Embed Size (px)
Citation preview

Navigating the Complexities of Dyslipidemia Management in Patients With
Cardiometabolic Disease
Educational Partner
November 30, 2011 Rosemont, IL

Session 4
Session 4: Navigating the Complexities of Dyslipidemia Management in Patients With Cardiometabolic Disease Learning Objectives
1. Describe the impact of comorbidities on cardiovascular risk in patients with dyslipidemia and ways to reduce risks. 2. Implement evidence-based strategies for assessing and managing dyslipidemia and cardiometabolic risk so as to
improve patient outcomes. 3. Compare and contrast lipid-lowering regimens based on stage of kidney disease and other comorbidities and apply
new scientific evidence into treatment decisions. Faculty Michael E. Cobble, MD, AAFP, FNLA Director, Canyons Medical Center Sandy, Utah Adjunct Faculty, University of Utah School of Medicine Salt Lake City, Utah Michael E. Cobble, MD, is director of Canyons Medical Center in Sandy, Utah, where he has been in private practice for 13 years. He is an adjunct faculty member of the University of Utah School of Medicine, where he is a preceptor for family practice physician assistants. He also serves as clinical trainer at University of Utah College of Nursing in Salt Lake City and accepts medical students and nurse practitioners in clinical rotations. Dr Cobble also serves as chief medical officer at Atherotech Diagnostic Laboratories. Dr Cobble graduated from the College of Idaho with a BS in chemistry. He earned his MD from the University of Utah School of Medicine in Salt Lake City as a student of the Family Practice Honors Program. He attended family medicine residency training at Holy Cross Hospital and is board-certified and designated by the National Lipid Association as a Master of Clinical Lipidology. The Neuroscience Education Institute has also designated Dr Cobble as a Master of Psychopharmacology. Peter P. Toth, MD, PhD Clinical Professor University of Illinois College of Medicine Peoria Director of Preventive Cardiology Sterling Rock Falls Clinic, Ltd. Sterling, Illinois Dr Toth received his BA in biochemistry from Princeton University, his PhD from Michigan State University, and his MD from Wayne State University School of Medicine in Detroit, Michigan. He completed residency training in family medicine at the University of Iowa Hospitals and Clinics. Dr Toth is a diplomate of the American Board of Family Practice and the American Board of Clinical Lipidology as well as fellow of the AAFP, the International College of Angiology, and the ACC, among others. He also is a member of the ACC’s Foundation Council on Cardiovascular Disease Prevention. Dr Toth has authored or coauthored more than 220 publications in peer-reviewed journals and textbooks, including Circulation, Current Opinion in Cardiology, and The Journal of Biological Chemistry. He is editor-in-chief of the Year in Lipid Disorders, associate editor for the Year Book of Endocrinology, and section editor for Current Atherosclerosis Reports. Dr Toth is coeditor of several textbooks, including Therapeutic Lipidology, Comprehensive Management of High Risk Cardiovascular Patients, Practical Lipid Management, and Clinical Challenges in Hypertension.

Session 4
Faculty Financial Disclosure Statements The presenting faculty report the following: Michael E. Cobble, MD, AAFP, FNLA, is a consultant to and a speakers’ bureaus member for Abbott, AstraZeneca, Bristol-Myers Squibb, GlaxoSmithKline, Eli Lilly & Company, Novo Nordisk Inc., and Forest Laboratories. Peter P. Toth, MD, PhD, has disclosed receiving honoraria from Merck & Co., Inc. as a consultant and a speaker. Education Partner Financial Disclosure Statement The content collaborators at Med-IQ report the following: Rachel Karcher, PharmD, has no financial relationships to disclose. Suggested Reading List American Diabetes Association. Standards of medical care in diabetes--2011. Diabetes Care. 2011;34(Suppl 1):S11-61. Baigent C, Keech A, Kearney PM, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet. 2005;366(9493):1267-1278. Barnett AH. The importance of treating cardiometabolic risk factors in patients with type 2 diabetes. Diabetes Vasc Dis Res. 2008;5(1):9-14. Blaha MJ, Blumenthal RS, Brinton EA, et al. The importance of non-HDL cholesterol reporting in lipid management. J Clin Lipidol. 2008;2:267-273. Brunzell JD, Davidson M, Furberg CD, et al. Lipoprotein management in patients with cardiometabolic risk: consensus statement from the American Diabetes Association and the American College of Cardiology Foundation. Diabetes Care. 2008;31(4):811-822. Grundy SM, Cleeman JI, Daniels SR, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Executive Summary. Circulation. 2005;112(17):2735-2740. Harper CR, Jacobson TA. Managing dyslipidemia in chronic kidney disease. J Am Coll Cardiol. 2008;51(25):2375-2384. Molitch ME, DeFronzo RA, Franz MJ, et al. Nephropathy in diabetes. Diabetes Care. 2004;27 (suppl 1):S79-S83. National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106(25):3143-3421. National Kidney Foundation. KDOQI Clinical Practice Guidelines and Clinical Practice Recommendations for Diabetes and Chronic Kidney Disease. Available at http://www.kidney.org/professionals/kdoqi/guideline_diabetes/guide2.htm. Rodbard HW, Jellineger PS, Davidson JA, et al. American Association of Clinical Endocrinologists/American College of Endocrinology Consensus Panel on type 2 diabetes mellitus: an algorithm for glycemic control. Endocr Pract. 2009;15(6):540-559. Shojania KG, Ranji Sr, McDonald KM, et al. Effects of quality improvement strategies for type 2 diabetes on glycemic control: a meta-regression analysis. JAMA. 2006;296(4):427-440. Wanner C, Krane V. Lessons learnt from the 4D trial. Nephrol Ther. 2006;2(1):3-7.

1
Navigating the Complexities of Dyslipidemia in Patients
With Cardiometabolic Disease
Drug List
• Atorvastatin (Lipitor)
• Cholestyramine (Prevalite, Questran)
• Colesevelam (Welchol)
• Colestipol (Colestid)
• Ezetimibe (Zetia)
• Ezetimibe + simvastatin (Vytorin)
• Fenofibrate (Antara, Fenoglide, Lipofen, Lofibra, Tricor, Triglide)
• Fluvastatin (Lescol)
• Gemfibrozil (Lopid)
• Lovastatin (Mevacor)
• Metformin (Fortamet, Glucophage, Glumetza, Riomet)
• Niacin (Niacor, Niaspan)
• Pitavastatin (Livalo)
• Pravastatin (Pravachol)
• Rosuvastatin (Crestor)
• Simvastatin (Zocor)
• Sitagliptin (Januvia)
Learning Objectives
• Assess the impact of comorbidities on cardiovascular risk in patients with dyslipidemia and outline ways to reduce risks
• Implement evidence-based strategies for assessing and managing dyslipidemia and cardiometabolic risk so as to improve patient outcomes
• Compare and contrast lipid-lowering regimens based on stage of kidney disease and other comorbidities and apply new scientific evidence to treatment decisions
A Growing Problem. . .
• Primary care practices see > 90% of people with type 2 diabetes
- Likely even a higher percentage of those who do not yet carry that diagnosis but who are at increased risk, ie, have cardiometabolic syndrome
• Data, such as NHANES, have suggested that we are falling short in our efforts to achieve targeted treatment goals for various cardiometabolic risk factors
• Therefore, awareness and education in primary care practice is needed to reduce the risk and burden of cardiometabolic risk
McCullough DK, et al. Eff Clin Pract. 1998;1:12-22.NHANES – National Health and Nutrition Examination Survey; http://www.cdc.gov/nchs/nhanes.htm.
Today’s Goals
• Assess the importance of - Effective assessment and management of dyslipidemia- How dyslipidemia interplays with cardiometabolic risk- How to best manage cardiometabolic risk
• Define how quality improvement practices canassist PCPs in cardiometabolic risk management
• Provide methods for you to directly assess your practice in cardiometabolic risk management
- Specific performance measures that can be applied to your practice
Slides available at:www.pri-med.com/10MDW11A/syllabus
Professional Societies
• Focus on disease management in the context of clinicians’ individual practice
• Move education closer to the point of care
• Build a framework for life-long learning for the clinician and his or her team
Clinician Perspective
• Insight to actual patient population
• Comparison with peer practices and national standards
• Maintenance of Certification (MOC), Pay for Performance (P4P), Maintenance of Licensure (MOL)
Patient Perspective
• Improve patient outcomes – reduce cardiometabolic risk
Why Quality Improvement (QI)?

