Embed Size (px)
Citation preview

To love or to pay: On consumption, health andhealth care
Loretti I. Dobrescu�� University of New South Wales, School of Economics, Australian School of Business,
UNSW Sydney 2052, NSW AustraliaE-mail: [email protected]
Version: April 30, 20101
People face heterogeneous health shocks and medical spending risks. Using a rich dynamicstructural life-cycle model, this paper investigates how these shocks a¤ect the savings behaviorof retired single households. Consumers are allowed to respond to health shocks in two dif-ferent ways: they can directly pay for their health care expenses (self-insure) or they can relyon health insurance contracts. There are two possible insurance options, one through formalcontracts and another through informal health care provided by family. Formal insurance con-tracts may be a¤ected by asymmetric information problems, while informal insurance dependson social ties (cohesion) and on the wealth available for bequeathing. I estimate the modelon SHARE data, using the simulated method of moments for four levels of wealth and threeEuropean country groups: Mediterranean, Central European and Scandinavian. I �nd thatthe risks of living long and facing high medical expenses can provide an explanation for in-creasing precautionary savings (and consequently bequests) after retirement. Most importantand novel, the estimates on family cohesion, by country and wealth level, con�rm two relevantsocial literature �ndings on the strength of family ties: it generally rises with age and declineswith wealth and it is higher in Mediterranean countries as opposed to Central European orScandinavian countries. Finally, I �nd that high family cohesion is usually accompanied by ahigh life expectancy.
Key Words: health, bequest, health insurance, family cohesion, life expectancy.JEL Classi�cation: D12, D31, D91, H51, I10
1. INTRODUCTION
What are the main reasons why the elderly decumulate wealth so slowly? Theeconomic literature has focused on explanations based on bequest motives and/or pre-cautionary savings motives. As has long been recognized, these two motives for savingsoverlap and cannot generally be distinguished from one another. This is mainly dueto an important consumption literature feature, namely allowing for uncertainty in life-cycle models. Moreover, while intergenerational transfers and availability of private andpublic health insurance appear to be of central importance in understanding patternsof wealth accumulation, relatively little is known about what motivates individuals toleave bequests.
1This paper is an extract from my Ph.D. dissertation. I am grateful to my supervisors, Prof.Guglielmo Weber and Prof. Larry Kotliko¤, to Prof. Randall Ellis and to the seminar participantsat University of Padua, Venice, Wharton School, University of New South Wales, CSEF, Universityof Tilburg and University of Aarhus for useful comments and suggestions. Financial support fromthe European Commission through the 6th framework program through the projects SHARE-I3, RII-CT-2006-062193, and COMPARE, CIT5-CT-2005-028857, is gratefully acknowledged. Any remainingerrors are of my responsibility.
1

The novel feature of this paper is twofold. First, using a realistic simulation exer-cise, I analyze the e¤ects of heterogeneous health shocks and medical spending riskson savings behavior in eleven European countries. Second, I consider intergenerationaltransfers to be actually used by the elderly to obtain health care in case of a healthshock. More speci�cally, the elderly are allowed to respond to health shocks in twodi¤erent ways, one involving direct payment for their health care expenses (self-insure)and another involving health insurance contracts. In the second case, I assume thathealth care can be provided formally by the market or informally by the family. Formalinsurance contracts may be a¤ected by asymmetric information problems, while infor-mal insurance depends on social consensus (cohesion) and on bequeathable wealth. Iestimate the model on SHARE data, using the simulated method of moments (SMM)for four levels of wealth and three country groups: Mediterranean, Central Europeanand Scandinavian. I make the strong assumption that there are no country-speci�cshocks.I �nd that the risks of longevity and facing high medical expenses can satisfactory
provide an explanation for increasing precautionary savings (and consequently bequests)with age after retirement. Moreover, the estimates of family cohesion, by country andwealth level, succeed in proving two relevant social literature �ndings on the strengthof family ties. First, family cohesion generally rises with age and declines with wealth.Second, it is higher in Mediterranean countries as opposed to Central European orScandinavian ones. Finally, I �nd that high family cohesion is usually accompaniedby a high life expectancy. More speci�cally, in Mediterranean countries the level offormal health insurance is low, health expenses being mainly covered by the family,while people tend to display rather high survival probabilities. On the contrary, inScandinavian countries, individuals register short life expectancies, despite the highformal coverage available.The remaining part of the paper is organized as follows: Section 2 develops the
dynamic model and Section 3 describes the data. Section 4 presents the estimationmethod, using Gauss-Herman quadrature and SMM. Results are illustrated in Section5, and Section 6 concludes.
2. THE MODEL
2.1. Utility function
For simplicity, I consider as the unit of analysis, the household consisting of onesingle individual who has just retired. This allows me to concentrate on consumption,health insurance and savings decisions, and not to consider labor supply and retirementchoices. The �rst period of observation occurs when the individual is 65 years old andentering retirement. The retirement age is assumed to be exogenous and deterministic,with all individuals retiring at the age of 65. Consequently, the model consists of a seriesof one-year periods, starting at the age of retirement and ending at the year of death,which is �nite and restricted to occur by maximum age 100. The maximum length ofthe retirement period therefore counts 36 periods (T = 36). Periods are indexed by t,the number of years in the retirement period, starting at 1 for age 65, so that overall1 � t � T; t 2 N: There is a stochastic survival probability st 2 [0; 1] in year t thatevolves in a matter de�ned in the model�s uncertainty section.Consider an individual seeking to maximize her expected lifetime utility at time t,
t 2 [1; T ], with an exponential discounting factor � > 0, by choosing current and futurelevel of consumption and insurance, both formal and informal. For each period, theindividual�s utility depends on her health status mt, consumption Ct, and face value
2

of insurance, formal Ft(ft�1) and informal It. All the variables mentioned above arefunctions of time, so they will be indexed by t, while Ft(ft�1) is at least of class C1
(�rst class of di¤erentiability). Consumption and insurance are additively separable,and the utility of being looked after (through formal and/or informal coverage) is aCES embedded in a constant-elastic function, with substitution parameter �.The within-period utility function is given by
u(mt; Ct; F (ft); It) : R+ ! R+ (1)
u(mt; Ct; F (ft); It) = �(mt)C1� t � 11� + �(mt)
��Ft(ft�1)
� + (1� �)I�t� 1��
� � 11� � ;
where mt 2 [0; 1] represents health status, and �t(mt) and �(mt) describe the healthstatus dependency of utility from consumption of non-durable goods and from beinglooked after respectively. Ct is consumption of non-durable goods in period t, Ft(ft�1)is the face value of the formal insurance policy, purchased the previous period (i.e.,health expenditures covered by insurance in period t) and It is the face value of theinformal insurance policy, purchased in period t. The parameters ; � > 0 are therelative risk aversion parameters for consumption of non-durables and medical goodsrespectively; � increases as individuals become less willing to substitute formal andinformal insurance across time, i.e., it measures the non-separability between formaland informal insurance.There are four health states modelled. State 1, mt(1) is death and state 2, mt(2) is
a state in which long term care of some form is required (invalidity or poor health). Instate 3, mt(3) the individual has medical problems but no need for long term care (fairhealth). State 4, mt(4) is the good health state.
�t(mt) determines how a person�s utility from consumption of non-durable goodsdepends on her health status, and is given by�
�t(mt) = 1 +mt; for 0 < mt � 1;�t(mt) = 0; for mt = 0;
(2)
so when dead (mt = 0); health status does not a¤ect utility from consumption, whilewhen healthy (mt = 1), it has a positive e¤ect on utility (the individual enjoys theconsumption of goods more when healthy).On the other hand, �(mt) determines how a person�s utility from insurance coverage
depends on her health status, and is given by��t(mt) = 1�mt; for 0 < mt � 1;�t(mt) = 0; for mt = 0;
(3)
so when sick (0 < mt � 1); health status does a¤ect utility from medical care, whilewhen healthy (mt = 1), it has no e¤ect on utility (healthy individuals do not enjoy anyconsumption of medical care).The face value of the formal insurance is given by
Ft(ft�1) = !ft�1 + f; ! � 0; ft�1 � 0; f > 0; (4)
with ft�1 as insurance premia paid in period t�1, before period�t health and medicalspending shocks are realized. The total amount paid for the formal insurance ft�1 isequal at the limit, with no public insurance provision, to the health care expenditurescovered through the health plan Ft(ft�1) adjusted by !; where ! is the inverse of theloading factor � (� < 1 allows for a tax subsidy for the insurance, while � > 1 is the
3

