Too little, too late Real World Insights on Current Practice
of Home Parenteral Nutrition in Germany
ESMO 2018, Munich
Prof. Dr. med. Ingolf Schiefke
Gastroenterology and Hepatology Klinikum St. Georg gGmbH
Leipzig, Germany
1
Agenda
2
Introduction parenteral nutrition
Objectives
Methodology
Results Demography Comorbidities Clinical outcomes: Survival
Drug costs utilisation
Summary
Conclusions
3
Nutrition SupportVolume 38 Number 2
Original Communication
Adapted from Hbuterne X, et al. JPEN J Parenter Enteral Nutr.
2014;38:196-204.
Prevalence of Malnutrition and Current Use of Nutrition
4Arends J, et al. Clin Nutr. 2017;36(1):11-48.
ESPEN Guidelines on Nutrition in Cancer Patients (1)
5Arends J, et al. Clin Nutr. 2017;36(1):11-48.
ESPEN Guidelines on Nutrition in Cancer Patients (2)
6
*Includes values of arm circumference, triceps skinfold, albumin
and transferrin normal values
7
Cancer-specific Survivals
Progression-freeSurvivals
Disease-freeSurvivals
Shachar SS, et al. Eur J Cancer. 2016;57:58-67.
Sarcopenia is a prognostic markerHazard Ratios for:
8
No Yes
Grade 3-4 Toxicity
Skel
etal
Mus
cle
Gau
ge(S
MG
)
2,500
2,000
1,500
1,000
500
P=0.04
Shachar SS, et al. Clin Cancer Res. 2017;23(3):658-665
Toxicity from Taxane in Breast Cancer Patients with
Sarcopenia
Study Objectives
9
This study1 is set out to investigate real-world use of home
parenteral nutrition (HPN) amongst cancer patients with 5 tumour
types in Germany.
The study quantified the number of deceased cancer patients who
received HPN
Data analysis described
1)patients demographic characteristics
2)patients comorbidities
3)clinical outcomes of patients who received PN
Additional data analysis provided an indication of cost share
between cancer treatment and parenteral nutrition across 5 tumour
types.
1) Data on file: Versorgungsforschung zur parenteralen Ernhrung
in Deutschlang in Zusammenarbeit HGC GesundheitsConsult GmbH,
2017
Observation window is 6 yearsBasic data
Age GenderRegion
Outpatient treatmentUtilization (EBM Figures)Diagnoses (ICD
codes)Physicians
Inpatient treatmentHospital stays (DRG, OPS)Diagnoses
(ICD)Length of stay
Pharmaceutical dataATC, PZNDDDPrescriptions/ prescriber
Treatment via medical devices medical aids, remedies
Disability and sick payCosts and resource use
Available SHI claims data
Long
itudi
nal P
atie
nt D
ata~4 million insured
individuals~70 Statutory
Health Insurances 5.5% nationwide
representative sample
10
Study Content Methodology (1)
There is a good overall accordance of the Health Risk Institute
database and the German population in terms of measures of
morbidity, mortality and drug usage.
Persistence of insurant with the database over time is high,
indicating suitability of the data source for longitudinal
epidemiological analyses1.
External validity of database
1 Andersohn, F; Walker, J (2016), Characteristics and external
validity of the German Health Risk Institute (HRI) Database2 Swart,
E et. al (2014), Gute Praxis Sekundrdatenanalyse (GPS): Leitlinien
und Empfehlungen
The analysis has been designed following the Good Practice in
Secondary Data Analysis (GPS) 2
The 11 guidelines range from ethical principles and study
planning through quality assurance measures and data preparation to
data privacy, contractual conditions and responsible communication
of analytical results.
