Embed Size (px)
Citation preview

TracheostomyTracheostomy
Prepared By
Dr. Hanan Said Ali

Objectives
Define of tracheostomy.tracheostomy. List indications, contraindications and
cautions of tracheostomy.tracheostomy. Explain how to prepare the patient. Explain how to insert the tube. Demonstrate the care of patient with a
tracheostomy tube. Perform tracheal suction.
TracheostomyTracheostomy
DefinitionA surgical incision in the trachea just below the
larynx.
Indications
To establish a definitive airway under the following emergent conditions:
Inability to perform endotracheal intubation.


TracheostomyTracheostomy
Indications Cont.
Sever laryngotracheal trauma or laryngeal fracture.
Epiglottitis, neoplasm, abscess, or foreign body in the pharynx that prevents endotracheal intubation.

TracheostomyTracheostomy
Contraindications and Cautions Complications in the emergency setting are usually
due to haste ( quickly) , inadequate lighting, equipment problems, and management of a patient who is struggling ( breath with effort) to breath.
The complexity of this procedure mandates that it be performed by an appropriately trained professional.

TracheostomyTracheostomy
Contraindications and Cautions Cont.
Patients with suspected neck injuries require spinal stabilization.
Universal precautions need to be used all involved because blood is likely to splatter during the procedure.
Equipment
Sterile gloves Masks Protective goggles Antiseptic solution Scalpel blades Local anesthetic Mosquito forceps Kelly clamps
5- ml syringe with an 18- G needle and a 27- G needle for anesthesia
Tracheostomy tube with an obturator.
Metzenbaum scissors Scissors ( sharp and
blunt) Tissue forceps ( with and
without teet

Equipment Cont.
Tracheal dilator and hook Retractors Adhesive tape Gauze dreesing Suction equipment, pharyngeal and tracheal Bag- mask High – flow oxygen source 3-0, 4-0 silk suture.


Patient Preparation
The patient should be ventilated through endotracheal tube or another method until the tracheostomy is completed.
Unless there may be cervical spine injury, place the patient in a supine position with the neck in extension, and provide support under the shoulders.
Inflate the tracheal tube cuff and check for leaks

Patient Preparation Cont. Cleanse the skin from the mandible to below the
clavicles with antiseptic solution.
Drape the chest and the neck.
Infiltrate the skin with a local anesthetic.
Provide analgesia. Restrain or sedate the patient as indicated.
Bleeding may be significant, prepare the tracheal and pharyngeal suction equipment


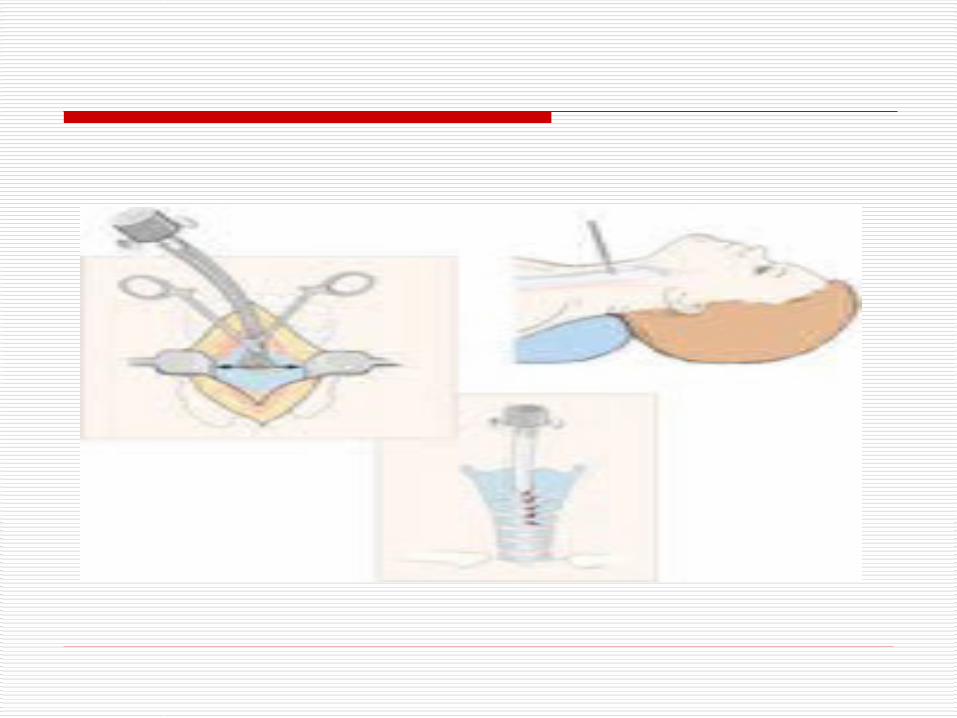
Procedural Steps Make a midline skin incision vertically to
expose the strap muscles.
Retract the strap muscles laterally to expose the pretracheal fascia and thyroid isthmus.
Clamp the thyroid and bluntly dissect to divide the isthmus and expose the trachea.
Procedural Steps Cont.
Transect the thyroid isthmus and ligate it by means of sutures.
Incise through the tracheal rings to enter the trachea through the second to fourth tracheal rings.
Suction the tracheal secretions.
Insert the tracheal tube and the obturator.

