Embed Size (px)
Citation preview

VIEWPOINT
Towards an Ecology of Eating Disorders:Creating Sustainability Through theIntegration of Scientific Research andClinical PracticeDavid Clinton*,
Karolinska Institutet, Resource Centre for Eating Disorders, Wollmar Yxkullsgatan, Stockholm, Sweden
Abstract
The field of eating disorders is currently at a crossroads and faces important challenges of sustainability. These
challenges include problems with the current diagnostic classification of eating disorders and the divide between
scientific research and clinical practice. If not addressed, there is a danger that the field will fail to evolve adaptively,
risking increased stagnation and reduced relevance. To meet these challenges, researchers and clinicians must work
toward a more holistic ecology of eating disorders based on the interaction of theory, research and practice. The
present paper proposes six steps towards increased sustainability based on developing clinically relevant diagnosis,
using systematic quality assurance, expanding the scope of treatment research and the definition of evidence,
promoting therapist development, as well as stimulating diversity and discourse. If we rise to the occasion and face
these challenges, then we will be better equipped to meet the evolving needs of clinicians, researchers, and most
importantly patients. Copyright # 2010 John Wiley & Sons, Ltd and Eating Disorders Association.
*Correspondence
David Clinton, M.A., M.App.Sci., Ph.D., Karolinska Institutet, Resource Centre for Eating Disorders, Wollmar Yxkullsgatan 27, 118 50
Stockholm, Sweden.
Email: [email protected]
yAssociate Professor of Medical Psychology, Psychoanalyst (IPA).
Published online in Wiley InterScience (www.interscience.wiley.com) DOI: 10.1002/erv.986
Introduction
As the year of the 200th anniversary of the birth of
Charles Darwin passes, we might pause to reflect on the
evolution of the field of eating disorders. Darwin died in
1882, only a few years after the publication of the
groundbreaking work of Gull and Lasegue on what we
now call anorexia nervosa. Initially, the field of eating
disorders went through a century of slow growth, only
to expand dramatically from roughly the publication of
Gerald Russell’s influential paper on bulimia nervosa in
1979 (Russell, 1979). Looking back over the prolifer-
ation of scientific research and clinical practice in the
field of eating disorders during the past 30 years, we
Eur. Eat. Disorders Rev. 18 (2010) 1–9 � 2010 John Wiley & Sons, Ltd and Eatin
might be tempted to rest complacent in the thought
that the rapid evolution of our field guarantees
continued growth and productivity. This, however, is
far from certain. Instead, when we pause to reflect on
the continuing evolution of the eating disorders field
there are grounds for serious concern.
Growth and the challenge ofsustainability
I will begin by borrowing a concept from the biological
sciences. Within ecology, sustainability refers to an
ecosystem’s capacity to maintain ecological functions
and processes, retain biodiversity, survive and remain
g Disorders Association. 1

Towards an Ecology of Eating Disorders D. Clinton
productive over the long-term. Today, the continuing
growth of the Earth’s population coupled with rapid
depletion of natural resources and climate change is
generating new environmental challenges. A delicate
balance of natural ecological cycles is threatened, and
we are becoming increasingly faced with a crisis of
sustainability.
Within our own field of eating disorders we are faced
with similar challenges of sustainability. The field has
witnessed a proliferation of scientific research and
treatment literature since the early 1980s. Evidence of
this can be seen in the number of papers on eating
disorders in the psychiatric literature, which was
underlined in Theander’s (2002) analysis of the
literature from Medline and PsycINFO from 1960 to
1999. Although Theander’s analysis helps to put things
in perspective, it does not tell us about the most recent
decade, or put things in a wider historical perspective.
Neither does his study take account of literature
trends in relation to eating disorder not otherwise
specified (EDNOS) or other related psychiatric
disorders.
If we extend Theander’s study both backwards and
forwards in time, and systematically analyse keywords
and topic headings in PsycINFO pertaining to eating
disorders, anorexia, bulimia and related terms from
1900 to the present, we are met with what appears to be
a clear-cut story, illustrated in Figure 1. For these
analyses data from PsycINFO, rather than Medline,
were used since there is more extensive historical
coverage of the literature in PsycINFO.