2
Performance Measures Support Guideline Adherence; Quality of Care Indicators
Clinical Studies,Medical
Literature
Patient Outcomes
Clinical Expertise
Guidelines andAlgorithms
Performance Measures
(eg, HEDIS)
Performance Measures
Common Sources• National Quality Forum (NQF)
• National Committee for Quality Assurance (NCQA)—HEDIS measures
• Physician Consortium for Performance Improvement (PCPI)
Examples—process or outcome related
• Diet and exercise plan discussed and noted in chart (process)
• Patients with type 2 diabetes with most recent LDL-C < 100 mg/dL (outcomes)
Cardiometabolic (CM) Syndrome
Working Definition:
• A clustering of risk factors predisposing individuals to cardiovascular and metabolic disease (type 2 diabetes)
Kahn R, et al. Diabetes Care. 2005;28:2289-304. Grundy SM, et al. Circulation. 2005;112:2735-40.Lui L, et al. J Clin Metab Diabetes. August 2011; http://www.slm-jcmd.com.
CM syndrome increases cardiovascular morbidity and mortality by 3- to 4-fold
Nearly one-third of Americans > 35 years old may have CM syndrome
Cardiometabolic Risk (CMR) Profile
Adapted from Barnett AH. Diabetes Vasc Dis Res. 2008;5:9-14.American Diabetes Association; 2007. http://professional.diabetes.org.
CMR
CVDDiabetes
Insulin Resistance
• LDL• Non-HDL• HDL• Triglycerides
Metabolic Syndrome
Overweight/Obesity/Waist Circumference
Age, Race, Sex, Genetics
Abnormal LipidMetabolism
Smoking,Physical Inactivity
Hypertension
Inflammation,Hypercoagulation
Lipids BP Glucose
Renal:• CKD
• AlbuminuriaNeed to treat risk factors
as a whole
Definition of CM Syndrome
NCEP ATP III. Circulation. 2002;106:3143-3421.
ATP III – 3 of 5 Risk Factors
Waist Circumference*≥ 40 in. or 102 cm (men)≥ 35 in. or 88 cm (women)
Triglycerides (TG) ≥ 150 mg/dLHigh-Density Lipoprotein Cholesterol (HDL-C)
< 40 mg/dL (men)< 50 mg/dL (women)
Blood Pressure (BP) ≥ 130/85 mm HgFasting Blood Glucose (FBG) ≥ 100 mg/dL
* Depends on ethnicity
Case Presentation – Part 1

3
Case Presentation – RG
• 55-y.o. WF comes for a routine physical examination• Pre-menopausal, takes no medication, is sedentary,
and reports she smokes cigarettes occasionally • She reports no personal history of cardiovascular
disease• Family history
- Parents are 72 and 74 years old; both have type 2 diabetes (T2DM)
- Father developed CHD at age 60; mother had a stroke at age 66; mother is currently on dialysis
- She has two brothers; one has T2DM- She also has four children, all of whom are obese; her
17-year-old daughter has been told that she has “pre-diabetes”
RG Case Presentation, Cont.
• Physical Examination- BP 138/88 mm Hg- Pulse 72- Weight 200 lb- Height 5’4”- BMI 34.4 kg/m2
- Waist 42”- Cardiac examination is
normal- Abdomen is obese
• Lab Results- FBG: 107 mg/dL- TC: 248 mg/dL- TG: 130 mg/dL- LDL-C: 162 mg/dL- HDL: 38 mg/dL- A1C: 6%- SCr: 0.7 mg/dL
Dyslipidemia, obesity, CM syndrome
Other diagnoses?
LDL Particles and Atherosclerosis
Fredrickson DS, et al. N Engl J Med. 1967;276:148-56.
• LDL particles: causal agents in atherosclerosis
• The more LDL particles, the higher the risk of plaque buildup
• More plaque buildup leads to greater risk of ACS, regardless of how much cholesterol the LDL particles carry
Rationale for therapeutic lowering of apoB lipoproteins: decrease the probability of inflammatory response to retention
Bloodapo B lipoproteinparticles
ModificationMacrophage
Monocytes bind toadhesion molecules
Smooth muscle
Cardiovascular Risk Increases With Increased Plasma apo B Lipoproteins
Foam cell
Inflammatory response
Tabas I, et al. Circulation. 2007;116:1832-44; Williams KJ, et al. Arterioscler Thromb Vasc Biol. 1995;15:551-61;Williams KJ, et al. Arterioscler Thromb Vasc Biol. 2005;25:1536-40; Hoshiga M, et al. Circ Res. 1995;77:1129-35;
Merrilees MJ, et al. J Vasc Res. 1993;30:293-302; Nakata A, et al. Circulation. 1996;94:2778-86; Steinberg D, et al. N Engl J Med. 1989;320:915-24.
What is Non–HDL-C?
HDL LDL IDL VLDLChylomicron
remnant
APOA-1 APOB APOB APOB APOB 48
CholesterolTriglyceride
BADGOOD All atherogenic lipoproteins
non-HDL
non–HDL-C =Total cholesterol − HDL-C
NCEP target level of non–HDL-C is 30 mg/dL greater than the LDL-C goal1
1. NCEP Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report Executive Summary. 2001; NIH Publication No. 01-3670.
Why Treat to Non–HDL-C Goals?
TG 120 mg/dL 400 mg/dLVLDL-C 24 mg/dL 88 mg/dL LDL-C 145 mg/dL 89 mg/dLHDL-C 40 mg/dL 32 mg/dLNon–HDL-C 169 mg/dL 177 mg/dLTG/HDL-C ratio 3.0 12.5TC 209 mg/dL 209 mg/dL
Case 1 Case 2
Cho
lest
erol
(mg/
dL)
50
100
150
200
225TC= 209 mg/dL
Non–HDL-C = 177 mg/dL
[Non–HDL-C goal = LDL-C goal + 30]
NCEP ATP III. JAMA. 2001;285:2486-97.
HDL HDL
LDLLDL
VLDLVLDL

