved
asre
scu
ean
dre
cov-
ery
wo
rker
s.
Wo
rkp
lace
deb
rief
ing
sP
sych
iatr
icd
iag
-n
ose
s;d
iag
no
stic
inte
rvie
wsc
hed
ule
.
Of
92
%h
adp
arti
ci-
pat
edin
wo
rk-
pla
ced
efu
sin
gs/
deb
rief
ing
s.T
wo
-th
ird
was
sati
sfie
dw
ith
this
and
on
e-th
ird
dis
sati
sfie
d;
how
ever
,8
9%
said
they
wo
uld
reco
mm
end
the
inte
rven
tio
n.
PT
SD
was
no
tre
late
dto
sati
s-fa
ctio
no
rre
com
-m
end
atio
no
fth
ed
ebri
efin
gs.
How
ever
,p
arti
ci-
pan
tsw
ith
oth
er(n
on
-PT
SD
)d
is-
ord
ers
wer
ele
ssli
kel
yto
rep
ort
sati
sfac
tio
n(5
0v
s.7
1%
,x
2¼
6.9
3,
p5
0.0
1)
or
rec-
om
men
dth
em(8
2vs.
92
%,
x2¼
4.2
4,
p5
0.0
5)
Rei
det
al.
(20
05
)U
SA
Hu
rric
anes
Cro
ss-s
ecti
on
al5
3F
lori
da
Dep
artm
ent
of
Hea
lth
emp
loyee
sT
rain
ing
on
kn
ow
-le
dge,
skil
lsan
dp
rep
ared
nes
s.
Imp
act
of
trai
nin
go
nk
now
led
ge,
skil
lsan
daw
aren
ess;
per
cep
tio
ns
of
pre
par
edn
ess
and
kn
ow
led
ge/
skil
lap
pli
cati
on
rela
-ti
ve
totr
ain
ing
;in
vo
lvem
ent
inth
e2
00
4h
urr
i-ca
nes
.O
pen
-en
ded
qu
esti
on
so
nre
com
men
da-
tio
ns,
over
all
imp
act
of
trai
n-
ing
,su
gges
tio
ns
for
imp
rov
ing
Lar
ge
maj
ori
tyre
po
rted
the
trai
nin
gin
crea
sed
thei
rk
now
led
ge
of
the
core
pro
-g
ram
con
cep
ts.
Mo
stin
dic
ated
the
trai
nin
gen
han
ced
thei
rab
ilit
yo
rp
re-
par
edth
emto
imp
lem
ent
the
13
spec
ific
skil
lsad
dre
ssed
inth
etr
ain
ing
.O
f9
0%
ind
icat
edth
etr
ain
ing
was
(co
nti
nu
ed)
12 S. K. Brooks et al. J Ment Health, Early Online: 1–25

Stu
dy
Co
un
try
Dis
aste
rD
esig
nP
arti
cip
ants
(n)
Ro
leo
fp
arti
cip
ants
Inte
rven
tio
nO
utc
om
esas
sess
edR
esu
lts
del
iver
yan
dad
d-
itio
nal
com
men
ts.
All
asse
ssed
via
stu
dy-s
pec
ific
surv
ey.
use
ful
for
thei
rjo
bs
and
98
%fe
ltb
ette
rp
rep
ared
tore
spo
nd
toa
maj
or
trau
ma
asa
resu
lto
fth
etr
ain
ing
.O
f8
9%
had
inco
rpo
rate
dth
etr
ain
ing
and
its
rela
ted
con
-ce
pts
/sk
ills
inth
eir
per
son
alli
fe;
83
%in
thei
rp
rofe
ssio
nal
life
Sey
leet
al.
(20
13
)In
do
nes
iaE
arth
qu
ake
4-y
ear
lon
git
ud
inal
stu
dy
43
Ele
men
tary
sch
oo
lte
ach
ers
Psy
cho
edu
cati
on
Po
st-t
rau
mat
icd
is-
tres
ssy
mp
tom
s;d
epre
ssio
n;
per
-ce
pti
on
so
fte
ach-
ing
effi
cacy
;p
erce
pti
on
so
fcl
assr
oo
mb
ehav
-io
ur.
PC
L;
CE
S-
D;
Tea
cher
Eff
icac
yS
cale
;m
od
ifie
dver
sio
no
fch
ild
beh
avio
ur
chec
kli
st.
Co
mp
ared
top
aren
tsfr
om
the
com
mu
-n
ity
:th
eyd
idn
ot
dif
fer
inte
rms
of
deg
ree
of
eart
h-
quak
eex
po
sure
or
dep
ress
ion
,b
ut
teac
her
sre
po
rted
low
erP
TS
Dsc
ore
s.P
re-i
nte
rven
tio
n,
CE
S-D
sco
res
wer
ea
sig
nif
ican
tp
red
icto
ro
fre
po
rted
neg
ativ
est
ud
ent
beh
avio
ur
(bet
a¼
0.3
54
,p¼
0.0
37
).P
CL
was
no
ta
sig
nif
i-ca
nt
pre
dic
tor
of
teac
her
s’p
erce
p-
tio
ns
of
neg
ativ
ecl
assr
oo
mb
ehav
-io
ur.
Pre
-in
terv
enti
on
,P
CL
sco
res
pre
-d
icte
din
crea
sed
gen
eral
teac
hin
gef
fica
cy(b
eta
¼0
.34
3,
p¼
0.0
25
).P
ost
-in
terv
enti
on
,C
ES
-Dan
dP
CL
sco
res
wer
en
ot
(co
nti
nu
ed)
DOI: 10.1080/09638237.2018.1437610 Psychological disaster interventions 13

Tab
le1
.C
on
tin
ued
Stu
dy
Co
un
try
Dis
aste
rD
esig
nP
arti
cip
ants
(n)
Ro
leo
fp
arti
cip
ants
Inte
rven
tio
nO
utc
om
esas
sess
edR
esu
lts
pre
dic
tive
of
per
-so
nal
teac
hin
gef
fica
cy.
Pai
red
-sam
ple
tte
sts
show
eda
sig
nif
i-ca
nt
dro
pin
PC
Lsc
ore
s(t
(42
)¼
1.9
5,
p¼
0.0
29
)an
dC
ES
-Dsc
ore
s(t
(42
)¼
2.3
07
,p¼
0.0
13
)fr
om
bef
ore
toaf
ter
the
inte
rven
tio
nT
ehra
ni
etal
.(2
00
1)
UK
Pad
din
gto
ntr
ain
cras
hO
ne
wee
kaf
ter
cras
h;
foll
ow
edu
p4
mo
nth
saf
ter
cras
h.
12
Sai
nsb
ury
’sem
plo
yee
s(t
he
sup
erm
arket
was
nea
rto
the
cras
hsi
tean
dth
eyw
ere
som
eo
fth
efi
rst
on
the
scen
e,p
rov
idin
gla
d-
der
sto
hel
pp
asse
n-
ger
scl
imb
up
fro
mth
etr
ack
and
giv
ing
imm
edia
tefi
rst
aid
).
