Embed Size (px)
Citation preview

TOWARDS UNITY FOR HEALTH, APRIL 2000 ■ 1
COORDINATING CHANGES IN HEALTH SERVICES AND
HEALTH PROFESSIONS PRACTICE AND EDUCATION
TowardsUnity forHealth
Dr Charles Boelen
New scope, new hopesCharles Boelen, World Health Organization, Geneva
From this issue on, the WHO newsletter Changing Medical Educationand Medical Practice will be called Towards Unity for Health. The
subtitle of the transformed newsletter, “Coordinating changes in healthservices and health professions practice and education”, is intended toshow that while there is continuing interest in the areas covered by its
predecessor, its scope has now been enlargedto deal with health system-wide concerns andapproaches.
More and more leaders in education, researchand services in the health sector realize that to en-sure sustainable achievement in their work, it isequally important to excel in a specific area of ex-pertise and to be able to relate to the wider con-text of health and development. This meansunderstanding that to create mutually reinforcinglinks with other areas and partners is not only in-tellectually rewarding but strategically importantfor support, expansion and impact.
This issue is transitional: most of the articles refer to health professionspractice and education issues,while only a few relate to thenew focus. We who produce thenewsletter anticipate thatfuture issues will more fullyreflect and contribute to an un-derstanding of the challengesof implementing unifyingapproaches in health servicesdelivery. Please read the column“Towards Unity for Health” on
continued page 2 ➤
No 1 • APRIL 2000WHO/EIP/OSD/NL/A/2000.1
2 Towards unity for health2 Rapid changes ahead4 Towards unity for action: in the field5 Partenariat pour la santé en Afrique
francophone7 Decentralized health information
management: the glue of a TUFHproject?
9 The community-oriented primarycare (COPC) approach and TowardsUnity For Health
11 Towards unity for health in medicaleducation
12 A snapshot from Canada13 Towards Unity for Health Project14 Towards Unity for Health: The Phuket
Consensus14 Towards Unity for Health: collabora-
tion wanted15 Project UNI-SOL: collaboration
wanted17 Working with the WHO17 Diarydates18 IMCI: A challenge for both health
professionals and teaching institu-tions
20 The WHO Reproductive HealthLibrary: a tool to incorporateevidence-based reproductive healthinto medical education and practice
21 Health personnel – a countrypriority: a viewpoint from Botswana
22 A five-star doctor for Africa:desirability and feasibility
23 Essential service package inBangladesh needs five-star doctors
24 Family practice and health systemevolution
26 Health care reforms in the Philip-pines
28 The contribution of the family doctor29 Seeking new ways to employ GPs:
Can an oil-spots strategy succeed?30 Lessons learnt at WHO by a prospec-
tive US family physician33 Are Sri Lankan medical schools
socially accountable?34 Global issues for medical educators35 Quality assurance and accreditation:
Where do they meet?36 Credentialing for the health profes-
sions38 A student’s view on social issues in
medical education38 Addresses
2 ■ TOWARDS UNITY FOR HEALTH, APRIL 2000
MOVING TOWARDS UNITY FOR HEALTH
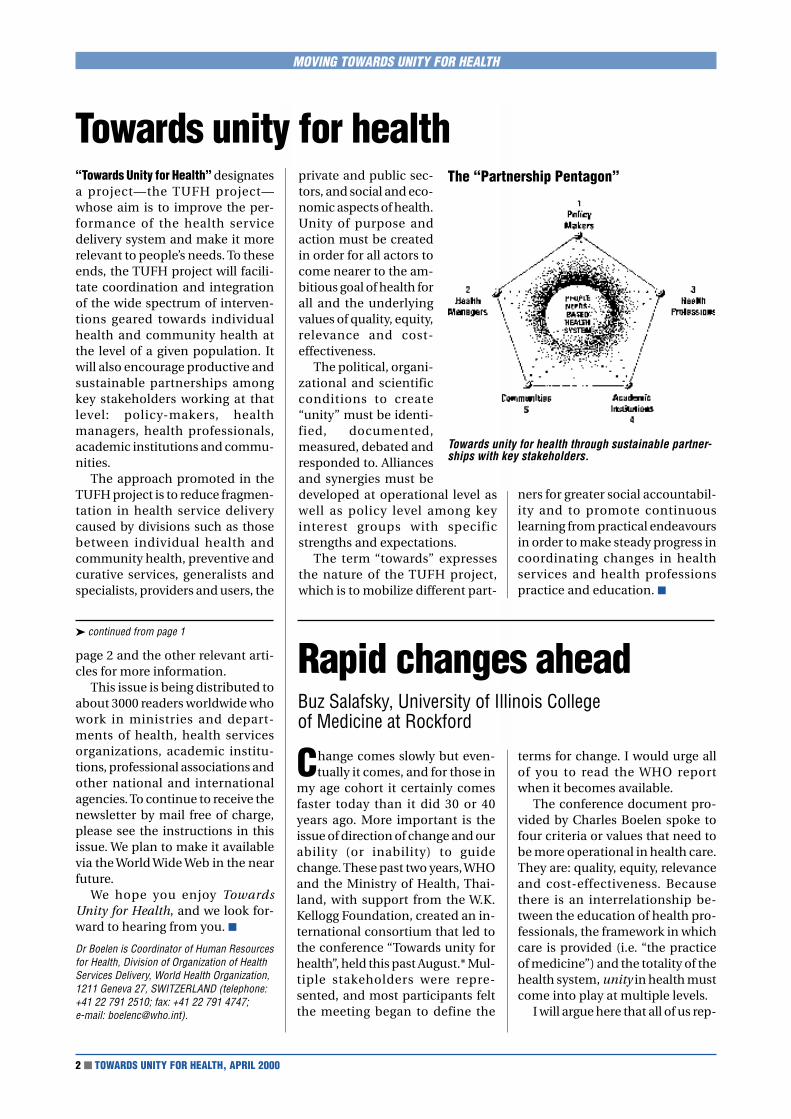
“Towards Unity for Health” designatesa project—the TUFH project—whose aim is to improve the per-formance of the health servicedelivery system and make it morerelevant to people’s needs. To theseends, the TUFH project will facili-tate coordination and integrationof the wide spectrum of interven-tions geared towards individualhealth and community health atthe level of a given population. Itwill also encourage productive andsustainable partnerships amongkey stakeholders working at thatlevel: policy-makers, healthmanagers, health professionals,academic institutions and commu-nities.
The approach promoted in theTUFH project is to reduce fragmen-tation in health service deliverycaused by divisions such as thosebetween individual health andcommunity health, preventive andcurative services, generalists andspecialists, providers and users, the
private and public sec-tors, and social and eco-nomic aspects of health.Unity of purpose andaction must be createdin order for all actors tocome nearer to the am-bitious goal of health forall and the underlyingvalues of quality, equity,relevance and cost-effectiveness.
The political, organi-zational and scientificconditions to create“unity” must be identi-fied, documented,measured, debated andresponded to. Alliancesand synergies must bedeveloped at operational level aswell as policy level among keyinterest groups with specificstrengths and expectations.
The term “towards” expressesthe nature of the TUFH project,which is to mobilize different part-
Towards unity for health
➤ continued from page 1
The “Partnership Pentagon”
Towards unity for health through sustainable partner-ships with key stakeholders.
ners for greater social accountabil-ity and to promote continuouslearning from practical endeavoursin order to make steady progress incoordinating changes in healthservices and health professionspractice and education. ■
page 2 and the other relevant arti-cles for more information.
This issue is being distributed toabout 3000 readers worldwide whowork in ministries and depart-ments of health, health servicesorganizations, academic institu-tions, professional associations andother national and internationalagencies. To continue to receive thenewsletter by mail free of charge,please see the instructions in thisissue. We plan to make it availablevia the World Wide Web in the nearfuture.
We hope you enjoy TowardsUnity for Health, and we look for-ward to hearing from you. ■
Dr Boelen is Coordinator of Human Resourcesfor Health, Division of Organization of HealthServices Delivery, World Health Organization,1211 Geneva 27, SWITZERLAND (telephone:+41 22 791 2510; fax: +41 22 791 4747;e-mail: [email protected]).
Rapid changes aheadBuz Salafsky, University of Illinois Collegeof Medicine at Rockford
Change comes slowly but even-tually it comes, and for those in
my age cohort it certainly comesfaster today than it did 30 or 40years ago. More important is theissue of direction of change and ourability (or inability) to guidechange. These past two years, WHOand the Ministry of Health, Thai-land, with support from the W.K.Kellogg Foundation, created an in-ternational consortium that led tothe conference “Towards unity forhealth”, held this past August.* Mul-tiple stakeholders were repre-sented, and most participants feltthe meeting began to define the
terms for change. I would urge allof you to read the WHO reportwhen it becomes available.
The conference document pro-vided by Charles Boelen spoke tofour criteria or values that need tobe more operational in health care.They are: quality, equity, relevanceand cost-effectiveness. Becausethere is an interrelationship be-tween the education of health pro-fessionals, the framework in whichcare is provided (i.e. “the practiceof medicine”) and the totality of thehealth system, unity in health mustcome into play at multiple levels.
I will argue here that all of us rep-

TOWARDS UNITY FOR HEALTH, APRIL 2000 ■ 3
MOVING TOWARDS UNITY FOR HEALTH
national budgets, as chronic dis-ease among an unaware or unre-sponsive public would otherwiseconsume available resources.
Responding to challengesTo deal with these forces we willneed to develop what JordanCohen, MD, President of the Asso-ciation of American Medical Col-leges, describes as a collaborativecare model for health care delivery.Its philosophy is analogous tounity for health, but with particu-lar relevance to the USA. Eventually,worldwide practitioners of healthcare will need to operate under thistype of system.
To define how this will bebrought about, medical schools,teaching hospitals, ministries ofhealth, professional organizationsand—most important, communi-ties—will need to come together todesign country-appropriate mod-els of health care and health edu-cation that adhere to the moretime-honoured principles andvalues of what is best in medicine.Our collective inability to bring thisoff will result in squanderedresources, non-articulated healthdelivery systems, narrowly focusedpractitioners and an unserved,possibly increasingly frustrated andangry public. In some places gov-ernment directives will dictatedirection, and possibly that hasalready happened.
What therefore is our role? Ibelieve that those who espouseunity for health now need to beginto create multi-stakeholder dia-logues in their regions. Pilotprojects at grassroots level need tobe defined and funded. We need toreach out to local, regional andnational governmental agenciesand NGOs alike. Private sectorresources need to be harnessed. Allof us need to become catalystsguiding change. Our roles would in-clude:
● soliciting interested constituents
● facilitating communication
● helping parties develop agendasfor change and meaningful tem-plates
● brokering alliances
● and above all, being advocates.
These are common pathways inall our cultures. The map for unityneeds to be in front of all of us. Allof us need to be players. ■
* WHO international conference “Towardsunity for health: challenges and opportu-nities for partnership in health develop-ment”, 10–13 August 1999, Phuket,Thailand.
Dr Salafsky is Dean, University of IllinoisCollege of Medicine at Rockford, 1601Parkview Avenue, Rockford, Illinois 61107-1897, USA (telephone: +815 395 5600,fax: +815 395 5887, e-mail: [email protected]).
resenting the six billion (and thenumber is still growing) individu-als on this planet will sooner or laterbe swept up in a series of changes—changes that I believe must criti-cally include the concept of unityfor health. Given the demographicsof humanity in the 21st century, thischange is unavoidable. The ques-tion each of us needs to answer is:Will we be helping to guide thischange relative to health, or not?
Global challengesFirst, let me spell out some of thereasons why multiple stakeholdersneed to come together to create abetter unity:
● Globalization is pervasive. It willhave an impact on medicine in gen-eral, and specifically in terms of thedifferences in the way we educateproviders, the way medicine ispractised and health care is deliv-ered. All these systems will increas-ingly come under scrutiny.
For example, we note that min-istries of health and/or education,international NGOs and WHO arebeginning to look at educationalstandards relative to the accredita-tion of medical schools. Until now,such standards existed in relativelyfew countries.
In terms of the practice of medi-cine, we increasingly note thatHMO-like systems have alreadybegun in a few short years to spreadglobally. HMO entities by their verynature will increasingly call forpractice guidelines, standards ofquality in medicine and uniformityin providing optimal care that iscost-effective.
● As mass communication contin-ues unabated, there is a greaterawareness of the wide disparities inhealth status as a function of race,ethnicity and socioeconomics.Advances in technology and post-genomic therapies will onlyheighten these disparities that willbe broadly perceived by globalpopulations.
● Health promotion will increas-ingly become a centre point in
Interested in accreditation?The issue of accreditation is being raised worldwide by governmental authori-ties, health service organizations, the health professions and academicinstitutions. Often heard are questions such as: “Are we good enough?” “Arewe as good as our neighbours?” “Are there any international norms?” “Is therean international accrediting body?”
Accreditation as a means to permit an institution or organization to functionand deliver certain goods in reference to a set of values is being increasinglyseen as a powerful lever for change.
The international implications of accreditation are important in the wake ofglobalization. Within the scope of accreditation, components relative to thecapacity to respond to people’s health needs from the perspective of improvedquality, equity, relevance and cost-effectiveness in health are of particularconcern to WHO. Look for more information in the next issue of the TUFHnewsletter. ■

4 ■ TOWARDS UNITY FOR HEALTH, APRIL 2000
MOVING TOWARDS UNITY FOR HEALTH
Dr Vic Neufeld
Towards unity for action: in the fieldVictor Neufeld, Hamilton, Ontario
1. Define the right problemThe great American educator JohnDewey once said: “A problem welldefined is half solved”. All the casestudies illustrate this idea, andthey represent a rich variety of ap-proaches, even though all of themshare an ultimate goal: to enhancethe health and well-being of a par-ticular population.
Some examples of defining theright problem include:
● the Liverpool story, where clearneeds were articulated by com-munity groups, and where aresponse was mobilized to ad-dress these needs;
● the Australia story, where theproblem was that initiallydoctors did not understand thesocial and environmental deter-minants of health;
● the Botswana story, in which,faced with a special need to lookafter persons with HIV/AIDS, thechallenge was to find a homecare solution that matched theavailable resources.
2. The lesson of context specificity(or “no easy models”)
It was clear, from listening to the sixstories, that each situation wasquite distinctive. In Baranquilla,Colombia, for example, there was acommunity with a special problem.In response to this problem, localleaders seized the opportunity ofthe resources made availablethrough the UNI project. In addi-tion, there was a favorable politicalclimate to support this initiative. Inthe Liverpool example, the modelthat emerged was one of progres-sive involvement of partners. Ini-tially, only two or three partnerorganizations were in the coalition;none of them were academic insti-tutions, which were added later.
The lesson here is that we must
not be too hasty and glib in “push-ing” models and approaches thatare right for one setting but may beinappropriate in another context.
3 Continuity and persistence: theimportance of the long term
Those of us involved in develop-ment work understand this lesson,where much too often we have seenprojects with artificially shorttimelines, dictated not by thenature of the project but by the re-quirements of the funding arrange-ments. Several of the case studiesillustrate the importance of long-term commitment and persistence.For example, the Australia casestudy summarized 30 years of ex-perience of a group working withan Aboriginal community. Thestory from Vellore, India, wheresome very important learning wasaccumulated over several decades,shows us the importance of con-tinuous institutional commitment.
4. New roles for academicinstitutions
Both the Australia and the Indiacase studies illustrate this lesson. InIndia, for example, the ChristianMedical College, Vellore, combineseducation and research with a clearand central commitment to com-munity service. In the Australia casestudy, the university played a keyrole in documenting actions andinputs, thus providing an institu-tional-memory base over time. This included documenting thetwo-way learning that occurredbetween academe and the commu-nity, including an account of themid-course corrections that weremade. This project also producedand disseminated an impressive setof publications over a 30-yearperiod.
A WHO international conference,“Towards Unity for Health: challengesand opportunities for partnership inhealth development”, took place inAugust 1999 in Phuket, Thailand.Some 200 delegates from 45 coun-tries participated, representing publichealth authorities, professionalassociations, academic institutionsand communities. Twenty casestudies among the 52 submitted wereselected to illustrate endeavours tocreate unity in health and werepresented in plenary sessions, groupdiscussions or as posters. Thefollowing article is an analysis byDr Vic Neufeld of the six case studiesdiscussed in groups. A monographwill be published by WHO thisautumn with a selection of fullydeveloped case studies.
Participants at the Phuket con-ference discussed six case stud-
ies in breakout groups. In eachgroup, rapporteurs were asked toprepare summaries of the discus-sions under three headings: specialfeatures, main challenges and spe-cific suggestions. The synthesisbelow is based, to a large extent, onthe excellent work of theserapporteurs.
Seven key messages can be iden-tified from the case study discus-sions.

TOWARDS UNITY FOR HEALTH, APRIL 2000 ■ 5
MOVING TOWARDS UNITY FOR HEALTH
Partenariat pour la santé enAfrique francophoneAyité M. D’Almeida, former Director of Programme Management of theWHO Regional Office for Africa
5. The need to develop newcapacities
As part of the response to variouskinds of community needs, severalof the case study accounts includeda description of new capacities thatwere developed. Examples includethe “skill” of team-building andcollaboration (particularly inter-sectoral collaboration); capacitiesrelated to the appropriate use of in-formation and communicationtechnologies; and the capacities in-volved in leadership developmentand succession planning. Two ofthe case studies also described howthe groups involved learned how to“go to scale” from initial pilotprojects. These were the Botswanastory, where a small-scale homecare project for HIV/AIDS patientsevolved to a similar system that wasapplied to other problems. In SouthAfrica, a pilot project focused on tu-berculosis was later expanded to in-clude other conditions.
6. Combining action and learningAll the cases illustrated this impor-tant lesson. In one way or another,all the case study reports involvethe documentation of lessonslearnt and the importance of set-ting up a system for combining ac-tion with periodic reflection. Insome cases, for example in theVellore story, the documentationand subsequent learning includedthe identification and use of basicperformance measures, in the formof community health indicators. Itwas also interesting to see, in sev-eral of the case studies, that thelearning occurred at several levels:individual, team and organization.
7. Building a global knowledgebase
The case studies illustrate the im-portance of developing a localknowledge base related to a projectand disseminating this experiencelocally. In Colombia, for example,
the project experience was welldocumented and disseminated topoliticians, to the public and topolicy-makers. The Liverpoolproject included the preparation ofattractive materials, disseminatedin large part through the WHO.
Now with the TUFH project, wehave some important contribu-tions to the global knowledge base,provided by case studies frommany parts of the world. Let us dis-seminate these important contri-butions using a variety of existingnetworks and coalitions, such asthe “Healthy Cities” movement, theNetwork of Community-OrientedEducational Institutions for HealthSciences, the Council on HealthResearch for Development, and ofcourse, the WHO network. ■
Dr Neufeld can be contacted at 70 ChedokeAvenue, Hamilton, Ontario, CANADA L8P 4N9(telephone: +1 905 526 8761; fax: +1 905 5269365; e-mail: [email protected]).
SummaryThe author describes the WHOinternational conference “TowardsUnity for Health” (Thailand, 1999) asa historic landmark for the implemen-tation of the health-for-all strategy.The “Towards Unity for Health”approach focuses on reference valuesand suggests organizational patternsof health service delivery as well asconditions for productive and sustain-able partnership. As such, it isrelevant to the African context ofhealth system development, promot-ing innovative ways to generate newalliances between key stakeholdersthat are very much needed to revamphealth development in Africa.
Introduction
L a conférence internationaleorganisée par l’OMS à Phuket
(Thaïlande) du 10 au 13 août 1999,vient de poser un jalon historiquevers la réalisation de l’objectif de lasanté pour tous et pour chacun.
Ses travaux ont concerné unepréoccupation partagée par toutela communauté des hommes etfemmes de santé publique: la con-vergence des énergies et des res-sources en faveur de la santé. Laconférence suggère une approcheoriginale et intégratrice qui reposesur trois piliers complémentaires:
● des valeurs de référence pourinspirer la planification
● des stratégies organisationnellescensées guider les interventions
● un appel au partenariat où lesressources humaines et institu-tionnelles se voient affecter desrôles et des responsabilités nou-velles.
Elle fait, par ailleurs, siennes lesorientations prônées par lesgrandes approches conceptuelles,stratégiques et opérationnelles depromotion de la santé dans lemonde.
Le contexteComplexité croissante, interdépen-dance et interaction dominent tousles secteurs de l’activité humaine

