Embed Size (px)
Citation preview
WHO recommendations for the prevention and management of
tobacco use and second-hand smoke exposure
in pregnancy

WHO recommendations for the prevention and management of
tobacco use and second-hand smoke exposure in pregnancy
WHO recommendations for the prevention and management of
tobacco use and second-hand smoke exposure
in pregnancy 2013
Who Library cataloguing-in-publication data
WHO recommendations for the prevention and management of tobacco use and second-hand smoke exposure in pregnancy.
1.Smoking – prevention and control. 2.Tobacco smoke pollution - adverse effects. 3.Pregnancy. 4.Pregnancy outcome. 5.Prenatal exposure delayed effects. 6.Environmental exposure – adverse effects. 7.Guideline. I.World Health Organization.
ISBN 978 92 4 150607 6(NLM classification: QV 137)
© World Health Organization 2013
All rights reserved. Publications of the World Health Organization are available on the WHO web site (www.who.int) or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]).
Requests for permission to reproduce or translate WHO publications –whether for sale or for non-commercial distribution– should be addressed to WHO Press through the WHO web site (www.who.int/about/licensing/copyright_form/en/index.html).
The designations employed and the presentation of the material in this publication do not imply the expres-sion of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.
Printed in (country name)
contents
ACKNOWLEDGEMENTS 9
ABBREVIATIONS AND ACRONYMS 11
PREFACE 13
EXECUTIVE SUMMARY 15
Why these guidelines were developed 15Objectives and scope of the document 16Who should use these guidelines 16How these guidelines were developed 17Recommendations 18
INTRODUCTION AND SCOPE 21
Harms of tobacco use and second-hand smoke exposure in pregnancy 22Prevalence of tobacco use and second-hand smoke exposure 22Existing national guidelines on management of tobacco use in pregnancy 25Guiding global treaties and frameworks 25Pregnancy as a window of opportunity 26Objectives 26Target audience 27
PROCESS OF FORMULATING GUIDELINES 29
Individuals and partners involved in development of the guidelines 29WHO Steering Group 30Guidelines Development Group 30External Review Group 30Management of conflicts of interest 30The scope 31Evidence search and retrieval 32Evidence to recommendations 33Group process and decision-making 35
RECOMMENDATIONS 37
Recommendation 1: Assessment of tobacco use and second-hand smoke exposure in pregnancy 39Recommendation 2: Psychosocial interventions for tobacco-use cessation in pregnancy 44Recommendations 3–5: Use of pharmacotherapy for tobacco-use cessation in pregnancy 51Recommendations 6–7: Protection from second-hand smoke in pregnancy (smoke-free public places) 56Recommendations 8–9: Protection from second-hand smoke in pregnancy (smoke-free homes) 61
RESEARCH PRIORITIES 65
PLANS FOR DISSEMINATING, ADAPTING AND IMPLEMENTING THE RECOMMENDATIONS 69
Guidelines dissemination 69Local adaptation 69Local implementation 70Evaluating the impact of the guidelines 72
REVIEW AND UPDATE OF THE RECOMMENDATIONS 75
REFERENCES 77
Introduction and Methodology Section 77Recommendations 79
Recommendation 1 79Recommendation 2 80Recommendations 3–5 81Recommendations 6–7 81Recommendations 8–9 81
ANNEXES 83
ANNEX 1: Technical Secretariat for the guidelines development 83ANNEX 2: WHO staff (HQ, regions and country offices) involved in the guidelines development 84ANNEX 3: Guidelines Development Group 85 3.1 GDG membership 85 3.2 Background of Guidelines Development Group members 86 3.3 Consultants supporting the Guidelines Development Group 86ANNEX 4: External reviewers who contributed to development and/or peer review of questions and draft recommendations document 87ANNEX 5: Declaration of Interest 88 5.1. Guidelines Development Group 88 5.2. External peer reviewers 89 5.3. Consultants 89 5.4. Technical Secretariat 89ANNEX 6: GRADE profile summaries 90ANNEX 7: Decision tables summarizing the values, preferences and judgements made about the strength of the recommendations 97

ACkNOWLEDGEMENTS 9
Acknowledgements
The development of these guidelines was coordinated by Lubna Ishaq Bhatti, Department of Prevention of Noncommunicable Diseases, World Health Organization (PND/WHO) under the supervision of Edouard Tursan d’Espaignet and Douglas Bettcher (PND/WHO).
This document is the result of collaboration between the PND/WHO and a large number of international agencies and organizations active in the field of tobacco and reproductive health. Funding and technical support for this project was provided by the Government of the United States of America through the US Centers for Disease Control and Prevention (CDC), and the U.S. National Cancer Institute (NCI). This support is gratefully acknowledged.
The technical secretariat included: Lubna Ishaq Bhatti and Edouard Tursan d’Espaignet (PND/WHO), Nicolas Clark and Vladimir Poznyak (MSD/WHO), Michele Bloch (NCI), Patricia Dietz, Lucinda England, Italia V Rolle and Van T Tong (CDC). (see Annex 1 for affiliations).
The project had a WHO Steering Group with members as: Avni Amin, Toker Erguder, Dongbo Fu, Helena Maria Nygren krug, Mathews Mathai, Mario Merialdi, James Rarick and Daravuth Yel (see Annex 2 for affiliations). Thanks are due to the staff at the WHO Guidelines Review Committee Secretariat for their support throughout the process.
Fernando Althabe, Linda Bauld, Jacqueline Bell, Yves Bergevin, Sophia Chan, Monique Chayya, Prakash Gupta (chair), Margaretha Haglund, Fatanah Ismail, katherine Murphy, Isabel Nerin, and Cheryl Oncken served as members of the Guidelines Development
10 ACkNOWLEDGEMENTS
Group (see Annex 3 for affiliations). Following experts contributed to the development of PICO questions and\or peer review of the draft guidelines: Wagida A. Anwar, Vincenzo Berghella, Naowarut Charoenca, kim Dickson, Bing Guthrie, James A Litch, Laura Llambí, Jeanne Mahoney, Saritha Nair, Emília Nunes, Qi Shi, Jorge Tolosa, and Michael Ussher. (see Annex 4 for affiliations).
Methodological support for producing the GRADE evidence tables and the balance work-sheets was provided by Margaret Harris (independent consultant).
Administrative support was provided by Carolyn Patten and Elizabeth Tecson.
WHO interns who offered support at various stages: Samantha kent, Helen Tam-Tham, Jessica Zamora.
WHO also wishes to thank the authors of the various systematic reviews used in these guidelines for their assistance and collaboration in updating them, especially Catherine Chamberlain (Monash University), and Shabana Abdullah and Jennifer Schindler (BLH Technologies, Inc.). WHO is also grateful to the Cochrane Pregnancy and Childbirth Group for their support in updating the Cochrane reviews. We are grateful to Tim Coleman and kate Flemming for sharing pre-publication copies of their systematic reviews to facilitate our work.
Special thanks are due to our copyeditor and proofreader Ms Angela Newill. We also thank the designer Ana Sabino.
ABBREVIATIONS AND ACRONYMS 11
Abbreviations and Acronyms
AusAID Australian Agency for International Development ANC antenatal care CDC Centers for Disease Control and Prevention, United States CI Confidence intervalCOP Conference of Parties (WHO Framework Convention for Tobacco Control)DFID Department for International Development, United kingdom ES Effect sizeFCTC Framework Convention for Tobacco ControlGDG Guidelines Development GroupGRADE Grading of Recommendations Assessment, Development and Evaluation GRC Guidelines Review CommitteeHMIS Health Management Information SystemHQ headquartersLBW Low birth weightLMIC Low- and/or middle-income countriesMSB Management of Substance AbuseNCI National Cancer Institute, United StatesNRT nicotine replacement therapyNGO Nongovernmental Organization
12 ABBREVIATIONS AND ACRONYMS
NORAD Norwegian Agency for Development Cooperation OR odds ratioPICO Population/Patient group, Intervention, Comparator and outcomeRCT Randomized controlled trialRR Relative riskSD Standard deviationSGA Small for gestational ageSHS second-hand smokeST smokeless tobaccoTFI Tobacco Free InitiativeUNFPA United Nations Population Fund UNICEF United Nations Children’s FundUSAID United States Agency for International DevelopmentVLBW Very low birth weightWHO World Health Organization
PREFACE 13
Preface
The current document makes recommendations on the prevention and management of tobacco use and second-hand smoke exposure in pregnancy. These recommendations are part of a larger project of the Noncommunicable Diseases and Mental Health (NMH) cluster of the World Health Organization (WHO). The aim is to make recommendations regarding the management of substance abuse in pregnancy, covering tobacco, alcohol and other psychoactive substances. Recommendations on alcohol and other psychoactive substances are expected to be available in 2014.

14
EXECUTIVE SUMMARY 15
Executive Summary
WHY THESE GUIDELINES WERE DEVELOPED
Exposure to tobacco smoke affects all stages of human reproduction. Tobacco smoking affects both male and female fecundity. Maternal cigarette smoking is associated with increased risks for ectopic pregnancy, premature rupture of membranes, abruptio pla-centae, placenta previa, miscarriage, stillbirth, preterm birth, low birth weight, small for gestational age, and congenital anomalies such as cleft lip. After birth, the risk for sudden infant death syndrome (SIDS) is increased among the offspring of women who smoked during or after pregnancy. The harms of tobacco use in pregnancy are not limited to smoked tobacco products only. Evidence suggests that infants born to women who use smokeless tobacco in pregnancy have a higher risk of several adverse outcomes such as stillbirth, preterm birth, and low birth weight. Additionally, maternal exposure to second-hand smoke (SHS) in pregnancy has also been associated with a modest reduction in birth weight, and can increase the risk of low birth weight (<2500 g) by 22%.
There are currently no up-to-date, evidence-based guidelines for identifying and managing tobacco use and exposure to SHS in pregnancy in most of the low- and middle-income countries. Most of the existing national guidelines are from high-income countries, and although they provide advice on the management of cigarette smoking in pregnancy (probably the most prevalent form of tobacco use in those countries), they do not ad-dress other forms of smoked tobacco or use of smokeless tobacco in pregnancy. Most of these guidelines also do not discuss recommendations on avoiding exposure to SHS
16 EXECUTIVE SUMMARY
in pregnancy, although some have addressed the smoking status of partners and other household members as a factor affecting pregnant women’s tobacco-cessation efforts and quit attempts.
OBjECTIVES AND SCOPE OF THE DOCUMENT
The primary objective of these guidelines is to reduce tobacco use and SHS exposure in pregnant women by providing evidence-based recommendations to health-care provid-ers and other related service providers on i) identification, management, and prevention of tobacco use and SHS exposure in pregnant women and ii), where relevant, advice for other members of their household on how to reduce SHS exposure of pregnant women.
In what follows, the pregnancy period is defined as ‘from the first antenatal care contact up to six weeks postpartum’.
These guidelines cover the following issues:
• Elements necessary for effective screening of pregnant women for tobacco use (smoked
and smokeless) and SHS exposure
• Safety and effectiveness of psychosocial interventions for tobacco use in pregnancy
• Safety and effectiveness of pharmacological treatment for tobacco use in pregnancy
• Effective interventions for reducing SHS exposure
I) at work and in public places
II) at home
WHO SHOULD USE THESE GUIDELINES
The target audience of these guidelines includes health-care professionals involved in the care and treatment of pregnant women in a health-facility setting (including general medi-cal practitioners, family physicians, obstetricians, midwives, nurses and other health-care workers). Many of the recommendations are also relevant for traditional birth attendants and community health workers who provide antenatal care to pregnant women in their homes. These guidelines are also intended for public-health policy-makers, health-care programme managers, health-facility managers, and health-care workers in setting up systems for optimal identification and management of tobacco use and SHS exposure in pregnancy.

EXECUTIVE SUMMARY 17
HOW THESE GUIDELINES WERE DEVELOPED
Guideline groups: A WHO steering group comprising members from relevant WHO departments (see Annex 2) was set up in January 2011. The WHO Tobacco Free Initiative (TFI)1 and Management of Substance Abuse (MSB) led the development of these guide-lines in collaboration with other WHO departments, the Division of Reproductive Health and the Office on Smoking and Health, the Centers for Disease Control and Prevention (CDC), USA and the Tobacco Control Research Branch, National Cancer Institute (NCI), USA. A Technical Secretariat was also established, consisting of the lead technical officers from WHO (TFI and MSB) and researchers from CDC and NCI. The Technical Secretariat established the provisional scope of the guidelines and selected members of the Guide-line Development Group (GDG) to reflect all WHO regions and appropriate expertise and achieve a gender balance (see Annex 3). A larger group of external reviewers (see Annex 4) commented on the PICO (Population, Intervention, Comparator, Outcomes) questions, draft recommendations and final documents. Their comments were considered by GDG.
Evidence search and retrieval: The Technical Secretariat drafted a list of scoping ques-tions and outcomes related to the identification and management of tobacco use and SHS exposure. These questions were provided to a group of international stakeholders (nurses, midwives, obstetricians, gynaecologists, researchers, experts in research synthesis, experts in health-care programmes, and consumer representatives) to review and prioritize the draft questions and outcomes. The revised scoping questions were modified and agreed upon during several electronic consultations with the GDG. Further consultations with the GDG involved review of scoping questions phrased using the PICO format. A set of scoping questions was finalized by the end of May 2011. These were then used to guide searches for relevant systematic reviews that had been performed within the past two years and had met inclusion criteria. Where relevant systematic reviews (a) did not exist, (b) were not recent (i.e. had not been done within the past two years), or (c) were not of suitable quality or applicability, new systematic reviews were commissioned.
Evidence to recommendations: The WHO Handbook for Guidelines Development was followed and the GRADE2 system for assessing quality of evidence and using evidence to inform decisions was applied to inform drafting of recommendations. For each ques-tion, an evidence profile was developed summarizing the evidence retrieved, including discussion of values, preferences, benefits, harms and feasibility. Wherever possible, the
1 The Tobacco Free Initiative department was renamed in 2013 as Prevention of Noncommunicable Diseases (PND).2 GRADE = Grading of Recommendations Assessment, Development and Evaluation.
18 EXECUTIVE SUMMARY
evidence retrieved was graded and GRADE tables provided. A decision table was used by the GDG during a recommendation drafting meeting in Geneva, Switzerland (September 2012) to agree on the quality of evidence and certainty about harms and benefits, values and preferences, feasibility and resource implications (see Annex 7 for details of each decision). The strength of the recommendation was assessed as either:
‘strong’: indicating that the GDG agrees that the quality of the evidence combined with
certainty about the values, preferences, benefits and feasibility of the recommendation
means that it should be done in most circumstances;
or ‘conditional’: indicating that there was less certainty about the combined quality of evidence
and its values, preferences, benefits and feasibility of this recommendation meaning that
there may be circumstances in which it will not apply.
On a number of occasions, the GDG decided to give a strong recommendation despite a GRADE assessment of the available evidence on effect as being of ‘very low’ or ‘low’ quality. This occurred when the following conditions applied: (a) when there was agreement that expected benefits outweighed harms and burdens for critical outcomes, (b) when the ex-pected values and preferences of the target population and their community were clearly in favour of the recommendation, and (c) when there was agreement that the expected benefits would not consume disproportionate resources.
RECOMMENDATIONS
This guidance includes nine recommendations for the prevention and management of tobacco use and SHS exposure in pregnancy. To assist in the formulation of recommen-dations, the GDG outlined a number of overarching principles that it believed should underpin all recommendations for optimal identification and management of tobacco use by, and SHS exposure in, pregnant women. These principles are based on the hu-man rights and ethics values, outlined in the WHO Framework Convention for Tobacco Control (WHO FCTC), the Convention on the Elimination of All Forms of Discrimination against Women (CEDAW) and the Programme of Action of the International Conference on Population and Development (ICPD). These principles, together with the suggested implementation strategies and indicators for monitoring and evaluation presented later in the document, should guide stakeholders and policy-makers in the process of plan-ning, implementing and evaluating the most suitable and relevant recommendation for their own circumstances. Each recommendation is followed by specific related remarks which are intended to explain the context in which these recommendations were made.
TO BE REPLACED 19
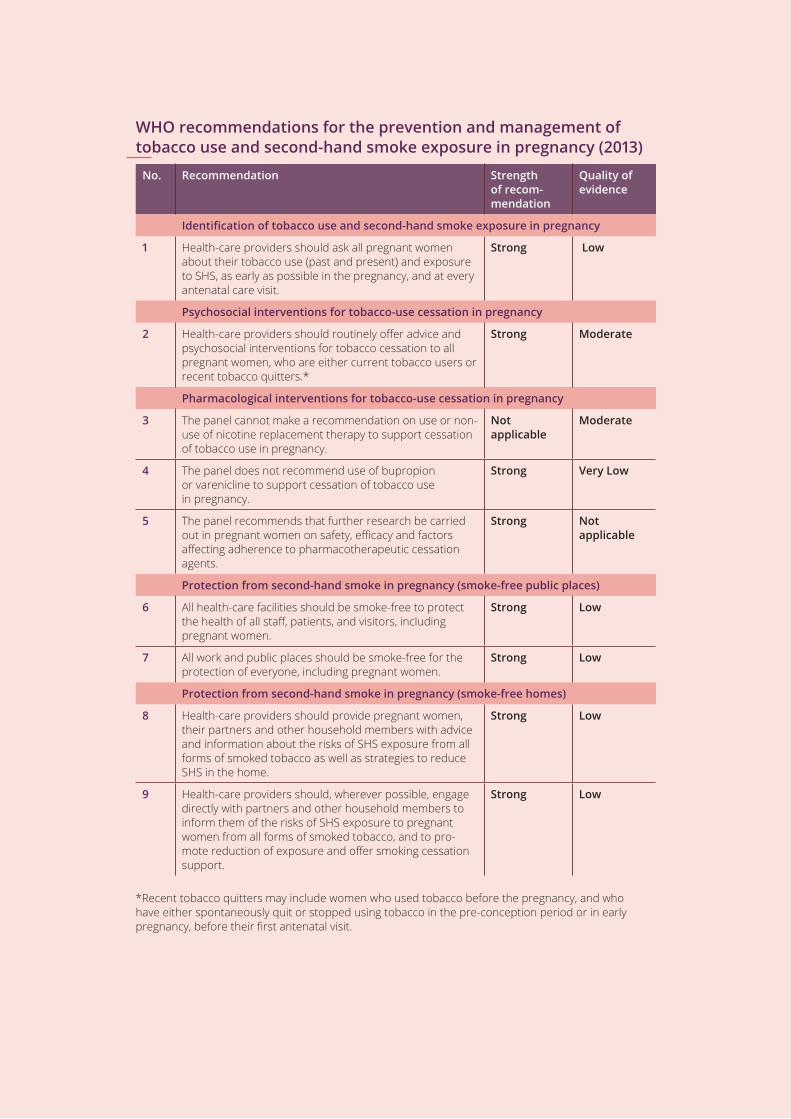
WHO recommendations for the prevention and management of tobacco use and second-hand smoke exposure in pregnancy (2013)
No. Recommendation Strength of recom-mendation
Quality of evidence
Identification of tobacco use and second-hand smoke exposure in pregnancy
1 Health-care providers should ask all pregnant women about their tobacco use (past and present) and exposure to SHS, as early as possible in the pregnancy, and at every antenatal care visit.
Strong Low
Psychosocial interventions for tobacco-use cessation in pregnancy
2 Health-care providers should routinely offer advice and psychosocial interventions for tobacco cessation to all pregnant women, who are either current tobacco users or recent tobacco quitters.*
Strong Moderate
Pharmacological interventions for tobacco-use cessation in pregnancy
3 the panel cannot make a recommendation on use or non-use of nicotine replacement therapy to support cessation of tobacco use in pregnancy.
Not applicable
Moderate
4 The panel does not recommend use of bupropion or varenicline to support cessation of tobacco use in pregnancy.
Strong Very Low
5 The panel recommends that further research be carried out in pregnant women on safety, efficacy and factors affecting adherence to pharmacotherapeutic cessation agents.
Strong Not applicable
Protection from second-hand smoke in pregnancy (smoke-free public places)
6 All health-care facilities should be smoke-free to protect the health of all staff, patients, and visitors, including pregnant women.
Strong Low
7 All work and public places should be smoke-free for the protection of everyone, including pregnant women.
Strong Low
Protection from second-hand smoke in pregnancy (smoke-free homes)
8 Health-care providers should provide pregnant women, their partners and other household members with advice and information about the risks of SHS exposure from all forms of smoked tobacco as well as strategies to reduce SHS in the home.
Strong Low
9 Health-care providers should, wherever possible, engage directly with partners and other household members to inform them of the risks of SHS exposure to pregnant women from all forms of smoked tobacco, and to pro-mote reduction of exposure and offer smoking cessation support.
Strong Low
*Recent tobacco quitters may include women who used tobacco before the pregnancy, and who have either spontaneously quit or stopped using tobacco in the pre-conception period or in early pregnancy, before their first antenatal visit.

20
INTRODUCTION AND SCOPE 21
introduction and scope
Tobacco is the only legal product that kills a large proportion of its consumers when used as intended by manufacturers. The World Health Organization (WHO) estimates that tobacco use is currently responsible for almost six million deaths each year – one death every six seconds. Unless strong action is taken to curb the tobacco epidemic, this number is projected to rise to eight million deaths per year by 2030 (1).
Tobacco comes in smoked and smokeless forms, both of which have been shown to cause adverse outcomes in pregnant women and their fetuses. Smoked forms of tobacco include various kinds of cigarettes (manufactured or hand-rolled), cigars, pipes and waterpipes.1 While cigarettes – particularly manufactured cigarettes – are by far the main form of smoked tobacco product globally, in many countries other forms of smoked tobacco are also predominant, including bidis and waterpipes. Smokeless tobacco is defined as use of a tobacco product with no combustion at the time of the use. A wide variety of smokeless tobacco products are available, for oral or nasal use. Products intended for oral use are sucked, chewed (dipped), gargled or applied to the gums or teeth, while fine tobacco mixtures are inhaled into the nostrils (2). Second-hand tobacco smoke (SHS) comprises the smoke released from the burn-ing tip of a cigarette (or other smoked tobacco product) between puffs (called sidestream smoke) and the smoke exhaled by the smoker (exhaled mainstream smoke) (3).
1 Waterpipes are also known as hookah, shisha, arghileh and narghile.
22 INTRODUCTION AND SCOPE
HARMS OF TOBACCO USE AND SECOND-HAND SMOKE EXPOSURE IN PREGNANCY
Exposure to tobacco smoke affects all stages of human reproduction. Tobacco smok-ing affects both male and female fecundity (4). maternal cigarette smoking is associated with increased risks for ectopic pregnancy, premature rupture of membranes, abruptio placentae, placenta previa, miscarriage, stillbirth, preterm birth, low birth weight, small for gestational age, and congenital anomalies such as cleft lip (4). After birth, the risk for sud-den infant death syndrome (SIDS) is increased among the offspring of women who smoked during or after pregnancy (5, 6). Some of these conditions, such as low birth weight and preterm birth, could have lifelong consequences including a heightened risk of developing chronic diseases in adulthood (7). The harms of tobacco use in pregnancy are not limited to smoked tobacco products only. Evidence suggests that infants born to women who use smokeless tobacco in pregnancy have a higher risk of several adverse outcomes such as stillbirth, preterm birth, and low birth weight (8–13).
The negative impact of tobacco smoking on birth outcomes is not limited to its direct use by the mother.
Maternal exposure to SHS in pregnancy has also been associated with a modest reduc-tion in birth weight, and can increase the risk of low birth weight (<2500 g) by 22% (14)
In addition to directly affecting the health of women and children, tobacco use also has indirect effects on health by increasing the risk of poverty at the individual, household and national levels (15). At the individual and household level, money spent on tobacco can have a very high opportunity cost. For the poor, money spent on tobacco is money not spent on basic necessities, such as food, transportation, housing, and health care, thus increasing the risk of adverse health outcomes for pregnant women and their fetuses (15).
PREVALENCE OF TOBACCO USE AND SECOND-HAND SMOKE EXPOSURE
Globally, 22% of the world’s adult population aged 15 years and over are estimated to be current tobacco smokers, including 36% of men and 8% of women (see Table 1). The WHO European and Americas regions have the highest prevalence of current tobacco smoking among adult women (16). There is a stark difference in smoking rates between women of low income and lower-middle income countries (whose tobacco smoking rates are very low) and women of upper-middle-income and high-income countries (whose tobacco smoking rates are very high).
INTRODUCTION AND SCOPE 23
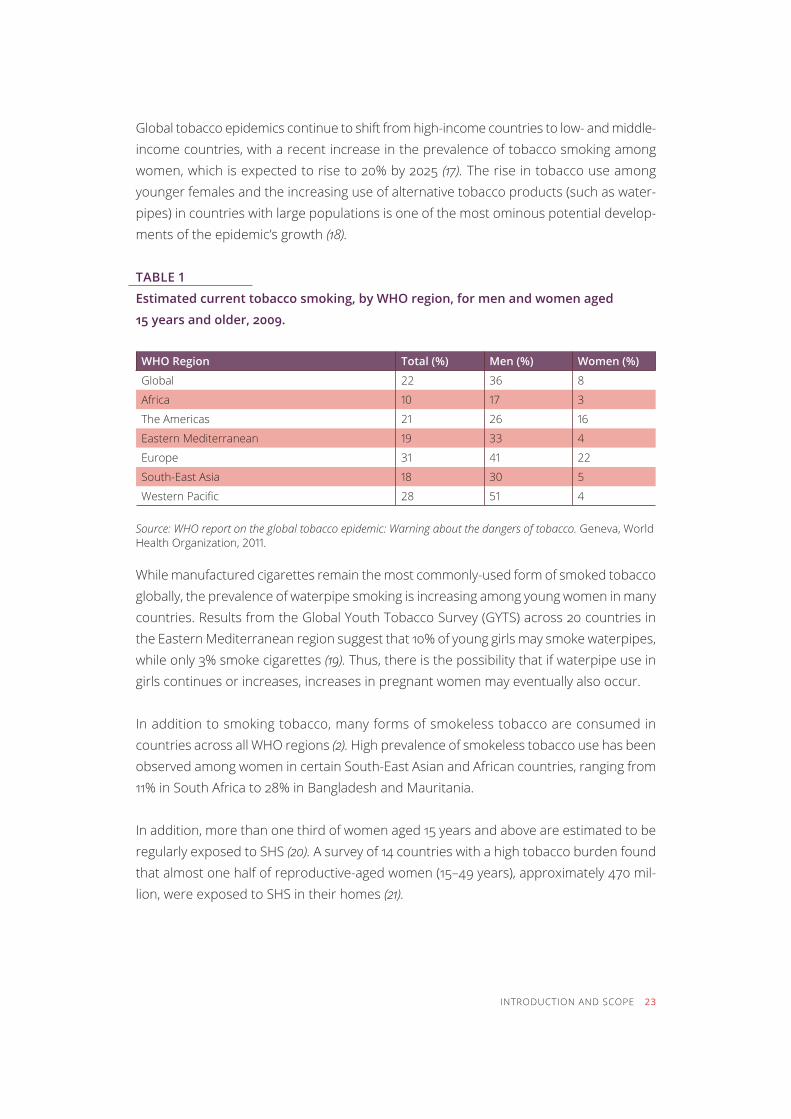
Global tobacco epidemics continue to shift from high-income countries to low- and middle-income countries, with a recent increase in the prevalence of tobacco smoking among women, which is expected to rise to 20% by 2025 (17). the rise in tobacco use among younger females and the increasing use of alternative tobacco products (such as water-pipes) in countries with large populations is one of the most ominous potential develop-ments of the epidemic’s growth (18).