Deb
rief
ing
PT
SD
dep
ress
ion
.E
xte
nd
edIm
pac
to
fE
ven
tsS
cale
;G
old
ber
gA
nx
iety
and
Dep
ress
ion
Sca
le.
Rec
ord
so
fsi
ckn
ess
abse
nce
.
On
ew
eek
afte
rth
eev
ent,
ther
ew
asa
hig
hle
vel
of
po
st-
trau
ma.
Fo
ur
mo
nth
sfo
llow
ing
the
deb
rief
ing
,th
ere
was
asi
g-
nif
ican
tre
du
ctio
nin
the
sym
pto
ms
mea
sure
dby
the
IES
-Ean
dG
old
ber
gin
stru
-m
ents
.B
efo
resc
ore
s,af
ter
sco
res,
mea
nd
if-
fere
nce
bet
wee
nsc
ore
s,T
-sco
re,
sig
nif
ican
ce,
resp
ecti
vel
y:
An
xie
ty:
5.9
,3
.1,
2.8
,3
.75
,0
.00
3D
epre
ssio
n:
4.8
,2
.2,
2.6
,4
.08
,0
.00
1A
vo
idan
ce:
18
.3,
9.7
,8
.6,
7.7
,0
.00
1A
rou
sal:
15
.8,
6.3
,9
.5,
4.3
,0
.00
1R
e-ex
per
ien
ce:
24
.2,
9.3
,1
5.1
,7
.5,
0.0
01
Th
ep
erfo
rman
cein
dic
ato
rssh
ow
edth
atal
lth
e
(co
nti
nu
ed)
14 S. K. Brooks et al. J Ment Health, Early Online: 1–25

Stu
dy
Co
un
try
Dis
aste
rD
esig
nP
arti
cip
ants
(n)
Ro
leo
fp
arti
cip
ants
Inte
rven
tio
nO
utc
om
esas
sess
edR
esu
lts
emp
loyee
sd
emo
nst
rate
dan
imp
rovem
ent
inp
erfo
rman
ceb
etw
een
Novem
ber
19
99
and
Ap
ril
20
00
wit
hth
eg
reat
est
imp
rovem
ent
bei
ng
inth
eir
chee
rfu
lnes
s,ab
ilit
yto
con
cen
-tr
ate
and
per
-fo
rman
ceo
nth
ejo
b.
Th
em
an-
ager
sas
sess
edth
ep
erfo
rman
ceo
fm
ost
of
the
emp
loyee
sas
exce
llen
to
rver
yg
oo
din
Ap
ril
20
00
.T
her
ew
asa
red
uc-
tio
nin
the
level
of
sick
nes
sab
sen
ceb
etw
een
the
firs
tq
uar
ter
of
19
99
and
20
00
.In
the
wh
ole
gro
up
,1
4fe
wer
day
sab
sen
cew
asre
c-o
rded
in2
00
0th
anh
adb
een
reco
rded
in1
99
9.
Wae
lde
etal
.(2
00
8)
US
AH
urr
ican
eK
atri
na
8-w
eek
pro
gra
mm
eb
egin
nin
g1
0w
eek
sp
ost
-dis
aste
r;m
id-
trea
tmen
tan
dp
ost
-tr
eatm
ent
qu
esti
on
-n
aire
sco
mp
lete
dat
3an
d8
wee
ks
po
st-
wo
rksh
op
.
Tw
enty
atb
asel
ine;
15
atfo
llow
-up
.M
enta
lh
ealt
hw
ork
ers
Fo
ur-
ho
ur
med
ita-
tio
nw
ork
sho
pfo
llow
edby
8-
wee
kh
om
est
ud
yp
rog
ram
me.
PT
SD
sym
pto
ms;
dep
ress
ion
;an
x-
iety
;fo
llow
-up
qu
esti
on
nai
reas
ked
them
tora
teim
pro
vem
ent
inw
ellb
ein
g,
stre
ssco
pin
g,
fru
stra
-ti
on
tole
ran
ce,
acti
vit
yle
vel
,d
epre
ssio
n,
anger
,p
hysi
cal
pai
n,
slee
pp
rob
lem
san
dfa
tig
ue
asa
Sco
res
for
tota
lP
TS
D,
re-e
xp
eri-
enci
ng
,h
yp
erar
-o
usa
lan
dst
ate
anx
iety
sig
nif
i-ca
ntl
yd
ecre
ased
over
tim
e.S
lop
esfo
rav
oid
ance
and
dep
ress
ion
wer
ein
the
exp
ecte
dd
irec
tio
ns
bu
tn
ot
stat
isti
call
yd
if-
fere
nt
fro
mze
ro.
All
trea
tmen
t
(co
nti
nu
ed)
DOI: 10.1080/09638237.2018.1437610 Psychological disaster interventions 15

Tab
le1
.C
on
tin
ued
Stu
dy
Co
un
try
Dis
aste
rD
esig
nP
arti
cip
ants
(n)
Ro
leo
fp
arti
cip
ants
Inte
rven
tio
nO
utc
om
esas
sess
edR
esu
lts
resu
lto
fin
ter-
ven
tio
n.
PC
L-S
;C
ES
-D;
Sta
te-
Tra
itA
nx
iety
Inven
tory
;st
ud
y-
spec
ific
qu
esti
on
s.
effe
ctsi
zes
wer
ein
the
med
ium
ran
ge,
exce
pt
dep
ress
ion
,w
hic
hw
asin
the
smal
lra
nge.
Of
93
%re
po
rted
feel
ing
som
ewh
ato
rm
uch
bet
ter
asa
resu
lto
fth
ein
terv
enti
on
.M
ore
than
60
%re
po
rted
imp
rovem
ents
inst
ress
cop
ing
,fr
ust
rati
on
tole
r-an
ce,
acti
vit
yle
vel
and
dep
res-
sio
n.
Of
47
%re
po
rted
imp
roved
abil
ity
tod
eal
wit
han
ger
.T
he
slo
pes
of
tota
lP
TS
Dan
dan
x-
iety
wer
eco
rre-
late
dw
ith
the
tota
ln
um
ber
of
min
ute
so
fm
edi-
tati
on
pra
ctic
eac
ross
the
8w
eek
s(r¼�
0.4
0,
p5
0.0
5an
dr¼�
0.3
8,
p5
0.0
5,
resp
ect-
ivel
y)
ind
icat
ing
that
mo
rem
edit
a-ti
on
pra
ctic
ew
asas
soci
ated
wit
hg
reat
erim
pro
vem
ents
.W
uet
al.
(20
12
)C
hin
a2
00
8S
ich
uan
eart
hqu
ake
On
em
on
th;
foll
ow
-up
com
ple
ted
by
7m
on
ths
po
st-d
isas
ter.