Figure 1 ED literature (numbers of publications) in PsycINFO 1900–20
2 Eur. Eat. Disorders Rev. 18 (2
Data in Figure 1 are based on the number of
publications within the eating disorders field at ten-year
intervals. What, however, is missing is a relevant anchor
point. As Theander (2002) pointed out, it is important
to look at publications on eating disorders relative to
the development of medical databases generally. If we
examine the growth of the eating disorders literature in
relation to publications in the field of psychiatry and
mental disorders as a whole the picture becomes more
complex.
In Figure 2 data on publications relating to eating
disorders are presented as a percentage of the overall
literature on psychiatry or mental disorders in
PsycINFO for the same intervals of time. Figure 2
suggests that, relatively speaking, the initial surge in
eating disorders literature came in fact during the
1970s, with a peak during the 1980s. It was during this
time that eating disorders captured a greater share of
the collective psychiatric consciousness, at least in terms
of publications. Since the 1990s the field of eating
disorders appears to have entered a period of relative
decline compared to publication trends within psy-
chiatry generally. These trends are similar to those
observed by Theander (2002), who talked about the
‘relative stagnation’ in the literature on eating disorders
during the 1990s. This stagnation would appear to have
continued into the present decade.
The picture becomes even more complex if historical
trends in other related psychiatric disorders are
considered. In Figure 3 hysteria and neurasthenia were
included in the analyses, since these disorders have
09
010) 1–9 � 2010 John Wiley & Sons, Ltd and Eating Disorders Association.
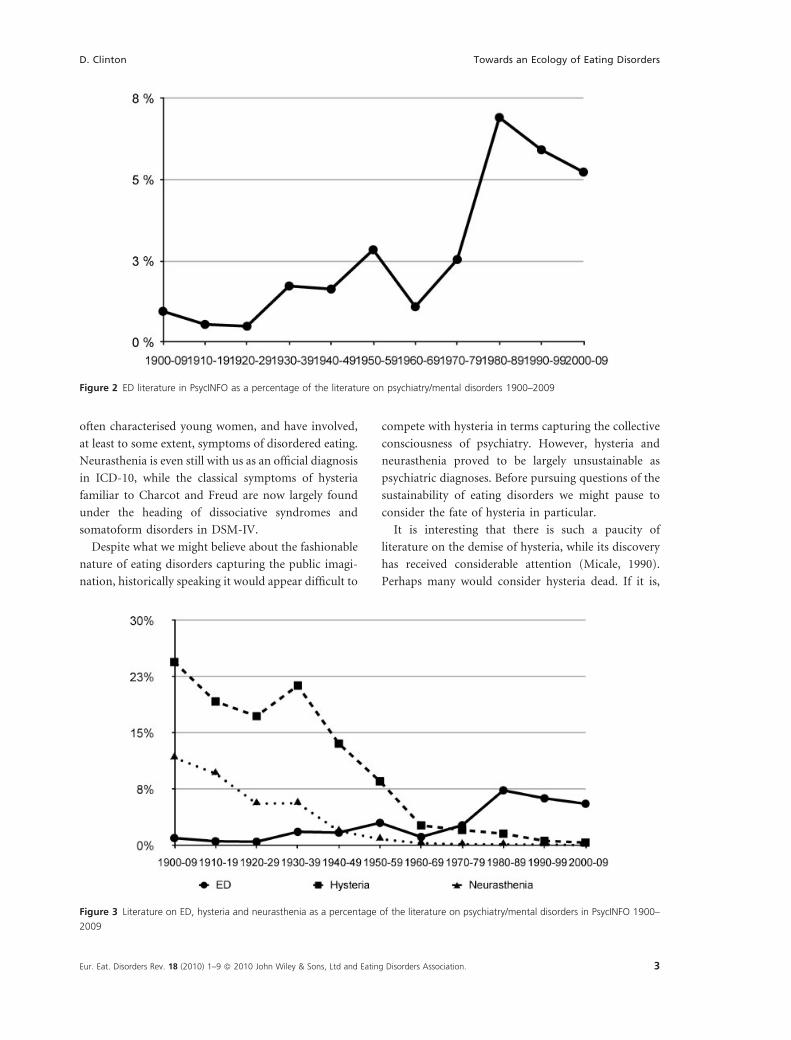
Figure 2 ED literature in PsycINFO as a percentage of the literature on psychiatry/mental disorders 1900–2009
D. Clinton Towards an Ecology of Eating Disorders
often characterised young women, and have involved,
at least to some extent, symptoms of disordered eating.
