-
8/10/2019 Toxic Ol
1/10
-
8/10/2019 Toxic Ol
2/10
These recent data indicate that GA is the primary causativeagent
for the high-dose developmental effects of EG in rodents,with the
accompanying metabolic acidosis playing a second-ary, exacerbating
role at higher dose levels.
The pharmacokinetics of EG metabolism have been studiedin
different animal models by several investigators. Most re-cently,
Frantz et al. (1996a,b,c) reported on the dose- androute-dependency
of EG metabolism in male and nonpregnantfemale rats and mice. In
particular, these authors reporteddose-proportional
pharmacokinetics for the elimination fromblood of orally (gavage)
administered EG in female rats andmice over the dose range
investigated (101000 mg EG/kgbw), with a shift to increasing
urinary elimination of EG and itsmajor metabolite GA, with
increasing dose. However, theirdata on blood levels of GA indicated
nonlinearity across doses,with a 1000- to 10,000-fold increase in
GA blood levels for a100-fold increase in administered EG dose.
This disproportion-ality for GA was also reected by an increased
urinary elimi-nation of GA with increasing administered EG doses.
Thus,administration of high doses of EG via gavage had the
potentialto result in accumulation of GA, the proximate
developmentaltoxicant. In contrast, dermal exposures of up to 1000
mg/kgshowed no such shift in metabolism, with the majority of theEG
dose being eliminated as CO 2.
No data have been published on the potential effect of pregnancy
on EG metabolism. The physiology of pregnancyresults in major
changes in physiological parameters thatcould have considerable
impact on pharmacokinetics andmetabolism of EG. Examples include
overall weight gainand increase in organ size, particularly liver;
increase intotal body water and blood volume; increased blood ow
to
uterus; decreased overall plasma protein level but increasesin
specic plasma proteins; altered hormone blood levels;decreased GI
motility and increased GI transit time (Miller,1983). These
parameters do not offer a comprehensive listof pregnancy-related
physiological changes, but do repre-sent a few that could easily
affect the pharmacokinetics andmetabolism of EG. Any
pregnancy-related changes in EGmetabolism and pharmacokinetics
would be expected tohave impact on the formation and elimination of
the prox-imate developmental toxicant, GA, and could be critical
tounderstanding the species-specic developmental toxicity of EG.
This study investigated the effect of pregnancy (GD 10)
on the pharmacokinetics and metabolism of EG in
femaleSprague-Dawley rats, comparing blood concentration-timeproles
and urinary excretion of parent and metabolitesacross doses between
pregnant and nonpregnant rats. GD 10was chosen based on prior in
vivo (Khera, 1991) and whole-embryo culture studies (Carney et al.,
1996) showing thisperiod to be highly sensitive to EG toxicity.
This study wasconducted in compliance with the requirements of
GoodLaboratory Practices (EPA-TSCA, 1989; OECD, 1982).
MATERIALS AND METHODS
Chemicals. Ethylene glycol (EG; 13C 2-labelled) was obtained
from IsotecInc. (Miamisburg, OH; purity 96.7% via 1H-NMR).
Pentauorobenzoyl chlo-ride and N -(tert-butyldimethylsilyl)- N
-methyltriuoroacetamide (MTBSTFA)were obtained from Aldrich
Chemical Company (Milwaukee, WI). All othercompounds and solvents
were reagent grade or better.
Test animals. Adult female (nonpregnant and time-mated)
Sprague-Daw-ley rats were purchased from Hilltop Lab Animals,
Scottsdale, Pennsylvania.Rats were shipped on GD 8 and arrived at
our laboratory on GD 9. All rats hadan in-dwelling jugular vein
cannula implanted at the suppliers facility on GD6 (or the same
calendar day for the nonpregnant rats). The rats were allowedto
recover for 2 days prior to being shipped. The cannula was
exteriorizedunder light methoxyurane anesthesia upon arrival at the
laboratory. Similarsurgical procedures in pregnant animals have
been used in the past in thislaboratory, and no untoward effects on
pregnancy were observed (Carney etal., 1999). Upon receipt the
animals were examined by a veterinarian andfound to be in good
health. The animals were acclimated to the laboratoryenvironment
for 1 day prior to dose administration. The rooms in which
theanimals were housed had a 12-h photocycle and are designed to
maintainadequate environmental temperature, relative humidity, and
airow for the rat.Municipal drinking water and Purina Certied
Rodent Chow #5002 (PurinaMills, Inc., St. Louis, MO) were provided
ad libitum during the predosing
period, except that on the day prior to dosing, a uniform amount
of chow wasfed (approximately 15 gram/rat). Also, food was
completely withdrawn ap-proximately 2 h prior to the administration
of the test material and was returnedabout 4 h postdosing. These
steps were intended to minimize between-animalvariation in
absorption of test material, yet limit any deleterious effects of
feedrestriction on the pregnant animal. Rats were selected from
those with patent jugular vein cannulae on GD 10 and then were
randomly assigned to treatmentgroups using a computerized procedure
based on animal body weight. Ratswere identied by a uniquely
numbered metal eartag.
Dose administration. 13C-labelled EG, as an aqueous solution,
was ad-ministered to 5 groups of 4 time-mated female Sprague-Dawley
rats by gavage,with blunted feeding needles, at the following dose
levels: 2500, 1000, 500,150, and 10 mg EG/kg body weight.
13C-labelled EG was also administered, inthe same fashion, to 2
groups of nonpregnant female rats (2500 mg EG/kg, n5; 10 mg EG/kg,
n 4). The target dose volume for all animal groups was 5
ml/kg. The experiment was divided into 2 replicates of
approximately 1415rats each, due to the number of rats involved.