TabLe 1
Estimated current tobacco smoking, by WHO region, for men and women aged
15 years and older, 2009.
WHO Region Total (%) Men (%) Women (%)
global 22 36 8
Africa 10 17 3
the americas 21 26 16
eastern mediterranean 19 33 4
europe 31 41 22
south-east asia 18 30 5
Western Pacific 28 51 4 Source: WHO report on the global tobacco epidemic: Warning about the dangers of tobacco. Geneva, World Health Organization, 2011.
While manufactured cigarettes remain the most commonly-used form of smoked tobacco globally, the prevalence of waterpipe smoking is increasing among young women in many countries. Results from the Global Youth Tobacco Survey (GYTS) across 20 countries in the Eastern Mediterranean region suggest that 10% of young girls may smoke waterpipes, while only 3% smoke cigarettes (19). Thus, there is the possibility that if waterpipe use in girls continues or increases, increases in pregnant women may eventually also occur.
In addition to smoking tobacco, many forms of smokeless tobacco are consumed in countries across all Who regions (2). High prevalence of smokeless tobacco use has been observed among women in certain South-East Asian and African countries, ranging from 11% in South Africa to 28% in Bangladesh and Mauritania.
In addition, more than one third of women aged 15 years and above are estimated to be regularly exposed to shs (20). A survey of 14 countries with a high tobacco burden found that almost one half of reproductive-aged women (15–49 years), approximately 470 mil-lion, were exposed to SHS in their homes (21).
24 INTRODUCTION AND SCOPE
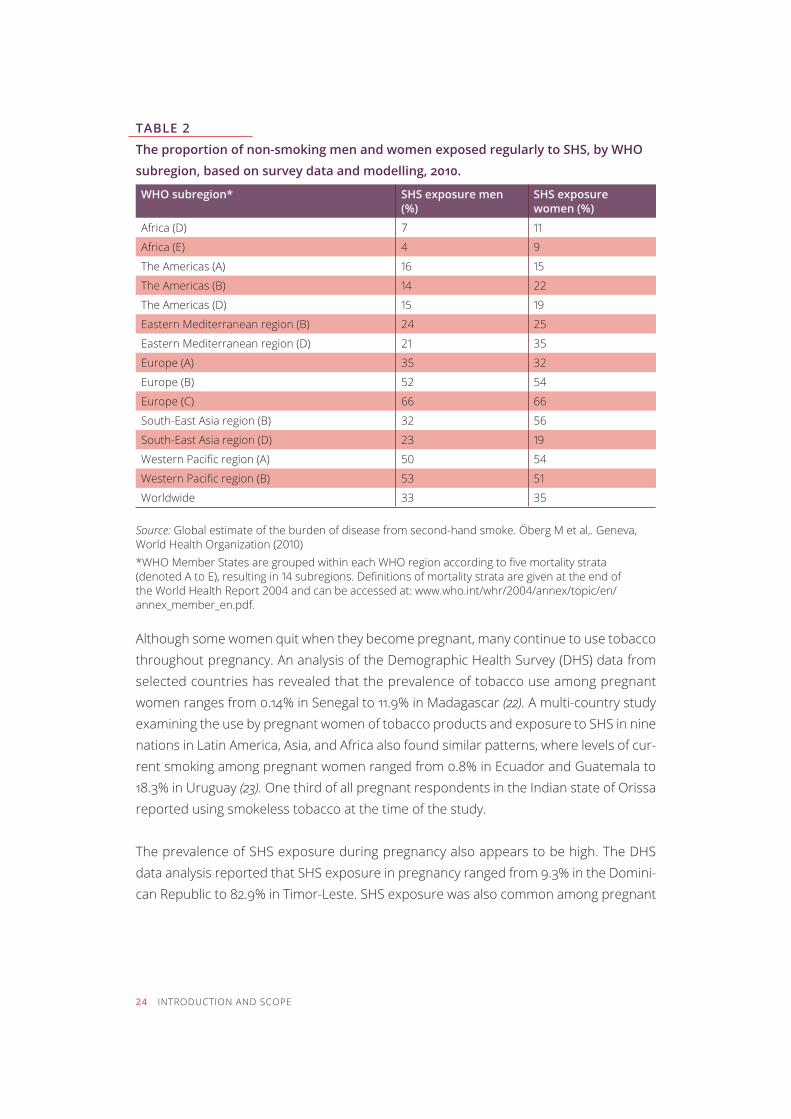
TABLE 2
The proportion of non-smoking men and women exposed regularly to SHS, by WHO
subregion, based on survey data and modelling, 2010.
WHO subregion* SHS exposure men (%)
SHS exposure women (%)
Africa (D) 7 11
Africa (E) 4 9
The Americas (A) 16 15
The Americas (B) 14 22
The Americas (D) 15 19
Eastern Mediterranean region (B) 24 25
Eastern Mediterranean region (D) 21 35
Europe (A) 35 32
Europe (B) 52 54
Europe (C) 66 66
South-East Asia region (B) 32 56
South-East Asia region (D) 23 19
Western Pacific region (A) 50 54
Western Pacific region (B) 53 51
Worldwide 33 35 Source: Global estimate of the burden of disease from second-hand smoke. Öberg M et al,. Geneva, World Health Organization (2010) *WHO Member States are grouped within each WHO region according to five mortality strata (denoted A to E), resulting in 14 subregions. Definitions of mortality strata are given at the end of the World Health Report 2004 and can be accessed at: www.who.int/whr/2004/annex/topic/en/annex_member_en.pdf.
Although some women quit when they become pregnant, many continue to use tobacco throughout pregnancy. An analysis of the Demographic Health Survey (DHS) data from selected countries has revealed that the prevalence of tobacco use among pregnant women ranges from 0.14% in Senegal to 11.9% in Madagascar (22). a multi-country study examining the use by pregnant women of tobacco products and exposure to SHS in nine nations in Latin America, Asia, and Africa also found similar patterns, where levels of cur-rent smoking among pregnant women ranged from 0.8% in Ecuador and Guatemala to 18.3% in Uruguay (23). One third of all pregnant respondents in the Indian state of Orissa reported using smokeless tobacco at the time of the study.
The prevalence of SHS exposure during pregnancy also appears to be high. The DHS data analysis reported that SHS exposure in pregnancy ranged from 9.3% in the Domini-can Republic to 82.9% in Timor-Leste. SHS exposure was also common among pregnant
INTRODUCTION AND SCOPE 25
women in the multi-country study mentioned earlier, and between 17.1% in the Democratic Republic of the Congo and 91.6% in Pakistan of pregnant women reported that smoking was permitted in their homes.
EXISTING NATIONAL GUIDELINES ON MANAGEMENT OF TOBACCO USE IN PREGNANCY
Guidelines on the management of tobacco dependence in pregnancy are available for some high-income countries such as Australia, Canada, the United kingdom and the USA; however, few if any low- and middle-income countries have such guidelines. Most of the existing national guidelines provide advice on how to manage cigarette smoking in pregnancy, but do not address other forms of smoked tobacco or the use of smokeless tobacco in pregnancy. Most guidelines do not discuss recommendations on avoiding ex-posure to SHS in pregnancy, and few address how having partners and other household members who smoke, adversely affects pregnant women’s tobacco-cessation efforts.
The proposed guidance addresses not only the active use of various forms of tobacco by pregnant women, but also exposure of the pregnant women and their fetuses to second-hand smoke.
GUIDING GLOBAL TREATIES AND FRAMEWORKS
In developing these recommendations, the team of experts assembled by WHO were guided by the WHO Framework Convention on Tobacco Control (WHO FCTC) (24). the Convention is an evidence-based treaty that reaffirms the right of all people to the high-est standard of health. In its preamble, the WHO FCTC (i) acknowledges that there is clear scientific evidence that prenatal exposure to tobacco smoke causes adverse health and developmental conditions for children; (ii) notes with alarm the increase in smoking and other forms of tobacco consumption by women and young girls worldwide; and (iii) calls for full participation of women at all levels of policy-making and implementation of the FCTC and the need for gender-specific tobacco control strategies.
The WHO FCTC guidelines and protocols provide orientation towards demand-reduction measures that can be put in place to manage tobacco use in pregnancy. These measures, already agreed upon by the overwhelming majority of countries that have signed the Convention, include protection from exposure to second-hand smoke, education, com-munication, training and public awareness, as well as demand-reduction measures linked to tobacco dependence and cessation.
26 INTRODUCTION AND SCOPE
There is emerging evidence that many of the chronic diseases that assail the world today (cardiovascular diseases, cancers, respiratory and metabolic diseases) have their origins in fetal life (7). The guidelines set out in this document will add to the existing tools avail-able to promote the UN Millennium Development Goals 4 and 5 that call on all nations to take immediate action to improve maternal and child health (25), as well as the more recent UN agenda on noncommunicable diseases as set in the UN High Level Meeting held in September 2011 in New York (26).
PREGNANCY AS A WINDOW OF OPPORTUNITY
Pregnancy is theorized as a ‘teachable moment’ for women, when their perception of health risk is heightened (27, 28). Pregnancy is a time of preparedness and tobacco ces-sation, not only for women, but also for their partners and other people living in their households. A study from Lebanon found that up to 40% of husbands changed their smoking behaviour when their wives were pregnant (29).
According to UN estimates, in 2010 there were 137 million births globally (30). At least 80% of pregnant women received antenatal care (ANC) provided by skilled health personnel (doctors, nurses, or midwives) at least once during their pregnancy, with 53% of women receiving antenatal care four or more times (31). This predictable interaction with the health-care system provides an opportunity to identify and address tobacco use and ex-posure to SHS with over 137 million pregnant women, their partners and other household members. This interaction with the health-care system also provides an opportunity to encourage women to quit tobacco use while they are still relatively young and healthy, and before they develop a tobacco-related disease. Quitting early in life (at 25–34 years of age) can save up to 10 years of life (32). Besides protecting the immediate health of the pregnant woman and her developing child, cessation has long-term health benefits for women, infants and children, and other family members.
OBjECTIVES
The primary objective of this guidance is to reduce tobacco use and SHS exposure in pregnant women by providing evidence-based recommendations to health-care provid-ers and other related service providers on i) identification, management, and prevention of tobacco use and SHS exposure in pregnant women and ii), where relevant, advice for other members of their household on how to reduce SHS exposure of pregnant women.
INTRODUCTION AND SCOPE 27
TARGET AUDIENCE
The target audience of these guidelines includes health-care professionals involved in the care and treatment of pregnant women in a health facility setting (including general medical practitioners, family physicians, obstetricians, physicians, midwives, nurses, and other health-care workers). Many of the recommendations are also relevant for traditional birth attendants and community health workers who provide antenatal care to pregnant women in their homes. These guidelines are also intended for public health policy-makers, health-care programme managers, health-facility managers, and health-care workers in setting up systems for optimal identification and management of tobacco use and SHS exposure in pregnancy.
The guidance provided is evidence-based and covers selected topics related to the man-agement of tobacco use and SHS exposure in pregnancy that were regarded as critical by an international, multidisciplinary group of health-care workers, public health research-ers, potential consumers of guidelines and other stakeholders. These guidelines are not intended as a globally comprehensive guide on management of tobacco use or SHS exposure in pregnancy. By providing broad guidance internationally, WHO assumes that countries will adapt and implement these recommendations to accommodate the political and health-systems context in which they operate.

28
PROCESS OF FORMULATING GUIDELINES 29
Process of Formulating Guidelines
The recommendations represent the work of WHO in supporting the use of evidence-based policies and practices in all countries. The guidelines were developed through standardized operating procedures described in the WHO Handbook for Guidelines De-velopment (33).
INDIVIDUALS AND PARTNERS INVOLVED IN DEVELOPMENT OF THE GUIDELINES
The WHO Tobacco Free Initiative (TFI)1 and Management of Substance Abuse (MSB) led the development of these guidelines in collaboration with other WHO departments, the Division of Reproductive Health and the Office on Smoking and Health, the Centers for Disease Control and Prevention (CDC), USA and Tobacco Control Research Branch, Na-tional Cancer Institute (NCI), USA. A Technical Secretariat was also established, consisting of the lead technical officers from WHO (TFI and MSB) and researchers from CDC and NCI. the technical secretariat both coordinated the research syntheses and other materials needed for the guidelines and led the development of the guidelines document. (A full list of names of members of the Technical Secretariat is provided in Annex 1.)
1 After internal realignment, the Tobacco Free Initiative was renamed in 2013 as the Prevention of Noncommunicable Diseases (PND) department.
30 PROCESS OF FORMULATING GUIDELINES
WHO STEERING GROUP
The WHO Steering Group consisted of staff members from the following WHO depart-ments: Gender, Equity and Human Rights (GER); Maternal, Newborn, Child and Adoles-cent Health (MCA); Mental Health and Substance Abuse (MSB); Reproductive Health and Research (RHR); and Tobacco Free Initiative (TFI). In addition to the above listed WHO HQ departments, TFI Headquarters (HQ) staff consulted extensively with WHO regional and country offices colleagues involved in tobacco control and the WHO Guidelines Review Committee (GRC) secretariat. (A full list of names of members of the WHO Steering Group is provided in Annex 2.)
GUIDELINES DEVELOPMENT GROUP
The Guidelines Development Group (GDG) was made up of people with content expertise in tobacco and\or reproductive health, relevant experience in low- and middle-income countries and expertise in evidence-based guidelines development. The GDG selection also took into consideration the need to ensure gender balance and regional diversity.
A consultant with expertise in evidence review and GRADE methodology supported the GDG. (A full list of the GDG and consultants along with their expertise, affiliations and geographical base is provided in Annex 3.)
EXTERNAL REVIEW GROUP
External reviewers were drawn from prospective end-users of these guidelines, interna-tional agencies, and partners working in the areas of tobacco and\or reproductive health. (A full list of names, affiliations, areas of interest and geographical base of the reviewers is provided in Annex 4.)
External reviewers were asked to evaluate and comment on the final recommendations. Reviewer response was compiled and comments used to revise the recommendations which were then circulated to the GDG for final agreement.
MANAGEMENT OF CONFLICTS OF INTEREST
The procedures for management of conflicts of interests followed the WHO Guidelines for Declaration of Interests (available on request from the secretariat). All GDG members,
PROCESS OF FORMULATING GUIDELINES 31
external reviewers and consultants completed the WHO Declaration of Interest forms. These were then reviewed by the secretariat for potential conflicts of interest (see summary in Annex 5). The WHO FCTC precludes the inclusion of anyone from the tobacco industry. As a consequence all GDG members and reviewers had to formally acknowledge having no links with the industry. At the beginning of the recommendation development meeting, all members of the GDG received a briefing regarding conflict of interests and were asked to discuss and declare to the meeting any conflicts they may have. Some observers (Dr Patricia Dietz and Ms Van Tong) were supported by their respective organization to partici-pate at the meeting. Dr Prakash Gupta declared that he had received consultancy funds from the Institute for Community Health, Hartford USA and National Institute for Research in Reproductive Health, Mumbai, India for a project on use of smokeless tobacco among Indian women in the previous year (2011). Dr Linda Bauld declared that she had served as the United kingdom government’s scientific adviser on tobacco control (2007–2010) and had recieved research funding from the National Institute of Clinical Excellence (NICE), the United kingdom, in 2009 to conduct a systematic review that informed the United kingdom guidance on smoking in pregnancy. Dr Cheryl Oncken declared a conflict of in-terest, financial and academic, as she was conducting a randomized controlled trial (RCT) of nicotine replacement therapy (NRT) and had received donated nicotine and placebo inhalers from Pfizer Inc. She did not participate in decision-making on recommendations about use of pharmacotherapy for tobacco cessation in pregnancy.
THE SCOPE
The scope of the guidelines was established by researching existing national guidelines (as described above) and the needs of the target population. It was agreed the guidelines should include the pregnancy period defined as: ‘from the first antenatal care contact up to six weeks postpartum.’
The Technical Secretariat drafted a list of questions and outcomes related to the identifica-tion and management of tobacco use and SHS exposure in pregnancy. These questions were provided to a group of international stakeholders (nurses, midwives, obstetricians, gynaecologists, researchers, experts in research synthesis, experts in health-care pro-grammes, and consumer representatives) to review and prioritize the draft questions and outcomes (via online consultations and at a side meeting at the World Conference on Tobacco or Health, Singapore 2012). The stakeholders commented on the importance of the drafted questions and outcomes and rated them. The international stakeholders were encouraged to revise the questions or suggest new questions and outcomes.
The following five scoping questions were finalized, and used in PICO2 format as guidance for evidence search and review:
1. What are the necessary elements for effective screening of pregnant women for smoking
and smokeless tobacco use?
2. Is use of psychosocial interventions for tobacco dependence safe and effective in
pregnancy?
3. Is use of pharmacological treatment for tobacco dependence safe and effective in
pregnancy?
4. What interventions are effective for preventing SHS exposure of pregnant women at
health-care facilities, workplaces and public places?
5. What interventions are effective for reducing SHS exposure to pregnant women in the
home?
EVIDENCE SEARCH AND RETRIEVAL
The Technical Secretariat coordinated efforts to review and synthesize the evidence on the identified PICO questions.
A literature search of the Cochrane Database, OVID-Medline and the Campbell Collabora-tion Library of systematic reviews was conducted in January to February 2011 to identify recent high quality, systematic reviews that were relevant to the priority PICO questions. Cochrane systematic reviews of randomized controlled trials were the primary source of evidence for the recommendations. On the basis of the list of selected questions and outcomes, the Technical Secretariat identified the relevant Cochrane systematic reviews and determined whether they needed to be updated. TFI also contacted the Cochrane Pregnancy and Childbirth Group and Cochrane Tobacco Addiction Group to identify any systematic reviews that may have been in the process of being updated. In addition, in the initial electronic search for each question, recognized experts in the field were contacted to identify unpublished studies that were not publicly available.
When data were not available or not up to date from these sources, systematic reviews were commissioned.
2 PICO is a standard format for framing research questions in evidence-based guidelines development:P=population or problem; I=intervention; C=control or comparison; O=outcomes.
32 PROCESS OF FORMULATING GUIDELINES
Studies from low- and middle-income as well as high-income countries were considered for inclusion in evidence reviews. Efforts were made to identify relevant English and non-English language articles. A standardized form was used to extract relevant information from studies and a narrative synthesis was developed.
In addition, systematic reviews of qualitative studies were used to provide information on values and preferences of the population of interest.
EVIDENCE TO RECOMMENDATIONS
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) system was applied by the GDG for assessing quality of evidence and using evidence to inform the recommendations.3 For each question, an evidence profile was provided summarizing the evidence retrieved, including evidence on values, preferences, benefits, harms and feasibility.
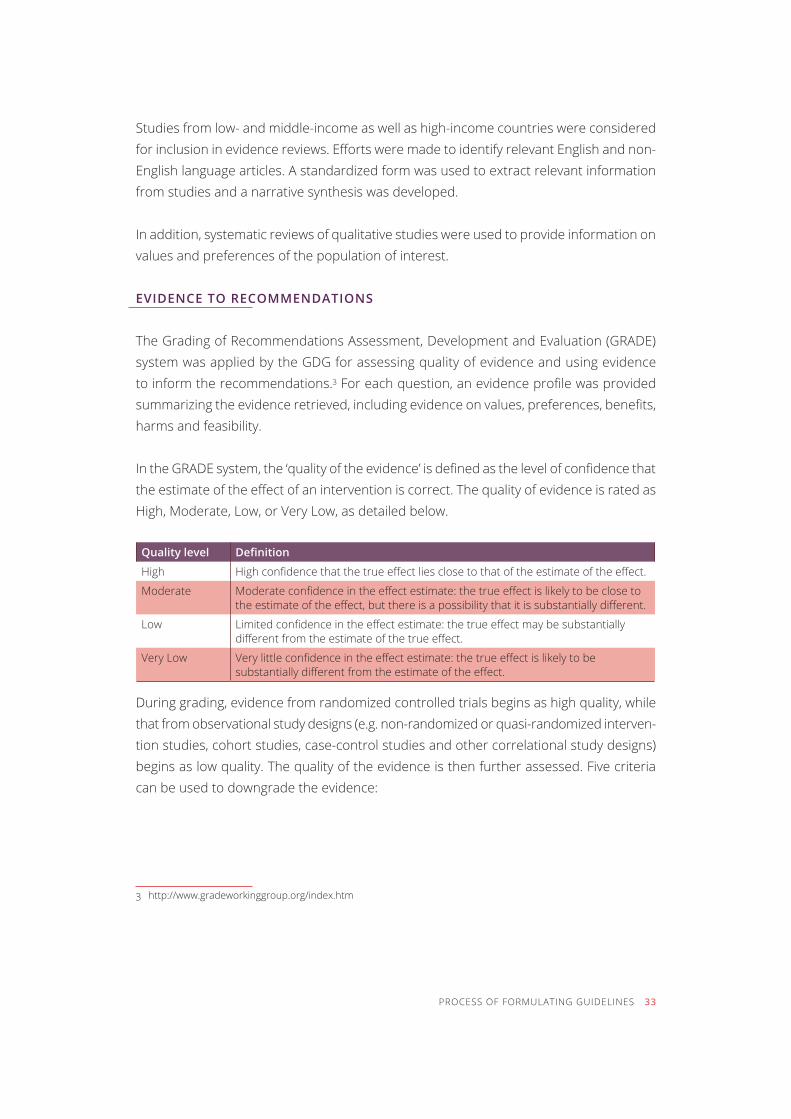
In the GRADE system, the ‘quality of the evidence’ is defined as the level of confidence that the estimate of the effect of an intervention is correct. The quality of evidence is rated as High, Moderate, Low, or Very Low, as detailed below.
Quality level Definition
high High confidence that the true effect lies close to that of the estimate of the effect.
moderate Moderate confidence in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.
Low Limited confidence in the effect estimate: the true effect may be substantially different from the estimate of the true effect.
Very Low Very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of the effect.
During grading, evidence from randomized controlled trials begins as high quality, while that from observational study designs (e.g. non-randomized or quasi-randomized interven-tion studies, cohort studies, case-control studies and other correlational study designs) begins as low quality. The quality of the evidence is then further assessed. Five criteria can be used to downgrade the evidence:
3 http://www.gradeworkinggroup.org/index.htm
PROCESS OF FORMULATING GUIDELINES 33
1. Risk of bias: Limitations in the study design that may bias the overall estimates of the
treatment effect.
2. Inconsistency: Unexplained differing estimates of the treatment effect (i.e. heterogeneity
or variability in results) across studies.
3. Indirectness: The question being addressed by the guidelines panel is different from the
available evidence regarding the population, intervention, comparator, or outcome.
4. Imprecision: Results are imprecise when studies include relatively few patients and few
events and thus have wide confidence intervals around the estimate of the effect.
5. Publication bias: Systematic underestimation or overestimation of the underlying ben-
eficial or harmful effect due to the selective publication (or reporting) of studies.
Three further criteria may be used to upgrade the quality of evidence rating: i) a strong association; ii) a dose-response gradient; and iii) lack of plausible confounding.
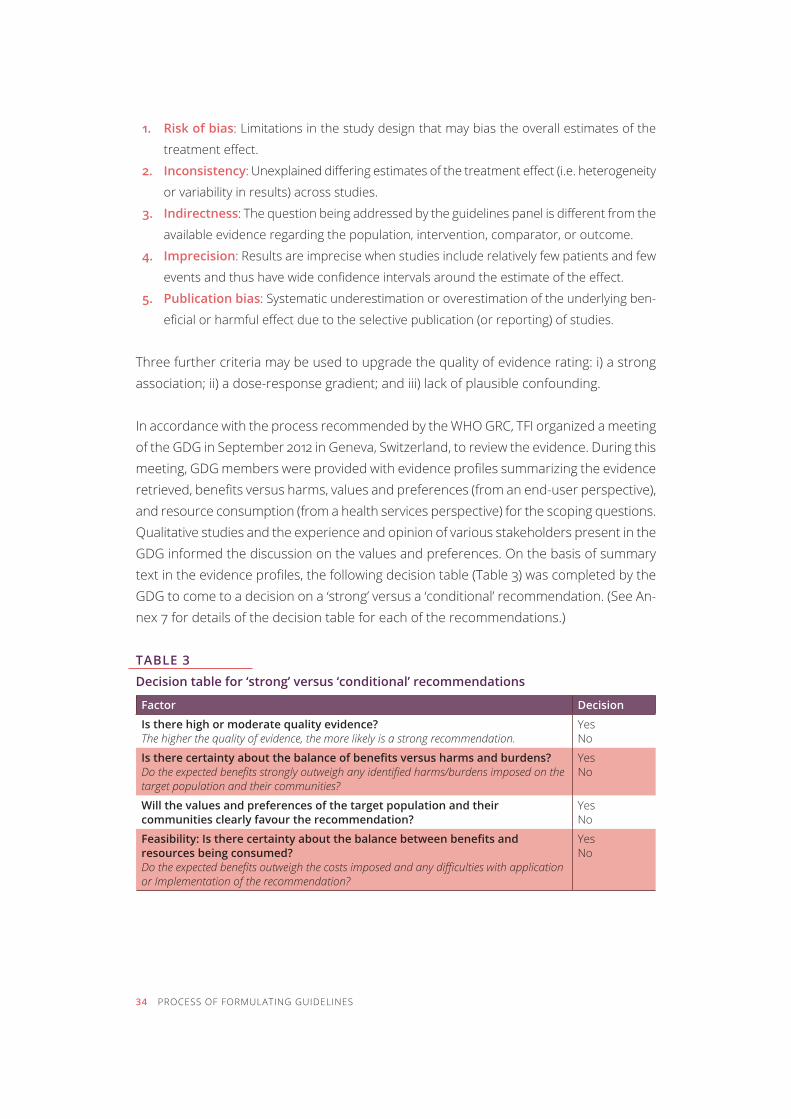
In accordance with the process recommended by the WHO GRC, TFI organized a meeting of the GDG in September 2012 in Geneva, Switzerland, to review the evidence. During this meeting, GDG members were provided with evidence profiles summarizing the evidence retrieved, benefits versus harms, values and preferences (from an end-user perspective), and resource consumption (from a health services perspective) for the scoping questions. Qualitative studies and the experience and opinion of various stakeholders present in the GDG informed the discussion on the values and preferences. On the basis of summary text in the evidence profiles, the following decision table (Table 3) was completed by the GDG to come to a decision on a ‘strong’ versus a ‘conditional’ recommendation. (See An-nex 7 for details of the decision table for each of the recommendations.)
TABLE 3
Decision table for ‘strong’ versus ‘conditional’ recommendations
Factor Decision
Is there high or moderate quality evidence? The higher the quality of evidence, the more likely is a strong recommendation.
Yes no
Is there certainty about the balance of benefits versus harms and burdens? Do the expected benefits strongly outweigh any identified harms/burdens imposed on the target population and their communities?
Yes no
Will the values and preferences of the target population and their communities clearly favour the recommendation?
Yes no
Feasibility: Is there certainty about the balance between benefits and resources being consumed? Do the expected benefits outweigh the costs imposed and any difficulties with application or Implementation of the recommendation?