Neurasthenia is even still with us as an official diagnosis
in ICD-10, while the classical symptoms of hysteria
familiar to Charcot and Freud are now largely found
under the heading of dissociative syndromes and
somatoform disorders in DSM-IV.
Despite what we might believe about the fashionable
nature of eating disorders capturing the public imagi-
nation, historically speaking it would appear difficult to
Figure 3 Literature on ED, hysteria and neurasthenia as a percentage
2009
Eur. Eat. Disorders Rev. 18 (2010) 1–9 � 2010 John Wiley & Sons, Ltd and Eatin
compete with hysteria in terms capturing the collective
consciousness of psychiatry. However, hysteria and
neurasthenia proved to be largely unsustainable as
psychiatric diagnoses. Before pursuing questions of the
sustainability of eating disorders we might pause to
consider the fate of hysteria in particular.
It is interesting that there is such a paucity of
literature on the demise of hysteria, while its discovery
has received considerable attention (Micale, 1990).
Perhaps many would consider hysteria dead. If it is,
of the literature on psychiatry/mental disorders in PsycINFO 1900–
g Disorders Association. 3

Towards an Ecology of Eating Disorders D. Clinton
historians have yet to perform the autopsy. Some steps
along these lines have been taken by Borch-Jacobsen
(2001) who has argued that mental illness is not simply
‘out there’, waiting to be described by researchers. He
views diagnostic entities more as interactive phenom-
ena, waxing and waning in accordance with changes in
theory, research, and clinical practice. This means that
it may be quite a natural phenomenon for diagnostic
categories to evolve and change over time.
Following the line adopted by Borch-Jacobsen, and
seeing diagnosis in an interactive and ecological
framework we might conjecture that diagnostic
sustainability will be achieved when there exists a
dynamic and productive interaction between theory,
research and practice. A field that encourages a diversity
of theoretical approaches, research strategies and
treatment techniques, and which promotes exchange
of ideas and findings, will be better fitted to adapt and
meet new challenges, productively integrating new
discoveries with tried and tested knowledge.
Getting back to eating disorders, there are signs that
we are currently facing challenges of sustainability.
These include the problems with the current diagnostic
classification of eating disorders and the lack of
productive interaction between scientific research and
clinical practice. If not addressed through the devel-
opment of more relevant diagnosis and increased
integration of research and practice, then there is a
danger that the field of eating disorders will fail to
evolve adaptively, and the risk may increase of meeting
the same fate as hysteria and neurasthenia.
The diagnostic crisis
Nowhere is the challenge of sustainability more evident
than in the field of eating disorder diagnosis. There is a
manifest lack of correspondence between the DSM and
ICD systems in terms of definitions and criteria. Within
DSM-IV there is a marked dichotomy between the
clear-cut syndromes of anorexia nervosa and bulimia
nervosa, and the amorphous mass of suffering relegated
to the catch-all category of EDNOS, which means that
the DSM system has limited clinical relevance. Several
recent studies bear witness to the overwhelming
number of eating disorder patients who are currently
categorised as EDNOS. Within a community-based
eating disorder service, EDNOS patients have been
found to constitute 67% of presenting cases (Turner &
Bryant-Waugh, 2004). In a two-stage community-
4 Eur. Eat. Disorders Rev. 18 (2
based study of the prevalence of eating disorders among
young females, 0.39% of the sample fulfilled DSM-IV
criteria for anorexia nervosa (AN), 0.30% for bulimia
nervosa (BN), and 2.37% were classified as EDNOS;
among the cases of eating disorders identified in the
study, 77.4% were EDNOS (Machado, Machado,
Goncalves, & Hoek, 2007).
It might be assumed that the largest diagnostic group
of eating disorders would also be the group that receives
greatest attention in the literature. However, this is
far from the case. If a systematic analysis of PsycINFO
is conducted and literature on anorexia, bulimia and
EDNOS are compared, the results are telling. In Figure 4
data on publications dealing with anorexia and
bulimia are contrasted with those dealing with EDNOS,
atypical eating disorders or binge eating disorder
(BED). These figures are presented as percentages, i.e.
numbers of publications relative to the number of
publications relating to eating disorders as a whole.