4
Evidence-Based Performance MeasuresPreventive Care
Assessing / preventing CMR
• Waist circumference measured (ACCF / AHA)
• BMI measured (PCPI)
• Exercise plan (NCQA)
• Smoking assessed (PCPI)
• Smoking cessation plan in patients who smoke (PCPI)
Each of the above measures should be obtained / monitored at each visit & noted in patient chart
ACCF/AHA = American College of Cardiology Foundation / American Heart Association; NCQA = National Committee for Quality Assurance; PCPI = Physician Consortium for Performance Improvement.
NCEP Report Suggests the Need for More Intensive Therapy
• Based on statin trials published since 2001
• Key points:
- Treat according to global risk level, not only cholesterol value
- Achieve at least a 30% to 40% reduction in LDL-C regardless of baseline LDL-C
- Initiate therapeutic lifestyle changes (TLC) in all patients with lifestyle-related risk factors regardless of LDL-C level
NCEP = National Cholesterol Education Program. Grundy SM, et al. Circulation. 2004;110:227-239. NCEP ATP III. JAMA. 2001;285:2486-97.
• What LDL-C goal would you set for RG?
1. < 70 mg/dL2. < 100 mg/dL3. < 130 mg/dL4. < 160 mg/dL5. < 190 mg/dL
Audience Response Question ? Pre-Test Question #1
• The physician has decided not to do any additional testing in patient RG at this time. Which intervention should be done at this step?
1. No further interventions2. Therapeutic lifestyle changes (TLC) only3. TLC plus lipid therapy with a statin4. TLC plus lipid therapy with niacin5. Unsure
?
Updated ATP III LDL-C Goals and Cutpoints for Therapy
Risk Category
LDL-C (mg/dL)
Goal
Initiation Level for
TLCConsideration Level
for Drug TherapyHigh risk: CHD or CHD risk equivalents (10-yr risk >20%)
< 100 (optional: < 70)
≥ 100 ≥ 100(< 100: consider drug
options)
Moderately high risk: 2+ risk factors (10-yr risk 10–20%)
< 130 (optional: < 100)
≥130 ≥ 130(100–129: consider
drug options)
Moderate risk:2+ risk factors(10-yr risk <10%)
< 130 ≥130 ≥160
Lower risk:0–1 risk factor
< 160 ≥160 ≥ 190 (160–189: LDL-C–
lowering drug optional)
Grundy SM, et al. Circulation. 2004;110:227-39.
Consider drug options if below goal, but above goal for next higher risk level
Standard Dietary Recommendations for Weight Reduction
• Reduce intake by 500–1000 kcal/day to lose 0.5–1.0 kg/wk
• Balanced deficit diet with:- ≤ 10% kcal from saturated fat- < 300 mg/day of cholesterol- ≤ 2400 mg/day of sodium- ≥ 20–30 g/day of fiber
Carbohydrate:≥ 55% of kcal
Protein: ~ 15% of kcal
Fat: ≤ 30% of kcal
NIH/NHLBI, NAASO. The Practical Guide: Identification, Evaluation, and Treatment of Overweight and Obesity in Adults. 2000. NIH Publication Number 00-4084.
5
Lipid-Lowering Pharmacotherapy
*Average reduction based on 20 or 40 mg of statin drug
Therapy TC LDL-C HDL-C TG
Statins* 19 – 37% 25 – 50% 4 – 12% 14 – 29%
Ezetimibe 13% 18% 1% 9%
Bile acid sequestrants 7 – 10% 10 – 18% 3% Neutral or
Nicotinic acid 10 – 20% 10 – 20% 14 – 35% 30 – 70%
Fibrates 19% 4 – 8% 11 – 13% 30%
Yeshurun D, et al. South Med J. 1995;88:379–391. | NCEP. Circulation. 1994;89:1333–445. | Knopp RH. N Engl J Med. 1999;341:498–511. | Gupta EK, et al. Heart Dis. 2002;4:399–409.
Downs JR, et al. JAMA. 1998;279:1615-22. | Shepherd J, et al. N Engl J Med.1999;333:1301-7. | Scandinavian Simvastatin Study Group. Lancet. 1994;344:1383-9. |
Sacks FM, et al. N Engl J Med. 1996;335:1001-9. | LIPID Study Group. N Engl J Med. 1998;339:1349-57. | Schwartz GG, et al.
JAMA. 2001;285:1711-8. | Pitt B, et al. N Engl J Med. 1999;341:70-6.
Endpoint Trials With Statins
Trial Drug CHD Risk ReductionPrimary Prevention
AFCAPS/TexCAPS Lovastatin –40%*WOSCOPS Pravastatin –31%*
Secondary Prevention4S Simvastatin –34%*CARE Pravastatin –24%*LIPID Pravastatin –24%*
IschemiaMIRACL Atorvastatin –26%**AVERT Atorvastatin –36%**
*Nonfatal MI or CHD death; **ischemic events
Comparable Efficacy of Statins
Special considerations:• No renal dosing: atorvastatin and fluvastatin• Use in chronic liver disease: pravastatin or rosuvastatin• Less drug interactions: pravastatin, fluvastatin, rosuvastatin (not metabolized via CYP3A4)• Less muscle toxicity: pravastatin and fluvastatin• Cost-effectiveness: rosuvastatin, atorvastatin, fluvastatin
Statin Drug (mg)
Rosuva-statin
Atorva-statin
Simva-statin
Lova-statin
Prava-statin
Fluva-statin
Pitava-statin
Serum CholesterolTotal LDL
– – 10 20 20 40 1 22% 27%
– 10 20 40 40 80 2 27% 34%
5 20 40 80 80 – 4 32% 41%
10 40 80 – – – – 37% 48%
20 80 – – – – – 42% 55%
40 – – – – – – 47% 63%
Facts and Comparisons Online, 2011www.factsandcomparisons.com.
Statins – Safety Considerations• Common side effects
– Headache – Myalgia – Fatigue– GI intolerance – Flu-like symptoms
• Increase in liver enzymes- 0.5% to 2.5% of cases in dose-dependent manner- Serious liver problems are rare- Manage by reducing statin dose or discontinue until levels return to
normal• Myopathy
- 0.2% to 0.4% of patients; rare cases of rhabdomyolysis- Reduce by
• Cautious use in impaired renal function; using lowest effective dose; cautiously combining statins with fibrates; careful monitoring of symptoms
- Presence of true muscle toxicity requires the discontinuation of the statin
Facts and Comparisons Online, 2011www.factsandcomparisons.com.
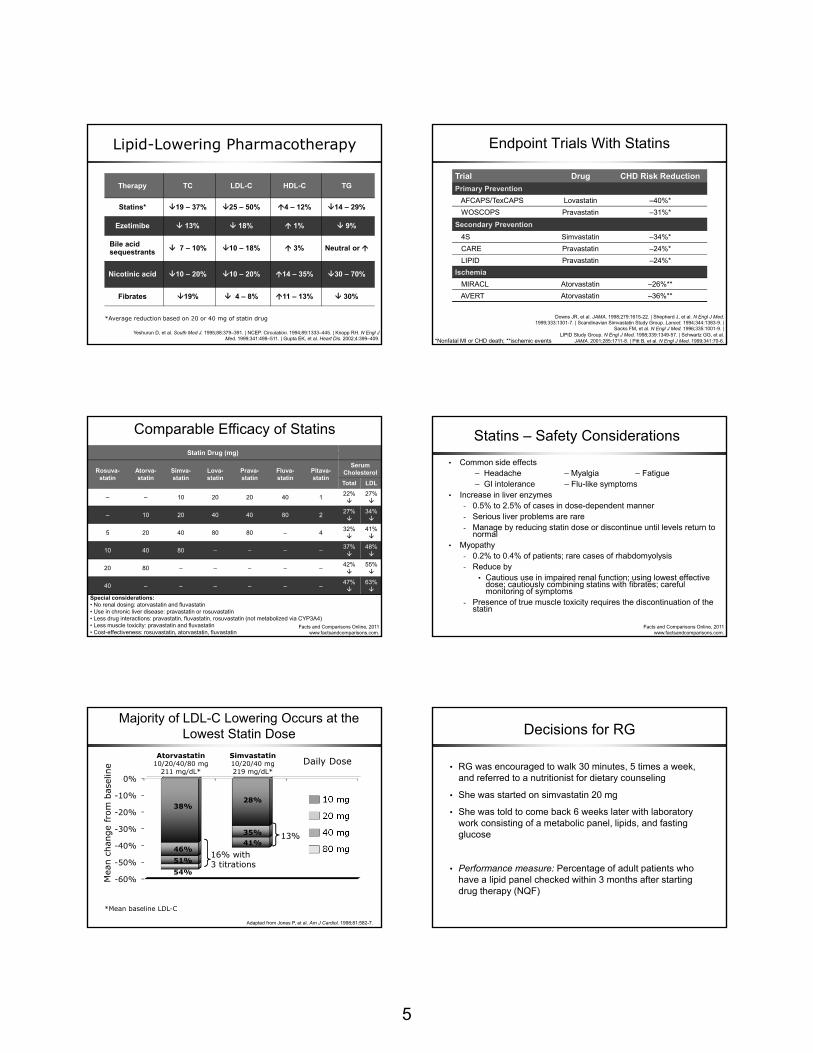
Atorvastatin10/20/40/80 mg
211 mg/dL*
Simvastatin10/20/40 mg219 mg/dL*
Majority of LDL-C Lowering Occurs at the Lowest Statin Dose
Adapted from Jones P, et al. Am J Cardiol. 1998;81:582-7.
*Mean baseline LDL-C
Daily Dose
10 mg
20 mg
40 mg
80 mg
-60%
-50%
-40%
-30%
-20%
-10%
0%
16% with3 titrations
13%
54%
38%
46%51%
28%
35%41%
Decisions for RG
• RG was encouraged to walk 30 minutes, 5 times a week, and referred to a nutritionist for dietary counseling
• She was started on simvastatin 20 mg
• She was told to come back 6 weeks later with laboratory work consisting of a metabolic panel, lipids, and fasting glucose
• Performance measure: Percentage of adult patients who have a lipid panel checked within 3 months after starting drug therapy (NQF)

