Embed Size (px)
Citation preview

Toxicological Risk Assessment
DEVICE: 3D Printed Material ABS-M30i
SPONSOR: Scott Drikakis Stratasys 7665 Commerce Way Eden Prairie, MN 55344
PROJECT#: MJ19045-STR02

- CONFIDENTIAL - Sponsor:
Scott Drikakis Stratasys
7665 Commerce Way Eden Prairie, MN 55344
REPORT | 801-290-7502 | www.nelsonlabs.com | [email protected] | Project MJ19045-STR02 | pg. 2
© 2018. All rights reserved.
TABLE OF CONTENTS Page Number
1.0 Background .............................................................................................................................. 4
2.0 Purpose .................................................................................................................................... 4
3.0 Device Description and Categorization .................................................................................... 4
4.0 Assessment .............................................................................................................................. 5
4.1 Calculations Discussion ........................................................................................................ 6
4.2 Threshold of Toxicological Concern Concept ...................................................................... 8
4.3 Extractable Compounds Review .......................................................................................... 8
4.3.1 Aluminum ....................................................................................................................... 10
4.3.2 Boron .............................................................................................................................. 12
4.3.2 Silicon .............................................................................................................................. 14
5.0 Limitations .............................................................................................................................. 17
6.0 Conclusion .............................................................................................................................. 18
7.0 References ............................................................................................................................. 19

- CONFIDENTIAL - Sponsor:
Scott Drikakis Stratasys
7665 Commerce Way Eden Prairie, MN 55344
REPORT | 801-290-7502 | www.nelsonlabs.com | [email protected] | Project MJ19045-STR02 | pg. 3
© 2018. All rights reserved.
LIST OF ABBREVIATIONS
ATSDR Agency for Toxic Substances and Disease Registry AI Adequate Intake CEF Concomitant Exposure Factor CVAAS Cold Vapor Atomic Absorption Spectroscopy DRI Dietary Reference Intake EAR Estimated Average Requirement FDA US Food & Drug Administration GC/MS Gas Chromatography Mass Spectrometry GRAS Generally Recognized As Safe ICP/OES Inductively Coupled Plasma-Optical Emission Spectroscopy ICP/MS Inductively Coupled Plasma Mass Spectrometry ISO International Organization for Standardization LC/MS Liquid Chromatography LC/QToF/MS Liquid Chromatography Quadrupole Time of Flight Mass Spectrometry LD50 Dose that is lethal in 50% of population tested LOAEL Lowest Observed Adverse Effect Level MF Modifying Factor MOS Margin of Safety MRL Minimal Risk Level ND Not detected NOAEL No Observed Adverse Effect Level NTP National Toxicology Program PDE Permitted Daily Exposure PEF Proportional Exposure Factor RDA Recommended Dietary Allowance RDI Recommended Daily Intake RfD Reference Dose TI Tolerable Intake TE Tolerable Exposure TIC Tentatively Identified Compound TTC Threshold of Toxicological Concern UF Uncertainty Factor USP U.S. Pharmacopeia UTF Utilization Factor UL Tolerable Upper Intake Level US EPA United States Environmental Protection Agency WHO World Health Organization

- CONFIDENTIAL - Sponsor:
Scott Drikakis Stratasys
7665 Commerce Way Eden Prairie, MN 55344
REPORT | 801-290-7502 | www.nelsonlabs.com | [email protected] | Project MJ19045-STR02 | pg. 4
© 2018. All rights reserved.
1.0 Background Stratasys manufactures materials and printers used for additive manufacturing across the three-dimensional (3D) printing spectrum. The art of 3D printing requires materials with custom tailored properties, and very specific printing parameters. Therefore, 3D printers and the materials they use are designed and considered together. 3D printing has wide-ranging applications from rapid prototyping and fabrication of parts with open interior surfaces and in a variety of medical applications. In medicine, this technology is commonly used to create personalized devices that have a patient’s anatomy, in the form of Magnetic Resonance Images, as input. Typical 3D printed medical devices include anatomical reproductions of a patient treatment site that allow doctors to explore surgical strategies, surgical guides, delivery systems, and permanent implants. Device manufacturers using Stratasys 3D printers and associated materials must evaluate the biocompatibility of their specific device, as printed, post-processed, packaged, and sterilized. The specific biological risks that must be addressed depend on the ISO 10993 device categorization. For many applications, systemic effects such as acute toxicity, subacute toxicity, subchronic toxicity, chronic toxicity, genotoxicity, and carcinogenicity must be addressed. Manufacturers in the process of selecting a material and printer for their specific application need information on these biological endpoints to be sure they are selecting technology/materials that have a low risk of failing biocompatibility testing at the end of the development cycle. To this end, this assessment evaluates the toxicological hazards associated with the 3D printing of the AMS-M30i material.
2.0 Purpose The purpose of this assessment is to use information from the literature on the extractable compounds detected from the ABS-M30i material, which was printed on a Stratasys 3D printer in order to closely examine the toxicological hazards and to evaluate and address any risks associated with the biological endpoints of acute, subacute, subchronic, and chronic toxicity, genotoxicity, and carcinogenicity. This assessment focuses on the requirements of International Organization for Standardization (ISO) 10993-1:2018, ISO 10993-11:2017, ISO 10993-3:2014, ISO 10993-17:2002/(R)2012, ISO 10993-18:2009, ISO 14971:2007/(R)2010, European Union Medical Device Regulation (EU) 2017/745/746, as well as the June 2016 Food and Drug Administration (FDA) Guideline on the Use of Internal Standard ISO 10993-1, “Biological evaluation of medical devices – Part 1: Evaluation and testing within a risk management process.”
3.0 Device Description and Categorization The 3D printed ABS-M30i material (Figure 1) may be used in a wide variety of medical applications. Typical use conditions would be as a surgical guide, in which case it would have limited contact with tissue/bone; however it is anticipated that this material may be used in more invasive applications. Permanent patient contact requires the evaluation of the most biological endpoints and encompasses

- CONFIDENTIAL - Sponsor:
Scott Drikakis Stratasys
7665 Commerce Way Eden Prairie, MN 55344
REPORT | 801-290-7502 | www.nelsonlabs.com | [email protected] | Project MJ19045-STR02 | pg. 5
© 2018. All rights reserved.
the endpoints of other shorter duration uses (with the exception of those related to contact with circulating blood). 3D printed ABS-M30i material coupons (see Figure 1) were evaluated as if one coupon were a permanent implant with tissue/bone/dentine. Each coupon had a surface area of 60 cm2 and material volume of 31.6 cm3. Extrapolation of this assessment from the material coupon to a proposed device must consider differences in surface area, material volume, and other processing differences. Extrapolation of results and conclusions of a material evaluation isn’t a substitute for evaluation of a device made from this material in its final, finished, sterilized, and packaged form.
Figure 1. ABS-M30i Coupons in Water Extraction
4.0 Assessment This document assesses the potential risk posed to patients on whom devices fabricated from this material are used as it they are intended. ISO 10993-1:2018 describes the principles governing the biological evaluation of medical devices. This standard applies to the non-clinical testing of the device. It should be noted that Clause 4.5 states: “All known possible biological hazards shall be taken into account for every material and final product, but this does not imply that testing for all possible hazards will be necessary or practical.” Clause 4.1 of this standard specifies: “Evaluation can include both a review of relevant existing preclinical and clinical data and actual testing. Such an evaluation might result in the conclusion that no testing is needed if the material has a demonstrable safe history of use in a specified role and physical form that is equivalent to that of the medical device under design.” ISO 14971:2007/(R)2010, Medical devices – Application of risk management to medical devices states that the risk assessment shall be based on:
The physical and chemical characteristics of the device components and materials;
Any history of clinical use or human exposure data;
Any existing toxicology and other biological safety data on the product components and materials;
Test procedures and results.