12
67
Mil
itar
yre
scu
ers
51
2P
IM,
1-m
on
thp
ost
-dis
aste
rA
nx
iety
,d
epre
ssio
nan
dP
TS
D.
Ho
spit
alA
nx
iety
and
Dep
ress
ion
Sca
le(H
AD
S);
Str
uct
ure
d
Bas
elin
ean
aly
sis
sug
ges
ted
no
sig
-n
ific
ant
dif
fer-
ence
sb
etw
een
the
stu
dy
gro
up
s.S
ever
ity
of
PT
SD
,an
xie
ty
(co
nti
nu
ed)
16 S. K. Brooks et al. J Ment Health, Early Online: 1–25

Stu
dy
Co
un
try
Dis
aste
rD
esig
nP
arti
cip
ants
(n)
Ro
leo
fp
arti
cip
ants
Inte
rven
tio
nO
utc
om
esas
sess
edR
esu
lts
Inte
rvie
wfo
rP
TS
D(S
I-P
TS
D).
and
dep
ress
ion
dec
reas
edover
tim
ein
all
thre
eg
rou
ps,
wit
hsi
g-
nif
ican
td
iffe
r-en
ces
bet
wee
nth
eg
rou
ps
insy
mp
-to
ms
of
PT
SD
(p\0
.01
).C
om
par
edw
ith
the
deb
rief
ing
and
con
tro
lg
rou
p,
sig
nif
ican
tly
low
ersc
ore
so
fP
TS
Dan
dp
osi
-ti
ve
effi
cacy
inim
pro
vin
gsy
mp
-to
ms
of
re-
exp
erie
nci
ng
,av
oid
ance
and
hyp
erar
ou
sal
wer
efo
un
din
the
‘‘5
12
PIM
’’g
rou
p.
DOI: 10.1080/09638237.2018.1437610 Psychological disaster interventions 17

Florida Department of Health employees preparing for
hurricanes (Reid et al., 2005).
Three studies involved interactive training workshops
providing education and allowing for discussion of key
issues (Aiello et al., 2011; Gershon et al., 2004; Reid et al.,
2005); one study involved interactive computer-based training
(Maunder et al., 2010) and one entailed a disaster simulation
exercise (Eid et al., 2004). Training courses lasted between
one hour (Aiello et al., 2011) and six days eighteen hours (Eid
et al., 2004). All five interventions were designed to educate
employees about what they may experience during a disaster
and how best to cope with this. The education that was
provided covered various aspects of disasters including
disaster planning (Eid et al., 2004; Gershon et al., 2004;
Maunder et al., 2010; Reid et al., 2005); common concerns of
employees during a disaster (Aiello et al., 2011); the potential
psychological impact of disasters (Aiello et al., 2011;
Gershon et al., 2004; Maunder et al., 2010); coping strategies
(Aiello et al., 2011; Maunder et al., 2010) and resources for
further support (Aiello et al., 2011; Maunder et al., 2010).
Further details of what each intervention entailed can be seen
in Table 2.
Outcomes
All five studies considered the effect of the intervention on
participants’ confidence. Aiello et al. (2011) found that pre-
intervention, only 34.9% of hospital workers felt confident in
being able to deal with a potential influenza pandemic.
Following the session, 69.7% agreed with the statement ‘‘The
session prepared me for a pandemic’’, while 76.1% felt more
confident in their ability to cope as a result of the session,
agreeing with the statement ‘‘Following today’s session, I
believe that I will be better able to cope in the event of a
pandemic’’. Reid et al. (2005) found that 98% of Department
of Health workers felt more confident and better prepared to
respond to a major trauma as a result of the skills training;
most of those who were involved in hurricane response in
2004, having received training in 2003, indicated that the
training had given them confidence and they had used the
acquired skills in their response efforts. Gershon et al. (2004)
found increased confidence in recognising symptoms of
terrorism exposure, treating victims of chemical exposure and
protecting oneself whilst caring for victims. Maunder et al.
(2010) found that participants showed significant improve-
ments from the start to the end of the training course in
‘‘pandemic self-efficacy’’ (i.e. confidence in one’s ability to
carry out their job effectively during a pandemic) and
significantly improved confidence in training and support
received. Eid et al. (2004) found that their submarine disaster
simulation exercise reinforced confidence in Navy sailors: on
a scale of 1–5 (with 5 being high) there was a median score of
4/5 when participants were asked to rate whether the exercise
had reinforced their confidence in the submarine service.
Maunder et al. (2010) found that participants showed
significant improvements from the start to the end of the
course in some interpersonal problems, including social
inhibition and non-assertive, overly accommodating, self-
sacrificing and intrusive/needy behaviours. The same
study found that the intervention led to better coping
strategies: those participants who did not report coping with
stress by using problem-solving or seeking support pre-course
tended to be more likely to use these positive coping
strategies post-course, and less likely to use negative coping
strategies, such as escape-avoidance.
Participants’ perceived usefulness of intervention
Aiello et al. (2011) reported that 87.5% of hospital workers
found the training session ‘‘useful’’ while 91.3% found it
‘‘helpful and informative’’. Reid et al. (2005) found that 90%
of Department of Health employees found the hurricane
training useful, and as a result 89% had incorporated the
training and its related concepts or skills into their personal
lives while 83% had incorporated these into their professional
lives. Eid et al. (2004) reported a median score of 5 (out of 5)
for whether similar exercises should be held on a regular
basis, showing that sailors did indeed feel the exercises were
useful and should be held regularly.
No studies reported any detrimental effects of pre-disaster
training on confidence and the one study (Maunder et al.,
2010) which considered the impact of the training on
interpersonal problems found only positive effects. No studies
measured whether there was any detrimental effect of pre-
disaster training on other mental health outcomes.
Post-disaster
Summary of studies
Ten studies explored the effects of interventions designed to
improve psychological wellbeing after disasters. Two studies
from the USA involved a worksite crisis intervention for
employees of various organisations following the 11
September terrorist attacks in New York (Boscarino et al.,
2005, 2006). Kenardy et al. (1996) examined the effects of
group stress debriefing on emergency services personnel and
disaster workers following an earthquake in Australia; North
et al. (2002) looked at the effects of debriefing on fire-fighters
after a bombing in the USA; Tehrani et al. (2001) examined the
effects of debriefing on supermarket workers in the UK after a
train crash; and Miller-Burke et al. (1999) examined the effects
of Critical Incident Stress Debriefing (CISD) for bank
employees following bank robberies in the USA. It is important
to note that though these articles all refer to ‘‘debriefing’’, the
procedures involved and focus of the intervention may have
differed between studies (see Table 2 for specific details).
Other interventions included cognitive behavioural therapy for
disaster workers who met full or subthreshold PTSD criteria
after the 11 September attacks in the USA (Difede et al., 2007);
psycho-education for elementary school teachers in Indonesia
who experienced an earthquake (Seyle et al., 2013); meditation
for mental health workers following a hurricane in the USA
(Waelde et al., 2008); and a psychological intervention called
the ‘‘512 PIM’’ (512 Psychological Intervention Model)
including discussions, training on cohesion and stress man-
agement, delivered to military rescuers following an earth-
quake in China (Wu et al., 2012).