case of administrative costs or adverse selection). Almost all individuals who are 65or older are eligible for some government-provided compulsory health coverage, whichsupplements any private insurance coverage (!ft�1); f can be considered to re�ectthe minimum level of formal insurance provided by government, given that individualsare opting for a combination of formal and informal insurance. Notice that from anoptimization perspective, f represents the minimum health care consumption �oor andhas an impact on parameter estimates.The face value of an informal insurance policy, It represents the money value of the
time and/or �nancial transfers from the family on the individual�s behalf. Informalinsurance is considered to be function of three variables: the bequest that the elderindividual will transfer to the extended family after her death Bt, the family cohesioncoe¢ cient towards the individual �t, and individual�s probability of survival at timet+ 1, given that she is alive at time t, st, namely
It = �t(1� st)Bt ; �t 2 [0; 1]; (5)
with Bt = at+1 representing the wealth the individual will transfer to next periodif alive or leave as bequest if dead. The parameter �t is allowed to vary with theindividual�s age and from one group of countries to another, capturing the degree offamily cohesion. As a result, I assume that �t can be written as
�t = �0(1 + �1 � t+ �2 � t2 + �3 � t3 + �4 � t4); (6)
where �0 represents strictly family cohesion, while the fourth order polynomial inretirement years captures its age-structure. Assume that the market for informal insur-ance is perfect from the informational point of view: the premia paid for the informalinsurance equals the face value of the insurance. The intuition is that, for each period,family is providing an amount of informal care that equals a fraction of the elder�swealth, weighted by the probability that the individual will die next period and sothe bequest will actually be received; the per-period cost to insure informally equalsthe informal coverage, with bene�ts being received each period while the individual isalive, and costs being paid after her death. Note that the informal insurance provisionscheme implies a complete lack of commitment of the retired individual to the family,with respect to the amount of bequest she will leave at her death in return for the carereceived. There is an extended literature (Bernheim et al. 1985, Venti and Wise 2004,Chiuri and Jappelli 2006) arguing that illiquid assets can be considered as instrumentsfor commitment to leave a bequest. Instead of using this approach, I considered themore realistic scenario in which the informal care scheme is a function of the wholeamount of wealth that can constitute a bequest (liquid and illiquid assets and the �owof interests, dividends and pension income), adjusted for the individual�s probability ofdying next period.Finally, the distribution parameter � helps explain the in�uence of the relative for-
mal/informal insurance share in health care costs, and it depends on the health statusmt, (� (mt) = a �mt). I consider � (mt) as the coe¢ cient that assigns higher impor-tance to the informal care rather than to the formal one, if in poor or fair health states.Notice that, since the individual prefers, in certain circumstances, informal to formalcare, this element motivates the introduction of the strategic bequest through which theindividual actually purchases informal insurance. Obviously, the individual can decideindirectly how much to informally insure through the amount she decides to leave as abequest. She does that by directly choosing consumption and formal insurance premia,while the family provides the informal care according the cohesion measure �t.
4

2.2. Uncertainty
The individual faces several sources of risk, treated as completely or partially ex-ogenous. The reason is that the focus is on older people who have already shaped theirhealth and lifestyle, but who also make choices in terms of their way to respond tomedical care uncertainty through insurance. The individual�s utility depends on threestochastic variables:1) Health status uncertainty. I allow the transition probabilities matrix for health
status to depend on previous health status, wealth and age, as follows:
�kj = Pr(mt = jjmt�1 = k;wealth; age); k; j 2 f1; 2; 3; 4g : (7)
2) Survival uncertainty. Let smt;age = st denote the probability that an individual isalive at time t+1, conditional on being alive at time t, having time-t health status mt,and a certain age. This means that the death probability (1� st) in the utility functioncan equivalently be computed as (1� st) = �k1 = �(mt(1)), where k 2 f1; 2; 3; 4g.3) Medical expense uncertainty. Besides formal and informal insurance, there is a
third possibility to �nance the health spending, namely out-of-pocket.2 Health costsout-of-pocket, hct, are de�ned as the residual of total health care costs consideredexogenous ht, after deducting the coverage (both formal and informal), and a shock t.I assume that out-of-pocket medical spending depends on health status and age, and isdecreasing in formal/informal insurance coverage,
hct = ht ��!ft�1 + f
�� �t(1� st)Bt + �"t � t: (8)
In fact, ht is not a su¢ cient statistic for health spending out-of-pocket; in orderto maintain a certain health status, a continuous investment in health costs is needed.Consequently, the health costs of an individual who passes from poor to good healthwill exceed the costs of an individual persisting in a good health state. Moreover, eachhealth status has associated with it a necessary and deterministic health cost, ht(mt).3
After the individuals purchase insurance coverage, the exogenous health care spendingshock is realized and it persists according to an AR(1),
ln( t) = (1� � ) ln + � ln( t�1) + "t ; "t v N(0; �2"t): (9)
The issue of health dynamics and death is crucial to the insurance motive, given thehigh expenses associated with poor health. The health state follows a Markov chainwith an age-varying one-period state transition matrix P (t) described below. In eachyear, this is a 4 � 4 matrix. Retirees reaching age 100 die with probability one in thefollowing year. Together with the initial health state, the Markov transition matricesP (t); t 2 [1; T ]; enable the computation of future probabilities attached to all healthstates, including death. Given the initial health state m1, the transition matrix isapplied repeatedly to derive the probability �(mt) that a retiree is in one of the fourhealth states at time t > 1. Following the calibration used by Ameriks et al. (2005), Iconsider the same structure of age-dependent adjustment matrices, but I estimate thehealth status shifting parameters. More precisely, the 1-period ahead transition matrixat age 65 + t is given by
P (t) =
26641 0 0 0�21 �22 �23 1� �21 � �22 � �23�31 �32 �33 1� �31 � �32 � �33�41 �42 �43 1� �41 � �42 � �43
3775 �At;2Health costs out-of-pocket were not considered in the utility function since I assumed that if no
insurance coverage was available, the individual will have to incurr the health costs entirely out-of-pocket; however, if prudent, she will have an additional utility from being covered.
3Death expenses, ht(mt(1)), are also deterministic and are subtracted from the bequest.
5