- CONFIDENTIAL - Sponsor:
Scott Drikakis Stratasys
7665 Commerce Way Eden Prairie, MN 55344
REPORT | 801-290-7502 | www.nelsonlabs.com | [email protected] | Project MJ19045-STR02 | pg. 6
© 2018. All rights reserved.
Collectively, knowledge of the composition of a medical device, including additives and processing aids, prior use of the relevant material(s) in a predicate device or similar device, and biological safety tests should provide predictive evidence of potential hazards to users of the device. Some factors that affect the biocompatibility of the material include the identity, concentration, availability, and toxicity of all constituents such as additives, processing aids, and any other compounds present. Biological safety should be considered giving special attention to the ISO 10993 series for a particular application. Evaluation of prior use, information on previous uses of the device/materials or intended additives, and any adverse reactions encountered should be reviewed. Account should be taken of the intended use, the concentration of the ingredients, and current toxicological information. The need for testing should be reviewed on a case-by-case basis. The amount of data required on a material, and the depth of the investigation, is dependent upon the intended use in manufacturing of devices and the function and duration of patient contact. Knowledge of a material’s composition and potential leachable compounds should provide predictive evidence of any potential toxicological risk to patients.
4.1 Calculations Discussion To help determine the toxicological hazard of the device, Tolerable Intake (TI) levels were examined. Thresholds calculated according to ISO 10993-171 include the TI level (in mg/kg∙day) and the Tolerable Exposure (TE) level (in mg/day). Each threshold, TI and TE, represents the maximum dose at which exposure to the substance does not produce adverse events or pose an unacceptable risk to human health.1 The TE includes experimental values shown to be without adverse effects, including the No Observed Adverse Effect Level (NOAEL) and the Lowest Observed Adverse Effect Level (LOAEL). The TE also incorporates modification factors for concomitant exposures to substances from other sources. Inter-individual variability in sensitivity to chemical effects is accounted for in the calculation of exposure thresholds using Uncertainty Factors (UFs). UFs are safety factors which take into account pharmacokinetic/toxicokinetic or metabolic differences among exposed people. The equation for TI is as follows:
𝑇𝐼 =𝑁𝑂𝐴𝐸𝐿 𝑜𝑟 𝐿𝑂𝐴𝐸𝐿
(𝑈𝐹1 × 𝑈𝐹2 × 𝑈𝐹3)
UFs used in calculation of TI include modifications for inter-individual variation among people (UF1), extrapolation of effects between animals and people (UF2), and the quality and relevance of the experimental data (UF3). Common industry practices apply a factor of 10 for UF1 and UF2. UF3 is dependent on the quality of the information used in the assessment as compared to the clinical application of the device. TE represents the tolerated exposure level of a chemical within a population including an additional Utilization Factor (UTF). The UTF accounts for variables affecting clinical exposure, such as frequency of device use [Concomitant Exposure Factor (CEF)] and potential exposure to similar leachables from other

- CONFIDENTIAL - Sponsor:
Scott Drikakis Stratasys
7665 Commerce Way Eden Prairie, MN 55344
REPORT | 801-290-7502 | www.nelsonlabs.com | [email protected] | Project MJ19045-STR02 | pg. 7
© 2018. All rights reserved.
sources [Proportional Exposure Factor (PEF)]. The following equation is used for the calculation of the TE:
𝑇𝐸 = 𝑇𝐼 × 𝑚𝐵 × 𝑈𝑇𝐹
𝑈𝑇𝐹 = 𝐶𝐸𝐹 × 𝑃𝐸𝐹
ISO 10993-17 specifies default values for body weight (mB), CEF, and PEF. The CEF is specified to be 0.2, and the PEF is maintained at 1. The default body weight for adult males, adult females, and pediatrics, are specified to be 70 kg, 58 kg, and 10 kg, respectively. The margin of safety (MOS), a unit-less index between the calculated threshold and exposure level, is used as a summary value to characterize the hazard of each substance. This ratio indicates a fold-level difference between exposure and threshold value. Using a conservative approach and default ISO 10993-17 default recommendations, a MOS greater than 1 is indicative of low toxicological hazard for the evaluated substance. When available, United States Environmental Protection Agency (US EPA, Reference Dose values (RfD) or Agency for Toxic Substances & Disease Registry (ATSDR) Minimal Risk Limits (MRL) will be used. RfDs are typically calculated from NOAEL values divided by UFs and/or Modifying Factors (MFs). 2,3 A RfD is an estimate (with uncertainty spanning approximately an order of magnitude) of a daily oral exposure for a chronic duration (up to a lifetime) to the human population (including sensitive subgroups) that is likely to be without an appreciable risk of deleterious effects during a lifetime. It can be derived from laboratory animal dosing studies in which a NOAEL, LOAEL, or benchmark dose (with uncertainty factors generally applied to reflect limitations of the data used) can be obtained. For MRLs, the ATSDR also uses the NOAEL/UF approach to derive MRLs for substances. They are set below levels that, based on current information, might cause adverse health effects in the people most sensitive to such substance-induced effects. MRLs are derived for acute (1-14 days), intermediate (>14-364 days), and chronic (365 days and longer) exposure durations, and for the oral and inhalation routes of exposure. MRLs are generally based on the most sensitive substance-induced end point considered to be of relevance to humans. ATSDR does not use serious health effects (such as irreparable damage to the liver or kidneys, or birth defects) as a basis for establishing MRLs. Exposure to a level above the MRL does not mean that adverse health effects will occur. The Reference Daily Intake (RDI; also known as Recommended Daily Intake) is the recent term for Recommended Daily Allowance (RDA). RDIs may be used as the TI for dietary metals (eg, calcium, phosphorus, potassium, sodium, magnesium, iron, cobalt, copper, zinc, manganese, molybdenum, and selenium). RDIs are nutrient reference values developed by the Institute of Medicine of The National Academies. They are intended to serve as a guide for good nutrition and provide the scientific basis for the development of food guidelines in both the United States and Canada. Dietary Reference Intake (DRI) values include the Estimated Average Requirement (EAR), RDA, Adequate Intake (AI), and Tolerable Upper Intake Level (UL). Exposure values below a published RDI for an essential metal would be considered safe. The Q3D Elemental Impurities Guidance for Industry on the Permitted Daily Exposures (PDE) for in finished drug products published by the U.S. Food and Administration4 will also be used for metals which do not have a RDI. Limits for metals not published in either of these sources may

