Embed Size (px)
DESCRIPTION
A Dec. 2007 presentation to the IEEE Medical Technology Policy Committee. The presentation outlines false assumptions, underestimations and knowledge gaps of the business IT community regarding clinical IT such as electronic medical records or EMR, computerized order entry or CPOE, and CDSS or clinical decision support systems. These issues make creation of effective clinical information technology and design that provides a quality user experience for clinicians difficult.
Citation preview

1
To The Moon In A Hot Air Balloon: Why Is Clinical IT Difficult?
Scot M. Silverstein, MDSuss Consulting, Inc.Drexel University, College of Information Science & Technology
Dec. 10, 2007

2
– Introduction to Medical Informatics– EMR vision, knowledge gaps, realities– Case examples– Recommendations– Questions

3
On Medical Informatics
• Medical Informatics is a cross-disciplinary field that studies information-seeking activities and tools, analytic processes, and workflows in biomedical research and clinical care delivery. It focuses upon the innovative use of computers in clinical medicine, molecular biology, neuroscience, and other areas of biomedical research.

4
NIH training programs in Medical Informaticshttp://www.nlm.nih.gov/ep/GrantTrainInstitute.html
1 - University of California Irvine (Irvine, CA), 2 -University of California Los Angeles (Los Angeles, CA), 3- Stanford University (Stanford, CA), 4- University of Colorado Denver/HSC Aurora (Denver, CO), 5- Yale University (New Haven, CT), 6- Regenstrief/Indiana University (Indianapolis, IN), 7- Harvard University (Medical School) (Boston, MA), 8- Johns Hopkins University (Baltimore, MD), 9- University of Minnesota Twin Cities (Minneapolis, MN), 10 - University of Missouri-Columbia (Columbia, MO), 11- Columbia University Health Sciences (New York, NY), 12- Oregon Health & Science University (Portland, OR), 13- University of Pittsburgh at Pittsburgh (Pittsburgh, PA), 14- Medical University of South Carolina (Charleston, SC), 15- Vanderbilt University (Nashville, TN), 16 - Rice University (Houston, TX), 17- University of Utah (Salt Lake City, UT), 18- University of Virginia Charlottesville (Charlottesville, VA), 19 - University of Washington (Seattle, WA), 20 - University of Wisconsin Madison (Madison, WI). Training is provided by other universities via internal funds as well.

5
The Informatics Subspecialties

6
Why is Medical Informatics important?• Healthcare IT and its environment are core competence• Recognition that organizations are simultaneously social (people, values,
norms, cultures) and technical (tools, equipment, technology). These elements are deeply interdependent and interrelated. Good design and implementation is not just a technology issue but also one of jointly optimizing the combined sociotechnical systems.
• Medical Informatics training recognizes these issues and trains cross-disciplinary specialists accordingly. Curriculum example:
– Fundamental of computer scienceMedical language and terminology systemsModeling of medical observations and dataMedical coding systemsMedical knowledge structuresInformation organization and flows in medical practiceQuantitative models for medical decision makingClinical decision supportMedical image processingUser interfaces and ergonomics in healthcareHealth information systems architectureSecurity and confidentialityEthical and legal issues in electronic medical recordsOrganizational and sociological issues in clinical IT projectsMetrics and methods for evaluating healthcare information systemsCost and investment issues in healthcare IT

7
The Vision …• "We will make wider use of electronic records and
other health information technology to help control costs and reduce dangerous medical errors."-- President Bush, January 31, 2006
• "..to link all health records through an interoperable
system that protects privacy as it connects patients, providers and payers, resulting in fewer medical mistakes, less hassle, lower costs and better health."-- HHS Secretary Mike Leavitt

8
Revolutionizing Healthcare• In April 2004, President George W. Bush revealed his vision for the future of healthcare in the
United States. The President's plan involves a health care system that puts the needs of the patient first, is more efficient, and is cost-effective. The President's plan is based on the following tenets:
– Medical information will follow consumers so that they are at the center of their own care – Consumers will be able to choose physicians and hospitals based on clinical performance results
made available to them – Clinicians will have a patient's complete medical history, computerized ordering systems, and
electronic reminders – Quality initiatives will measure performance and drive quality-based competition in the industry – Public health and bioterrorism surveillance will be seamlessly integrated into care – Clinical research will be accelerated and post-marketing surveillance will be expanded.
• Together, these tenets will revolutionize healthcare, making it more consumer-centric, and will improve both the quality and the efficiency of healthcare in the United States.
Source: http://www.hhs.gov/healthit/vision.html

9
Revolutionizing Healthcare?
• MS-HUG meeting, late 1990’s, CEO’s of Cerner, HBOC and other vendors calling for room to “revolutionize healthcare”– How many people here think they will revolutionize
healthcare?
– How many people here have true clinical experience, or have read a medical text such as Harrison’s or The Merck Manual?