Yes no
34 PROCESS OF FORMULATING GUIDELINES
The strength of the recommendation was assessed as being either:
‘strong’: indicating that the GDG agrees that the quality of the evidence combined with
certainty about the values, preferences, benefits and feasibility of this recommendation
means that it should be done in most circumstances;
or ‘conditional’: indicating that there was less certainty about the combined quality of evidence
and its values, preferences, benefits and feasibility of this recommendation meaning that
there may be circumstances in which it will not apply.
On a number of occasions, the GDG decided to give a strong recommendation despite very low quality evidence. This occurred when the following conditions applied:
(a) when there was agreement that expected benefits outweighed harms and burdens for
critical outcomes;
(b) when the expected values and preferences of the target population and their community
were clearly in favour of the recommendation; and
(c) when there was agreement that the expected benefits would not consume disproportion
ate resources.
GROUP PROCESS AND DECISION-MAKING
Decisions were made by consensus. At the beginning of the guidelines development meet-ing, it was agreed by the GDG that should there be disagreement on a decision, a vote would be taken and a two-thirds majority would be required for a decision to be carried. In the event, however, there was consensus on all recommendations.
PROCESS OF FORMULATING GUIDELINES 35

36
RECOMMENDATIONS 37
recommendations
To assist in the formulation of the recommendations, the GDG outlined a number of overarching principles that it agreed should underpin all recommendations for optimal identification and management of tobacco use by and SHS exposure in pregnant women. These principles are based on the human rights and ethics values, outlined in the WHO fctc (24), Convention on the Elimination of All Forms of Discrimination against Women (CEDAW) (34), and the Programme of Action of the International Conference on Popula-tion and Development (ICPD) (35). These principles, together with the implementation strategies and indicators for monitoring and evaluation presented later in the document, should guide stakeholders and policy-makers in the process of planning, implementing and evaluating the most suitable and relevant recommendation for their own circumstances.
It is necessary to note that all population-level policies and interventions for comprehensive tobacco control that are proven to be effective for the general population, would also help protect the health of pregnant women as well. These policies create an enabling environ-ment which is promotive of non-use of tobacco, and enable and empower women to be able to implement their own choices.
38 RECOMMENDATIONS
OVERARCHING PRINCIPLES
It is a basic right of every pregnant woman to be informed about the harms of tobacco use in any form, as well as the harms of SHS exposure.
Every pregnant woman has the right to a smoke-free environment at the home, and at work and in public places.
All interventions addressing the prevention of tobacco use and SHS exposure in pregnancy should be:
• woman-centred and gender-sensitive; • culturally appropriate and socially acceptable; and • delivered in a non-judgemental and non-stigmatizing manner.
Health centres, hospitals and clinics need to ‘practice what their providers preach’ by providing tobacco-free health-care facilities, and having the health-care pro-viders as ‘tobacco-free role models’.
The presented recommendations are consistent with the guiding principles set out in the Who fctc (24).
RECOMMENDATIONS
This section includes nine recommendations for the prevention and management of to-bacco use and SHS exposure in pregnancy. Each recommendation is followed by specific remarks related to that recommendation, which are intended to explain the context in which these recommendations were made. Narrative summaries of evidence support-ing the recommendations are also included below each recommendation. (The decision tables summarizing the values, preferences and judgements made about the strength of the recommendations are available in Annex 7.)
RECOMMENDATIONS 39
IDENTIFICATION OF TOBACCO USE AND SECOND-HAND SMOKE EXPOSURE
RECOMMENDATION 1
Assessment of tobacco use and second-hand smoke exposure in pregnancy Health-care providers should ask all pregnant women about their tobacco use (past and present) and exposure to SHS as early as possible in the pregnancy and at every antenatal care visit.
Strength of recommendation: Strong. Quality of evidence: Low
REMARKS
Tobacco use includes all forms of smoking and use of smokeless tobacco.
Second-hand smoke exposure includes exposure to smoke from combustible tobacco products at home, work and in public places.
Tobacco use (smoking and smokeless) status of husbands/partners and other household members should also be assessed.
At the first prenatal visit, health-care providers should ask all pregnant women about their tobacco use (past and present). Pregnant women with prior history of tobacco use should be asked about their present tobacco use at every ante-natal care visit. Providers should ask women about their SHS exposure at the first prenatal visit, and whenever there is a change in living or work status and when SHS intervention has been initiated.
Before assessment is initiated in a clinic setting:
• training and resource materials should be provided to clinicians and other health-care workers to enable effective and non-judgemental assessment of tobacco use; and
• clinicians and other health-care workers should be trained to refer or inter-vene with all pregnant women who are identified as tobacco users (past and present) or exposed to SHS.
eVIDeNCe FOR ReCOMMeNDaTION 1
Overall question: What are the necessary elements for effective screening of pregnant women for smoking and smokeless tobacco use?
The first step in treating tobacco use and dependence is to identify tobacco users. Iden-tification of smokers increases rates of clinician intervention. Effective identification of tobacco-use status not only opens the door for successful interventions (e.g. clinician advice and treatment), but also guides clinicians to identify appropriate interventions based on the tobacco-use status of patients and their willingness to quit.
pico (Population, Intervention, Comparison, and Outcome) question used to examine evidence
population Pregnant women (all trimesters and postpartum)Intervention Active screening for current and past tobacco use (frequency of use of
smoked and smokeless tobacco; quantities of smoked and smokeless tobacco consumed), assessment of tobacco dependence, screening for SHS exposure
comparison treatment as usualoutcomes • Identification of current tobacco-use status
• Identification of recent or past tobacco-use status • Identification of nicotine dependence• Identification of exposure to SHS
SYSTEMATIC REVIEWS AND OTHER SOURCES (E.G. QUALITATIVE STUDIES, COST-EFFECTIVENESS ANALYSES) IDENTIFIED BY THE SEARCH PROCESS
Although the search for evidence did not identify any relevant recent systematic reviews on screening pregnant women for tobacco use or SHS exposure, previous research has indicated efficacy of screening in a general health-care setting on successful cessation ef-forts (or intent) (36). WHO has developed the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST), an instrument to detect and manage substance use and related problems in primary and general medical care settings. This instrument provides some in-formation on how to assess tobacco use and provide brief intervention, but does not include any recommended action for the management of smokeless tobacco use or SHS exposure (37). The current recommendations have used guidance from various national guidelines as well as resource documents from international agencies to develop the narrative synthesis.
40 RECOMMENDATIONS
Methods for evaluating tobacco control policies. IARC Handbook of Cancer Prevention (Volume
12), 2008 (38).
Treating tobacco use and dependence: 2008 update. US Department of Health and Human
Services, 2008 (36).
How to stop smoking in pregnancy and following childbirth. National Institute for Health and
Clinical Excellence (NICE), the United kingdom, 2010 (39).
Flemming H et al. (2012) Using qualitative research to inform interventions to reduce smoking
in pregnancy in England: a systematic review of qualitative studies. The Journal of Advanced
Nursing, 2010 (40).
The WHO ASSIST package: Manuals for the Alcohol, Smoking and Substance Involvement
Screening Test (ASSIST) and the ASSIST-linked brief interventions, 2010 (37).
Gender, women, and the tobacco epidemic. WHO monograph, 2010 (41).
WHO guidelines for control and monitoring the tobacco epidemic. World Health Organization,
1998 (42).
NARRATIVE SYNTHESIS OF KEY FINDINGS
tobacco use:
The first step in effective intervention for tobacco cessation is assessment of tobacco-use status. The 2008 USA guidelines on ‘Treating tobacco use and dependence’, recommend that clinicians and health-care systems should use health-care visits for universal assess-ment and intervention for tobacco use (36). Specifically, it is recommended that every patient who presents to a health-care facility be asked if she/he uses tobacco. All patients should have their tobacco-use status documented on a regular basis. Evidence has shown that clinic screening systems, such as expanding the vital signs to include tobacco-use status or the use of other reminder systems such as chart stickers or computer prompts, significantly increase rates of intervention by health-care providers (36).
Studies have shown that not all health-care staff ask all pregnant women about their smoking status during consultations (39). There is evidence that health-care staff may not ask about smoking status fearing that doing so will negatively impact the relationship between themselves and their pregnant patients.
When asking about tobacco use, health-care staff should screen for current use as well as for past tobacco use, in order to identify pregnant women who may have quit recently (in the pre-conception period or early in the pregnancy) and are therefore vulnerable to relapse (36).
RECOMMENDATIONS 41
Research has shown that the use of multiple choice questions, as opposed to a simple yes/no question, can increase disclosure of tobacco use among pregnant women by as much as 40%. For example, giving women the opportunity to answer, ‘I am still smoking but I have cut down on my use’ or a similar response when asked about their tobacco-use status provides women with an opportunity to disclose that they are smoking while also showing they have taken steps to reduce exposure (36). it is important to communicate with the pregnant women in a sensitive, client-centred manner, particularly as some pregnant women find it difficult to say that they smoke. Such an approach is important in reducing the likelihood that pregnant women will conceal their tobacco use and thus miss out on the opportunity to get help (39).
nicotine dependence:
Nicotine dependence is a chronic disease that often requires repeated intervention and multiple attempts to quit (36). nicotine is the drug in tobacco products that causes de-pendence. Nicotine dependence among adult smokers is characterized by the emergence of withdrawal symptoms in response to abstinence and by unsuccessful attempts to re-duce the use of tobacco or to quit altogether. This dependence is not limited to smoked tobacco products: use of smokeless tobacco also results in nicotine dependence. The IARC handbook of cancer prevention on ‘Methods for Evaluating Tobacco Control Policies’ provides a list of instruments which could be used in different settings to assess tobacco dependence for various tobacco products (38).
second-hand smoke exposure:
The United kingdom’s guidance on ‘Quitting smoking in pregnancy and following childbirth’ recommends that during the first face-to-face antenatal care visit, health-care staff enquire if anyone else in the household smokes. This includes the woman’s husband or partner if applicable (39). This is intended to determine both support for cessation, as well as an assessment of SHS exposure from other family members.
Frequency of assessment for tobacco use and SHS exposure:
Although quitting early in pregnancy and remaining abstinent through the pregnancy will produce the greatest benefits to the fetus and expectant mother, even quitting at a late stage during pregnancy can yield benefits (36). Hence, the tobacco control programmes should strive to reach pregnant smokers as early as possible in the pregnancy and follow
42 RECOMMENDATIONS
them throughout the pregnancy, and early postpartum to promote and support sustained smoking cessation (41). There is evidence that many women under-report smoking in preg-nancy due to a strong stigma against smoking (36, 39, 43). during the multiple interactions with the health-care providers, women may become sufficiently comfortable to disclose their tobacco-use status. Therefore, it is important that clinicians assess tobacco-use status of pregnant women not only at the first prenatal visit, but also throughout the course of pregnancy as indicated.
Health-care workers should assess SHS exposure at the first prenatal visit as well as throughout the course of pregnancy, as circumstances may change at home or in the workplace (e.g. the arrival of a relative who smokes indoors, career moves, etc.).
The USA guidelines also advise that once a tobacco user is identified, the clinician should assess the patient’s willingness to quit at this time (36). The patient should be asked, ‘Are you willing to make a quit attempt at this time?’ Such an assessment (willing or unwilling) is a necessary first step in treatment. In addition, every patient should be assessed for social, physical or existing medical conditions that may affect the use of planned cessa-tion treatments (36).
Grading of evidence: Evidence was graded as low due to indirectness.
STRENGTH OF THE RECOMMENDATION
The GDG reviewed the above evidence and considered the harms, benefits, values, prefer-ences, feasibility and cost-effectiveness of the proposed recommendation when drafting the recommendation. It was decided that the potential benefits strongly outweighed any harms, values were in support, and that it was cost effective and feasible in the antenatal care settings, and therefore should be classified as a strong recommendation. (See An-nex 7 for detailed description of all issues considered in these domains.)
RECOMMENDATIONS 43
INTERVENTIONS FOR TOBACCO-USE CESSATION
RECOMMENDATION 2
Psychosocial interventions for tobacco-use cessation in pregnancy Health-care providers should routinely offer advice and psychosocial interventions for tobacco cessation to all pregnant women, who are either current tobacco users or recent tobacco quitters.
Strength of recommendation: Strong. Quality of evidence: Moderate
REMARKS
Psychosocial interventions involve behavioural support that may include one or more of the following: counselling, health education, incentives and peer or social support.
Psychosocial interventions should be offered to pregnant women who are cur-rent or former tobacco users as early in pregnancy as possible.
The recommendation for recent tobacco quitters is based on population-based studies in non-pregnant populations. Recent tobacco quitters may include wom-en who used tobacco before the pregnancy, and who have either spontaneously quit or stopped tobacco use in the pre-conception period or in early pregnancy, before their first antenatal visit.
There is emerging evidence from some countries that the use of financial incen-tives may be more effective than other interventions. However, it is difficult to generalize the reported effectiveness to the global population as the evidence is limited and is derived from select small populations.
The Stages of Change approach is not effective in pregnancy. The Stages of Change approach to tobacco cessation suggests that health behaviour change involves progress through six stages of change: pre-contemplation, contempla-tion, preparation, action, maintenance, and termination (44). as this approach is not effective, all women should be offered support irrespective of their inten-tion to quit.
44 RECOMMENDATIONS
More heavily dependent tobacco users may require high intensity interventions.
Interventions should address concerns of the pregnant smokers about gaining weight as a result of tobacco cessation.
Interventions should recognize and address the impact of partner’s smoking status and their attitudes towards tobacco use or cessation.
Recognizing that there is no safe level of tobacco use, there is evidence of some benefit from reduction in smoking if quitting is not achieved.
Almost all existing evidence for interventions is for smokers of manufactured cigarettes, but emerging evidence suggests that similar psychosocial strategies could be applied to users of other forms of tobacco (smokeless tobacco, water-pipes, etc.). There is limited evidence that stopping use of smokeless and other forms of tobacco may improve some birth outcomes.
Given the cost-effectiveness of these interventions, and long-term cost recovery to the health system through tobacco-related disease burden being averted, programme cost should not be a deterrent to immediate implementation.
EVIDENCE FOR RECOMMENDATION 2
Overall question: Is use of psychosocial interventions for tobacco dependence effective in pregnancy?
The complexity of smoking in pregnancy has generated many perspectives about the most appropriate approaches and strategies to support cessation.
PICO (Population, Intervention, Comparison, and Outcome) question used to examine evidence
population Pregnant women (all trimesters and postpartum) who use tobaccoIntervention Psychosocial interventions including counselling, health education, incen-
tives, and peer or social support comparison treatment as usual
RECOMMENDATIONS 45
outcomes • tobacco cessation in pregnancy• tobacco abstinence postpartum• smoking reduction from first antenatal visit to late pregnancy• maternal outcomes (mode of birth e.g. caesarean section rate) • fetal outcomes: – birth weight – mean birth weight, low birth weight (proportion less than 2500 g), very low birth weight (proportion less than 1500 g) – perinatal mortality (stillbirth, neonatal deaths, all perinatal deaths)
SYSTEMATIC REVIEWS AND OTHER SOURCES (E.G. QUALITATIVE STUDIES, COST-EFFECTIVENESS ANALYSES) IDENTIFIED BY THE SEARCH PROCESS
Cochrane systematic reviews of the range of interventions to support smoking cessation have been performed since 1995. The most recently published Cochrane review on this topic was carried out in 2009 (45). The 2009 review was then updated in 2012. The 2012 update was split into two separate reviews. Coleman et al. in 2012 evaluated pharma-cotherapy to support smoking cessation (presented in a separate evidence profile on pharmacotherapy) (46), while Chamberlain et al. in 2012 evaluated the effectiveness of individual psychosocial interventions for supporting women to stop smoking in pregnancy and interventions to prevent smoking relapse among women who have spontaneously quit (47).
In addition to the Cochrane reviews, the following reviews were also used for the evidence retrieval and to inform the discussion on the values and preferences.
Baxter et al. Systematic review of how to stop smoking in pregnancy and following childbirth:
review 2: factors aiding delivery of effective interventions (review prepared for NICE Public
Health guidance 26), 2008 (48).
Taylor M. Economic analysis of interventions for smoking cessation aimed at pregnant women
(paper prepared for NICE, the United kingdom guidelines), 2009 (49).
Ebbert et al. Cochrane systematic review on interventions for smokeless tobacco-use ces-
sation, 2011 (50).
Flemming H et al. Using qualitative research to inform interventions to reduce smoking in
pregnancy in England: a systematic review of qualitative studies, 2012 (40).
Treating tobacco use and dependence: 2008 update. US Department of Health and Human
Services, 2008 (36).
46 RECOMMENDATIONS
NARRATIVE SYNTHESIS OF KEY FINDINGS
A major limitation was the lack of studies conducted in low- to middle-income countries. Only 2 of 65 studies on psychosocial interventions during pregnancy were from low- or middle-income countries (Poland and four countries in South America). The criteria for ‘smoker’ varied, and only one study included women using smokeless tobacco products.
Many of the trials had multimodal interventions, but the main intervention strategies involved counselling (39 trials), health education (7 trials), feedback (7 trials), incentives (3 trials), and peer or social support (11 trials). Three trials offered optional nicotine replace-ment therapy as part of a multimodal intervention. Women in the control groups in 38 of the 67 trials received information about the risks of smoking in pregnancy and were advised to quit as part of ‘usual care’. The most frequent comparison was ‘usual care’ from a woman’s antenatal care provider (30 trials).
Pooled data from 63 trials revealed that women receiving psychosocial interventions (counselling, health education, feedback, incentives, or peer or social support) were ap-proximately 30% more likely to not smoke (i.e. be abstinent) late in pregnancy (RR=1.36, 95% confidence interval [CI] 1.22–1.52), compared to women in the comparison group (Number Needed to Benefit [NNTB]=25, 95% CI 17–40). This included both self-reported and bio-chemically validated smoking cessation. However, the heterogeneity was high (I2=58%).
The effect of the intervention on smoking in late pregnancy was still statistically significant among a subgroup of 17 trials with biochemically validated smoking cessation, assessed as ‘low risk of bias’ in this review (RR=1.43, 95% CI 1.13–1.80). It is unclear whether interven-tions to support women who spontaneously quit in early pregnancy reduce the rate of relapse in late pregnancy (RR=0.89, 95% CI 0.74–1.08). Although the effect on smoking in late pregnancy was still statistically significant among a subgroup of trials with ‘low risk of bias’, caution is urged in interpreting other results as potential sources of bias were identified and there is high heterogeneity. There was some weak evidence that women in intervention groups reduced smoking in late pregnancy, but the evidence was not consistent.
Among a subset of studies that examined cessation in the postpartum period, women receiving the psychosocial interventions were significantly more likely to remain abstinent in the early postpartum period (1–5 months) (RR=1.33, 95% CI 1.07–1.66), but this was not sustained in the longer term (6–12 months) (RR=1.10, 95% CI 0.83–1.44).
RECOMMENDATIONS 47
Interventions were grouped into five main intervention strategies: (i) counselling (n=38), (ii) health education (n=6), (iii) feedback (n=5), (iv) incentives (n=3), and (v) peer or social support (n=11). Interventions with incentives were the most effective (RR=2.86, 95% CI 2.25–3.46; n=3). This was followed by feedback (RR=2.26, 95% CI 1.77–2.75; n=5) and then counselling (RR=1.34, 05% CI 1.19–1.48; n=38). The pooled effect size estimates for social/peer support (RR=1.20, 95% CI 0.98–1.42; n=11) and health education (RR=1.14, 95% CI 0.69–1.59; n=6) were not statistically different.
Pooled data from 14 trials demonstrated that psychosocial interventions to support women to stop smoking in pregnancy reduce the rate of infants born low birth weight (<2500 g) (RR=0.83, 95% CI 0.71–0.97; NNTB=61, 95% CI 37–292) and preterm birth (<37 weeks) (RR=0.85, 95% CI 0.72–0.99; NNTB=97, 95% CI 53–1554). It is unclear whether interven-tions to stop smoking reduce: the rate of infants born very low birth weight (<1500 g); neonatal deaths; neonatal intensive care admissions or total perinatal mortality, as the outcome numbers were small. There were no differences reported in rates of caesarean section (two trials). One study examined maternal weight gain as an outcome, and found a mean excess weight of 2.8 kg among women who had stopped smoking compared to the women who did not quit.
The review defined intensity rating of interventions and controls as follows:
Low intensity Provision of leaflet, posters or self-help materials available AND advice to quit and written or verbal information on risks.
medium intensity Provision of low intensity intervention AND self-help materials on strategies for quitting.
high intensity Provision of medium intensity intervention AND other forms of support, such as personal contacts, reminders, incentives, phar-macological agents.
Interventions categorized as ‘high intensity’, such as counselling (Pooled RR=1.36, 95% CI 1.20–1.54) are slightly more effective than those categorized as ‘low intensity’, such as pro-vision of advice and self-help materials (Pooled RR=1.30, 95% CI 1.00–1.70), in supporting women to stop smoking. There was strong significant correlation between the intensity of both the intervention and control arms (i.e. higher intensity interventions were compared with higher intensity control conditions, and trials with lower intensity interventions were compared with lower intensity controls).
48 RECOMMENDATIONS
Newly included studies in this update of the review demonstrated a borderline effect of smoking cessation interventions in supporting pregnant women to stop smoking (RR=1.28, 95% CI 1.00–1.60), when compared to studies in the previous version of this review (RR=1.40, 95% CI 1.23–1.60) (45). The median intensity of ‘standard care’ provided in antenatal care in the comparison group has also increased over time, perhaps explaining attenuation of the association between the intervention and cessation.
There does not appear to be psychological harm caused by psychosocial interventions and two studies suggest some interventions may improve psychological well-being for women. Studies reporting women’s views regarding the interventions (n=13) suggest personal con-tact may be important, though trials of emerging technologies, such as computer-based interventions and telephone support, have received positive feedback from women. In six studies looking at peer and partner support for smoking cessation, women reported mixed (both positive and negative) support experiences.
Studies reporting provider’s views of the interventions suggest challenges to implementa-tion in clinical settings, including competing demands on time and uncertainty over the effectiveness of interventions. These barriers may be overcome by including educational interventions directed at providers, use of referral services and technological aids.
Although psychosocial interventions administered in randomized controlled trials (RCTs) were effective (RR=1.37, 95% CI 1.22–1.54), the effect of interventions provided in cluster-randomized trials was smaller and not statistically significant (RR=1.23, 95% CI 0.84–1.78), suggesting challenges implementing research evidence into more general settings. How-ever, the group noted that there were few cluster RCTs in general for smoking cessation in pregnancy and the data could be more robust if evidence from more RCTs was available.
Four studies conducted in high-income countries reported that the interventions were highly cost effective using a variety of measures. Pregnancy-specific self-help materi-als were more cost effective than standard smoking cessation information or self-help materials.
Tobacco control programme interventions should reach a pregnant smoker as early as possible in the pregnancy and follow her throughout the pregnancy and early postpartum to promote and support sustained smoking cessation (41).
RECOMMENDATIONS 49
Use of psychosocial interventions to support smokeless tobacco cessation in pregnant women
There have been no trials to study effect of psychosocial intervention in pregnant women using smokeless tobacco (ST). A 2011 Cochrane review of interventions for smokeless to-bacco cessation identified 12 trials involving behavioural interventions in the adults, but these trials did not involve pregnant women (50). The results are as follows:
Behavioural interventions appear to be effective for increasing tobacco abstinence rates among smokeless tobacco users.
Behavioural interventions which include telephone support or an oral examination with feedback may be effective for increasing tobacco abstinence rates among smokeless tobacco users. These estimates combine both population-based interventions and indi-viduals self-selecting for treatment.
The 2008 USA guidelines on ‘Treating tobacco use and dependence’ also recommend that smokeless tobacco users should be identified, strongly urged to quit, and provided counselling cessation interventions.
Grading of evidence: The quality of the evidence in Chamberlain et al. was graded as moderate quality for all outcomes. (See Annex 6 for GRADE tables.)
STRENGTH OF THE RECOMMENDATION
The GDG reviewed the above evidence and considered the harms, benefits, values, prefer-ences, feasibility and cost-effectiveness of the proposed recommendation when drafting the recommendation. It was decided that the benefits strongly outweighed any harms, values were in support, and that it was cost-effective and feasible, and therefore should be classified as a strong recommendation. (See Annex 7 for detailed description of all issues considered in these domains)
50 RECOMMENDATIONS
RECOMMENDATIONS 3–5
Use of pharmacotherapy for tobacco-use cessation in pregnancy The panel cannot make a recommendation on use or non-use of nicotine replacement therapy (NRT) to support cessation of tobacco use in pregnancy.
Strength of recommendation: Not applicable. Quality of evidence: Moderate The panel does not recommend use of bupropion or varenicline to support cessation of tobacco use in pregnancy.
Strength of recommendation: Strong. Quality of evidence: No evidence available The panel recommends that further research be carried out in pregnant women on safety, efficacy and factors affecting adherence to pharmacotherapeutic agents for tobacco-use cessation.
Strength of recommendation: Strong. Quality of evidence: Not applicable
REMARKS
The evidence search found no quality evidence on the use of pharmacotherapy with bupropion or varenicline for tobacco-use cessation in pregnancy.
There is currently insufficient evidence to determine whether or not pharma-cotherapy (NRT, bupropion, varenicline) is effective when used in pregnancy for tobacco-use cessation.
There is currently insufficient evidence to determine whether or not pharmaco-therapy (NRT, bupropion, varenicline) is safe when used in pregnancy for tobacco-use cessation.
Given the known considerable harms caused by tobacco smoking in pregnancy and the known benefits of using NRT from studies in the general population, it is acknowledged that various national guidelines have recommended use of NRT in pregnancy under medical supervision.
RECOMMENDATIONS 51
Urgently needed research includes: studies of factors improving or impeding adherence to pharmacotherapeutic agents; a review of the effects (safety profiles, effectiveness) of use of NRT in pregnant women, particularly in the United king-dom where a historical cohort exists for use of NRT in pregnancy; use of client preference trials (client’s preference of pharmacotherapy treatment versus no treatment); and surveillance of current use of pharmacotherapy in pregnancy (focused on determining whether women use pharmacotherapy when recom-mended or prescribed by health-care providers).
EVIDENCE FOR RECOMMENDATIONS 3–5
Overall question: Is use of pharmacological treatment for tobacco dependence safe and effective in pregnancy?
Three first-line pharmacological agents were approved by the United States Food and Drug Administration (FDA) to treat tobacco-use dependence (36). The following agents have been found to be safe and effective in assisting with tobacco cessation (smoking and smokeless tobacco) in the general population: 1. Nicotine replacement therapy (NRT) in several forms (patches, gum, nasal sprays, oral
sprays, inhalers, microtabs and lozenges)
2. Bupropion
3. varenicline
PICO (Population, Intervention, Comparison, and Outcome) question used to examine evidence
population Pregnant women (all trimesters and postpartum who are dependent on tobacco)
Intervention Nicotine replacement therapy, bupropion, varenicline comparison treatment as usual outcomes • Adherence to or compliance with treatment
• Efficacy: tobacco-use cessation• Safety: maternal outcomes (e.g. preterm birth, caesarean section rate
and fetal outcomes (e.g. miscarriage/spontaneous abortion, stillbirth, congenital abnormalities, any effects of fetal growth, neonatal intensive care admissions.)
52 RECOMMENDATIONS
SYSTEMATIC REVIEWS AND OTHER SOURCES (E.G. QUALITATIVE STUDIES, COST-EFFECTIVENESS ANALYSES) IDENTIFIED BY THE SEARCH PROCESS
The evidence search found randomized controlled trials and observational studies on the use of NRT in pregnancy, one observational study on use of bupropion in pregnancy and none for varenicline. The latter two medications are not recommended for use in pregnancy in most countries (36, 39).