6 ■ TOWARDS UNITY FOR HEALTH, APRIL 2000
contemporaine. Etablie désormaiscomme l’un les déterminantsessentiels du développement hu-main, la santé partage les mêmescaractéristiques. De plus, en raisonde sa nature et de ses cibles, elle estplus que jamais soumise aus effetsdes autres secteurs dont les turbu-lences l’affectent grandement.
Les nombreux acquis, enregis-trés notamment au cours des cinqdernières décennies, sont manifes-tes mais inégalement partagés. Lesphilosophies, les approches etstratégies mises on oeuvre n’ontpas produit les effets durablesescomptés.
En effet, les Services de Santé deBase, les Soins de Santé Primaireset l’Initiative de Bamako furentutiles, mais jamais déterminantspour assurer l’accès universel à dessoins et services de santé de qua-lité. Plus récemment, les efforts etsacrifices consentis en vue de la ré-forme des secteurs nationaux desanté ne semblent pas non plusconcluants. Les inégalités parais-sent même s’être approfondiesdans certaines régions du globe, surle continent africain en particulier.
La caractéristique principale deces approches semble de ne consi-dérer que certaines composantesdu système de santé ou de sa ges-tion. Elle paraissent également enavoir privilégié les dimensionstechnique, technologique et parfoissociale. Les préoccupations pour
les aspects éthiques et moraux sontplus récentes, sans que celles-ciconstituent les sources d’inspira-tion pour l’action de santé publiqueet individuelle.
Pour l’unité en faveur de la santéL’originalité de la présente initiativeest de suggérer une vision holi-stique et un cadre de référence à lafois conceptuel et stratégique quiintègre cette triple exigence. Saconceptualisation se fonde surl’identification de quatre valeurscomplémentaires et, à bien deségards, fondamentales en matièrede santé:
● l’équité, valeur éthique
● la qualité, valeur technique
● la pertinence, valeur sociale
● le cout-efficacité, valeur gestion-naire.
Dans le contexte africain, la so-lidarité—valeur culturelle et opéra-tionnelle—devrait compléter lesexigences énoncées ci-dessus.
Les relations établies entre cesvaleurs présentent deux avantages:
● servir de référence pour détermi-ner l’écart entre la situation d’unsystème de santé donné au re-gard de son adhérence aux ditesvaleurs. Il sera nécessaire, pouropérationnaliser chacune de cesdernières, d’en identifier les in-dicateurs;
● mesurer les progrès réalisés dansla mise en oeuvre des initiativesvisant à répondre aux exigencesde couverture universelle ensoins de qualité.
La stratégie énoncée vise à ras-sembler ce qui est épars, incohé-rent et parfois contradictoire. Elleest censée induire un environne-ment favorable à la coordination età l’intégration, pour une plusgrande convergence et une effi-cience accrue des interventions.Les conditions sine qua non du suc-cès résident en l’intégration de lasanté publique et de la médecine,ainsi qu’en la mise en place d’unsystème d’information sanitairefonctionnel qui en soutienne lesdécisions et les prestations. Cesdernières découleront des fonc-tions essentielles de promotion etde restauration de la santé, de pré-vention de la maladie et de sesséquelles, de réduction des incapa-cités. On admet aujourd’hui que lasanté publique se préoccupe ausside santé de l’individu au sein de sacommunauté ou de son grouped’appartenance.
La mise en oeuvre de ce cadrestratégique requiert une révisiondes rôles et responsabilités des res-sources humaines impliquées. Elleexigera de redéfinir les attributionsdes institutions concernées et deprocéder, en conséquence, à leurrestructuration. La réforme desprogrammes de formation et deprestation de soins sera tout aussinécessaire pour les adapter à cesnouvelles exigences.
Enfin, l’initiative appelle lagénération et la mise en place denouvelles alliances, ainsi que lerenforcement des anciens partena-riats. Elle nous semble, plus quetoutes les autres, constituer unesource d’inspiration suffisammentholistique pour guider les réformesdes systèmes de santé. ■
Dr D’Almeida is currently Director, RegionalInstitute of Public Health; Projet OMS;01 BP 918; Cotonou, BENIN (telephone: +22930 54 78; fax: +229 30 54 79;e-mail: [email protected]).
MOVING TOWARDS UNITY FOR HEALTH
Création d’un réseau “Francophonie Santé”A la suite de la conférence internationale francophone des sciences de la santé,qui s’est tenu à Moncton, Nouveau-Brunswick, Canada, au mois de juin 1999,et en marge du sommet des chefs d’états francophones qui s’est tenu enseptembre 1999 dans la même ville, le projet de la création d’un réseau“Francophonie Santé” est né.
Ce réseau a pour but d’offrir l’opportunité d’échanges d’information et d’expé-riences, ainsi que d’une collaboration internationale sur le problématique d’unemeilleure réponse des systèmes de santé aux besoins des individus et despopulations. Le partenariat entre décideurs politiques, gestionnaires de santé,professions de santé, institutions académiques et communautés sera mis enexergue. Ce réseau s’appelera tout simplement “Vers l’Unité Pour la Santé”, lecorrespondant de “Towards Unity for Health”.
Pour toute information, prière de contacter le secrétariat du réseau:C.P. 946, Moncton (N.-B.), CANADA E1C 8N8. ■

TOWARDS UNITY FOR HEALTH, APRIL 2000 ■ 7
Decentralized health informationmanagement: the glue of a TUFH project?Theo Lippeveld, John Snow, Inc./Morocco
tion system (HIS) generates the in-formation necessary for rationaldecision-making at each level of thehealth services system: the primarylevel, the secondary level and thetertiary level. Each of these levelshas specific “management” func-tions that can be grouped in threecategories:
● individual care managementfunctions, directly related to thedelivery of high-quality care toindividuals consulting the healthservices system;
● health unit management func-tions, related to the provision ofhealth care to a defined popula-tion in the catchment area sur-rounding the health unit;
● health system managementfunctions, which include, inaddition to coordination andmanagement support for deliv-ery of health services, a set ofpublic health functions for aparticular reference population.
When management functionsare clearly defined, it is relativelyeasy to identify the informationneeded to make appropriate deci-sions at each management level.
The next question is how toobtain this information in the mosteffective and efficient way. Classi-cally, two main sources of informa-tion exist: routine data systems,mainly health unit-based, andnon-routine data systems, such assurveys. No single data source canprovide all the informationrequired for planning and manage-ment of health services. A nationalhealth information system in sup-port of health services will alwaysuse a combination of data collec-tion methods, depending on thenature and use of the information
for which data need to be collected.Since both individual health careand public health interventions arecarried out within the health serv-ices system, it seems obvious thatthe main information source forintegration of both activities shouldbe the routine health informationsystem.
Yet most experts agree that rou-tine health information systems inmost countries, industrialized aswell as developing, are generatingirrelevant and low-quality informa-tion. Various explanations for thissituation have been cited in theliterature, but one is particularlydetrimental to the TUFH approach:centralization of information man-agement.
Routine health information sys-tems in most countries are centrallyplanned and managed. Indicators,data collection instruments, andreporting forms usually have beendesigned by centrally locatedepidemiologists, statisticians andadministrators (the “data people”),with minimal involvement oflower-level line managers and pro-viders of the health services (the“action people”).
Data processing and analysis aremainly the responsibility of a cen-trally located office. Complex datatransmission and compiling sys-
MOVING TOWARDS UNITY FOR HEALTH
“Towards unity for health” activitiesaim at the integration of individualhealth and public health interven-tions. The assumption is that suchactivities would contribute to thedevelopment of a coherent andcohesive health system, able toimprove the health status of indi-viduals in a population.
Health status is classicallyknown to be determined by at leastfour main groups of factors: (1) bio-logical assets; (2) personal lifestyle;(3) the environment; and (4) thehealth care system. The potentialimpact of interventions within eachof these groups can be debated, butseveral authors have stressed thatthe contribution of the health caresystem alone is only marginal com-pared to the potential impact ofinterventions on personal lifestyleand on the environment.
While health care interventionsfocus primarily on individuals,interventions on personal lifestyleand on the environment are inessence community-oriented.Clearly, individual health interven-tions and community health inter-ventions are complementary andinterdependent and need coher-ence to ensure maximum impacton health status. The question iswhere to find the glue to stick themtogether.
Information and integrationWell-conceived health informationsystems can definitely play a majorrole in facilitating the integration ofindividual health and public healthinterventions. In fact, poor use ofinformation for evidence-baseddecision-making is probably one ofthe main causes of the present lackof linkages between individual careand public health systems.
A well conceived health informa-
Dr Theo Lippeveld

8 ■ TOWARDS UNITY FOR HEALTH, APRIL 2000
tems slow down the production offeedback, so that information isfrequently obsolete for decision-making when it arrives at the lowerlevels. The result is that informationuse is found to be the weakest at thedistrict and health unit levels,where the main individual andcommunity health interventionsare planned, implemented andmonitored.
The challenge of simple, efficientand integrated data collectionIn order to transform routine healthinformation systems into manage-ment tools for integration of bothindividual health and public healthfunctions, the key strategy is to de-centralize the information systemmanagement responsibilities tothe district level (see Fig. 1). Yet thetask of developing such district-managed routine informationsystems is both formidable andcomplex, particularly in the contextof government bureaucracies indeveloping countries.
Broad participation of futureusers in the system design is re-quired, especially at critical stepssuch as the definition of informa-
tion needs and of key indicators.The challenge is to combine simple,efficient, and integrated data col-lection with the production of highquality action-oriented informa-tion. District managers need train-ing in the use of this information inorder to implement both individualcare and community interventionsin a coherent manner.
Most of all, the district level is theideal starting point for the develop-ment of community health andinformation systems. Communityhealth systems stress local partici-pation of communities in respond-ing to the health needs of thepopulation.
Thus, within the district healthsystem the community addsanother management level with itsown information needs. The com-munity itself provides informationfor the management of mostessential public health functions.Examples include reporting ofbirths and deaths; notification ofcases of infectious diseases andoutbreaks; identification of high-risk children, pregnant women, andfamilies; coverage and defaulters ofcritical services; coverage and qual-
ity of water and sanitation; moni-toring air, water, land, and noisepollution; coverage of disadvan-taged populations with health andsocial services.
Most examples of communitymanaged health information sys-tems come from research settings,for example, Matlab (Bangladesh),Aga Khan University (Pakistan) andKasongo (Zaire). Private voluntaryor nongovernmental organizationsin numerous developing countriesas well as in developed countries(Goldfield, 1996) have also adoptedthis approach.
The glueAlthough they are clearly ambitiousand long-term efforts, district-managed and at least partiallycommunity-managed HIS couldprovide the glue to bind togetherindividual and community healthinterventions. Further research andexperiences are required to expandand scale up existing projects.
First of all, a comprehensivereview study should be set up togather existing scientific evidencethat decentralized routine HIScontribute to more effective andefficient integration of individualand community health interven-tions. We also invite the researchcommunity to help answer the fol-lowing illustrative list of researchquestions:
● How can district managers, serv-ice providers and particularlycommunities—as key informa-tion users—be more activelyinvolved in HIS developmentefforts?
● How can community-managedhealth information systemsmost effectively be linked toroutine health unit-based HIS?
● What management structuresare required to better linkroutine health service statisticswith other data collectionsystems (surveys, vital eventsregistration, rapid assessmentmethods)?
MOVING TOWARDS UNITY FOR HEALTH
Figure 1. District-managed routine health unit-basedinformation systems
Districthealth
managementteam
HEALTHCARELEVEL
PRIMARY
SECONDARY
TERTIARY
GENERAL POPULATION
CATCHMENT AREA POPULATION
Patient/clientcontact
First-levelcare unit
Districthospital
Regionalhospital
Universityhospital
Regional healthmanagement
INDIVIDUALCARE
MANAGEMENT
HEALTHUNIT
MANAGEMENTSYSTEM
MANAGEMENT
HEALTH SERVICES SYSTEM
DISTRICTLEVEL
REGIONALLEVEL
NATIONALLEVEL
OTHER SECTORS:– Agriculture
– Water/sanitation– EducationNO
N-RO
UTIN
E DA
TA C
OLLE
CTIO
N M
ETHO
DS
DISTRICT POPULATION
Routine healthinformationsystem
Referredpatients
Referredpatients
Referredpatients
Ministryof Health
UniversitiesOther healthinstitutions

TOWARDS UNITY FOR HEALTH, APRIL 2000 ■ 9
● What is the ideal process andlevel for development of inter-disciplinary social informationsystems, through which inter-actions between health,education, and economic devel-opment can be identified in anaction-oriented manner?
● What is the role of informationtechnology in the developmentand implementation of districtand community-managedHIS? ■
References● Goldfield N. The hubris of healthstatus measurement: a clarificationof its role in the assessment ofmedical care. International Journalfor Quality in Health Care, 1996,8(2):115–123.
● Lippeveld T, Sauerborn R, BodartC, eds. Design and implementationof health information systems. Inpress. Geneva, World HealthOrganization, 1999.
● Marsh D. Population-basedcommunity health informationsystems. In: Lippeveld T, SauerbornR, Bodart C, eds. Design andImplementation of Health Informa-tion Systems. In press. Geneva,World Health Organization, 1999.
● Neame R, Boelen C. Informationmanagement for improving rel-evance and efficiency in the healthsector: a framework for the develop-ment of health information systems.Geneva, World Health Organization,1993 (unpublished documentWHO/HRH/95.4; available onrequest from Department ofOrganization of Health ServicesDelivery, World Health Organiza-tion, 1211 Geneva 27, Switzerland).
● Information support for newpublic health action at the districtlevel. Report of a WHO ExpertCommittee. Geneva, World HealthOrganization, 1994 (WHO TechnicalReport Series, No. 845).
Dr Lippeveld is Director, John Snow, Inc./Morocco, and can be reached c/o John SnowInternational, 44 Farnsworth Street, Boston,Massachusetts 02210, USA (e-mail:[email protected]; [email protected]).
MOVING TOWARDS UNITY FOR HEALTH
The community-orientedprimary care (COPC)approach and Towards UnityFor Health: unity of actionand purposeJaime Gofin, Hebrew University, Jerusalem
T he practice of community-oriented primary care (COPC)
integrates clinical medicine withpublic health at the communitylevel and is directed to theepidemiologically defined healthneeds of the population undercare.(1) The COPC approach wasinitiated in a rural area of SouthAfrica in the 1940s and since the 50swas further developed by SidneyKark and his team in a neigh-borhood of Jerusalem, Israel.(2)The principles of COPC are embod-ied in the Alma Ata Declaration (3–4), and the ongoing application ofCOPC in various countries (5)creates a rich experience attestingto the feasibility of this approach.
In the COPC approach, the localhealth service decides on one ormore health priority conditions,carries out a detailed communitydiagnosis, formulates and imple-ments an appropriate interventionprogramme and evaluates the im-pact of the programme. Thus, thedevelopment of a COPC practice isbased on a cyclical process in whichprogramme activities are continu-ously fed and influenced by epide-miological information.(6)
Our purpose in this paper is tobriefly illustrate this approachaccording to specific elements thathave been formulated by theTowards Unity for Health (TUFH)project.
Population and territorialityIn the COPC approach, health careis provided to all members of the
defined population (not only theusers or the ill) and therefore theservice is required to know the“name and address” of each mem-ber of the population, to identifythe target population and to usedenominator data for the requiredpopulation’s measurements. Whileservices might be provided for allage groups, specific programmesmight address subsegments of thepopulation according to theprioritized health problem (e.g.child immunization) or age-relatedhealth risks (e.g. smoking amongadolescents, physical functioningin the elderly).
Range of servicesThe COPC approach considers allstages of the natural history ofselected conditions and thereforethe aims and activities of the healthprogrammes are to integrate cura-tive, promotive, preventive andrehabilitative care at the clinical sitetogether with an active outreachapproach.
Dr Jaime Gofin