6
Practical Patient Care StrategiesPatient Care Tools
• Physical Activity and Nutrition Adherence Interview
• Daily Food Diary• Visual Cues for Portion
Sizes• Grocery Shopping List
Template• Exercise Tracker
https://pri-med.pi-iq.com
Case Presentation – Part 2
Dyslipidemia Management in the Evolving Complex Patient – Case Cont.
• Previous- FBG: 107 mg/dL- TC: 248 mg/dL- TG: 130 mg/dL- LDL-C: 162 mg/dL- HDL: 38 mg/dL- SCr: 0.7 mg/dL
• Current- FBG: 140 mg/dL- TC: 180 mg/dL- HDL-C: 48 mg/dL- LDL-C: 97 mg/dL- TG: 110 mg/dL- SCr: 1.0 mg/dL- Urinalysis: 1+ protein- GFR: 63 mL/min/1.73 m2
- A1C: 7.8%
• It is 6 months later
• RG returns and reports that she has lost 8 pounds through exercise, but has made few changes in her diet. Her blood pressure is now 130/80 mm Hg. However, she now complains of increasing thirst and urinary frequency.
• Lab results:
Case Cont.
New considerations for RG:
• Potential diagnoses- Diabetes- Renal insufficiency- Persistent dyslipidemia
• Changes in goals?
• Changes in treatment?
Pre-Test Question #2
• Which of the following is the best course of action to manage RG’s lipid profile at this time?
1. Maximize her simvastatin dose 2. Add gemfibrozil to her simvastatin3. Add ezetimibe to her simvastatin4. Discontinue her simvastatin and start either gemfibrozil
or ezetimibe5. Unsure
?
Fasting glucose
Type 2 diabetes
Years from diagnosis
0 5–10 –5 10 15
Pre-diabetes
Onset Diagnosis
Postprandial glucose
Macrovascular complications
Adapted from Holman RR. Diabetes Res Clin Pract. 1998;40(suppl):S21-S25.Ramlo-Halsted BA, Edelman SV. Prim Care. 1999;26:771-89.
Nathan DM. N Engl J Med. 2002;347:1342-9; UKPDS Group. Diabetes. 1995;44:1249-58.
Microvascular complications
Insulin resistanceInsulin secretion
β-cell function
Progression to Type 2 Diabetes