Nicotine replacement therapy is available as patches, gum, nasal sprays, inhalers, and lozenges; all have been used to treat tobacco dependence in pregnancy. Concerns about fetal safety and possible adverse maternal outcomes have led to limitations on its use in pregnancy in many countries. National and professional guidelines from Canada and the United kingdom recommend use of NRT in pregnancy only when psychosocial interven-tions fail (39, 51). Randomized controlled trials of NRT have been performed, all of them in high-income countries, measuring continuous smoking abstinence or point prevalence of smoking abstinence and comparing adverse effects – maternal and fetal – between the intervention and control groups.
The following Cochrane and other systematic reviews were used for evidence retrieval.
Coleman et al. Pharmacological interventions for promoting smoking cessation in pregnancy,
2012 (46).
Myung et al. Efficacy and safety of pharmacotherapy for smoking cessation among pregnant
smokers: a meta-analysis, 2010 (52).
Taylor M. Economic analysis of interventions for smoking cessation aimed at pregnant women
(paper prepared for NICE Public Health guidance 26), 2009 (49).
Baxter et al. Systematic review of how to stop smoking in pregnancy and following childbirth:
review 2: factors aiding delivery of effective interventions (review prepared for NICE Public
Health guidance 26), 2008 (48).
Ebbert et al. Cochrane systematic review on interventions for smokeless tobacco-use cessa-
tion in general population, 2011 (50).
Inclusions: systematic reviews performed within the past two years.
Exclusions: Myung et al., 2012, was not used for grading of evidence on NRT because it gave a
pooled effect using combined studies on NRT and one using bupropion. However, informa-
tion on side effects and attitudes in this review was used to inform values and preferences
domains for this recommendation.
RECOMMENDATIONS 53
NARRATIVE SYNTHESIS OF KEY FINDINGS
Use of NRT to support smoking cessation in pregnant women
Coleman et al. found that NRT had a small (RR=1.3, 95% CI 0.93–1.91) but non-significant effect on smoking cessation (46). There were non-significant increases in rates of stillbirth, miscarriage and birth by caesarean section, and non-significant reductions in preterm births, neonatal intensive care admissions and neonatal deaths. Adherence to recom-mended treatment was generally low in the included studies. Nicotine is metabolized faster in pregnant women than in non-pregnant women. This means that pregnant women are likely to need higher doses of NRT as compared to non-pregnant women to substitute for nicotine received from tobacco. Subsequently a higher dose of NRT may be needed for cessation. Many of the studies in the Coleman review used the standard NRT dose (prin-cipally 15 mg, delivered via a 16-hour patch). This, together with low adherence would lead to very low exposure to the intervention, which may explain the lack of observed effect.
Use of pharmacotherapy to support smokeless tobacco cessation in pregnant women
There have been no trials comparing pharmacotherapy to placebo in pregnant women using smokeless tobacco. A 2011 Cochrane review of interventions for smokeless tobacco cessation identified 11 trials comparing pharmacotherapy to a placebo in the adults but these trials did not involve pregnant women (50). The results are as follows:
Two small trials of bupropion did not detect an effect on smokeless tobacco abstinence, although the wide confidence intervals (OR=0.86, 95% CI 0.47–1.57) do not rule out a small benefit.
Four trials of nicotine patch did not detect a benefit (OR=1.16, 95% CI 0.88–1.54), nor did two trials of nicotine gum (OR=0.98, 95% CI 0.59–1.63).
Data from one study among Swedish snus users suggests that varenicline can increase tobacco abstinence rates at six months (OR=1.6, 95% CI 1.08–2.36).
Grading of evidence: The quality of the evidence in Coleman et al. was graded as moderate. (See Annex 6 for GRADE tables.)
54 RECOMMENDATIONS

STRENGTH OF THE RECOMMENDATION
The GDG reviewed the above evidence and considered the harms, benefits, values, pref-erences, feasibility and cost-effectiveness of the proposed recommendation during the recommendation drafting process. Given that there was good quality but inconclusive evidence on both the effectiveness and impact on fetal outcomes for NRT, and acknowl-edging that in some countries NRT is recommended for smoking cessation in pregnant women when behavioural therapy fails, the panel decided they could not make a specific recommendation on the use or non-use of NRT. The group also noted that this is an area of great public health importance where presently there are large gaps in research and evidence, and made a strong recommendation for further research to be carried out on safety, efficacy and factors affecting adherence to pharmacotherapeutic agents in pregnant women for tobacco-use cessation. (See Annex 7 for a detailed description of all issues considered in these domains.)
RECOMMENDATIONS 55
PROTECTION FROM SECOND-HAND SMOKE
RECOMMENDATIONS 6–7
Protection from second-hand smoke in pregnancy (smoke-free public places) All health-care facilities should be smoke-free to protect the health of all staff, patients and visitors including pregnant women.
Strength of recommendation: Strong. Quality of evidence: Low All work and public places should be smoke-free for the protection of everyone includ-ing pregnant women.
Strength of recommendation: Strong. Quality of evidence: Low
REMARKS
Health-facility staff who use tobacco should be offered cessation services.
EVIDENCE FOR RECOMMENDATIONS 6–7
Overall question: What are the effective interventions to prevent SHS exposure to pregnant women at health-care facilities, workplaces and other public places?
Article 8 of the WHO Framework Convention for Tobacco Control (WHO FCTC) on protec-tion from exposure to tobacco smoke obliges WHO Member States who have ratified the treaty (176 parties as of 23 August 2012) to protect all people from exposure to SHS in indoor workplaces, public transport and indoor public places. As a result, many countries around the world have banned smoking in public places (24). At its second session in July 2007, the Conference of the Parties (COP) adopted guidelines for implementation of Article 8 of the WHO FCTC on protection from exposure to SHS (53).
Many countries, regardless of their FCTC ratification status, are taking steps to protect their citizens from the harms of SHS in public places, through either planning the steps or
56 RECOMMENDATIONS
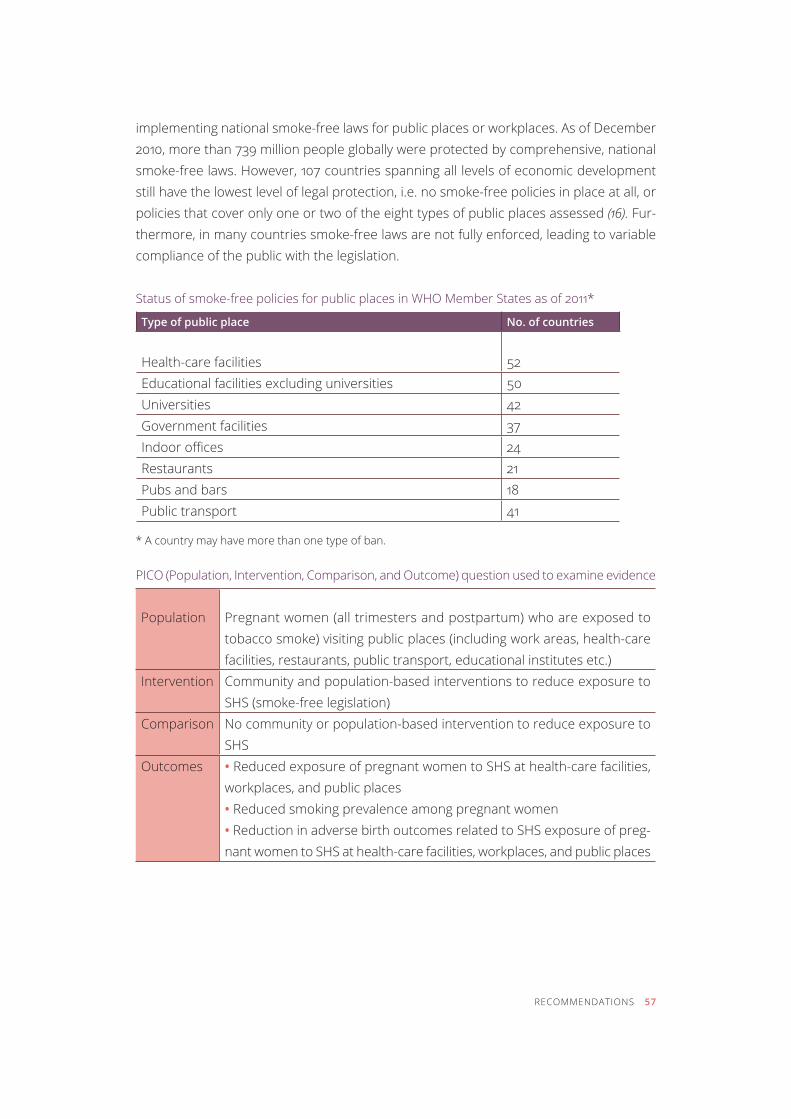
implementing national smoke-free laws for public places or workplaces. As of December 2010, more than 739 million people globally were protected by comprehensive, national smoke-free laws. However, 107 countries spanning all levels of economic development still have the lowest level of legal protection, i.e. no smoke-free policies in place at all, or policies that cover only one or two of the eight types of public places assessed (16). fur-thermore, in many countries smoke-free laws are not fully enforced, leading to variable compliance of the public with the legislation.
Status of smoke-free policies for public places in WHO Member States as of 2011*
Type of public place No. of countries
Health-care facilities 52Educational facilities excluding universities 50Universities 42Government facilities 37Indoor offices 24restaurants 21pubs and bars 18public transport 41
* A country may have more than one type of ban.
PICO (Population, Intervention, Comparison, and Outcome) question used to examine evidence
population Pregnant women (all trimesters and postpartum) who are exposed to tobacco smoke) visiting public places (including work areas, health-care facilities, restaurants, public transport, educational institutes etc.)
Intervention Community and population-based interventions to reduce exposure to SHS (smoke-free legislation)
comparison No community or population-based intervention to reduce exposure to shs
outcomes • Reduced exposure of pregnant women to SHS at health-care facilities, workplaces, and public places• Reduced smoking prevalence among pregnant women• Reduction in adverse birth outcomes related to SHS exposure of preg-nant women to SHS at health-care facilities, workplaces, and public places
RECOMMENDATIONS 57
SYSTEMATIC REVIEWS AND OTHER SOURCES (E.G. QUALITATIVE STUDIES, COST-EFFECTIVENESS ANALYSES) IDENTIFIED BY THE SEARCH PROCESS
No recent systematic reviews were identified that were specific to the impact of the smoke-free policies on SHS exposure in pregnant women. However, there is strong evidence to support smoke-free policies to protect the general population from SHS; in turn these policies will also benefit the subpopulation of pregnant women.
The following systematic reviews and peer-review publications were used to develop the narrative synthesis.
Callinan et al. Legislative smoking bans for reducing SHS exposure, smoking prevalence and
tobacco consumption. Cochrane Database of Systematic Reviews, 2010 (54).
Charrier et al. Smoking habits in Italian pregnant women: any changes after the ban? 2010 (55).
Puig et al. Assessment of prenatal exposure to tobacco smoke by cotinine in cord blood for
the evaluation of smoking control policies in Spain, 2012 (56).
Mackay et al. Impact of Scotland’s smoke-free legislation on pregnancy complications: retro-
spective cohort study, 2012 (57).
Adams et al. Reducing prenatal smoking: the role of state policies, 2012 (58).
NARRATIVE SYNTHESIS OF KEY FINDINGS
There has been an increase in the number of countries implementing national and sub-national policies which ban or restrict smoking in public places and workplaces. The main reason for these policies is to protect non-smokers from the harmful health effects of exposure to shs (54). Smoke-free environments also help smokers who want to quit, and bans on smoking in public places and workplaces may also encourage people to make their homes smoke-free to protect the non-smokers (59).
Impact of smoke-free policies on SHS exposure
General population: A 2010 Cochrane review looking at the impact of smoke-free policies on exposure to SHS in the general population found that smoking bans reduced exposure to SHS in workplaces, restaurants, pubs and in public places. Hospitality workers experi-enced a greater reduction in exposure to SHS after implementing the ban as compared to the general population. There was no change in exposure to SHS in private cars. In general, there was no change in the levels of SHS exposure at home after the implementa-tion of the smoking bans across all studies, though some studies reported reductions in
58 RECOMMENDATIONS
exposure to SHS at home after public smoking bans were implemented (54). Following the implementation of legislation in Scotland prohibiting smoking in all partially or completely enclosed public spaces in 2006, many studies have shown a reduction in smoking and in shs exposure in adults and children (57).
Pregnant women: Italy introduced smoke-free legislation in 2005. A study looking at the impact of the ban on smoking in indoor public places on pregnant women in Italy, reported a marked drop in exposure to SHS in pregnant women in the workplace but not in the home (55). Spain introduced smoke-free legislation to reduce SHS in 2005. A cross-sectional survey assessed cotinine concentrations in infant cord blood in separate cohorts of mothers and newborns at three time points: 1996–98, 2002–04 (immediately before implementation in 2005), and 2008 (after implementation) of smoke-free work-place bans in Spain. In the 2008 cohort, the percentage of infants with no prenatal SHS exposure (cord blood cotinine 0.2–1 ng/mL) was 73.4%, compared to 56.9% in 2002–04, and 10.8% in 1996–98, showing that public smoking bans reduced prenatal SHS expo-sure (56).
Impact of smoke-free policies on smoking prevalence
General population: There is limited evidence regarding the impact of smoke-free legisla-tion on reduction in active smoking (54).
Pregnant women: In Scotland, researchers found that following implementation of the smoking bans, rates of current smoking among pregnant women dropped significantly from 25.4% to 18.8% (57). Similar results were also observed in a study from the United States, in which pooled data from 225 445 women with live births during 2000–2005 in 29 states and New York City were analyzed. The researchers found that implementing a full private worksite smoking ban increased third trimester quit prevalence by five percent-age points. This suggests that national and local tobacco control policies can effect an increase in smoking cessation in pregnant women (58).
Impact of smoke-free policies on health outcomes
General population: There is strong evidence to suggest that the health of those affected by the smoking ban improves as a result of implementation of the ban (54). A 2010 In-stitute of Medicine report concluded that smoking bans are effective in reducing the risk of coronary heart disease and heart attack (59). The implementation of smoke-free
RECOMMENDATIONS 59
legislation in Scotland has been accompanied by significant reductions in the incidence of both cardiovascular and respiratory disease (57).
Pregnant women: Few studies have demonstrated improvement in birth outcomes fol-lowing smoking bans. Following the introduction of national, comprehensive smoke-free legislation in Scotland, there was a significant drop in overall preterm births (-11.72%, 95% CI -15.87, -7.35, p<0.001), and spontaneous preterm labour (-11.35%, 95% CI -17.20, -5.09, p=0.001), which remained after adjustment for potential confounding factors. Likewise, there was a significant decrease in the number of infants born small for gestational age (24.52%, 95% CI 28.28, 20.60, p=0.024). These significant reductions occurred in both smoking and never-smoking mothers, suggesting that the introduction of smoking bans in Scotland was associated with significant reductions in preterm birth and babies being born small for gestational age (57).
Grading of evidence: Evidence was graded as low due to indirectness.
STRENGTH OF THE RECOMMENDATION
The GDG reviewed the above evidence and considered the harms, benefits, values, pref-erences, feasibility and cost-effectiveness of the proposed recommendation during the drafting process. It was decided that potential benefits strongly outweighed harms, values were in support, and that it was cost effective and feasible and therefore should be clas-sified as a strong recommendation. (See Annex 7 for a detailed description of all issues considered in these domains.)
60 RECOMMENDATIONS
RECOMMENDATIONS 8–9:
Protection from second-hand smoke in pregnancy (smoke-free homes) Health-care providers should provide pregnant women, their partners and other house-hold members with advice and information about the risks of SHS exposure as well as strategies to reduce SHS in the home.
Strength of recommendation: Strong. Quality of evidence: Low Health-care providers should, wherever possible, engage directly with partners and other household members to inform them of the risks of SHS exposure to pregnant women and to promote reduction of exposure and offer smoking cessation support.
Strength of recommendation: Strong. Quality of evidence: Low
REMARKS
The overall goal of the intervention should be to eliminate SHS exposure at home.
Efforts to reduce SHS exposure can also help to reduce active tobacco use in pregnant women.
EVIDENCE FOR RECOMMENDATIONS 8–9
Overall question: What interventions are effective for reducing shs exposure in the home?
PICO (Population, Intervention, Comparison, and Outcome) question used to examine evidence
population Pregnant women (all trimesters) exposed to SHS in their homes Intervention Interventions to reduce SHS exposure at home (e.g. education and coun-
selling to increase awareness in women of harms of exposure and means to minimize them, counselling of husbands, partners or other tobacco-smoking household members)
RECOMMENDATIONS 61

comparison Usual care, no intervention to reduce exposureoutcomes • Reduced exposure of pregnant women to SHS at home
• Quit rates in smoking partners
SYSTEMATIC REVIEWS AND OTHER SOURCES (E.G. QUALITATIVE STUDIES, COST-EFFECTIVENESS ANALYSES) IDENTIFIED BY THE SEARCH PROCESS
No recent systematic reviews of interventions to reduce the exposure of pregnant women to SHS at home were identified. Although the following two reviews focused on the re-duction of SHS exposure of infants rather than pregnant women, these were used for evidence retrieval for interventions aimed at fathers or partners of pregnant women to make homes smoke-free.
Baxter et al. Which interventions are effective and cost-effective in encouraging the establish-
ment of smoke-free homes? 2009 (48, 60).
Hemsing et al. Interventions to improve partner support and partner cessation in pregnancy, 2012 (61).
There is mixed evidence in regard to the effect of counselling plus other interventions (such as provision of written materials or telephone support) on making homes of pregnant women smoke-free. There was also mixed evidence from studies reporting on interven-tions based on the use of motivational interviewing of parents to promote smoke-free homes, and evaluations of individually adapted smoke-free home plans.
WHO commissioned a systematic review on ‘Interventions to reduce SHS exposure among non-smoking pregnant women’, which searched the Cochrane library and eight databases, yielding five studies (62). The results from this review are reported as a narrative synthesis below.
NARRATIVE SYNTHESIS OF KEY FINDINGS
Five studies were found that evaluated a clinical intervention to reduce SHS exposure among non-smoking pregnant women. One RCT conducted in the United States (Wash-ington, DC) among non-smoking African-American pregnant women tested a behavioural intervention that included counselling, role play, skills practice and building negotiation skills with partners and household members who smoked (63). Pregnant women in the intervention group were less likely to report SHS exposure than women in the control group (OR=0.57, 95% CI 0.38–0.84). In an RCT conducted in Guangzhou, China, pregnant women in the intervention group received educational materials and brief advice (2–3
62 RECOMMENDATIONS
minutes) on the harms of SHS from their obstetrician (64). Husbands of women in the intervention group were more likely than those in the control group to not smoke in the previous seven days (8.4% versus 4.8%, p=0.04); however, no difference was found in reported not smoking in the previous 30 days (6.1% versus 4.2%, p=0.26). Another study conducted in Sichuan, China found that by providing educational materials on SHS as well as counselling by obstetricians, significantly decreased mean nicotine concentration in the hair of the mothers in the intervention compared to the controls (for intervention: 0.3 log micro g/g at follow-up compared to 0.5 at baseline; and for control: 0.5 log micro g/g at follow-up compared to 0.4 at baseline) (65).
In an RCT conducted in Isfahan, Iran, midwives were trained to provide 15–20 minutes of education during prenatal care visits on the harms of SHS exposure during prenatal care visits (66). The authors found that pregnant women’s self-reported weekly SHS exposure was lower in the intervention group compared with the control group at each of the third, fourth, and fifth prenatal care sessions, p<0.001 (e.g. at the fifth visit, 12.3 versus 25.4 weekly mean number of cigarettes husband smoked near the woman). There was no difference between the two groups at the initial session. The fifth study in Brisbane, Australia, involved both counselling by a general practitioner and use of a nicotine patch to help partners of pregnant women to quit smoking (67). The authors found that 48 out of 291 men (16.5%) in the intervention group self-reported quitting compared to 25 out of 270 men (9.3%) in the control group (p=0.011, OR=0.52, 95% CI 0.31–0.86); biochemical verification (carbon monoxide testing) was carried out on a subsample of men who reported quitting.
Interventions:
A small number of randomized controlled trials suggest that providing brief advice or counselling to non-smoking pregnant women may reduce SHS exposure; however, stud-ies are needed with biochemical measures of SHS exposure.
Only one study has examined the effect of partner cessation in reducing SHS exposure among non-smoking pregnant women. Similar to other studies in the general population, this study found that counselling and use of a nicotine patch increased quitting among the partners or husbands of pregnant women.
Cost effectiveness: No evidence
Adverse outcomes: No evidence
RECOMMENDATIONS 63
Grading of evidence: The evidence has been graded as low indicating we are uncertain about the estimate of effect. (See annex 6 for GRaDe tables.)
STRENGTH OF THE RECOMMENDATION
The GDG reviewed the above evidence and considered the harms, benefits, values, prefer-ences, feasibility and cost-effectiveness of the proposed recommendation when drafting the recommendation. It was decided that the potential benefits strongly outweighed the harms, values were in support, and that it was feasible and therefore should be classi-fied as a strong recommendation. (See Annex 7 for a detailed description of all issues considered in these domains.)
RESEARCH PRIORITIES 65
research priorities
The GDG identified important gaps in research and knowledge that need to be addressed through primary research and support for development of RCTs of interventions in preg-nancy and the postpartum period. In the evidence review, it was found that very few studies were conducted in low- to middle-income countries. Additionally, there was a dearth of studies on effective interventions for alternative types of smoked tobacco use or smoke-less tobacco use in pregnancy and for creating smoke-free homes for pregnant women.
The group noted that for some research priorities there is planned or ongoing research. Since there is no certainty that the planned or ongoing research would give conclusive results, those research topics are listed as research priorities in this document. Some of these research gaps are crucial as results from these studies will be needed to update the guidelines. GDG also suggested undertaking research on integrated interventions that address tobacco use, as well as other related risk behaviours and mental health conditions in pregnancy.

66 RESEARCH PRIORITIES
RESEARCH PRIORITIES BASED ON SPECIFIC QUESTIONS
Identification of tobacco use and SHS exposure in pregnancy
Implementation research on effective ways to assess tobacco use is needed, with con-centration on major elements such as:
• How to maximize the identification of tobacco use and SHS exposure in pregnant women?
(How to ask, what to ask, who to ask, how to document.)
• Self-reported versus biochemically validated assessment.
• How to conduct objective assessment of smokeless tobacco use and exposure to SHS in
pregnant women? Interview-based versus self-administered.
• Does biochemical validation of tobacco use affect smoking reduction and quit rates in
pregnancy?
• What are the accurate and cost-effective means for biochemically-validating smokeless
tobacco use (urine, saliva etc.)?
• What are the appropriate pregnancy specific cut-off points for validating abstinence?
• What are the cost-effective ways to assess tobacco use and SHS exposure?
Interventions for tobacco-use cessation in pregnancy (psychosocial interventions)
Most research in this area has been carried out in high-income countries. Efficacy and effectiveness studies and implementation research need to be conducted in low- and middle-income countries for various psychosocial interventions such as noted below to promote tobacco-use cessation:
• Brief intervention using ‘5As’ (Ask, Assess, Advise, Assist, and Arrange)
• Feedback to the pregnant woman on fetal health status or measurement of by-products of
tobacco smoke biomarkers
• Motivational interviewing
• Financial incentives (contingency management) to promote cessation
It is important to also find effective interventions that can prevent late pregnancy or postpar-tum relapse in women who spontaneously quit in early pregnancy. Further evaluation of effec-tiveness of specific psychosocial interventions is also required for different types of tobacco product used and for different types of health-care providers implementing the intervention.
RESEARCH PRIORITIES 67
Interventions for tobacco-use cessation in pregnancy (pharmacological interventions)
The evidence base remains limited for making recommendations on the use of phar-macological products for tobacco-use cessation in pregnancy. There are clinical trials in process studying use of various NRT products, varenicline and bupropion in pregnancy. The research topics are listed as research priorities in this document.
As per the GDG’s recommendation, urgently needed research on pharmacological inter-ventions includes:
• studies of factors improving or impeding adherence to pharmacotherapeutic agents;
• a review of the effects (safety profiles, effectiveness ) of NRT use in pregnant women, par-
ticularly in the United kingdom where a historical cohort exists for use of NRT in pregnancy;
• studies comparing the use of lower and higher dose of NRT for tobacco cessation in
pregnancy;
• the use of client preference trials (client’s selection of type of NRT);
• surveillance of current use of pharmacotherapy in pregnancy (focused on determining
whether women use pharmacotherapy when recommended or prescribed by health-care
providers, as well as in the absence of provider advice); and
• use of pharmacotherapy by pregnant women who have a high level of nicotine dependence.
Protection from SHS in pregnancy (smoke-free public places)
The health benefits of smoke-free public places have been well demonstrated in the literature. As more countries are implementing smoke-free legislation, it is essential to assess the impact of smoke-free public policies on pregnant women’s tobacco-use ces-sation, SHS exposure and pregnancy outcomes.
It is important to assess the public’s compliance with smoke-free legislation, specifically in low- and middle-income countries, by studying individual SHS exposure (through self-reported or biochemically-validated means) in public places and workplaces as well as in the home. For source of exposure studies, air quality studies of various sites homes will be needed.
Smoke-free legislation (and compliance) focuses on workplaces and public places. Any ef-fect on reduction in smoking in homes will likely occur through increased public awareness
and changing social norms. It is equally important to assess the impact of smoke-free legislation on the prevalence of smoke-free homes or homes with smoking bans.
Protection from SHS in pregnancy (smoke-free homes)
There is a strong evidence base in favour of smoke-free homes for pregnant women to pro-tect the health of their fetus. However, the evidence base for effective interventions to cre-ate smoke-free homes to protect women’s health is limited. More research is needed on:
• How best to approach and engage the partners of pregnant women, and other household
members to decrease tobacco use among family members and subsequently reduce SHS
exposure in homes for pregnant women.
• How best to biochemically verify SHS exposure reduction in pregnant women and smoking
cessation among partners.
• Identifying inexpensive and simple air quality monitors and their effectiveness as an inter-
vention tool to encourage reduction of smoking in homes.
• Determining the level of intensity that is required for interventions to be effective in prevent-
ing SHS exposure in homes.
• How to increase awareness of health-care providers regarding the importance of screening
pregnant woman for SHS exposure.
68 RESEARCH PRIORITIES
PLANS FOR DISSEMINATING, ADAPTING AND IMPLEMENTING THE RECOMMENDATIONS 69
Plans for disseminating, adapting and implementing the recommendations
GUIDELINES DISSEMINATION
The recommendations in these guidelines will be disseminated through a broad network of international partners, including WHO country and regional offices, ministries of health, WHO collaborating centres, other United Nations agencies (UNICEF, UNFPA, etc.), inter-national development agencies (AusAID, DFID, NORAD, USAID etc.) and nongovernmental organizations. They will also be published on the WHO web site. In addition, a policy brief aimed at policy-makers, programme managers and clinicians will be developed and disseminated.
LOCAL ADAPTATION
These guidelines have been developed for a global audience. It is expected that countries will adapt the recommendations to suit their national needs. These recommendations are intended to be adapted to local needs in line with national and subnational tobacco-control strategies and must be inclusive of all local partners including national and subnational governments, civil society and professional societies of various health-care providers involved in care of the pregnant women.