10 ■ TOWARDS UNITY FOR HEALTH, APRIL 2000
LinkageThe same health team implementsthe activities directed to individualclinical primary care and tocommunity health programmesdirected at individuals (e.g. pro-moting physical activity) and thecommunity (e.g. organizing groupsfor physical exercises at a localfacility).
Availability of informationThe recording of the communityprogramme activities and the indi-vidual health status data are anintegral part of the same clinicalfile, and should be easy to retrievefor monitoring purposes. The teamperiodically reviews data about in-dividuals and the community.
Use by allSelected information gathered aspart of clinical care and related tothe community health status isshared with community membersand leaders and with other healthagencies operating in the area.
Health professionals and theirnew rolesWhenever possible, the healthworkers involved in COPC practiceshave public health training (in ad-dition to their basic training),which allows them to perform theintegrated individual-based andpopulation-based care. This train-ing facilitates the complex (buteffective!) complementarity ofclinical and epidemiological skillsrequired by this type of approach.A multidisciplinary team is essen-tial for COPC.
Social accountability ofeducational institutionsThe COPC programme in Jerusa-lem was initiated as part of an ex-tension of services provided by auniversity teaching hospital, andvery soon became integrated intothe the university. As in many othersites where COPC is practised,teaching to health science studentsis based on the work done at thepractice, and therefore is related to
policy-making and the establish-ment of an Iron SupplementationProgramme at national level by theMinistry of Health and an EarlyStimulation Programme in thePublic Health Services of the Mu-nicipality in Jerusalem. In addition,the largest Sick Fund in Israeladapted the Hypertension ControlProgramme in half of the commu-nity clinics in the country.
Usually the professionals in-volved in the COPC approach arealso involved in research and teach-ing activities, which in itself pro-motes the dissemination of theconcepts and experiences withinthe scientific and clinical commu-nities.(11)
COPC is a care delivery approachat the community level that couldinitiate and facilitate a cascadeeffect and lead other stakeholdersto integrate their policy and actionsin the “country-wide” approach ofTUFH. This in itself would facilitatethe desired unified approach ofpractice and education. TUFHcould/should learn and grow (frompurpose to action!) from experi-ences of various approaches, likeCOPC, which have already beenevaluated and proven their feasibil-ity of integrating individual careand community medicine with im-provement of the health status ofthe population. ■
References1. Last JM, ed. A dictionary of
epidemiology (IEA), 3rd ed. NewYork, Oxford University Press,1995.
the health prioritiesidentified in the par-ticular population.
EducationalprogrammesThe “dialogue”between the healthservices and thechallenging aca-demic involve-ment havecreated a richenvironment for continuouscritical analysis and renewedproposals for changes and im-provements at the service level.
Principal partnersAlthough care is provided by thehealth service, there are differentlevels of coordination with otherlocal agencies (community centres,schools and social welfare).
Community involvementThroughout the years we haveobserved various expressions ofcommunity involvement. At the be-ginning of this type of delivery ofcare in Jerusalem, both the healthservice and the community weregoing through the stages of devel-oping a new type of health care andof finding answers to the commu-nity’s basic needs. During thatperiod there was an intensive in-volvement of the community in theservice affairs. Later on, witheconomic and social progress,community members changed to amore passive attitude of “tell uswhat to do”. The type of linksbetween health services and thecommunity relates to the particu-lar cultural and social values pre-vailing in each population.
DisseminationThere is an extensive literature onthe planning, implementation andevaluation of COPC programmesdeveloped in different countries (3,7–10) that illustrates their impacton the populations’ state of health.In Israel, the outcome of theseevaluations has been the basis for
MOVING TOWARDS UNITY FOR HEALTH
TOWARDS UNITY FOR HEALTH, APRIL 2000 ■ 11
2. Kark SL. The practice of commu-nity-oriented primary care. NewYork Appleton-Century-Crofts,1981.
3. Susser M. Pioneering commu-nity oriented primary care.Bulletin of the World HealthOrganization, 1999, 77(5):436–438.
4. Ashton J. Public health andprimary care: towards a com-mon agenda. Public Health,1990, 104:387–398.
5. Abramson JH. Community-oriented primary care: strategy,approaches and practice—areview. Public Health Review,1988, 16:35–98.
6. Abramson JH. Application ofepidemiology in community-oriented primary care. PublicHealth Reports, 1984, 99:437–442.
7. Rhyne R et al., eds. Community-oriented primary care: healthcare for the 21st century. Wash-ington, DC, American PublicHealth Association, 1998.
8. Gillam J, Miller R. COPC: apublic health experiment inprimary care. London, King’sFund, 1997.
9. Kark SL et al., eds. Atencionprimaria orientada a lacomunidad. [Community-oriented primary care.] Barce-lona, Ediciones DOYMA, 1994.
10. Epstein L. The planning anddelivery of primary health care:Can it be adapted the needs ofthe community? Annual Pro-ceedings of InternationalMedical Association Bulgaria,1998, 4:7–13.
11. Gofin J, Gofin R, Knishkowy B.Evaluation of a community-oriented primary care workshopfor family medicine residents inJerusalem. Family Medicine,1995, 27:28–34.
Dr Gofin is Director, Community OrientedPrimary Care Teaching Programs; Departmentof Social Medicine; Hadassah School ofPublic Health and Community Medicine;Hebrew University; P.O.B. 12272; Jerusalem91120, ISRAEL (telephone: +972 2 6777119;fax: +972 2 6431086; e-mail:[email protected]).
MOVING TOWARDS UNITY FOR HEALTH
Towards unity for healthin medical educationZamboanga Medical School Foundation –a case study in the PhilippinesFortunato L. Cristobal, Zamboanga MedicalSchool Foundation, Inc.
The call for health for all articulatedin the Alma-Ata Charter is a formida-ble goal with great potential for“unity for health”. But 20 years afterthe charter’s inception, the need forinnovative reforms in medicaleducation is still great. Althoughmedical schools have been highlycriticized as isolated ivory towers,lacking in proactive contributions tosociety’s health needs, academicinstitutions actually have largepotential for addressing the complexissues of health unity and therefore tocreate synergies between the com-munity, health professionals, healthmanagers and policy-makers towardsunity for health. Here we report theexperience of stakeholders collabo-rating to establish an innovativemedical school in the southernPhilippines.
Health in our region
Nearly one-third of the Philip-pines’ 72 million people live on
Mindanao Island. Zamboanga City(population 0.5 million) is the hubfor services in Western Mindanaoand the Sulu Archipelago (popula-tion 3.5 million), one of the mostunderserved areas of the southernPacific. Travel is predominantly byboat, and access to inland areas ismostly by foot. Some 70% of thepeople live along the shorelines ofthe islands; 80% of this rural popu-lation has no health services.
Neonatal tetanus, measles,typhoid, cholera, dengue fever,tuberculosis, malaria, diarrhoeaand respiratory infections aremajor problems. The fertility rate isabout 5, and infant mortality is
more than75 per 1000births. Safewater, bal-anced nutri-tion, prenatalcare and fullimmunization remain long-termhealth goals. There are 29 medicalschools in the Philippines, butuntil recently none in this region,and few physicians are willing tomove to this under-resourced area.
Planning a medical school inpartnershipAgainst this background and awareof the challenge of starting a newmedical school with very limitedresources, community leaders,health professionals and academicstakeholders initiated consulta-tions in 1992. As a result of theseintensive intersectoral meetings, anew, private, not-for-profit medicalschool was proposed as a collabo-rative effort.
A local university was to sharethe use of teaching facilities, library,buildings and other infrastructureresources free of charge. Local doc-tors would serve as volunteer fac-ulty. The community would assistin setting priority curriculum areasand in student selection, andprovide support and protection tostudents during their community-based experiential learning place-ments. Local business peoplewould provide fund-raising sup-port. The local health system wouldprovide financial assistance forcommunity health research.
A board of 15 members, com-

12 ■ TOWARDS UNITY FOR HEALTH, APRIL 2000
posed of three academicians, fivecivic leaders and seven doctors, wasestablished to oversee its govern-ance. The Zamboanga MedicalSchool Foundation (ZMSF) wasborn in 1994.
The vision and mission were es-tablished by the dean and board oftrustees at the beginning:
The Vision: The ZMSF envisionsthat the medical school willpioneer and implement acurriculum that combines com-petence and problem-basedinstruction with experientiallearning in the community thatis responsive to the changingpatterns of health care develop-ment and the needs of thesecommunities and is sensitive tothe social and cultural realities ofWestern Mindanao.
The Mission: The medical schoolexists to help provide solutionsto the health problems of thepeople and communities ofWestern Mindanao . . . . notlimited to individual medical
MOVING TOWARDS UNITY FOR HEALTH
care alone, but achieved throughsocial, economic, political andeducational development of thecommunities.
Piece by piece, we developed anintegrated curriculum with prob-lem-based learning, community-oriented and community-basededucation and competence-basedevaluations. All basic science, clini-cal issues and social/communitycontexts for health are integratedinto the problem-based learningapproach.
Three educational strands areintertwined: a working-problemstrand, a population strand and aprofessional skills strand. As earlyas their first year, students are ex-posed to patients both in clinicsand communities, where the focusis on the practice of medicine in itssocial or community setting. About18 months are spent studying andworking under supervision in re-mote rural communities; of this,only 20% is spent in hospital-basedtraining.
A snapshot from CanadaAurel Schofield, Université de Sherbrooke
Since 1994 we have enrolled 15to 25 students each year, depend-ing on the quality of the applicants.Ten graduates of the first class(1998) passed the examinations ofthe Philippine Medical Board in1999, and some are now working asphysicians in remote regions,equipped with skills in communityhealth development. We havealready seen many changes in somecommunities where the studentswork.
Developing an innovative medi-cal school in pursuit of the goals ofhealth for all is a challenging anddemanding project. However, thepressing unfulfilled health needs ofour communities require no lessthan that we focus our efforts oncollaborating with all sectors to thisend. ■
Dr Cristobal is Dean, Zamboanga MedicalSchool Foundation, Inc.; Ateneo deZamboanga; La Purisima Street; Zamboanga,PHILIPPINES (telephone: +62 991 0871; fax:+62 991 0870) and was the founding dean ofZamboanga Medical School Foundation.
New Brunswick is one of the fourAtlantic Provinces of Canada. It
is a small province, covering about77 000 square kilometres. It has atotal population of 760 000, ofwhom 33% are French-speakingand another 66% are English-speaking; within its boundaries afew small native communities arealso dispersed. It is the only offi-cially bilingual province in Canada.
This small province offers a well-structured health system organizedthrough a central health ministry.Regional hospital corporations areresponsible for health services tothe communities, and mentalhealth services and public healthare delivered through regional
offices. New Brunswick also has awell-developed education systemin both official languages, but itlacks a medical school and does notoffer specialty training in healthservices. There is also a well-developed information networkthroughout the province.
However, the rising cost of healthservices; the relative lack andmaldistribution of physicians,nurses and other health care pro-viders; insufficient services forhigh-risk populations; increasingdemand for mental health services;and special health needs of theaged, adolescents and nativepopulations are all factors that willcertainly contribute to a major
crisis in the years to come. A majorinnovative effort must be made toreduce the present fragmentationin the health system and make thebest use of all existing resources.
For these reasons, a “Towards
New Brunswick
Canada

TOWARDS UNITY FOR HEALTH, APRIL 2000 ■ 13
Unity for Health” approach to theNew Brunswick health services sys-tem would be most beneficial. Witha small province like ours and witha well-developed infrastructure, itwould certainly be possible toengage in a province-wide project.How should we proceed?
We are convinced that the prin-cipal partners must share a com-mitment towards interventions
that positively influence the healthof the population. A joint consulta-tive group has already been formedto pursue a medical educationinitiative for the French-speakingpopulation. This consultativegroup could be expanded toinclude all major stakeholders toidentify common goals and objec-tives and to determine jointactions.
We will soon make a proposal topolicy-makers, health managers,health professions associations,academic institutions and commu-nity representatives in New Bruns-wick to develop a “Towards Unityfor Health” project and we lookforward to reporting on its develop-ment in a future issue of thisnewsletter. ■
Dr Schofield is Coordonateur de la Formationmédicale francophone du Nouveau-Brunswickand Vice-Doyen Adjoint pour le Nouveau-Brunswick, Faculté de Médecine, Universitéde Sherbrooke, 667 rue Champlain, Suite 101,Dieppe, Nouveau-Brunswick, CANADA E1A1P6 (fax: +1 506 862 4179; e-mail:[email protected]).
Dr Aurel Schofield
MOVING TOWARDS UNITY FOR HEALTH
Towards Unity for Health ProjectProposed Activities in 2000–2001,as of 10 March 2000The activities of the TUFH project aregrouped as follows:
■ Advocacy and strengthening of col-laboration
■ Learning from field project sites■ Consultation with stakeholders’
groups■ Scientific and technical work■ Production and exchange of infor-
mation.
Year 20001st quarterEstablishment of a “Towards Unity forHealth” Advisory Committee (TUFH-AC) composed of representatives ofdifferent stakeholders and healthagencies.
Establishment of a World Wide Website.
2nd quarterDissemination of the first issue of theWHO newsletter Towards Unity forHealth.
Publication of four documents relatedto the TUFH international conferenceheld in Thailand in 1999: workingpaper, conference proceedings (longand short version) and monograph ofcase studies.
Dissemination of TUFH documents toconference participants and con-cerned organizations and associa-tions.
Exchange of information and explora-tion of collaboration with national andinternational organizations and asso-ciations.
Presentation of the TUFH approach atinternational meetings.
Collaboration to apply the TUFHapproach in selected disease control(i.e. tuberculosis) or health develop-ment programmes (i.e. maternal andchild health).
3rd quarterSelection of up to 12 field project siteswith contracts to document endeav-ours over a period of two to four yearsin developing the TUFH approach.
International workshop on the use ofhealth information at district level tocreate unity for health.
Presentation of the TUFH approach atinternational meetings.
4th quarterRegional meeting (site to be decided)to promote the TUFH approach anddevelop opportunities for its applica-tion at national level.
Consultation on “Family Medicine/General Practice and Towards Unityfor Health”.
Second issue of the WHO newsletterTowards Unity for Health.
Year 20011st quarterInternational consultation to streng-then collaboration of NGO’s (non-governmental organizations) in theTUFH project.
Regional meeting (site to be decided)to promote the TUFH approach anddevelop opportunities for its applica-tion at national level.
Reports of activities from selected fieldproject sites, based on a commonprotocol to develop a TUFH approach.
2nd quarterPlanning/implementation of joint workwith selected NGOs, as determinedduring the international consultationheld in the first quarter of 2001.
Third issue of the WHO newsletterTowards Unity for Health.
Reports of activities from selected fieldproject sites based on a commonprotocol to develop a TUFH approach.
Review of opportunities to hold asecond TUFH international confer-ence.
3rd quarterReports of activities from selected fieldproject sites based on a commonprotocol to develop a TUFH approach.
4th quarterFourth issue of the WHO newsletterTowards Unity for Health.
Reports of activities from selected fieldproject sites based on a commonprotocol to develop a TUFHapproach. ■

14 ■ TOWARDS UNITY FOR HEALTH, APRIL 2000
MOVING TOWARDS UNITY FOR HEALTH
Towards Unity for Health:The Phuket ConsensusBackground
The participants in the interna-tional “Towards Unity for
Health” Conference in Phuket,Thailand, on this day of 13 August1999 present this statement ofConsensus to serve as a foundationfor the development of partner-ships to promote health for allpeople worldwide.
This Consensus is grounded inthe fundamental principles out-lined in the United Nations Univer-sal Declaration of Human Rights,resolution 1997/71 of the UnitedNations Commission on HumanRights; the Declaration of Alma Ata;and the World Health Organiza-tion’s Global Strategy for Healthfor All, derived from resolutionWHA30.43 (1977) of the WorldHealth Assembly and the WorldHealth Organization’s definition ofhealth. In addition, the Consensushas imbedded within it the notionsof health-related human rightsfound in the codes of professionalethics and conduct and patients’rights promulgated by many pro-fessions in many nations.
We agree that:
● The health of individuals andfamilies reflects the health of thecommunities and environments inwhich they live, work and play.● Each person has the right tohealthy environments and equita-ble, humane and ethical healthservices.● The good of individuals, commu-nities and the environment must berespected and considered in allmatters relating to health.● Policies and practices that affecthealth must be evidence-based,rational and sustainable and mustaim at achieving both individualand societal good.● Effective partnerships betweenindividuals and communities andall sectors—private, public, profes-
sional and voluntary—are essentialto creating and sustaining effectivehealth interventions and pro-grammes.● Global society must ensure ad-equate resources for the health ofall its members.● Responsibility and accountabil-ity for health, particularly that ofthe most vulnerable, are shared byall partners across all sectors.
Recommendations forAction AgendaThe following agenda for action isproposed. Implementation of thisagenda will depend on a funda-mental reorientation of the educa-tion, training and continueddevelopment of the wide range ofstakeholders in health.● Synthesise and promote theTUFH Consensus.● Identify the key determinants ofpartnerships that impinge onhealth.● Create mechanisms for develop-ing the new skills needed for com-munity alliances: cross-sectoralconsensus-building, communityengagement, leadership training,
management and resource devel-opment and deployment.● Develop shared knowledge andinformation systems for appraisingpartnerships and benchmarkingthe outcomes and impacts of TUFHprojects.● Engage civil society, the publicand private sectors and communityleadership in the TUFH partnershipmovement.● Ensure support for TUFH by allstakeholders.● Ensure adequate resources toprovide appropriate technical as-sistance, demonstration projects,research and evaluation of sustain-able TUFH partnerships.● Develop, disseminate and imple-ment a strategic plan to advanceexpand a sustainable collaboratingTUFH network.
The World Health Organization,as the world’s key agency in inter-national health, should take thelead in developing and promotingthis Consensus. A resolution shouldbe drafted for adoption by theWorld Health Assembly to giveeffect to the implementation ofUnity for Health. ■
Towards Unity for Health:collaboration wantedIf your organization or institution
is interested in participating inWHO’s “Towards Unity for Health”(TUFH) project, please read fur-ther. A WHO contract and grant willbe offered to 12 field project sitesworldwide, selected on the basis ofwritten proposals.
The TUFH project aims at reduc-ing fragmentation in the healthservice delivery system and facili-
tating the implementation of a pri-mary health care-oriented systemfor a given population through in-novative patterns of services to in-tegrate medicine and public healthand promote sustainable partner-ships among key stakeholders atthe level of the target population. Adescription of the TUFH projectappears in the WHO working paper“Towards unity for health: chal-

TOWARDS UNITY FOR HEALTH, APRIL 2000 ■ 15
MOVING TOWARDS UNITY FOR HEALTH
lenges and opportunities for part-nership in health development” (apreliminary draft of which is avail-able from WHO headquarters,Geneva, at the address below).
Criteria for selection
The field projects should aim tomeet the four following sets ofcriteria:
1.Innovative patterns of services forintegrating medicine and publichealth1.1 using a reference population
and focusing on a territory1.2 developing an organizational
model for integration1.3 promoting comprehensive
health information manage-ment
2.Implications for health profes-sions2.1 promoting new roles and
rewards in practice2.2 ensuring social accountability
of educational institutions andprogrammes
3.Partnerships3.1 creating alliances with
principal partners (policy-makers, health managers, thehealth professions, academicinstitutions, communities)
3.2 ensuring sustainability inpartnership
4.Evidence of impact4.1 planning dissemination4.2 measuring effects in terms of
quality, equity, relevance andcost-effectiveness.
Coordination mechanismIn addition, the field projectsshould provide evidence of coordi-nation by the five proposed keystakeholders/partners—policy-makers, health managers, profes-sional associations, academicinstitutions and communities—atthe level where the project is beingimplemented.
ProposalsA proposal of about three pages(double-spaced) indicating howthe project is currently meeting orintends to meet the four sets of pro-posed criteria and ensure coordina-tion among partners should besubmitted by 31 August 2000 to:
Dr Charles Boelen, EIP/OSDWorld Health Organization1211 Geneva 27SWITZERLAND(Telephone: +41 22 791 2510;Fax: +41 22 791 4747;E-mail: [email protected]).
Up to 12 field project sites will beselected by the TUFH advisory
committee. In return for a WHOcontract and grant of up to USD10 000, each selected institution ororganization must submit fourquarterly reports on progress inmeeting the proposed criteria. It isessential that all collaboratinginstitutions communicate withWHO headquarters in either Eng-lish or French. ■
Project UNI-SOL:collaboration wantedProposals are invited from uni-
versities interested in collabo-rating with the WHO/UNESCOproject UNI-SOL (which stands for“Universities in Solidarity forHealth of the Disadvantaged”). AWHO contract and grant will beoffered to six universities world-wide, selected on the basis of theirproposals.
The UNI-SOL project aims atmobilizing the broad potentialwithin universities to improve thehealth and well-being of the dis-advantaged. This will be accom-plished through a multidisciplinaryapproach involving coalitionsbetween the participating universi-ties, communities, local govern-ment and the health professions.
The UNI-SOL project expects toweave global links among univer-sities that share the values andcommitment outlined in the “Ari-zona Charter” (ratified at the WHOand UNESCO-sponsored globalconference, “Universities andHealth of the Disadvantaged”, heldin Tucson, Arizona, USA, in July1999). UNI-SOL will be a strongadvocate to encourage the aca-demic world to study and activelyparticipate in both improving thehealth of the disadvantaged andin peace and social justice issuesthat support the design and imple-mentation of internationalprogrammes.
Through developing privilegedlinks with a sample of universityprojects, UNI-SOL wishes to learnfrom field experience and dissemi-nate information on outstandingefforts to meet its objectives.
Project featuresUNI-SOL is interested in activelycollaborating in university projectsthat meet the following four sets ofcriteria:
1. Targeting the disadvantagedThe university clearly indicates itsfocus on one or more targeteddisadvantaged groups, such asstreet children; illiterate mothers;illegal immigrants; the chronicallyjobless; socially proscribed groups(for cultural, religious and otherreasons); the handicapped; thelonely aged; people at war; andrefugees.
The university should be in aposition to justify its choice oftarget group(s), as well as its antici-pated action. This involves demon-strating having considered thepriority health and social concernsin the given national or local con-text, and opportunities to pursuethe proposed action on a widerscale or with other disadvantagedgroups.
In the selection process, prioritywill be given to a university thatchooses one or more disadvan-