7
Selection of Patients for More Aggressive LDL-Lowering: Risk Curve Concept
Robinson JG, Stone NJ. Am J Cardiol. 2006;98:1405-8.
0
Car
diov
ascu
lar
Even
t Rat
e (%
)
0 20 40 60 80 100 120 140 160 180 200
LDL (mg/dL)
No CVD - No Diabetes
Diabetes - No CVD
CHD – No CMS or IFG
CHD + CMS or IFG
CHD + Diabetes
80
70
60
50
40
30
20
10
CHD = coronary heart disease; CMS = cardiometabolic syndrome; IFG = impaired fasting glucose.
Why Is Screening for Nephropathy Important?
• Microalbuminuria: independent marker of ↑CHD risk
• Early intervention with effective treatments can slow progression of kidney dysfunction
• Diabetes-related nephropathy: leading cause of ESRD
– 7% have microalbuminuria at diagnosis
– ~ 20% to 40% will eventually develop diabetic nephropathy
– Of patients with nephropathy, 20% will eventually develop ESRD
Klausen K, et al. Circulation. 2004;110:32-5.Adler AI, et al. Kidney Int. 2003;63:225-32.
Molitch ME, et al. Diabetes Care. 2004;27(suppl 1):S79-83.ADA. Diabetes Care. 2011;34(suppl 1):S11-61.
Calculating eGFR
www.kidney.org/professionals/kdoqi/gfr_calculator.cfm
NKF’s KDOQI guidelines recommend MDRD Study Equation to estimate GFR
CKD EPI & MDRD GFR Calculator – (With SI Units)4 variable MDRD CKD EPI Equation (with SI units)
using standardized serum creatinine, age, race, gender
Serum creatinine 1.0mg/dL μmol/L
Age 56
Race African American All other races
Gender Male Female
Traceable to IDMS Yes No
CKD EPI Value: 63 mL/min/1.73 m2 in a 56-y.o. white female
Stage Description GFR (mL/min/1.73 m2)
1 Kidney damage with normal or GFR ≥ 90
2 Kidney damage with mild ↓ GFR 60‐89
3 Moderate ↓ GFR 30‐59
4 Severe ↓ GFR 15‐29
5 Kidney failure < 15 (or dialysis)
CKD is defined as either kidney damage or GFR of < 60 mL/min/1.73 m2 for ≥ 3 months. Kidney damage is defined as pathologic abnormalities or markers of damage, including abnormalities in the blood or urine tests or imaging studies.
NKF / KDOQI. Am J Kidney Dis. 2002;39(suppl 1):S1-S266.
Stages of CKD
Microalbuminuria Screening Algorithm
KDOQI. 2007. http://www.kidney.org/professionals/kls/pdf/tool12-10-2089.pdf.
*Exercise within 24 hours, infection, fever, congestive heart failure, marked hyperglycemia, pregnancy, marked hypertension, urinary tract infection, hematuria.
No
No
No
No
Yes
Yes
Yes
Yes
Yes
Test for microalbuminuria
+ for albumin
Condition that may invalidate* urine albumin excretion
Treat and/or wait until resolved Repeat test
+ for protein?
Repeat microalbuminuria test twice within 3- to 6-month period
2 of 3 tests positive?
Microalbuminuria, begin treatment
Rescreen in 1 year
Evidence-Based Performance MeasuresKidney Function and Lipid Control in T2DM
• Microalbumin testing (urine protein screening) at least once during past year (NCQA)
• Patients who had at least one creatinine screening or eGFR during past year (NQF, BMA)
• One or more lipid profiles within the last year (HEDIS)
• Patients with T2DM with most recent LDL-C < 100 mg/dL (HEDIS)
• Lifestyle modification and lipid-lowering agent if LDL-C > 100 mg/dL (NQF)
BMA = British Medical Association; HEDIS = Healthcare Effectiveness Data and Information Set; NQF = National Quality Forum.
8
Prevalence of CVD in CKD
• CVD is present in the majority of patients with CKD and is the leading cause of mortality
• High prevalence suggests CVD develops in early CKD
• Pathophysiologic process involves atherosclerosis, arteriosclerosis, and cardiomyopathy involving altered lipid metabolic pathways that result in oxidative stress, inflammation, and dyslipidemia
• To improve outcomes – early intervention with targeted lipid therapy
USRDS. www.usrds.org/2009/pdf/V1_01_09.PDF.Shastri S, et al. Am J Kidney Dis. 2010;56:399-417.
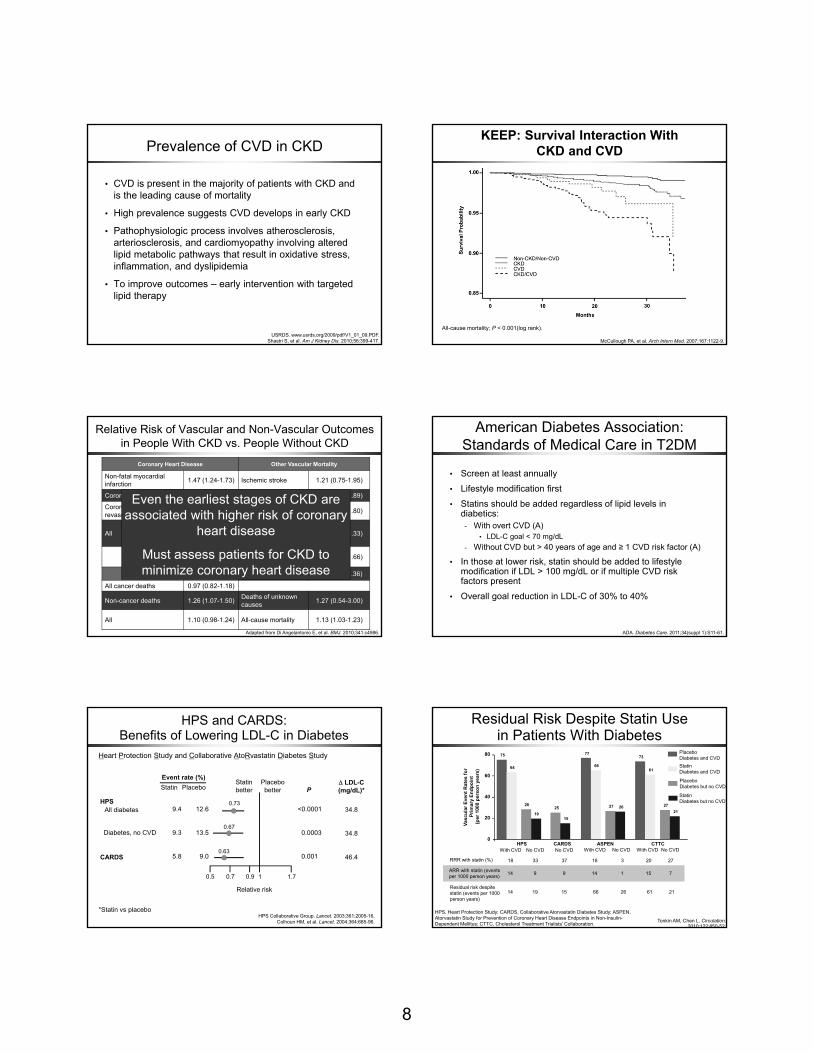
KEEP: Survival Interaction With CKD and CVD
McCullough PA, et al. Arch Intern Med. 2007;167:1122-9.
All-cause mortality; P < 0.001(log rank).
Relative Risk of Vascular and Non-Vascular Outcomes in People With CKD vs. People Without CKD
Coronary Heart Disease Other Vascular Mortality
Non-fatal myocardial infarction 1.47 (1.24-1.73) Ischemic stroke 1.21 (0.75-1.95)
Coronary deaths 1.21 (0.98-1.48) Hemorrhagic stroke 1.02 (0.55-1.89)
Coronary revascularization 1.54 (1.17-2.01) Unclassified stroke 1.18 (0.77-1.80)
All 1.45 (1.29-1.62)Other cerebrovascular deaths
0.71 (0.37-1.33)
Other cardiovascular deaths 1.22 (0.89-1.66)
Non-Vascular Mortality All 1.11 (0.92-1.36)
All cancer deaths 0.97 (0.82-1.18)
Non-cancer deaths 1.26 (1.07-1.50) Deaths of unknown causes 1.27 (0.54-3.00)
All 1.10 (0.98-1.24) All-cause mortality 1.13 (1.03-1.23)
Adapted from Di Angelantonio E, et al. BMJ. 2010;341:c4986.
Even the earliest stages of CKD are associated with higher risk of coronary
heart disease
Must assess patients for CKD to minimize coronary heart disease
American Diabetes Association: Standards of Medical Care in T2DM
ADA. Diabetes Care. 2011;34(suppl 1):S11-61.
• Screen at least annually
• Lifestyle modification first
• Statins should be added regardless of lipid levels in diabetics:
- With overt CVD (A)• LDL-C goal < 70 mg/dL
- Without CVD but > 40 years of age and ≥ 1 CVD risk factor (A)
• In those at lower risk, statin should be added to lifestyle modification if LDL > 100 mg/dL or if multiple CVD risk factors present
• Overall goal reduction in LDL-C of 30% to 40%
HPS and CARDS: Benefits of Lowering LDL-C in Diabetes
HPS Collaborative Group. Lancet. 2003;361:2005-16.Colhoun HM, et al. Lancet. 2004;364:685-96.
Δ LDL-C(mg/dL)*
34.8
46.4
Statinbetter
Placebobetter
All diabetesHPS
CARDS
Relative risk
0.5 0.7 0.9 1
<0.0001
0.0003
0.001
Event rate (%)
12.6
13.5
9.0
Placebo
9.4
9.3
5.8
Statin
0.63
0.67
0.73
P
Diabetes, no CVD
1.7
*Statin vs placebo
34.8
Heart Protection Study and Collaborative AtoRvastatin Diabetes Study
Residual Risk Despite Statin Use in Patients With Diabetes
Tonkin AM, Chen L. Circulation. 2010;122:850-52.
HPS, Heart Protection Study; CARDS, Collaborative Atorvastatin Diabetes Study; ASPEN, Atorvastatin Study for Prevention of Coronary Heart Disease Endpoints in Non-Insulin-Dependent Mellitus; CTTC, Cholesterol Treatment Trialists’ Collaboration.
Placebo Diabetes and CVD Statin Diabetes and CVD
PlaceboDiabetes but no CVD
StatinDiabetes but no CVD
80 75 77
60
40
20
0HPS CARDS ASPEN CTTC
64
28
1925
15
66
27 26
73
61
2721
Vasc
ular
Eve
nt R
ates
for
Prim
ary
Endp
oint
(per
100
0 pe
rson
yea
rs)
RRR with statin (%)
With CVD No CVD
18 33 37 18 3 20 27
ARR with statin (events per 1000 person years) 14 9 9 14 1 15 7
No CVD With CVD No CVD With CVD No CVD
Residual risk despite statin (events per 1000 person years)
14 19 15 66 26 61 21

9
Combination Lipid-Lowering Strategies
• Consider combination therapy if:- Lipid goals not met; higher statin dose not well tolerated- “Rule of 6” – doubling statin dose generally achieves a
reduction of LDL-C of ~ 6% over starting dose reduction
• Statins + bile acid resins or ezetimibe- ↓LDL-C > 50%
• Fibrates, niacin, omega-3 fatty acids- ↓Triglycerides and non-HDL-C; ↑HDL-C
• Combination therapy may increase risk for drug interactions and myopathy
- Simvastatin and gemfibrozil combination now contraindicated
Vasudevan AR, Jones PH. Curr Cardiol Rep. 2005;7:471–9.FDA Drug Safety Communication. http://www.fda.gov/Drugs/DrugSafety/ucm256581.htm.
Safety Factors in Therapy Selection
• Fibrates- Potential for increased creatinine with fibrates (less with
gemfibrozil), dyspepsia, gallstones, myopathy• Nicotinic acid
- Flushing, hyperglycemia, hepatotoxicity (cannot use if liver disease and peptic ulcer disease), increased uric acid
• Cholesterol absorption inhibitors- Low incidence of side effects when used alone, slightly
higher incidence of myopathy and transaminitis when used with statins
• Bile acid sequestrants- Gastrointestinal upset, nausea, bloating, constipation,
impaired absorption of other drugs (such as warfarin and fat-soluble vitamins)
Bruckert E, et al. Cardiovasc Drugs. 2005;19:403-14; Brown WV. Curr Opin Lipidol. 2008;19:558-62; Onusko E. J Fam Pract. 2008;57:449-52; Navaneethan SD, et al. Cochrane Database Syst Rev. 2009:CD007784.
Treating RG’s DiabetesAACE Algorithm
A1C 7.6% to 9.0%
MET +
GLP-1or DPP-4
+ TZD
GLP-1or DPP-4 + SU
TZD
Triple Therapy
MET +
GLP-1 or DPP-4 or TZD
SU or Glinide
Dual Therapy
RG’s A1C = 7.8%; FG = 130 mg/dL
Available at www.aace.com/publications
© AACE October 2009
2 to 3 months
Insulin±Other Agent(s)
2 to 3 months
Decisions for RG
• RG’s LDL-C goal was set at < 70 mg/dL
• RG’s A1C goal is < 7.0%
• Treatment plan:- Continue exercise and diet plan- For dyslipidemia, ezetimibe was added to her simvastatin- For T2DM, she was started on metformin plus a
sulfonylurea- RG to return in 4 weeks for glucose review and in 3
months for A1C testing• Her A1C remained above goal at the 3-month point – her
sulfonylurea was discontinued and sitagliptin (a DPP-4 inhibitor) was started
Case Presentation – Part 3
Dyslipidemia Management in CKD – Case Cont
• Previous- A1C: 7.8% - FBG: 130 mg/dL- TC: 180 mg/dL- HDL-C: 48 mg/dL- LDL-C: 97 mg/dL- TG: 110 mg/dL- SCr: 1.0 mg/dL- Urinalysis: 1+ protein- GFR: 63 mL/min/1.73 m2
• Current- A1C: 7.3% - FBG: 114 mg/dL- PPG: 120 to 160 mg/dL*- HDL-C: 50 mg/dL- LDL-C: 90 mg/dL- TG: 108 mg/dL- AST: 18; ALT: 30- SCr: 1.5 mg/dL- GFR : 38 mL/min/1.73 m2
• It is now 6 months later
• She reports difficulties adhering to medical regimen, citing some muscle cramping and forgetfulness
• Lab tests:
* Postprandial glucose based on self-monitoring blood glucose