The adaptation would also need to take into consideration the types of tobacco products predominantly used in the country. Regional and local requirements should be informed by epidemiological and needs assessments and take into account the capacity of the
70 PLANS FOR DISSEMINATING, ADAPTING AND IMPLEMENTING THE RECOMMENDATIONS
health-care system and economic feasibility. Adaptation will include translation into na-tional and local languages. Selection of interventions should be appropriate for specific contexts, such as resources (human and financial) available, health-care setting, and local culture.
Policy-makers should consider how the recommendations in this set of guidelines align with those in other WHO guidelines. This guidance is not intended as a stand-alone docu-ment. It should be viewed in the context of previous WHO guidance on broader issues relating to tobacco, pregnancy and maternal and child health.
LOCAL IMPLEMENTATION
The GDG noted that the first step towards successful implementation of these recom-mendations at the local level would be to obtain endorsement of the stakeholders at country level, including the ministry of health, local professional societies, civil society and community leaders.
For effective use of these recommendations, it is absolutely essential that the health sys-tems at country level create an enabling tobacco control environment for the health-care workers. This may include for example, making health facilities tobacco-free, provision of smoking cessation services for health-care providers who use tobacco, providing tailored training and materials to diverse levels of health-care providers (physicians, mid-level health workers, first-level, community and lay health workers), and modifying antenatal care forms or other recording instruments of the health system to include a check-box and space for provider notes to document tobacco use and SHS exposure and record relevant actions taken. An example of such a document is the antenatal care form used in the Centro Latinoamericano de Perinatología, Salud de la Mujer y Reproductiva (CLAP/SMR-OPS/OMS) system in the Pan American region.1 Table 3 outlines steps that could be taken for implementing specific recommendations.
1 http://new.paho.org/clap
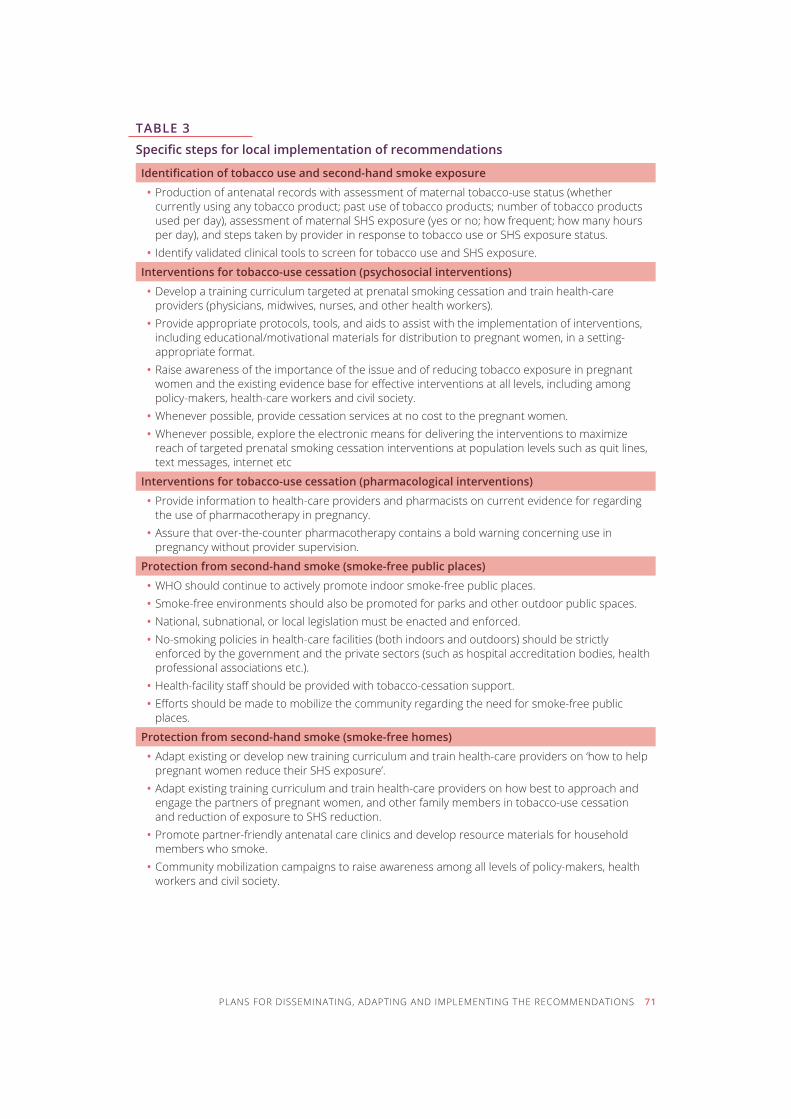
PLANS FOR DISSEMINATING, ADAPTING AND IMPLEMENTING THE RECOMMENDATIONS 71
TABLE 3
Specific steps for local implementation of recommendations
Identification of tobacco use and second-hand smoke exposure
• Production of antenatal records with assessment of maternal tobacco-use status (whether currently using any tobacco product; past use of tobacco products; number of tobacco products used per day), assessment of maternal SHS exposure (yes or no; how frequent; how many hours per day), and steps taken by provider in response to tobacco use or SHS exposure status.
• Identify validated clinical tools to screen for tobacco use and SHS exposure.
Interventions for tobacco-use cessation (psychosocial interventions)
• Develop a training curriculum targeted at prenatal smoking cessation and train health-care providers (physicians, midwives, nurses, and other health workers).
• Provide appropriate protocols, tools, and aids to assist with the implementation of interventions, including educational/motivational materials for distribution to pregnant women, in a setting-appropriate format.
• Raise awareness of the importance of the issue and of reducing tobacco exposure in pregnant women and the existing evidence base for effective interventions at all levels, including among policy-makers, health-care workers and civil society.
• Whenever possible, provide cessation services at no cost to the pregnant women. • Whenever possible, explore the electronic means for delivering the interventions to maximize
reach of targeted prenatal smoking cessation interventions at population levels such as quit lines, text messages, internet etc
Interventions for tobacco-use cessation (pharmacological interventions)
• Provide information to health-care providers and pharmacists on current evidence for regarding the use of pharmacotherapy in pregnancy.
• Assure that over-the-counter pharmacotherapy contains a bold warning concerning use in pregnancy without provider supervision.
Protection from second-hand smoke (smoke-free public places)
• WHO should continue to actively promote indoor smoke-free public places. • Smoke-free environments should also be promoted for parks and other outdoor public spaces. • National, subnational, or local legislation must be enacted and enforced. • No-smoking policies in health-care facilities (both indoors and outdoors) should be strictly
enforced by the government and the private sectors (such as hospital accreditation bodies, health professional associations etc.).
• Health-facility staff should be provided with tobacco-cessation support. • Efforts should be made to mobilize the community regarding the need for smoke-free public
places.
Protection from second-hand smoke (smoke-free homes)
• Adapt existing or develop new training curriculum and train health-care providers on ‘how to help pregnant women reduce their SHS exposure’.
• Adapt existing training curriculum and train health-care providers on how best to approach and engage the partners of pregnant women, and other family members in tobacco-use cessation and reduction of exposure to SHS reduction.
• Promote partner-friendly antenatal care clinics and develop resource materials for household members who smoke.
• Community mobilization campaigns to raise awareness among all levels of policy-makers, health workers and civil society.
EVALUATING THE IMPACT OF THE GUIDELINES
During the guidelines development meeting, the GDG discussed two sets of outcome and process indicators that could be used to measure the impact of the recommendations made in this document (see Table 4). The first set would measure the acceptance and incorporation of these recommendations at the national health system level, such as measured by the number of countries who will adopt these recommendations or num-bers of countries that routinely document tobacco use and SHS exposure in their ANC forms. The second set of indicators would help evaluate the improved health status of the population as a result of successful implementation of the recommendations, such as improvement in perinatal and neonatal outcomes (such as low birth weight, fetal growth restrictions, preterm births, premature rupture of membranes, perinatal mortality etc.), reduction in rates of SIDS, decrease in tobacco use in pregnancy, increase in quit rates and reduction in SHS exposure among pregnant women or women of reproductive age. It may also be measured by improved satisfaction of the pregnant women with antenatal care.
This list is not an exhaustive list of indicators, but provides guidance and variables to measure in assessing uptake of these recommendations and related impacts. Information on many of these indicators may be available through the existing health management information system (HMIS) or national surveillance systems, while for others indicators, periodic surveys or evaluations may be required.
Some of these indicators may be difficult to obtain in low- and middle-income countries. The GDG also noted the need to have a system in place for quality assurance of collected data for these indicators.
72 PLANS FOR DISSEMINATING, ADAPTING AND IMPLEMENTING THE RECOMMENDATIONS
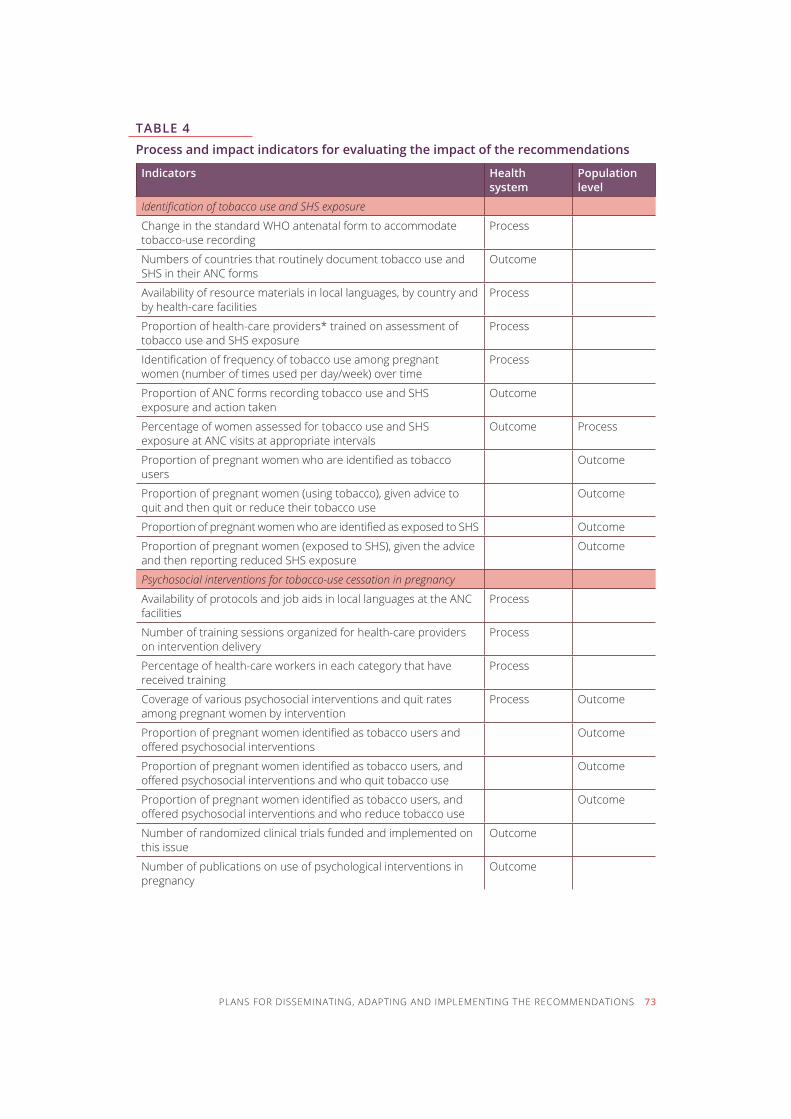
TABLE 4
Process and impact indicators for evaluating the impact of the recommendations
Indicators Health system
Population level
Identification of tobacco use and SHS exposure
Change in the standard WHO antenatal form to accommodate tobacco-use recording
process
Numbers of countries that routinely document tobacco use and SHS in their ANC forms
outcome
Availability of resource materials in local languages, by country and by health-care facilities
process
Proportion of health-care providers* trained on assessment of tobacco use and shs exposure
process
Identification of frequency of tobacco use among pregnant women (number of times used per day/week) over time
process
Proportion of ANC forms recording tobacco use and SHS exposure and action taken
outcome
Percentage of women assessed for tobacco use and SHS exposure at ANC visits at appropriate intervals
outcome process
Proportion of pregnant women who are identified as tobacco users
outcome
Proportion of pregnant women (using tobacco), given advice to quit and then quit or reduce their tobacco use
outcome
Proportion of pregnant women who are identified as exposed to SHS outcome
Proportion of pregnant women (exposed to SHS), given the advice and then reporting reduced shs exposure
outcome
Psychosocial interventions for tobacco-use cessation in pregnancy
Availability of protocols and job aids in local languages at the ANC facilities
process
Number of training sessions organized for health-care providers on intervention delivery
process
Percentage of health-care workers in each category that have received training
process
Coverage of various psychosocial interventions and quit rates among pregnant women by intervention
process outcome
Proportion of pregnant women identified as tobacco users and offered psychosocial interventions
outcome
Proportion of pregnant women identified as tobacco users, and offered psychosocial interventions and who quit tobacco use
outcome
Proportion of pregnant women identified as tobacco users, and offered psychosocial interventions and who reduce tobacco use
outcome
Number of randomized clinical trials funded and implemented on this issue
outcome
Number of publications on use of psychological interventions in pregnancy
outcome
PLANS FOR DISSEMINATING, ADAPTING AND IMPLEMENTING THE RECOMMENDATIONS 73
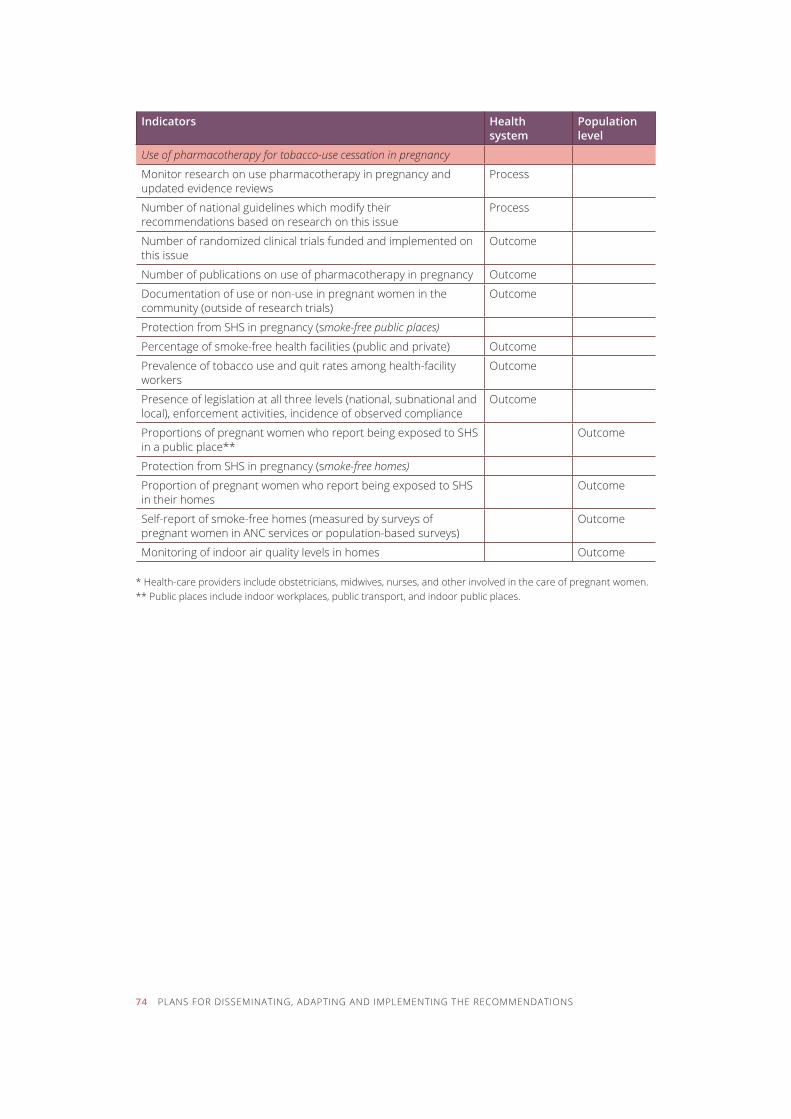
Indicators Health system
Population level
Use of pharmacotherapy for tobacco-use cessation in pregnancy
monitor research on use pharmacotherapy in pregnancy and updated evidence reviews
process
Number of national guidelines which modify their recommendations based on research on this issue
process
Number of randomized clinical trials funded and implemented on this issue
outcome
Number of publications on use of pharmacotherapy in pregnancy outcome
Documentation of use or non-use in pregnant women in the community (outside of research trials)
outcome
Protection from SHS in pregnancy (smoke-free public places)
Percentage of smoke-free health facilities (public and private) outcome
Prevalence of tobacco use and quit rates among health-facility workers
outcome
Presence of legislation at all three levels (national, subnational and local), enforcement activities, incidence of observed compliance
outcome
Proportions of pregnant women who report being exposed to SHS in a public place**
outcome
Protection from SHS in pregnancy (smoke-free homes)
Proportion of pregnant women who report being exposed to SHS in their homes
outcome
Self-report of smoke-free homes (measured by surveys of pregnant women in ANC services or population-based surveys)
outcome
Monitoring of indoor air quality levels in homes outcome
* Health-care providers include obstetricians, midwives, nurses, and other involved in the care of pregnant women.** Public places include indoor workplaces, public transport, and indoor public places.
74 PLANS FOR DISSEMINATING, ADAPTING AND IMPLEMENTING THE RECOMMENDATIONS
REVIEW AND UPDATE OF THE RECOMMENDATIONS 75
Review and update of the recommendations
These recommendations will be regularly updated as new evidence becomes available. The next major update will be considered in 2018, with the oversight of the WHO Guidelines Review Committee, as new evidence becomes available.
Feedback from communities and other stakeholders will help guide revision of the next edition of these guidelines. WHO welcomes suggestions regarding additional questions for inclusion in the next update.
please e-mail your suggestions to [email protected].

76
References
INTRODUCTION AND METHODOLOGY SECTION
1. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to
2030. PLoS Medicine, 2006, 3(11):e442.
2. IARC monographs on the evaluation of carcinogenic risks to humans: volume 100E: a review of
human carcinogens: personal habits and indoor combustions. Lyon, International Agency for
Research on Cancer, 2010.
3. The health consequences of smoking: a report of the surgeon general. Atlanta, GA, US Depart-
ment of Health and Human Services, Centers for Disease Control and Prevention, Office
on Smoking and Health, 2004.
4. Alverson CJ et al. Maternal smoking and congenital heart defects in the Baltimore-Wash-
ington infant study. Pediatrics, 2011, 127:3 e647–e653, [published ahead of print February
28, 2011, doi:10.1542/peds.2010–1399].
5. How tobacco smoke causes disease: the biology and behavioral basis for smoking-attributable
disease: a report of the surgeon general. Atlanta, GA, US Department of Health and Human
Services, Centers for Disease Control and Prevention, Office on Smoking and Health, 2010.
6. The health consequences of involuntary exposure to tobacco smoke: a report of the surgeon
general. Atlanta, GA, US Department of Health and Human Services, Centers for Disease
Control and Prevention, Office on Smoking and Health, 2006.
7. Barker DJ. The fetal and infant origins of adult disease. British Medical Journal, 1990, 301:1111.
8. Health effects of smokeless tobacco products. Scientific Committee on Emerging and Newly
Identified Health Risks (SCENIHR), 2008, [available at: http://ec.europa.eu/health/ph_risk/
REFERENCES 77
committees/04_scenihr/docs/scenihr_o_013.pdf, [accessed 12 August 2013].
9. IARC monographs on the evaluation of carcinogenic risks to humans: volume 85: betel-quid
and areca-nut chewing and some areca-nut-derived nitrosamines. Lyon, France, International
Agency for Research on Cancer, 2004.
10. IARC monographs on the evaluation of carcinogenic risks to humans: volume 89: smokeless
tobacco and some tobacco-specific N-Nitrosamines. Lyon, France, International Agency for
Research on Cancer, 2007.
11. Gupta PC, Subramoney S. Smokeless tobacco use and risk of stillbirth: a 556 cohort study
in Mumbai, India. Epidemiology, 2006, 17(1):47–51.
12. Wikström Ak et al. Effect of Swedish snuff (snus) on preterm birth. BJOG: An International
Journal of Obstetrics and Gynaecology, 2010, 117(8):1005–1010.
13. Wikström Ak et al. Maternal use of Swedish snuff (snus) and risk of stillbirth. Epidemiology,
2010, 21(6):772–778.
14. Leonardi-Bee J, Britton J, Venn A. Secondhand smoke and adverse fetal outcomes in non-
smoking pregnant women: a meta-analysis. Pediatrics, 2011 Apr;127(4):734–41
15. World Health Organization. The Millennium development goals and tobacco control: an op-
portunity for global partnership. Geneva, World Health Organization, 2004.
16. World Health Organization. WHO report on the global tobacco epidemic: warning about the
dangers of tobacco. Geneva, World Health Organization, 2011.
17. Samet JM, Yoon SY. Women and the tobacco epidemic: challenges for the 21st century. WHO,
Institute for Global Tobacco Control, Johns Hopkins School of Public Health, 2011.
18. World Health Organization. WHO report on the global tobacco epidemic, 2008: the MPOWER
package. Geneva, World Health Organization, 2008.
19. Warren CW et al. Change in tobacco use among 13–15 year olds between 1999 and 2008: findings
from the Global Youth Tobacco Survey. Global Health Promotion, 2009, Sep;16(2 Suppl):38–90.
20. Global estimate of the burden of disease from second-hand smoke. Öberg M et al. Geneva,
World Health Organization, 2010.
21. Current tobacco use and secondhand smoke exposure among women of reproductive
age – 14 countries, 2008–2010. Centers for Disease Control and Prevention (CDC), Morbidity
and Mortality Weekly Report (MMWR), 2012, Nov 2;61:877–82.
22. Global report on the tobacco use and second-hand smoke exposure in pregnancy. Geneva,
World Health Organization [in press].
23. Bloch M et al. Tobacco use and secondhand smoke exposure in pregnancy: an investi-
gative survey of women in 9 developing nations. American Journal of Public Health, 2008,
98(10):1833–40.
24. WHO framework convention on tobacco control. Geneva, World Health Organization, 2003 (up-
dated 2004, 2005), [available at: http://www.who.int/tobacco/framework/WHO_FCTC_english.
78 REFERENCES
pdf, accessed 12 August 2013].
25. United Nations General Resolution 55/2. United Nations Millennium Declaration, 2000,
[available at: www.un.org/millennium/declaration/ares552e.pdf, accessed 12 August 2013).
26. United Nations General Resolution 66/2. Political declaration of the high-level meeting of
the General Assembly on the prevention and control of non-communicable diseases, 2011,
[available at: http://www.un.org/depts/dhl/resguide/r66.shtml, accessed 12 August 2013].
27. McBride CM et al. Understanding the potential of teachable moments: the case of smoking
cessation. Health Education Research, 2003, 18(2):156–170.
28. DiClemente C, Dolan-Mullen P, Windsor R. The process of pregnancy smoking cessation:
implications for interventions. Tobacco Control, 2000, 9(Suppl 3):16–21.
29. Mahfoud Z et al. Determinants of change in paternal smoking trends during pregnancy in
Lebanon. Acta Obstetricia et Gynecologica Scandinavica, 2012, 89(4):587–591.
30. World population prospects: the 2010 revision [CD-ROM Edition] United Nations, Department
of Economic and Social Affairs, 2011.
31. Global Health Observatory Data Repository. World Health Organization, 2012, [available at:
http://apps.who.int/gho/data/#, accessed 12 August 2013].
32. Jha P et al. 21st-century hazards of smoking and benefits of cessation in the United States.
New England Journal of Medicine, 2013, 368:341–350.
33. WHO handbook for guideline development. World Health Organization [available at: http://www.
who.int/iris/bitstream/10665/75146/1/9789241548441_eng.pdf, accessed 12 August 2013].
RECOMMENDATIONS
34. Convention on the Elimination of All Forms of Discrimination against Women (CEDAW), United
Nations, 1979.
35. Report of the International Conference on Population and Development. International Con-
ference on Population and Development – ICPD – Programme of Action. A/CONF.171/13/
Rev.1.,Cairo, 1994.
Recommendation 1
36. Fiore MC et al. Treating tobacco use and dependence: 2008 update. Rockville, MD, US Depart-
ment of Health and Human Services.
37. The ASSIST-linked brief intervention for hazardous and harmful substance use: manual for use in pri-
mary care. Prepared by R. Humeniuk et al. World Health Organization, 2010b [available at: http://
whqlibdoc.who.int/publications/2010/9789241599399_eng.pdf, accessed 12 August 2013].
38. Methods for evaluating tobacco control policies 2008. Lyon, International Agency for Research
REFERENCES 79
80 REFERENCES
on Cancer and the World Health Organization, 2008 (IARC Handbooks of Cancer Preven-
tion, Tobacco Control, Vol. 12.
39. How to stop smoking in pregnancy and following childbirth. NICE public health guidance 26,
London, National Institute for Health and Clinical Excellence.
40. Flemming k et al. Smoking in pregnancy: a systematic review of qualitative research of
women who commence pregnancy as smokers. The Journal of Advanced Nursing, 2012, Dec
19, doi: 10.1111/jan.12066, [Epub ahead of print].
41. WHO Monograph – Gender, women, and the tobacco epidemic. Geneva, World Health Organiza-
tion, 2010a. [available at: http://who.int/tobacco/publications/gender/women_tob_epidemic/
en/index.html, accessed 12 August 2013).
42. Guidelines for controlling and monitoring the tobacco epidemic. Geneva, World Health Orga-
nization, 1998.
43. Shipton D et al. Reliance on self-reported smoking in pregnancy underestimates smoking
prevalence and reduces the reach of specialist cessation services: results from a retrospec-
tive, cross-sectional study. British Medical Journal, 2009, 339:4347.
Recommendation 2
44. Prochaska J, Velicer W. Introduction: the transtheoretical model. American Journal of Health
Promotion, 1997, 12:6–7.
45. Lumley J et al. Interventions for promoting smoking cessation in pregnancy. Cochrane
Database of Systematic Reviews, 2009, Issue 3.
46. Coleman T et al. Pharmacological interventions for promoting smoking cessation in preg-
nancy. Cochrane Database of Systematic Reviews, 2012, Issue 9.
47. Chamberlain C et al. Psychosocial interventions to support women to stop smoking in pregnancy:
a systematic review. Preliminary report of evidence from a Cochrane Systematic Review for
the World Health Organization, October 2012.
48. Baxter S et al. The health consequences of pregnant women cutting down as op-
posed to quitting. Supplementary Report for National Institute for Health and Clinical
Excellence, the United kingdom, 2009, [available at: http://www.nice.org.uk/nicemedia/
live/13023/49420/49420.pdf, accessed 12 August 2013].
49. Taylor M. Economic analysis of interventions for smoking cessation aimed at pregnant women.
Supplementary Report for National Institute for Health and Clinical Excellence, the United
kingdom, 2009, [available at: http://www.nice.org.uk/nicemedia/live/13023/49421/49421.pdf,
accessed 12 August 2013].
50. Ebbert J et al. Interventions for smokeless tobacco-use cessation. Cochrane Database of
Systematic Reviews, 2011, Issue 2.
REFERENCES 81
Recommendations 3–5
51. Greaves, L et al. (2nd ed.) Expecting to quit: a best practices review of smoking cessation
interventions for pregnant and post-partum women. Vancouver, British Columbia Centre of
Excellence for Women’s Health, 2011.