16 ■ TOWARDS UNITY FOR HEALTH, APRIL 2000
taged groups known for their vul-nerability and their representative-ness in the national context.
2. Multidimensional approachThe university gives evidence thatit can mobilize several faculties ordepartments to study and act infavour of a particular disadvan-taged group. Its activities vis-à-visthe disadvantaged are not re-stricted only to interventions ofhealth sciences (medicine, nursingor public health), but incorporateinputs from other faculties ordepartments, such as politicalsciences, social sciences, econom-ics, etc. The leadership of theproject can rest with faculties ordepartments outside the healthsciences.
Priority in the selection processwill be given to a university that in-volves in its activities with regard tothe disadvantaged a wide spectrumof faculties/departments beyondthose of the health sciences.
3. Comprehensive approachThe university shows evidence of itscontribution through education,research and service functions. Forexample, its students may beoffered learning opportunities inreal-life situations early andthroughout their curricula, prefer-ably in multiprofessional groups.
In research, activities couldcentre on situation analysis of aparticular target group from ahealth and social perspective or onoperational research, with assess-ment concerning the impact ofintervention programmes.
In service, activities may bedirected towards the planning anddelivery of services, taking intoaccount the main determinants ofdisadvantages and prejudices, witha particular emphasis on preven-tive measures from a health andsocial perspective.
Priority in the selection processwill be given to a university thatshows balanced inputs from and toeducation, research and services.
MOVING TOWARDS UNITY FOR HEALTH
4. Institutional change andsustainability
The university has developed astrong relationship with local gov-ernments, communities and pro-fessions active in the health andsocial sectors, for the purpose ofestablishing a durable partnershipin support of a particular disadvan-taged group or of contributing toinstitutional change.
Action could be related to politi-cal lobbying, social advocacy,development of strategies for sus-tainable actions or establishinglocal, national or international net-works. While the university playsthe role of a catalyst, the major re-sponsibility for execution of thework lies with other partners.
In the selection process, prioritywill be given to a university thatshows evidence of its consistentcommitment to institutionalchange in favour of the disadvan-taged.
University commitmentThe project should offer evidenceof the university’s commitment tothe disadvantaged by meeting thefollowing criteria:
● Institutional backing: The com-mitment of the university isconfirmed by a letter signed bythe president, vice chancellor oranother representative of theuniversity’s leadership.
● Coordination mechanism withinthe university: A list of repre-sentatives of the different facul-ties and departments involved inthe project is provided, as well asan indication of how coordina-tion will be ensured.
● Coordination with partnersoutside the university: A list ofrepresentatives of partners out-side the university is provided, aswell as an indication of howcoordination will be ensured.
Submission of proposalsA proposal of no more than threepages, presenting arguments rela-tive to the above-mentioned four
project features and three indica-tors of university commitment,should be submitted by 31 August2000 to the following address:
UNI-SOL secretariatWHO Collaborating Centre on
Border and Rural Health Re-search
College of MedicineUniversity of Arizona Rural Health
Office2501 East Elm StreetTucson, Arizona 85716USA(Telephone: +1 520 626 7862;Fax: +1 520 321 7763;E-mail: [email protected]).
Up to six universities will beselected by the UNI-SOL advisorycommittee. In return for a WHOcontract and grant of up toUSD 10 000, each selected univer-sity must pursue its project for twoyears and submit reports onprogress in developing the projectaccording to the proposed featuresand criteria. It is essential that allcollaborating universities commu-nicate with WHO headquarters ineither English or French.
For further information on theUNI-SOL project and on the selec-tion, please contact the UNI-SOLsecretariat.
For contact with WHO on theUNI-SOL project:
Dr Charles Boelen, EIP/OSDWorld Health Organization1211 Geneva 27SWITZERLAND(Telephone: +41 22 791 2510;Fax: +41 22 791 4747;E-mail: [email protected]).
For contact with UNESCO on theUNI-SOL project:
Mrs Christine von FurstenbergUnited Nations Educational,
Scientific and Cultural Organiza-tion
1 rue Miollis75015 ParisFRANCE(Telephone: +33 1 45 68 45 16;Fax: +33 1 45 68 57 24;E-mail: c.von-

TOWARDS UNITY FOR HEALTH, APRIL 2000 ■ 17
Working withthe WorldHealthOrganizationIn implementing its programme,
WHO is looking forward to collabo-rating with institutions and individu-als with recognized expertise andinternational experience in thefollowing areas:
■ Accreditation: accreditation orcredentialing of educational institu-tions or programmes, primary healthcare services or health professionals.
■ Family medicine/general practice:the contribution of family medicineor general practice to health systemreform; family medicine/generalpractice and community health/public health; population-basedapproaches; primary health careteams.
■ Integrated health services: integra-tion of individual and communityhealth at district level; innovativeorganizational patterns to supportintegrated approaches; competenceand motivation of health profession-als working in such settings.
■ Changing roles of professions:methodologies to identify determi-nants for changing roles of healthprofessions; adaptation to health sys-tem changes; reallocation of respon-sibilities and health professions mix;motivation and remuneration.
■ Universities and the disadvan-taged: strategies to mobilize a widerange of faculties and departmentswithin a university in favour of healthof the disadvantaged; coalitions be-tween universities and civil societyfor sustainable action for health ofthe disadvantaged.
Collaboration may take severalforms, but will not necessarily in-volve financial support from WHO. Itis essential that collaborators befluent in English or French. Forfurther information, please contact:Dr Charles Boelen, EIP/OSD; WorldHealth Organization; 1211 Geneva27; SWITZERLAND. ■
Diarydates✍ ✍ ✍Congrés National Annuel de la Société Marocaine desSciences Médicales8–10 JUNE 2000, RABAT, MOROCCOLe projet “Vers l’Unité pour la Santé” sera lancé à cette occasion.
Pour de plus amples informations, prière de contacter le Dr Theo Lippeveld(Courriel: [email protected]; [email protected]).
[On the occasion of the Annual National Congress of the Moroccan Society of MedicalSciences, to be held in Rabat, Morocco, 8–10 June 2000, a “Towards Unity for Health”project will be launched. For further information, please contact Dr Theo Lippeveld(E-mail: [email protected]; [email protected]).]
✍ ✍ ✍4th Rural Health Conference16–19 AUGUST, 2000, CALGARY, ALBERTA, CANADAConvened by the University of Calgary.
For more information, please contact Ms Irene Pullar, Continuing Medical Education,University of Calgary, 3330 Hospital Drive N.W., Calgary, Alberta, CANADA T2N 4N1(E-mail: [email protected]).
✍ ✍ ✍International Conference on Health Research for Development10–13 OCTOBER 2000, BANGKOK, THAILANDConvened by the World Health Organization, World Bank, Council on Health Researchfor Development and Global Forum for Health Research.
For more information, please contact the Council on Health Research for Developmentc/o UNDP, Palais des Nations, 1211 Geneva 10, SWITZERLAND (E-mail:[email protected]).
✍ ✍ ✍Innovation in Health Professions Education and CommunityOrientation21–26 OCTOBER 2000, MANAMA, BAHRAINConvened by The Network: Community Partnerships for Health Through InnovativeEducation, Service and Research, in collaboration with the College of Medicine andMedical Sciences of Arabian Gulf University.
For more information, please contact Ms Jolanda Koetsier, The Network Office, Facultyof Medicine, Maastricht University, PO Box 616, 6200 MD Maastricht, Netherlands(E-mail: [email protected]).
✍ ✍ ✍International workshop: a primer on the Maastricht approach tomedical education23–24 NOVEMBER 2000, MAASTRICHT, NETHERLANDSThis workshop will be held in November and March each year; the next dates plannedare 22–23 March 2001 and 29–30 November 2001.
For more information, please contact Ms Jolanda Koetsier, Workshop Secretariat,Office for International Relations, Faculty of Medicine, Maastricht University, P.O. Box616, 6200 MD Maastricht, Netherlands (E-mail: [email protected]).
MO MO

18 ■ TOWARDS UNITY FOR HEALTH, APRIL 2000
PRACTICE GUIDELINES
Integrated management of childhood illness (IMCI):A challenge for both health professionals andteaching institutionsIvan Lejnev and Rebecca Bailey, World Health Organization, Geneva
Each year more than 10 millionchildren in developing coun-
tries die before they reach their fifthbirthday. About 70% of these deathsare associated with infectious dis-eases and inadequate nutrition.Among the children who do sur-vive, many are still unable to growand develop to their full potential.Doctors have an important role inimproving this situation throughthe effective prevention and man-agement of childhood diseases andmalnutrition.
The WHO Department of Childand Adolescent Health and Devel-opment (CAH), together with itspartners, is working to develop andintroduce approaches to combatchildhood illness and to promotehealthy growth and development.These efforts have resulted in a newstrategy that focuses on the child asa whole, rather than on a single dis-ease or condition. It is called Inte-grated Management of ChildhoodIllness (IMCI).
Action is being taken to intro-duce the teaching of IMCI in medi-cal schools to help ensure thatfuture doctors:
● know proven methods for pre-venting and managing majorchildhood illnesses,
cedures. In addition, the guidelinesinclude methods for teachingparents how to give treatments athome, for assessing a child’s feed-ing, for counseling parents to solvefeeding problems and for advisingparents about when to return to ahealth facility.
Why is IMCI needed in medicaleducation?Doctors play a key role in promot-ing the correct management ofmajor childhood illnesses and inensuring the best preventive inter-ventions for children, families andcommunities. In many countriesdoctors are responsible for the in-service training or the supervisionof other cadres of health workers.Yet doctors can give proper supportonly if they understand and agreewith recommended proceduresand if they apply them in their ownpractices on a routine basis. For thisreason, appropriate training formedical students is a logical firststep towards establishing scientifi-cally sound practices among doc-tors and subsequently among otherhealth professionals.
IMCI is relevant to medical edu-cation because it:
● encompasses basic elements ofhigh-quality care
● ensures that sick children arethoroughly assessed and treated
● addresses the most frequenthealth problems of children
● provides additional skills in im-portant areas such as nutritioncounseling
● influences care-seeking behav-iours
Dr Ivan Lejnev Ms Rebecca Bailey
● have the skills needed to care forsick children in an integratedand effective manner,
● are able to work together withfamilies,
● are able to support and follownational guidelines.
Yet numerous challenges mustbe overcome in a country beforehealth professionals and teachinginstitutions are able to practise andteach the IMCI guidelines. Thesechallenges include, for example,reaching consensus on health pri-orities in a country, preparing thehealth system to support IMCI-trained graduates, incorporatingIMCI into already crowded teach-ing agendas, strengthening or evenchanging teaching methods andensuring coordination betweendisease-specific programmes andbetween different teaching units.
What are the IMCI clinicalguidelines and where should theybe used?The IMCI clinical guidelines useproven, practical measures for theprevention and cure of the mostserious or lethal childhood ill-nesses. The guidelines promotestandard assessment and treat-
ment, using syndrome-based methods thatsupport the rational,effective and affordableuse of drugs. The guide-lines are designed for usein outpatient clinical set-tings where health pro-fessionals have limiteddiagnostic tools, limitedmedications and limitedopportunities to practisecomplicated clinical pro-

TOWARDS UNITY FOR HEALTH, APRIL 2000 ■ 19
PRACTICE GUIDELINES
● provides a link to real-life situa-tions
● prepares doctors to manage sickchildren in outpatient settings
● combines preventive and cura-tive care
● links different levels of healthprofessionals and different levelsof a health system
● rationalizes some outpatientprocedures and emphasizesaffordable interventions
● helps doctors recognize theseverity of a child’s conditionand take necessary action attimes when a single diagnosis isdifficult
● promotes rapid treatment andreferral for severely ill children.
What are the challenges to intro-ducing IMCI into medical schools?
Reaching consensus on healthpriorities: Introduction of the IMCIstrategy in a country takes an im-portant step towards tailoring pae-diatric teaching to the needs anddemands of a society. During thisprocess, agencies within the gov-ernment, the academic commu-nity, professional societies andnumerous other individuals andinstitutions work together to ensurethat the IMCI clinical guidelinesreflect national guidelines and poli-cies, fit cultural and languagedifferences and address the mostserious childhood illnesses in acountry. Reaching consensusamong a broad group of individu-als with various interests is atremendous challenge.
Strengthening the health system toallow graduates to practise newlyacquired skills: Teaching IMCI inmedical schools will not ensure thatstudents actually follow thoseguidelines after graduation. It iswell known that a discrepancyexists between what is taught inmedical schools and what is prac-tised. Experience shows thatstudents use case management
guidelines when instructed to doso. Afterwards, when working asresidents, however, they do notalways follow those guidelines.Negative forces in the clinical envi-ronment, such as lack of supplies,lack of supervision or lack of skillreinforcement, influence practices.In order to encourage graduates topractise what they have learned,health facilities must be organizedand equipped to implement IMCIand both professors and practition-ers must use those procedures.
Reshaping the way paediatrics istaught: In essence, integrated casemanagement is not something new.Because IMCI focuses also on out-patient management, its principlesmay not be fully compatible withhospital-based, diagnostic meth-ods that are frequently used toteach paediatrics. For this reason,careful planning is needed toensure that IMCI is incorporatedinto the overall paediatrics agenda.The same concepts should also beincluded in the formal evaluation ofstudent knowledge and skills inorder to reinforce the importanceof the guidelines.
Giving priority to interactive and skill-oriented teaching: The introductionof integrated case managementpresents an opportunity to
strengthen more dynamic learningprocesses. Students are helped todevelop case management skillsthrough supervised clinical prac-tice with a variety of patients in out-patient settings. Ideally, studentsshould learn clinical skills in an en-vironment where integrated casemanagement is being practised.Consequently, medical facultieswill need to prepare appropriateclinical training sites and to traininstructors and relevant clinicalstaff in the IMCI guidelines.
Ensuring coordination betweendisease-specific programmes andbetween different teaching units: TheIMCI strategy encourages differentagencies and institutions in a coun-try to work together to identify childhealth problems and to agree on acommon approach to those prob-lems. This coordination requirescareful planning as well as mecha-nisms for sustaining interaction.The introduction of IMCI in medi-cal schools will require similarefforts to coordinate teachingamong different academic depart-ments and units. ■
Dr Lejnev is a Medical Officer and Ms Bailey isa Technical Officer, Department of Child andAdolescent Health and Development (CAH),World Health Organization, 1211 Geneva 27,SWITZERLAND (telephone: +41 22 791 3288;e-mail: [email protected]).
Family medicine/general practice andhealth system changes: a new WHO/WONCA*collaborative projectThe aim of this project is to produce a reference guide to help policy-makerswith major decisions regarding the development and strengthening of familymedicine/general practice in the wake of important health system changes inspecific national contexts.
Chapters of the guide will focus on: opting for family medicine/general practiceas a foundation for health services delivery; educating family physicians/general practitioners; organizing a professional association; conducting healthsystem research, including in family medicine and general practice.
More information will be provided in the next issue of the TUFH newsletter. ■
*WONCA is the World Organization of Family Doctors.
20 ■ TOWARDS UNITY FOR HEALTH, APRIL 2000
The WHO Reproductive Health Library:A tool to incorporate evidence-based reproductivehealth into medical education and practiceA. Metin Gülmezoglu and José Villar, World Health Organization, Geneva
views, commentaries and practicalaspects documents. The latter twocomment on the relevance of thereview findings to under-resourcedsettings and are published after in-ternal and external peer review. TheUseful information section con-tains lists of funding agencies andnongovernmental organizations inreproductive health.
Challenge of changing behavioursIn the initial phase of the projectour aim has been to disseminateRHL as widely as possible by meansof WHO mailing lists, conferences,workshops and relevant e-maildiscussion lists around the world.There are now RHL focal pointsin Argentina, China, Cuba, India,
I n d o n e s i a ,Mexico, the Phil-ippines, SouthAfrica, Thailandand Uruguay.
While theseactivities mayhave been veryuseful in raisingawareness aboutRHL and provid-ing access to
many health care workers, moreneeds to be done towards gettingthe evidence presented into prac-tice. There is now compelling evi-dence of the ineffectiveness ofpassive dissemination to affect be-haviour change (1). Receiving RHLdiskettes in the mail is thereforeunlikely to make a big difference inpractice, at least in the short term.
To evaluate this issue, we haveinitiated a cluster randomized trialto evaluate a programme of educa-tional outreach using RHL in 40 dis-trict hospitals in Mexico, SouthAfrica and Thailand. If effective, this
strategy can be introduced on awider scale to influence the prac-tices at that level. The trial will becompleted by end of 2001.
We believe that incorporatingevidence-based practices as rec-ommended in RHL will requireaction in undergraduate and post-graduate training as well in target-ing practising health workers. RHLis currently included in the fourth-year obstetrics and gynaecologysyllabus at the University of Preto-ria, South Africa. The Royal ThaiCollege of Obstetricians andGynaecologists has recommendedRHL to doctors undergoing special-ist training since 1999. This is thebeginning of a worldwide effortaiming at undergraduate and post-graduate education and clinicalpractice levels of the health systemto incorporate evidence-basedreproductive health into practice.
We look forward to collaborationwith more medical schools aroundthe world interested in using RHLin their medical curriculum. ■
Reference1. NHS Centre for Reviews and
Discussion. Getting evidenceinto practice. Effective HealthCare, 1999, 5:1–16.
Dr Gülmezoglu and Dr Villar are RHLCoordinating Editors, Department ofReproductive Health and Research, WorldHealth Organization, 1211 Geneva 27,SWITZERLAND (e-mail:[email protected]; [email protected]).
PRACTICE GUIDELINES
The WHO Reproductive HealthLibrary (RHL) is an annually up-
dated electronic review journalpublished by the WHO Departmentof Reproductive Health andResearch since 1997. RHL includessystematic reviews of effectivenessof reproductive health care inter-ventions relevant to important re-productive health problems indeveloping countries.
The systematic reviews are takenin their entirety from the CochraneDatabase of Systematic Reviewspublished in The Cochrane Library.Each review is supplemented by acommentary prepared by an indi-vidual from a developing country orsomeone with extensive knowledgeof conditions of those settings.
RHL is dis-seminated tohealth workersin developingcountries on afree-subscrip-tion basis. RHLNo. 3 will bepublished inearly 2000 onthree diskettes:13,000 copieswill be made available in Englishand 5000 in Spanish. In English,3000 CD-ROMs will also be pub-lished.
RHL contents are arranged infour sections. The first section con-tains editorials relating to priorityreproductive health problems,evidence-based medicine andmethodological issues. Effective-ness summaries categorize in onesentence the evidence synthesizedin the database according to thelevel of benefit or harm.
The Reproductive Health Data-base contains the Cochrane Re-
RHL contents:
■ Reproductive health indeveloping countries
■ Effectiveness summaries■ Reproductive Health
Database■ Useful information

TOWARDS UNITY FOR HEALTH, APRIL 2000 ■ 21
FIVE-STAR PRACTITIONERS
Health personnel – a country priority:a viewpoint from BotswanaTeguest Guerma, WHO Representative, Gaborone
many of the public health pro-grammes of national importance.The current pool of physicians inthe country is 410, among whom347 are expatriates, which meansthat only 15% are locals. Further-more, all district medical officers ofthe country are expatriates. Facedwith this shortage of local physi-cians, the government recentlydecided to establish a medicalschool in the country, but this is along process that will take years torealize.
Deciding on prioritiesBuilding capacity by offeringfellowships to scientists in develop-ing countries is an important partof the WHO programme. Severalresolutions adopted by the WorldHealth Assembly have reinforcedthis commitment in recent years.
A recent retreat organized jointlyby the Ministry of Health of Bot-
swana and WHOto set prioritiesfor the comingfive years’ techni-cal cooperationidentified humanresources forhealth develop-ment as a top pri-ority. This meantreducing thebudget of otherongoing priorityprogrammes inorder to focusmore on training.
This was not an easy exercise to gothrough, but after a comprehensiveanalysis of its merits the govern-ment upheld this decision.
WHO’s contribution is expectedto serve as a catalyst for an intensi-fied training programme of physi-cians by the Ministry of Education
and other partners. The long-termobjective of this decision is to in-crease the proportion of Batswana,or local, physicians to at least 40%by the year 2008. The cost-effective-ness of this investment appearsevident when we consider theamount of the health budget cur-rently spent to employ expatriates.
The development of human re-sources for health, although thebasis of the health system, is oftenneglected by countries facing manyother health priorities. The currentmoves of the government of Bot-swana to redress the imbalancesare commendable and are worthemulating elsewhere in the Africanregion. ■
References● Coordinated health and humanresources development. Report of aWHO Study Group. Geneva, WorldHealth Organization, 1990 (WHOTechnical Report Series, No. 801).
● Health manpower plan forBotswana, 1998–2002. Gaborone,Ministry of Health, 1999.
● Report of Ministry of Health/WorldHealth Organization retreat.Mokolodi Nature Reserve, 4–5December 1998. Gaborone, Ministryof Health, 1999.
Dr Guerma is the WHO Representative,Gaborone, BOTSWANA (fax: +267 35 94 83).
The objective of the WHO GlobalStrategy for Health for All is to
enable each country to provide itscitizens with all potentially usefulhealth services. This will never beachieved without the developmentof skilled and appropriate humanresources. A country’s capacity toimplement public health pro-grammes and ensure effectivedelivery of health care services to itspeople is determined by the extentto which its human resourcesdevelopment keeps pace with therequirements of health.
Human capitalIn order to fulfil this importantneed, several developing countrieshave identified investment in hu-man resources as their priority inhealth and have developed com-prehensive policies and plans.Many of them have establishedtheir own training institutions inorder to traintheir human re-sources locallybecause of po-litical decisions,existing infra-structure orsometimes na-tional pride.Others haveopted not to es-tablish local in-stitutions, partlybecause of hightraining costsand partly be-cause of easy access to suitabletraining institutions in neighbour-ing countries; Botswana was part ofthis group.
Over the years, however,Botswana has experienced an in-creasingly serious shortfall in theworkforce needed to implement
Dr Teguest Guerma