Outcomes
Boscarino et al. (2005) reported that between 1 and 3 worksite
crisis sessions appeared to protect workers from binge
18 S. K. Brooks et al. J Ment Health, Early Online: 1–25

Table 2. Overview of interventions.
Study Details of intervention
Qualityappraisalscore (%)
Aiello et al. (2011) One-hour training session on predicted stressors associated with influenza; commonconcerns; normal responses to extraordinary stress; organisational approaches tobuilding resilience and reducing stress; coping and resources for further support.Sessions focused on principles such as ‘‘hoping for the best but preparing for the worst’’and making implicit coping strategies explicit. Interaction, in terms of discussion,identification of problems and suggested solutions, was encouraged.
66.7
Boscarino et al. (2005) Brief employer-provided worksite crisis interventions. These could be any brief sessionsrelated to coping with the 9/11 disaster received shortly after the event, arranged by theemployer and led by mental health professionals or counsellors. These included criticalincident stress management, psychological debriefing or any other short-term inter-ventions designed to provide emergency mental health support following trauma.Interventions were different for different workplaces, but 60–70% reported that theintervention involved coping/relaxation techniques and strategies for positive thinking.
93.8
Boscarino et al. (2006) See above 93.8Difede et al. (2007) Twelve weekly sessions of cognitive behavioural therapy modified for disaster workers.
Including psychoeducation; treatment rationale and contracting; breathing exercises;cognitive reprocessing; relapse prevention and homework involving imaginal exposureusing audio-taped imaginal exposure from treatment sessions, graduated in vivoexposure and cognitive reprocessing.
75
Eid et al. (2004) Simulated submarine disaster exercise lasting 6 d 18 h. Participants were seated in a sectionof the submarine in seawater of 35 m depth with lighting, ventilation and heating shutoff. Activities and schedules were organised as closely as possible to SUBSUNKprocedures – an operation carried out to search for a submarine that is known to havesunk.
80
Gershon et al. (2004) Half-day terrorism educational workplace programme, including: role of emergencymanagement in a disaster; information on reporting guidelines, diagnosis, treatment,infection control and bioterrorism effects; methods to diagnose and treat chemical andradiological agents; an overview of disaster mental health and treatment options; keyelements in workplace disaster planning.
73.3
Kenardy et al. (1996) Group stress debriefing 87.5Maunder et al. (2010) ‘‘Pandemic Stress Vaccine’’, a computer-assisted course comprised of audio and video
mini-lectures, onscreen notes, printed fact sheets, quizzes and games and audio modulesfor relaxation skills. Topics addressed included what to expect during a pandemic; whatis resilience; normal stress responses; psychological first aid; working outside of one’scomfort zone; moral and ethical dilemmas, coping approaches; active listening;expressing oneself constructively; balancing work and family; talking to children aboutdisasters/emergencies; personal and home preparation; managing drugs and alcohol;danger signals; and resources for getting help. Participants were randomly assigned toeither the short course (7 sessions, median 111 min total); medium course (12 sessions,158 min); or long course (17 sessions, 223 min).
87.5
Miller-Burke et al. (1999) Critical Incident Stress Debriefing emphasising containment of feelings and expression offeelings in a safe and supportive environment, aimed at moving participants from‘‘shock’’ to ‘‘acceptance’’. This was delivered by an external employee-assistanceservice.
66.7
North et al. (2002) Workplace debriefings/defusings. Debriefings were carried out in groups of 15–20 workers,while ‘‘mental health defusing’’ was carried out individually, after each shift in whichparticipants worked at the bomb site.
80
Reid et al. (2005) Bioterrorism Trauma Intervention Specialist Training (BTIST): Providing skills inassessment, triage, trauma stabilisation, individual and group defusing, debriefing, stressmanagement, compassion fatigue, grief intervention, cultural competence, criticalincident stress management and team development. The 5-d training course includedinteractive teaching methods, such as case studies, role-playing and scenarios. Moduleswere also available on CDs and DVDs.
60
Seyle et al. (2013) Psychoeducational material about impact of disasters on thoughts, emotions and behavioursin adults; relaxation and coping exercises such as deep breathing; psychoeducationalinformation about impact of disasters on children and basic information aboutsupporting children’s emotional stability; education on child misbehaviour andsupporting children’s attention in class.
75
Tehrani et al. (2001) Group debriefing one-week post-disaster, beginning with a short presentation on post-trauma stress giving the opportunity to ask questions and learn about the commonreactions/symptoms experienced after a traumatic event. The debriefing then allowedemployees to share their experiences of what they went through, focusing on theirbehaviours and things that were seen, heard, smelled, touched and tasted. This allowedthem to examine what had happened during the day of the crash, to fill gaps in the story,check understanding and share knowledge.
50
Waelde et al. (2008) Four-hour meditation workshop, including instruction and guided practice in meditation;breathing; guided breathing-focused imagery; mantra repetition and letting go of
81.3
(continued )
DOI: 10.1080/09638237.2018.1437610 Psychological disaster interventions 19

drinking or alcohol dependence, while 2–3 sessions were
protective for PTSD, depression, somatisation, anxiety and
global severity. A follow-up study using propensity scores to
match intervention cases to non-intervention controls
(Boscarino et al., 2006) found that outcomes tended to be
better for intervention cases: they were less likely to show
symptoms of depression and alcohol dependence in the past
year and less likely to show symptoms of PTSD, depression
and anxiety over the past month. Similarly, Tehrani et al.
(2001) found a high level of trauma symptoms immediately
post-disaster, but four months after the debriefing intervention
participants reported reduced anxiety, depression, and PTSD
symptoms – however, there was no control group to determine
whether this recovery was due to the intervention. Tehrani
et al. (2001) also found that post-intervention, all employees
demonstrated an improvement in ‘‘cheerfulness’’ and ability
to concentrate. However, one study did not find any
improvement in psychological outcomes following debrief-
ing: in Kenardy et al.’s (1996) study of group stress
debriefing, the participants who were debriefed reported
significantly higher scores on the GHQ-12 than those who
were not debriefed, and showed less improvement in PTSD.
Even when level of exposure was taken into account, there
was no evidence of debriefing improving psychological
wellbeing.
North et al. (2002) measured PTSD symptoms but not as
an effect of the intervention; instead, they explored whether
PTSD symptoms were associated with satisfaction with, or
recommendation of, the intervention. They found no such
association, though participants with other, non-PTSD dis-
orders were less likely to report satisfaction or recommend the
intervention.
In Wu et al.’s (2012) study of the ‘‘512 Psychological
Intervention Model’’, anxiety, depression and PTSD symp-
toms decreased over time for all three groups (the ‘‘512 PIM’’
group, the debriefed group and the control group), with
significant differences between groups with regard to PTSD
symptoms. The ‘‘512 PIM’’ group had significantly lower
scores of PTSD and positive efficacy in improving symptoms
of re-experiencing, avoidance and hyperarousal.