Immediately following dosing,the animals were placed in glass
Roth-type metabolism cages for bloodsampling and for the separation
and collection of urine.
Specimen Collection
Urine. All urine voided during the study was collected in dry
ice-cooledtraps at 12-h intervals and the cage was rinsed with a
minimal volume ( 10ml) of deionized water. Analyses were done on
the combined urine specimenand cage rinse.
Whole blood. Approximately 0.2 ml blood/rat were collected at 0
(pre-dose), 1, 3, 6, 9, 12, 18, and 24 hours after administration
of test material.Following collection of each blood sample,
approximately 0.2 ml of heparin-ized saline was slowly injected to
ush the cannula and provide a heparin
lock.Terminal sacrice. After collection of the last blood
sample, the animals
were euthanized via carbon dioxide inhalation. The uterus of
each rat then wasexamined for implantation sites to determine
pregnancy status. Blood and urinesamples from any time-mated rats
that were found to be nonpregnant duringnecropsy were analyzed and
included in the comparative nonpregnant group,as appropriate.
Specimen analysis. Samples of whole blood and urine were
analyzed viagas chromatography-mass spectrometry (GC/MS) to
quantitate parent 13C 2-EG, and the metabolites 13C 2-GA and
13C 2-OX. Samples were derivatized as
11EG METABOLISM IN PREGNANT RATS
-
8/10/2019 Toxic Ol
3/10
described below to increase analyte volatility and detector
response. The use of a stable isotope-labeled form of EG test
material ( 13C 2-), resulted in theformation of 13C 2-labeled
metabolites (
13C 2-GA and 13C 2-OX). Analysis of
blood and urine samples via mass spectral detection allowed for
the determi-nation of 13C 2-EG and the
13C 2-labelled metabolites independent of the pres-ence of
background, and perhaps varying levels of unlabelled EG, GA, andOX.
Unlabeled GA and OX served as internal standards in the
quantitation of 13C 2-labelled GA and OX. These unlabeled analogs
were added to the blood
and urine samples at concentrations of approximately 100 g/ml or
1000g/ml, respectively, which was approximately 50 background
levels of these
compounds. Deuterium-labelled EG (D 4-EG) was utilized as an
internal stan-dard in the quantitation of 13C 2-EG. Quantitation
limits for
13C 2-EG, 13C 2-GA,
and 13C 2-OX in blood were 0.1, 2.1, and 4.9 g/g blood,
respectively. Quan-titation limits for 13C 2-EG,
13C 2-GA, and 13C 2-OX in urine were 1.0, 0.94, and
2.0 g/g urine, respectively.Aliquots of each blood sample from
the time-course experiment (approxi-
mately 0.1 g) were added to 0.9 ml of an internal standard
solution (0.9 ml 1NHCl containing 11.5 g/ml D 4-EG) in a 4-ml glass
vial. An additional 0.1 mlof a second internal standard solution
(approximately 100 g/ml GA and OX)was also added to each sample.
Samples were treated with 0.51 g NaCl andextracted with methyl- t
-butyl ether (MTBE) containing 0.5% tri- n-octylphos-phine oxide (2
2 ml). The combined MTBE extracts (containing GA andOX) were
evaporated to dryness (nitrogen stream), reconstituted in 0.9
ml
toluene and derivatized with 100 l N -methyl- N -(t
-butyldimethylsilyl)triu-oroacetamide (60C 1 h). The derivatized
sample was transferred to a 2-mlglass vial for analysis of 13 C
2-GA and
13 C 2-OX. A second aliquot of each bloodsample (approx. 0.1 g)
was prepared as above for analysis of parent 13C 2-EG,without NaCl,
to minimize chromatographic interferences. The aqueous
phaseremaining after MTBE extraction (containing EG) was treated
with 300 l 5NNaOH and derivatized with 20 l pentauorobenzoyl
chloride and 1 mltoluene (vortex-mixed at 45C 30 min). The toluene
layer was transferred toa 2-ml glass vial for analysis of 13C
2-EG.
Aliquots (0.1 g) of urine samples were added to 0.8 ml 1N HCl,
and fortiedwith 5 l or 100 l of internal standard solution (approx.
1000 g/ml GA, OXand D 4-EG) and extracted with MTBE containing 0.5%
tri- n-octylphosphineoxide (2 2 ml). Further treatment of the
combined MTBE extracts (con-taining GA and OX) was as described
above for the blood samples. A secondaliquot (0.1 g) of each urine
sample was fortied with 100 l of internal
standard solution (approx. 1000 g/ml GA, OX and D 4-EG), treated
with 50l 5N NaOH and derivatized with 50 l pentauorobenzoyl
chloride and 2 mltoluene (vortex-mixed at 45C 30 min). The toluene
layer was transferred toa 2-ml glass vial for analysis of 13C
2-EG.