22 ■ TOWARDS UNITY FOR HEALTH, APRIL 2000
PRACTICE GUIDELINES
A five-star doctor for Africa:desirability and feasibilityAlan A. Fatayi-Williams, WONCA, Lagos
ary and tertiary levels.The primary levelcomprises healthposts, health clinics, dis-trict primary healthcentres and comprehen-sive health centres. Thesecondary level com-prises all general anddistrict hospitals. Thetertiary level comprisesall specialist hospitals,such as those for teaching or fororthopaedic or psychiatric care.
Since 1990, however, successivegovernments have not provided anadequate level of funding to sustainthese services, and this has resultedin Nigeria’s having among the high-est infant and maternal mortalityrates in the developing world. Thebasic three-tier structure is still inplace, however.
A five-star MD for NigeriaThe five-star doctor, like a four-stargeneral, has to be equipped to workat any of the three levels, and espe-cially at the primary and secondarylevels.
★ Community leader and motivator:He or she must lead by example andbe able to both teach and motivatethe community: to impart thehabits of cleanliness and sensiblepreventive medical care; advocatethe importance of child health,well-baby clinics and family plan-ning services; and encourageinvolvement in appropriatecommunity programmes.
★ Medical scientist: He or she mustremember that as a doctor he or sheis also a scientist, and that researchcan be done not only in a teachinghospital laboratory but also at thevillage level.
★ Decision-maker:He or she must learnto make decisions onhealth matters thatwill be seen andproven to be in thebest interest of thecommunity, andmust endeavour toconvince and enlistcommunity leaders.
★ Health care manager: He or shemust be able to efficiently manageresources and learn to improvisewhere necessary. Dwindling gov-ernment resources in developingcountries translate directly intodwindling health services budgets,which in any case have never beena priority.
★ Communicator: He or she mustdevelop the ability not only totranslate ideas into action but alsoto move freely between the pri-mary, secondary and tertiary levelsof care, as increasingly the generalpractitioner/family physician isbeing trained and equipped to lookafter patients holistically, and toacquire skills that hitherto werethought to be the exclusivepreserve of the general surgeon orobstetrician. ■
Reference● Primary health care curriculumfor community health officers.Lagos, FMOH, Training and Man-power Development Division, 1990.
Dr Fatayi-Williams is Regional Vice-President,Africa Region of WONCA; 54/56 BankoleStreet, PO Box 3870, Lagos, NIGERIA(telephone: +234 1 2660584;fax: +234 1 5830648; e-mail: [email protected]).
Providing health care for Niger-ia’s 110 million people has never
been seen as an easy task. Withnearly one-quarter of the popula-tion of Africa and a largelyrural-based agriculture-orientedpopulation scattered over a variedgeographical terrain, Nigeria hasyet to achieve WHO’s dream ofhealth for all by the year 2000.
Primary health care in progressThe evolution of the health caresystem as it operates today can betraced back to 1986, when primaryhealth care (PHC) programmeswere implemented as the baselinestrategy for the development ofnational PHC services. With thisapproach, even though develop-ment was still centred around thelocal government areas, PHC pro-grammes were now provided withthe technical support to superviseand run the services.
In 1986, technical support wasprovided to 52 local governmentareas (LGAs) by various institutionssuch as the 12 colleges of medicine/university teaching hospitals wherecommunity health officers weretrained. Other local governmentareas were supported by schools ofhealth technology, and by 1990almost all the LGAs had joined as“willing” LGAs.
The result of this system was bet-ter coverage of the population, withpreventive and curative healthservices receiving adequate em-phasis. Appropriate technology wasbeing used, thereby reducing costsand making health care affordable.There was also better managementand coordination of the activities ofthe nongovernmental and interna-tional organizations.
As in most countries, the systemis organized into primary, second-
Dr Alan A. Fatayi-Williams

TOWARDS UNITY FOR HEALTH, APRIL 2000 ■ 23
Essential service package in Bangladeshneeds five-star doctorsM. Muzaherul Huq, Centre for Medical Education, Dhaka
Country profile
Bangladesh is a country tryinghard to overcome its health sec-
tor problems. The Health and Fam-ily Planning Programme has maderemarkable progress over the lasttwo decades. The fertility rate hasdeclined and the immunizationprogramme is successful.
Despite these advances, Bangla-desh still has some major healthproblems. For example, the life ex-pectancy at birth is lower forfemales than for males. Less than40% of the population has access tobasic health care. About 70% ofmothers sufferfrom nutritionaldeficiency anae-mia, and 75% ofpregnant womendo not receiveantenatal care orassistance from atrained attend-ant at the time ofchildbirth, whichindicates inad-equate progress with respect tomaternal mortality and morbidity.Other issues of concern are overallpoor use of government services, aswell as the cost-effectiveness,sustainability and quality of serv-ices.
The present structure of thehealth service delivery system hasseparate cadres at all levels forhealth and family welfare services.Therefore it is not cost-effectiveand its potential for increasing therange, quality and effectiveness ofservices is limited. The presentservice system does not allowclients to obtain services in basichealth, reproductive health andfamily planning from a single serv-ice point, though recent studies ofconsumer preferences by a number
service. Client orientation willrequire a shift in attitudes fromserving the system to serving thepeople for whom the system isdesigned. This change will motivatethe behaviour of both the provid-ers and the managers. Client focuscuts across several areas of con-cern: coverage and quality ofservices; cost-effectiveness; andaccountability.
At the thana and below, the ESPdelivery will be through a unifiedstructure comprising health andfamily planning workers under asingle manager, responsible for theoverall management and adminis-tration of all activities.
Relevance of the five-star doctorThe doctor who will be the pro-posed thana manager should be a“five-star doctor”. The concept ofthe five-star doctor was proposedby Charles Boelen of WHO. Accord-ing to Dr Boelen, the front-linedoctor of tomorrow, who will servethe needs of all health systems andservices, should play the followingprincipal roles:
★ Care provider: who considers thepatient holistically as an individualand as an integral part of a familyand the community, and who pro-vides high-quality, comprehensive,continuous and personalized carewithin a long-term relationshipbased on trust. To deliver ESPefficiently, the doctor should try toprovide as much care as possible tohis patient from one site.
★ Decision-maker: who chooseswhich technologies to apply, ethi-cally and cost-effectively, whileenhancing the care he or she pro-vides. The doctor is the decision-maker in the case of ESP delivery,who decides whether he or she can
FIVE-STAR PRACTITIONERS
of agencies have shown that thepeople of Bangladesh want “one-stop service”.
Essential service packageTo satisfy the needs of the most vul-nerable in the society—women,children and the poor—it has beendecided to develop, in the Healthand Population Sector Programme(HPSP) 1998–2003, an essentialservices package (ESP) for phasedimplementation. The ESP will bedelivered through different levels ofthe primary health care system(community, union, thana and dis-
trict). It is stipu-lated that theprovision anduse of ESP serv-ices wil attain theHPSP objectives.
The ESP aimsto maximizehealth benefitsrelative to percapita expendi-ture, meet felt
needs of the clients, strengthenservice delivery and improve sys-tem management. The elements ofESP are grouped into five majorareas: reproductive health care;child health care; communicabledisease control; limited curativecare; and behaviour change com-munication.
The ESP delivery strategy is toestablish community clinics thatwill provide one-stop community-level ESP services in a consistentlocation for easy access at the timeof need. Thus, a much more com-prehensive range of services can beprovided. ESP is to be delivered onthe thana [sub-district] level andbelow, with referral care at second-ary and tertiary levels.
The ESP will be a client-oriented
Bangladesh

24 ■ TOWARDS UNITY FOR HEALTH, APRIL 2000
provide the care needed or to referthe patient.
★ Communicator: who is able topromote healthy lifestyles by effec-tive explanation and advocacy,thereby empowering individualsand groups to enhance and protecttheir health. Behaviour changecommunication is a cross-cuttingintervention that will use the facili-ties of the rapidly expandingcommunication networks in Bang-ladesh and the growing capacitiesfor planning, designing and imple-menting comprehensive, highlyeffective communication pro-grammes. To realize this compo-nent of ESP, the doctor should be avery good communicator.
★ Community leader: who, havingwon the trust of the people amongwhom he or she works, can recon-cile individual and communityhealth requirements and initiateactions on behalf of the commu-nity. Rural ESP will be delivered
through community clinics. Com-munity participation is essential toensure the service, which meansinvolvement and participation ofthe community in designing, plan-ning, monitoring and helping toimplement the programme. Herethe role of the doctor will be that ofcommunity leader.
★ Manager: who can work harmo-niously with individuals and or-ganizations inside and outside thehealth care system to meet theneeds of patients and communi-ties, making appropriate use ofavailable health data. ESP deliverydepends on the teamwork of a teamcomprising personnel from thehealth and family planning sectors.The doctor is the manager of theteam. For effective and efficienthealth services delivery, the doctormust execute this managerial roleproperly.
In Bangladesh today, clientswant the health system to very effi-
FAMILY PRACTICE
ciently deliver one-stop service inminimum waiting time with a har-moniously working health servicesteam. They therefore expect theESP delivery system to be staffed byfive-star doctors. ■
References● Health and population sectorprogramme 1998–2003. Part 1 andPart 2. Dhaka, Government of thePeople’s Republic of Bangladesh(Ministry of Health and FamilyWelfare), 1998.
● Boelen C. Frontline doctors oftomorrow. World Health, 1994, 47:4–5.
● Personal communication withDr Khaleda Islam, Assistant Profes-sor, Centre for Medical Education,IPH Building (2nd floor),Mohakhali, Dhaka-1212, BANGLA-DESH.
Dr Huq is Director, Centre for MedicalEducation, IPH Building (2nd floor),Mohakhali, Dhaka-1212, BANGLADESH(telephone: +8802 870830; fax: +8802881809; e-mail: [email protected]).
➤ continued from page 23
Family practice and health system evolutionWes Fabb, World Organization of Family Doctors – WONCA, Melbourne
Balance is important: Who woulddisagree with a balanced diet of
animal protein, complex carbohy-drates, leafy greens and yellow veg-etables and fruit? A healthy lifestylebalances work, exercise, recreation,rest, and family life.
Health systems out of balanceHealth care systems, too, need to bebalanced. Many are, but some areseriously out of balance, focusingtoo heavily on hospital and special-ist care, giving scant emphasis tofront-line primary care.
In such health care systems, ter-tiary and secondary care consumesa large proportion of the resources,depriving the primary sector, al-though it usually caters for most ofthe population. This imbalance isseen even in some developing
settings, are valued by the peopleand communities they serve, butoften not to the same extent byacademe, health planners and gov-ernments, who too often favourhigh-profile, high-tech hospitalsand specialists. Hospitals are visiblestatus symbols—monumentsattractive to politicians. In contrast,family doctors provide low-techcare in modest settings that attractlittle attention. Yet this care isessential to balanced health caresystems.
The need for family doctorsFamily doctors need to be able tomanage any problem that presentsand therefore require a broad rangeof general knowledge and skills.Because some problems presentfrequently, such as respiratory ➤
countries where most of the peoplelive in rural areas and dependalmost entirely on primary care.Achieving balance in such situa-tions requires major enhancementof the primary care sector.
There are a variety of primarycare providers, among whom fam-ily doctors comprise a large propor-tion. The World Organization ofFamily Doctors (WONCA) has 63member organizations, the indi-vidual membership of which totals140,000. Add to this the familydoctors in countries where WONCAis not yet represented, such as inCentral and South America andmuch of Africa and Eastern Europe,and the number rises to well over200,000.
Family doctors, who provide pri-mary care for people in community

TOWARDS UNITY FOR HEALTH, APRIL 2000 ■ 25
FAMILY PRACTICE
Professor Wes Fabb
and cardiovascular problems, hy-pertension, diabetes, arthritis andpsychological and family problems,they need knowledge in depth inthese areas. Most people with thesecomplaints are managed almostentirely by their family doctor.
People and their problems aremanaged in the context of the fam-ily and the community. The familycontext is central to the under-standing and management of so
many prob-lems. Familyd o c t o r sbuild up arelationshipof trust andconfidencewith peopleand familiesthat they used i a g n o s t i -cally and
therapeutically. The doctor-patientrelationship is central to familypractice, and indeed to the wholeof medicine.
Longitudinal care, too, is a cen-tral element of family practice.Many illnesses can be understoodonly over time. The high level ofchronic illness now present in mostcommunities demands continuingcare for long periods.
Because family doctors providecare to a broad practice population,they are able to monitor the healthof the populations they serve andtake anticipatory action to improveit. They use the opportunities thatexist in community practice forhealth promotion, preventive care,patient education and rehabilita-tion. They take an approach tohealth care that puts into practicethe principles of systems theory,which expresses the interrelated-ness of biological, psychological,family, occupational, social, eco-nomic, community and environ-mental factors.
Because in family practice a low-tech approach is the norm, thecosts of providing care are modest.A study by Starfield published in1994 showed that: “At least among
western industrialized nations, aprimary care orientation of a coun-try’s health care system is associatedwith lower costs of care, higher sat-isfaction of the population with itshealth care services, better healthlevels, and lower medication use”(Starfield, 1994).
The case of ChinaFamily doctors have a central roleto play in every health care system.Where they are not available, theirabsence results in overloading oftertiary and secondary care facili-ties, and high-cost care, which isoften inappropriate for the prob-lems that present. China is an ex-ample.
In China, the primary care sec-tor, staffed by health workers withlittle training, is not highly regardedand is therefore bypassed by manyfor the secondary and tertiary sec-tors, where doctors provide most ofthe care. Realizing that this situa-tion is too costly and not effectivefor many health problems, thehealth authorities in China haveembraced the concept of familypractice as the basis for their healthcare system for the 21st century.The consequent large number offamily doctors needed is a hugechallenge.
The Capital University of Medi-cal Sciences in Beijing has alreadyestablished a training programmein family medicine. In the prov-inces, where most of China’s popu-lation lives in rural settings, thereis much interest in family practice,but the meagre resources makeit difficult to train the doctorsneeded. Moreover, since the eco-nomic downturn in Asia there hasbeen diminished central govern-ment support. In the meantime,there is interest in applying theabove-mentioned concepts of fam-ily practice through the existingsystem of health care workers.
A guide for developing familymedicineRecognizing the need for a practi-cal manual of guidelines to assist
those who wish to introduce fam-ily practice into their evolvinghealth care system or enhance itsinfluence, WHO and WONCA haveembarked on a collaborative en-deavour to produce such a guide.After preliminary meetings wherethe content outline was developed,writing has commenced, with aview to publication in 2000. Theguide will include not just the ex-pected description of undergradu-ate and postgraduate education,training and assessment, but willcover the anticipated obstacles andways of overcoming them, and thepolitical aspects, so important tothe numerous stakeholders. It willbe designed to give practical helpand advice at every stage.
There are three purposes for thisguide:
● To help leaders improve people’shealth by reorienting healthsystems towards the goals of qual-ity, equity, relevance and cost-effectiveness.
● To help leaders understand therole of family practice in this effortto reorient the health system.
● To help leaders make decisionsfor the development of family prac-tice in their country or region.
The guide is being designed toassist international consultants (or-ganizations and institutions) whoare responding to requests for fam-ily practice assistance, ministers ofhealth and other policy-makerswho want to reorient their healthsystem, and pioneers/leaders whowant to develop family practice asa means of reorienting the healthcare system.
It will be yet another step on thepath of health for all throughprimary health care. ■
Professor Fabb is Chief Executive Officer,World Organization of Family Doctors—WONCA, Locked Bag 11, Collins Street EastPost Office, Melbourne Victoria 8003AUSTRALIA (telephone: +61 3 9650 0235;fax: +61 3 9650 0236;e-mail: [email protected];WONCA Website: www.wonca.org).