Note that the given percentages do not always total 100,
especially from the 1960s onwards, due to a general
widening of interest in the literature and an increased
number of studies looking at phenomena such as
‘disordered eating’, ‘eating habits’, ‘purging syndrome’,
etc.
In all fairness, EDNOS, atypical eating disorders and
BED are relatively new concepts compared with
anorexia and bulimia. However, what nonetheless
becomes abundantly clear, especially when we examine
data from the past decade, is that scientific interest in
eating disorders is to be found almost exclusively in
relation to the two classic syndromes of AN and BN.
What’s more, of the 1021 publications to date on
EDNOS during the present decade 822 (80%) dealt with
BED. Coupled with the literature on the overwhelming
prevalence of EDNOS, questions arise about why the
vast majority of patients with eating disorders appear to
receive relatively little scientific attention. Perhaps the
sufferers of eating disorders are not the only ones to fall
victim to unrealistic, glamorised ideals. Even though
EDNOS patients may suffer from equally serious clinical
conditions as full-syndrome patients, and despite the
increased attention shown to bulimia from the 1980s
onwards, researchers still seem to see AN as the ‘sexy’
eating disorder.
There are one or two other interesting trends in
Figure 4 that deserve comment. The dramatic dearth of
publications on anorexia from 1910–1919 likely reflects
the prevailing interest in anorexia as a purely medical
010) 1–9 � 2010 John Wiley & Sons, Ltd and Eating Disorders Association.

Figure 4 Literature on AN, BN and EDNOS as a percentage of the literature on ED in PsycINFO 1900–2009
D. Clinton Towards an Ecology of Eating Disorders
condition at that time, following Simmonds (1914)
influential paper on anorexia as a form of pituitary
insufficiency. Since the purely endocrinological litera-
ture is lacking in PsycINFO, the data give a somewhat
distorted picture of paucity of interest in AN during this
period. Nevertheless, there is a dramatic surge of
interest in AN from the 1930s and into the 60s, when it
dominated the eating disorder literature completely.
This coincides with the period of psychoanalytic
dominance in the field. It is also interesting that although
there is a dramatic surge of publications relating to bulimia
during the 1980s, the phenomenon is by no means absent
from the literature in previous decades. Nevertheless,
despite various developments in the field of eating
disorders, it is striking that anorexia still dominates our
collective consciousness, and that the ‘discovery’ of
bulimia in the 1980s has not been matched by the same
degree of interest during the present decade.
The research-practice divide
Knowledge of eating disorders has increased signifi-
cantly since the 1970s. At the same time, specialist
services have expanded to an extent that would have
been difficult to imagine 40 years ago. For example, in
Stockholm, where I work, specialist services have grown
from a handful of pioneers in the mid 1980s to well over
100 specialists currently involved in publicly and
privately operated care for eating disorders. These
developments have, of course, benefited patients.
Eur. Eat. Disorders Rev. 18 (2010) 1–9 � 2010 John Wiley & Sons, Ltd and Eatin
However, even though research and clinical practice
have grown, they have also tended to grow apart.
The divide between scientific research and clinical
practice is evident in many ways. One such way
concerns the difficulties in integrating evidence-based
treatment into clinical practice. Since the mid-1980s
important strides have been made in the development
and evaluation of evidenced-based treatment for eating
disorders. The treatment of choice is often cognitive
behavioural therapy for adults, at least in the case of BN,
or family therapy in the case of adolescent AN. These
developments have resulted in the adoption of national
guidelines for treatment provision in various countries
(e.g. NICE, 2004; RCP, 2001; APA, 2006). Despite the
promotion of such guidelines, many clinicians appear
not to use them or even be aware of them. In a survey of
primary care physicians Currin and colleagues (2007)
found that only 4% of those surveyed reported using
published ‘best practice’ guidelines for eating disorders.
And they found no evidence that guidelines on ‘best
practice’ promote evidence-based management of eating
disorders. What’s more, adoption of ‘best practice’
provides no guarantee that patients will get better. As
Vanderlinden (2008) has pointed out, evidence-based
approaches to eating disorders are unsuccessful in
treating many patients. For example, systematic long-
term studies suggest that CBT is successful in treating
approximately 45–50% of bulimics (Gowers et al., 2007).