52. Myung S-k et al. [and for the korean Meta-Analysis (kORMA) Study Group]. Efficacy and
safety of pharmacotherapy for smoking cessation among pregnant smokers: a meta-anal-
ysis. BJOG: International Journal of Obstetrics & Gynaecology, 2012, 119:1029–1039.
Recommendations 6–7
53. WHO framework convention on tobacco control. Guidelines for implementation. [Article 5.3;
Article 8; Article 11; Article 13]. Geneva, World Health Organization, 2009 [available at: http://
whqlibdoc.who.int/publications/2009/9789241598224_eng.pdf, accessed 12 August 2013].
54. Callinan JE et al. Legislative smoking bans for reducing secondhand smoke exposure,
smoking prevalence and tobacco consumption. Cochrane Database of Systematic Reviews,
2010, Issue 4.
55. Charrier L et al. Smoking habits in Italian pregnant women: any changes after the ban?
Journal of Public Health Policy, 2010, Apr 31(1):51–8.
56. Puig C et al. Assessment of prenatal exposure to tobacco smoke by cotinine in cord blood for
the evaluation of smoking control policies in Spain. BMC Pregnancy Childbirth, 2012, Apr 5;12:26.
57. Mackay DF et al. Impact of Scotland’s smoke-free legislation on pregnancy complications:
retrospective cohort study. PLoS Med. 2012, 9(3):e1001175 [Epub 2012 Mar 6].
58. Adams Ek et al. Reducing prenatal smoking: the role of state policies. American Journal of
Preventive Medicine, 2012, 43;1:34–40.
59. Secondhand smoke exposure and cardiovascular effects: making sense of the evidence. National
Research Council, Washington, DC, The National Academies Press, 2010.
Recommendations 8–9
60. Baxter S et al. The effectiveness of interventions to establish smoke-free homes in preg-
nancy and in the neonatal period: a systematic review. Health Education Research, 2011,
26(2):265–282.
61. Hemsing N et al. Partner support for smoking cessation In pregnancy: a systematic review.
Nicotine & Tobacco Research, 2012, 14(7):767–776
62. Tong et al. Clinical interventions to reduce second-hand smoke among non-smoking preg-
nant women: a systematic review. Unpublished, 2012.
82 REFERENCES
63. El-Mohandes AAE et al. An intervention to reduce environmental tobacco smoke exposure
improves pregnancy outcomes. Pediatrics, 2010, 125(4):721–8.
64. Loke AY, Lam TH. A randomized controlled trial of the simple advice given by obstetricians
in Guangzhou, China, to non-smoking pregnant women to help their husbands quit smok-
ing. Patient Education and Counseling, 2005, 59(1):31–37.
65. Yang L, Mao Z. Intervention on the exposure to passive smoking for non-smoking pregnant
women. Chinese Journal of Prevention and Control of Chronic Diseases, 2012, 18(3):226–228.
66. kazemi A et al. A randomized trial to promote health belief and to reduce environmental
tobacco smoke exposure in pregnant women. Health Education Research, 2012, 27(1):151–159.
67. Stanton WR et al. Randomised control trial of a smoking cessation intervention directed
at men whose partners are pregnant. Preventive Medicine, 2004, 38(1):6–9.
annexes
aNNeX 1
Technical Secretariat for the guidelines development
name Affiliation
Dr Lubna Ishaq Bhatti World Health Organization
Dr Edouard Tursan d’Espaignet World Health Organization
dr nicolas clark World Health Organization
Dr Vladimir Poznyak World Health Organization
Dr Michele Bloch National Cancer Institute, USA
Dr Patricia Dietz Centers for Disease Control and Prevention, USA
dr Lucinda england Centers for Disease Control and Prevention, USA
dr italia v rolle Centers for Disease Control and Prevention, USA
ms van t tong Centers for Disease Control and Prevention, USA
ANNEXES 83

ANNEX 2
WHO staff (HQ, regions and country office) involved in the guidelines development
name Affiliation
Dr Avni Amin Gender, Reproductive Rights, Sexual Health and Adolescence
Dr Lubna Ishaq Bhatti Prevention of Noncommunicable Diseases
dr nicolas clark mental health and substance abuse
dr toker erguder WHO Country office Turkey
dr dongbo fu Prevention of Noncommunicable Diseases
mrs helena maria nygren Krug Gender, Equity and Human Rights
Dr Mathew Mathai Epidemiology, Monitoring and Evaluation
dr mario merialdi Research, Evidence and Norms
Dr Vladimir Poznyak mental health and substance abuse
Dr Edouard Tursan d’Espaignet Prevention of Noncommunicable Diseases
Mr James Rarick WP/TFI Tobacco-free initiative
Dr Daravuth Yel WHO Country office Cambodia
84 ANNEXES
ANNEX 3
Guidelines Development Group
3.1 GDG membership
Dr Fernando ALTHABE
Principal Investigator and Director, Institute for Clinical Effectiveness and Health Policy (ICES),
Buenos Aires, Argentina
Professor Linda BAULD
School of Management and Uk Centre for Tobacco Control Studies, University of Stirling,
United kingdom
Dr jacqueline BELL
Senior Officer, Health Department, Maternal, Newborn & Child Health, International Federation
of Red Cross and Red Crescent Societies, Geneva, Switzerland
Dr Yves BERGEVIN
Senior Maternal Health Advisor, Coordinator, Maternal Health Thematic Fund, TD, United Na-
tions Population Fund (UNFPA), New York, USA
Professor Monique CHAAYA
Professor & Chair, Department of Epidemiology and Population Health, Faculty of Health Sci-
ences, American University of Beirut, Beirut, Lebanon
Professor Sophie CHAN
Professor and Director of Research, School of Nursing, The University of Hong kong, Hong
kong, China
Dr Prakash GUPTA
Director, Healis – Sekhsaria Institute for Public Health, Mumbai, India
Ms Margaretha HAGLUND
Tobacco Control Expert, ThinkTank Tobaksfakta, Stockholm, Sweden
Dr Fatanah ISMAIL
Senior Principal Assistant Director (Primary Care Section), Family Health Development Division,
Ministry of Health, Malaysia
Dr Katherine MURPHY
Chronic Disease Initiative in Africa, Department of Medicine, University of Cape Town, South Africa
Dr Isabel NERIN
Professor, Department of Medicine and Psychiatry, Faculty of Medicine, University of Zaragoza, Spain
Dr Cheryl ONCKEN
Department of Medicine and Obstetrics & Gynecology, University of Connecticut School of
Medicine, Farmington, CT, USA
ANNEXES 85
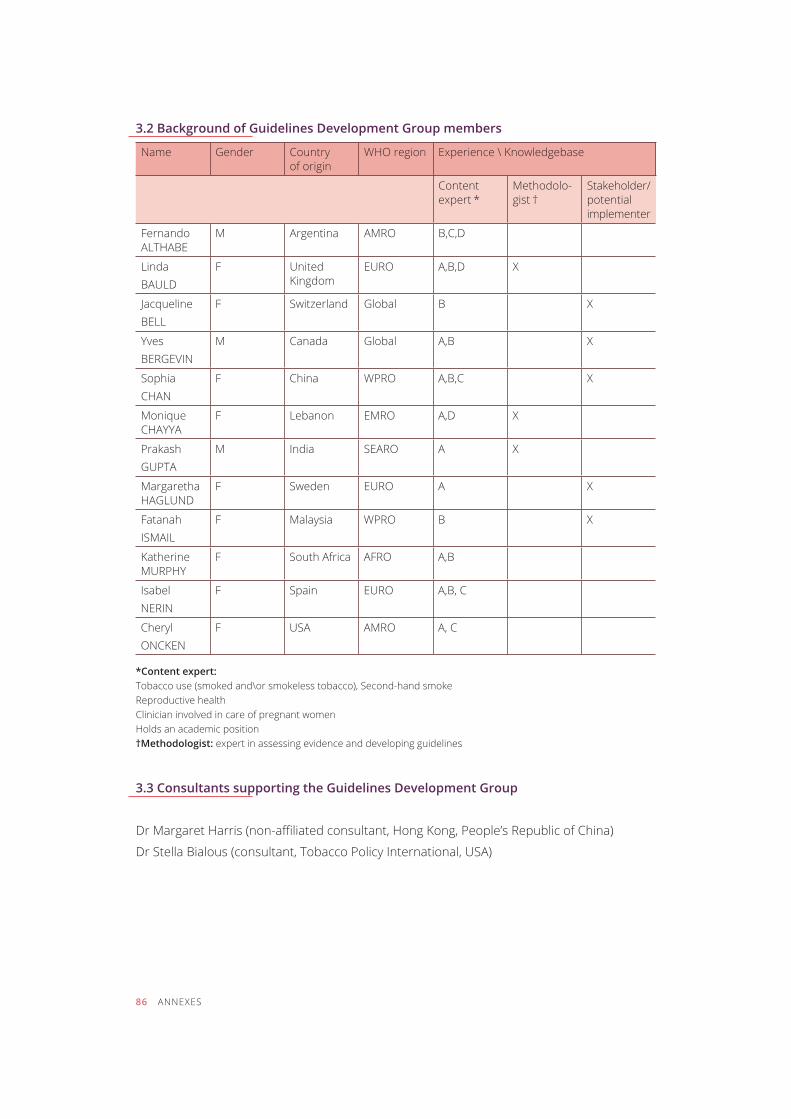
3.2 Background of Guidelines Development Group members
name gender country of origin
Who region Experience \ knowledgebase
content expert *
methodolo-gist †
Stakeholder/ potential implementer
fernando ALTHABE
m argentina amro B,C,D
Linda BAULD
f United Kingdom
EURO A,B,D X
Jacqueline BELL
f Switzerland global B X
Yves BERGEVIN
m canada global A,B X
sophia chan
f china Wpro A,B,C X
monique CHAYYA
f Lebanon emro A,D X
prakash GUPTA
m india searo a X
margaretha HAGLUND
f Sweden EURO a X
fatanah ismaiL
f malaysia Wpro B X
Katherine MURPHY
f South Africa afro A,B
isabel nerin
f spain EURO A,B, C
cheryl oncKen
f USA amro A, C
*Content expert:Tobacco use (smoked and\or smokeless tobacco), Second-hand smokeReproductive healthClinician involved in care of pregnant womenholds an academic position†Methodologist: expert in assessing evidence and developing guidelines
3.3 Consultants supporting the Guidelines Development Group
Dr Margaret Harris (non-affiliated consultant, Hong kong, People’s Republic of China)
Dr Stella Bialous (consultant, Tobacco Policy International, USA)
86 ANNEXES
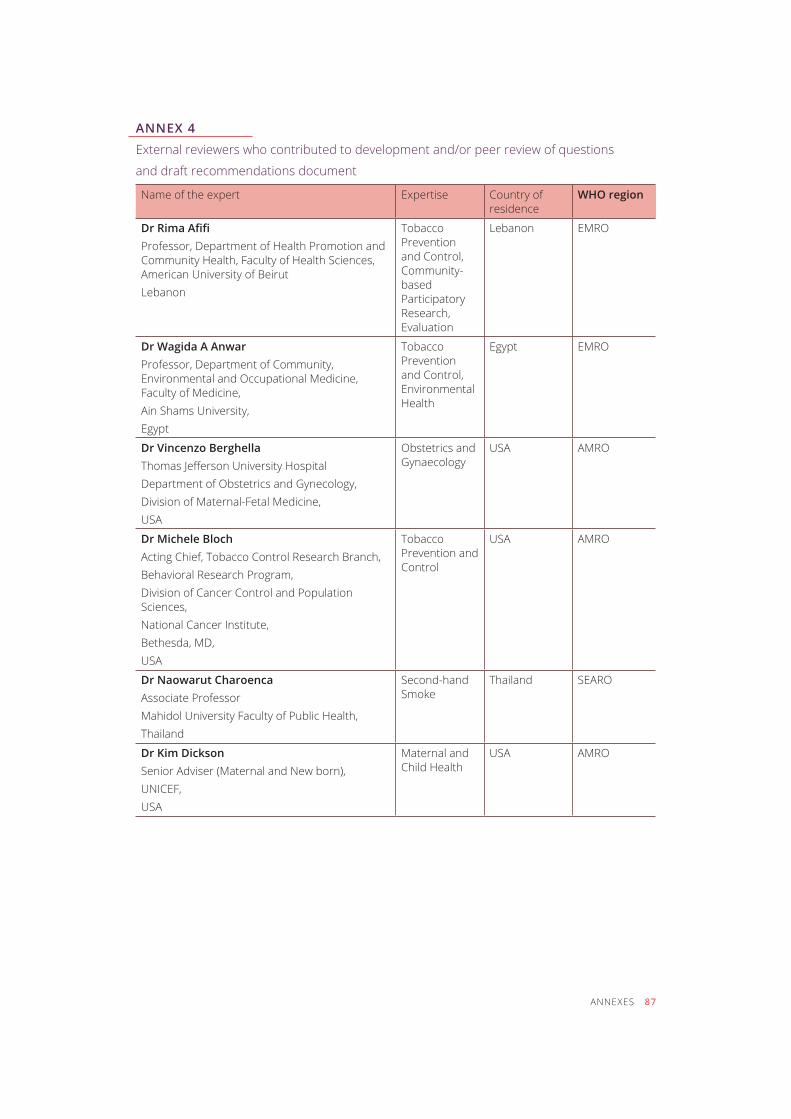
ANNEX 4
External reviewers who contributed to development and/or peer review of questions
and draft recommendations document
Name of the expert expertise Country of residence
WHO region
Dr Rima afifi Professor, Department of Health Promotion and Community Health, Faculty of Health Sciences, American University of BeirutLebanon
tobacco Prevention and Control, community-based participatory Research, Evaluation
Lebanon emro
Dr Wagida A AnwarProfessor, Department of Community, Environmental and Occupational Medicine, Faculty of Medicine,Ain Shams University,egypt
tobacco Prevention and Control, Environmental health
egypt emro
Dr Vincenzo BerghellaThomas Jefferson University HospitalDepartment of Obstetrics and Gynecology,Division of Maternal-Fetal Medicine,USA
obstetrics and gynaecology
USA amro
Dr Michele Bloch Acting Chief, Tobacco Control Research Branch, Behavioral Research Program,Division of Cancer Control and Population Sciences, National Cancer Institute, Bethesda, MD, USA
tobacco Prevention and control
USA amro
Dr Naowarut CharoencaAssociate ProfessorMahidol University Faculty of Public Health,thailand
second-hand smoke
thailand searo
Dr Kim DicksonSenior Adviser (Maternal and New born),UNICEF,USA
maternal and child health
USA amro
ANNEXES 87
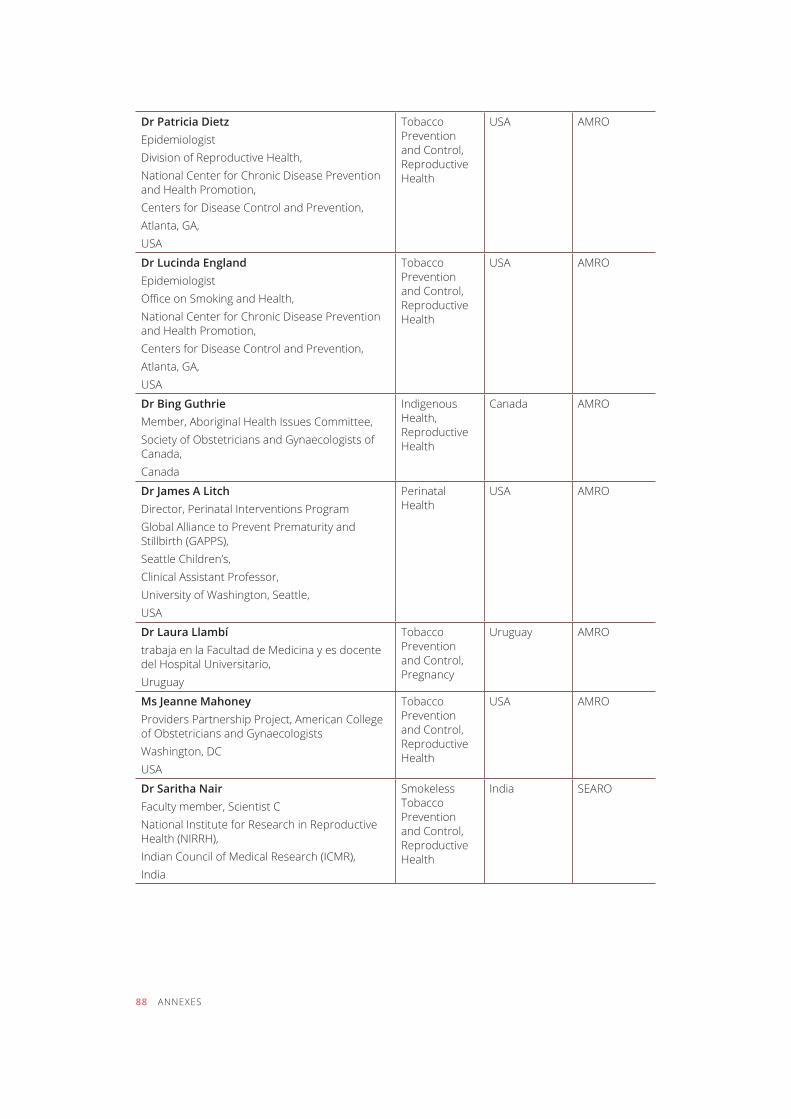
Dr Patricia Dietzepidemiologist Division of Reproductive Health, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention,Atlanta, GA,USA
tobacco Prevention and Control, Reproductive health
USA amro
Dr Lucinda England epidemiologist Office on Smoking and Health,National Center for Chronic Disease Prevention and Health Promotion,Centers for Disease Control and Prevention, Atlanta, GA,USA
tobacco Prevention and Control, Reproductive health
USA amro
Dr Bing GuthrieMember, Aboriginal Health Issues Committee,Society of Obstetricians and Gynaecologists of Canada,canada
indigenous Health, Reproductive health
canada amro
Dr james A LitchDirector, Perinatal Interventions Program Global Alliance to Prevent Prematurity and Stillbirth (GAPPS), Seattle Children’s,Clinical Assistant Professor,University of Washington, Seattle,USA
perinatal health
USA amro
Dr Laura Llambí trabaja en la facultad de medicina y es docente del Hospital Universitario, Uruguay
tobacco Prevention and Control, pregnancy
Uruguay amro
Ms jeanne MahoneyProviders Partnership Project, American College of Obstetricians and GynaecologistsWashington, DCUSA
tobacco Prevention and Control, Reproductive health
USA amro
Dr Saritha NairFaculty member, Scientist CNational Institute for Research in Reproductive Health (NIRRH), Indian Council of Medical Research (ICMR),india
smokeless tobacco Prevention and Control, Reproductive health
india searo
88 ANNEXES
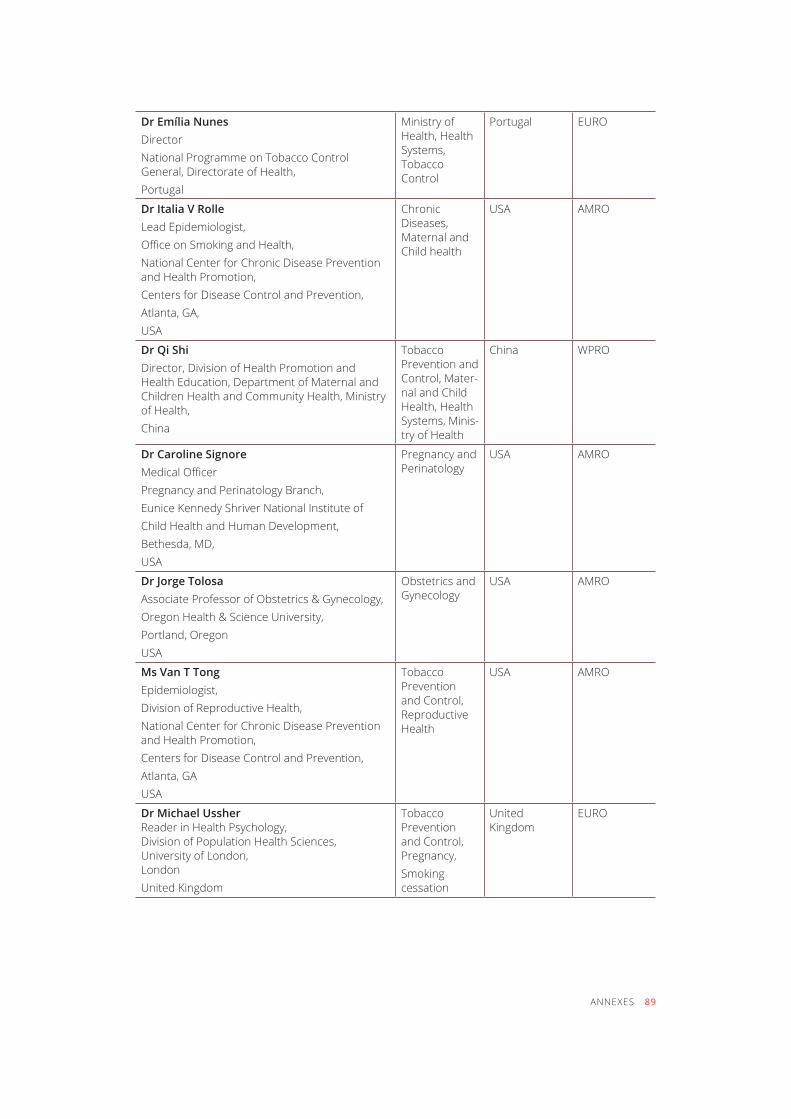
Dr Emília Nunesdirector national programme on tobacco control General, Directorate of Health,portugal
Ministry of Health, Health Systems, tobacco control
portugal EURO
Dr Italia V RolleLead Epidemiologist, Office on Smoking and Health,National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention, Atlanta, GA,USA
chronic Diseases, maternal and child health
USA amro
Dr Qi ShiDirector, Division of Health Promotion and Health Education, Department of Maternal and Children Health and Community Health, Ministry of Health, china
tobacco Prevention and Control, Mater-nal and child Health, Health Systems, Minis-try of Health
china Wpro
Dr Caroline Signore Medical OfficerPregnancy and Perinatology Branch,Eunice kennedy Shriver National Institute ofChild Health and Human Development,Bethesda, MD, USA
pregnancy and perinatology
USA amro
Dr jorge TolosaAssociate Professor of Obstetrics & Gynecology,Oregon Health & Science University,Portland, Oregon USA
obstetrics and gynecology
USA amro
Ms Van T Tong Epidemiologist, Division of Reproductive Health,National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention, Atlanta, GAUSA
tobacco Prevention and Control, Reproductive health
USA amro
Dr Michael Ussher Reader in Health Psychology, Division of Population Health Sciences, University of London, London United kingdom
tobacco Prevention and Control, Pregnancy,smoking cessation
United Kingdom
EURO
ANNEXES 89
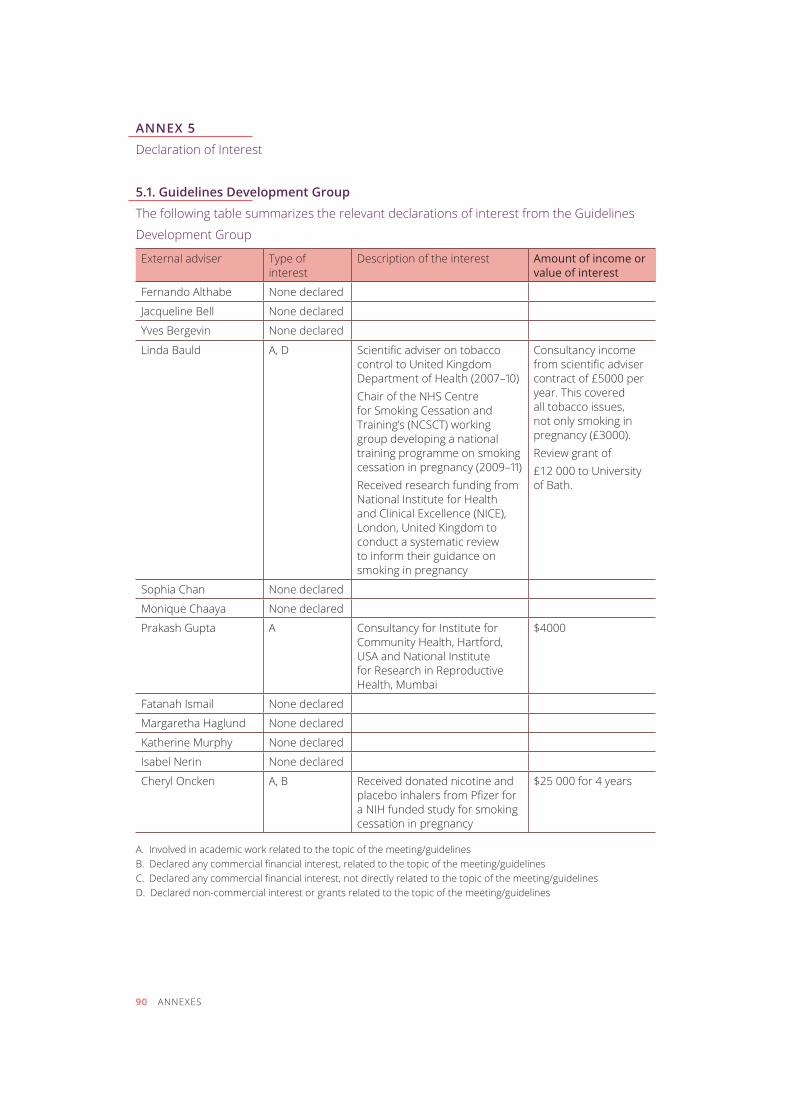
ANNEX 5
Declaration of Interest
5.1. Guidelines Development Group
The following table summarizes the relevant declarations of interest from the Guidelines
Development Group
External adviser Type of interest
Description of the interest amount of income or value of interest
fernando althabe none declared
Jacqueline Bell none declared
Yves Bergevin none declared
Linda Bauld A, D Scientific adviser on tobacco control to United kingdom Department of Health (2007–10) Chair of the NHS Centre for Smoking Cessation and Training’s (NCSCT) working group developing a national training programme on smoking cessation in pregnancy (2009–11)Received research funding from National Institute for Health and Clinical Excellence (NICE), London, United kingdom to conduct a systematic review to inform their guidance on smoking in pregnancy
consultancy income from scientific adviser contract of £5000 per year. This covered all tobacco issues, not only smoking in pregnancy (£3000).Review grant of £12 000 to University of Bath.
sophia chan none declared
monique chaaya none declared
prakash gupta a Consultancy for Institute for Community Health, Hartford, USA and National Institute for Research in Reproductive Health, Mumbai
$4000
fatanah ismail none declared
margaretha haglund none declared
Katherine murphy none declared
isabel nerin none declared
cheryl oncken A, B Received donated nicotine and placebo inhalers from Pfizer for a NIH funded study for smoking cessation in pregnancy
$25 000 for 4 years
A. Involved in academic work related to the topic of the meeting/guidelinesB. Declared any commercial financial interest, related to the topic of the meeting/guidelinesC. Declared any commercial financial interest, not directly related to the topic of the meeting/guidelinesD. Declared non-commercial interest or grants related to the topic of the meeting/guidelines
90 ANNEXES
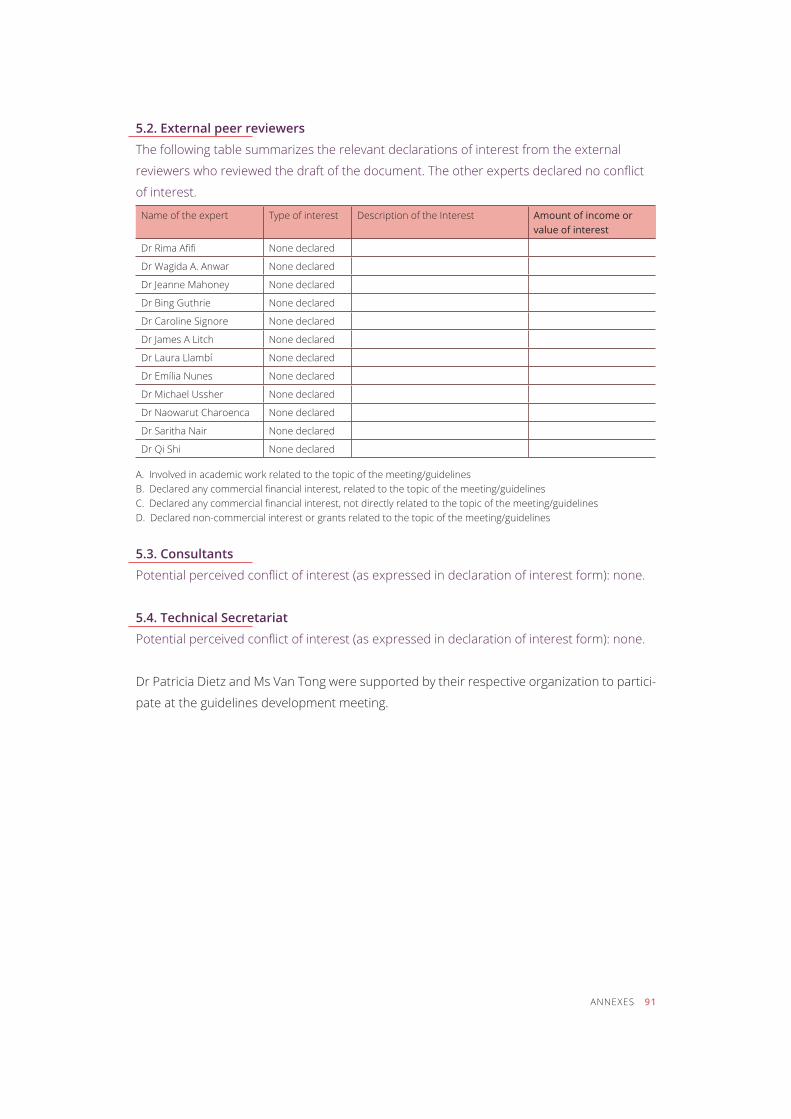
5.2. External peer reviewers
The following table summarizes the relevant declarations of interest from the external
reviewers who reviewed the draft of the document. The other experts declared no conflict
of interest.