10
Stage Description GFR (mL/min/1.73 m2)
1 Kidney damage with normal or GFR ≥ 90
2 Kidney damage with mild ↓ GFR 60‐89
3 Moderate ↓ GFR 30‐59
4 Severe ↓ GFR 15‐29
5 Kidney failure < 15 (or dialysis)
CKD is defined as either kidney damage or GFR of < 60 mL/min/1.73 m2 for ≥ 3 months. Kidney damage is defined as pathologic abnormalities or markers of damage, including abnormalities in the blood or urine tests or imaging studies.
NKF / KDOQI. Am J Kidney Dis. 2002;39(suppl 1):S1-266.
Stages of CKD CKD as a CHD Risk Equivalent
• In NHANES, for patients with CKD-3:- 53.0% had a history of CHD or a
risk equivalent• 24.7% reported a history of
myocardial infarction or stroke• 17.7% had diabetes• 9.6% had angina• 26.9% had a 10-year CHD
risk greater than 20%- Per current ATP III guidelines,
lipid-lowering therapy is recommended for 61.4% of adults with moderate CKD
- If CKD-3 is reclassified as a CHD risk equivalent (figure), this percentage would increase to 87.7%
0
10
20
30
40
50
60
70
80
90
61.4
31.6
87.7 87.7
% o
f pat
ient
s re
com
men
ded
lipid
lo
wer
ing
trea
tmen
t
CurrentGuidelines
CKD as CHDrisk equivalent
Hyre AD, et al. Am J Kidney Dis. 2007;49:7-45.NHANES = National Health and Nutrition Examination Survey.
CKD 3 without CHD or risk equivalents
All CKD 3
Metabolic and Pathologic Comorbidities Appear in CKD Stage 3
Acid-Base
Anemia
Mineral / Bone
Disorder
Vascular Calcification
↑Insulin Resistance
Dyslipidemia
Hypertension
_
_
_
_
_
_
_
_
_
Andress DL. Semin Dial. 2005;18:315-21.; Becker B, et al. J Am Soc Nephrol. 2005;16:1091:8. McClellan, et al. Cur Med Res Op. 2004;20:1501-10.; Kramer H, et al. J Am Soc Nephrol. 2005;16:507-13.
NKF / KDOQI. Am J Kidney Dis. 2002;39(suppl 1):S1-266.
≥ 90 60 - 89 30 - 59 15 - 29 < 150
1
2
3
4
5
6
7
8
CKDStage 1 CKD
Stage 2
CKDStage 3
CKDStage 4
CKDStage 5N
umbe
r of P
atie
nts
(Mill
ions
)
Goals of Therapy for CVD in CKD
• Delay CVD progression
• Delay progression to ESRD
• Balance the need to optimize effectiveness while minimizing adverse effects
Pre-Test Question #3
• Which of the following treatments have demonstrated a reduction in cardiovascular events in clinical trials of patients with severe CKD?
1. Atorvastatin
2. Rosuvastatin + ezetimibe
3. Atorvastatin + colesevelam
4. Simvastatin + ezetimibe
5. Unsure
? NKF K/DOQI:Clinical Practice Guidelines for Dyslipidemia in CKD
• Guideline 1- All CKD patients should be evaluated for dyslipidemias (B)- Test should be done after the patient has fasted and should
include measurements of total cholesterol, LDL, HDL, and triglycerides (B)
- For CKD-5 patients, dyslipidemias should be evaluated upon presentation, 2-3 months after change in treatment, and at least annually thereafter
• Guideline 2- For CKD-5 patients, measurement preferably should be done
after an overnight fast (B)- For hemodialysis patients, measurement should be pre-HD or
on non-HD days (B)• Guideline 3
- CKD-5 patients with dyslipidemias should be evaluated for remediable, secondary causes (B)
NKF / KDOQI. Am J Kidney Dis. 2003;41(Suppl 3):S1-93.
11
NKF K/DOQI:Clinical Practice Guidelines for Dyslipidemia in CKD
Dyslipidemia Goal Initial Therapy
Triglycerides ≥ 500 mg/dL < 500 mg/dL Lifestyle ± fibrate or niacin
LDL-C > 100-129 mg/dL < 100 mg/dL Lifestyle
LDL-C ≥ 130 mg/dL < 100 mg/dL Lifestyle + low-dose statin
TG ≥ 200 mg/dL and non-HDL ≥ 130 mg/dL
Non-HDL < 130 mg/dL Lifestyle + low-dose statin
NKF / KDOQI. Am J Kidney Dis. 2003;41(4 suppl 3):S1-93.
Guideline 4
NKF K/DOQI:Clinical Practice Guidelines for CVD in Dialysis
• Guideline 13- Association between dyslipidemia and CVD in dialysis patient
(weak)- Indirect evidence supports lipid lowering in CKD- Acknowledge NCEP ATP III update regarding lowering LDL-C
to < 70 mg/dL in very-high-risk patients
NKF / KDOQI. Am J Kidney Dis. 2005;45(suppl 3):S1-156.
Effects of Statins on Cardiovascular Outcomes in CKD/ESRD Patients
• 4D: Der Deutsche Diabetes Dialysis Studie– n = 1,255 CKD patients; atorvastatin 20 mg vs.
placebo; 4-year follow-up• AURORA: A Study to Evaluate the Use of Rosuvastatin
in Subjects on Regular Hemodialysis: An Assessment of Survival and Cardiovascular Events– n = 2,776 CKD patients on dialysis; rosuvastatin 10
mg vs. placebo; 3.8-year follow-up
• Primary CV composite endpoint showed no benefit with either atorvastatin or rosuvastatin therapy in these patients
• Take home: study findings left it unclear how to manage patients with severe CKD
Wanner C, et al. N Engl J Med. 2005;353:238-48. Fellstrom BC, et al. N Engl J Med. 2009;360:1395-1407.
Choudhury D, et al. Semin Nephrol. 2009;29:610-20.
Evolving Concepts: SHARP TrialStudy of Heart and Renal Protection
• Evaluated the CV effects of lipid-lowering therapies in patients with CKD
• Eligibility: history of CKD- Not on dialysis: SCr - men: ≥ 1.7 mg/dL; women: ≥ 1.5 mg/dL- On dialysis: hemodialysis or peritoneal dialysis
• Randomization- Ezetimibe 10 mg plus simvastatin 20 mg daily - Simvastatin 20 mg daily - Placebo
• Primary endpoint: major atherosclerotic events—coronary death, MI, non-hemorrhagic stroke, or any revascularization
• Secondary endpoint: ESRD
Presented at American Society of Nephrology Meeting, November 20, 2010. http://www.ctsu.ox.ac.uk/~sharp/.
0 1 2 3 4 5 Years of Follow-up
0
5
10
15
20
25
Prop
ortio
n su
fferin
g ev
ent (
%)
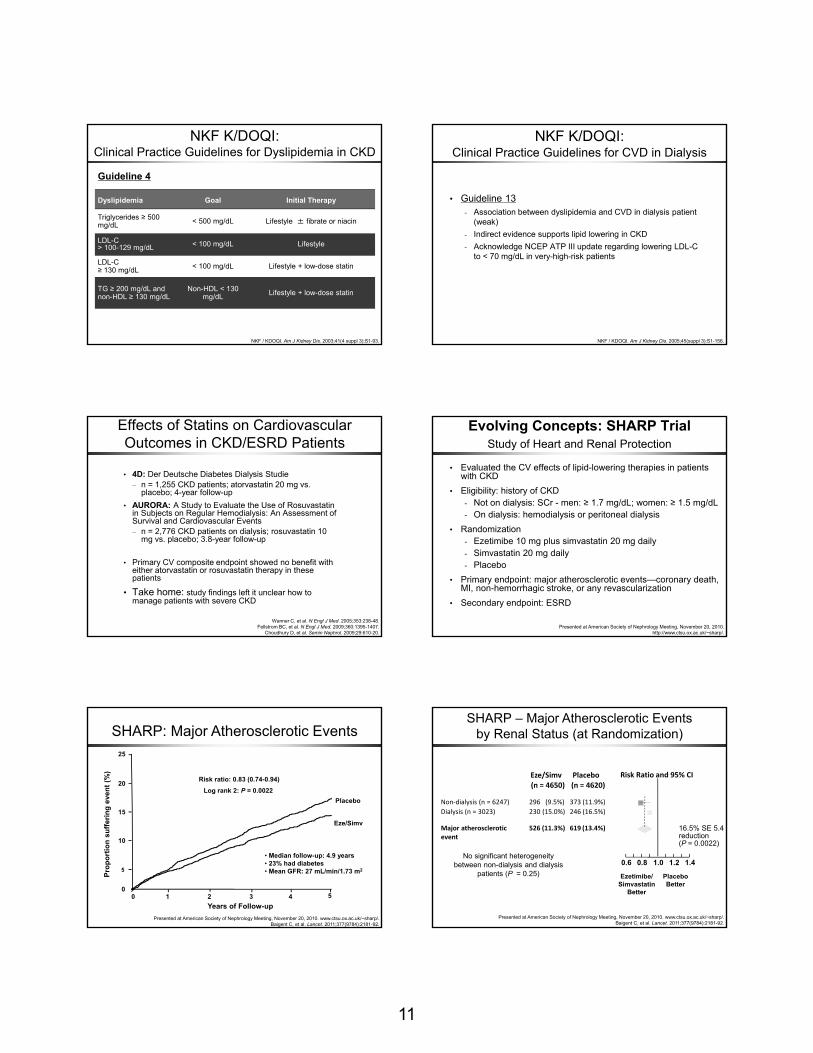
Risk ratio: 0.83 (0.74-0.94) Log rank 2: P = 0.0022
Placebo
Eze/Simv
SHARP: Major Atherosclerotic Events
Presented at American Society of Nephrology Meeting, November 20, 2010. www.ctsu.ox.ac.uk/~sharp/.Baigent C, et al. Lancet. 2011;377(9784):2181-92.
• Median follow-up: 4.9 years• 23% had diabetes• Mean GFR: 27 mL/min/1.73 m2
Risk Ratio and 95% CIPlaceboEze/Simv
Ezetimibe/Simvastatin
Better
Placebo Better
(n = 4620)(n = 4650)
Non‐dialysis (n = 6247) 296 (9.5%) 373 (11.9%) Dialysis (n = 3023) 230 (15.0%) 246 (16.5%)
Major atherosclerotic event
526 (11.3%) 619 (13.4%) 16.5% SE 5.4 reduction (P = 0.0022)
0.6 0.8 1.0 1.2 1.4
SHARP – Major Atherosclerotic Eventsby Renal Status (at Randomization)
No significant heterogeneity between non-dialysis and dialysis
patients (P = 0.25)
Presented at American Society of Nephrology Meeting, November 20, 2010. www.ctsu.ox.ac.uk/~sharp/.Baigent C, et al. Lancet. 2011;377(9784):2181-92.