- CONFIDENTIAL - Sponsor:
Scott Drikakis Stratasys
7665 Commerce Way Eden Prairie, MN 55344
REPORT | 801-290-7502 | www.nelsonlabs.com | [email protected] | Project MJ19045-STR02 | pg. 8
© 2018. All rights reserved.
be drawn from the current US EPA Table of Regulated Drinking Water Contaminates5 or the World Health Organization (WHO) Guidelines for Drinking-Water Quality.6
4.2 Threshold of Toxicological Concern Concept The Threshold of Toxicological Concern (TTC) concept was developed to define an acceptable intake for any unstudied/understudied chemical that, if below the TTC, will not pose a risk of carcinogenicity or other toxic effects. The concept was developed for chemicals present in the human diet and is accepted by the US Food & Drug Administration (FDA), International Conference on Harmonization and the European Medicines Agency for the evaluation of impurities in pharmaceuticals. It has also been used for assessing contaminants in consumer products and environmental contaminants. The methods upon which the TTC is based are generally considered very conservative since they involve data for the most sensitive species and most sensitive site induction (several “worst case” assumptions). The TTC concept provides an estimate of safe exposures values for any compound not on the TTC exclusion list (ie, metals and polycyclic aromatic hydrocarbons). The most conservative TTC value has been set at 1.5 μg/day and is assigned for greater than 10 years to a lifetime of exposure. By using this value, a 10-5 safety probability factor is built in. A TTC of 120 ug/day has been proposed for genotoxic compounds for exposures limited to one month or less.7 When using such a conservative approach, it is reasonable to conclude there is no need to add additional safety factors to account for route-to-route exposure or for protection of sensitive populations. European Food Safety Authority (EFSA) has found that the TTC approach adequately protects infants and children. Generally speaking, this is due to the TTC values expressed according to body weight and therefore take into account the lower body weights of infants and children. EFSA has also noted, particularly when exposures are low, the differences between young infants and children or adults in respect to metabolism are small enough not to invalidate the use of the TTC approach. However, EFSA does recommend that if the estimated exposure is in the range of the TTC value for young infants, additional considerations, such as predicted metabolism, frequency and duration of exposure may need to be made, on a case-by-case basis, to determine whether the TTC approach can be relied on. However, exceeding the TTC is not necessarily associated with an increased risk given the conservative assumptions employed in the derivation of the TTC value.8-12 When adequate evidence exists that a constituent is non-carcinogenic, a non-carcinogenic TTC value may be used to address the constituent (eg, Cramer Classification13,14).
4.3 Extractable Compounds Review The device underwent an extractable study per ISO 10993-18 (Nelson Labs Europe 1104831-S01). The coupons were extracted in purified water and hexane at 50°C for 72 hours. Nine devices were extracted by full immersion with 350 mL of water and nine devices in 350 mL of hexane. The water extracts were analyzed by inductively coupled plasma-optical emission spectroscopy (ICP/OES), ICP-mass spectrometry (ICP/MS), gas chromatography-mass spectrometry (GC/MS) methods for metals, volatile organics, semi-volatile organics, and amenable non-volatile organics. The hexane extraction process degraded the device, and is therefore was not appropriate for toxicological assessment. Using these analytical chemistry techniques, the extractable compounds were identified and quantified to determine the chemical dose to the user as if the material coupon were a device. The quantitative amount extractable compounds detected are listed below in Table 1. Compounds that were less than the analytical evaluation threshold of 0.75 μg per coupon after blank correcting were considered not detected (ND).

- CONFIDENTIAL - Sponsor:
Scott Drikakis Stratasys
7665 Commerce Way Eden Prairie, MN 55344
REPORT | 801-290-7502 | www.nelsonlabs.com | [email protected] | Project MJ19045-STR02 | pg. 9
© 2018. All rights reserved.
The number of devices pooled and the extraction volumes were selected to target a per device analytical sensitivity less than 1.5 μg/device so that any undetected compounds would be below the TTC. Due to degradation of the material in hexane, no further evaluation of this extract is appropriate; therefore only results from the water extraction are shown.
Table 1. Quantitatively Detected Extractable Compounds
Analyte Name Water Extract* (µg/coupon**)
Aluminum 0.162
Boron 4.12
Calcium 15.5a
Copper 0.134b
Iron 0.128c
Magnesium 9.63d
Nickel 0.0897e
Potassium 1.05f
Silicon 12.8
Sulfur 2.72g
Sodium 101h
Zinc 0.336i
*Amount of compound shown was detected after a 72-hour extraction at 50°C; this amount was assessed as a possible worst case amount that could be released clinically every 24 hours ** Coupon surface area equals 60 cm2 and a material volume of 31.6 cm3 a) Below the most conservative RDI of 20,000 µg/day for calcium b) Below the most conservative RDI of 700 µg/day for copper c) Below the most conservative RDI of 8,000 µg/day for iron d) Below the most conservative RDI of 30,000 µg/day for magnesium e) Below the Q3D PDE for parental exposure to nickel 22 µg/day f) Below the most conservative RDI of 4,500,000 µg/day for potassium g) Below the sulfur component of methionine which has an RDA of 14,000 μg/day (corresponding to 3,000 μg/day sulfur)15 h) Below the most conservative RDI of 120,000 µg/day for sodium i) Below the most conservative RDI of 8,000 µg/day for zinc
Table 2. Semi-Quantitatively Detected Extractable Compounds
Analyte Name CAS Number Water Extract* (µg/coupon**)
No Compounds Detected *Amount of compound shown was detected after a 72-hour extraction at 50°C; this amount was assessed as a possible worst case amount that could be released clinically every 24 hours ** Coupon surface area equals 60 cm2 and a material volume of 31.6 cm3 ND = Not detected above AET of 0.75 μg/coupon

- CONFIDENTIAL - Sponsor:
Scott Drikakis Stratasys
7665 Commerce Way Eden Prairie, MN 55344
REPORT | 801-290-7502 | www.nelsonlabs.com | [email protected] | Project MJ19045-STR02 | pg. 10
© 2018. All rights reserved.
Compounds below the most conservative TTC value of 1.5 µg (excludes metals) and essential metals below their respective RDI levels, will not be further assessed as they are not indicated as a toxicological concern. Compounds above the TTC value of 1.5 μg/device [aluminum, boron, and silicon] will be assessed individually in the sections that follow.
4.3.1 Aluminum Aluminum compounds have a wide variety of uses, including production of ceramic and glass. They are also used in rubber, wood preservatives, pharmaceuticals (eg, antacids, buffered aspirin, antiperspirants), and for waterproofing textiles. Natural aluminum minerals such as bentonite and zeolite are used in water purification and paper industries. Aluminum is naturally present in many foods. It is also a commonly used food additive (eg, preservatives, leavening and anticaking agents).16 American adults have been reported to consume 2-25 mg aluminum per day from food and beverages.17 Common medications such as antacids contain 104-208 mg per tablet.18 Typical gastrointestinal absorption of aluminum from diets is less than 1%. The gut therefore acts as the most effective organ in preventing tissue aluminum accumulation after oral exposure.17 Both passive and active transcellular processes and paracellular transport are believed to occur in the mechanisms of aluminum absorption.17 The absorption of aluminum is also affected by the speciation of aluminum and a variety of other substances, including the gut milieu.17 In the brain, aluminum entry from blood may involve transferrin-receptor mediated endocytosis and a more rapid process for transporting small molecular weight aluminum species.19 Upon absorption, it is bound to plasma proteins and widely distributed to the organs, including the brain. There is prolonged retention of a fraction of aluminum that enters the brain, which suggests the potential for accumulation with repeated exposure.19 Not all aluminum that makes it into the circulatory system is excreted in urine. Aluminum has low glomerular filtration which reflects its high protein binding with plasma proteins, predominantly transferrin.17,20 Patients with decreased renal function are expected to have an increased risk of aluminum-induced accumulation and toxicity.21 The mechanism of aluminum biliary secretion is poorly understood. The biliary secretion of aluminum and its resulting fecal elimination appears to be saturatable at fairly low oral doses of aluminum.17 Aluminum has the ability to produce neurotoxicity by many mechanisms.19 There is also some evidence to suggest aluminum is an important factor in the down-regulation of genes controlling neuronal protein metabolism.22 A Canadian study has reported cognitive and other neurological deficits among groups of workers occupationally exposed to dust containing high levels of aluminum (annual exposure estimated at 375 mg/year).23 In renal dialysis patients, excessive parenteral exposure to aluminum can cause a progressive fatal neurological syndrome called dialysis dementia.24 In rabbits, injection of an aluminum phosphate solution (0.16 mg aluminum) via intracerebral or intrathecal routes, results in the development of neurofibrillary tangles, which are indicators of Alzheimer’s disease25 and have produced behavioral, neuropathological, and neurochemical changes that partially model Alzheimer’s disease.19 Other experimental evidence has demonstrated aluminum exposure leads to excess inflammatory activity in the brain.26 Aluminum has been implicated in the etiology of sporadic Alzheimer's disease and other neurodegenerative disorders.19,20 This topic is highly controversial and has not been resolved by