Validity of Methodology
Valid
ity o
f dat
aset
11
Study Content Methodology (2)
The study population was defined as deceased stage IIIb/ IV
cancer patients
Five cancer types were included ovarian, pancreas, colorectal
carcinoma (CRC), gastric, head & neck (H&N); defined
regarding to ICD 10 GM Coding Chapter C (confirmed outpatient or
inpatient diagnoses)
Observation period was defined as period between initial therapy
of Stage IIIb/IV cancer until day of death
Definition of initial treatment to identify Stage IIIb/IV
patients (metastatic or recurrent carcinoma)
Definition of home parenteral nutrition based on prescriptions
(Pharmacy Registration Number) in the outpatient sector
12
We observed deceased Stage IIIb/IV cancer patients with or
without home parenteral nutrition (HPN)
Study Content Methodology (3)
Deceased cancer patients Stage IIIb/IV
Index Day of death/
calendar quarterIndividual observation period
Index Quarter in which the initial
therapy pursuant to guidelines of stage IV
cancer started
13
Head & NeckCetuximab
without radiation
CRCBevacizumab or
Cetuximab
OvarianCarboplatin and Paclitaxel
and/or Bevacizumab
Gastricdiagnosis, directly followed by prescription of
parenteral
or enteral nutrition
PancreaticGemcitabin, if there was no surgery 3
months before
Study Content Methodology (4)
20122011 2013 2014 2015 2016
14
Maximum
Minimum
MedianMean
0
20
40
60
80
100
Head & Neck CRC Ovarian Gastric
95 y
71.6 y
21 y
92 y
69.9 y
33 y
85 y
63.4 y
26 y
93 y
67.0 y
23 y
88 y
62.9 y
27 y
SD:10,1SD:11 SD:11,1 SD:9,7
SD:12,6
Age per cancer indication / age at pick up stage IIIb/IV
Pancreatic
Mean age of the patients at 1st line cancer treatment is 67
years with a higher share of male patientsH&N CRC Ovarian
Pancreas Gastric
No HPN 300 1,675 228 1,197 447
HPN 43 290 53 209 153
H&N CRC Ovarian Pancreas GastricM (%) 83.4 62.8 - 57.3 63.7F
(%) 16.6 37.2 100 42.7 36.3
Gender distribution
Study Content Demographics (1)
The number of HPN users differs substantially in each cancer
group
Head & Neck
43 300
HPN No HPN
Number of patients in DB*1(cancer all stages)Indexing period:
Date of death between 2010-16No multiple cancer diagnosesIndexing:
1st line patients and no previous HPN*2
Number of patients with or without HPN
290 1,675
HPN No HPN
53 228
HPN No HPN
209 1,197
HPN No HPN
153 447
HPN No HPN
CRC Ovarian GastricPancreatic
*1 The total database (DB) comprises data of 4 million insured
individuals per year*2 initial therapy pursuant to guideline of
Stage IV cancer (metastatic or recurrent carcinoma) 15
19,313
6,027
5,437
343
53,390
19,574
17,742
1,966
8,900
3,353
2,765
281
10,143
7,633
6,784
1,406
12,480
6,783
5,716
600
Study Content Demographics (2)
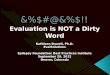
Share of patients with / without PN per cancer indication
Share of patients with HPN Share of patients without HPN
H&N CRC Ovarian Pancreatic Gastric
The share of patients with HPN in overall cancer types is on
average 16% The highest share of HPN patients is observed in
patients with Gastric cancer at 25% (153
out of 600). The lowest share of HPN patients is observed in
patients with Head & Neck cancer at 12%
(43 out of 343). Caveat: Enteral nutrition therapy is not
covered within this analysis
43 290 53 209153
300 1676 228 1197447
0%
20%
40%
60%
80%
100%
12% 15% 15%19% 25%
16
Study Results Demographics (1)
61%71%
14%21%
28%37%37% 38%
10% 11%
27%16%
0%
20%
40%
60%
80%
100%
Year 1 Year 2 Year 1 Year 2 Year 1 Year 2
Cachexia Infection With at least one of
definedcomorbidities*
PN No PN
Up to 40% of the gastric cancer patients suffering from cachexia
are not treated with HPN
Share of Gastric cancer patients with comorbidities
17
Only 2 years of observation. Third follow-up year n
Share of Gastric cancer patients with Decubitus vs. no Decubitus
(in year 1)
22%
78%
without HPN
Dekubitus
No Dekubitus
12%
88%
with HPN
The share of patients with decubitus is higher in year 2
compared to year 1, especially for patients with HPN
That indicates a physical decline in patients with HPN Patients
without HPN suffer less from decubitus in year 2
18
Year 1 Year 2 Year 3 Year 4 Year 5 Year 6Patients with PN 124 38
11
376.7days
295.7days
Mean period until death per patient without HPN in days
472.4days
718.8days
209.3days
237.7days
+ 81 d + 29 d + 41 d + 84 d + 118 d HPN - No HPNMean period
until death per patient withHPN in days
500.7days
760.1days
292.9days
355.5days