GC-MS analyses were performed on a Finnigan TSQ-700, SSQ-710,
orHewlett Packard 5989X mass spectrometer (Finnigan MAT, San Jose,
CA;Hewlett Packard, Avondale, PA), equipped with a Hewlett Packard
5890 gaschromatograph and a 7673A autosampler. Separations were
achieved using aJ&W DB-5 fused silica capillary column (J&W
Scientic, Folsom, CA)(GA/OX: 30 m 0.25 mm id 0.25 m lm; EG: 30 m
0.32 mm id1 m lm); helium carrier gas (10 psig) at a ow rate of
approximately 0.5ml/min; gas chromatograph oven temperature program
for GA/OX: 100C (0.5min initial hold) to 280C at 15/min, then to
300C at 25/min with injectorand capillary transfer line at 200C and
250C, respectively; gas chromato-graph oven temperature program for
EG: 100C (0.5 min initial hold) to 280Cat 20/min with injector and
capillary transfer line at 250C; 1- l autosamplerinjection (GA/OX:
40 ml split; EG: 0.1 min splitless). The mass
spectrometerconditions for GA/OX were electron impact ionization
(EI): ion source tem-perature, 150C; ionizing current, 0.4 mA;
electron energy, 70 eV. The massspectrometer conditions for EG were
negative-ion chemical ionization (NCI):ion source temperature,
150C; ionizing current, 0.4 mA; electron energy, 70eV. Quantitation
of the t-butyldimethylsilyl derivatives of GA, 13C 2-GA, OXand 13C
2-OX was achieved by selected ion monitoring (m/z 247, 249, 261
and263 @ 70 msec/ion/scan). Quantitation of the pentauorobenzoyl
ester deriv-atives of 13C 2-EG and D 4-EG was achieved by selected
ion monitoring (m/z452 and 454 @ 75 msec/ion/scan).
Statistics and data analysis. Descriptive statistics were used
(i.e., meanSD). Results were generally expressed as percentage of
administered doseand/or as g of parent EG or metabolite. Certain
pharmacokinetic parameterswere estimated for blood data, including
Cmax and AUC for parent materialand GA (Gibaldi and Perrier, 1982),
time to reach maximum blood levels(Tmax), and half-life of
elimination ( t1/2). The reported pharmacokinetic (PK)values were
estimated using a commercially available computer modelingprogram
(PK Solutions v2.02, Summit Research Services, Ashland, OH).
RESULTS
Actual concentrations of EG in the various dose solutionsranged
from 95102% of target. Administered dosage of EGranged from 92100%
of target across all dose groups. Atdosing, individual animal body
weights ranged from 211 to264 g across all dose groups. There were
no remarkablechanges in behavior or demeanor recorded during
thedaily animal observations. At terminal sacrice, the preg-nancy
status of the time-mated rats was determined, and thenumber of
implantations/animal ranged from 722 for thepregnant rats.
Blood Concentration-Time Course of EG and Metabolites
Individual blood samples were analyzed for parent EG, GA,and OX
concentrations. The mean values for the concentration-time courses
of EG, GA, and OX are presented in Table 1, andFigures 1 and 2
depict the concentration-time course prolesfor EG and GA,
respectively. The pharmacokinetic parameters,estimated using the
blood data, are presented in Table 2. Nopharmacokinetic parameters,
including area-under-the-curve(AUC) data, were calculated for the
OX concentration-timecurve, as the blood levels of 13C 2-OX were
either at or near thequantitation limit of 4.9 g/g blood in all
samples analyzed.
Comparison of the data collected for pregnant (P) and
non-pregnant (NP) groups at both the high (2500 mg EG/kg) andlow
(10 mg EG/kg) dose clearly demonstrated that pregnancyat this stage
(GD 1011) did not have any signicant impact onthe blood
concentration-time proles of EG, GA, or OX. Asshown in Figures 1
and 2, the time-courses for the mean EGand GA blood levels of P and
NP rats administered either 2500or 10 mg EG/kg were superimposable.
Thus, the pharmacoki-netic parameters summarized in Table 2 did not
differ signif-icantly between the P and NP dose groups.
Time course of parent EG. Parent EG was not detectable inany
pretreatment blood samples. The Tmax for EG for all dosegroups
occurred as expected at 1 h postdosing, the rst sam-
pling time. The blood concentration of EG decreased in a
linearfashion following the 1 h Cmax. Blood EG was no
longerdetectable for the low dose groups (10 mg EG/kg) by 12
hpostdosing, and for the 150 and 500 mg EG/kg dose groups by24 h
postdosing, although parent EG was detected at 24 hpostdosing for
the 2500 and 1000 mg EG/kg dose groups.
Comparison of Cmax values across dose levels demon-strated
linearity in the dose-response for parent EG for all dosegroups
except the 2500 mg EG/kg. The linearity of the dose-
12 POTTENGER, CARNEY, AND BARTELS
-
8/10/2019 Toxic Ol
4/10
response for parent EG was also supported by comparison of AUC
values for EG, where the AUC increased across doselevels
proportionately with dose for all the groups, except thehigh dose.
The 1000 and 2500 mg EG/kg doses differed by2.5-fold, while the
respective AUC and Cmax values demon-strated about a 4-fold
difference. This disproportionate in-crease may indicate that blood
clearance of EG was initiallysaturated at the 2500 mg EG/kg dose
level. Such initial satu-ration could be due to either saturation
of metabolic clearanceof EG from blood (i.e., saturation of
formation of GA fromEG) or to saturation of renal elimination of EG
from blood.The estimated t 1/2 of elimination of EG from blood was
short,less than 2 h for all dose levels, indicating that, overall,
parentEG was rapidly cleared from blood. Thus, any initial
saturationin blood levels at the high dose did not last long enough
to alterits half-life of elimination from blood.
Time course of GA in blood. GA, recognized as an endo-genously
present compound (Jolivet et al., 1985; Poore et al.,1997), has
been shown to be present in human plasma and
urine at concentrations of approximately 0.1 and 20
g/g,respectively (Hoffman et al., 1989; Tanaka et al., 1980).