with
At =
26641 0 0 0c1t
e 1� c1te 0 0c1t
e 11+c2
c1te c21+c2
1� c1te 0
c1te 11+c2+c2c3
c1te c21+c2+c2c3
c1te c2c31+c2+c2c3
1� c1te
3775 : (10)
The At matrix is the so-called age-adjustment matrix. It shifts probability mass fromthe left (worse health states and death) towards the right (better health states), relativeto the transition matrix at age 65, P (1). The three parameters c1; c2; and c3 controlhow fast this shifting occurs. Loosely speaking, parameter c1 controls the transitionfrom invalidity to death as age increases; c2 determines how much more likely death is,relative to invalidity, when in a fair or good health state, and c3 determines how muchmore likely a good health state will be when an individual is in good health. Basically, asthe agent becomes older, the exponent c1 allows for faster than linear shifting. Becausethe system is non-linear, there is no unique solution to the system of twelve equationand twelve parameters. Consequently, I estimate the parameters that control for thespeed at which the shifting occurs, together with the persistence and standard deviationof the Markov process characterizing the health spending uncertainty.
2.3. Budget constraint
Households enter retirement with wealth a1 � 0, and wealth at the beginning of timet is denoted as at. Assuming there is one composite riskless asset in which a householdcan invest, that yields a constant rate of interest r. Next period�s wealth is given by
at+1 = at + (y + rat)� ft � Ct � hct; (11)
where (y+rat) represents the income �ow, which includes constant pension paymentas well as wealth interests and dividends. Associated with this budget rule there is theborrowing constraint
at+1 = (1 + r)at + y � ft � Ct � hct � 0;8t: (12)
Note that I include in the borrowing constraint the medical expenses out-of-pocket,assumed to be realized at the beginning of the period, after health and medical spendingshocks are realized. I consider this assumption as more reasonable than the alterna-tive, namely that time-t medical expenses are fully unknown when individuals decidewhether to hold on to their formal or informal health insurance. Under this borrowingconstraint, given the timing of medical expenses, an individual with extremely highmedical expenses this year could have zero net worth next year.
2.4. Timing of the model
The timing of events is the following: The individual enters period t with health statemt, wealth state at and formal insurance Ft(ft�1), bought the previous period. At thebeginning of the period, she receives pension income and pays the formal insurancepremia for the next period. Then the health shock is realized and, if she is still alive,medical costs are realized, she consumes and saves; if she doesn�t survive the next period,funeral costs ht(mt(1)) are paid and the bequest Bt equals the remaining net resourcesafter accounting for the formal insurance purchased previously, down to a minimum ofzero,
Bt = max [at+1; 0] � 0;8t: (13)
6

One remark on the timing of insurance provision and payment: While in the formalmarket, the two moments are successive (coverage through the insurance becomes activefrom the next period with respect to the one in which the payment was made); inthe informal market, the moments have a considerable lag between them (individualbene�ts of medical services provided by the extended family in the current period,but she will get to pay at the end of her life). Assuming that there is a bequestinvolved (and so the elderly individual is not consuming all the wealth by the time ofher death), which the data will relate to country speci�c features, there is a higherincentive for the elderly to insure informally rather than exclusively through formalmarkets. On the other hand, medical goods provided in an institutionalized frameworkare less substitutable than the ones provided by the family or, in the case of the familyactually paying for the professional medical care, less expensive due to the risk-poolingof the formal insurance market (it is more pro�table to pay them through the formalinsurance purchased previously, and consequently consume more in the current period).Moreover, for the family, any optimal allocation involving informal care provision doesnot involve leisure, since its opportunity cost is certainly higher than the informal care�sprovision. Note that ht represents the annual health care costs and will be coveredthrough informal insurance up to a maximum amount which accounts for the yearlylabor time.
2.5. Recursive framework
Assuming the existence of a maximum, and given the functions continuity on thecompact space of wealth and formal insurance premia, the recursive form is
MaxCt;ft
Vt(mt; Ct; F (ft�1); It) =MaxCt;ft
((1 +mt)
C1� t � 11� +
+(1�mt)
h�(!ft�1 + f)
� + (1� �) (�t(1� st)Bt)�i 1��
� � 11� � +
+�stEt [Vt(mt+1; Ct+1; F (ft); It+1)]g ; (14)
subject to equation (12). An individual�s decision thus depends on her state vari-ables, Xt = (at; ft�1;mt; t) 2 R4+, and her overall set of parameters,
� = (�; �mt; �mt!; r; e; �; ; �; a; � ; �"t ; c1; c2; c3; �t(�0; �1; �2; �3; �4)) 2 R20:
From the discrete dynamic optimization principle it follows that the solution to theindividual�s problem is found in two steps: the �rst one consists of �nding the set ofconsumption fCt(Xt; �)g; formal insurance bene�ts fft(Xt; �)g; and, using these rules,the set of informal insurance bene�ts f�t(1�st)at+1(Xt; �)g; rules that solve the system(14). Inserting these decision rules into the wealth accumulation equation yields nextperiod�s wealth, at+1(Xt; �), for all the values that compose the grid for formal insurancepurchased in the previous period. Using the optimal values for wealth in the secondstep, the value function is maximized and the optimal value for the formal insurance isfound.I used backward induction to compute value functions and policy functions. The
optimization problem is solved by a grid search, and the state-space for wealth, formalinsurance and stochastic processes are made discrete. Given that t 2 [1; T ]; the solutionof the problem is obtained in a �nite number of periods. In the last period, the decision istrivial, with the agent consuming whatever is left, since at time T she has no probabilityto survive the next period. Once the policy function is solved, the corresponding value
7

function in the last period can be obtained and used in computing policy rules for theprevious period. This iteration is continued until t = 1.4
3. DATA
I estimate the dynamic model using data from the �rst wave of the SHARE dataset,a cross-national microeconomic database, containing household level information re-garding health, socioeconomic status and social and family networks of individuals aged50 or over. SHARE was conducted in 2004 in eleven countries covering the representa-tive regions of Europe: Scandinavia (Denmark and Sweden), Central Europe (Austria,France, Germany, Switzerland, Belgium, and the Netherlands) and the Mediterranean(Spain, Italy and Greece). Notice that, since the model refers only to single individu-als, observations regarding married people or those who have a registered partner weredropped. Mainly, the dataset used to estimate the model in Section 2 is formed by theannual values of voluntary (supplementary) private insurance (formal insurance hence-forth), expenditures on non-durables (consumption henceforth) and total wealth as aoverall measure of �nancial and real assets, as well as yearly income �ow.5 The datasetselected included only observations on individuals age 65 and over, who are divorced,widewers or do not have a registered partner. Also excluded are individuals with missingnet worth, net worth less than consumption of food at home, outside home or telephonebills or missing information for the variables used in the estimation. I also excludeindividuals with negative or zero wealth, according to the borrowing constraint of themodel.Based on the observations of formal insurance, consumption, total wealth and in-
dividual observable characteristics, a linear model was used to obtain the predictedvalues of formal insurance for all individuals that reported wealth. Consumption, onthe other hand, considers the amount spent on food at home, on food outside and ontelephone bills, all weighted according to coe¢ cients extrapolated from national datasetsof SHARE countries, through an ordinary least square procedure. Using only informa-tion contained in the �rst wave of SHARE made it impossible to obtain a temporaldimension of the variables that could latter be used to match the simulated series.To overcome this problem, data was further detailed by age and three total wealthpercentile: 25th, 50th and 75th wealth percentile. For the representative agent, anadditional pro�le was created to match the aggregate median value accross the data.By selecting wealth-speci�c groups of individuals, I recreated life-pro�les of identicalindividuals from the wealth point of view, with ages between 65 and 100. The missingvalues within each pro�le were obtained by linear interpolation. For ages beyond thelast year of age reported by the median individual, extrapolation proved much less reli-able than interpolation, especially since decision rules were non-linear. Each pro�le wasthen smoothed by taking �ve year moving averages, and extrapolated to age 100 (theassumed maximum age) based on average relative rate of growth of the variables in thelast 15 years. Finally, the procedure was repeated for all three groups of countries. Tomodel the medical costs associated with each health state, I identi�ed the mean annualfuneral, long-term care and curative and rehabilitation costs for the seniors using dataprovided by the OECD statistics.There are two econometric issues related to the use of cross-section data. First,
in a cross-section, because wages have increased over time (with productivity), olderindividuals are poorer at every age, and the measured saving pro�le will overstatewealth decumulation over the life cycle. By not accounting for this e¤ect, the model
4For further details, see Appendix B.5Details on variables de�nitions and motivation for their selection are in Appendix C.
8