12
SHARP: Safety
Adverse Effect Eze/Simv (n = 4,650)
Placebo ( n = 4,620)
Myopathy
CK > 10 but ≤ 40 x ULNCK > 40 x ULN
17 (0.4%)4 (0.1%)
16 (0.3%)5 (0.1%)
Hepatitis 21 (0.5%) 18 (0.4%)
Persistently elevated LFTs 30 (0.6%) 26 (0.6%)
Gallstone complications 85 (1.8%) 76 (1.6%)
Pancreatitis without gallstones 12 (0.3%) 17 (0.4%)
Presented at American Society of Nephrology Meeting, November 20, 2010. www.ctsu.ox.ac.uk/~sharp/.
No significant difference in cancerrisk ratio 0.99 (0.87-1.13); log rank 2P = 0.89
LFTs = liver function tests; ULN = upper limit of normal.
Take-Home Points From SHARP
• There is a clear benefit to LDL-lowering with a statin plus ezetimibe in people who are not on dialysis- Patients with GFR between 45 and 15 mL/min/1.73m2
- Possible benefit in patients on dialysis
• Lipid-lowering therapy reduced the risk of first cardiovascular event (non-fatal MI, stroke, cardiac death, or revascularization) by 16.1% (P = 0.001)
- Consider LDL goal of ≤ 70 mg/dL in patients with CKD
Take-Home Points From SHARP
• Patients with diabetes should be recognized as being at high risk of adverse outcomes and eligible for lipid-lowering therapy, regardless of baseline LDL cholesterol levels
• Adverse-effect profile of combination lipid-lowering therapy was comparable with placebo
- No significant difference in cancer
• In renally impaired patients, consider combination lipid lowering therapies rather than maximizing statin doses
Lipid-Altering Therapies for the CKD Patient
LDL-C Reduction
• Statins are first-line therapy
– Statins are safe to use in CKD as long as appropriate dosage adjustments are made based on renal function
– Use caution with highest doses of statins, as side effects increase with statin dose and limited added benefit
• Add: ezetimibe or colesevelam for further LDL reduction
– Ezetimibe— no dose adjustment needed in CKD
– Colesevelam—increases TG; contraindicated if TG > 400
Key point: Beneficial to use multiple low doses of drugs rather than a high dose of a single drug in CKD patients
SHARP study; Individual Drug Prescribing Information; Jones P, et al. Am J Cardiol. 1998;81:582-7.
Other Factors in Therapy Selection
• Safety – dosing reductions
• Adherence – dosing convenience
• Drug interactions with statins (cyclosporine, azole antifungals, fibrates, nicotinic acid, macrolide antibiotics, calcium channel blockers)
• Potential for combination therapy
Farnier M, et al. Am Heart J. 2010;160:785-94.
Doses of Lipid Therapies in CKD
Adjust for Reduced GFR (mL/min/1.73 m2)Notes
Agent 60-90 15-59 < 15Atorvastatin No No NoFluvastatin ? ? ?Lovastatin No ↓ to 50% ↓ to 50%Pravastatin No No No Not metabolized by p450Simvastatin ? ? ?Nicotinic acid No No ↓ to 50% 34% Kidney excretionEzetimibe No No NoColestipol No No No Not absorbedCholestyramine No No No Not absorbedColesevelam No No No Not absorbedFenofibrate ↓ to 50% ↓ to 25% Avoid May ↑ serum creatinineGemfibrozil No No No May ↑ serum creatinine
Am J Kidney Dis. 2003;41(suppl 3):S1-93.