Anal-ysis of control blood samples from untreated rats, in the
ab-sence of added GA internal standard, afforded true
concentra-tions of endogenous, background GA of up to 2.1 g/g
ratblood (data not shown).
Blood levels of the 13C 2-GA, derived from the test
material,increased to a peak at 3 h postdosing, except for the 10
mgEG/kg dose groups, which demonstrated nondetectable levelsof 13C
2-GA over the entire 24-h time course. For all dosegroups, blood
levels of GA decreased by 24 h postdosing toundetectable levels.
Elimination of GA from blood appearedbiphasic until it reached
background levels, with the phasefor each curve dened as follows:
918 h (2500 mg EG/kg),618 h (1000 mg EG/kg), 612 h (500 mg EG/kg),
and 39 h(150 mg EG/kg). Estimation of the t1/2 of elimination of
GAfrom blood resulted in similar values across dose levels (1.11.9
h), based on these biphasic elimination curves. No phar-macokinetic
parameters were estimated for GA data from the10 mg EG/kg dose
groups, as those samples were below LOQlevels.
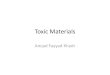
Examination of GA blood levels as a function of dosedemonstrated
nonlinear, dose-dependent kinetics. Figure 3 de-picts graphically
the Cmax blood levels determined for GA,and compares them with
estimated examples of what the Cmax
levels would have been for a linear relationship between Cmaxand
administered dose (GA Ex Cmax). At the 10 and 150 mgEG/kg dose
levels, GA blood levels appeared to be roughlyproportional to dose,
given that GA levels were 2.1 g/g forthe 10 mg EG/kg dose, as
compared to 20.6 g/g for the 150mg EG/kg dose (15-fold higher
dose). A marked shift in GAblood kinetics was observed as the dose
increased from 150 to500 mg EG/kg. Over this 3.3-fold dose
interval, the Cmax forGA increased by a factor of 6.4, which was a
clear dispropor-
tionate increase. This disproportionality with dose persisted
toa somewhat lesser degree between the 500 and 1000 mg EG/kgdose
levels, where the 2-fold increase in dose brought about a2.8-fold
increase in GA Cmax.
A similar shift, with a disproportionate increase, was foundfor
the AUC values obtained from the GA blood concentration-time
courses, particularly between 150 to 500 mg EG/kg. Thisshift is
depicted graphically in Figure 3, where the actual AUCvalues for GA
are compared with estimated values for a linearrelationship between
AUC and administered dose (GA ExAUC). Estimated AUC for GA
increased by 7.6- and 2.9-foldfor a 3.3- and a 2-fold increase in
administered dose, for the150500 and 500-1000 mg EG/kg dose group
intervals, re-spectively. Thus, elimination of GA from blood
demonstratedsaturation at dose levels of 500 mg EG/kg and
above.
Comparison of GA Cmax values for the 2 top dose levelsshowed a
less than dose-proportionate increase, with only a25% increase for
a 2.5-fold increase in dose. In fact, the GACmax for 1000 mg EG/kg
was basically equivalent to the GACmax for the 2500 mg EG/kg dose
level. However, AUCvalues for GA were dose-proportionate for this
dose interval of 1000 to 2500 mg EG/kg, indicating that over time,
a similarfraction of administered dose of EG was converted to GA
forboth 1000 and 2500 mg EG/kg.
Time course of OX in blood. OX, another endogenouslypresent
compound (Poore et al., 1997; Ribaya-Mercado andGershoff, 1984),
has been found in human urine at concentra-tions of approximately
20 g/g (Tanaka et al., 1980). Analysisof control blood samples from
untreated rats, in the absence of added OX internal standard,
afforded true concentrations of endogenous, unlabelled OX of up to
4.9 g/g rat blood (datanot shown).
The concentrations of blood 13
C 2-OX, derived from the testmaterial, varied between
undetectable and about 2 times thelimit of quantitation (4.9 g OX/g
blood) over the 24-h col-lection period. There was no obvious
pattern to OX bloodlevels; while the 2500 mg EG/kg dose groups had
the mosttime points with detectable OX levels, the highest mean
OXvalue was obtained with a sample from the 18-h 1000 mgEG/kg dose
group (9.2 5.3). Based on these data, it does notappear that OX
accumulates in P or NP female rats followingoral gavage
administration of EG. Given what appeared asmostly trace levels of
OX, no additional analysis of the OXdata was indicated or feasible.
The lack of any obvious dose-response relationship in OX blood
levels over such a large doserange (250-fold increase) suggests
that OX does not play amajor role in the expression of
developmental toxicity of EG inrats.