Part of the problem may be that cases seen in the
community bear little resemblance to those used in the
g Disorders Association. 5

Towards an Ecology of Eating Disorders D. Clinton
randomised controlled trials that form the backbone of
practice guidelines. This makes the research in question
less relevant for clinicians. Remember that the majority
of eating disorder cases being seen by therapists are
EDNOS, whereas randomised controlled trials are
based on full-syndrome patients. Using four common
exclusion criteria from randomised controlled trials,
Thompson-Brenner and Westen (2005a) found that
40% of bulimics treated in the community would have
been excluded from randomised controlled trials. The
same researchers found that among those patients in
the community receiving CBT, treatment was sub-
stantially longer than that prescribed in manuals (i.e. on
average 69 sessions).
It might be argued that practitioners are simply not
applying tested therapeutic techniques, as they should,
at least as regards the full-syndrome patients where
there is more evidence of efficacy. However, it could
also be argued that researchers are not sufficiently in
touch with clinical reality, and are not testing their
treatments on clinically relevant samples of patients. It
is also interesting that Thompson-Brenner and Westen
(2005b) found that although CBT and psychodynamic
therapists treating BN in the community used
substantially different forms of treatment, distinguish-
able in terms of their differing theoretical orientations,
they both tended to practice more integrative inter-
ventions than those prescribed in manuals. Examples of
integrative approaches to eating disorders can be found
in the literature. Schaffner and Buchanan (2008)
combined cognitive-behavioural therapy with clinical
experience and strategies such as group, family and
individual therapy. Murphy, Russell and Waller (2005)
have described an integrative form of treatment for BN
and BED based on the combination of psychodynamic
and behavioural principles.
Another important part of the research-practice
divide concerns the way results from empirical research
tends to be interpreted. Systematic treatment research
focuses on statistical analysis of means and variance
between groups. When significant differences are found
between treatment and control groups in randomised
studies, inferences are made about the efficacy of
particular therapeutic techniques. However, what is
often not discussed or systematically analysed is the vast
reservoir of within-group variance in these studies.
Regardless of the form of treatment used in a study,
there will always be variability within a particular
treatment group. The problem for researchers involves
6 Eur. Eat. Disorders Rev. 18 (2
systematically tapping into within-group variance to
better understand how and why patients respond the
way they do.
Contemporary ‘best practice’ guidelines are often
assumed to suggest that good treatment results will
follow provided clinicians use good (i.e. evidence-
based) techniques. Here the underlying implication is
that it is technique that results in change. Although
technique is one variable in the change equation, it is by
no means the only one. As early as 1936 Rosenzweig
discussed the importance of common factors in
psychotherapy (Rosenzweig, 1936). Over the years
the contribution of general and specific factors to
outcome has received considerable attention in meta-
analyses of the psychotherapy literature. In a meta-
meta-analysis of 17 previous meta-analyses in the
psychotherapy literature Luborsky and colleagues
(2002) found that when active treatments were
compared with each other the mean effect size was
small and non-significant (i.e. Cohen’s d¼ 0.20
uncorrected, and even lower d¼ 0.12 when corrected
for the researcher’s allegiance). The large and significant
effect sizes in the psychotherapy literature are to be
found when active treatments are compared to no
treatment or waiting list controls. In a review of the
literature Wampold (2007) surmises that these absolute
effects of psychotherapy lie in the region of d¼ 0.80 (i.e.
considerably large effects).
One factor that may go a long way to explaining the
considerable within-group variance in randomised
controlled trials in both the psychotherapy and eating
disorder literature is the therapist. Individual therapists
practising the same methods produce varying results
with different patients that cannot be explained on the
basis of patient background or severity (Luborsky,
McLellan, Diguer, Woody, & Seligman, 1997). What’s
more, Wampold and Serlin (2000) have found that
treatment effects can be systematically overestimated
when therapist effects are not taken into account. Even
in randomised trials where therapists are selected for
their technical skill and monitored for adherence to a
treatment manual, there will be a significant proportion
outcome variance that is attributable to therapists
within treatments. This therapist effect has been
estimated to be at least one order of magnitude greater
than any differences among treatments in randomised
trials (Kim, Wampold, & Bolt, 2006). More impor-
tantly, it appears that much of the variability among
therapists is due to differences in therapists’ ability to
010) 1–9 � 2010 John Wiley & Sons, Ltd and Eating Disorders Association.