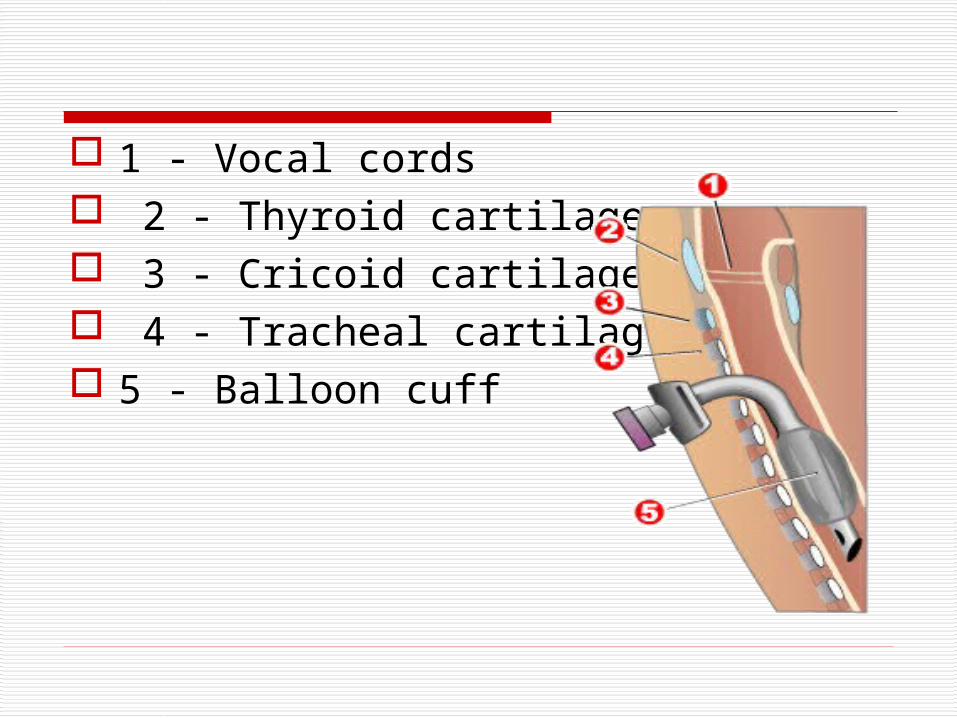
1 - Vocal cords 2 - Thyroid cartilage 3 - Cricoid cartilage 4 - Tracheal cartilages 5 - Balloon cuff

Procedural Steps Cont.
Remove the obturator, inflate the cuff with 5 to 8 ml of air, and ventilate the patient with a bag- mask.
Auscultate the lungs to assess tube placement, and verify tube position with a chest radiograph.
Procedural Steps Cont.
Tie the tracheostomy tube in place around the neck with tracheostomy tape.
Clean and dress the insertion site.
Deliver humidified oxygen as soon as possible.

Complications Cardiopulmonary arrest secondary to
hypoxia.
Hemorrhage and injury to the thyroid gland esophagus, laryngeal nerve, trachea.
Pneumothorax.
False passage of the tube into the pleura, esophagus, or surrounding vessels.
Complications Cont. Bradycardia or hypotension secondary to
hypoxia.
Inadvertent ( careless) decannulation of the tracheostomy.
Late complications include subglottic stenosis, tracheal stenosis, artery erosion, pneumonia, aspiration.