Urinary Proles and Interval Excretion of EG, GA, and OX
Urinary 13C-labeled-EG, -GA, and -OX levels were quanti-ed over
12-h intervals, and the results are summarized inTable 3, both as
total amount excreted ( g) and as fraction of
13EG METABOLISM IN PREGNANT RATS
-
8/10/2019 Toxic Ol
5/10
TABLE 1Concentration-Time Course for Mean Blood Levels of
Ethylene Glycol (EG), Glycolic Acid (GA), and Oxalic Acid (OA)
following Oral Administration to Female S-D Rats
Time
EG GA OX
Mean a SD Mean SD Mean SD
High dose
2500 mg/kg NP0 h NQ NA NQ NA NQ NA1 h 2795 536 252 39.5 NQ NA3 h
1908 221 432 62.1 NQ NA6 h 539 186 364 59.4 NQ NA9 h 180 41.4 234
52.6 NQ NA12 h 49.0 14.6 122 48.4 NQ NA18 h 4.1 4.1 NQ NA NQ NA24 h
1.1 0.9 NQ NA NQ NA
2500 mg/kg P b
0 h NQ c NA NQ NA NQ NA1 h 3528 1599 313 79.2 NQ NA3 h 1693 344
452 125 5.9 0.76 h 482 33.0 359 77.4 NQ NA9 h 155 44.1 253 92.0 5.7
0.612 h 42.1 22.6 126 75.0 6.4 2.218 h 2.0 1.1 4.7 5.6 NQ NA24 h
0.5 0.3 NQ NA 5.5 0.6
1000 mg/kg P0 h NQ NA NQ NA NQ NA1 h 886 90.6 213 44.8 NQ NA3 h
450 51.8 363 89.7 NQ NA6 h 127 30.7 155 16.1 NQ NA9 h 23.6 7.8 40.7
11.7 NQ NA12 h 3.9 1.4 2.0 1.1 NQ NA18 h 0.6 0.2 NQ NA 9.2 5.324 h
0.2 0.1 NQ NA NQ NA
500 mg/kg P0 h NQ NA NQ NA NQ NA1 h 392 46.8 80.7 9.8 NQ NA3 h
188 27.3 131 23.9 NQ NA6 h 40.5 12.0 60.5 6.9 NQ NA9 h 7.1 0.6 2.1
1.5 NQ NA12 h 1.2 0.3 NQ NA NQ NA18 h 0.3 0.4 NQ NA NQ NA24 h NQ NA
NQ NA NQ NA
150 mg/kg P0 h NQ NA NQ NA NQ NA1 h 88.9 48.6 15.8 2.8 NQ NA3 h
43.4 32.0 20.6 7.1 7.0 2.96 h 13.3 0.9 2.0 0.7 NQ NA9 h 2.3 0.7 NQ
NA NQ NA
12 h 0.5 0.3 NQ NA NQ NA18 h 0.1 0.1 NQ NA NQ NA24 h NQ NA NQ NA
NQ NA
14 POTTENGER, CARNEY, AND BARTELS
-
8/10/2019 Toxic Ol
6/10
the administered dose. Again, there were no substantial
differ-ences between the P and NP dose groups, at comparable
doselevels. Therefore, gestation has no impact on urinary
elimina-tion of orally administered EG to female rats at this stage
of pregnancy (GD 1011).
Overall urinary elimination of EG and its metabolites
dem-onstrated dose-dependency, with the high dose groups (2500
mg EG/kg) eliminating almost 70% of administered dose inurine,
compared with about 16% of administered dose elimi-nated via urine
by the low dose groups (10 mg EG/kg).
Quantitation of individual metabolites in urine demonstratedthat
the shift in urinary elimination was mainly due to in-creased
urinary GA and EG, and not to increased eliminationof OX (Table 3).
Parent EG was always detectable in urine.
FIG. 1. Concentration-time prole of unchanged parent ethylene
glycol(EG) in the blood of pregnant or nonpregnant female S-D rats
following oraladministration of EG. Symbols represent the mean SD
from 5 rats. LOQ0.1 g EG/g blood.
FIG. 2. Concentration-time prole of glycolic acid (GA) in the
blood of pregnant or nonpregnant female S-D rats following oral
administration of EG.Symbols represent the mean SD from 5 rats. GA
was not quantiable at anytime points for both of the 10 mg EG/kg
dose groups. LOQ 2.1 g GA/gblood.
TABLE 1 Continued
Time
EG GA OX
Mean a SD Mean SD Mean SD
Low dose
10 mg/kg NP0 h NQ NA NQ NA NQ NA1 h 9.3 2.5 NQ NA NQ NA3 h 3.8
0.5 NQ NA NQ NA6 h 0.9 0.3 NQ NA NQ NA9 h 0.2 0.1 NQ NA NQ NA12 h
NQ NA NQ NA NQ NA18 h NQ NA NQ NA NQ NA24 h NQ NA NQ NA NQ NA
10 mg/kg P0 h NQ NA NQ NA NQ NA1 h 7.9 0.6 NQ NA NQ NA3 h 3.4
0.5 NQ NA NQ NA6 h 0.7 0.3 NQ NA NQ NA9 h 0.1 0.1 NQ NA NQ NA12 h
NQ NA NQ NA NQ NA
18 h NQ NA NQ NA NQ NA24 h NQ NA NQ NA 5.3 0.6
Note. EG, GA, and OX given in g/g blood.a Values represent mean
SD from 5 rats.b P, pregnant; NP, nonpregnant.c NQ, not quantiable
(LOQ: 0.1 g EG/g blood; 2.1 g GA/g blood; 4.9 g OX/g blood); NA,
not applicable.
15EG METABOLISM IN PREGNANT RATS
-
8/10/2019 Toxic Ol
7/10
The fraction of administered dose represented by urinary
EGincreased with increasing dose, reaching a maximum of about42% of
administered dose at the 500 mg EG/kg dose group,above which
urinary EG remained around 40%. Therefore, the
3 highest dose groups all resulted in elimination of a
similarfraction of administered dose as urinary EG. This suggests
thatrenal elimination of EG was never saturated, even at thehighest
dose level. This supports the hypothesis that the initialsaturation
in EG blood levels was due to saturation of meta-bolic conversion
of EG to GA and not to saturation of renalelimination of EG.