26 ■ TOWARDS UNITY FOR HEALTH, APRIL 2000
FAMILY PRACTICE
Health care reforms in the Philippines:the contribution of family physiciansZorayda E. Leopando and Eduardo Banzon, University of the Philippines
decision-maker, communityleader, communicator and teammember, five roles have been iden-tified for family physicians. Theroles and their correspondingresponsibilities are as follows:
★ Health care provider: He or sheprovides family-oriented care. Heor she provides promotive,preventive, curative and rehabilita-tive care and acts as the gatekeeperof health care. Conscious of theneed for quality of care to be givento patients and their families, he orshe participates in quality improve-ment projects.
★ Counselor: He or she listens,clarifies doubts, helps facilitateresolution of problems andreassures patients and their rela-tives.
★ Teacher/educator: He or she advo-cates a healthy lifestyle and ensurescompliance through education. Heor she not only disseminates infor-mation to patients but is also a rolemodel to residents and medicalstudents.
★ Researcher, scientist and lifelonglearner: He or she practises scien-tific clinical decision-making. He orshe is committed to continuingprofessional development andquality assurance. In essence, he orshe is committed to continuing life-long learning and the conduct ofresearch.
★ Community leader: He or she goesbeyond the four walls of the clinicand hospital by being involved incommunity issues such as environ-mental protection, the campaignagainst smoking, responsible par-enthood, child survival and safemotherhood and other issues withan impact on the community. Bymoving people to support a worthy
On the other hand, the Depart-ment pioneered residency trainingin family medicine. It also intro-duced various innovative curricu-lar additions such as behaviouralscience, family systems theory,counseling, hospice care, evidence-based family medicine and familywellness.
Together, the Academy and theDepartment have guided thegrowth of Filipino family physi-cians towards not only taking careof the family but using the inherentstrength of the Filipino family inaddressing their health needs.
Indeed, the family continues toplay a big role in the life of everyFilipino. The family is not only thesmallest unit of society and thecentre of human development, butis also the top priority in the hier-archy of needs of Filipinos. Withvarious challenges from urbaniza-tion, industrialization, increasingmigration of Filipino workers,psychosocial problems, mentalhealth concerns and the traditionalscourge of infectious diseases andlifestyle-related diseases, Filipinofamilies more than ever need thefamily care a Filipino family physi-cian provides.
But this care should be made inconsonance with the ongoingchanges occurring in the country’shealth care system. Family physi-cians should not just contribute tohealth reforms, but should be driv-ers of reforms. And as the five-starphysician, as espoused by both theAcademy and the Department,family physicians have contributedto health reforms.
The five-star family physicianInspired by the five-star doctordescribed by the World HealthOrganization as a care provider,
Introduction
The decade of the 90s saw the in-troduction of health care re-
forms in apparent response to thefailure of the health care deliverysystems of several or nearly allcountries to appropriately respondto the health needs of the people.Ranging from the provider/pur-chaser split in the United Kingdomto the Bamako Initiative, the userfees revolution and the rise of“managed care” in the UnitedStates, health reforms envelopedthe whole globe. And the Philip-pines was no exception.
The idealism of their purposeand the difficulty of their imple-mentation characterize health carereforms in the Philippines. Fromthe devolution of primary healthservices to local government units(LGUs) in 1992 to the institution-alization of a national healthinsurance programme in 1995 andup to the present, the country’shealth care system has been in fluxas various stakeholders strive toidentify new roles in the system.And in this flux, Filipino family phy-sicians have played and shouldcontinue to play the role of driversto make the reforms work.
The Filipino family physicianand the familyThe Philippine Academy of FamilyPhysicians and the Department ofFamily and Community Medicineof the University of the Philippinesled the development of the field offamily medicine in the Philippines.The Academy organized continu-ing medical education for familydoctors, introduced a system ofevaluation and accreditation ofmembers, and instituted a systemof evaluating and accrediting resi-dency programmes.
TOWARDS UNITY FOR HEALTH, APRIL 2000 ■ 27
FAMILY PRACTICE
cause, he or she becomes a socialmobilizer.
And in these five roles, familyphysicians have contributed andwill continue to contribute tohealth reforms in the Philippines.
Family physicians and healthreformsThe devolution of health care serv-ices to local government units ledto the need for new skills for boththe rural health physician and thedistrict hospital physician. Drivenby the five-star philosophy, severalgraduates of the Department andthe other family medicine resi-dency training programmes nur-tured by the Department havebecome rural health physicians.The Department also trains and en-hances the professional growth ofthese doctors. And with the Acad-emy, which has become a sort ofmother professional association ofthese doctors, devolution has beensustained.
Devolution can fail if the serviceproviders cannot provide the serv-ices expected from them. The five-star family physician have shownthat they can fulfil the needs ofdevolution. The continuing chal-lenge is for the family physician bethe health service provider orimpart the five-star philosophy tothe non-family medicine serviceprovider.
The national health insuranceprogramme is a recently imple-
mented policy that is presentlysuffering growing pains.
Before family physicianshad played a major role inthe programme, experi-ence from other countrieshad shown the very crucialrole of family physicians to
the success of a nationalhealth insurance programme.
The institutionalization of familyphysicians as gatekeepers shouldbe strongly advocated.
The growing acceptance oftraditional and/or alternativemedical modalities in the countryhas led to the passage of a lawgiving them tacit admission. As themedical field that looks beyond thebiomedical model and takes socialand cultural considerations intoaccount, family medicine can bestlead the integration of traditionaland/or alternative medicine. It isalso in the position to preventabuses that may accompany thesemodalities.
In the end, as family physiciansgrow into their roles as five-starphysicians in the care of the Fili-pino family, they will contribute tohealth reforms in the country. Theywill be drivers of reform. Consist-ency with the five-star physicianrole will ensure that this contribu-tion and impetus lead to a moreresponsive health care system forFilipinos. ■
References● Developing standards in familymedicine. Manila, Philippine
Academy of Family Physicians,1979.
● Competencies of family physi-cians. Manila, Philippine Academyof Family Physicians, 1983.
● Competencies of family physi-cians, 2. Manila, Philippine Acad-emy of Family Physicians, 1999.
● Strategic action development plan.Manila, Philippine Academy ofFamily Physicians, 1995.
● Making medical practice andmedical education more relevant topeople’s needs: the contribution ofthe family doctor. Report of theWHO–WONCA (World Organizationof Family Doctors) conference 6–8November 1994, London, Ontario,Canada. Geneva and Hong Kong,1995 (available on request fromDivision of Organization of HealthServices Delivery, World HealthOrganization, 1211 Geneva 27,Switzerland).
● Social reform agenda: winning thefuture. Manila, Republic of thePhilippines, 1996.
Dr Leopando is Associate Professor andChair, Department of Family and CommunityMedicine, College of Medicine and PhilippineGeneral Hospital, University of the Philip-pines; Regional Vice President for AsiaPacific, World Organization of Family Doctors;and Immediate Past President, PhilippinesAcademy of Family Physicians.
Dr Banzon is Clinical Associate Professor,Department of Family and CommunityMedicine, College of Medicine and PhilippineGeneral Hospital, University of the Philip-pines. Both authors can be contacted at:Department of Family and CommunityMedicine; College of Medicine and PhilippineGeneral Hospital; Taft Avenue, Manila 1100,PHILIPPINES (telephone: +632 5232358;e-mail: [email protected]).
Coming soon
Available from May 2000 will be the seventh edition of WHO’s World directoryof medical schools: xiv + 441 pages, ISBN 92 4 150010 7 (WHO Order No.1157268). The Directory contains information on 1641 medical schools in157 countries. Anticipated prices will be: CHF 45.00, USD 40.50; the price indeveloping countries will be CHF31.50. Addresses of national WHO distributorscan be requested from <[email protected]> or can be found on the WHOpublications electronic catalogue Web pages: <http://www.who.int>. ■

28 ■ TOWARDS UNITY FOR HEALTH, APRIL 2000
FAMILY PRACTICE
Dr Daniel J. Ostergaard
Making medical practice and medicaleducation more relevant to people’s needs:the contribution of the family doctorDaniel J. Ostergaard, American Academy of Family Physicians, Kansas City
Medical meetings held through-out the world frequently pro-
duce voluminous proceedings thatare widely distributed and in-frequently read. When a meetingproduces a document that is ex-traordinarily widely used and help-ful towards meeting the originalgoals of the conference, there isreason to take note. A workingpaper of the World Health Organi-zation and the World Organizationof Family Doctors entitled Makingmedical practice and educationmore relevant to people’s needs: thecontribution of the family doctor issuch a document. Indeed, thisdocument and the initiatives thathave resulted from its publicationhave done more towards the devel-opment of the family doctorthroughout the world than has anyprior document.
A historical eventThe preamble to the executivesummary of this document in-cludes the following statement:
To meet people’s needs, funda-mental changes must occur inthe health care system, in themedical profession and in medi-cal schools and other educa-tional institutions. The familydoctor (general practitioner/family physician) should have acentral role in the achievementof quality cost-effectiveness andequity in health care systems. Tofulfil this responsibility, thefamily doctor must be highlycompetent in patient care andmust integrate individual andcommunity health care. The co-operation between the WorldHealth Organization (WHO) andthe World Organization of Fam-
progress related to these strategieswas to be composed, and edited byDr Mark Rivo of the USA.
The life of this document hasbeen dynamic rather than dor-mant. Nearly 10,000 copies havebeen printed—in English, Spanish,Portuguese, Chinese and most re-cently in Russian. The documenthas been distributed to all minis-tries of health and all medicalschools of all countries of the world.It has been used in personal meet-ings between representatives offamily practice organizationsthroughout the world as they havemet with ministries of health in dis-cussions of health care reform andthe role of the family doctor to-wards improvement of health forall. The individual recommenda-tions have assisted health careplanners and medical educators inthe development of specific plansfor the training of family doctors inmany countries.
Following the original WHO/WONCA conference in the autumnof 1994, additional regional and“specific topics” conferences havebeen held in Argentina, Cuba,Korea, Switzerland and the UnitedKingdom. The conference in Argen-tina, entitled “Family medicine andhealth care reform in the Americas”,
ily Doctors (WONCA) towardsthis vision is historic.
From November 6 to 8, 1994,WONCA and WHO convened a stra-tegic action forum in London,Ontario, Canada, involving 60government health officials, medi-cal educators, family doctors andpublic representatives from aroundthe world. The purpose of the meet-ing was to identify specific actionsto make health care, medical prac-tice and medical education morerelevant to people’s needs, therebycontributing to the health-for-allgoals.
The 100-page report of thismeeting analyses challenges forhealth care systems, medical prac-tice and medical education. Itemphasizes a vision of changes inthe health structures of all thecountries in the world. The fifth andfinal chapter contains 21 specificand forceful recommendations foraction to build a publicly respon-sive health care and medicaleducation system. These recom-mendations contain suggestionsfor action by medical schools,medical associations, governmentsand many other relevant bodies.
Global follow-upThe planning and editorial com-mittees that worked on this jointWHO/WONCA working paper de-termined from the beginning thatthis would not be a project or exer-cise that would become dormant inthe near future. Strategies for im-plementing the 21 recommenda-tions outlined in chapter 5 weredeveloped, including additionalkey conferences, new initiatives,special reports and survey-relatedactivities. A detailed explanation of

TOWARDS UNITY FOR HEALTH, APRIL 2000 ■ 29
FAMILY PRACTICE
Seeking new ways to employ GPs:Can an oil-spots strategy succeed?Saeed Asefzadeh, Qazvin University of Medical Sciences
resulted in the Declaration of Bue-nos Aires, which adapted many ofthe original 21 recommendationsfor appropriate use in Central andLatin America as well as the IberianPeninsula.
In 1995 the World Health Assem-bly adopted resolution WHA48.8,“Reorientation of medical educa-tion and medical practice for healthfor all”, and called upon WHO andits Member States to undertake co-ordinated reform of health careand, necessarily, education of phy-sicians and health care workers.This resulted in several reports, sur-veys and publications, most oftencoordinated by the WHO Depart-ment of Organization of HealthServices Delivery (OSD).
A major survey currently underway is the “World survey of familymedicine and general practice”,being undertaken by WHO andWONCA. This survey will assess
development and status of generalfamily medicine and its contribu-tion to health development world-wide.
That a report written nearly fiveyears ago has enduring and ex-panding impact is a tribute not somuch to its framers but to the prin-ciples and philosophies it articu-lates and the recommendations itmakes. Ministries of health, profes-sional associations and medicaleducation establishments through-out the world have used these prin-ciples and recommendations todefine and refine their plans forhealth care system reform andchange in medical education.
Perhaps eventually the originaldocument will be lost in favour ofthe refinements, updated reports,translations into other languagesand permutations tailored to meetthe needs of specific countries. If so,all is well if there is continued
progress towards encouraging thecontribution of the family doctor inmaking medical practice and edu-cation more relevant to people’sneeds. ■
Dr Ostergaard is Vice President, Internationaland Interprofessional Activities, AmericanAcademy of Family Physicians; 8880 WardParkway; Kansas City, Missouri 64114-2797(telephone: +816 333 9700; fax: +816 3332237; e-mail: [email protected]).
● Making medical practice andeducation more relevant to people’sneeds: the contribution of the familydoctor is available in English onrequest from the Department ofOrganization of Health ServicesDelivery, World HealthOrganization, 1211 Geneva 27,SWITZERLAND or from the WorldOrganization of Family Doctors,Locked Bag 11, Collins Street EastPost Office, Melbourne, Victoria8003, AUSTRALIA. For copies inChinese, Portuguese, Russian orSpanish, please contact WONCA.
Medical workforce mismatch
O nce again, the old story ofimbalanced production of doc-
tors was experienced in Iran, as inmany developing countries.(1) Thenumber of medical facultiesjumped from 9 in 1975 to more than54 in 1995. Accordingly, the numberof medical students rose from 6099to 40 162. This represented a 10%growth rate in production of doc-tors per year. In 1998, more than37 700 GPs and 18 300 specialistswere working in the market; it isestimated that the total number ofphysicians will reach 70 000 by theyear 2002.(2)
The policy-makers’ primary goalwas to produce enough doctors tomeet health needs at the nationallevel, but their target was only the
raw index of one doctor per 1000people, irrespective of the culturalconsiderations, socioeconomicfactors, the inefficient health serv-ice system that cannot absorb theoverflow of doctors and the future“changes”, etc. Studies have shownthat the quality of medical educa-tion has been sacrificed to quantity.The medical faculties have soughtprimarily to produce more doctors,but many universities still lack theexpert human resources to educatethem.
Although the universities ofmedical sciences are also responsi-ble for the delivery of health serv-ices to the people, they cannotemploy their own products—theyoung GPs—even in their ownvicinity. The labour market for GPs
is being saturated even in the moredeprived areas.
General constraintsMajor factors leading to the abovesituation may be as follows:
● People do not have a regularpersonal physician they know andwith whom they have sustained arelationship over time. They oftenapproach any accessible doctor,whether a specialist or a generalpractitioner. Only a few patients arereferred by doctors.● The health of families is notaddressed by both the health sys-tem and the family members them-selves.● People are not directed to theappropriate medical services, nor

30 ■ TOWARDS UNITY FOR HEALTH, APRIL 2000
are they well enough in-formed to approach theappropriate services ontheir own.● The coming change inneeds, which directlyreflects the effectivedemand for health serv-ices, is overlooked.● The economic factorsaffecting demand forhealth services are notnoted, but these play animportant role in determining thefamily’s demand basket.● Medical education is not yet suf-ficiently community-oriented.● Health insurance organizationsare not well enough engaged inmedical and preventive services tosupport the demand.● Doctors compete for patients toincrease their income.
Educating societyThe above facts were discussedwithin our university. It was con-cluded that the major problem inhealth is the cultural habits of thepeople. People should be encour-aged to use doctors’ services appro-priately. But changing people’sattitudes towards regarding GPs asfamily doctors is difficult and maynot happen in the short run.(3)Moreover, GPs have not beentrained to function in the role offamily doctors.
We must therefore act on bothsides of the supply/demand equa-tion:
● Develop family physicians.
● Change people’s use of doctors.
But how can these be done? Ourresources are limited and legal for-malities constrain us.
We decided to use what might becalled an oil-spot strategy: wewould start in one place and spreadout from there, much as an oil spotspreads on a surface.
With this strategy in perspective,we surveyed the communities inthe Qazvin region—a developingcity of 600 000—in order to findsome areas we could influence. We
also tried to identifycompetent youngGPs to be trained asfamily doctors.
We decided to pro-ceed cautiously. It isexpected that thefamily doctors will beresponsible for thehealth of whole fami-lies and will encour-age family membersto seek health serv-
ices. We believe that word-of-mouth contact will be anefficient and effective means ofinfluence, once people receive sat-isfactory services from the familydoctors. We hope that by this strat-egy the GPs will be working in theright direction and that at the sametime the demand for medicalservices will be reoriented appro-priately.
How will these expectations bemet? The future will tell us. ■
References1. Bankowski Z, Fülop T. Health
manpower out of balance:conflicts and prospects.Highlights of the AcapulcoConference. Geneva, Council forOrganizations of MedicalSciences, 1987.
2. Marandi SA et al. [Health in theIslamic Republic of Iran] Tehran,World Health Organization/United Nations Children’s Fund,1999.
3. Asefzadeh S. Rethinking thehealth services insurance system:the family doctor and familynurse in a new model for IranianRailway households. EasternMediterranean Health Journal,1999, 5(2) [in press].
Dr Asefzadeh is Director of Research Centrefor Students’ and Graduates’ Progress,Department of Research, Qazvin University ofMedical Sciences, Qazvin, IRAN (fax: +9828136007; e-mail: [email protected]).
FAMILY PRACTICE
Dr Saeed Asefzadeh
Lessons learnt at WHO by aprospective US family physicianMichael Coffey, University of Cincinnati Collegeof Medicine
This article was contributed by Michael Coffey, who wrote it during a nine-month internship in the Department of Health Systems (now the Department ofOrganization of Health Services Delivery) of the World Health Organization. Heis now finishing his fourth year of medical school at the University of CincinnatiCollege of Medicine.
As my internship at WHO drawsto a close and I prepare to re-
turn to the USA to finish medicalschool, I find myself reflecting onall that I have learned this year.During the eight months I’ve spenthere, I have come to recognizesome important aspects of a modelhealth care system and the ways inwhich WHO is trying to make thismodel a reality. My experience thisyear working on various projectsand listening to visiting speakershas allowed me to compare the US
system to this model, and to envi-sion the type of system in which Ihope to practise after I become adoctor.
Through my involvement in the“Towards unity for health” (TUFH)project, I have seen the need to linkthe health care of communities andindividuals. TUFH seeks to studyand promote worldwide efforts tocreate unity in health services or-ganizations, particularly throughthe integration of medicine andpublic health. It also advocates the

TOWARDS UNITY FOR HEALTH, APRIL 2000 ■ 31
FAMILY PRACTICE
at WHO’s broad definition of healthas “a state of complete physical,mental and social well-being andnot merely the absence of diseaseor infirmity”. My belief in the im-portance of social dimensions has,in part, inspired me to pursue acareer in family practice.
By working with the socialaccountability model put forth byDr Charles Boelen, WHO, andDr Jeffery Heck, University ofCincinnati, I have seen that healthcare providers and organizers needto promote quality of care. DonnaShalala, the US Secretary of Healthand Human Services, recently em-phasized the importance of thesetwo aspects when she spoke in apresentation at WHO about the Ad-visory Commission on ConsumerProtection and Quality in theHealth Care Industry. This commis-sion, which brought together con-sumers, businesspeople, healthplan managers, doctors and gov-ernment officials to talk aboutquality, came to a consensus thatthe USA needs a “national commit-ment to quality improvement”. It
also recommendedthat “steps should betaken to ensure thatcomparative informa-tion on health carequality is valid, reli-able, comprehensible,and widely available inthe public domain”.
My internship atWHO has been bothformative and instruc-tive; I want to build on
the research and health systemsexperience I have gained this yearand become an academic familyphysician. I feel that in this type ofposition I can best practise the typeof medicine I have come to view asideal: one that embodies a balanceof research, public health and high-quality patient care. ■
Michael Coffey can be reached at Universityof Cincinnati College of Medicine, Office ofStudent Affairs, 231 Bethesda Avenue,Cincinnati, Ohio 45267, USA(e-mail: [email protected]).
formation of active partnershipsbetween the different health carestakeholders. I agree with its tenetthat governments, professionalassociations, academic institutionsand provider organizations likehealth maintenance organization(HMOs) need to share a commongoal to act on priority healthconcerns of individuals andpopulations.
I have also seen that the merg-ing of individual and communitycare is an important component ofcommunity-oriented primary care(COPC), a health-planning processthat blends primary care and pre-ventive measures with epidemiol-ogy to determine factors that affectthe health of the community. COPCaims to define the relevant issuesfacing a community, prioritizethose issues, develop and imple-ment strategies to address thepriorities, and evaluate the strate-gies to continually make the proc-ess better and more cost-effective.At my own medical school, thisconcept is taught and used in theDepartment of Family Medicine.Seeing the model’ssuccess in a large uni-versity group practicehas been an importantpart of my training andhas helped me definethe type of practice Iwant to have.
In studying healthsystems of variouscountries from aroundthe world, I have seenthe need for a balancebetween biomedical and socialdimensions in health programmingand practice. The US systemalready has a strong focus on bio-medical dimensions, but its deci-sion-makers in health care need toput more emphasis on the socialones. Physicians especially shouldnot neglect these aspects, becausethere are many social problems—such as alcoholism, stress anddepression—that have a greatimpact on a person’s well-being, particularly when one looks
Michael Coffey
PublicationsThe publications listed below arerecommended as particularly relevant tothe “Towards Unity for Health” initiativeand to coordinating changes in healthservices and health professions practiceand education. Some of them can beobtained free of charge.
Due to the limited supply and for thesake of better dissemination, WHO willgive preference to filling requests for itspublications from heads of institutions,organizations and programmes, with theexpectation that they will be madeaccessible and available to large groupsof readers.
■ World directory of medical schools.Seventh edition. Geneva, World HealthOrganization (available for sale in spring 2000from Department of Marketing and Dissemi-nation, World Health Organization, 1211Geneva 27, Switzerland).
■ Improving the social responsiveness ofmedical schools: Proceedings of the 1998Educational Commission for Foreign MedicalGraduates/World Health OrganizationInvitational Conference, Barcelona,12–14 March 1998. Academic MedicineSupplement, August 1999. Available fromAssociation of American Medical Colleges,2450 N Street, N.W., Washington, DC 20037,USA.
■ Physician funding and health caresystems: an international perspective.Summary of the conference hosted by theWorld Health Organization (WHO), WorldOrganization of Family Doctors (WONCA)and Royal College of General Practitioners(RCGP), 12–13 December 1997, St John’sCollege, Cambridge. London, RCGP, 1999.Available from RCGP, 14 Princes Gate, Hydepark, London, SW7 1PU, UK.
■ Making medical practice and medicaleducation more relevant to people’s needs:The contribution of the family doctor. Reportof the WHO-WONCA (World Organization ofFamily Doctors) conference 6–8 November1994, London, Ontario, Canada. Geneva andHong Kong, 1995, in Chinese, English,Portuguese, Russian and Spanish. Availableon request from Department of Organizationof Health Services Delivery, World HealthOrganization, 1211 Geneva 27, Switzerlandand World Organization of Family Doctors,Locked Bag 11, Collins Street East PostOffice, Melbourne Victoria 80, Australia.
PUBLICATIONS
continued page 32 ➤