will generate simulated data for which the degree to which elderly people run downtheir wealth is overstated. Second, rich people tend to live longer: the average survivorat each age has higher lifetime income than the average individual who has becomedeceased at that same age. This �mortality bias�tends to overstate asset growth. Morethan that, as time passes, the surviving people will be, relative to the deceased ones,healthier and knowing that they will live longer, will tend to save more than theirdeceased counterparts, displaying a slower wealth decumulation during the retirementyears. By not accounting for mortality bias, the model will simulate data that understatethe wealth decumulation process. The solution to both biases is o¤ered by the chosenestimation procedure: using a structural approach, these biases can be accounted fordirectly, by recreating them with the data generating process. Basically, each simulatedindividual is endowed with a certain age, total wealth and initial health status. If olderpeople have lower lifetime wealth in the data, they will have lower total wealth in thesimulated data as well. Similarly, the estimated decision rules and the simulated pro�lesincorporate mortality e¤ects, by di¤erent wealth percentile, as in the data.
4. CALIBRATIONS AND ESTIMATION METHODOLOGY
This section describes the parameters estimation procedure and provides a quantita-tive analysis of its predictions. I am conscious of literature uncertainty regarding the val-ues of many of the model parameters. Due to this reason, I estimate most of the parame-ters involved in the model and use literature values for those ones that I did not focus on,but used just as instruments for the dynamic programming model. The approach is sim-ilar to the two-step strategy used by Gourinchas and Parker (2002), Cagetti (2003), andFrench and Jones (2004): In the �rst step calibrate those parameters that can be cleanlyidenti�ed without explicitly using the model (�mt
; �mt!; r; e); in the second step esti-
mate the interest parameters � = (�; ; �; a; �; � ; �"t ; c1; c2; c3; �t(�0; �1; �2; �3; �4))with the two-stage SMM, taking as given the parameters estimated in the �rst step.The estimation will generate the parameter vector, yielding the simulated life-cycledecision pro�les that �best match�the data ones.Because the underlying motivation aims to explain why the elderly retain so much
wealth and why they insure formally and informally, I match total wealth, consumptionand formal insurance pro�les, conditional on age and wealth percentiles; in practice, Iconsider four samples corresponding to three wealth percentiles (25, 50 and 75) and themedian one, and for each of them I generate the time series of wealth, consumption andformal insurance for an individual aged between 65 and 100. I used a real risk-free assetreturn of (1+r) = 1:02; and for the health status shock, persistence coe¢ cient, �mt
, wasset to 0.5, volatility, �mt , was set to 0.214, while the age-adjustment matrix elementswere estimated based on the data. The grid and simulation starting point for wealth,consumption and formal insurance were set to match the data; for the bequest, I use thesame grid of values as for wealth. For the adjustment heath status-transition matrix, Iconsider the parameter e to be held �xed at e = 1:5 as in Ameriks et al. (2005). Finally,I set the loading factor � to its average value within each group of countries, considering� > 1 (administrative costs case).6
Assume the retirees at age 65 in good health (m1(4) = 1), following the healthdistribution of the sample selected. I realize that the sample is a¤ected by mortalitybias in the sense discussed at the end of the data section. However, since I actuallyestimate the health-transition matrix based on a sample of 100 simulated individualsthat face a cross-section of mortality rates in a given year, the model manages to recreate
6The country level of the loading factor was considered to match the administrative costs as per-centage of premia in 1999 (since no other data was available). See Comino (2003).
9

the health distribution of the real data. The construction of the transition matrix forthe health care stochastic process is described in Appendix D. To compute optimalstrategies, I �rst discretize the state space using the Gauss - Hermite quadrature method.The model is then solved by backwards induction, from the age of 65 to 100. For eachwealth group, I compute the life-cycle history for 100 arti�cial individuals, using randomdraws for the two stochastic variables. To each of these individuals, I assign a valueof the state vector Xt = (at; ft�1;mt; t) which endows them with a value of wealth,health coverage, health status and health costs consistent with the stochastic processesdescribed in Section 2.2.The SMM technique used for this work is the standard one. Solving the model
numerically and considering the stochastic structure of the solutions, allowed the simu-lation of each individual�s wealth, consumption, formal insurance and mortality. I thencompute pro�les from the arti�cial histories and take moments of each simulated pro�le.Comparing the mean of the arti�cial moments vectors to the ones computed from thereal data, parameters were adjusted until the di¤erence between the data and simulatedmoments was minimized.7 The goodness of �t between the two series is assessed by a�2�test statistic or corresponding p � value; the associated interpretation is whetheror not the true data moments (mT ) are equal to the realized data moments, given thestochastic processes for which the true time series is just one realization (mn(e�)) andperfectly �ts the set of parameters to be estimated. Analytically, as T ! 1; keepingthe number of random sequences �xed, if the weighting matrix W is chosen optimally,then
T [mT �1
N
NXn=1
mn(e�)]0cW [mT �1
N
NXn=1
mn(e�)]! �2(j � k);
where j is the number of moments, k is the number of estimated parameters and� 2 Rk unknown parameter vector. As a reasonable compromise between speed ande¢ ciency, I set N = 100 (number of simulated individuals). In practice, minimizationof the SMM estimator is done by a grid search where each parameter takes on di¤erentvalues. Note that the SMM requires a large number of simulations to compute thestandard errors of the estimator, even if the estimator is consistent for a �xed numberof simulations.The choice of SMM moments is still an open issue in the literature. In order to ease
the interpretation and restrain the set of moments that would potentially be too large,the model limited itself to considering measures of variability, instantaneous correlationcoe¢ cients and persistence. In particular, I restrict the estimation to a set of threevariables, namely wealth, consumption and formal insurance, and estimate the modelusing a set of �fteen true and simulated moments (mT =mN ), shown in Table 1.
5. RESULTS AND MODEL FIT
This section reports the estimation results and discusses the model�s implications inbehavioral terms. Tables 2 - 4 report the structural parameters estimates, while Tables5 - 88 present results on the set of �fteen moments match, as well as model �t for theaggregated and disaggregated models.
7The �rst stage takes place under the condition that the weighting matrix WT = IT : Obtainingthe estimates from this stage will allow us to repeat the procedure and use, at the second stage, theweighting matrix WT consistently estimated using the estimator proposed by Newey and West (1994),to obtain the �nal estimates. This matrix, heuristically, gives more weight to moments that are preciselyestimated in the data.
8See Appendix A.
10

TABLE 1Choice of Moments8>>>><>>>>:
�ln(at); �ln(Ct); �ln(Ct=at);corr(at; Ct); corr(at; Ft); corr(at; Ct=at);corr(Ct; Ft); corr(Ct; Ct=at); corr(at; at�1);corr(at; at�2); corr(Ct; Ct�1); corr(Ct; Ct�2);corr(Ft; Ft�1); corr(Ct=at; Ct�1=at�1); corr(Ct=at; Ct�2=at�2)
9>>>>=>>>>;Common wisdom would suggest that the simulated variables pro�les at the wealth-
speci�c level (disaggregated pro�le) �t the real ones much better than the averagepro�les, displaying less elevated values of the overidenti�cation test statistics. Whilethis is the case for the Scandinavian countries, it is not equally true for the Mediter-ranean wealth-speci�c models (all wealth-speci�c models register a worse �t than therepresentative agent model), or for the Central European group (only the 75th-wealthpercentile model outperforms the representative agent one).The structural parameters are estimated quite precisely.9 In most of the cases, we
are unable to reject the null hypothesis, that the sets of unconditional moments in themodel and in the data are the same. Only in few cases, the model does not displaya high goodness of �t with the empirical data. Nonetheless, even though the modelsare formally rejected, the generated life-cycle pro�les resemble, for the most part, thelife-cycle pro�les displayed by true data.10
As estimates illustrate, the simulated wealth pro�les of the �tted models track theactual wealth in a good proportion, and they can be considered to produce fairly goodpredictions. Analyzing the second-order moments, it is easily noticed that the simulatedwealth pro�les are �atter than the actual pro�les, but this might re�ect a weakness ofthe data, rather than a weakness of the model. The simulations show, for all twelveestimated models, that the pro�les generated by the data display quite high coe¢ cientsof relative risk aversion associated with consumption. With a lower discount factor,individuals are not willing to save, and this is shown by a drop in wealth for the �rstthree quarters of the retirement period. Because health-transition probabilities predictthat health worsens with age, simulated wealth turns back to increasing in the last periodquarter, since health and medical spending uncertainty give an incentive to insure.The simulated consumption pro�les follow the wealth pro�les, monotonically falling
during the entire period except for the last quarter. Even if neither monotonicity norsmoothness of the decline are displayed by the actual data, they do record a decreas-ing trend. This general tendency is consistent with most empirical studies of old-ageconsumption, suggesting that consumption falls with age (Banks et al. 1998).Turning �nally to the formal insurance pro�le, this also seems to register a monoton-
ically decreasing path: the lower the level of wealth, the lower the formal coveragepurchased for the next period. This e¤ect can be noticed for all wealth percentiles,especially in the �rst part of the time framework, while in the last years, even thoughwealth increases, formal insurance continues to decrease. Besides wealth, what deter-mines the values of formal insurance are not just di¤erences in mean medical expenses.More important, the di¤erences in the persistence coe¢ cient and the variance of the
9The overidentifying restrictions implied by the models pass a �2 -test at standard signi�cance levels.10These weak signi�cance levels registered for some models are also due to the real data pro�les. For
instance, in the case of Scandinavian countries, institutionalized individuals that enter nursing homesare excluded by sample design. As a result, it can be seen that the moments of the real data are quitedi¤erent with respect to Mediterranean and Central European data.
11