The increase in urinary EG elimination probably corre-sponded in
large part with saturation of metabolism of EG toGA, resulting in
an increased amount of EG available for renalelimination. In fact,
the rst collection intervals for the 500 and1000 mg EG/kg dose
groups showed 23 times as muchurinary EG as GA. Then, once the
metabolic conversion was
no longer saturated and the excess EG had cleared (i.e.,
duringthe 1224 h collection interval), the ratio of urinary
GA/EGwas roughly 1, while the overall percentage of the
administereddose eliminated in the second interval was considerably
de-
creased.Urinary GA was quantiable at all intervals, except
the
lowest dose levels for the 1224-h interval. The 150 mg EG/kgand
10 mg EG/kg dose levels resulted in similar percentages of
administered dose eliminated as urinary GA, representing onlyabout
1% of the administered dose, clearly a minor fraction.However, the
fraction of the administered dose eliminated asurinary GA then
increased with increasing dose above 150 mgEG/kg, until it was
present in roughly equal proportions withEG, as mentioned above.
Comparison across dose levels dem-onstrated a disproportionate
increase in urinary GA startingwith the 500 mg EG/kg dose group,
where the percentage of administered dose eliminated as urinary GA
increased about11-fold compared with 150 mg EG/kg, over a dose
range of only 3.3-fold. The fraction of administered dose
represented byurinary GA increased for the 1000 mg EG/kg and again
for the2500 mg EG/kg dose groups, up to about 20% and 33% of
theadministered dose, respectively. The shift in urinary GA
levelscorresponded with the shift in blood GA levels
discussedearlier, indicating that renal elimination of GA was
neversaturated.
Urinary OX represented a constant fraction of administereddose
across all dose levels. This resulted in a larger totalamount of
urinary OX with increasing dose, despite the con-tinued
endogenous/background blood concentrations of OX, asdiscussed
above.
DISCUSSION
The data presented here clearly demonstrate that the
phar-macokinetic parameters for EG and its metabolites reportedhere
were not affected by GD 1011 stage pregnancy inSprague-Dawley rats.
This signies that the rich database onEG pharmacokinetics and
metabolism, collected in NP rats,
FIG. 3. Disproportionate dose-response relationship between
orally ad-ministered dose of ethylene glycol (EG) and resulting
blood Cmax and AUCvalues quantied for its metabolite, glycolic acid
(GA), in pregnant S-D rats.Experimental data are found in Table 2.
Values for a linear response wereestimated based on the 150 mg
EG/kg dose measured values for GA, and areshown as dotted lines (-
- - -) for comparison.
TABLE 2Pharmacokinetic Parameters Estimated for EG and GA
following Oral Administration of EG to Female Rats
Parameter a Units
2500-NP b 2500-P 1000-P 500-P 150-P 10-P c 10-NP c
EG GA EG GA EG GA EG GA EG GA EG EG
Tmax h 1 3 1 3 1 3 1 3 1 3 1 1
Cmax g/g 2795 432 3528 452 886 363 392 131 88.9 20.6 7.9 9.3AUC
g-h/g 11,368 3807 11,638 4031 2928 1829 1208 641 292 84 23 27t1/2 h
1.9 1.1 1.7 1.5 1.8 1.6 1.7 1 1.7 1.4 1.4 1.5Corr. (x:y) 0.9913
0.9511 0.9915 0.9717 0.9693 0.8552 0.9714 0.8739 0.9836 0.9032
0.9828 0.9998
a PK parameters estimated using a noncompartmental analysis with
PK Solutions (v2.0.2).b NP Nonpregnant; P pregnant.c PK parameters
estimated only on EG values for 10 mg/kg dose groups, as GA and OX
data were mostly background levels.
16 POTTENGER, CARNEY, AND BARTELS
-
8/10/2019 Toxic Ol
8/10
-
8/10/2019 Toxic Ol
9/10
1000 to 2500 mg EG/kg, with about a 4-fold increase in Cmaxvs. a
2.5-fold one in administered dose. This suggests that theapparent
initial saturation of EG elimination from blood, seenat the 2500 mg
EG/kg dose, was most probably due to satura-tion of the metabolic
conversion of EG to GA, rather than tosaturation of renal
elimination of EG. The conversion of EG toGA by alcohol/aldehyde
dehydrogenase (ADH/ALDH) is oneof 2 known rate-limiting steps in
the EG metabolic pathway.The other major rate-limiting step is the
further oxidationof GA.
Overall urinary elimination (percentage of the administereddose)
was not affected by pregnancy at GD 1011, and P andNP rats
demonstrated similar urinary elimination kinetics forEG and its
metabolites for the 10 and 2500 mg EG/kg doses,respectively.
However, overall urinary elimination did demon-strate
dose-dependency, with the high dose groups (2500 mgEG/kg)
eliminating almost 70% of the administered dose inurine, compared
with about 16% of the administered doseeliminated via urine by the
low dose groups (10 mg EG/kg).This is in agreement with previously
published data demon-strating a shift in disposition of
14C-EG-derived radioactivityfrom exhalation of 14CO 2 at low doses
to urinary elimination of radioactivity at high doses following
intravenous and oraladministration of 14C-EG to female rats (Frantz
et al., 1996b;Marshall, 1982).
The shift in urinary GA levels corresponded with the shift
inblood GA levels discussed earlier, indicating that renal
elimi-nation of GA was not saturated. In fact, on a wt/wt
basis,urinary elimination of GA increased about 3.5- and 4-fold
overa 2- and 2.5-fold increase in administered dose, between 500and
1000 mg EG/kg, and between 1000 and 2500 mg EG/kg,respectively.