32 ■ TOWARDS UNITY FOR HEALTH, APRIL 2000
■ Tuberculosis control and medical schools.Report of a workshop convened by the WorldHealth Organization, 29-31 October 1997,Rome, Italy. Geneva, World Health Organiza-tion, 1998 (unpublished document WHO/TB/98.236; available on request from Departmentof Organization of Health Services Delivery,World Health Organization, 1211 Geneva 27,Switzerland).
■ Pelc I, Cassiers L (eds). La faculté demédecine et le médecin praticien du XXIèmesiècle. Journées d’Etudes internationales.Organisée par l’Organisation mondial de laSanté et la Conférence internationale desDoyens, 9–12 avril 1996, Bruxelles.Bruxelles, Fondation pour l’Etude et laPrévention des Maladies de Civilisation, 1998.
■ Doctors for Health. A WHO global strategyfor changing medical education and medicalpractice for health for all. Geneva, WorldHealth Organization, 1996 (unpublisheddocument WHO/HRH/96.1, in Chinese,English, French and Spanish; available onrequest from Department of Organization ofHealth Services Delivery, World HealthOrganization, 1211 Geneva 27, Switzerland).
■ Boelen C, Heck J. Defining and measuringthe social accountability of medical schools.Geneva, World Health Organization, 1995, inEnglish, French, Spanish (unpublisheddocument WHO/HRH/95.7; available onrequest from Department of Organization ofHealth Services Delivery, World HealthOrganization, 1211 Geneva 27, Switzerland).
Coming up soon■ Towards Unity for Health. Working paper.World Health Organization internationalconference, 10–13 August 1999, Phuket,Thailand. Geneva, World Health Organization(available in autumn 2000 in English andFrench from Department of Organization ofHealth Services Delivery, World HealthOrganization, 1211 Geneva 27, Switzerland).
■ Towards Unity for Health. Challenges andopportunities for partnership in healthdevelopment. Proceedings of the WorldHealth Organization international confer-ence, 10–13 August 1999, Phuket, Thailand.Geneva, World Health Organization (availablein autumn 2000 from Department of Organiza-tion of Health Services Delivery, World HealthOrganization, 1211 Geneva 27, Switzerland).
■ Towards Unity for Health. Monograph ofcase studies. Geneva, World Health Organiza-tion (available in autumn 2000 from Depart-ment of Organization of Health ServicesDelivery, World Health Organization, 1211Geneva 27, Switzerland). ■
PUBLICATIONS
Dear Reader,
Towards Unity For Health: Coordinating Changes in Health Services andHealth Professions Practice and Education is the World Health Organizationnewsletter that succeeds Changing Medical Education and Medical Practice,which was published from June 1992 through December 1998.
This new newsletter reflects an enlarged scope, consistent with WHO’spolicy for developing new alliances and partnerships among educationalinstitutions, health professions, health managers, policy-makers andcommunities to ensure sustainable improvement of quality, equity,relevance and cost-effectiveness in health interventions. Topics relative tohealth professions education and practice will continue to be addressed,along with other issues in health services development and healthsystem changes.
If you wish to continue receiving this newsletter, please complete and returnthe form below by 1 July 2000 to:
World Health OrganizationAttention: Mrs. S. Bernasconi, OSD1211 Geneva 27SWITZERLAND
or let us know by fax: +41 22 791 4747 or E-mail: <[email protected]>.Please note that Towards Unity for Health will also be available in both .pdfand text-only formats from the WHO Web site: <http://www.who.int>.
I hope this new WHO newsletter will be as well received as ChangingMedical Education and Medical Practice, and that through topics of sharedinterest, collaborative links will be strengthened worldwide.
Yours sincerely,
Dr Charles BoelenEditor-in-Chief, Towards Unity for Health
Please note: The newsletter Towards Unity for Health will systematically besent to all WHO Representatives, WHO regional offices and WHO collaborat-ing centres and to international NGOs in official relations with WHO. Theserecipients therefore need not confirm their wish to continue receiving thenewsletter. ■
➤ continued from page 31
Yes, I wish to continue receiving the WHO newsletter Towards Unity for Health
Full name:(please underline family name)
Position:
Institution name:
Postal address: Street P.O. Box
City, State
Country
Postal code
Fax:
Telephone:
E-mail:
Please return to: World Health OrganizationAttention: Mrs S. Bernasconi, OSD20, Avenue Appia1211 Geneva 27SWITZERLAND
✁For your urgent attention, please

TOWARDS UNITY FOR HEALTH, APRIL 2000 ■ 33
SOCIAL ACCOUNTABILITY
Are Sri Lankan medical schoolssocially accountable?Nimal D. Kasturiaratchi, Faculty of Medicine, University of Peradeniya
Such words from a per-son who is a politician—arepresentative of the laypublic—and the personwho bears considerableresponsibility for thehealth of the nationshould have attracted theattention of all Sri Lankanhealth professionals. Theminister’s point was thatphysicians should askthemselves how they respond topeople’s health needs. He was ask-ing the medical profession to becreative, pragmatic, courageousand determined to venture outsidethe usual boundaries. (2)
The concept of socialaccountabilityVenturing outside the usualboundaries can yield socialaccountability, a concept based onthe four values of relevance, qual-ity, equity and cost-effective-ness.(3) The minister’s plea was alsoa reference to a particular valueportfolio in the country’s healthscene.
In the scenario described by theminister, quality of care seemed
to be preferred toequity of servicesrendered. Andthere was lessconcern with thecost-effectivenessof the services and
overall relevance inplanning human
resources deploy-ments. In sum, there
seemed to be a bias in the overallaccountability by the medical edu-cation system in responding tosocietal needs demonstrated by theskewed emphasis of certain values.
The concept of social account-
An international meeting, “To-wards Quality in Medical Edu-
cation: Partnerships for Action”,was held in Kandy, Sri Lanka, tomark the 25th anniversary of theWHO Regional Teacher TrainingCentre (Medical Education Unit) atthe Faculty of Medicine, Universityof Peradeniya. The Minister ofHealth of Sri Lanka used the oppor-tunity to identify what he called“some of the issues in medical edu-cation that need consideration bythe medical professionals in SriLanka”.
While complimenting the excel-lent technical training offered bymedical schools in the country, theminister was critical of the medicalprofession for its lack of socialresponsibility. He referred specifi-cally to the failure of the PostGraduate Institute of Medicine toformulate a policy regardingspecialist requirements for thecountry, as well as to the reluctanceof doctors to serve the underservedareas, com-partmentalizing thehealth system by marginalizing the
Ayurveda medical system and theinability of the educational systemto recognize the pedagogical im-portance of non-university healthpersonnel in the training of physi-cians. (1)
ability as applied tomedical educa-tional institutionsentails that service,research and educa-tion rendered by theinstitution incorpo-rate the four valuesmentioned above.The traditional triad(education, serviceand research) of
functions of a medical facultyshould, in order to demonstratesocial accountability, be evaluatedby the extent to which they takerelevance, quality, equity and cost-effectiveness into account.
All Sri Lankan medical schoolsare government-owned and areunder the Ministry of Higher Edu-cation. However, they provide valu-able service functions at assignedteaching hospitals, furnish exper-tise to the general health care sceneand are involved in research and inundergraduate and postgraduateteaching. As institutions, however,the extent to which they move outof this traditional agenda to activelyengage in issues of securing equity,promoting cost-effectiveness in theprovision of health care to desig-nated populations or are involvedin sustaining and promoting qual-ity is rather questionable.
Internal and external factorsThis observable “closed” nature ofmedical schools is determined bymany factors. Within medicalschools two key features seem toperpetuate the lack of initiative tobreak away from the traditionalteaching contexts and involve thestudents in more active service andresearch performed by the teacherswithin the social accountabilityparadigm.
Dr Nimal D. Kasturiaratchi

34 ■ TOWARDS UNITY FOR HEALTH, APRIL 2000
One of these is the workload ofundergraduate teaching resultingfrom increased intake of studentswithout considerable expansion intrained human resources. The sec-ond is mostly attitudinal, in thatmost teachers shy away fromengaging in collaborative workwith external agencies that are alsocomponents of the national healthsystem.
Similarly, many factors externalto university environments limitthe involvement of a given medicalfaculty with the regional andnational level, servicing, planning,monitoring and evaluation ofhealth care delivery. Placingmedical faculties under the respon-sibility of the Ministry of HigherEducation makes accountabilitybeyond the patient care operatingwithin the private space almostimpossible.
Although the health care deliverysystem in Sri Lanka is decentralized
to the provinces, the universitiesare national institutions. Althoughthe health system has been decen-tralized, the teaching hospitals arenot, and they come directly underthe health ministry of the centralgovernment.
Public accountability for healthin a given province where there is amedical faculty is therefore tornamong the university, the provin-cial health authority and theMinistry of Health of the centralgovernment. Within this complex-ity, invitations for the university’sinvolvement in health as an ac-countable agency are unrealistic. ■
References1. De Silva S. Inaugural address. In:
Proceedings of the internationalconference on Towards Quality ofMedical Education—Partnershipsfor Action. December 1998.Peradeniya, Sri Lanka.
2. Doctors for health: a WHO globalstrategy for changing medicaleducation and medical practicefor health for all. Geneva, WorldHealth Organization, 1996(unpublished document WHO/HRH/96.1; available on requestfrom Department of Organiza-tion of Health Services Delivery,World Health Organization, 1211Geneva 27, Switzerland).
3. Boelen C, Heck J. Defining andmeasuring the social account-ability of medical schools.Geneva, World Health Organiza-tion, 1995 (unpublished docu-ment WHO/HRH/95.7; availableon request from Department ofOrganization of Health ServicesDelivery, World Health Organiza-tion, 1211 Geneva 27, Switzer-land).
Dr Kasturiaratchi is Director, MedicalEducation Unit, Faculty of Medicine,University of Peradeniya, Peradeniya,SRI LANKA (telephone/fax: +948 388949;e-mail: [email protected]).
SOCIAL ACCOUNTABILITY
After four years as President ofthe Educational Commission
for Foreign Medical Graduates(ECFMG), I have had considerableopportunity to meet with medicaleducators and ministers of healthand to attend international meet-ings on a variety of subjects. I havealso visited several medical schoolsabroad and met with the adminis-trators and faculty.
The diversity among schools inadmissions processes, educationalmethodology and evaluation isquite interesting. I am also im-pressed by the commonality ofmedical educators’ concernsworldwide about the best prepara-tion of those who will care for theill members of society and prevent
schools have included instructionalexperiences in remote, sparselypopulated areas served by a districthealth officer, clinic or hospital farfrom the high technology andspecialist-oriented universityhospital. Delivery of health care topeople residing in densely inhab-ited urban locations is part of theeducational experience in somemedical schools.
● Another topic under discussionis how the medical school can bestserve its immediate community.Most schools provide care to thesick and injured. Attention by theacademic faculty to illness preven-tion and public health may requirecollaboration with local officials ingovernment, health and education.
illness and injury to others. Facul-ties seem committed to enrichingand enhancing their educationalprogrammes to keep them contem-porary.
Common issues for medicaleducators include the following:
● The careful assessment of thelocal, country or regional healthneeds of those whom medicalschool graduates will serve. The re-sults of this kind of analysis can betranslated back to the medicalschool and woven into the fabric ofthe undergraduate and postgradu-ate curricula.
● Preparing medical students forthe environment in which theywill practise as physicians. Some
QUALITY ASSURANCE IN EDUCATION
Global issues for medical educatorsNancy E. Gary, Educational Commission for Foreign Medical Graduates, Philadelphia

TOWARDS UNITY FOR HEALTH, APRIL 2000 ■ 35
QUALITY ASSURANCE IN EDUCATION
The faculty’s conduct of biomedi-cally relevant research can alsoyield results that will benefit notonly the local community but alsothe world’s population.
● Internationally, medical educa-tors are working to enhance theevaluation of students’ acquisitionof knowledge, clinical judgement,behaviour and skills to betterassure their preparation to be phy-sicians.
Finally, I have observed a world-wide interest in discussion of thematter of globalization of medical
education, perhaps through thesetting of some internationalstandards or an accrediting processthat would require establishment ofstandards for the educational pro-gramme. The diversity in medicaleducation and differences amongcountries, regions and hemi-spheres would have to be taken intoaccount. Most importantly, theneeds of the people to be servedmust be paramount. Several coun-tries have been enhancing theirsystems for accreditation in recentyears. The ECFMG has providedconsultation to Malaysia to assist
that country as it worked towardsenhancing its system of healthprofessional school accreditation.Perhaps it is time to formalize thesediscussions about internationalstandards and accreditationthrough conferences with globalrepresentation. ■
Dr Gary is President and Chief ExecutiveOfficer, Educational Commission for ForeignMedical Graduates, 3624 Market Street,Philadelphia, Pennsylvania 19104-2685, USA(telephone: +1 215 823 2101; fax: +1 215 3868151) and Dean Emeritus and Professor ofMedicine, Uniformed Services University ofthe Health Sciences, F. Edward Hébert Schoolof Medicine, Bethesda, Maryland.
Quality assurance and accreditation:Where do they meet?Alistair Stewart, University of Dundee
Introduction
Accreditation has been an issuein medical and other health
professions education for longerthan that of quality assurance, andcontinues to be very important,particularly as ideas in globalaccreditation and standards areexplored. Quality assurance hasassumed a new importance in re-cent years as governments aroundthe world have held health profes-sions schools accountable for the
professional bodies must, ofcourse, concern themselves withthe curriculum, the teaching andlearning environment, and the as-sessment of students. With respectto the curriculum, they will want toassure themselves that it is up todate, but the criteria for determin-ing this could be quite subjective.With respect to the teaching andlearning environment, they willwant to assure themselves that thefacilities are good, that the student/staff ratio is acceptable, and thatopportunities for learning extendbeyond the confines of the institu-tion, particularly to clinicalsettings. With respect to the assess-ment of students, they will want toassure themselves that the passmarks are not too low and that thepass rate is of an acceptable level.
The quality assurance processQuality assurance has connotationof “fitness for purpose”, so it is ap-propriate to ask whether the teach-ing and learning in an institutionare equipping the students to meetthe requirements of their future
quality of preparation of doctors,nurses and others [endash] particu-larly those who, it is claimed, arebeing trained to meet the healthcare needs of the society they willserve.
The processes of accreditationand quality assurance are similar,and many institutions object towhat appears to be duplication ofeffort in satisfying the requirementsof both. Surely it must be possibleto develop a model that wouldallow both processes to be under-taken and the requirements of eachto be met, without duplication ofeffort?
The accreditation processIn many countries accreditation ofcourses and, by implication,professional standards for healthprofessionals are, by statute, the re-sponsibility of the respective pro-fessional bodies. Professionalbodies tend to be concerned pri-marily with the maintenance ofstandards, since the reputation ofthe profession as a whole is at stake.
To be able to assess standards,Dr Alistair Stewart

36 ■ TOWARDS UNITY FOR HEALTH, APRIL 2000
employment. In other words, as faras medical and other health profes-sions education is concerned, arethese students going to be able todeliver the kind of health care thatsociety needs and expects?
The quality assurance process istherefore concerned not only withteaching and learning; it is con-cerned with an institution’s ap-proach to what is being learned,how it is being learned, and whetherit has been learned. The QA pro-cess is concerned with the curricu-lum and the procedures that aregone through in determining whatthat curriculum should be; with theteaching and learning environmentand how the learning opportunitiesprovided will enable the student toacquire the knowledge, skills andattitudes that underpin thecompetences required for the per-formance of health care tasks inprofessional practice; and with theassessment of students to ensurethat they are, in fact, able to usethese competences in practice forthe benefit of society.
In the process of quality assur-ance, an institution must be able to
demonstrate that it has an organi-zational structure conducive to theongoing monitoring and evaluationof its courses; analysing perform-ance indicators; obtaining feed-back from students on theirlearning experiences; obtainingfeedback from the employers ofgraduates on the appropriatenessof the training received; analysingexternal examiners’ reports;accepting and responding to exter-nal inspection from relevant pro-fessional bodies; and, within aframework of staff appraisal anddevelopment, offering training tostaff in educational issues.
So what’s the difference?The processes of accreditation andquality assurance are very similar.Each is concerned with the curricu-lum, with teaching and learning,and with assessment. The differ-ence is essentially in the perspec-tive from which these issues areanalysed and evaluated. Accredita-tion is concerned primarily withstandards—but standards in rela-tion to what? Quality assurance isconcerned, inter alia, with fitness
for purpose—but what purpose?This is where the respective per-spectives come in. They can bequite different, but they need notbe. Is it beyond the ingenuity ofman that what a professional bodyis looking for and what a society islooking for can be reconciled?
Active responseAt the Centre for Medical Educationin the University of Dundee, staffand doctoral students are currentlyexploring the relationship betweencurriculum evaluation and qualityassurance and between quality assurance, including total qualitymanagement, and accreditationand credentialing. They are build-ing up expertise that could be ofcrucial interest to health profes-sions teachers around the world ata time when issues such as globalaccreditation are fairly high up onthe agenda. ■
Dr Stewart is Educational Consultant, Centrefor Medical Education, University of Dundee,Tay Park House, 484 Perth Road, Dundee,DD2 1LR, SCOTLAND (telephone: +01382631968; fax: +01382 645748;e-mail: [email protected]).
QUALITY ASSURANCE IN EDUCATION
Credentialing for the health professions:an international nursing perspectiveFadwa A. Affara, International Council of Nurses, Geneva
cation, practice and services (ICN,1986). In 1996 the position was up-dated to take account of the chang-ing health care environment.
For ICN the term regulationrefers to “all of those legitimate andappropriate means—governmen-tal, professional and private—whereby order, consistency,identity and control are brought tothe profession. The profession andits members are defined; the scopeof practice is determined; stand-ards of education and of ethical andcompetent practice are set; and sys-tems of accountability are estab-
lished through these means” (Mad-den-Styles and Affara, 1997). Thus,the concept of credentialing is en-compassed within this definition asit constitutes one major category ofregulatory mechanisms, includingregistration, licensure, accredita-tion and certification.
Current credentialing challengesAs for all health professionals, life-long learning and verified continu-ing competence are necessary toequip nurses for the ever-changingknowledge bases, technologies,roles and settings that characterize
The role of the InternationalCouncil of Nurses (ICN) inregulation
As a global advocate for nursingand health care, the Interna-
tional Council of Nurses has, fromits inception in 1899, defined animportant role in promoting effec-tive regulatory systems. In the early1980s, ICN developed and widelydisseminated its position on regu-lation. The position and accompa-nying guidelines addressed thebroad issues of professional regu-lation, including standards andmodels for regulating nursing edu-