13
Reasonable Algorithm for Treatment of CVD in CKD
TG≥ 500?
LDL≥ 100?
LDL≥ 130?
LDL≥ 100
(or 70)?
TLC and considera fibrate or niacin
Consider niacin, ezetimibe, or bile acid sequestrant
TLC
TLC + statin
TLC + statin
+/-eze or niacin
Continueto monitor
LDL100-129?
LDL≥ 100?
TG ≥ 200 and Non-HDL
Chol.≥ 130?
No No No
No
No
No
No
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Modified from Am J Kidney Dis. 2003;41(suppl 3):S1-93.
TLC
Reports of Adherence
• Electronic monitoring- Overall Adherence: 71%
• Once daily dosing: 79%• Twice daily dosing: 69%• 3x daily dosing: 65%• 4x daily dosing: 51%
• Tracking electronic prescribing- New Prescriptions: 72% filled
• Dyslipidemia: 71.8% filled• Hypertension: 71.6% filled• Diabetes: 68.9% filled
Claxton AJ. Clin Ther. 2001;23:1296-1310.Fischer MA, et al. J Gen Intern Med. 2010;25:284-90.
Major Predictors of Poor Adherence
• Psychological problems, especially depression
• Cognitive impairment
• Treatment of asymptomatic disease
• Inadequate follow-up or discharge planning
• Side effect concerns
• Patient’s lack of belief in treatment
• Patient’s lack of insight into pathophysiology of disease
• Poor provider-patient relationship
• Presence of barriers to care or medications
• Complex regimens
• Costs (medication, copayment, or both)
Osterberg L, Blaschke T. N Engl J Med. 2005;353:487-97.
Decisions for RG
• RG’s LDL-C goal is < 70 mg/dL and A1C goal is < 7.0%
• Treatment plan:- Continue simvastatin and ezetimibe combination- Discontinue metformin – contraindicated if SCr ≥ 1.5
mg/dL in men and ≥ 1.4 mg/dL in women - Decrease sitagliptin dose to 50 mg once daily due to renal
impairment- Discuss use of insulin with patient- Refer to a certified diabetes educator for education and goal
setting related to diet, exercise, and medication adherence
Future Considerations in Dyslipidemia and Cardiometabolic Risk Management
1. Should the goals for LDL-C in primary prevention be lowered?
2. What to do with CRP – routine use in risk stratification, secondary target?
3. What about secondary targets?- Non-HDL-C, HDL-C, apo B, LDL particle
concentration?
4. Move from 10-year to lifetime risk?
Predictions for NCEP ATP IV
1. LDL-C goals in primary prevention may be lowered
2. There will be a stronger statement on hs-CRP, but routine use in risk stratification or use as secondary target will not be specifically endorsed
3. Non-HDL-C will remain the secondary lipid target, but optional use of apo B or LDL-P will be endorsed
4. A new risk calculator providing lifetime risk estimates will be provided
5. CKD may be added as a CV risk equivalent
Allison TG. Lipid Management Standard and Advanced Preview of ATP-IV. Mayo Clinic.

14
Possible New ATP IV Recommendations?
• All patients with CVD should have an LDL-C < 70 mg/dL and a non-HDL-C < 100 mg/dL
• All patients older than 40 years with type 2 DM, a Framingham score > 20%, or an hs-CRP > 2.0 should be taking a statin to lower LDL-C by at least 35%
• Reemphasize the need for patients with low HDL-C and/or high TG to achieve non-HDL-C goals
• Apolipoprotein B will be an optional target (< 80 mg/dL) in high-risk patients
• ATP will probably not recommend the triple target LDL-C < 70 mg/dL, TG < 150 mg/dL, and HDL-C > 40 mg/dL
• Combination therapy will be advocated to achieve the goals
The Role of QI-CME in Patient Care
Have you participated in QI-CME or performance improvement (PI-CME)?
?Audience Response Question
1. Yes2. No, but considering it3. No, haven’t considered it4. What is PI-CME?
• Performance Improvement CME (PI-CME) – Individual QI– Standardized format—retrospective assessment of
patient chart data, application of improvement measures, re-assessment
– Measures change in clinician performance related to specific measures between two time points
– Practice is assessed on nationally standardized performance measures
– 20 credits (AMA PRA Category 1 Credit™)
What Is QI-CME?
Performance/Quality ImprovementAn Integral Component of…
• Maintenance of board certification (MOC)– ABIM: www.abim.org/moc– ABFM: www.theabfm.org/moc/index.aspx
• “Pay for reporting”– Centers for Medicare and Medicaid (CMS):
Physician Quality Reporting System (PQRS)
• “Pay for performance”– National Committee for Quality Assurance
Diabetes Recognition Program (NCQA/DRP)– Health plan recognition programs
• Maintenance of licensure (MOL)?– State medical boards
PI-CME – AMA Definition
• Stage A: Learning from current practice performance assessment
– Assess current practice using identified performance measures, either through chart reviews or some other appropriate mechanism
• Stage B: Learning from the application of PI to patient care– Implement an intervention based on the performance
measures selected in Stage A, using suitable tracking tools (eg, flow sheets)
• Stage C: Learning from the evaluation of the PI effort– Re-evaluate and reflect on performance in practice (Stage B)
by comparing with the assessment done in stage A
American Medical Association. www.ama-assn.org/ama1/pub/upload/mm/455/pra2006.pdf.

15
QI-CME Goals
• Assess actual practice performance
• Gain valuable insight into real patient outcomes within the practice compared with national standards of care
• Employ new tools and perspectives on how to improve patient care
• This program – use of QI performance measures can improve:
– CMD risk identification and management– Management of lipid control in context of CKD and other
comorbidities of cardiometabolic disease
Evidence-Based Performance MeasuresT2DM
• One or more A1C tests per year (HEDIS)
• Patients who are at goal (A1C < 7.0%) (HEDIS)
• Patients with elevated A1C who are receiving treatment (NQF)
• Annual comprehensive foot examination (NCQA)
• Dilated or retinal eye exam during past year (HEDIS)
• Most recent BP < 140/90 mm Hg (HEDIS)
- Note: ADA goal is BP < 130/80 mm Hg
• Elevated BP treated with ARB or ACE inhibitor (NQF)
What Do I Have to Do?
Multiple Ways to Register:• Onsite: registration forms
available
• Via web: https://pri-med.pi-iq.com
• Via e-mail: [email protected]
• Via phone: 866 858 7434
• Please refer to the “Pri-Med Performance Improvement CME Program”
Post-Test Questionsand
Conclusions
Post-Test Question #1
• RG is a 55 y.o. obese white woman, occasional smoker with dyslipidemia: TC = 248 mg/dL; LDL-C = 162 mg/dL; HDL-C = 38 mg/dL; TG – 130 mg/dL
• The physician has decided not to do any additional testing in patient RG at this time. Which intervention should be done at this step?1. No further interventions2. Therapeutic lifestyle changes (TLC) only3. TLC plus lipid therapy with a statin4. TLC plus lipid therapy with niacin5. Unsure
? Post-Test Question #2
• RG has been on TLC and simvastatin 20 mg for over 6 months; TC = 180 mg/dL; LDL = 97 mg/dL; HDL-C = 48 mg/dL; TG = 110 mg/dL. She was also diagnosed with type 2 diabetes (T2DM)
• Which of the following is the best course of action to manage RG’s lipid profile at this time?
1. Maximize her simvastatin dose 2. Add gemfibrozil to her simvastatin3. Add ezetimibe to her simvastatin4. Discontinue her simvastatin and start either gemfibrozil
or ezetimibe5. Unsure
?

16
Post-Test Question #3
• Which of the following treatments have demonstrated a reduction in cardiovascular events in clinical trials of patients with severe CKD?
1. Atorvastatin
2. Rosuvastatin + ezetimibe
3. Atorvastatin + colesevelam
4. Simvastatin + ezetimibe
5. Unsure
? Key Points
• LDL-C: strong predictor of CV events in CM syndrome- Non-HDL-C is an important secondary target
• Reducing LDL-C with combination lipid-lowering therapy decreases the risk of CV events in patients with CKD
• Maximizing statin dose may provide limited LDL-C reduction and may increase the risk of adverse events; consider combination therapy with a non-statin agent
• CM syndrome is progressive and multi-factorial
• Early assessment and targeted intervention are needed to treat and prevent all risk factors associated with CV disease, dyslipidemia, and diabetes





