This suggests that the saturation in elimination of
GA from blood was due to saturation of downstream metabo-lism of
GA, and not to saturation of renal elimination of GA.Data from
Frantz et al. (1996b), demonstrating a shift in thedisposition of
14C-labeled EG, from formation of 14CO 2 at alow dose level
(presumably representing downstream metabo-lism of the GA), to
increased urinary radioactivity at a highdose level, supports the
conclusion of no saturation of renalelimination of GA. Marshall
(1982) showed that GA in urineaccounted for approximately 2% of a
20 or 200 mg EG/kgbolus dose of EG, but approximately 20% of a 1000
or 2000mg EG/kg dose.
OX blood levels remained consistently at or below quanti-tation
levels in blood, even with increasing doses of EG. These
data are consistent with a slower conversion of GA to OX
thanmetabolism of OX to downstream products such as CO 2.
Incontrast, the fraction of dose eliminated via the urine as
OXremained constant across doses, resulting in increasingamounts of
urinary OX eliminated with increased dose levelsof EG. Renal
formation of OX from EG and/or GA is onepossible explanation of the
differences between blood andurinary OX levels. If intrarenally
formed OX were then elim-inated via urine without any reabsorption,
there would not be
any reection of its formation in systemic blood OX levels.There
are no data on intrarenal formation and elimination of OX from EG.
In any case, OX was a very minor metabolite inboth blood and urine
at all dose levels, suggesting that it is nota major factor in EG
developmental toxicity. This conclusion isfurther supported by data
from a preliminary study in whichlevels of OX were measured in the
exocoelomic uid of GD 10rat conceptuses following gavage exposure
to EG. Exocoelo-mic uid OX averaged approximately 16.4 g/g (0.13
mM)after a 2500 mg EG/kg dose, and was nondetectable (LOD5 g/g)
following a 500 mg EG/kg dose (Carney et al., 1998).A rat whole
embryo culture study with OX indicated onlyminor growth inhibitory
effects at a concentration of 126
g/ml (1 mM) oxalate (Klug and Jaeckh, 1999), suggestingthat
embryonic OX levels in vivo are too low to cause signif-icant
toxicity to the embryo.
Consistent with GA being the proximate developmentaltoxicant,
the location of the shift in GA metabolism along thedose response
spectrum corresponds quite well with the dose
response for developmental toxicity in the rat, as
previouslydiscussed (NOEL 500 mg EG/kg; LOEL 1000 mg EG/kg;Carney
et al., 1996, 1999; Neeper-Bradley et al., 1995). Themean Cmax GA
blood levels from the 2500 and 1000 mgEG/kg dose groups were 452
and 363 g GA/g blood, respec-tively, indicating that very high
maternal blood levels of GAare required to cause developmental
toxicity. These valuescorrespond with about 5.9 and 4.8 mM GA,
respectively,falling between the concentrations resulting in
abnormal em-bryos (12.5 mM GA) and normal embryos (2.5 mM)
fromwhole embryo culture studies in vitro (Carney et al., 1996;Klug
and Jackh, 1999). Recent evidence also has shown thatlevels of GA
in rat exocoelomic uid are almost 2-fold higherthan in maternal rat
blood, such that the critical level of GAexposure to the embryo may
be closer to 1012 mM followingEG doses at or above 1000 mg/kg
(Carney et al ., 1998). To putthese GA levels into perspective,
clinical studies of human EGintoxications associated with
intentional ingestion showedpeak GA blood levels of 729 mM
(Jacobsen et al., 1984).However, blood GA levels associated with
normal handlingand use of EG would not be expected to even approach
thesevalues, based on the slower dose-rate for dermal and
inhalationexposures and the consequently low likelihood of
saturatingEG metabolizing enzymes.
In summary, the salient ndings of this study were: (1) the
shift in GA kinetics previously seen in NP rats also occurs inP
(GD 10 11) rats; (2) the onset of this shift occurs at a gavagedose
level of 150500 mg EG/kg; (3) the correspondence of the shift in GA
kinetics with the NOEL and LOEL for devel-opmental toxicity adds
further evidence supporting GA as theproximate developmental
toxicant; and (4) developmental tox-icity appears to require
maternal blood GA levels in the mil-limolar range. Achievement of
such high GA levels seemsplausible only for high dose, oral bolus
exposures to EG, but is
18 POTTENGER, CARNEY, AND BARTELS
-
8/10/2019 Toxic Ol
10/10
extremely unlikely for typical human occupational and
ambientexposures.
ACKNOWLEDGMENTS
Expert technical assistance in conducting this study was
provided by A.Liberacki, A. Wardynski, K. Gibson, C. Thornton, J.
Whalen, J. Ormand, B.Kropscott, J. Hammond, and F. Lee. Expert
analytical support was provided byD. McNett, D. Markham, and K.
Engle. We are also grateful for the veterinaryexpertise of J.
Lacher. Financial support was provided by The MonoethyleneGlycol
Sector Group of CEFIC, and the Ethylene Glycol Panel of TheAmerican
Chemistry Council.
REFERENCES
Carney, E. W. (1994). An integrated perspective on the
developmental toxicityof ethylene glycol. Reprod. Toxicol. 8,
99113.
Carney, E. W., Freshour, N. L., Dittenber, D. L., and Dryzga M.
D. (1999).Ethylene glycol developmental toxicity: Unraveling the
roles of glycolicacid and metabolic acidosis. Toxicol. Sci. 50,
117126.
Carney, E. W., Liberacki, A. B., Bartels, M. J., and Breslin, W.
J. (1996).Identication of proximate toxicant for ethylene glycol
developmental tox-
icity using rat whole embryo culture. Teratology 53,
3846.Carney, E. W., Pottenger, L. H., Bartels, M. J., Jaeckh, R.,
and Quast, J. F
(1998). Comparative pharmacokinetics and metabolism of ethylene
glycol inpregnant rats and rabbits. Toxicol. Lett . 95 (Suppl. 1),
P4C27.