TABLE 2Estimated Structural Parameters, Mediterranean Countries
Param:25th wealthpercentile
50th wealthpercentile
75th wealthpercentile
Represent:agent
� �0:0169(0:0352)
�0:7135(0:0096)
�5:5296(0:0990)
�0:0009(0:0013)
3:4731(0:1269)�
4:7171(0:1282) � �
3:9661(0:0388) � �
5:6015(0:2793)�
� 0:1006(0:0059)�
�0:5426(0:0125)
0:5465(0:0058) � �
�0:0012(0:0075)
a 0:3931(0:0015) � �
0:2300(0:0296)�
�2:0994(0:0015)
0:0025
(0:10 � 10�4) � �� 1:2937
(0:1499)�0:8501
(0:0080) � ��0:7148(0:0045)
0:9500(0:0279) � �
�"t 0:1697(0:0035) � �
0:1120(0:0609)�
0:0453(0:0007) � �
3:6617(0:0172) � �
c1 0:0010(0:0152)
0:00088(0:0378)
0:00065(0:0287)
0:0024(0:0001)�
c2 1:1142(0:0036) � �
1:0902(0:0308) � �
1 + 10�7
(0:0626) � �10:1230
(0:0097) � �c3 0:1634
(0:0036) � �0:0012(0:0006)
10�7
(0:0056)0:5470(0:1821)
�0 1:5690(0:2015)�
2:8535(0:0337) � �
0:3902(0:0109)�
1:1453(0:0105) � �
�1�10�2 �0:0517(0:0115)
0:3247(0:2555)
�0:0051(0:0062)
�0:0388(0:0937)
�2�10�4 0:0120(0:0495)
�0:0092(0:7421)
0:85�10�4(0:96 � 10�6) � �
�0:268�10�4(0:77 � 10�6)
�3�10�4 0:0082(0:0725)
0:0015(0:0004)
0:1507(0:0038) � �
0:0037(0:0513)�
�4�10�8 0:1993(0:0030) � �
1:6948(0:0040) � �
�0:43 � 10�4(7:41 � 10�6)
0:69 � 10�4(4:26 � 10�6)�
Standard errors are in parentheses below each estimated parameter. (*) indicatessigni�cance at 5%, while (**) stands for signi�cance at 1%.
12

TABLE 3Estimated Structural Parameters, Central European Countries
Param:25th wealthpercentile
50th wealthpercentile
75th wealthpercentile
Represent:agent
� 1:7638(0:0121) � �
�0:0069(0:0085)
�1:4470(0:0197)
�0:0011(0:0188)
2:4325(6:714)
6:1664(0:0287) � �
8:4024(0:0030)�
6:4460(0:6250)�
� �1:2733(0:1743)
�0:7040(0:0008)
0:0739(0:0003)
�0:0113(0:0121)
a �1:8572(0:1202)
�0:0009(0:0651)
4:4950(1:3605)
�0:0100(0:0144)
� 2:0432(0:0108) � �
1:4332(0:0408) � �
0:9331(0:0066) � �
0:9472(0:0164) � �
�"t 0:2192(0:0102)�
0:1141(0:0051) � �
0:0731(0:0008) � �
3:0756(0:6404)
c1 0:00173(0:0030)
0:00172(0:0005)�
0:00017
(1:4810�5)�
0:0015
(2:67 � 10�4) � �c2 0:3123
(0:7190)0:2883(0:0571)�
0:2620(0:0462)
0:6067(0:4303)
c3 0:1230(0:0017) � �
0:0008(0:0007)�
2:2850(0:0266) � �
0:0039
(3:55 � 10�4) � ��0 �1:4336
(5:3515)�3:5498(0:7818)
�1:6974(0:0164)
0:7259(0:0137) � �
�1�10�2 �0:0215(0:1024)
0:0680(0:0008) � �
0:1300(0:0046) � �
�0:7195(0:0204)
�2�10�4 �7�10�5(0:319)
0:0024
(2:4 � 10�3) � ��1:5�10�5(0:0408)
�2:06�10�4(0:0696)
�3�10�4 0:0242(0:0009) � �
0:0012
(1:8 � 10�4)�0:1634(0:0378)�
0:0614(0:0022) � �
�4�10�8 0:0239(0:0009) � �
10:2053(0:5738) � �
0:0725(0:0085)�
2:50 � 10�4(0:0055)
Standard errors are in parentheses below each estimated parameter. (*) indicatessigni�cance at 5%, while (**) stands for signi�cance at 1%.
13

TABLE 4Estimated Structural Parameters, Scandinavian Countries
Param:25th wealthpercentile
50th wealthpercentile
75th wealthpercentile
Represent:agent
� 11:3468(6:5991)
7:9393(0:0064) � �
0:4968(0:0034) � �
�0:9787(0:1164)
2:0872(0:2420)�
8:7925(44:5089)
9:0303(0:8525)�
7:7751(3:2682)
� �2:1693(0:6424)
�3:4009(0:0075)
�0:8630(0:0196)
�2:2705(0:0433)
a 0:2135(0:0726)�
�1:6057(0:0016)
�0:0804(0:0211)
0:8859(0:0111) � �
� 2:1500(0:0766) � �
1:4540(0:0018) � �
0:9906(0:0017) � �
1:0077(0:0098) � �
�"t 0:2291(0:0023) � �
0:7538(0:0036) � �
0:1549(0:0011) � �
2:4373(0:1833)�
c1 0:0008
(3 � 10�5)�0:0042(0:2650)
0:0032(0:0002)�
0:0020(0:0041)
c2 0:0632(0:0012) � �
0:0101(0:1039)
0:0250(0:0075)
0:0411(0:0024)�
c3 1:3987(0:018) � �
0:0024(0:105)
0:0758(0:0022) � �
0:0051(0:0193)
�0 1:4956(0:0045) � �
�2:5466(2:2644)
�1:2619(0:0012)
�2:1472(2:8192)
�1�10�2 �0:0654(0:0100)
5:2107(2:5801)
2:3081(0:0033)�
3:5298(0:0617)
�2�10�4 0:0083(0:0352)
�9:4�10�4(2:66 � 10�4)
7:5�10�5(2:26 � 10�3)
2:242�10�2(0:0044)
�3�10�4 0:0156
(1:1 � 10�4) � �0:0565(0:0460)
0:0182(0:0093)�
0:2340(0:9837)
�4�10�8 0:4282(0:0029) � �
�0:0162(1:56 � 10�2)
�0:0064(0:2652)
�0:0518(0:0019)
Standard errors are in parentheses below each estimated parameter. (*) indicatessigni�cance at 5%, while (**) stands for signi�cance at 1%.
14