The study which explored the effects of CBT (Difede et al.,
2007) found a significant decrease in PTSD scores for the
CBT group compared to the treatment-as-usual group, 21% of
which actually increased in PTSD scores. However, there
were no significant differences between groups in terms of
alcohol misuse.
One study looked at the effects of a psycho-educational
intervention (Seyle et al., 2013). This article reported a
significant decrease in depression and PTSD symptoms post-
intervention.
The study exploring meditation as an intervention (Waelde
et al., 2008) found that scores for total PTSD, re-experiencing,
hyperarousal and state anxiety significantly decreased over
time. Total PTSD and anxiety scores were correlated with the
total number of minutes of meditation practiced across the
8 weeks, suggesting more meditation was associated with
greater improvements. The majority of the participants (93%)
in this study reported feeling somewhat or much better as a
result of the intervention. More than 60% reported improve-
ments in stress coping, frustration tolerance, activity level and
depression, while 47% reported improved ability to deal with
anger.
Participants’ perceived usefulness of intervention
In Boscarino et al.’s (2005) study, 21.2% reported that the
worksite crisis intervention helped a lot; 22.8% said it helped
some; 33.7% said it helped a little and 22.4% found it not at
all helpful. North et al. (2002) found that two-third of
participants were ‘‘satisfied’’ with the workplace
Table 2. Continued
Study Details of intervention
Qualityappraisalscore (%)
thoughts, feelings and sensations as they arise. Followed by 8-week home studyprogramme including manual and 4 audio recordings of guided meditations.
Wu et al. (2012) One month post-disaster, one group of participants received the 512 PIM. This included:introduction (explaining goals of the session and developing a friendly and trustfulatmosphere); facts and thoughts (participants describe the facts of the trauma as they seethem, and then recall their first thoughts during the trauma); reaction and symptoms(participants reconstruct the trauma and accompanying emotions in detail, and thendescribe stress symptoms they experienced during and just after the event and currently);stress management (tips and advice about ways of coping with the trauma or the stresssymptoms); training of cohesion (e.g. participants were instructed to play games whichneed team co-operation). Comparison groups included a debriefing group and a no-treatment group.
100
0
2
3
4
Num
ber o
f ar�
cles
0.51
1.52
.53
.54
.55
41-50% 51-60% 61-70%Qualit
71-80% 81y %
-90% 91-100%
Figure 2. Quality appraisal scores.
20 S. K. Brooks et al. J Ment Health, Early Online: 1–25

defusings/debriefings they had taken part in; although one-
third were dissatisfied, 89% still said they would recommend
the intervention. Miller-Burke et al. (1999) found that almost
80% of participants who attended a formally presented CISD
session found it to be helpful. Interventions with co-workers
were also perceived as successful by 77%; interventions with
supervisors were found to be helpful by 64%; and 54% found
interventions with family or friends to be helpful. In Kenardy
et al.’s (1996) study – which showed no positive effect of
debriefing – there was no correlation between the number of
debriefing sessions and the perceived helpfulness of the
intervention; debriefing was reported to be ‘‘very’’ or
‘‘extremely’’ helpful by 34% of participants, ‘‘somewhat’’
helpful by 46% and ‘‘not at all’’ helpful by 20%.
Discussion
This review aimed to explore the literature on interventions
designed to improve the wellbeing of employees exposed to
disasters. We aimed to assess the success of such interven-
tions by looking at their effect on psychological constructs,
such as confidence and ability to cope, and on symptoms of
psychological disorders, such as PTSD and anxiety. We also
aimed to explore how helpful or useful the participants found
the interventions.
We found only a limited amount of relevant literature. Five
studies considered the impact of pre-disaster training courses,
focusing mainly on whether they improved confidence and
whether participants found them useful. Overall, we found
that pre-disaster training was found to be helpful in increasing
confidence in all five studies. Three of the five studies asked
participants to rate the usefulness of the intervention, with all
three reporting positive results. There was very little explor-
ation of the impact of training on psychological outcomes,
though one study reported that it led to improvements in
‘‘inter-personal’’ problems and more effective coping mech-
anisms (i.e. problem-solving or seeking support, rather than
avoidance).
It appears that evidence-based approaches, providing
education and focusing on mediators of distress, may be
relevant and useful in terms of improving employees’
confidence in their own abilities to act appropriately during
a disaster and their ability to cope. Realistic simulated crisis
training, such as the rehearsal training explored by Eid et al.
(2004) appears to also be valuable in improving confidence.
While these are positive findings, confidence on its own is not
an especially useful outcome for pre-disaster training as it is
likely to be a temporary outcome, especially if measured
directly after training. It would perhaps be more useful for
studies to focus on how participants rate the usefulness of the
training, and whether they plan to or succeed in implementing
their learning into their work – as in the Reid et al. (2005)
study which reported that over 80% of participants had
incorporated training concepts into their professional lives.
This is more likely to be a long-lasting outcome than
increased confidence.
Importantly, no negative effects associated with pre-
disaster skills training were reported in any of the five pre-
disaster training studies. No studies reported a detrimental
effect on confidence and the study which considered
interpersonal problems found only positive effects of training.
Participants typically rated training as useful and something
they would recommend. This is a positive finding especially
since it could be possible for any disaster training to increase
feelings of worry or anxiety in employees, as it requires them
to consider worst-case scenarios and perhaps causes them to
think about stressful situations they may not have considered
before. However, it is possible that the lack of findings
regarding detrimental effects is due to the nature of the post-
training questions asked; future studies should include a
measure of worry or anxiety to further explore whether
training could have a detrimental effect.
Ten studies explored post-disaster interventions, focusing
mainly on their impact on psychological symptoms. Three
studies suggested that workplace interventions such as
debriefings can have long-term positive effects, with ideally
more than one session being most helpful (Boscarino et al.,
2005). However, one study found that debriefing was not
helpful and could in fact lead to poorer outcomes. Other
interventions such as the ‘‘512 Psychological Intervention
Model’’ (Wu et al., 2012), CBT, psychoeducation and
meditation were all found to be useful in improving psycho-
logical symptoms. It is also important to note that the studies
exploring these interventions were among the highest-scoring
studies in the quality appraisal, in particular the 512
Psychological Intervention Model study which described the
appropriate statistical tests fully and considered confounding
variables and was the only study to receive 100% on our
quality assessment. However, these interventions were only
explored in one study each, therefore, we cannot be sure that
the results are generalisable to other employee populations.
Four studies explored how useful participants rated the
interventions, and the results were not especially positive
overall. The most positive result came from Miller-Burke
et al.’s (1999) study of bank employees who participated in
CISD – 80% reported finding it useful. Three studies on
workplace debriefings suggested that participants did not find
them particularly helpful. The other studies did not include
any measure of helpfulness of the intervention, and, therefore,
we do not know whether the 512 Psychological Intervention
Model, CBT, psychoeducation or meditation were rated as
helpful by the employees who participated in them.