EPA-TSCA (1989). US Environmental Protection Agency-TSCA GLPS.
Title40 CFR, Part 792-Toxic Substances Control Act (TSCA); Good
LaboratoryPractice Standards, Final Rule.
Frantz, S. W., Beskitt, J. L, Grosse, C. M., Tallant, M. J.,
Dietz, F. K., andBallantyne, B. (1996a). Pharmacokinetics of
ethylene glycol. I. Plasmadisposition after single intravenous,
peroral, or percutaneous doses in femaleSprague-Dawley rats and
CD-1 mice. Drug Metab. Dispos . 24, 911921.
Frantz, S. W., Beskitt, J. L., Grosse, C. M., Tallant, M. J.,
Dietz, F. K., andBallantyne B. (1996b). Pharmacokinetics of
ethylene glycol. II. Tissuedistribution, dose-dependent
elimination, and identication of urinary me-tabolites following
single intravenous, peroral or percutaneous doses in thefemale
Sprague-Dawley rat and CD-1 mouse. Xenobiotica 26, 11951220.
Frantz, S. W., Beskitt, J. L., Grosse, C. M., Tallant, M. J.,
Zourelias, L. A., andBallantyne, B. (1996c). Pharmacokinetics of
ethylene glycol. III. Plasmadisposition and metabolic fate after
single increasing intravenous, peroral orpercutaneous doses in male
Sprague-Dawley rats. Xenobiotica 26, 515539.
Gibaldi, M., and Perrier, D. (1982). Pharmacokinetics , 2nd ed.
Marcel Dekker,Inc., New York.
Hoffman, G., Aramaki, S., Blum-Hoffman, E., and Sweetman, L.
(1989).Quantitative analysis for organic acids in biological
samples: Batch isolationfollowed by gas chromatographic-mass
spectrometric analysis. Clin. Chem.35, 587595.
Jacobsen, D., and McMartin, K. E. (1986). Methanol and ethylene
glycolpoisonings: Mechanism of toxicity, clinical course, diagnosis
and treatment. Med. Toxicol . 1, 309334.
Jacobsen, D., Ovrebo, S., Ostborg, J., and Serjersted, O. M.
(1984). Glycolatecauses the acidosis in ethylene glycol poisoning
and is effectively removedby hemodialysis. Acta. Med. Scand. 216,
409416.
Jolivet, P., Gans, P., and Triantophylides, C. (1985).
Determination of glycolicacid level in higher plants during
photorespiration by stable isotope dilutionmass spectrometry with
double-labelling experiments. Anal. Biochem. 147,8691.
Khera, K. S. (1991). Chemically induced alterations in maternal
homeostasisand histology of conceptus: Their etiologic signicance
in rat fetal anoma-lies. Teratology 44, 259297.
Klug, S., and Jaeckh, R. (1999). Effects of ethylene glycol and
metabolites onin vitro development of rat embryos during
organogenesis. German Soc.Toxicol .
Marshall, T. C. (1982). Dose-dependent disposition of ethylene
glycol in therat after intravenous administration. J. Toxicol.
Environ. Health . 10, 397409.
Miller, R. K. (1983). Perinatal toxicology: Its recognition and
fundamentals. In Reproductive Toxicology (D. R. Mattison, Ed.), pp.
205244. Alan R. Liss,Inc., New York.
Munley, S. M., Kennedy, G. L., and Hurtt, M. E. (1999).
Developmentaltoxicity study of glycolic acid in rats. Drug Chem.
Toxicol . 22, 569582.
Neeper-Bradley, T. L., Tyl, R. W., Fisher, L. C., Kubena, M. F.,
Vrbanic,M. A., and Losco, P. E. (1995). Determination of a
no-observed-effect-levelfor developmental toxicity of ethylene
glycol administered by gavage to CDrats and CD-1 mice. Fundam.
Appl. Toxicol . 27, 121130.
OECD (1982). Organisation for Economic Co-Operation and
Development-Principles of Good Laboratory Practice, The OECD
Principles for GLP asspecied by the European Economic Community,
Council Directive 87/18EEC.
Poore, R. E., Hurst, C. H., Assimos, D. G., and Holmes, R. P.
(1997). Pathwaysof hepatic oxalate synthesis and their regulation.
Am. J. Physiol . 272,C289294.
Price, C. J., Kimmel, C. A., Tyl, R. W., and Marr, M. C. (1985).
Thedevelopmental toxicity of ethylene glycol in rats and mice.
Toxicol. Appl.Pharmacol . 81, 113127.
Ribaya-Mercado, J. D., and Gershoff, S. M. (1984). Effects of
sugars andvitamin B-6 deciency on oxalate synthesis in rats. J.
Nutr. 114, 14471453.
Tanaka, K., West-Dull, A., Hine., D. G., Lynn, T. B., and Lowe,
T. (1980).Gas-chromatographic method of analysis for urinary
organic acids. II.Description of the procedure, and its application
to diagnosis of patients withorganic acidurias. Clin. Chem. 26,
18471853.
Tyl, R. W., Price, C. J., Marr, M. C., Myers, C. B., Seely, J.
C., Heindel, J. J.,and Schwetz, B. A. (1993). Developmental
toxicity evaluation of ethyleneglycol by gavage in New Zealand
White rabbits. Fundam. Appl. Toxicol . 21,402412.
19EG METABOLISM IN PREGNANT RATS