- CONFIDENTIAL - Sponsor:
Scott Drikakis Stratasys
7665 Commerce Way Eden Prairie, MN 55344
REPORT | 801-290-7502 | www.nelsonlabs.com | [email protected] | Project MJ19045-STR02 | pg. 11
© 2018. All rights reserved.
epidemiological studies, as only some found a small association between increased incidence of dementia and aluminum exposure.19,27,28 Studies of brain aluminum concentrations in Alzheimer’s patients have not produced consistent findings.19 Additionally, high intake of aluminum from antacid for gastrointestinal ailments has not been reported to cause any adverse effects and has not been correlated with neurotoxicity or Alzheimer’s disease.5 The precise pathogenic role of aluminum in Alzheimer's disease remains to be elucidated and present data does not support a causative role for its involvement with Alzheimer’s disease.
ATSDR has derived a chronic-duration oral MRL of 1 mg/kg·day. This MRL is based on a LOAEL of 100 mg/kg·day for neurological effects demonstrated in mice exposed to aluminum lactate in the diet during gestation, lactation, and postnatally until two years of age.29 The MRL was derived by dividing the LOAEL by an uncertainty factor of 300 (3 for the use of a minimal LOAEL multiplied by 10 for animal to human extrapolation, and multiplied by 10 for human variability) and a modifying factor of 0.3 to account for the higher bioavailability of the aluminum lactate used in the referenced study, as compared to the bioavailability of aluminum in the human diet and drinking water. The FDA has established an acceptable limit of 850 μg/dose for exposure to aluminum per dose as an additive in biologics administered parenterally for an adult, assumed here to have a weight of 70 kg (see 21CFR 610.15(a)). The most conservative chronic oral RfD of 1 mg/kg·day will be used as the TI level. UF1 and UF2 are already accounted for in the RfD value and therefore assigned a value of 1. A value of 100 was used for UF3 according to the Q3D guidance and to account for the difference in route of exposure and differences in bioavailability (chronic oral vs. bone implant). The TI is therefore calculated as follows:
𝑇𝐼 =𝑅𝑓𝐷
𝑈𝐹1 × 𝑈𝐹2 × 𝑈𝐹3
𝑇𝐼 =1 mg/kg ∙ day
1 × 1 × 100
𝑇𝐼 = 0.01 mg/kg ∙ day
The TE is calculated as follows:
𝑇𝐸 = 𝑇𝐼 × 𝑚𝐵 × 𝑈𝑇𝐹
𝑈𝑇𝐹 = (𝐶𝐸𝐹) × (𝑃𝐸𝐹)
𝑈𝑇𝐹 = (0.2) × (1) = 0.2
𝑇𝐸 = (0.01 mg/kg ∙ day) × (70 kg) × (0.2) = 0.14mg
day or 140
µg
day
Values for the CEF, PEF, and adult body weight were used according to ISO 10993-17 default recommendations. The MOS between amount of aluminum theoretically calculated for three Bone Composite Strips and the adult male TE is:

- CONFIDENTIAL - Sponsor:
Scott Drikakis Stratasys
7665 Commerce Way Eden Prairie, MN 55344
REPORT | 801-290-7502 | www.nelsonlabs.com | [email protected] | Project MJ19045-STR02 | pg. 12
© 2018. All rights reserved.
Margin of Safey =TE
Exposure=
( 140 µg
day)
(0.162 µg
day)
= 864
A summary of the MOS values for the possible populations that could come into contact with the material is shown below. Table 3. Margin of Safety Summary for Aluminum
a) Coupon surface area equals 60 cm2 and a material volume of 31.6 cm3 b) Using the conservative assumptions herein and default ISO 10993-17 default recommendations, a MOS greater than a value
of 1 is indicative of low toxicological hazard for the evaluated substance
Several conservative approaches were used in the calculations of the MOS values: 1) the total amount of compound detected after a 72-hour extraction at 50°C was assessed as a possible worst case amount that could be released clinically every 24-hours, 2) UF3 was adjusted to account for the different route of exposure, and 3) the calculated TE incorporated a UTF that was not adjusted from default values, which lowers the TE by 1/5. The calculated MOS values above support a low toxicological hazard associated with the extractable boron from the material if one coupon is considered equivalent to a device.
4.3.2 Boron Boron is a solid metalloid element that occurs in nature bound to oxygen in the form of inorganic borates. Elemental boron is rarely found in nature. Boron enters the environment mainly thought the weathering of rocks, boric acid volatilization from seawater, and volcanic activity. Boron and its associated compounds, have many industrial applications. These include: the production of borosilicate glass, laundry bleaches, wood preservatives, fire retardants, pesticides, fertilizers, cosmetics, and pharmaceuticals. The general public’s exposure is primarily dietary. Boron is an essential plant nutrient and occurs naturally in fruits and vegetables. The average American adult intake is 1 mg/day.30 Studies have demonstrated benefits which support the consideration of 3 mg/day boron supplementation for any individual who is consuming a diet lacking in fruits and vegetables or who is at risk for or has osteopenia, osteoporosis, or osteoarthritis.31 Inorganic boron supplements are completely absorbed from the intestinal tract and the bioavailability is expected to be very high for most mammals.32 The oral lethal dose in adults is reported as 15-20 g, but 80-297 g has been tolerated in a single ingestion.33,34 The effects of boron toxicity are hemorrhagic
Target Population Weight (kg) TE
(µg/day) Extractable Amount
(µg/coupona) Margin of Safetyb
Adult Male 70 140
0.162
(water extract)
864
Adult Female 58 116 716
Pediatrics 10 20 124
Neonate 3.5 7 43.2