Overall, we found little evidence of what kind of post-
disaster interventions are most useful. The fact that we found
such a small number of relevant studies, many of which
looked at different interventions, means we cannot identify
which intervention is most successful. It does appear that
debriefing led to an improvement in psychological symptoms
but, as one study found that debriefing did not improve
wellbeing at all and in fact led to poorer outcomes, it is likely
that the effectiveness of debriefing is dependent on factors,
such as how and when it is carried out, what it involves, and
how many sessions are provided. It is also important to note
that there was little consistency within the articles regarding
what constituted debriefing, and so it would be inappropriate
to generalise from this review. The lack of longitudinal
studies also means that there was no evidence on the potential
long-term effects of psychological debriefing.
Literature reviews focusing on the mental health impact of
disasters on communities in general have shown similar
DOI: 10.1080/09638237.2018.1437610 Psychological disaster interventions 21

findings. For example a review of the mental health response
to community disasters (North & Pfefferbaum, 2013)
identified PFA, debriefing and ‘‘crisis counselling’’ as the
three most commonly applied early psychosocial interven-
tions. Their discussion of PFA was fairly positive, suggesting
it should be embedded into emergency response systems,
although they point out that it has not been empirically tested.
They concluded that debriefing was ineffective for PTSD
prevention or treatment and that it could actually be harmful
in the long term, suggesting that instead, individuals at risk
for psychopathology should be identified and referred for
psychiatric services. Finally, they found that ‘‘crisis counsel-
ling’’ was poorly defined in the literature and that overall it
appeared to be insufficient in meeting the needs of individuals
who require formal psychiatric treatment. Another review on
disaster impact at the community level (Goldmann & Galea,
2014) supported the ideas that debriefing is not recommended
and that PFA is the preferred post-disaster intervention,
although empirical studies evaluating its effectiveness are still
needed. They also found empirical support for CBT, in
particular exposure therapy where the individual is asked to
recollect the traumatic experience, though they point out that
there are few randomised controlled trials for CBT in disaster
survivors and few studies looking at the long-term effects.
This review also proposes that pre-disaster, it is helpful to
develop and test response methods within communities that
are adaptable to different disaster situations, and to build on
knowledge gained from previous disasters. They suggest that
addressing modifiable stressors and helping victims return to
pre-disaster routines may be effective in reducing post-
disaster distress; they also cite an association between media
exposure of the disaster and PTSD, suggesting that commu-
nities should look into ways of communicating information in
such a way as to reduce fear and promote calm.
Limitations
Two-third of the included articles (n¼ 10) were from North
America. It may have been useful to consider widening the
search and translating foreign language articles to provide
further evidence about the effectiveness of interventions. The
decision to restrict the search to articles published in peer-
reviewed journals may have limited the results; future
research may consider searching grey literature for relevant
studies. The quality appraisal tool we used was the same one
we used to assess articles in our previous reviews (Brooks
et al., 2015, 2016, 2017); it was a deliberate choice to use the
same tool throughout our reviews to ensure consistency.
However, this particular tool does not specifically assess the
quality of intervention studies, and it may have been useful to
include questions specifically relating to the potential for bias
which are relevant only for intervention studies.
There were also a number of key limitations of the studies
included in this review. The pre-disaster intervention studies
tended to limit their analysis to exploring confidence and
perceived self-efficacy, and did not measure other psycho-
logical outcomes. Most of the pre-disaster studies were cross-
sectional rather than prospective or randomised controlled
trials. Often, confidence pre-training was measured retro-
spectively, so while participants may have felt their
confidence improved, it is difficult to ascertain whether
this is true and by how much it improved. The articles
reviewed here also failed to explore the impact this
reported increase in confidence may have on coping and
other psychological outcomes. Follow-up periods tended to
be short, with participants completing measures immedi-
ately following their training sessions, and so long-term
effects on confidence and competency are not known.
Furthermore, while participants clearly reported feeling
more confident after training, there is no evidence to
suggest whether this would translate to better coping during
an actual disaster. A useful way of assessing this might
involve having simulated crisis events (i.e. emergency
preparedness exercises or drills), where employees have to
act and respond exactly as they would in a disaster
situation. This would give a better idea of whether the
training has actually been successful in terms of improving
skills, though it would still not be clear – without
experiencing a real disaster – whether the training really
does improve employees’ ability to cope psychologically.
Though several of the post-disaster intervention studies
showed positive effects of interventions, such as workplace
debriefings, some studies (e.g. Boscarino et al., 2005, 2006)
looked at many different workplaces, all of whom had
received their own workplace interventions. These presum-
ably differed in terms of how they were offered, the timing of
the intervention, who led the sessions, the length of the
sessions and what exactly was involved. As there was no
attempt to differentiate the results of different workplaces, it
is difficult to ascertain which aspects of debriefing are
important in terms of improving outcomes. Many of the post-
disaster studies failed to ask participants to rate the usefulness
of, or their satisfaction with, the interventions. Many had no
control groups or ‘‘treatment-as-usual’’ groups to compare
results with, and many had no follow-up or pre-disaster
comparisons. Therefore, even when results were positive and
indicated that employees coped well after disasters, it is
impossible to know whether this is due to the interventions:
perhaps the employees involved were particularly resilient, or
perhaps symptoms would have improved over time even
without an intervention.
In addition, many studies had small sample sizes and high
dropout rates, making it difficult to generalise from the
results. Often no standardised measures were used, and the
questionnaires given to participants were brief. Several
studies presented few statistical details and did not measure
psychological outcomes. Very few studies considered other
factors which may affect the effectiveness of interventions,
such as prior psychiatric history or previous exposure to
trauma.
Implications
The paucity of good quality work in this area is striking. More
and better quality, studies are required before any firm
recommendations can be made on how best to prepare
employees for a possible disaster or to intervene following a
disaster. Future studies should include comparison groups.
Reliance on non-randomised study techniques, especially
ones without a suitable control group and accounting for
22 S. K. Brooks et al. J Ment Health, Early Online: 1–25

known confounders, can lead to misguided practice. A review
on psychological debriefing (Greenberg, 2001) highlights
this, with six of eight randomised trials of debriefing showing
it to be at best unhelpful and at worst harmful, while the
uncontrolled trials showed mixed results, sometimes finding
debriefing to be unhelpful but sometimes finding it to be
beneficial.
The small number of studies examining pre-disaster
training courses appeared to show that these courses were
successful in increasing confidence and feelings of self-
efficacy; however, it is unclear whether this would translate to
better coping if faced with a real disaster, or whether
increased confidence would be protective of mental health
post-incident. It is also unclear what impact training may have
on psychological wellbeing, as no studies measured this,
focusing instead on confidence and satisfaction with the
training course. Taking account of the limitations of the
included studies is particularly important given that whilst
some of the studies we found reported that psychological
debriefing was helpful, there is good evidence from
randomised controlled studies of debriefing techniques in
other populations that not only is it ineffective in improving
mental health status in the longer term but also has the
potential to cause harm (NICE, 2005; Rose et al., 2009).