D. Clinton Towards an Ecology of Eating Disorders
form a working alliance with a variety of patients
(Baldwin, Wampold, & Imel, 2007).
Perhaps Cole Porter was right, ‘it’s not what you do,
it’s the way that you do it’. That’s what it’s all about.
Although there has as yet been relatively little systematic
research in the eating disorders field that has attempted
to disentangle how effective treatments work, there is a
growing body of evidence within psychotherapy
research generally that outcome is not so much
dependent on what psychological ingredients are
delivered but how they are delivered. This in turn
raises challenges for researchers. We need to knowmore
about what makes good therapists, and how therapists
contribute to outcome.
This brings us back to the research-practice divide,
and the question of sustainability within the eating
disorders field. There may be an inherent problem in
how eating disorder researchers and therapists view the
question of evidence. Scientists and proponents of ‘best
practice’ guidelines may tend to see evidence as simply a
question of weighing up the data on the efficacy of
specific techniques and implementing practice accord-
ingly, whereas clinicians may view evidence more in
terms of their own experience and what works for them
‘out there’. The result may be frustration on both parts.
Researchers feel frustrated over therapists who adopt
‘prejudice-based’ practice and refuse to integrate hard-
won scientific knowledge in treatment, while therapists
feel frustrated over rigid researchers who fail to grasp
the complexity of everyday clinical practice. If there is
no constructive dialogue between clinicians and
researchers then the gulf will widen, and sustainable
growth will be threatened.
Steps towards create greatersustainability
Despite the challenges, there is much that can be done
to affect adaptive evolution in the field of eating
disorders. Here I would like to propose six steps
towards greater sustainability that focus on closer
integration of scientific research and clinical practice.
Developing clinically relevant eating
disorder diagnosis
We stand on the verge of DSM-V. It will be essential
that the new system of eating disorder diagnosis is more
clinically relevant than at present. To this end it will be
Eur. Eat. Disorders Rev. 18 (2010) 1–9 � 2010 John Wiley & Sons, Ltd and Eatin
essential that the new system reduces the number of
eating disorder patients who are relegated to EDNOS.
This could, for example, involve relinquishing the
amenorrhoea criterion for AN, and widening the
frequency criteria for BN. There should also be an
attempt to define what constitutes an ‘eating disorder’
per se, so eating disorders can be distinguished from
other psychiatric syndromes. Attention should also be
directed towards bringing the DSM and ICD systems
into better alignment.
Developing systematic quality
assurance
Quality assurance of specialist eating disorder care is in
increasing demand from public health officials,
practitioners and the patient community. There is a
need to know more about how treatment works in real-
life clinical settings, and the extent to which patients
attain empirically definable treatment goals. Today,
computer-based quality assurance is one possible way
of meeting demands for evaluating the real-life
effectiveness of eating disorder treatment, in a large-
scale, cost-effective and highly structured way. In
Sweden there is growing experience of the opportu-
nities and challenges involved in implementing such a
system (Birgegard, Bjorck & Clinton, in press). For
clinicians, computer-based quality assurance facilitates
systematic assessment of eating disorders and increases
the knowledge base for informed selection and evalua-
tion of services. For researchers, a rich database is
generated within a naturalistic setting, which allows
access to a large and clinically relevant sample of eating
disorder patients. Development of systematic quality
assurance alsomeans that differences between clinicians
and researchers come to the fore, and points of conflict
become more apparent. This poses challenges, but also
creates tangible opportunities for researchers and
clinicians to meet, discuss and solve these problems,
ultimately bringing them closer together.
Expanding the scope of treatment
research
Randomised controlled trials have added enormously
to our knowledge of eating disorder treatment. Such
work will continue to be important, but it is now time
to expand the scope of treatment research. We need to
know more about how treatment works in everyday
g Disorders Association. 7

Towards an Ecology of Eating Disorders D. Clinton
practice. It will be important to explore questions
relating to the contribution of general and specific
factors, investigate how the therapeutic alliance can be
strengthened in work with eating disorder patients, and
how expectations may influence response to treatment
and outcome. Definitions of recovery should be
explored and expanded in order to encompass a richer
array of relevant variables. Statistically, there needs to
be greater attention paid to studying interaction effects,
so we can better understand the clinically relevant
question of what works for whom.