- CONFIDENTIAL - Sponsor:
Scott Drikakis Stratasys
7665 Commerce Way Eden Prairie, MN 55344
REPORT | 801-290-7502 | www.nelsonlabs.com | [email protected] | Project MJ19045-STR02 | pg. 13
© 2018. All rights reserved.
gastroenteritis with weakness, lethargy, headache, restlessness, and tremors. Frequently, the skin shows signs of erythema with exfoliation.35,36 Chronic oral animal experiments indicate that boric acid or borax is toxic to the male reproductive system with testicular lesions being observed in rats, dogs and mice.37,38 At present, there are insufficient human data to determine if boron causes male reproductive toxicity in humans, but boric acid is considered a high-priority chemical for study with respect to human reproductive health.39,40 Borates have long been known to be essential for plants, but a specific biochemical role in humans remains to be determined.41 Although boron deficiency has been reported in rats, chickens, and humans, as of yet, no requirement has been established in humans. However, a boron Upper Limit (UL) of 20 mg/day has been set for adults.42-44 The EPA’s oral RfD for boron is 0.2 mg/kg·day. Decreased fetal body weight was considered the critical effect in the RfD determination. The ATSDR has not established chronic MRLs for boron. Boron has not been shown to have genotoxic in vitro activity at concentrations ranging from 0.1-40 mg/mL).45 The anti-genotoxic effects of boron have been demonstrated to provide ameliorative effects against genotoxicity by enhancing antioxidant defense mechanisms in rat and in vitro assays.45,46 However, boronic acid compounds have been shown to be weak eukaryotic genotoxins; positive results are only produced at concentrations between 1mM and 10mM.45,47-49 No human studies are available for carcinogenicity of boron in humans. The Department of Health and Human Services, the International Agency for Research on Cancer (IARC), and the EPA have not classified boron as to its human carcinogenicity. One animal study found no evidence of cancer after lifetime exposure to boric acid in food.50 The most conservative RfD of 0.2 mg/kg·day will be used as the TI level. UF1 and UF2 are already accounted for in the RfD value and therefore assigned a value of 1. A UF3 of 3 is used to account for uncertainties in the different possibility in exposure route (chronic oral vs. implant directly in contact with tissue). The TI is calculated as follows:
𝑇𝐼 =𝑅𝑓𝐷
𝑈𝐹1 × 𝑈𝐹2 × 𝑈𝐹3
𝑇𝐼 =0.2 mg/kg ∙ day
1 × 1 × 3
𝑇𝐼 = 0.07 mg/kg ∙ day
The TE is therefore calculated as follows:
𝑇𝐸 = 𝑇𝐼 × 𝑚𝐵 × 𝑈𝑇𝐹
𝑈𝑇𝐹 = (𝐶𝐸𝐹) × (𝑃𝐸𝐹)
𝑈𝑇𝐹 = (0.2) × (1) = 0.2

- CONFIDENTIAL - Sponsor:
Scott Drikakis Stratasys
7665 Commerce Way Eden Prairie, MN 55344
REPORT | 801-290-7502 | www.nelsonlabs.com | [email protected] | Project MJ19045-STR02 | pg. 14
© 2018. All rights reserved.
𝑇𝐸 = (0.07mg
kg∙ day) × (70 kg) × (0.2) = 0.98
mg
day𝑜𝑟 980
µg
day
Values for the CEF, PEF, and adult male body weight were used according to ISO 10993-17 default recommendations. The MOS between the amount of extractable boron detected from one coupon and the adult male TE is:
Margin of Safey =TE
Exposure=
(980 µg
day)
(4.12 µg
day)
= 238
A summary of the MOS values for the possible populations that could come into contact with the material is shown below. Table 3. Margin of Safety Summary for Boron
a) Coupon surface area equals 60 cm2 and a material volume of 31.6 cm3 b) Using the conservative assumptions herein and default ISO 10993-17 default recommendations, a MOS greater than a value
of 1 is indicative of low toxicological hazard for the evaluated substance
Several conservative approaches were used in the calculations of the MOS values: 1) the total amount of compound detected after a 72-hour extraction at 50°C was assessed as a possible worst case amount that could be released clinically every 24-hours, 2) UF3 was adjusted to account for the different route of exposure, and 3) the calculated TE incorporated a UTF that was not adjusted from default values, which lowers the TE by 1/5. The calculated MOS values above support a low toxicological hazard associated with the extractable boron from the material if one coupon is considered equivalent to a device.
4.3.2 Silicon Silicon is an abundant chemical and has widespread industrial utility in the production of building materials, composites, and electronics. Human environmental exposure to silicon is chiefly through the diet, where plant matter and beverages contribute appreciably to silicon daily intake.51 Naturally-occurring silicon is often complexed with oxygen to form silica (also known as silicon dioxide), which is consumed in drinking water at relatively low levels. Silica is also introduced into foods and pharmaceutical formulations where it is used as an anti-caking agent.51 Silica comes in different forms, each with a unique toxicological profile. Inhalation exposure to crystalline silica carries the highest toxicological hazard, while oral exposure to amorphous silica is
Target Population Weight (kg) TE
(µg/day) Extractable Amount
(µg/coupona) Margin of Safetyb
Adult Male 70 980
4.12
(water extract)
238
Adult Female 58 812 197
Pediatrics 10 140 34.0
Neonate 3.5 49 11.9

- CONFIDENTIAL - Sponsor:
Scott Drikakis Stratasys
7665 Commerce Way Eden Prairie, MN 55344
REPORT | 801-290-7502 | www.nelsonlabs.com | [email protected] | Project MJ19045-STR02 | pg. 15
© 2018. All rights reserved.
rather benign, even at high doses. The major classes of synthetic amorphous silica are used in a variety of products, e.g. as fillers in the rubber industry, as free-flow and anti-caking agents in powder materials, and as liquid carriers, particularly in the manufacture of animal feed and agrochemicals; other uses are found in toothpaste additives, paints, silicon rubber, insulation material, liquid systems in coatings, adhesives, printing inks, plastisol car undercoats, and cosmetics. Silicon is considered to be a micronutrient in the body and is used in the formation of structural tissues, including elastin, nails, bone, and some detectable levels present in the aortic walls.52 Silica is absorbed from the gastrointestinal tract at a level between 20-75%.51 Free systemic silica is primarily eliminated by the kidneys. Repeated administration of crystalline silica to rats in the feed over a period of 13 weeks produced a decrease in body weight, with a NOAEL of 2.5 g/kg/day for this effect.52 Very high oral dose levels of amorphous silica have been shown to elicit no systemic adverse effects.52 Relatively little data is available on systemic/parenteral exposure to crystalline silica. Most data that exists in this exposure group exists for nano-silica used in biomedical applications, such as drug delivery. The acute toxicity was evaluated for silica that was systematically varied in geometry, porosity, and surface characteristics in immune-competent mice. When administered intravenously, the in vivo toxicity of silica was shown to be influenced by size, porosity, and surface characteristics. The maximum tolerated dose (MTD) increased from 30-450 mg/kg based on size and porosity. The adverse reactions above MTDs were primarily caused by the mechanical obstruction of silica in the vasculature. This led to congestion in multiple vital organs and subsequent organ failure. In general, the larger the hydrodynamic size of silica in the presence of serum protein, the lower the MTD.53 Nano-sized silica particles have been developed as nano-carriers for pharmaceutical drugs. These nano-carriers are used to permeate the blood-brain barrier to allow drugs to permeate brain tissue and the central nervous system.54 Silica-based nanoparticles have been embedded in a biodegradable scaffold and been proposed to offer several advantages when used in laser-tissue-soldering of blood vessels in the brain.55 Microglial cells were analyzed for autophagy and inflammatory cytokines after silica-based nanoparticles exposure. Silica-based nanoparticle incubation did not modulate cytokine secretion and autophagy at any time point investigated.55 In another study evaluating the acute toxicity of nano-silica, particles at 70 nm induced liver injury at 30 mg/kg, while silica particles at 300 nm or 1000 nm had no effect at 100 mg/kg. The administration of silica particles at 70 nm dose-dependently increased serum markers of liver injury, serum aminotransferase, and inflammatory cytokines. Repeated administration of these particles twice a week for four weeks caused hepatic fibrosis at 10 mg/kg.56 The hematological and biochemical parameters were assessed in Sprague-Dawley rats at 5, 21, and 60 days after administration of silica nanoparticles (size 10 nm and 13 nm). Intravenous infusion of 7 mg/kg was not associated with significant changes in hemodynamic parameters. Hearing function (using otoacoustic emission testing) remained unchanged at 21 and 60 days after infusion. Blood counts and biochemical markers were not statistically different. No apparent histological abnormalities in seen in