Name of the expert Type of interest Description of the Interest amount of income orvalue of interest
Dr Rima Afifi none declared
Dr Wagida A. Anwar none declared
Dr Jeanne Mahoney none declared
Dr Bing Guthrie none declared
dr caroline signore none declared
Dr James A Litch none declared
Dr Laura Llambí none declared
Dr Emília Nunes none declared
Dr Michael Ussher none declared
Dr Naowarut Charoenca none declared
dr saritha nair none declared
dr Qi shi none declared A. Involved in academic work related to the topic of the meeting/guidelinesB. Declared any commercial financial interest, related to the topic of the meeting/guidelinesC. Declared any commercial financial interest, not directly related to the topic of the meeting/guidelinesD. Declared non-commercial interest or grants related to the topic of the meeting/guidelines
5.3. Consultants
Potential perceived conflict of interest (as expressed in declaration of interest form): none.
5.4. Technical Secretariat
Potential perceived conflict of interest (as expressed in declaration of interest form): none.
Dr Patricia Dietz and Ms Van Tong were supported by their respective organization to partici-
pate at the guidelines development meeting.
ANNEXES 91
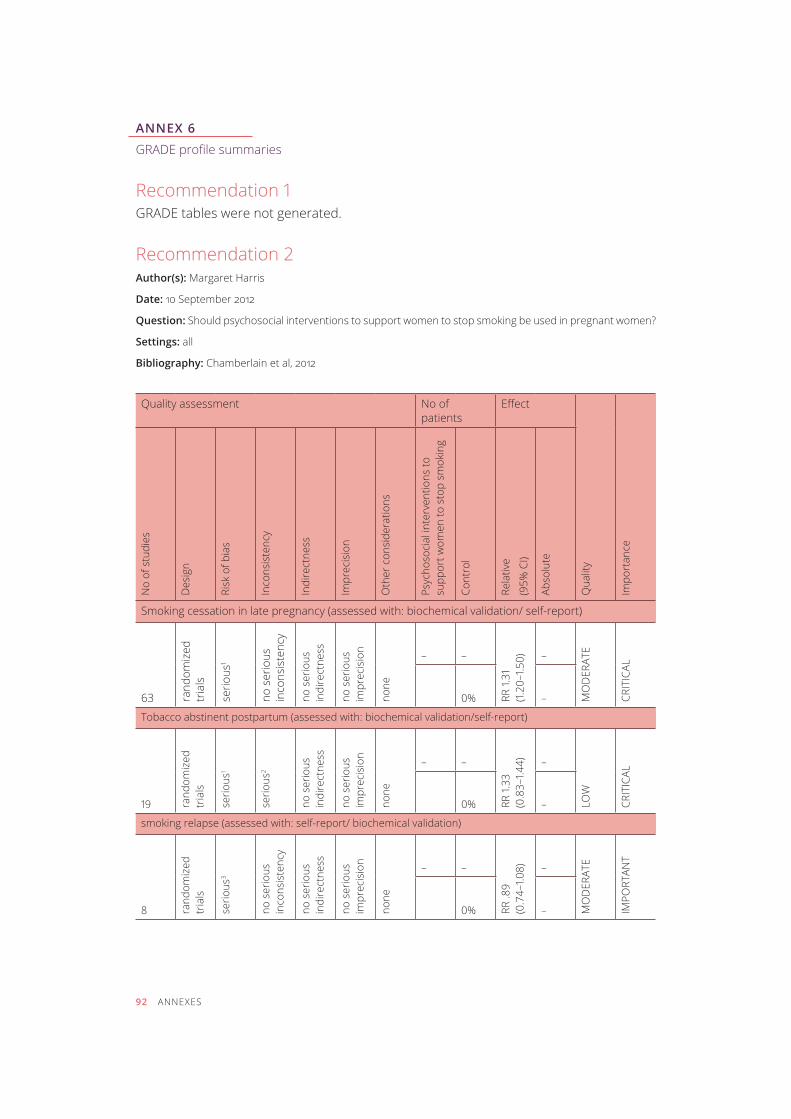
ANNEX 6
GRADE profile summaries
Recommendation 1GRADE tables were not generated.
Recommendation 2Author(s): margaret harris
Date: 10 September 2012
Question: Should psychosocial interventions to support women to stop smoking be used in pregnant women?
Settings: all
Bibliography: Chamberlain et al, 2012
Quality assessment No of patients
Effect
Qua
lity
impo
rtan
ce
No
of s
tudi
es
des
ign
Risk
of b
ias
inco
nsis
tenc
y
indi
rect
ness
impr
ecis
ion
oth
er c
onsi
dera
tions
Psyc
hoso
cial
inte
rven
tions
to
supp
ort w
omen
to s
top
smok
ing
cont
rol
Rela
tive
(95%
CI)
abso
lute
Smoking cessation in late pregnancy (assessed with: biochemical validation/ self-report)
63 rand
omiz
ed
tria
ls
serio
us1
no s
erio
us
inco
nsis
tenc
y
no s
erio
us
indi
rect
ness
no s
erio
us
impr
ecis
ion
none
– –
RR 1.
31
(1.20
–1.5
0) –
mo
der
ate
crit
icaL
0% –
Tobacco abstinent postpartum (assessed with: biochemical validation/self-report)
19 rand
omiz
ed
tria
ls
serio
us1
serio
us2
no s
erio
us
indi
rect
ness
no s
erio
us
impr
ecis
ion
none
– –
RR 1.
33
(0.8
3–1.4
4) –
LoW
crit
icaL
0% –
smoking relapse (assessed with: self-report/ biochemical validation)
8 rand
omiz
ed
tria
ls
serio
us3
no s
erio
us
inco
nsis
tenc
y
no s
erio
us
indi
rect
ness
no s
erio
us
impr
ecis
ion
none
– –
RR .8
9 (0
.74–
1.08) –
mo
der
ate
impo
rtan
t
0% –
92 ANNEXES
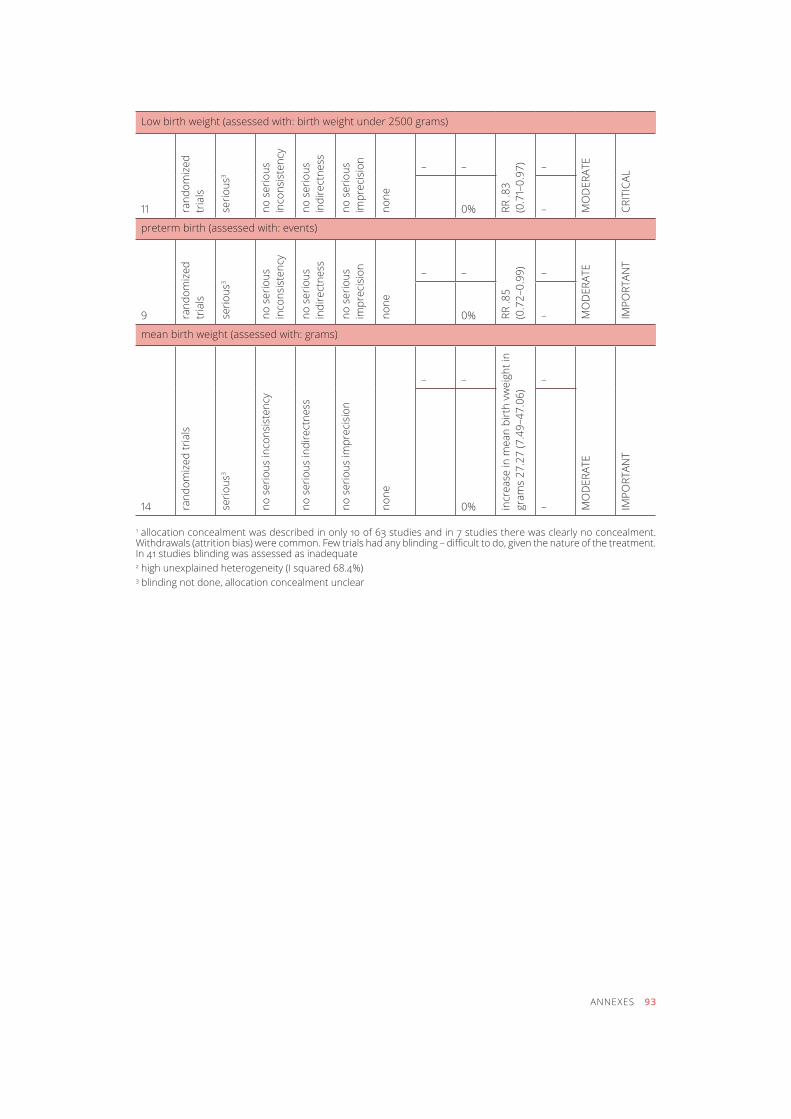
Low birth weight (assessed with: birth weight under 2500 grams)
11 rand
omiz
ed
tria
ls
serio
us3
no s
erio
us
inco
nsis
tenc
y
no s
erio
us
indi
rect
ness
no s
erio
us
impr
ecis
ion
none
– –
RR .8
3 (0
.71–
0.97
) –
mo
der
ate
crit
icaL
0% –
preterm birth (assessed with: events)
9 rand
omiz
ed
tria
ls
serio
us3
no s
erio
us
inco
nsis
tenc
y
no s
erio
us
indi
rect
ness
no s
erio
us
impr
ecis
ion
none
– –
RR .8
5 (0
.72–
0.99
)
–
mo
der
ate
impo
rtan
t
0% –
mean birth weight (assessed with: grams)
14 rand
omiz
ed tr
ials
serio
us3
no s
erio
us in
cons
iste
ncy
no s
erio
us in
dire
ctne
ss
no s
erio
us im
prec
isio
n
none
– –
incr
ease
in m
ean
birt
h vw
eigh
t in
gram
s 27
.27
(7.4
9–47
.06)
–
mo
der
ate
impo
rtan
t
0% –
1 allocation concealment was described in only 10 of 63 studies and in 7 studies there was clearly no concealment. Withdrawals (attrition bias) were common. Few trials had any blinding – difficult to do, given the nature of the treatment. In 41 studies blinding was assessed as inadequate2 high unexplained heterogeneity (I squared 68.4%)3 blinding not done, allocation concealment unclear
ANNEXES 93

Recommendation 3 GRADE TABLEAuthor(s): margaret harris
Date: 13 September 2012
Question: Should Nicotine replacement therapy be used in pregnant women?
Settings: all
Bibliography: Coleman et al, 2012
Quality assessment No of patients
Effect
Qua
lity
impo
rtan
ce
No
of s
tudi
es
des
ign
Risk
of b
ias
inco
nsis
tenc
y
indi
rect
ness
impr
ecis
ion
oth
er c
onsi
dera
tions
nic
otin
e re
plac
emen
t th
erap
y
cont
rol
Rela
tive
(95%
CI)
abso
lute
smoking cessation (assessed with: biochemical validation/self-report)
6 rand
omiz
ed
tria
ls
no s
erio
us ri
sk
of b
ias
no s
erio
us
inco
nsis
tenc
y
no s
erio
us
indi
rect
ness
serio
us1
none
0/841 (0%)
0/904 (0%)
RR 1.
33
(0.9
3–1.9
1) –
mo
der
ate
crit
icaL
0% –
miscarriage/spontaneous abortion (assessed with: number of events)
3 rand
omiz
ed
tria
ls
no s
erio
us ri
sk
of b
ias
no s
erio
us
inco
nsis
tenc
y
no s
erio
us
indi
rect
ness
serio
us1
none
– –
RR 1.
24
(0.3
7–4.
17)
–
mo
der
ate
impo
rtan
t
0% –
stillbirths (assessed with: number of events)
3 rand
omiz
ed
tria
ls
no s
erio
us ri
sk
of b
ias
no s
erio
us
inco
nsis
tenc
y
no s
erio
us
indi
rect
ness
serio
us1
none
– –
RR 1.
98
(0.5
5–7.
07)
–
mo
der
ate
impo
rtan
t
0% –
Preterm birth (assessed with: number of events)
4 rand
omiz
ed
tria
ls
no s
erio
us ri
sk
of b
ias
no s
erio
us
inco
nsis
tenc
y
no s
erio
us
indi
rect
ness
serio
us1
none
– –
RR 0
.85
(0.5
7–1.2
6) –
mo
der
ate
impo
rtan
t
0% –
94 ANNEXES
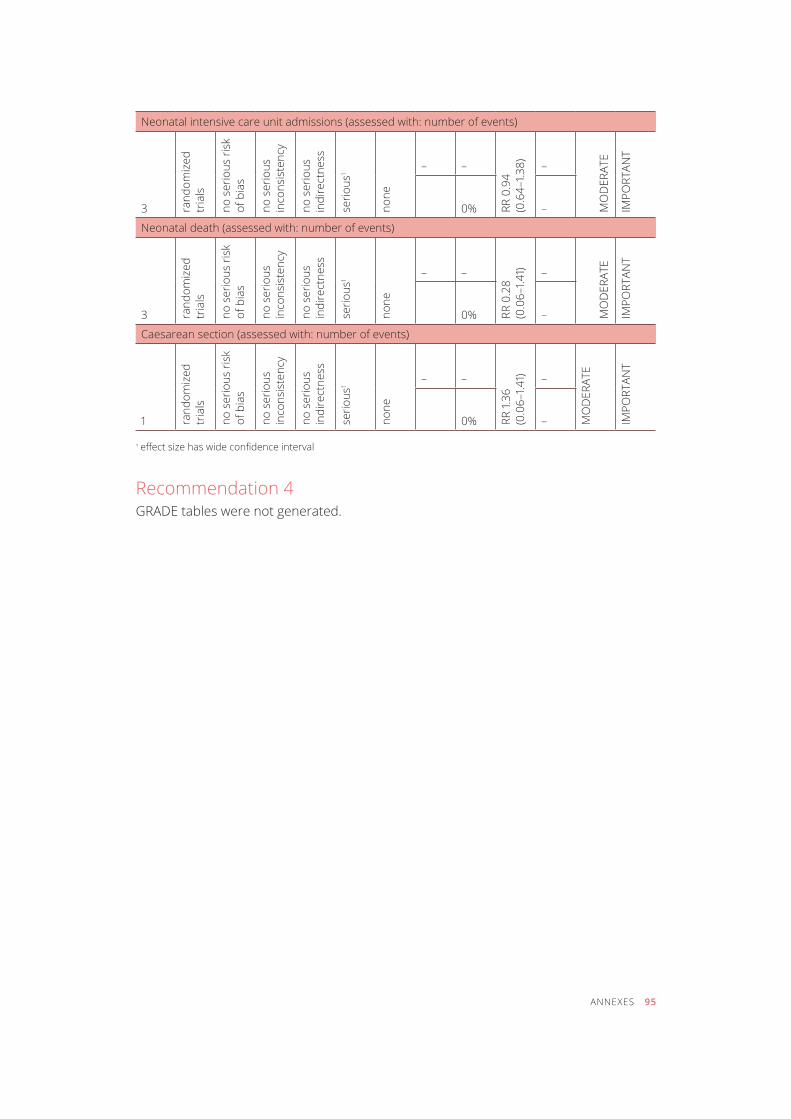
Neonatal intensive care unit admissions (assessed with: number of events)
3 rand
omiz
ed
tria
ls
no s
erio
us ri
sk
of b
ias
no s
erio
us
inco
nsis
tenc
y
no s
erio
us
indi
rect
ness
serio
us1
none
– –
RR 0
.94
(0.6
4–1.3
8) –
mo
der
ate
impo
rtan
t
0% –
Neonatal death (assessed with: number of events)
3 rand
omiz
ed
tria
ls
no s
erio
us ri
sk
of b
ias
no s
erio
us
inco
nsis
tenc
y
no s
erio
us
indi
rect
ness
serio
us1
none
– –
RR 0
.28
(0.0
6–1.4
1) –
mo
der
ate
impo
rtan
t
0% –
Caesarean section (assessed with: number of events)
1 rand
omiz
ed
tria
ls
no s
erio
us ri
sk
of b
ias
no s
erio
us
inco
nsis
tenc
y
no s
erio
us
indi
rect
ness
serio
us1
none
– –
RR 1.
36
(0.0
6–1.4
1) –
mo
der
ate
impo
rtan
t
0% –
1 effect size has wide confidence interval
Recommendation 4GRADE tables were not generated.
ANNEXES 95
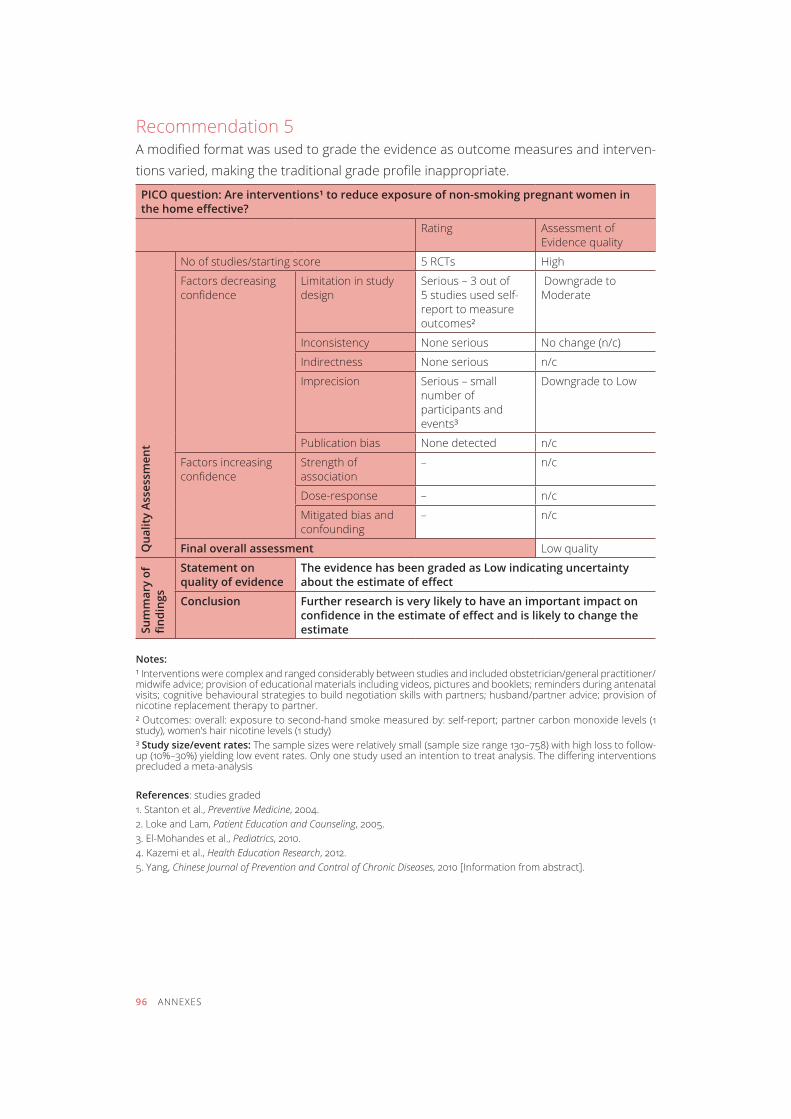
recommendation 5A modified format was used to grade the evidence as outcome measures and interven-tions varied, making the traditional grade profile inappropriate.
PICO question: Are interventions¹ to reduce exposure of non-smoking pregnant women in the home effective?
rating Assessment of Evidence quality
Qua
lity
Asse
ssm
ent
No of studies/starting score 5 rcts high
factors decreasing confidence
Limitation in study design
Serious – 3 out of 5 studies used self-report to measure outcomes²
Downgrade to moderate
inconsistency none serious No change (n/c)
indirectness none serious n/c
imprecision Serious – small number of participants and events³
Downgrade to Low
publication bias none detected n/c
factors increasing confidence
Strength of association
– n/c
dose-response – n/c
mitigated bias and confounding
– n/c
Final overall assessment Low quality
Sum
mar
y of
fin
ding
s
Statement on quality of evidence
The evidence has been graded as Low indicating uncertainty about the estimate of effect
Conclusion Further research is very likely to have an important impact on confidence in the estimate of effect and is likely to change the estimate
Notes:¹ Interventions were complex and ranged considerably between studies and included obstetrician/general practitioner/midwife advice; provision of educational materials including videos, pictures and booklets; reminders during antenatal visits; cognitive behavioural strategies to build negotiation skills with partners; husband/partner advice; provision of nicotine replacement therapy to partner.² Outcomes: overall: exposure to second-hand smoke measured by: self-report; partner carbon monoxide levels (1 study), women’s hair nicotine levels (1 study)³ Study size/event rates: The sample sizes were relatively small (sample size range 130–758) with high loss to follow-up (10%–30%) yielding low event rates. Only one study used an intention to treat analysis. The differing interventions precluded a meta-analysis
References: studies graded1. Stanton et al., Preventive Medicine, 2004.2. Loke and Lam, Patient Education and Counseling, 2005.3. El-Mohandes et al., Pediatrics, 2010.4. kazemi et al., Health Education Research, 2012.5. Yang, Chinese Journal of Prevention and Control of Chronic Diseases, 2010 [Information from abstract].
96 ANNEXES
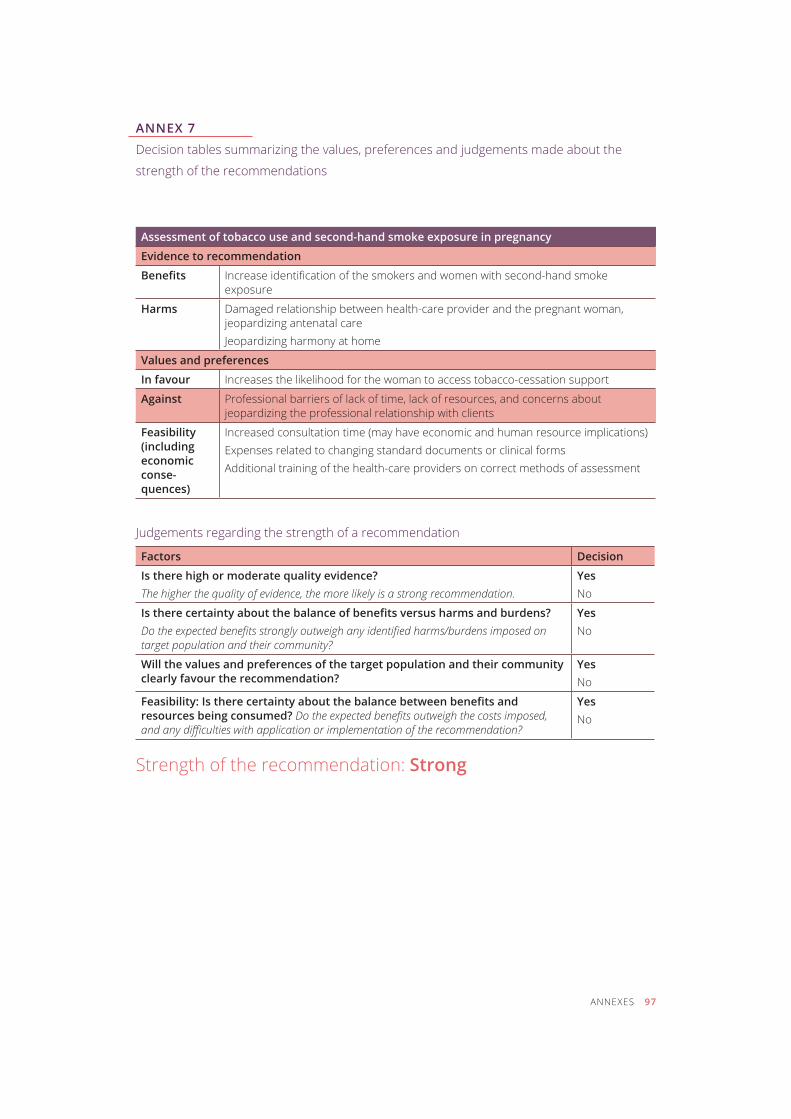
ANNEX 7
Decision tables summarizing the values, preferences and judgements made about the
strength of the recommendations
Assessment of tobacco use and second-hand smoke exposure in pregnancy
Evidence to recommendation
benefits Increase identification of the smokers and women with second-hand smoke exposure
Harms Damaged relationship between health-care provider and the pregnant woman, jeopardizing antenatal careJeopardizing harmony at home
Values and preferences
In favour Increases the likelihood for the woman to access tobacco-cessation support
Against Professional barriers of lack of time, lack of resources, and concerns about jeopardizing the professional relationship with clients
Feasibility (including economic conse- quences)
Increased consultation time (may have economic and human resource implications)Expenses related to changing standard documents or clinical forms Additional training of the health-care providers on correct methods of assessment
Judgements regarding the strength of a recommendation
Factors Decision
Is there high or moderate quality evidence?The higher the quality of evidence, the more likely is a strong recommendation.