The longest mean period until death per patient without HPN is
observable in Ovarian cancer patients (~2 years)
The biggest difference in the period until death between HPN and
no HPN can be seen in Gastric patients (+118 days)
The period between start HPN and death amounts is around 3
months, which is too late according to the definition of refractory
cachexia
Overview of average duration until death per patient in each
cancer indication
H&N CRC Ovarian Pancreas Gastric
No HPN 300 1,675 228 1,197 447
HPN 43 290 53 209 153
19
Data suggests that patients receiving HPN survive on average 70
days longer than patients not receiving HPN (caveat: descriptive
readout only)
Study Results Survival (1)
Head & Neck CRC Ovarian GastricPancreatic
The longest average period until HPN initiation per patient is
observable in Ovarian cancer patients ~ 2 yrs
The shortest average period until HPN initiation per patient is
observable in Gastric cancer patients ~ 6 mos
Head & Neck CRC Ovarian GastricPancreaticAverage duration
until PN initiation per patient in days
266.6days
394.5days
625.8days
200.1days
195.7days
Average period until PN initiation per patient in each cancer
indication
H&N CRC Ovarian Pancreas Gastric
No HPN 300 1,675 228 1,197 447
HPN 43 290 53 209 153 20
H&N CRC Ovarian GastricPancreatic
The time from initiation of cancer treatment to initiation of
HPN varied widely by cancer indication, with on average of 1 year
(337 days) delay
Study Results Survival (2)
Diagramm1
H&N
CRC
Ovarial-CA
Pankreas
Magen
266.6
394.5
625.8
200.1
195.7
Job 1 - Means
time to PE, Time to death, time from PE until to death, by
PE-Type ( days)Fischoel
gruppetypeVariableMinimumMittelwertMedianMaximumStd.abweichungH&NCRCOvarial-CAPankreasMagengesamt
halskopfFischoeldauerbispedauerbistotdauerpebistot0.009.002.00235.37349.33113.96143.00321.0063.00887.00953.00410.00277.36272.20127.21H&NDauer
bis PE/pat in TagenMW235.4371.9541.4186.6207.7308.6
Olivenoeldauerbispedauerbistotdauerpebistot5.0063.000.00319.31422.88103.56254.00410.5071.001041.001138.00468.00314.37314.45127.74
kolonFischoeldauerbispedauerbistotdauerpebistot1.004.001.00371.94482.27110.33288.50391.5062.501507.001727.00933.00311.17344.47152.20CRC
Olivenoeldauerbispedauerbistotdauerpebistot6.0062.003.00443.10540.3997.29316.50437.0051.501494.001663.00723.00365.80382.20142.97
magenFischoeldauerbispedauerbistotdauerpebistot1.0018.001.00207.74389.59181.8581.00278.0089.001851.001852.001062.00307.76381.73234.02Magen
Olivenoeldauerbispedauerbistotdauerpebistot0.0011.000.00173.63292.94119.3189.00238.5067.00826.00844.00699.00191.09216.56142.33
ovarioFischoeldauerbispedauerbistotdauerpebistot3.0059.003.00541.44691.21149.77396.00614.0090.001608.001762.00628.00458.19435.60167.83Ovarial-CA
Olivenoeldauerbispedauerbistotdauerpebistot286.00305.0013.00860.86952.0091.14911.001044.0044.501520.001562.00275.00349.97352.9386.90
pankreasFischoeldauerbispedauerbistotdauerpebistot1.0013.000.00186.56273.3086.73119.00225.0046.001322.001322.00595.00199.71218.35105.86Pankreas
Olivenoeldauerbispedauerbistotdauerpebistot2.0024.001.00232.23339.29107.06139.50216.0052.001002.001232.00801.00261.34304.40157.83
time to PE, Time to death, time from PE until to death, total (
days)Total
gruppetypeVariableMinimumMittelwertMedianMaximumStd.abweichungH&NCRCOvarial-CAPankreasMagengesamt
halskopfTotaldauerbispedauerbistotdauerpebistot0.009.000.00266.60376.70110.09170.00387.0067.001041.001138.00468.00290.87287.18125.98Dauer
bis PE total /pat in TagenMW266.6394.5625.8200.1195.7336.54
kolonTotaldauerbispedauerbistotdauerpebistot1.004.001.00394.51500.71106.20295.50398.0055.501507.001727.00933.00330.51357.23149.21
magenTotaldauerbispedauerbistotdauerpebistot0.0011.000.00195.70355.48159.7887.00259.0082.001851.001852.001062.00272.15335.34208.02
ovarioTotaldauerbispedauerbistotdauerpebistot3.0059.003.00625.81760.09134.28485.00707.0069.001608.001762.00628.00451.94428.11152.16
pankreasTotaldauerbispedauerbistotdauerpebistot1.0013.000.00200.11292.8892.77127.00219.0049.001322.001322.00801.00220.14248.10123.52
Page: &Z of Pages:&F
Job 1 - Means
The period between start of HPN and death amounts around 3
months, which is too late according to the definition of refractory
cachexia
The data indicates that the patients initiated HPN, receive it
too late
Average duration until HPN initiation per patient in days
Average period until HPN initiation and until death per patient
in each cancer indication
H&N CRC Ovarian Pancreas Gastric