- CONFIDENTIAL - Sponsor:
Scott Drikakis Stratasys
7665 Commerce Way Eden Prairie, MN 55344
REPORT | 801-290-7502 | www.nelsonlabs.com | [email protected] | Project MJ19045-STR02 | pg. 16
© 2018. All rights reserved.
the kidneys. However, the appearance of foreign body-type granulomas in the liver and spleen as well as microgranulation in the liver after administration were noted.57 In 1987 the IARC classified crystalline silica as a probable carcinogen and in 1997 reclassified it as a Group 1 carcinogen58 (sufficient evidence for carcinogenicity in experimental animals and sufficient evidence for carcinogenicity in humans). The Working Group noted that "carcinogenicity in humans was not detected in all industrial circumstances studied; carcinogenicity may be dependent on inherent characteristics of the crystalline silica or on external factors affecting its biological activity or distribution of its polymorphs."58 In a separate study review it was determined that inflammation is the driving force for genotoxicity and that primary genotoxicity of deposited silica would play a role only at very high, possibly implausible, exposures and deposited doses. Although based on rat studies and in vitro studies, and therefore with caveats, the analysis supports the hypothesis that the mechanism of silica genotoxicity is via inhalation inflammation-driven secondary genotoxicity.59 Without knowing the geometric form or the particle size of silica that extracted from the devices, the most conservative intravenous NOAEL of 7 mg/kg∙day presented in the literature above will be used to derive the TI. The UFs assigned in this calculation are as follows: UF1 = 10 (default value) for inter-individual differences among humans; UF2 = 10 (default value) for animal-to-human toxicity extrapolation; UF3 = 1 for the use of an intravenous route of exposure. The TI was calculated as follows:
𝑇𝐼 =𝑁𝑂𝐴𝐸𝐿
𝑈𝐹1 × 𝑈𝐹2 × 𝑈𝐹3
𝑇𝐼 =7 mg/kg ∙ day
10 × 10 × 1
𝑇𝐼 = 0.07 mg/kg ∙ day
The TE is therefore calculated as follows:
𝑇𝐸 = 𝑇𝐼 × 𝑚𝐵 × 𝑈𝑇𝐹
𝑈𝑇𝐹 = (𝐶𝐸𝐹) × (𝑃𝐸𝐹)
𝑈𝑇𝐹 = (0.2) × (1) = 0.2
𝑇𝐸 = (0.07) × (70) × (0.2) = 0.98mg
day𝑜𝑟 980
µg
day
Values of the CEF, PEF, and adult male body weight were used according to ISO 10993-17 default recommendations. The MOS between the amount of extractable silicon (as crystalline silicon dioxide) detected from one coupon and the adult male TE is:
Margin of Safey =TE
Exposure=
( 980 µg
day)
(27.4 µg
day)
= 35.7
- CONFIDENTIAL - Sponsor:
Scott Drikakis Stratasys
7665 Commerce Way Eden Prairie, MN 55344
REPORT | 801-290-7502 | www.nelsonlabs.com | [email protected] | Project MJ19045-STR02 | pg. 17
© 2018. All rights reserved.
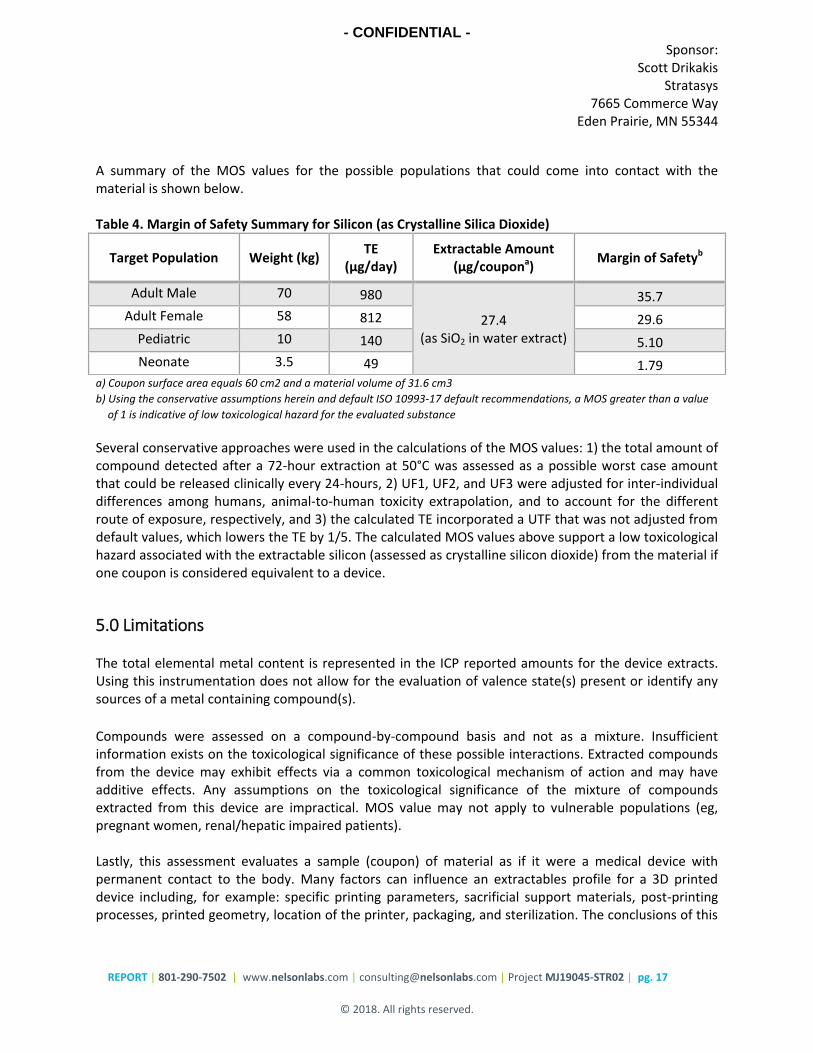
A summary of the MOS values for the possible populations that could come into contact with the material is shown below. Table 4. Margin of Safety Summary for Silicon (as Crystalline Silica Dioxide)
a) Coupon surface area equals 60 cm2 and a material volume of 31.6 cm3
b) Using the conservative assumptions herein and default ISO 10993-17 default recommendations, a MOS greater than a value
of 1 is indicative of low toxicological hazard for the evaluated substance
Several conservative approaches were used in the calculations of the MOS values: 1) the total amount of compound detected after a 72-hour extraction at 50°C was assessed as a possible worst case amount that could be released clinically every 24-hours, 2) UF1, UF2, and UF3 were adjusted for inter-individual differences among humans, animal-to-human toxicity extrapolation, and to account for the different route of exposure, respectively, and 3) the calculated TE incorporated a UTF that was not adjusted from default values, which lowers the TE by 1/5. The calculated MOS values above support a low toxicological hazard associated with the extractable silicon (assessed as crystalline silicon dioxide) from the material if one coupon is considered equivalent to a device.
5.0 Limitations The total elemental metal content is represented in the ICP reported amounts for the device extracts. Using this instrumentation does not allow for the evaluation of valence state(s) present or identify any sources of a metal containing compound(s).
Compounds were assessed on a compound-by-compound basis and not as a mixture. Insufficient information exists on the toxicological significance of these possible interactions. Extracted compounds from the device may exhibit effects via a common toxicological mechanism of action and may have additive effects. Any assumptions on the toxicological significance of the mixture of compounds extracted from this device are impractical. MOS value may not apply to vulnerable populations (eg, pregnant women, renal/hepatic impaired patients). Lastly, this assessment evaluates a sample (coupon) of material as if it were a medical device with permanent contact to the body. Many factors can influence an extractables profile for a 3D printed device including, for example: specific printing parameters, sacrificial support materials, post-printing processes, printed geometry, location of the printer, packaging, and sterilization. The conclusions of this
Target Population Weight (kg) TE
(µg/day) Extractable Amount
(µg/coupona) Margin of Safetyb
Adult Male 70 980
27.4 (as SiO2 in water extract)
35.7
Adult Female 58 812 29.6
Pediatric 10 140 5.10
Neonate 3.5 49 1.79
- CONFIDENTIAL - Sponsor:
Scott Drikakis Stratasys
7665 Commerce Way Eden Prairie, MN 55344
REPORT | 801-290-7502 | www.nelsonlabs.com | [email protected] | Project MJ19045-STR02 | pg. 18
© 2018. All rights reserved.
assessment should be understood in this context, and any devices manufactured from this material should by independently evaluate so that all variables affecting toxicity can be considered.
6.0 Conclusion This risk assessment was supported by information gathered from an extractable chemical characterization study on coupons of the material as printed, published literature on the quantitatively detected compounds, and the derived favorable MOS for these compounds. This risk assessment indicates that the likelihood of adverse effects from the material is considered low for all these compounds. This assessment also indicates that acute, subacute/subchronic, and chronic toxicity, genotoxicity, and carcinogenicity from the exposure to these compounds from the coupon of material as printed are not expected. Assessment completed by:
Matthew R. Jorgensen, PhD Chemistry and Materials Scientist Nelson Laboratories, LLC P: 801-290-7794 E: [email protected]
Assessment reviewed by:
Thor S. Rollins, B.S., RM (NRCM) Director, Toxicology and E&L Consulting Nelson Laboratories, LLC P: 801-290-7832 E: [email protected]