Expanding the definition of evidence
Using randomised controlled trials is one important
form of evidence, but it is not the only important form
of evidence. A greater rapprochement between clin-
icians and researchers will be aided by increased use and
discussion of results obtained by other types of research.
Attention should be directed towards qualitative
research, systematic cases studies, as well as naturalistic
and longitudinal work. Discussing and appraising these
different forms of evidence will contribute to a more
clinically relevant and holistic picture of what works in
the treatment of eating disorders and how it works.
Promoting therapist development
The therapist could be considered the lost variable of
treatment research. More attention needs to be directed
at understanding the how therapists actually work in
everyday clinical settings, and helping them to learn
new ways of better using their strengths and improving
on their weaknesses. This will involve attention to new
questions on the part of researchers, as well as increased
openness on the part of clinicians. Promoting the
development of individual therapists will need to go
beyond the use of treatment manuals, and focus more
on how treatment is conducted in real-life settings. To
this end, developments in the use of systematic quality
assurance can have an important role to play by
providing clinicians with relevant feedback on their
own work.
Stimulating diversity and discourse
In biological systems diversity forms the basis for
evolutionary adaptation in a changing environment.
Within the field of eating disorders we need to
8 Eur. Eat. Disorders Rev. 18 (2
encourage diversity of treatment approaches and
research strategies. Promoting diversity can help us
to understand the emerging complexity of eating
disorders, and make it easier to develop effective
treatment strategies. But in order for diversity to be
effective we will also need to stimulate discourse and the
exchange of ideas, between practitioners and research-
ers as a whole, and between groupings of practitioners
and researchers with differing theoretical orientations.
Discourse will help us to find common ground and
delineate points of difference. It will stimulate treat-
ment development and help us to achieve more widely
held standards of evidence for better understanding
eating disorders and evaluating treatment. This could
be done by organising workshops and panels at
conferences focusing on greater collaboration and
exchange of ideas by clinicians and researchers,
stimulatingmore longitudinal and naturalistic research,
greater involvement of clinicians in research and
researchers in treatment, as well as organising discus-
sions of clinical and research problems from a trans-
theoretical perspective where therapists and researchers
of differing orientations take on common problems.
Summary and conclusions
Pausing to reflect on the evolution of the field of eating
disorders there is cause for concern. We are currently at
a crossroads and facing important challenges of
sustainability. These challenges include problems with
the current diagnostic classification of eating disorders
and the tangible divide between scientific research and
clinical practice. If not addressed, there is a danger that
the field of eating disorders will fail to evolve adaptively,
with the risk of increased stagnation and reduced
relevance. To meet these challenges we need to work
together towards a more holistic ecology of eating
disorders based on a dynamic and productive
interaction of theory, research and practice. The
present paper proposes six steps towards increased
sustainability based on developing clinically relevant
diagnosis, systematic quality assurance, expanding the
scope of treatment research and the definition of
evidence, promoting therapist development, as well as
stimulating diversity and discourse within the field.
If we rise to the occasion and face these challenges,
then we will be better equipped to meet the evolving
needs of clinicians, researchers, and most importantly
patients.
010) 1–9 � 2010 John Wiley & Sons, Ltd and Eating Disorders Association.

D. Clinton Towards an Ecology of Eating Disorders
References
American Psychiatric Association (APA). (2006). Practice
guidelines for the treatment of patients with eating dis-
orders (3rd ed.). Arlington, VA: American Psychiatric
Association.
Baldwin, S., Wampold, B., & Imel, Z. (2007). Untangling the
alliance-outcome correlation: Exploring the relative
importance of therapist and patient variability in the
alliance. Journal of Consulting and Clinical Psychology,
75, 842–852.
Birgegard, A., Bjorck, C., & Clinton, D. (in press). Quality
assurance of specialised treatment of eating disorders
using large-scale Internet-based collection systems:
Methods, results and lessons learned from designing
the Stepwise database. European Eating Disorders Review.
Borch-Jacobsen, M. (2001). Making psychiatric history:
Madness as folie a plusieurs. History of the Human
Sciences, 14, 19–38.