No HPN 300 1,675 228 1,197 447
HPN 43 290 53 209 153
21
2016 2017 2018 2019 2020H&N PancreaticCRC Ovarian
Gastric
Average period until death per patient with HPN in days
The average period until initiation of HPN is approximately 337
days, which is similar to the average period from HPN initiation
until death (380 days)
Study Results Survival (3)
Diagramm1
376.7266.6
500.7394.5
760.1625.8
292.9200.1
355.5195.7
Sheet1
376.7500.7760.1292.9355.5
266.6394.5625.8200.1195.7
0 500 1000 1500 2000
Tage von 1st-Therapie bis erste PE (Gesamt)
0
200
400
600
800
1000
Tage
von
ers
ter P
E (G
esam
t) bi
s zu
m V
erst
erbe
n
Effekt der PE auf MortalittKohort: Magen
R-Quadrat= 0.0019
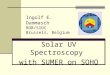
Correlation analysis Overall Survival of Gastric cancer
patients, n=153
Effect on cancer survival Gastric
0 500 1000 1500 2000
Tage von 1st-Therapie bis erste PE (Gesamt)
0
500
1000
1500
2000
Tage
bis
zum
Ver
ster
ben
Pat ohne PE
95% CI=(211.71-263.67)SD=279.51Mean=237.69Pat ohne PE:
Effekt auf berleben/MortalittKohort: Magen
R-Quadrat= 0.6159
Days from 1st line cancer Tx to first HPN initiationD
ays
from
1st
HPN
unt
il de
ath
Effect on cancer survival - Gastric
Days from 1st line cancer Tx to first HPN initiation
Day
s un
til d
eath
Patients without PN - - -
R2=0.0019R2=0.6159
Patients without PN
22
Average period until death: 339 days95% CI: 262-417 days
The average survival of Gastric cancer patients after first HPN
treatment initiation is approximately 118 days
Study Results Survival (4)
Patients without PNMean=237.69SD=279,5195%
CI=(211.71-263,67)
The largest share of HPN costs of total drug treatment costs is
observable in the gastric cancer patient groups
Ovarian cancer has the lowest share of HPN costs
The largest share of cancer drug costs can be seen in Head &
Neck and CRC cancer patient groups
23
9282 9694 9304
50273948
1823 945588
1937
2527
H&N CRC Ovarian Pancreatic GastricH&N CRC Ovarian
Pancreatic Gastric
16% 9%6%
28%39%
Share of cancer
drug costs
Share of HPN drug
costs
Share of HPN drug costs of total drug costs per patient in
(Q0-Q4)
The cost share between cancer & HPN therapies varies between
6% to 39%; in non-GI cancers the cost share of nutrition is lower
than of cancer drugs
Study Results Costs
Clinical nutrition use in oncology is currently very low, and
patterns of use do not allow to achieve the best possible patient
outcomes
Across five cancer types the share of patients who received HPN
is on average 16%, with the highest share observed in gastric
cancer patients (25%) and the lowest share (12%) amongst patents
with Head & Neck cancer
Up to 40% of patients, who were not artificially fed displayed
cachexia, which suggests a significant care deficiency in cancer
management. Patients who did not receive HPN also showed higher
rate of infections and other co-morbidities including decubitus
The study data suggested that patients who did not receive HPN
survived on average 70 days less, compared to those who did receive
HPN and lived longer, - which highlights the potential benefit of
HPN on overall survival
Across five tumor types the share of costs between cancer
treatment and home parenteral nutrition varies significantly; with
the lowest proportion of costs spent on HPN in comparison with
conventional cancer therapy was observed in patients with CRC,
ovarian and Head & Neck cancers
24
Summary
Early screening to identify patients at risk of malnutrition, as
well as best practices for targeted intervention, including
supplemental parenteral nutrition, will be key to improve patients
outcomes.
The benefits of appropriate clinical nutrition treatment
including overall survival, treatment tolerance and quality of life
have to be taken into consideration in patients at risk and/or
suffering from malnutrition.
Further research and a clear understanding of the current
practices to address benefits of clinical nutrition in oncology is
warranted.
Best practices needed to be delineated for early MN diagnosis
and clinical nutrition treatment further research is essential
25
Conclusion
Foliennummer 1Foliennummer 2Foliennummer 3Foliennummer
4Foliennummer 5Foliennummer 6Foliennummer 7Foliennummer
8Foliennummer 9Foliennummer 10Foliennummer 11Foliennummer
12Foliennummer 13Foliennummer 14Foliennummer 15Foliennummer
16Foliennummer 17Foliennummer 18Foliennummer 19Foliennummer
20Foliennummer 21Foliennummer 22Foliennummer 23Foliennummer
24Foliennummer 25