- CONFIDENTIAL - Sponsor:
Scott Drikakis Stratasys
7665 Commerce Way Eden Prairie, MN 55344
REPORT | 801-290-7502 | www.nelsonlabs.com | [email protected] | Project MJ19045-STR02 | pg. 19
© 2018. All rights reserved.
7.0 References 1. ANSI/AAMI/ISO. 10993-17: Biological evaluation of medical devices - Part 17: Establishment of allowable limits for leachable substances. Arlington, VA Association for the advancement of Medical Instrumentation; 2008. 2. Dourson ML, Stara JF. Regulatory history and experimental support of uncertainty (safety) factors. Regulatory toxicology and pharmacology : RTP. 1983; 3(3): 224-38. 3. Dourson ML, and DeRosa, C.T. Statistics in Toxicology. New York: Gordon and Breach; 1991. 4. Q3D Elemental Impurities Guidance for Industry. In: U.S. Department of Health and Human Services FaDA, Center for Drug Evaluation and Research, Center for Biologics Evaluation and Research, editor.; 2015. 5. Virk SA, Eslick GD. Brief Report: Meta-analysis of Antacid Use and Alzheimer's Disease: Implications for the Aluminum Hypothesis. Epidemiology. 2015; 26(5): 769-73. 6. Guidelines for drinking-water quality. 2011 2011 [cited 24 Feb 2017]; Fourth:[Available from: http://www.who.int/water_sanitation_health/publications/2011/dwq_guidelines/en/ 7. Draft - Biological evaluation of medical devices — Part XX: Application of the threshold of toxicological concern (TTC) for assessing biocompatibility of extractable substances from medical devices. In: Standarization IOf, editor. ISO/PDTS 10993-XX:2016(E); 2016. 8. Kroes R, Kleiner J, Renwick A. The threshold of toxicological concern concept in risk assessment. Toxicological sciences. 2005; 86(2): 226-30. 9. Munro I, Renwick A, Danielewska-Nikiel B. The threshold of toxicological concern (TTC) in risk assessment. Toxicology letters. 2008; 180(2): 151-6. 10. Hennes E. An overview of values for the threshold of toxicological concern. Toxicology letters. 2012; 211(3): 296-303. 11. Guideline IHT. Assessment and Control of DNA Reactive (Mutagenic) Impurities in Pharmaceuticals to Limit Potential Carcinogenic Risk. International Conference on Harmonization of Technical Requirements for Registration of Pharmaceuticals for Human Use (ICH): Geneva; 2014: Citeseer; 2014. 12. Review of the Threshold of Toxicological Concern (TTC) approach and development of new TTC decision tree. European Food Safety Authority and World Health Organization; 2016. 13. Cramer G, Ford R, Hall R. Estimation of toxic hazard—a decision tree approach. Food and cosmetics toxicology. 1976; 16(3): 255-76. 14. Munro IC, Ford RA, Kennepohl E, Sprenger J. Correlation of structural class with no-observed-effect levels: a proposal for establishing a threshold of concern. Food and Chemical Toxicology. 1996; 34(9): 829-67. 15. Nimni ME, Han B, Cordoba F. Are we getting enough sulfur in our diet? Nutrition & metabolism. 2007; 4: 24-. 16. Soni MG, White SM, Flamm WG, Burdock GA. Safety evaluation of dietary aluminum. Regulatory toxicology and pharmacology : RTP. 2001; 33(1): 66-79. 17. Greger JL, Sutherland JE. Aluminum exposure and metabolism. Crit Rev Clin Lab Sci. 1997; 34(5): 439-74. 18. Public Health Statement for Aluminum. 2008 [cited; Available from: http://www.atsdr.cdc.gov/phs/phs.asp?id=1076&tid=34
- CONFIDENTIAL - Sponsor:
Scott Drikakis Stratasys
7665 Commerce Way Eden Prairie, MN 55344
REPORT | 801-290-7502 | www.nelsonlabs.com | [email protected] | Project MJ19045-STR02 | pg. 20
© 2018. All rights reserved.
19. Yokel RA. The toxicology of aluminum in the brain: a review. Neurotoxicology. 2000; 21(5): 813-28. 20. Hulla JE. Hayes' Princliples and Methods of Toxicology. 6th Edition ed. Boca Raton, Florida: CRC Press; 2014. 21. Willhite CC, Ball GL, McLellan CJ. Total allowable concentrations of monomeric inorganic aluminum and hydrated aluminum silicates in drinking water. Crit Rev Toxicol. 2012; 42(5): 358-442. 22. McLachlan DR, Lukiw WJ, Kruck TP. New evidence for an active role of aluminum in Alzheimer's disease. Can J Neurol Sci. 1989; 16(4 Suppl): 490-7. 23. Rifat SL, Eastwood MR, McLachlan DR, Corey PN. Effect of exposure of miners to aluminium powder. Lancet. 1990; 336(8724): 1162-5. 24. Alfrey AC. Aluminum toxicity in patients with chronic renal failure. Ther Drug Monit. 1993; 15(6): 593-7. 25. Klatzo I, Wisniewski H, Streicher E. Experimental Production of Neurofibrillary Degeneration. I. Light Microscopic Observations. J Neuropathol Exp Neurol. 1965; 24: 187-99. 26. Bondy SC. Prolonged exposure to low levels of aluminum leads to changes associated with brain aging and neurodegeneration. Toxicology. 2014; 315: 1-7. 27. Graves AB, Rosner D, Echeverria D, Mortimer JA, Larson EB. Occupational exposures to solvents and aluminium and estimated risk of Alzheimer's disease. Occup Environ Med. 1998; 55(9): 627-33. 28. Savory J, Exley C, Forbes WF, Huang Y, Joshi JG, Kruck T, et al. Can the controversy of the role of aluminum in Alzheimer's disease be resolved? What are the suggested approaches to this controversy and methodological issues to be considered? J Toxicol Environ Health. 1996; 48(6): 615-35. 29. Golub MS, Germann SL, Han B, Keen CL. Lifelong feeding of a high aluminum diet to mice. Toxicology. 2000; 150(1-3): 107-17. 30. Rainey CJ, Nyquist LA, Christensen RE, Strong PL, Culver BD, Coughlin JR. Daily boron intake from the American diet. J Am Diet Assoc. 1999; 99(3): 335-40. 31. Pizzorno L. Nothing Boring About Boron. Integrative medicine (Encinitas, Calif). 2015; 14(4): 35-48. 32. Hunt CD. Methods in Nutritional Research, Chapter 14: Dietary Boron Deficiency and Supplementation. 1997 [cited 28 Sep 2017]; Available from: https://naldc.nal.usda.gov/naldc/download.xhtml?id=45629&content=PDF 33. Von Burg R. Boron, boric acid, borates and boron oxide. J Appl Toxicol. 1992; 12(2): 149-52. 34. Siegel E, Wason S. Boric acid toxicity. Pediatr Clin North Am. 1986; 33(2): 363-7. 35. Litovitz TL, Klein-Schwartz W, Oderda GM, Schmitz BF. Clinical manifestations of toxicity in a series of 784 boric acid ingestions. Am J Emerg Med. 1988; 6(3): 209-13. 36. Lung D, Clancy C. "Boiled lobster" rash of acute boric acid toxicity. Clin Toxicol (Phila). 2009; 47(5): 432. 37. Chapin RE, Ku WW. The reproductive toxicity of boric acid. Environ Health Perspect. 1994; 102 Suppl 7: 87-91. 38. Fail PA, George JD, Seely JC, Grizzle TB, Heindel JJ. Reproductive toxicity of boric acid in Swiss (CD-1) mice: assessment using the continuous breeding protocol. Fundam Appl Toxicol. 1991; 17(2): 225-39. 39. Moore JA. An assessment of boric acid and borax using the IEHR Evaluative Process for Assessing Human Developmental and Reproductive Toxicity of Agents. Expert Scientific Committee. Reprod Toxicol. 1997; 11(1): 123-60.