Currin, L., Waller, G., Treasure, J., Nodder, J., Stone, C.,
Yeomans, M., et al. (2007). The use of guidelines for
dissemination of ‘best practice’ in primary care of patients
with eating disorders. International Journal of Eating
Disorders, 40, 476–479.
Gowers, S., Clark, A., Roberts, C., Griffiths, A., Edwards, V.,
Bryan, C., et al. (2007). Clinical effectiveness of treatments
for anorexia nervosa in adolescents: Randomised con-
trolled trial. British Journal of Psychiatry, 191, 427–
435.
Kim, D.,Wampold, B., & Bolt, D. (2006). Therapist effects in
psychotherapy: A random effects modelling of the NIMH
TDCRP data. Psychotherapy Research, 16, 161–172.
Luborsky, L., McLellan, A., Diguer, L., Woody, G., & Selig-
man, D. (1997). The psychotherapist matters: Compari-
son of outcomes across twenty-two therapists and seven
patient samples. Clinical Psychology: Science and Prac-
tice, 4, 53–65.
Luborsky, L., Rosenthal, R., Diguer, L., Andrusyna, T.,
Berman, J., Levitt, J., et al. (2002). The Dodo Bird verdict
is alive and well—mostly. Clinical Psychology: Science
and Practice, 9, 2–12.
Machado, P., Machado, B., Goncalves, S., & Hoek, H.
(2007). The Prevalence of eating disorders not otherwise
specified. International Journal of Eating Disorders, 40,
212–217.
Micale, M. (1990). Hysteria and its historiography: The
future perspective. History of Psychiatry, 1, 33–124.
Murphy, S., Russell, L., & Waller, G. (2005). Integrated
psychodynamic therapy for bulimia nervosa and binge
Eur. Eat. Disorders Rev. 18 (2010) 1–9 � 2010 John Wiley & Sons, Ltd and Eatin
eating disorder: Theory, practice and preliminary find-
ings. European Eating Disorders Review, 13, 383–391.
National Institute of Clinical Excellence (NICE). (2004).
Eating disorders: Core interventions in the treatment and
management of anorexia nervosa, bulimia nervosa and
related eating disorders. CG9. London, UK: The British
Psychological Society.
Rosenzweig, S. (1936). Some implicit common factors in
diverse methods of psychotherapy. American Journal of
Orthopsychiatry, 6, 412–415.
Royal College of Psychiatrists (RCP). (2001). Primary care
protocols for common mental illnesses—protocol III:
Eating disorders (18þyears) Identification and referral.
London, UK: Royal College of Psychiatrists.
Russell, G. F. M. (1979). Bulimia nervosa: An ominous
variant of anorexia nervosa. Psychological Medicine, 9,
429–448.
Schaffner, A., & Buchanan, L. (2008). Integrating evidence-
based treatments with individual needs in an outpatient
facility for eating disorders. Eating Disorders, 16, 378–
392.
Simmonds, M. (1914). Uber embolische Prozesse in der
Hypophysis. Archives of Pathology and Anatomy, 217,
226–239.
Theander, S. (2002). Literature on eating disorders during
40 years: Increasing number of papers, emergence of
bulimia nervosa. European Eating Disorders Review,
10, 386–398.
Thompson-Brenner, H., & Westen, D. (2005a). A natura-
listic study of psychotherapy for bulimia nervosa, part 1.
Journal of Nervous and Mental Disease, 193, 573–
584.
Thompson-Brenner, H., & Westen, D. (2005b). A natura-
listic study of psychotherapy for bulimia nervosa, part 2.
Journal of Nervous and Mental Disease, 193, 585–595.
Turner, H., & Bryant-Waugh, R. (2004). Eating disorder not
otherwise specified (EDNOS): Profiles of clients present-
ing at a community eating disorder service. European
Eating Disorders Review, 12, 18–26.
Vanderlinden, J. (2008). Many roads lead to Rome: Why
does cognitive behavioural therapy remain unsuccessful
for many eating disorder patients? European Eating
Disorders Review, 16, 329–333.
Wampold, B., & Serlin, R. (2000). The consequences of
ignoring a nested factor on measures of effect size in
analysis of variance designs. Psychological Methods, 4,
425–433.
Wampold, B. (2007). Psychotherapy: The humanistic (and
effective) treatment. American Psychologist, 62, 857–873.
g Disorders Association. 9