10
Achilles’ Heel: False assumptions and underestimations
• Balloons go up in the sky.• The moon is up in the sky.• With enough process and resources, we can travel to the moon in a balloon.• What we don’t know can’t hurt us, and it’s bad for business anyway.

11
Implementing EMR not as easy as it seems
• Not a technology problem any longer. • Medical informaticists study the issues that impede EMR
adoption in clinical settings.• What if clinical computing and business computing are
different, distinct subspecialties of computing, much as neurosurgery and psychiatry are highly distinct medical subspecialties?
• What few talk about regarding clinical information technology: social and organizational causes of healthcare IT difficulties– “Sociotechnologic issues in clinical computing: Common examples of
healthcare IT difficulties” at http://www.ischool.drexel.edu/faculty/ssilverstein/medinfo.htm

12
To an information scientist, Google is revealing
• Relevant hits on “Healthcare IT Failure” or similar concepts: almost none
• Hits on “Medical Malpractice” 294,000
• Why?

13
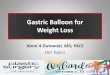
Access Patterns to a Website on Healthcare IT Failure Scot M. Silverstein MD, Yunan Chen, Christine Wania
College of Information Science & Technology, Drexel University
Organizational and human factors (sociotechnical) issues associated with healthcare IT have led to project difficulties and failures. Detailed case accounts might improve knowledge sharing between healthcare organizations on lessons learned and best implementation practices. Based on an online search for web-based resources, there appears to be few relevant sites containing either high-level or case-level information regarding healthcare IT difficulty and failure. Case-level accounts describing issues at a fine level of granularity, such as detailed accounts of interactions among clinicians, IT personnel and healthcare executives, are potentially useful learning resources. Knowledge sharing via the Web on best practices for management of sociotechnical impediments to healthcare IT is thus suboptimal.
We studied access patterns to our website on healthcare IT difficulties. The distribution of countries, website visitor types and query types are shown in the following charts:
To illustrate the level of interest and knowledge sharing about Healthcare IT difficulties, we explored two research questions:
What case-level information about healthcare IT project difficulty and failure is available via the Web?
Who is seeking this information?
Background
Case Study Results
Conclusion
Research Questions
Visitor Input Types
Visitor types
Our website “Sociotechnologic Issues in Clinical Computing: Common Examples of Healthcare IT Failure” is at URL:
http://www.ischool.drexel.edu/faculty/ssilverstein/medinfo.htm
It was created by our first author via an informal collaboration of AMIA clinical information systems working group members (CIS-WG) during 1998-2001.
Methods
We used our website, entitled “Sociotechnologic Issues in Clinical Computing: Common Examples of Healthcare IT Failure”, online since 1999, as a representative information resource.
We first conducted a detailed Web search on various search phrases representing the concept “healthcare IT failure” using three major search engines (Google, Yahoo, and MSN). The results showed that our website was nearly unique. We then tracked views of our website from Sep 27th, 2005 to June 30th, 2006 with a free public tracking service, eXTReMe Tracking (http://extremetracking.com).
We examined the access logs to determine viewer IP and referrer (primarily search engine query, or link from another site) to identify viewer demographics including country and organization type, where available. No personally-identifiable information was sought or obtained.
Visitor Search Engine Referrer Input
It appears there is an ongoing interest in information about healthcare IT difficulty among searchers of varied demographics, as evidenced by searches on these issues and resultant “hits” on our website, one of the few websites that specifically addresses these issues. At present such material is uncommon. We believe Medical Informatics specialists can contribute significantly to filling this information gap, and that doing so would be very helpful to the healthcare IT community.
Note: The terms in this diagram represent our categorization of the concepts used by Web searchers to find our website. For example: “healthcare IT” might have been expressed as “medical computing” or “clinical information technology.”
Visitor Countries distribution
2252
206166 132
0
500
1000
1500
2000
2500
Search Engine Healthcare IT Site Other Non Healthcare ITSite
774
423389
227193
116
0
100
200
300
400
500
600
700
800
Healthcare ORIT OR Failure
HealthcareAND IT
IT Failure Healthcare ITFailure
Unrelated ProjectManagement
2842
564
332239
149 93 9711
0
500
1000
1500
2000
2500
3000
ISP University /EducationalInstitution
OtherOrganization
HealthcareOrganization
Unknown GovernmentOrganization
HealthcareRelatedIndustry
OtherIndividual