- CONFIDENTIAL - Sponsor:
Scott Drikakis Stratasys
7665 Commerce Way Eden Prairie, MN 55344
REPORT | 801-290-7502 | www.nelsonlabs.com | [email protected] | Project MJ19045-STR02 | pg. 21
© 2018. All rights reserved.
40. Moorman WJ, Ahlers HW, Chapin RE, Daston GP, Foster PM, Kavlock RJ, et al. Prioritization of NTP reproductive toxicants for field studies. Reprod Toxicol. 2000; 14(4): 293-301. 41. Blevins DG, Lukaszewski KM. Boron in Plant Structure and Function. Annu Rev Plant Physiol Plant Mol Biol. 1998; 49: 481-500. 42. Otten JJ HJ, Meyers LD. Dietary Reference Intakes: The Essential Guide to Nutrient Requirements. Washington DC: The National Academies Press; 2006. 43. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc. Washington (DC); 2001. 44. Nielsen FH. Biochemical and physiologic consequences of boron deprivation in humans. Environ Health Perspect. 1994; 102 Suppl 7: 59-63. 45. Sarikaya R, Erciyas K, Kara MI, Sezer U, Erciyas AF, Ay S. Evaluation of genotoxic and antigenotoxic effects of boron by the somatic mutation and recombination test (SMART) on Drosophila. Drug and chemical toxicology. 2016; 39(4): 400-6. 46. Ince S, Kucukkurt I, Demirel HH, Acaroz DA, Akbel E, Cigerci IH. Protective effects of boron on cyclophosphamide induced lipid peroxidation and genotoxicity in rats. Chemosphere. 2014; 108: 197-204. 47. Barbafieri M, Giorgetti L. Contaminant bioavailability in soil and phytotoxicity/genotoxicity tests in Vicia faba L.: a case study of boron contamination. Environmental science and pollution research international. 2016; 23(23): 24327-36. 48. Gulsoy N, Yavas C, Mutlu O. Genotoxic effects of boric acid and borax in zebrafish, Danio rerio using alkaline comet assay. EXCLI journal. 2015; 14: 890-9. 49. Scott H, Walmsley RM. Ames positive boronic acids are not all eukaryotic genotoxins. Mutation research Genetic toxicology and environmental mutagenesis. 2015; 777: 68-72. 50. Boron - ToxFaqs. Centers for Disease Control, Agency for Toxic Substances and Disease Registry, Division of Toxicology and Human Health Sciences 2007. 51. F. Aguilar URC, B. Dusemund, P. Galtier, J. Gilbert, D.M. Gott, S. Grilli, R. Guertler, G.E.N. Kass, J. Koenig, C. Lambré, J-C. Larsen, J-C. Leblanc, A. Mortensen, D. Parent-Massin, I. Pratt, I.M.C.M. Rietjens, I. Stankovic, P. Tobback, T. Verguieva, R.A. Woutersen. . Inability to assess the safety of silicon-enriched yeast added for nutritional purposes as a source of silicon in food supplements and the bioavailability of silicon from this source, based on the supporting dossier EFDA Journal. 2009; (1070): 1-6. 52. SIDS O. SIDS Initial Assessment Report for Soluble Silicates. In: 18 S, editor. Paris, France 2004. 53. Yu T, Greish K, McGill LD, Ray A, Ghandehari H. Influence of geometry, porosity, and surface characteristics of silica nanoparticles on acute toxicity: their vasculature effect and tolerance threshold. ACS Nano. 2012; 6(3): 2289-301. 54. Jampilek J, Zaruba K, Oravec M, Kunes M, Babula P, Ulbrich P, et al. Preparation of silica nanoparticles loaded with nootropics and their in vivo permeation through blood-brain barrier. Biomed Res Int. 2015; 2015: 812673. 55. Zielinski J, Moller AM, Frenz M, Mevissen M. Evaluation of endocytosis of silica particles used in biodegradable implants in the brain. Nanomedicine. 2016. 56. Nishimori H, Kondoh M, Isoda K, Tsunoda S, Tsutsumi Y, Yagi K. Silica nanoparticles as hepatotoxicants. Eur J Pharm Biopharm. 2009; 72(3): 496-501. 57. Sergey Ivanov SZ, Galina Yukina, Vladimir Tomson, Dmitry Korolev,, Galagudza M. In Vivo Toxicity of Intravenously Administered Silica and Silicon Nanoparticles. Materials. 2012; 5: 1873-89. 58. Orginization WH. Silica Monograph. In: (IARC) IAfRoC, editor.; 1997.

- CONFIDENTIAL - Sponsor:
Scott Drikakis Stratasys
7665 Commerce Way Eden Prairie, MN 55344
REPORT | 801-290-7502 | www.nelsonlabs.com | [email protected] | Project MJ19045-STR02 | pg. 22
© 2018. All rights reserved.
59. Borm PJ, Tran L, Donaldson K. The carcinogenic action of crystalline silica: a review of the evidence supporting secondary inflammation-driven genotoxicity as a principal mechanism. Crit Rev Toxicol. 2011; 41(9): 756-70.





![ENDOSULFAN - UNECE€¦ · environmental risk assessment [ii] and the Health Effects Division (HED)´s part on human health risk assessment [iii]. A comprehensive toxicological profile](https://img.dokumen.tips/doc/110x75/60602cad2b30a0548c0e3839/endosulfan-environmental-risk-assessment-ii-and-the-health-effects-division.jpg)