However, some suggest that the evidence that debriefing is
unhelpful or even harmful is unreliable and that, if protocols
are followed correctly, debriefing can have positive effects on
wellbeing (Hawker & Hawker, 2015). This is an area which
merits further research within disaster-exposed organisations.
From the results of this review, it appears possible that
CBT, psychoeducation and meditation may be useful in
improving the psychological wellbeing of employees after a
disaster. However, these findings come from a very limited
number of studies, without randomised controlled trials, and,
therefore, any suggestion that these could be helpful is
extremely tentative. Future research is needed to support these
findings.
Based on the findings of this review as well as the
findings of reviews on interviews for disaster-exposed
communities, our suggestions for organisations would be as
follows:
� Pre-disaster training appears to be helpful for employees;
prepare them for both the practical issues involved and
the potential psychological distress they may experience.
Develop and test response methods adaptable to different
emergency situations; simulated crisis training may be
useful in helping them to understand how to respond
should a disaster occur. Use any previous experience of
emergency situations to inform these response methods
and crisis training. Educate employees on the symptoms
of distress they should look out for post-disaster and
where they should go to seek help should they need to.
Workshops focusing on appropriate coping skills may be
useful – for example encouraging problem-solving rather
than avoidance, and encouraging them to seek support
from others. PFA training for employees may help them
feel able to listen to and support their colleagues. These
steps are likely to enhance their confidence both in their
abilities to act appropriately during a disaster and their
ability to cope with it psychologically.
� Communicate calmly and effectively about the emer-
gency situation with employees in a way as to not
produce fear.
� Do not ‘‘debrief’’ following a disaster as this has the
potential to be harmful. Instead, encourage a supportive
atmosphere within the workplace where employees feel
able to discuss their feelings with their colleagues.
Managers who are educated in the possible risks of
disaster exposure and the symptoms to look out for may
be able to identify employees who are particularly
vulnerable and may need more support than the organ-
isation can provide and these employees should be
signposted on to the appropriate psychiatric services.
Declaration of interest
NG runs a psychological health consultancy which provides
disaster support training and support.
The research was funded by the National Institute for
Health Research Health Protection Research Unit (NIHR
HPRU) in Emergency Preparedness and Response at King’s
College London in partnership with Public Health England
(PHE). The views expressed are those of the author(s) and not
necessarily those of the NHS, the NIHR, the Department of
Health or Public Health England. The funding body did not
play a role in the design, collection, analysis or interpretation
of data; the writing of the manuscript; or the decision to
submit the manuscript for publication.
ORCID
Samantha K. Brooks http://orcid.org/0000-0003-3884-
3583
Richard Amlot https://orcid.org/0000-0003-3481-6588
Neil Greenberg http://orcid.org/0000-0003-4550-2971
G. James Rubin http://orcid.org/0000-0002-4440-0570
References
Aiello A, Young-Eun Khayeri M, Shreyshree R, et al. (2011). Resiliencetraining for hospital workers in anticipation of an influenza pandemic.J Contin Educ Health Prof, 31, 15–20.
American Psychiatric Association. (1980). Diagnostic and statisticalmanual of mental disorders. 3rd ed. Washington, DC: Author.
Boscarino JA, Adams RE, Figley CR. (2005). A prospective cohort studyof the effectiveness of employer-sponsored crisis interventions after amajor disaster. Int J Emerg Ment Health, 7, 9–22.
Boscarino JA, Adams RE, Foa EB, Landrigan PJ. (2006). A propensityscore analysis of brief worksite crisis interventions after the WorldTrade Center disaster: Implications for intervention and research. MedCare, 44, 454–62.
Brooks SK, Dunn R, Sage CAM, et al. (2015). Risk and resilience factorsaffecting the psychological wellbeing of individuals deployed inhumanitarian relief roles after a disaster. J Ment Health, 24, 385–413.
Brooks SK, Dunn R, Amlot R, et al. (2016). Social and occupationalfactors associated with psychological distress and disorder amongdisaster responders: A systematic review. BMC Psychol, 4, 18.
Brooks SK, Dunn R, Amlot R, et al. (2017). Social and occupationalfactors associated with psychological wellbeing among occupationalgroups affected by disaster: A systematic review. J Ment Health, 26,373–384.
Centre for Research on the Epidemiology of Disasters (2009). Disasterlist. Available from: http://www.emdat.be/disaster-list.
Chang CM, Connor KM, Lai TJ, et al. (2005). Predictors ofposttraumatic outcomes following the 1999 Taiwan earthquake. JNerv Ment Dis, 193, 40–6.
DOI: 10.1080/09638237.2018.1437610 Psychological disaster interventions 23

Difede J, Malta LS, Best S, et al. (2007). A randomized controlledclinical treatment trial for World Trade Center attack-related PTSD indisaster workers. J Nerv Ment Dis, 195, 861–5.
Drummond M, Jefferson T. (1996). Guidelines for authors and peerreviewers of economic submissions to the BMJ. TheBMJ Economic Evaluation Working Party. British Med J, 313,275–83.
Dunn R, Brooks SK, Rubin GJ, Greenberg N. (2015). Psychologicalimpact of traumatic events: Guidance for trauma-exposed organisa-tions. Occup Health Work, 12, 17–21.
Effective Public Health Practice Project (EPHPP) (2009). Qualityassessment tool for quantitative studies. Available from: http://www.ephpp.ca/tools.html.
Eid J, Johnsen BH, Saus E-R, Risberg J. (2004). Stress and coping in aweek-long disabled submarine exercise. Aviat Space Environ Med, 75,616–21.
Gershon RRM, Gemson DH, Qureshi K, McCollum MC. (2004).Terrorism preparedness training for occupational health professionals.J Occup Environ Med, 46, 1204–9.
Goldmann E, Galea S. (2014). Mental health consequences of disasters.Annu Rev Public Health, 35, 169–83.
Greenberg N. (2001). A critical review of psychological debriefingand a proposal for the future: The management of psycho-logical health after traumatic experiences. J R Nav Med Serv,87, 158–61.
Greenberg N, Langston V, Jones N. (2008). Trauma riskmanagement (TRiM) in the UK Armed Forces. J R Army MedCorps, 154, 124–7.
Guha-Sapir D, Hoyois P, Below R. (2013). Annual Disaster StatisticalReview 2013. Available from: http://cred.be/sites/default/files/ADSR_2013.pdf.
Hawker D, Hawker D. (2015). What can be learned from the debriefingcontroversy? In: Yule W, Hawker DD, Alexander D, Holowenko H,Tehrani N, Durkin J, Hacker Hughes J, eds. Early Interventions forTrauma. Proceedings from symposia; 2014 Nov 25 and 2015 Jan 8.Crisis, Disaster and Trauma Section; Leicester, UK: BritishPsychological Society, 6–17 p.