TOWARDS UNITY FOR HEALTH, APRIL 2000 ■ 37
QUALITY ASSURANCE IN EDUCATION
today’s health care en-vironment. Therefore,credentialing mod-els must go beyondensuring initialcompetence. Theymust also assesscontinuing, ad-vanced and specializedcompetence. Moreover,in countries with advancedpractice programmes, which pre-pare nurses for expanded and moreautonomous roles, credentialingcan be and is used to acknowledgeand sanction these enlargeddimensions of practice.
In response to these new de-mands and to the dramatic changesin nursing practice, various govern-mental forms of credentialingare being supplemented withcredentialing developed by thenursing profession itself. Forexample, the American NursesCredentialing Centre (ANCC), asubsidiary of the American Nurses’Association, provides a range of ac-creditation and certification serv-ices. These include accreditation ofcontinuing education providers,and recognition programmes forexcellence in nursing services.According to the ANCC, it has cer-tified 130,000 nurses in specificfields of nursing practice.
In the future, health care provid-ers will increasingly work acrosstraditional job and hierarchicalboundaries. For the nursing profes-sion, the growing demand to prac-tise more autonomously andfunction within multidisciplinaryand interdisciplinary environmentspresents new educational andregulatory challenges, includingpreparation for evolving and lessrestricted scopes of practice thatmay even overlap with those ofother health professionals. Healthprofessionals need to explore to-gether the credentialing policiesand practices that will respond tothe changing face of all health prac-tice, and create credentialingframeworks that promote collabo-rative practice.
The trend toglobalization ofthe economy alsop r e s e n t schallenges forp r o f e s s i o n a l
c re d e n t i a l i n g .Regional treaties,
and organizationssuch as the World
Trade Organization, facili-tate cross-border movement of per-sons and services as well as ofgoods. This development may raisestandards in some jurisdictions, orlower standards or impose inappropriate ones in others. In ad-dition, progress in telecommunica-tion and information technologiesis accelerating the growth oftransborder education and healthcare services. Programme accredi-tation and jurisdictional issuessuch as recognition of qualifica-tions, right to practise and legalliability are emerging and need tobe addressed as globalization takesfurther hold and advanced tech-nologies spread.
Questions related to what stand-ards and whose standards will beapplied, need to be resolved so thatthe free movement of health profes-sionals and health services does nothave a negative impact on the qual-ity and safety of health care serv-ices. Broadly recognizedcredentialsmay become more important infacilitating the transfer of “expertauthority” and practice rights fromplace to place. ICN believes that theglobalization of services is anopportunity for health profession-als to collaborate in developingaccreditation frameworks and
mechanisms for internationallyprovided education and health careservices.
Future directions for credentialing:an ICN perspectiveCurrent credentialing models needto evolve to remain pertinent. Theywill need to demonstrate a numberof characteristics, including:
● the capacity to ensure continuedcompetence, maintenance ofsafe health care practices andongoing relevance and quality ofeducation;
● the ability to provide opportuni-ties for health professionals todemonstrate advanced areas ofexpertise with transferable cre-dentials;
● an open-ended and dynamicstructure able to adapt to thechanging health care environ-ment;
● the capacity for a direct role incredentialing for the professions;
● support for internationalcredentialing services.
ICN is committed to moving inthis direction. If populations are toreceive skillful and knowledgeablehealth care, this must be done inpartnership—within the nursingprofession itself, with other healthprofessionals, with private andpublic health care and educationalagencies and with governments. ■
References● Report on the regulation ofnursing. A report on the present, aposition for the future. Geneva,International Council of Nurses,1986.
● Madden-Styles M, Affara FA. ICNon regulation: towards 21st centurymodels. Geneva, InternationalCouncil of Nurses, 1997.
Dr Affara is Consultant, Nursing and HealthPolicy; International Council of Nurses;3, place Jean-Marteau; 1201 Geneva,SWITZERLAND (telephone: +41 22 908 0100;fax: +41 22 908 0101; e-mail:[email protected]).
Dr Fadwa A. Affara

38 ■ TOWARDS UNITY FOR HEALTH, APRIL 2000
■ WHO headquartersWorld Health Organization
1211 Geneva 27, Switzerland(Telegraph: UNISANTE GENEVA;Telex: 415 416;Telephone: +(022) 791 21 11;Fax: +(022) 791 31 11)
■ WHO regional officesWHO Regional Office for Africa
Temporary address:Parirenyatwa Hospital; P.O. BoxBE 773; Harare, Zimbabwe(Telephone: +(001) 407 733 9244;Fax: +(001) 407 726 5062)
WHO Regional Office for the Americas/Pan American Sanitary Bureau
525-23rd Street, N.W.;Washington, D.C. 20037; USA(Telegraph: OFSANPANWASHINGTON;Telex: 248338;Telephone: +(1 202) 974 3000;Fax: +(1 202) 974 3663)
WHO Regional Office for the EasternMediterranean
P.O. Box 1517; Alexandria 21511, Egypt(Telegraph: UNISANTE ALEXANDRIA;Telex: 54028 or 54684;Telephone: +(203) 48 202 23;Fax: +(203) 48 38 916)
WHO Regional Office for Europe8, Scherfigsvej; DK-2100 Copenhagen(Telegraph: UNISANTE COPENHAGEN;Telex: 15348 or 15390;Telephone: +(45) 3917 1717;Fax: +(45) 3917 1818)
WHO Regional Office for South-EastAsia
World Health House; IndraprasthaEstate; Mahatma Gandhi Road; NewDelhi 110002, India(Telegraph: WHO NEW DELHI;Telex: 3165095 or 3165031;Telephone: +(91) 11 331 7804;Fax: +(91) 11 332 7972)
WHO Regional Office for the WesternPacific
P.O. Box 2932; 1099 Manila, Philippines(Telegraph: UNISANTE MANILA;Telex: 27652;Telephone: +(632) 528 8001;Fax: +(632) 521 1036)
■ WHO regional training centreWHO Regional Training Centre forHealth Development
School of Medical Education;University of New South Wales;Sydney 2052, Australia(Telephone: +(612) 9 385 2500;Fax: +(612) 9 385 1526;E-mail: [email protected])
A student’s view on socialissues in medical educationThiago Monaco, International Federation of MedicalStudents’ Associations
of academic knowledge, throughthe application of this to everydaypractice and through training inmedical ethics. Social values andresponsibilities must underpin allmedical studies, but even the bestfaculties and schools could domore in this area.
Often medical ethics is nottaught at all, and there is strongemphasis on the biological sciencesbut little attention is paid to socialmedicine. Moreover, students to-day have to acquire a huge amountof specialized knowledge that ischanging all the time. Thus, the cur-riculum and teaching methodsmust be constantly assessed andupdated to keep pace with thesedevelopments.
For this and other reasons, stu-dents should participate actively inthe governance and policy-makingstructures of their institutions.Students are usually aware of theissues affecting their education andof the trends in their chosen field.They also bring the perspective ofyouth to social questions, whichshould be recognized as an impor-tant input by institutional leaders.
Medical education should bemuch more attuned to the actualneeds of society—that is to say, itshould be problem-based, withearly and regular contact with realpatients. This implies a new role forthe medical teacher, who wouldbecome more of a tutor orcounselor in the future. ■
Thiago Monaco is Director, StandingCommittee on Medical Education, Interna-tional Federation of Medical Students’Associations; Al. dos Ciclames 153, Alphaville06, Stna de Parnaiba, SP, BRAZIL 06487-330(e-mail: [email protected]).
QUALITY ASSURANCE IN EDUCATION
It is generally thought today thatmedical education is not meeting
the expectations of students. Themedical profession is influenced bythe constant questioning of the roleof the modern doctor in society.Students are not well-orientedwhen they start their studies, and,as a result, they are often not clearas to what they want from the pro-fession, which now is more special-ized than ever. At the same time, theneed for general practitioners hasincreased sharply to meet socialand community needs. Despitethis dilemma, a good number ofstudents remain idealistic abouttheir medical studies, which is for-tunate.
But the unmet expectations areimportant, given the diverse rea-sons that motivate people to studymedicine and the costs involved. Itis true that the medical labour mar-ket is not as empty as it was 40 yearsago and many young doctors haveproblems finding a stable and well-paid job. Once into their studies,idealism can be blunted by thepractical aspects of the profession,including the need to understandthe reasoning of national healthcare systems—and we should notforget that, in time, responsibilityfor public health systems will beassumed by today’s students.
Medical education must alsoprepare doctors for health care de-livery, to train future professors ofmedicine and to ensure lifelonglearning opportunities for healthprofessionals. The search for thebest methods of education to meetsocial needs will ensure that medi-cal education will be relevant.
Undergraduate medical educa-tion should prepare doctorsthrough the traditional acquisition
ADDRESSES

TOWARDS UNITY FOR HEALTH, APRIL 2000 ■ 39
WHO Collaborating Centre for HealthManpower Development
Office for International Relations;Faculty of Medicine; RijksuniversiteitLimburg; Postbus 616; 6200 MDMaastricht, Netherlands(Telex: 56880 fg rl nl;Telephone: +(3143) 881 520;Fax: +(3143) 670 708)
WHO Collaborating Centre for Researchin Health Manpower Development;Community-Based Educational Systems(COBES) Programme
Faculty of Health Sciences; University ofIlorin; PMB 1515; Ilorin, Nigeria(Telex: 33144 unilon ng;Telephone: +(23431) 221 844)
WHO Collaborating Centre for Researchand Training in EducationalDevelopment of Health Personnel
Department of Medical Education(DME), College of Physicians andSurgeons, 7th Central Street, DefenceHousing Authority, Karachi 75500,Pakistan(Telephone: +(92 21) 588 7111/588 3285; Fax: +(92 21) 589 3062)
WHO Collaborating Centre for Quality ofCare
Medical University of Southern Africa,Box 203 Medunsa 0204,Republic of South Africa(Telex: 32 0580 sa;Telephone: +(27 12) 529 4669;Fax: +(27 12) 560 0274)
WHO Collaborating Centre for HealthCare Professionals Development
Institut d'Estudis de la Salut; Balmes132–136; 08010 Barcelona; Spain(Telephone: +(3493) 238 6900;Fax: +(3493) 238 6910;E-mail: [email protected];Web: http://www.iesalut.es)
WHO Collaborating Centre for Researchand Training in EducationalDevelopment
Educational Development Centre;Faculty of Medicine; University ofGezira; P.O. Box 20; Wad Medani; Sudan
WHO Collaborating Centre for MedicalEducation
Faculty of Medicine; ChulalongkornUniversity; Rama IV Road; Bangkok10330; Thailand(Telephone: +(662) 252 7859;Fax: +(662) 254 1931)
■ WHO collaborating centres inhuman resources development
Centre collaborateur de l’OMS pour laRecherche en matière deDéveloppement des Ressourceshumaines pour la Santé
Faculté des Sciences de la Santé;Université nationale de la République duBénin; B.P. 188; Cotonou, Benin(Telephone: +(229) 300 001;Fax: +(229) 301 288)
WHO Collaborating Centre forEducation and Medical Practice
Faculdade de Medicina; UniversidadeFederal de Minas Gerais; CP 100; BeloHorizonte, Minas Gerais 30.130-100,Brazil (Telephone: +(55 31) 239 7167;Fax: +(55 31) 273 4985)
WHO Collaborating Centre in MedicalEducation and Practice
Centro de Ciências da Saúde;Universidade Estadual de Londrina; Cx.Postal 6001; CEP 86051; Londrina,Paraná, Brazil(Telex: +(55 432) 268;Telephone: +(55 432) 21 2000;Fax: +(55 432) 27 6932)
WHO Collaborating Center for HealthManpower Development
Centre for International Health;McMaster University;1200 Main Street West; Hamilton,Ontario, Canada L8N 3Z5(Telex: 21618347;Telephone: +(1905) 525 9140, ext.22033; Fax: +(1905) 525 1445)
WHO Collaborating Centre for MedicalEducation and Practice
Facultad de Medicina; Universidade dela Frontera; Montt 112 - Casilla 54-D;Temuco, Chile(Telephone: +(56 45) 212108Fax: +(56 45) 212108)
WHO Collaborating Centre forDevelopment of Human Resources forHealth
Faculty of Medicine; Suez CanalUniversity; Ismailia, Egypt(Telex: 63297 scufm un;Telephone: +(20 64) 328 935;Fax: +(20 64) 229 982)
WHO Collaborating Centre for theDevelopment of Human Resources forHealth and Primary Health Care
Department of General Practice andPrimary Health Care; University ofHelsinki; Lääkärinkatu 8 F; SF-00250Helsinki, Finland(Telex: 124690 unih sf;Telephone: +(3580) 434 6680;Fax: +(3580) 434 6689)
Centre collaborateur de l’OMS pour leDéveloppement des Ressourceshumaines pour la Santé
Département de Pédagogie desSciences de la Santé; U.F.R. sur laSanté, Médecine et Biologie humaine deBobigny; 74, rue Marcel Cachin; 93012Bobigny CEDEX, France(Telephone: +(3311) 48 38 76 40, ext.224 / (3311) 48 38 76 41;Fax: +(3311) 48 38 77 77)
Centre collaborateur de l’OMS pour leDéveloppement des Ressourceshumaines
Fondation Mérieux, Centre desPensières; 55, avenue d’Annecy;74290 Veyrier-du-Lac, France(Telephone: +(33) 50 64 80 80;Fax: +(33) 50 60 19 71)
WHO Collaborating Centre forEducational Development of Medicaland Health Personnel
Educational Development Centre;Shaheed Beheshti University of MedicalSciences and Health Services; Teheran,Islamic Republic of Iran(Telephone: +(98) 21 293 211;Fax: +(98) 21 294 228)
WHO Collaborating Centre for Problem-based Learning in Health ProfessionsEducation
International Health ManagementCentre; Istituto Superiore di Sanitá;Viale Regina Elena 299; I-00161 Rome;Italy(Telephone: +(396) 4938 7294;Fax: +(396) 4938 7295)
WHO Collaborating Centre for Trainingof Health Professionals
Department of Training in Public Healthand Bioethics; Istituto Superiore diStudi Sanitari, Largo del l’Artide 11,Rome, Italy-00144
WHO Collaborating Centre for Problem-Based/Problem-Solving Approaches toEducation and Practice in Public Health
Faculty of Health Sciences;Moi University; PO Box 4606;Eldoret 0321, Kenya(Telex: moivarsity 35047;Telephone: +(254 321) 33059, 32781/2/3; Fax: +(254 321) 33041)
Centro Colaborador de la OrganizacionMundial de la Salud para la Formaciónde Recursos Humanos
Facultad de Medicina; UniversidadNacional Autónoma de México; Edificio“B” Primer Piso; Apartado Postal 70-443; México, DF 04510, Mexico(Telephone: +(52 5) 616 1162;623 2401/2402;Fax: +(52 5) 616 1616;E-mail: [email protected])
ADDRESSES

Centre collaborateur de l’OMS pour laRecherche et la Formation en matièrede Développement de la Formation desPersonnels de Santé
Centre National de FormationPédagogique des Cadres de la Santé;67, boulevard Hedi Saidi; Bab Saadoun;Tunis 1005, Tunisia
WHO Collaborating Centre for PrimaryHealth Care/Public Health Education
School of Public Health; Loma LindaUniversity; Loma Linda 92350;California; USA
WHO Collaborating Centre for Leader-ship Development for Health for All
School of Public Health; University ofHawaii; 1960 East-West Road;Honolulu; Hawaii 96822; USA(Telephone: +(1808) 956 7486;Fax: +(1808) 956 5286)
WHO Collaborating Centre forEducational Development of HealthProfessionals and Health Care Systems
Department of Medical Education(M/C 591); University of Illinois Collegeof Medicine at Chicago; Box 6998;Chicago, Illinois 60680, USA(Telephone: +(1312) 996 3590;Fax: +(1312) 413 2048)
WHO Collaborating Centre forEducational Development of HealthProfessionals and Health Care Systems
University of Illinois College of Medicineat Rockford; 1601 Parkview Avenue;Rockford, Illinois 61107-1897, USA(Telephone: +(1815) 395 5600;Fax: +(1815) 395 5887;E-mail: [email protected] [email protected])
WHO Collaborating Centre forPostgraduate Public Health Educationand Research
School of Hygiene and Public Health;Johns Hopkins University;615 North Wolfe Street; Baltimore,Maryland 21205-2179, USA(Telephone: +(1410) 955 3540;Fax: +(1410) 955 0121)
WHO Collaborating Centre for theDissemination of Community-oriented,Problem-based Learning
Primary Care Curriculum; SocialMedicine Program; Department ofFamily and Community Medicine;School of Medicine; University of NewMexico; 2400 Tucker Avenue, NE;Albuquerque; New Mexico 87131-5241,USA(Telex: 660 461;Telephone: +(1505) 277 2165;Fax: +(1505) 277 0657)
WHO Collaborating Centre forInternational Health
Center for International Health;University of Texas Medical Branch atGalveston; 7.104 Shearn Moody Plaza;Galveston, Texas 77555-1095, USA(Telex: 765603;Telephone: +(1409) 772 0870;Fax: +(1409) 772 0875)
■ Nongovernmental organizationsin official relations with WHO ineducational development
Conférence internationale des Doyensdes Facultés de Médecine d’Expressionfrançaise
(Monsieur le Professeur Pierre Farah,Président); Doyen de la Faculté deMédecine; Université St.-Joseph; B.P.11-5076, Beirut, Lebanon (Telephone:+(961) 1 614 004; Fax: +(961) 1 614054; E-mail: [email protected])
International Federation of MedicalStudents Associations
(The President); Faculteit derGeneeskunde; Academisch MedischCentrum; Meibergdreef 15;NL-1105 AZ Amsterdam(Telephone: +(31 20) 566 5366;Fax: +(31 20) 697 2316)
The Network: Community Partnershipsfor Health through InnovativeEducation, Service and Research
(Coordinating Secretary:Mrs P. Vluggen); P.O. Box 616; NL-6200 MD Maastricht (Telex: 56880;(Telephone: +(31 43) 388 1522/1524;Fax: +(31 43) 367 0708;E-mail: [email protected] Wide Web: http://www.unimaas.nl/~network/welcome.htm)
World Federation for Medical Education(Dr Hans Karle, President);Faculty of Health Sciences;University of Copenhagen;The Panum Institute; Blegdamsvej 3;2200 Copenhagen N, Denmark(Telephone: +(45) 35 32 70 68;Fax: +(45) 32 32 70 70;E-mail: [email protected])
World Organization of Family Doctors(WONCA)
(Dr W.E. Fabb, Chief Executive Officer);World Organization of Family Doctors;Locked Bag 11; Collins Street East PostOffice; Melbourne Victoria 8003,AUSTRALIA(Telephone: +(61) 3 9650 0235;Fax: +(61) 3 9650 0236;E-mail: [email protected])
ADDRESSES
40 ■ TOWARDS UNITY FOR HEALTH, APRIL 2000
Towards UnityFor HealthThe newsletter Towards Unity for Healthis issued in April and October by theWorld Health Organization, Geneva,Switzerland. It aims to provide a forumfor reflection on initiatives worldwide tofoster coordinated changes in healthservices organization and healthprofessions practice and education. It isalso intended to help create a climate ofsolidarity among health authorities,academics, health professionals andrepresentatives of the community toencourage more appropriate approachesto pursuing relevance, quality, cost-effectiveness and equity in healthservices.
© World Health Organization, April 2000
This document is not a formal publicationof the World Health Organization (WHO),and all rights are reserved by theOrganization. The document may,however, be freely reviewed, abstracted,reproduced or translated, in part or inwhole, but not for sale or for use inconjunction with commercial purposes.
The views expressed in documents bynamed authors are solely theresponsibility of those authors.
The designations employed and thepresentation of material on maps in thisdocument do not imply the expression ofany opinion whatsoever on the part of theWorld Health Organization concerning thelegal status of any country, territory, cityor area or of its authorities, or concerningthe delimitation of its frontiers orboundaries. Dotted lines representapproximate border lines for which theremay not yet be full agreement.
Comments are invited from individualsand institutions interested in healthsystems development and health servicesdelivery. Contributions of short articles(less than 800 words long) areparticularly welcome. Please addresscomments and contributions to:
Dr Charles Boelen,Department of Organization of HealthServices Delivery (OSD);World Health Organization,1211 Geneva 27, SWITZERLAND(telephone: +41 22 791 2510;fax: +41 22 791 4747;e-mail: [email protected]).
Designed by minimum graphicsPrinted in France





