Patient Education
Report any respiratory difficulty or tubing disconnections immediately.
Do not touch or move the tube.
You will not be able to speak with the tube in place.

Care of the Patient With a Tracheostomy Tube
Steps Rational
Gather the needed equipment including Sterile gloves Hydrogen peroxide, Normal saline solution or sterile water,Cotton tippedApplicatorsDressing and twill tape
Everything needed to care for a tracheostomy should be readily on hand for the most effective care.

Care of the Patient With a Tracheostomy Tube
Steps Rational
Perform hand hygiene. Hand hygiene reduces bacteria on hands.
Explain procedure to patient and family as appropriate.
A patient with a tracheostomy is apprehensive and requires ongoing assurance and support.
Put on clean gloves; remove and discard the soiled dressing in abiohazard container.
Observing body substance isolation reduces cross-contaminationfrom soiled dressings.

Care of the Patient With a Tracheostomy Tube
Steps Rational
Prepare sterile supplies, including hydrogen peroxide, normalsaline solution or sterile water, cotton-tipped applicators,dressing, and tape.
Having necessary supplies and equipment readily available allowsthe procedure to be completed efficiently.
Put on sterile gloves. Sterile equipment minimizes transmission of surface flora to the sterile respiratory tract.

Care of the Patient With a Tracheostomy Tube
Steps Rational
Cleanse the wound and the plate of the tracheostomy tube with sterile cotton-tipped applicators moistened with hydrogen peroxide. Rinse with sterile saline solution.
Hydrogen peroxide is effective in loosening crusted secretions.Rinsing prevents skin residue.

Care of the Patient With a Tracheostomy Tube
Steps Rational
Soak inner cannula in peroxide and rinse with saline solution or replace with a new disposable inner cannula.
Soaking loosens and removes secretions from the inner lumen of the tracheostomy tube.
Remove soiled twill tape with clean tape, after the new tape is in place.


Steps RationalPlace clean twill tape in position to secure the tracheostomy tube by inserting one end of the tape through the side opening of the outer cannula.
This taping technique provides a double thickness of tape aroundthe neck, which is needed because the tracheostomy tube can be dislodged by movement or by a forceful cough if left unsecured.
Take the tape around the back of the patient’s neck and thread it through the opposite opening of the outer cannula.

Care of the Patient With a Tracheostomy Tube
Steps Rational
Bring both ends around so that they meet on one side of the neck.
Tighten the tape until only two fingers can be comfortably inserted under it..

Care of the Patient With a Tracheostomy Tube
Steps Rational
Secure with a knot. For a new tracheostomy, two people should assist with tape changes
Remove old tapes and discard in a biohazard container.
Tapes with old secretions may harbour bacteria.

Performing Tracheal Suction
Equipment
• Suction catheters
• Gloves
• Goggles for eye protection
• Basin for sterile normal saline solution for irrigation
• Manual resuscitation bag with supplemental oxygen
• Suction source

Performing Tracheal Suction
Procedure 1. Explain the procedure to the patient before
beginning and offer reassurance during suctioning; the patient may be apprehensive about choking and about an inability to communicate.
Begin by carrying out hand hygiene. Turn on suction source (pressure should not exceed
120 mm Hg). Open suction catheter kit.

Performing Tracheal Suction
Procedure Cont. Fill basin with sterile normal saline solution. Ventilate the patient with manual resuscitation bag
and highflow oxygen. Put sterile glove on dominant hand. Pick up suction catheter in gloved hand and
connect to suction.

Performing Tracheal Suction
Hyperoxygenate the patient’s lungs for several deep breaths.
Instill normal saline solution into airway only if there are thick, tenacious secretions.
Insert suction catheter at least as far as the end of the tube without applying suction, just far enough to stimulate the cough reflex.


Performing Tracheal Suction
Apply suction while withdrawing and gently rotating the catheter 360° (no longer than 10 to 15 seconds, because hypoxia and dysrhythmias may develop, leading to cardiac arrest).
Reoxygenate and inflate the patient’s lungs for several breaths.

Performing Tracheal Suction
Repeat previous three steps until the airway is clear.
Rinse catheter in basin with sterile normal saline solution between suction attempts if necessary.
Suction oropharyngeal cavity after completing tracheal suctioning.
Rinse suction tubing. Discard catheter, gloves, and basin appropriately.

Thank You