Kenardy JA, Webster RA, Lewin TJ, et al. (1996). Stress debriefing andpatterns of recovery following a natural disaster. J Trauma Stress, 9,37–49.
Maunder RG, Lancee WJ, Mae R, et al. (2010). Computer-assistedresilience training to prepare healthcare workers for pandemicinfluenza: A randomized trial of the optimal dose of training. BMCHealth Serv Res, 10, 72.
Miller-Burke J, Attridge M, Fass PM. (1999). Impact of traumatic eventsand organizational response – A study of bank robberies. J OccupEnviron Med, 41, 73–83.
Mitchell JT. (1983). When disaster strikes . . . the critical incidentdebriefing process. JEMS, 8, 36–9.
National Institute for Health and Care Excellence (NICE) (2005). Post-traumatic stress disorder (PTSD): The management of PTSD in adultsand children in primary and secondary care. Available from: http://www.nice.org.uk/guidance/cg26/chapter/guidance#the-treatment-of-ptsd.
National Institute for Health (2014). Quality assessment tool forobservational cohort and cross-sectional studies. Available from:http://www.nhlbi.nih.gov/health-pro/guidelines/in-develop/cardiovas-cular-risk-reduction/tools/cohort.
North CS, Pfefferbaum B. (2013). Mental health response to communitydisasters: A systematic review. JAMA, 310, 507–18.
North CS, Tivis L, McMillen C, et al. (2002). Coping, functioning andadjustment of rescue workers after the Oklahoma City bombing.J Trauma Stress, 15, 171–5.
Pekevski J. (2012). First responders and psychological first aid. J EmergManag, 11, 39–48.
Reid WM, Ruzycki S, Haney ML, et al. (2005). Disaster mental healthtraining in Florida and the response to the 2004 hurricanes. J PublicHealth Manag Pract, 11, S57–62.
Rose S, Bisson J, Churchill R, Wessely S. (2009). Psychologicaldebriefing for preventing post traumatic stress disorder (PTSD). In:The Cochrane Library. Oxford, UK: Update Software.
Seyle DC, Widyatmoko CS, Cohen Silver R. (2013). Coping with naturaldisasters in Yogyakarta, Indonesia: A study of elementary schoolteachers. Sch Psychol Int, 34, 387–404.
Strohmeier H, Scholte WF. (2015). Trauma-related mental healthproblems among national humanitarian staff: A systematic review ofthe literature. Eur J Psychotraumatol, 6, 28541.
Tehrani N, Walpole O, Berriman J, Reilly J. (2001). A specialcourage: Dealing with the Paddington rail crash. Occup Med(Lond), 51, 93–9.
Waelde LC, Uddo M, Marquett R, et al. (2008). A pilot study ofmeditation for mental health workers following Hurricane Katrina. JTrauma Stress, 21, 497–500.
Wessely S, Bisson J, Rose S, et al. (2000). A systematic review of briefpsychological interventions (‘debriefing’) for the treatment of imme-diate trauma related symptoms and the prevention of post traumaticstress disorder. In: Oakley-Browne M, Churchill R, Gill D, eds.Depression, Anxiety and Neurosis Module of the Cochrane Databaseof Systematic Reviews. Oxford, UK: Update Software.
West C, Bernard B, Mueller C, et al. (2008). Mental health outcomes inpolice personnel after Hurricane Katrina. J Occup Environ Med, 50,689–95.
Wu S, Zhu X, Zhang Y, et al. (2012). A new psychological intervention:‘‘512 Psychological Intervention Model’’ used for military rescuers inWenchuan earthquake in China. Soc Psychiatry Psychiatr Epidemiol,47, 1111–9.
Appendix I – Search strategy
Search: EMBASE 1980–2015; EMBASE 1974–1979; EMBASE Classic1947–1973; Ovid Medline 1946–2015; PsycINFO 1806–2015; Web ofScience.
Search 1 (psychological wellbeing);Well-being; anxiety; panic; posttraumatic stress; PTSD; stress;
‘‘mental health’’; depress*; neurosis; adjustment disorder*; distress;
psychological; resilience; coping; ‘‘mental disorder*’’; ‘‘positive psych-
ology’’; ‘‘satisfactory life’’; mindfulness; flourish; pleasure; flow;
growth¼COMBINE WITH ORSearch 2 (disasters);Anthrax; avalanche; avian influenza; bioterrorism; bird flu; blizzard;
bomb*; chemical spill; Chernobyl; cyclone; drought; disaster*; earth-
quake; Ebola; emergenc*; explosion; fire; flood; Fukushima; H1N1;
H5N1; hurricane; industrial accident; landslide; massacre; mass killing;
MERs; Middle East respiratory syndrome; pandemic; nuclear radiation;
radiological; SARs; severe acute respiratory syndrome; 11 September;
shooting*; storm; swine flu; terroris*; Three Mile Island; tidal wave;
tornado; tsunami; typhoon; volcanic eruption; volcano; World Trade
Center.¼COMBINE WITH ORSearch 3 (occupational search terms);Organisation*; organisation*; occupation*; employee*; employer*;
workforce*; worker*; business; team; emergency response; healthcareprovider*; healthcare worker*; construction work*; fire-fighter*; fireofficer*; paramedic*; doctor*; nurse*; police; first aid responder*;personnel; hospital administrator; military.¼COMBINE WITH ORCombine Search 1 AND Search 2 AND Search 3
Appendix II – Quality appraisal form
All questions are answered with ‘‘yes’’ or ‘‘no’’.
Section 1: Study design(1) Was the research question/objective clearly stated?(2) Were all subjects selected or recruited from the same or similar
populations (including the same time period)?(3) Were the inclusion and exclusion criteria for being in the study pre-
specified and applied uniformly to all participants?(4) Was the study population and size clearly specified and defined?
24 S. K. Brooks et al. J Ment Health, Early Online: 1–25

Section 2: Data collection and methodology(1) Were standardised measures used, or where measures are designed
for the study, attempts to ensure reliability and validity were made?(2) Were the data collected in a way that addressed the research issue?(3) Was the participation rate stated and at least 50%?(4) Was the number of participants described at each stage of the
study?(5) If the study followed participants up, were reasons for loss to
follow-up explained?
Section 3: Analysis and interpretation of results(1) Were details of statistical tests sufficiently rigorous and described?(2) Were details of confidence intervals given?(3) Were potential confounding variables measured and adjusted
statistically for their impact on the relationship between exposure(s)and outcome(s)?
(4) Was the answer to the study question provided?(5) Are the findings related back to previous research?(6) Do conclusions follow from the data reported?(7) Are conclusions accompanied by the appropriate caveats?
DOI: 10.1080/09638237.2018.1437610 Psychological disaster interventions 25