medical spending risk are relevant for the formal insurance purchase. If health insur-ance in general reduces health cost volatility, risk averse individuals may value healthinsurance at well beyond the cost paid. However, since they are at the end of their life,they may value more informal insurance.Results show that medical expenses for the elderly are high, and they tend to be
more persistent for the poor and median wealth individuals rather than for the rich.11
Additionally, I �nd that for Mediterranean and Central European countries, healthspending volatility is higher for the poor than for median wealth individuals, and higherfor the latter ones than for the rich. Since the poor are the ones that experience worsehealth with age, they will also register higher and more volatile medical expenses withrespect to median and high wealth individuals. The same is not registered for theScandinavian group, where, although the poor have more volatile medical spendingthan the rich, median wealth individuals have the highest spending variability. At thecountry level, for each wealth speci�c model, Mediterraneans experience less persistentand less volatile medical expenses than Central Europeans who, in turn, register a lowerpersistence and variability of health spending than the Scandinavians.Within the same country-group, the poor are more risk averse to medical care than
the rich. On the other hand, Mediterraneans display lower risk aversion than CentralEuropeans, who respectively register lower risk aversion than Scandinavians. This �nd-ing is consistent with the higher risk registered for out-of-pocket health expenditures inScandinavian countries rather than in the Mediterranean ones, and for the poor ratherthan for the rich, so it is not surprising that we �nd a high risk aversion for the poor andalso for the Scandinavians. Moreover, this result is con�rmed by the substitution coef-�cient estimates. As expected, the poor substitute less than the rich and Scandinaviansless than Central Europeans and Mediterraneans.Standard values for the relative risk aversion coe¢ cient for consumption in life-cycle
models are between 2 and 6. The estimated coe¢ cient for this model displays valuesbetween 3.2 and 5.6 for the Mediterranean countries, 2.4 and 8.4 in Central Europeanones and between 2.1 and 9.1 for the Scandinavian ones. These high values in some casesre�ect the relationship of age and wealth with the relative risk aversion, which indicatesits tendency to increase with age at any given level of wealth.12 While the absoluterisk aversion decreases with wealth, there is no such clear consensus on the relative riskaversion tendency to increase or decrease. In this case, for all country groups, I �ndthat poor individuals are less risk averse than the rich, the median and the averageones. Furthermore, Scandinavians are more risk averse than Central Europeans, whoare more risk averse than Mediterraneans, except for the poor who are less risk averse.Consequently, those with low wealth will tend not to save for consumption of non-durables, while their consumption of medical goods will never drop under a certainthreshold, even in the presence of a high negative health spending shock.The main result of family cohesion and life expectancy adds considerably to the
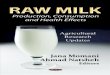
existing knowledge on inter-individual health and life expectancy disparities by wealthin Europe. Figure 1 shows relative cohesion coe¢ cients: the top four graphs refer to
11 I estimate the medical spending structural parameters, allowing for di¤erences from one healthstatus to another to be function of age. The estimates of the health spending risk are not understatedbecause the measure of medical expenditures risk included compulsory formal insurance provided bythe government.12Based on the life-cycle of risky asset positions, some research has argued that older investors are
more risk averse (Morin and Suarez 1983), but there is debate about their �ndings (Wang and Hanna1997 and Bajtelsmit and Bernasek 2001). Note that wealth does not include housing, and, althoughthere are no minimum wealth and consumption levels speci�ed in the model, I considered a minimumformal insurance provided compulsory by the government and I calibrated the model to �t wealth andconsumption data when constructing wealth pro�les.
15

Mediterranean countries, the middle ones to Central Europe, and the last ones to theScandinavian group.For all European country groups, estimates certify the social literature �ndings and
indicate that family cohesion rises with age, while it decreases with wealth. Moreaccurately, for poor and rich, family cohesion slightly decreases with age during the �rstretirement years, which corresponds to a drop in wealth, and then rises in the last partof the period (more for poor than for rich), causing wealth accumulation. A reasonableexplanation is that advanced ages are equivalent to higher probability of getting sick,which translates into an increased need for health care (especially informal) that induceswealth accumulation (for bequest) and family cohesion strengthening. Regardless of thewealth level, the Mediterranean group bene�ts from a stronger family cohesion thanCentral European group, that, in turn, displays a higher cohesion coe¢ cient than theScandinavian group, which is consistent with the sociological explanations provided inReher (1998).13
Finally, con�rming the demographic literature, I �nd that high family cohesion isusually accompanied by a high life expectancy and vice-versa. Figures 2 - 5 presenthealth-transition probability matrices conditional on age, previous health status andwealth for the three country groups.For Mediterranean countries, the lowest two panels in Figure 2 show the invalidity
and death probability for the individuals in good health. As can be seen, the probabilityof death within the next year of life rises from 0.20% at age 65 to 10.19% at age 100,while the probability of poor health (invalidity) is about 9.70% at age 65 and increasesto 17.53% for the poor and to 14.65% for the rich at age 100. Moreover, for eachage-group, rich people in poor health are less likely to die than poor people with thesame health condition and age: being in the 75th wealth percentile instead of the 25thpercentile lowers the probability of dieing by 40.74% at age 80. Likewise, invalidity isa very persistent health status: being a 69-year-old and having poor health implies a55.79% probability of having poor health also at age 70, and this probability falls withage, as the survival probability decreases. Moreover, rich people, at any age, have alower probability of dieing than poor individuals of the same age. In addition, rich aremore likely to maintain and to return in good health: high-wealth percentile individualsdisplay a higher probability of persisting in a good health state and returning to it if ina fair or poor health state.In Central Europe, healthy poor have a 7.50% higher chances of dieing than the
healthy rich at age 65, but only 9.52% higher chances at age 90 (see Figure 3), whichis similar to the Mediterranean countries. Overall, probability of death within oneyear of life if in good health increases from 0.27% at age 65 to almost 30% at age100. Regardless of the wealth levels, individuals in these countries tend to maintaingood health less than their Mediterranean counterparts, but the fact that the rich stayhealthy more than the poor is maintained. Rich people in Central Europe display alower probability to become invalid than the poor who are in good health, but eachcategory is more likely to die than its Mediterranean match.In Scandinavian countries, the probability of death when in good health rises with
age, surprisingly faster for rich and median wealth people than for the poor as shownby Figure 4; furthermore, it must be noted that the chances that death occurs whenin good health are extremely high, both in general (0.57% at age 65 and 89.91% for100 years old) and with respect to the Mediterranean and Central European countries.The same is not registered when the individual su¤ers poor health (invalidity), wherehealthy 65 year-old Scandinavians are as likely to become invalid as the Mediterranean
13The only exceptions are poor Central Europeans who display less cohesion than poor individualsin Scandinavian countries.
16

FIG. 1 Cohesion Coe¢ cient by Country Group and Wealth Percentile
17

FIG. 2 Health transition probabilities, Mediterranean countries
FIG. 3 Health transition probabilities, Central European countries
18