14
Why is good clinical IT difficult?
• Lindberg: “Computer Failures and Successes”, Southern Medical Bulletin 1969;57:18-21
– Computer experts per se have virtually no idea of the real problems of medical or even hospital practice, and furthermore have consistently underestimated the complexity of the problems…in no cases can [building appropriate clinical information systems] be done, simply because they have not been defined with the physician as the continuing major contributor and user of the information.
• Nemeth & Cook: “Hiding in Plain Sight”, Journal of Biomedical Informatics 38 [2005], 262–263
– Just beneath the apparently smooth-running operations [of healthcare] is a complex, poorly bounded, conflicted, highly variable, uncertain, and high-tempo work domain. The technical work that clinicians perform resolves these complex and conflicting elements into a productive work domain. Occasional visitors to this setting see the smooth surface that clinicians have created and remain unaware of the conflicts that lie beneath it. The technical work that clinicians perform is hiding in plain sight. Those who know how to do research in this domain can see through the smooth surface and understand its complex and challenging reality. Occasional visitors cannot fathom this demanding work, much less create IT systems to support it.

15
The Gaps …• IT Industry View
– Computers are the solution.– If it’s information, we do it, and with a few
domain experts helping us, we can automate anything.
– Clinical computing is a subspecies of MIS.– We take specs, build the system employing SLC
and other methodologies, deliver product, do a few tweaks, and we’re done.
– End users are to be managed, and occasionally listened to.
– The world operates like an assembly line. – With enough process, “skill sets” and resources,
we can go to the moon in a hot air balloon.– We don’t need space scientists interfering in our
endeavors. What do they know about IT and about project management?
– Our way is the only way. Agile methodologies? Iterative and incremental development? Doctors leading computing projects? No way.
• Medical Informatics View– Computers are inanimate objects. A computer
with appropriate software developed incorporating appropriate domain expertise is a tool. A tool in the right hands and right contexts is a solution – maybe – assuming no unpredictables intervene.
– Clinical computing is a subspecies of “scientific” computing.
– Throwing IT at a health care system to remedy its problems will not be effective unless the organizational reasons for those failures also are addressed.
– These reasons are hidden in the "messy details" of clinical work: complexity; uncertainty; conflicting goals; gaps in supplies, procedures, and coordination; brittleness of tools and organizational routines.
– These cannot be “modeled” and automated in the traditional MIS manner.
– “Changing the culture” of healthcare involves changing the culture of clinicians AND changing the culture of healthcare IT professionals.

16
The Gaps …• IT Industry View • Medical Informatics View

17
From Kling, Rosenbaum & Sawyer: Understanding and Communicating Social Informatics, Information Today (1st Edition, 2005)

18
Hubris? – Observed by me …• Medical data is the same as anyone else’s data.• Don’t worry about it, you can’t understand it, we’ll make it better. • I don't think a degree gets you anything. There's nothing like the school of
Hard Knocks [for healthcare CIO’s].• I don’t think clinical experience yields healthcare IT workers who have
broad enough perspective. Physicians in particular make poor choices for CIOs. They don't think of the business issues at hand because they're consumed with patient care issues.
• Only satellites in Earth orbit need protection from x-rays.• Doctors don’t do things with computers.• Medical Informatics is too academic.• We only support Compaq computers in our hospital.• We have a “turnkey system only” rule. No customizations.• Doctors just don’t want to do things the way the application requires.

19
The Realities
• "Many information systems simply don't reflect the health care professional's hectic work environment with its all too frequent interruptions from phone calls, pages, colleagues and patients. Instead these are designed for people who work in calm and solitary environments. This design disconnect is the source of both types of silent errors …Some patient care information systems require data entry that is so elaborate that time spent recording patient data is significantly greater than it was with its paper predecessors," the authors wrote. "What is worse, on several occasions during our studies, overly structured data entry led to a loss of cognitive focus by the clinician.“ – OHSU research on CPOE
Source: http://www.eurekalert.org/pub_releases/2003-11/ohs-mhd112403.php

20

21

22
• In 2005 University of Pennsylvania sociologist Ross Koppel, PhD and clinical colleagues, at some risk to their professional reputations, published findings that a leading Computerized Practitioner Order Entry (CPOE) system often facilitated medication error risks, with many reported to occur frequently.
• “Role of Computerized Physician Order Entry Systems in Facilitating Medication Errors” (JAMA 2005;293:1197-1203)
– link to abstract: http://jama.ama-assn.org/cgi/content/abstract/293/10/1197