Yes no
Is there certainty about the balance of benefits versus harms and burdens?Do the expected benefits strongly outweigh any identified harms/burdens imposed on target population and their community?
Yesno
Will the values and preferences of the target population and their community clearly favour the recommendation?
Yesno
Feasibility: Is there certainty about the balance between benefits and resources being consumed? Do the expected benefits outweigh the costs imposed, and any difficulties with application or implementation of the recommendation?
Yesno
Strength of the recommendation: Strong
ANNEXES 97
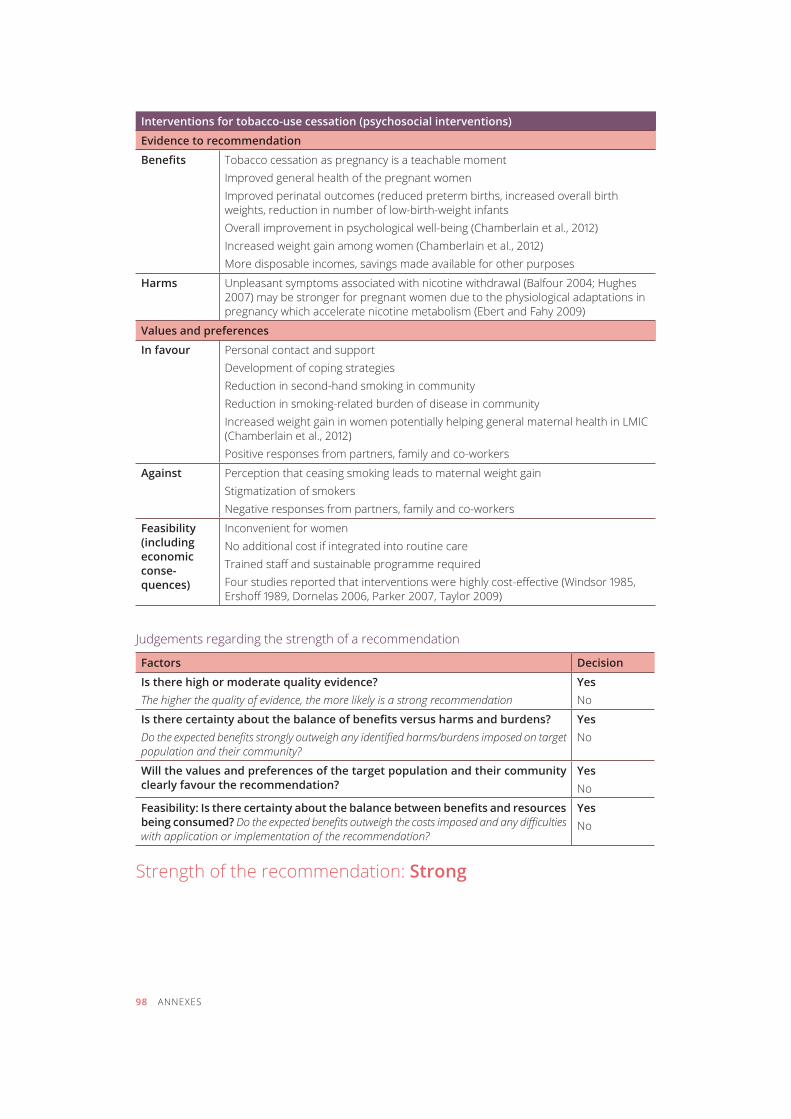
Interventions for tobacco-use cessation (psychosocial interventions)
Evidence to recommendation
benefits tobacco cessation as pregnancy is a teachable momentImproved general health of the pregnant womenImproved perinatal outcomes (reduced preterm births, increased overall birth weights, reduction in number of low-birth-weight infants Overall improvement in psychological well-being (Chamberlain et al., 2012)Increased weight gain among women (Chamberlain et al., 2012)More disposable incomes, savings made available for other purposes
Harms Unpleasant symptoms associated with nicotine withdrawal (Balfour 2004; Hughes 2007) may be stronger for pregnant women due to the physiological adaptations in pregnancy which accelerate nicotine metabolism (Ebert and Fahy 2009)
Values and preferences
In favour personal contact and supportDevelopment of coping strategiesreduction in second-hand smoking in communityReduction in smoking-related burden of disease in communityIncreased weight gain in women potentially helping general maternal health in LMIC (Chamberlain et al., 2012)Positive responses from partners, family and co-workers
Against Perception that ceasing smoking leads to maternal weight gainStigmatization of smokers Negative responses from partners, family and co-workers
Feasibility (including economic conse- quences)
Inconvenient for women No additional cost if integrated into routine careTrained staff and sustainable programme requiredFour studies reported that interventions were highly cost-effective (Windsor 1985, Ershoff 1989, Dornelas 2006, Parker 2007, Taylor 2009)
Judgements regarding the strength of a recommendation
Factors Decision
Is there high or moderate quality evidence?The higher the quality of evidence, the more likely is a strong recommendation
Yesno
Is there certainty about the balance of benefits versus harms and burdens?Do the expected benefits strongly outweigh any identified harms/burdens imposed on target population and their community?
Yesno
Will the values and preferences of the target population and their community clearly favour the recommendation?
Yesno
Feasibility: Is there certainty about the balance between benefits and resources being consumed? Do the expected benefits outweigh the costs imposed and any difficulties with application or implementation of the recommendation?
Yesno
Strength of the recommendation: Strong
98 ANNEXES
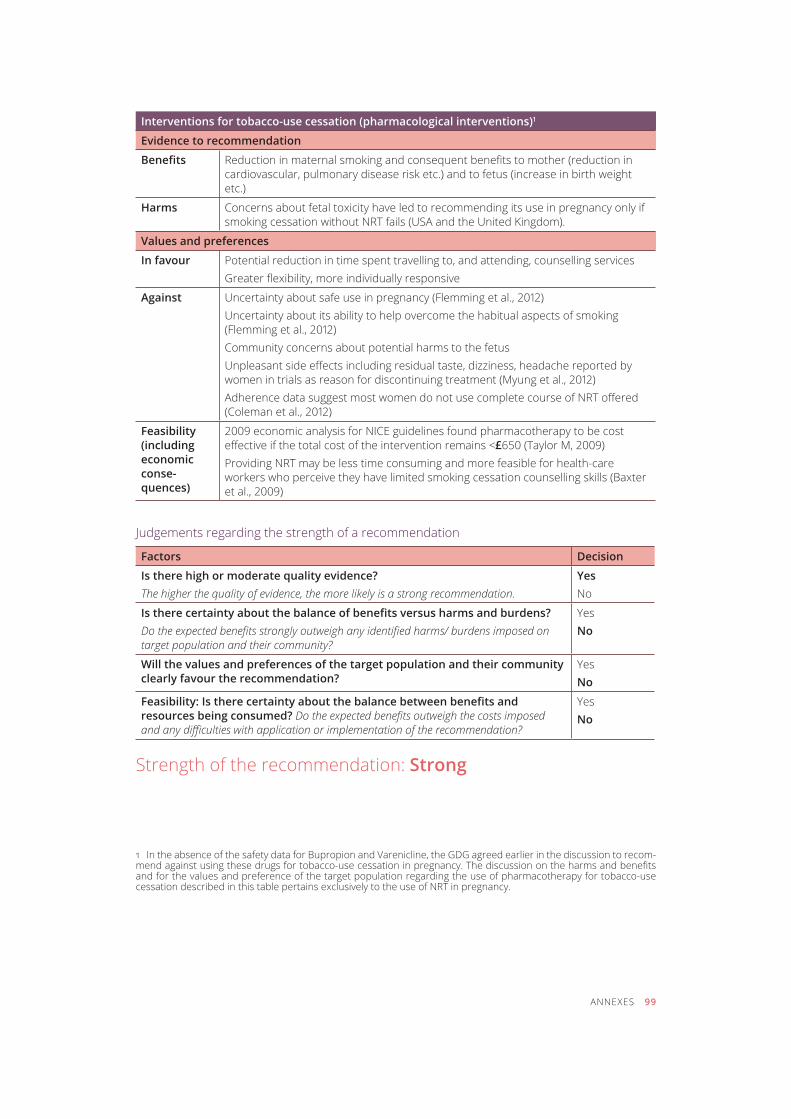
Interventions for tobacco-use cessation (pharmacological interventions)1
Evidence to recommendation
benefits Reduction in maternal smoking and consequent benefits to mother (reduction in cardiovascular, pulmonary disease risk etc.) and to fetus (increase in birth weight etc.)
Harms Concerns about fetal toxicity have led to recommending its use in pregnancy only if smoking cessation without NRT fails (USA and the United kingdom).
Values and preferences
In favour Potential reduction in time spent travelling to, and attending, counselling servicesGreater flexibility, more individually responsive
Against Uncertainty about safe use in pregnancy (Flemming et al., 2012)Uncertainty about its ability to help overcome the habitual aspects of smoking (Flemming et al., 2012)Community concerns about potential harms to the fetusUnpleasant side effects including residual taste, dizziness, headache reported by women in trials as reason for discontinuing treatment (Myung et al., 2012)Adherence data suggest most women do not use complete course of NRT offered (Coleman et al., 2012)
Feasibility (including economic conse- quences)
2009 economic analysis for NICE guidelines found pharmacotherapy to be cost effective if the total cost of the intervention remains <£650 (Taylor M, 2009)Providing NRT may be less time consuming and more feasible for health-care workers who perceive they have limited smoking cessation counselling skills (Baxter et al., 2009)
Judgements regarding the strength of a recommendation
Factors Decision
Is there high or moderate quality evidence?The higher the quality of evidence, the more likely is a strong recommendation.
Yesno
Is there certainty about the balance of benefits versus harms and burdens?Do the expected benefits strongly outweigh any identified harms/ burdens imposed on target population and their community?
Yes No
Will the values and preferences of the target population and their community clearly favour the recommendation?
Yes No
Feasibility: Is there certainty about the balance between benefits and resources being consumed? Do the expected benefits outweigh the costs imposed and any difficulties with application or implementation of the recommendation?
YesNo
Strength of the recommendation: Strong
1 In the absence of the safety data for Bupropion and Varenicline, the GDG agreed earlier in the discussion to recom-mend against using these drugs for tobacco-use cessation in pregnancy. The discussion on the harms and benefits and for the values and preference of the target population regarding the use of pharmacotherapy for tobacco-use cessation described in this table pertains exclusively to the use of NRT in pregnancy.
ANNEXES 99
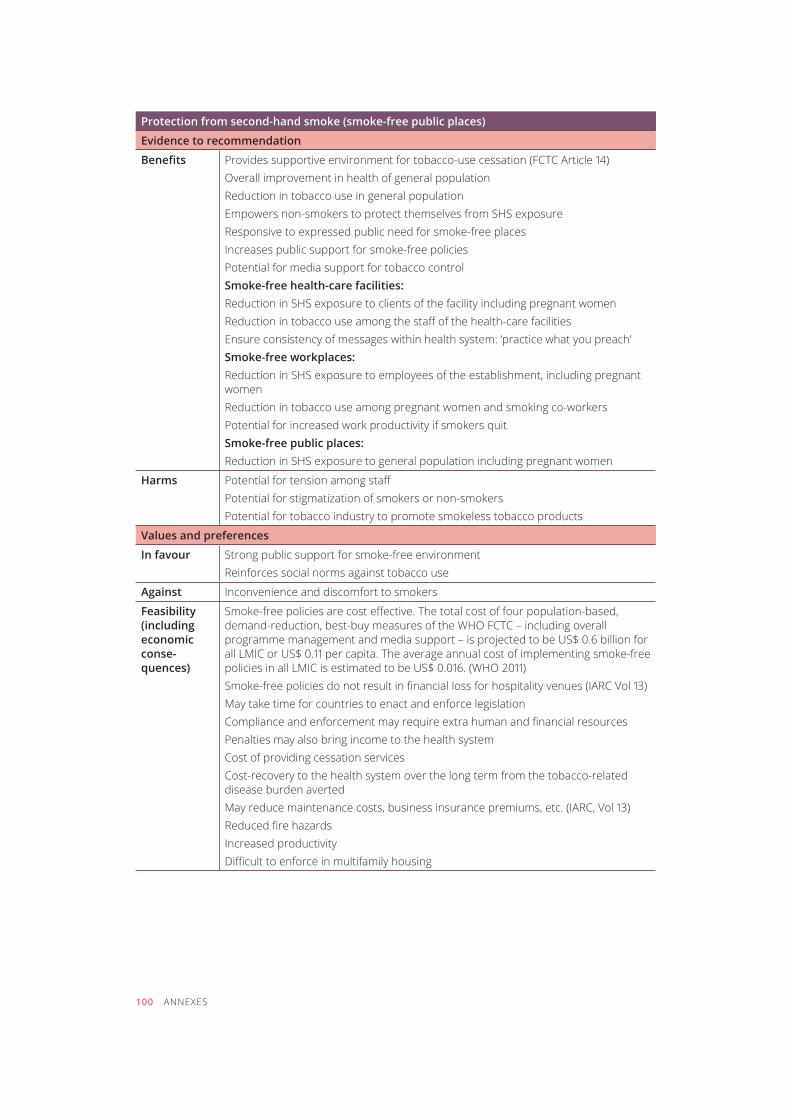
Protection from second-hand smoke (smoke-free public places)
Evidence to recommendation
benefits Provides supportive environment for tobacco-use cessation (FCTC Article 14)Overall improvement in health of general population reduction in tobacco use in general populationEmpowers non-smokers to protect themselves from SHS exposureResponsive to expressed public need for smoke-free placesIncreases public support for smoke-free policies Potential for media support for tobacco controlSmoke-free health-care facilities:Reduction in SHS exposure to clients of the facility including pregnant women Reduction in tobacco use among the staff of the health-care facilitiesEnsure consistency of messages within health system: ‘practice what you preach’Smoke-free workplaces:Reduction in SHS exposure to employees of the establishment, including pregnant womenReduction in tobacco use among pregnant women and smoking co-workersPotential for increased work productivity if smokers quitSmoke-free public places:Reduction in SHS exposure to general population including pregnant women
Harms Potential for tension among staffPotential for stigmatization of smokers or non-smokersPotential for tobacco industry to promote smokeless tobacco products
Values and preferences
In favour Strong public support for smoke-free environmentReinforces social norms against tobacco use
Against Inconvenience and discomfort to smokers
Feasibility (including economic conse- quences)
Smoke-free policies are cost effective. The total cost of four population-based, demand-reduction, best-buy measures of the WHO FCTC – including overall programme management and media support – is projected to be US$ 0.6 billion for all LMIC or US$ 0.11 per capita. The average annual cost of implementing smoke-free policies in all LMIC is estimated to be US$ 0.016. (WHO 2011) Smoke-free policies do not result in financial loss for hospitality venues (IARC Vol 13) May take time for countries to enact and enforce legislationCompliance and enforcement may require extra human and financial resourcespenalties may also bring income to the health systemCost of providing cessation servicesCost-recovery to the health system over the long term from the tobacco-related disease burden averted May reduce maintenance costs, business insurance premiums, etc. (IARC, Vol 13) Reduced fire hazardsIncreased productivityDifficult to enforce in multifamily housing
100 ANNEXES
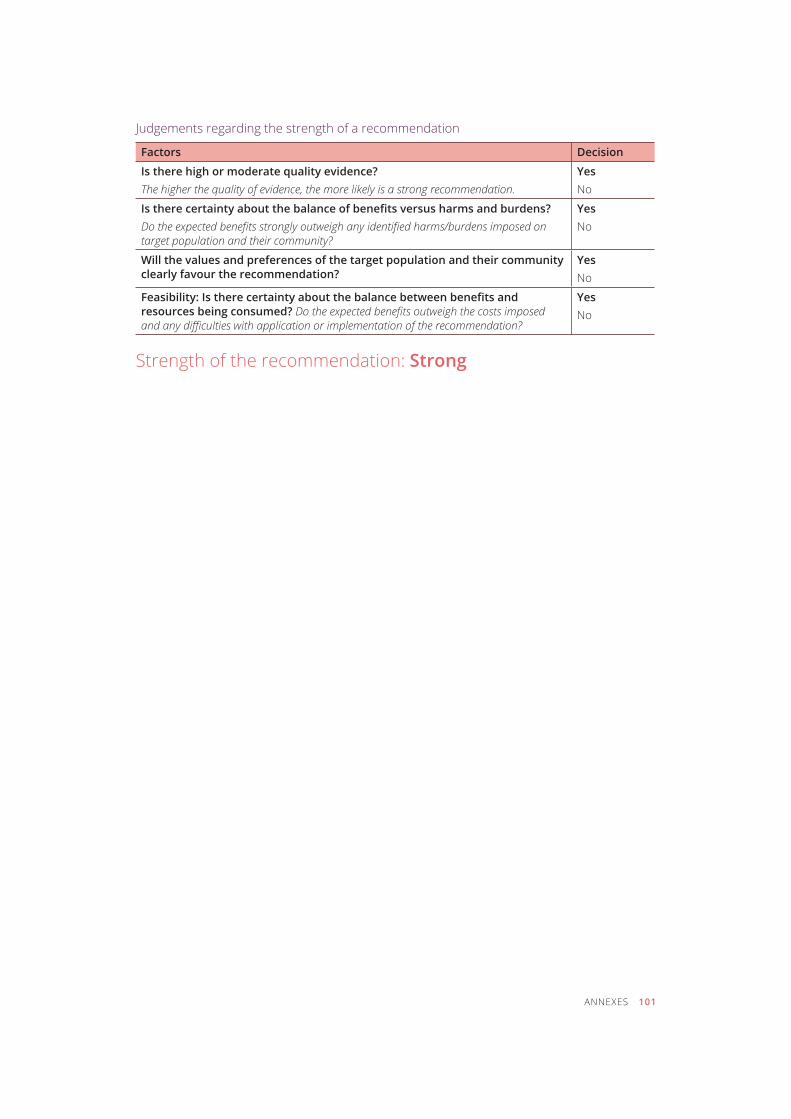
Judgements regarding the strength of a recommendation
Factors Decision
Is there high or moderate quality evidence?The higher the quality of evidence, the more likely is a strong recommendation.
Yesno
Is there certainty about the balance of benefits versus harms and burdens?Do the expected benefits strongly outweigh any identified harms/burdens imposed on target population and their community?
Yesno
Will the values and preferences of the target population and their community clearly favour the recommendation?
Yesno
Feasibility: Is there certainty about the balance between benefits and resources being consumed? Do the expected benefits outweigh the costs imposed and any difficulties with application or implementation of the recommendation?
Yesno
Strength of the recommendation: Strong
ANNEXES 101
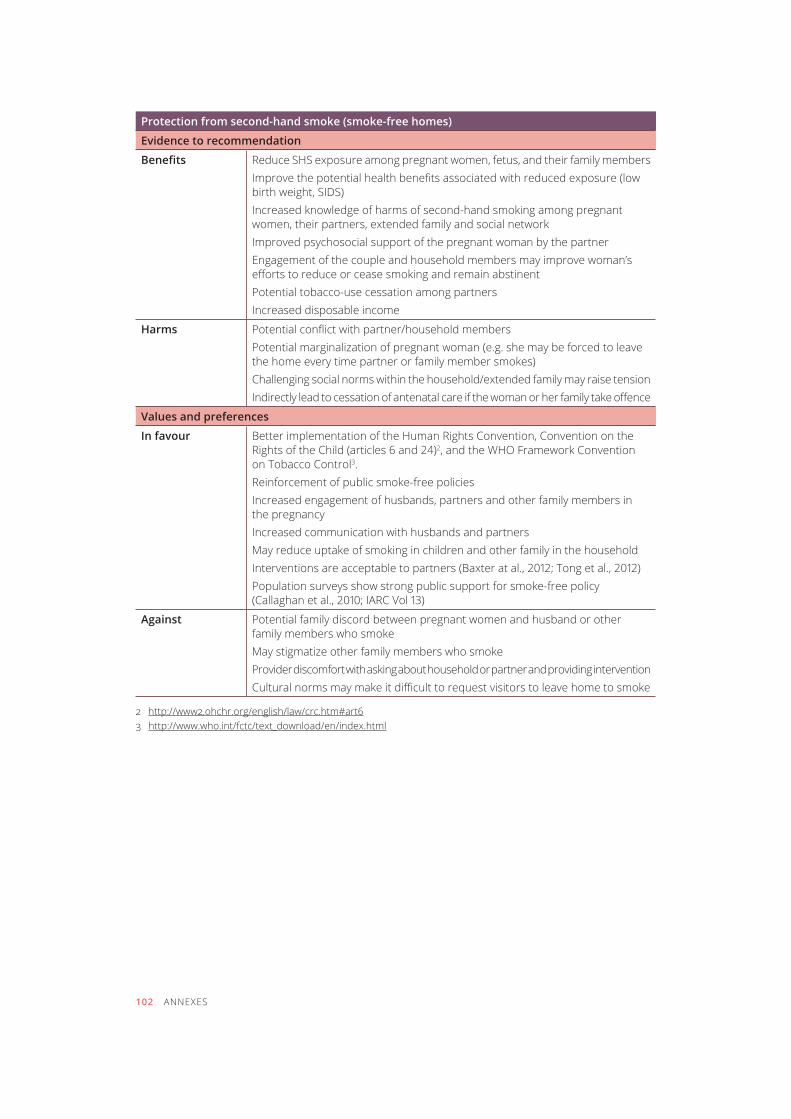
102 ANNEXES
Protection from second-hand smoke (smoke-free homes)
Evidence to recommendation
benefits Reduce SHS exposure among pregnant women, fetus, and their family members Improve the potential health benefits associated with reduced exposure (low birth weight, SIDS)Increased knowledge of harms of second-hand smoking among pregnant women, their partners, extended family and social network Improved psychosocial support of the pregnant woman by the partnerEngagement of the couple and household members may improve woman’s efforts to reduce or cease smoking and remain abstinentpotential tobacco-use cessation among partnersincreased disposable income
Harms Potential conflict with partner/household members Potential marginalization of pregnant woman (e.g. she may be forced to leave the home every time partner or family member smokes)Challenging social norms within the household/extended family may raise tensionIndirectly lead to cessation of antenatal care if the woman or her family take offence
Values and preferences
In favour Better implementation of the Human Rights Convention, Convention on the Rights of the Child (articles 6 and 24)2, and the WHO Framework Convention on tobacco control3. Reinforcement of public smoke-free policies Increased engagement of husbands, partners and other family members in the pregnancyIncreased communication with husbands and partners May reduce uptake of smoking in children and other family in the household Interventions are acceptable to partners (Baxter at al., 2012; Tong et al., 2012)Population surveys show strong public support for smoke-free policy (Callaghan et al., 2010; IARC Vol 13)
Against Potential family discord between pregnant women and husband or other family members who smokeMay stigmatize other family members who smokeProvider discomfort with asking about household or partner and providing interventionCultural norms may make it difficult to request visitors to leave home to smoke
2 http://www2.ohchr.org/english/law/crc.htm#art6 3 http://www.who.int/fctc/text_download/en/index.html
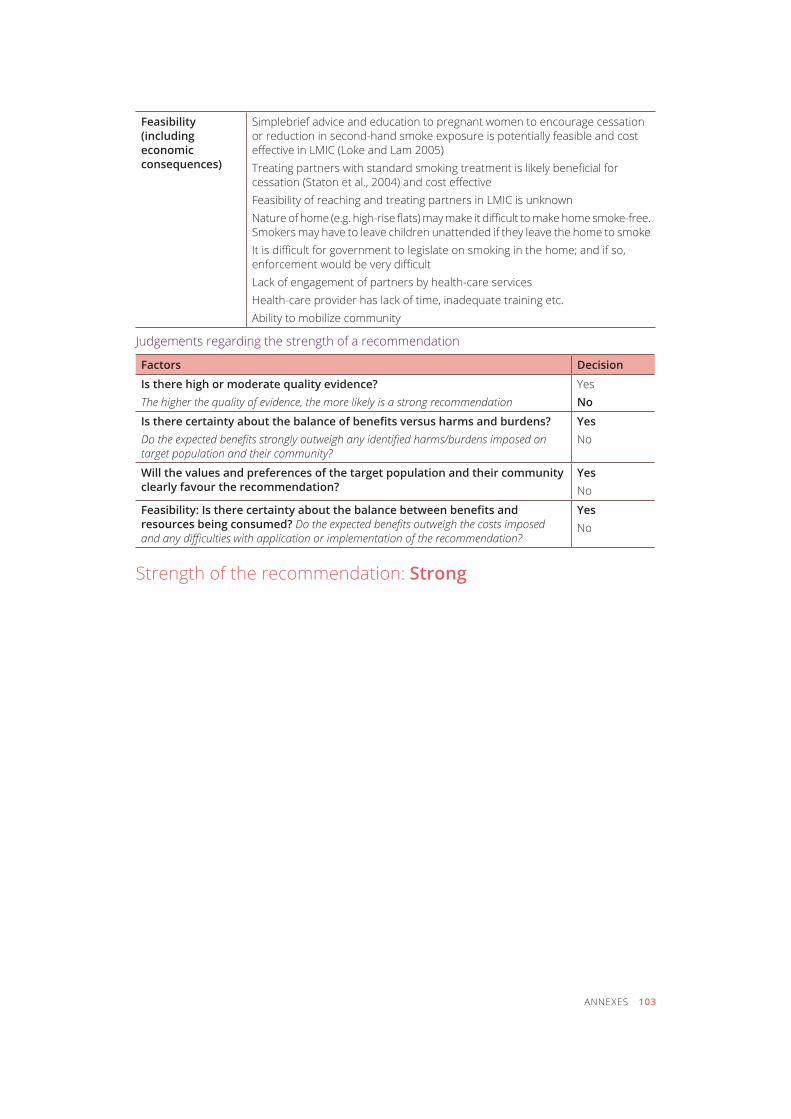
ANNEXES 103
Feasibility (including economic consequences)
Simplebrief advice and education to pregnant women to encourage cessation or reduction in second-hand smoke exposure is potentially feasible and cost effective in LMIC (Loke and Lam 2005)Treating partners with standard smoking treatment is likely beneficial for cessation (Staton et al., 2004) and cost effectiveFeasibility of reaching and treating partners in LMIC is unknownNature of home (e.g. high-rise flats) may make it difficult to make home smoke-free. Smokers may have to leave children unattended if they leave the home to smokeIt is difficult for government to legislate on smoking in the home; and if so, enforcement would be very difficultLack of engagement of partners by health-care servicesHealth-care provider has lack of time, inadequate training etc. Ability to mobilize community
Judgements regarding the strength of a recommendation
Factors Decision
Is there high or moderate quality evidence?The higher the quality of evidence, the more likely is a strong recommendation
YesNo
Is there certainty about the balance of benefits versus harms and burdens?Do the expected benefits strongly outweigh any identified harms/burdens imposed on target population and their community?
Yesno
Will the values and preferences of the target population and their community clearly favour the recommendation?
Yesno
Feasibility: Is there certainty about the balance between benefits and resources being consumed? Do the expected benefits outweigh the costs imposed and any difficulties with application or implementation of the recommendation?
Yesno
Strength of the recommendation: Strong
For further information please contact:Prevention of Noncommunicable DiseasesTobacco Free Initiative World Health Organization20 Avenue Appia, 1211 Geneva 27, SwitzerlandE-mail: [email protected] site: www.who.int\tfi





