FIG. 4 Health transition probabilities, Scandinavian countries
or Central Europeans. Staying healthy or returning to good health is less likely as ageincreases, and the poor will do so at a rate of only 20% higher than the rich�s rate ofstaying healthy or returning in good health. Overall though, Scandinavians are morelikely to die than both Mediterraneans and Central Europeans.Although maintaining good health is becoming less possible as one moves to the
end of life, Mediterraneans display both a higher life expectancy and a higher inva-lidity probability than Central Europeans. Scandinavians, on the other hand, are theones that among all, register the smallest survival probability, having also the lowestchances of becoming invalid if they are in good health (see Figure 5). Moreover, in theMediterranean and Central Europe, at each age, rich are only slightly less likely to diethan poor, despite the wealth discrepancies, which are more accentuated in these coun-tries than in the Scandinavian ones. This is inconsistent with the expected outcome ofthe North European health care system, recognized to be the widest and most e¢ cientsystem in Europe, or with the fact that the poor are considerably more likely to diethan the rich. Instead, these �ndings con�rm the real demographic trends that indeedunderline an input - output discrepancy in the European health care systems.To summarize the empirical results, precautionary incentives implied by a dynamic
model in which retirees�face uncertain future medical spending, help reduce predictedconsumption towards levels of consumption actually registered among the elderly. Evenwith unusual estimates, such as the high risk aversion coe¢ cients, this model succeedsin explaining the wealth pro�les displayed by the elderly, decreasing right after theretirement and increasing towards the end of their life. Moreover, it fully con�rms thesociological and demographic �ndings on family cohesion and life expectancy.
19

FIG. 5 Health Transition for Representative Agent
20

6. CONCLUSIONS
It is well known that the risk of living long and facing high medical expenses isan important factor in elderly behavior. However, there is large heterogeneity in thehealth shocks and the medical spending risks that people face. In some cases, even inthe presence of health insurance, out-of-pocket health and nursing homes costs can bevery high, generating signi�cant low rates of dissaving among elderly. If individualsplace a high value on health insurance, provision of both formal and informal bene�tsmay have a large e¤ect on retirement behavior.To see if this is the case, I constructed and estimated a simulated life-cycle model
designed to outline the savings decisions of retired single households. As a novelty, itsimultaneously considered the e¤ects of both health risks and medical spending uncer-tainty on the saving choices of elderly in eleven European countries. It did so in thecontext of health insurance, provided formally by the market and informally by thefamily. Informal insurance was considered to depend on the strength of family ties (co-hesion) and on the wealth available for bequeathing. Using the �rst wave of SHAREdata and SMM, I estimated the model for four levels of wealth and three country groups:Mediterranean, Central European and Scandinavian.This paper provides several contributions. First, for all twelve speci�cations, para-
meters estimates are quite reasonable and the model �ts quite well. Second, I found thatthe sources of heterogeneity that I considered have a signi�cant role in explaining theelderly savings behavior, with a high level of medical expenses at advanced ages being akey factor for insuring by keeping large amounts of wealth. Third, results showed thatmedical expenses for the elderly are high and rising fast with age, while they tend to bemore persistent and volatile for the poor rather than for the rich, for all three categoriesof countries. In addition, poor Mediterraneans experience less persistent medical ex-penses than their Central European match that, in turn, register less persistent healthspending than their Scandinavian counterparts. Fourth, the paper carefully estimatedmortality probabilities by age as a function of health and wealth. It �nds that, al-though health deteriorates with age across all country groups, Mediterraneans displayboth higher life expectancy and higher probability of poor health than Central Euro-peans, con�rming the demographic data. Scandinavians, on the other hand, are the onesthat among all, register the smallest survival probability, having also the lowest chancesof becoming invalid if in good health, despite the vast and e¢ cient health care system.Finally, I found that high life expectancy usually accompanies a high family cohesion.Empirically, the estimates on family cohesion for all European country groups con�rmedthe social literature �ndings that family cohesion rises with age, while it decreases withwealth. Moreover, Mediterranean countries bene�t of a stronger family cohesion thanCentral European countries, that in turn display a higher cohesion coe¢ cient than theScandinavian group.From a policy perspective, it is important to understand why retirees dissave so
slowly. If the reason is to cover longevity risks or medical spending uncertainty, thendirect government changes in the public health insurance programs or indirect changes inthe social and family policies may in�uence saving behavior by controlling the exposureto such risks. In this sense, identifying a model capable of explaining consumers decisionsof elderly Europeans and estimating parameters for that population segment, allows abetter understanding of the e¤ects of reforming policies. The fundamental message ofthis paper is that in order to correctly evaluate any policy reform a¤ecting the elderlysaving decisions in Europe, one needs to accurately account for health care spending andcountry-speci�c family cohesion in relation to life expectancy, both by age and wealth.
21

REFERENCES
[1] Ameriks, J., Caplin, A., Laufer, S., Van Nieuwerburgh, S., 2005, Strategic Surveysand the Bequest Motive, Working Paper New York University
[2] Bajtelsmit, V. L., Bernasek, A., 2001, Risk Preferences and the Investment Deci-sions of Older Americans, AARP Working Paper 2001-11
[3] Banks, J., Blundell, R., Tanner, S., 1998, Is there a retirement-savings puzzle?,American Economic Review 88 (4), pp. 769�88
[4] Bernhein, B. D., Shleifer, A., Summers, L. H., 1985, The strategic bequest motive,Journal of Political Economy 93, pp. 1045-1076
[5] Brown, J. R., Finkelstein, A., 2004, The Interaction of Public and Private In-surance, Medicaid and the Long Term Care Insurance Market, Working Paper,Downloadable from Amy Finkelstein�s homepage, National Bureau of EconomicResearch, http://www.nber.org/~a�nkels/
[6] Bjornerud, S., Oliveira Martins, J., 2005, Disentangling demographic and nondemo-graphic drivers of health spending: a possible methodology and data requirements,Economics Department, OECD, Joint EC/OECD Workshop
[7] Cagetti, M., 2003, Wealth accumulation over the life cycle and precautionary sav-ings, Journal of Business and Economic Statistics, 21(3), pp. 339�353
[8] Chiuri, M. C., Jappelli, T., 2006, Do the elderly reduce housing equity? An inter-national comparison, CSEF Working Paper No. 158
[9] Comino, S., 2003, Analisi di casi esteri si assicurazioe sanitaria complementare:un quadro comparativo, in I fondi sanitari integrativi: quale futuro per la sanita�italiana?, ed. Milano Franco Angeli, Chapter 2.
[10] French, E., Jones, J. B., 2004, The e¤ects of health insurance and self-insurance onretirement behavior, Center for Retirement Research Working Paper WP 2004-12
[11] Gourinchas, P. O., Parker, J. A., 2002, Consumption over the life cycle, Economet-rica 70(1), pp. 47�89
[12] Morin, R.A., Suarez A.F., 1983, Risk Aversion Revisited, Journal of Finance 38(4),pp. 1201-1216
[13] Newey, W.K., West, K.D., 1994, Automatic Lag Selection in Covariance MatrixEstimation, Review of Economic Studies vol. 61(4), Blackwell Publishing, pp. 631-53
[14] OECD (2005b), Long-term Care for Older People, Paris.
[15] OECD in Figures 2006-2007, Demography and health - Healthspending and resources, OECD c 2006 - ISBN 9264022635,http://dx.doi.org/10.1787/427077022807
[16] OECD, 2006, Projecting OECD health and long-term expenditures: what are themain drivers?, OECD Economics Department Working Papers No. 477
[17] OECD, 2008, OECD Health Data 2008, http://www.oecd.org/document/27/0,3343,en_2649_34631_40902299_1_1_1_1,00.html
22

[18] Reher, D.S., 1998, Family ties in western Europe: persistent contrasts, Populationand Development Review. 24(2), pp. 203 - 234
[19] Venti, S. F., Wise, D. A., 2004, Aging and housing equity: Another look, in D. A.Wise (Ed.), Perspectives on the Economics of Aging, Chicago: The University ofChicago Press, pp. 127-175
[20] Wang, H., Hanna, S., 1997, Does Risk Tolerance Decrease With Age?, Associationfor Financial Counseling and Planning Education 8(2)
[21] Westerhout, E., Pellikaan, F., 2005, Can We A¤ord to Live Longer in BetterHealth?, Bureau for Economic Policy Analysis Netherlands, Document No. 85
23