23
• In a 2007 research study involving the University at Buffalo and other institutions, "Design of Patient Tracking Tools May Have Unintended Consequences", researchers found that “Virtual Patient Status Whiteboard” systems to replace traditional, dry-erase patient status boards in hospital Emergency Departments (ED’s), but designed by technologists without adequate domain expertise, often do not work as expected. The computer-based system interferes with staff communications.
• In some cases, providers noted that computer systems hid some of the information; if only three comments could be viewed per screen, they had to click to get to another screen, requiring them to search for information that might demand immediate attention. The study also found that there were fewer visual cues with the computational system. Some providers noted that they used to be able to get a sense of the status of the emergency department just by walking through the room and visually checking the manual whiteboard. “Without that public display, providers have to sit down at the computer and check it, which can add time or reduce awareness,” said a principal investigator.
Reference: http://www.eurekalert.org/pub_releases/2007-11/uab-dop112607.php

24
• Research article in the Archives of Internal Medicine - “Electronic Health Record Use and the Quality of Ambulatory Care in the United States” (Arch Intern Med. 2007;167:1400-1405, link to abstract here):
– The authors examined electronic health records (EHR) use throughout the U.S. and the association of EHR use with 17 basic quality indicators. They concluded that “as implemented, EHR’s were not associated with better quality ambulatory care.”
– On several indicators, physicians using paper did better.

25
Case Example
• Serious clinical computing problems in the worst of places: an ICU
– http://www.ischool.drexel.edu/faculty/ssilverstein/failurecases/?loc=cases&sloc=clinical%20computing%20problems%20in%20ICU

26
Recommendations• Temper the irrational exuberance that now prevails.• Recognize sociotechnical barriers and work with them, not
against them.• Address need for specialized approaches to clinical computing
(vs. business computing). • Improve Medical Informatics professionals’ representation in
health IT management• Incorporate medicine’s rigor into the medical IT leadership
and staff – end “pre-Flexner report healthcare IT”– Familiarity with nuances of healthcare and healthcare IT– Specialized educational experience– Standards and certification for healthcare IT workers

27
Red Sand Dunes area, ~ 50 km w. of Riyadh
Medical Informatics can take us to exotic places!

28
Supplementary slides

29
The iSchools
• University of California, BerkeleySchool of Information Management and Systems
• University of California, IrvineThe Don Bren School of Information and Computer Sciences
• University of California, Los AngelesGraduate School of Education and Information Studies
• Drexel UniversityCollege of Information Science and Technology
• Florida State UniversityCollege of Information
• Georgia Institute of TechnologyCollege of Computing
• University of Illinois Urbana-ChampaignThe Graduate School of Library and Information Science
• Indiana UniversitySchool of Informatics
• Indiana UniversitySchool of Library and Information Science
• University of MarylandCollege of Information Studies
University of MichiganThe School of Information
University of North CarolinaSchool of Information and Library Science
The Pennsylvania State UniversitySchool of Information Sciences and Technology
University of PittsburghSchool of Information Sciences
Rutgers, the State University of New JerseySchool of Communication, Information, and Library Studies
Syracuse UniversitySchool of Information Studies
University of Texas, AustinSchool of Information
University of TorontoFaculty of Information Studies
University of WashingtonInformation School
Focus is on how people seek, use or interact with information using technology, not simply on technologic devices and computer programs.

30
Medical Informatics: What it is not• Medical informatics is a formal field of study and a scientific discipline. Computers in
medicine is not the equivalent of medical informatics.
• Position descriptions with requirements for neither clinical nor medical informatics training or experience, are often seen. From the Philadelphia Inquirer:
– Medical informatics analyst. [Company name] seeks a Medical Informatics Analyst to support resource management and medical affairs in their data analysis needs. Through downloading of MCS database, PC-based analysis of clinical and clinically-relevant financial data will be performed. Qualifications: BA/BS in computer science or related discipline, 3-5 years experience in PC-based data analysis of health care information, knowledge of SAS or similar analysis software, knowledge of mainframe DB2 database architectures, working knowledge of CPT-4 and ICD-9-CM coding."
– From an Internet biomedical employment service, Medzilla.com: [Company name] seeks a Director of Clinical Informatics. Overall coordination of design specifications, implementation and support for all internet/browser based systems. Assurance of continued, reliable and consistent resources and applications to all corporate personnel and external users who may rely upon these systems. Documentation and control of said software systems including package systems and license control if necessary. Provide ongoing maintenance oversight and management support for said systems. Organize and train personnel, both internal and external, who will be using said products. Client contact and development and assist Sales and Marketing as necessary in client presentations. Minimum of a BA. MBA preferred.