APPENDIX A: ESTIMATED MOMENTS AND GOODNESS OF FIT
Table 5. Estimated Moments and Goodness of Fit Test - Mediterranean CountriesMoments 25th per:
Artif: Emp:50th per:Artif: Emp:
75th per:Artif: Emp:
�ln(at) 0:35 0:36 0:31 0:33 0:20 0:24�ln(Ct) 0:36 0:38 0:28 0:25 0:25 0:25�ln(Ctat )
0:62 0:61 0:39 0:33 0:24 0:21
corr(at; Ct) -0:32 -0:38 0:28 0:37 0:58 0:66corr(at; F t) 0:87 0:26 0:95 0:89 0:81 0:79corr(at;
Ctat) -0:69 -0:77 -0:60 -0:59 -0:38 -0:38
corr(Ct; F t) -0:07 -0:12 0:06 0:07 0:40 0:41corr(Ct;
Ctat) 0:79 0:77 0:49 0:47 0:42 0:42
corr(at; at�1) 0:79 0:85 0:80 0:94 0:78 0:91corr(at; at�2) 0:54 0:64 0:55 0:88 0:52 0:81corr(Ct; Ct�1) 0:62 0:68 0:88 0:91 0:87 0:87corr(Ct; Ct�2) 0:50 0:47 0:81 0:73 0:78 0:69corr(F t; F t�1) 0:67 0:94 0:77 0:97 0:79 0:95corr(Ct=at;Ct�1=at�1)
0:79 0:80 0:84 0:91 0:66 0:78
corr(Ct=at;Ct�2=at�2)
0:64 0:59 0:65 0:81 0:38 0:34
JT 0:55 0:32 0:16�2(1) 11:52 6:82 3:36p� value 0:0007 0:0100 0:0670
Table 6. Estimated Moments and Goodness of Fit Test - Central European CountriesMoments 25th per:
Artif: Emp:50th per:Artif: Emp:
75th per:Artif: Emp:
�ln(at) 0:40 0:40 0:32 0:38 0:34 0:33�ln(Ct) 0:45 0:45 0:20 0:24 0:05 0:14�ln(Ctat )
0:40 0:25 0:35 0:37 0:35 0:37
corr(at; Ct) 0:74 0:87 0:28 0:20 -0:15 -0:24corr(at; F t) 0:97 0:90 0:96 0:84 0:86 0:79corr(at;
Ctat) -0:33 0:02 -0:72 -0:84 -0:94 -0:95
corr(Ct; F t) 0:73 0:84 0:19 0:86 0:09 0:10corr(Ct;
Ctat) 0:33 0:48 0:35 0:26 0:36 0:30
corr(at; at�1) 0:78 0:95 0:80 0:88 0:78 0:85corr(at; at�2) 0:52 0:89 0:55 0:63 0:52 0:50corr(Ct; Ct�1) 0:94 0:94 0:87 0:94 0:67 0:68corr(Ct; Ct�2) 0:88 0:84 0:80 0:84 0:53 0:50corr(F t; F t�1) 0:74 0:98 0:74 0:98 0:73 0:94corr(Ct=at;Ct�1=at�1)
0:61 0:76 0:83 0:93 0:79 0:82
corr(Ct=at;Ct�2=at�2)
0:30 0:31 0:62 0:78 0:55 0:40
JT 0:45 0:40 0:1�2(1) 9:45 8:52 2:1p� value 0:0020 0:0035 0:147
24

Table 7. Estimated Moments and Goodness of Fit Test - Scandinavian CountriesMoments 25th per:
Artif: Emp:50th per:Artif: Emp:
75th per:Artif: Emp:
�ln(at) 0:45 0:44 0:57 0:53 0:80 0:73�ln(Ct) 0:18 0:18 0:04 0:27 0:04 0:27�ln(Ctat )
0:54 0:53 0:54 0:29 0:77 0:49
corr(at; Ct) -0:23 -0:26 0:71 0:93 0:69 0:92corr(at; F t) 0:76 0:47 0:99 0:96 0:99 0:80corr(at;
Ctat) -0:84 -0:82 -0:99 -0:85 -0:99 -0:85
corr(Ct; F t) 0:05 0:20 0:66 0:87 0:68 0:74corr(Ct;
Ctat) 0:61 0:60 -0:62 -0:72 -0:62 -0:79
corr(at; at�1) 0:78 0:89 0:78 0:97 0:77 0:95corr(at; at�2) 0:52 0:70 0:52 0:93 0:52 0:86corr(Ct; Ct�1) 0:59 0:81 0:89 0:93 0:86 0:89corr(Ct; Ct�2) 0:45 0:45 0:81 0:82 0:78 0:74corr(F t; F t�1) 0:58 0:98 0:76 0:98 0:77 0:98corr(Ct=at;Ct�1=at�1)
0:81 0:88 0:73 0:94 0:74 0:92
corr(Ct=at;Ct�2=at�2)
0:67 0:67 0:42 0:86 0:43 0:92
JT 0:36 0:74 0:74�2(1) 7:56 15:51 15:54p� value 0:0060 0:08 � 10�3 0:05 � 10�3
Table 8. Estimated Moments and Goodness of Fit Test - Representative AgentMoments Med: Gr:
Sim: Emp:Centr: Gr:Sim: Emp:
Scan: Gr:Sim: Emp:
�ln(at) 0:22 0:25 0:25 0:24 0:55 0:49�ln(Ct) 0:13 0:15 0:19 0:26 0:10 0:23�ln(Ctat )
0:24 0:25 0:24 0:14 0:50 0:29
corr(at; Ct) 0:35 0:28 0:50 0:85 0:67 0:88corr(at; F t) 0:85 0:84 0:63 0:61 0:98 0:92corr(at;
Ctat) -0:74 -0:79 -0:61 -0:78 -0:96 -0:91
corr(Ct; F t) 0:27 0:28 0:34 0:32 0:59 0:74corr(Ct;
Ctat) 0:23 0:28 0:29 0:45 -0:45 -0:73
corr(at; at�1) 0:79 0:92 0:79 0:87 0:78 0:96corr(at; at�2) 0:54 0:85 0:54 0:63 0:52 0:91corr(Ct; Ct�1) 0:72 0:51 0:76 0:82 0:80 0:89corr(Ct; Ct�2) 0:60 0:24 0:65 0:48 0:70 0:76corr(F t; F t�1) 0:81 0:97 0:80 0:98 0:76 0:98corr(Ct=at;Ct�1=at�1)
0:77 0:78 0:64 0:72 0:67 0:95
corr(Ct=at;Ct�2=at�2)
0:51 0:51 0:34 0:46 0:31 0:88
JT 0:15 0:32 0:87�2(1) 3:15 6:72 18:27p� value 0:0759 0:0095 0:0002
25

APPENDIX B: NUMERICAL SIMULATION
As mentioned, for the simulation I used the prospective-retrospective method ofthe dynamic programming and, more precisely, I used backward induction to computevalue functions and policy functions. Given that the model lacks a closed form solution,these decision rules are found numerically. The optimization problem is solved by agrid search, and the state-space for wealth and formal insurance is made discrete. Inthe last period, the decision is trivial, with the agent consuming and leaving bequestall available residual wealth. Here and throughout the paper, I normalized utility afterdeath at zero.At time T , the individual does not formally insure for the next period, and so the
issue is choosing consumption
MaxCt;ft
Vt(mt; Ct; F (ft�1); It) =MaxCt;ft
((1 +mt)
C1� t � 11� +
+(1�mt)
h�(!ft�1 + f)
� + (1� �) (�t(1� st)Bt)�i 1��
� � 11� � +
+�stEt [Vt(mt+1; Ct+1; F (ft); It+1)]g ;s:t:aT+1 = aT + y � CT �
�hT �
�!fT�1 + f
�� �T (1� sT )aT+1 + �"T � T
�;
under the condition sT = 0 and fT = 0:
Once the policy function was solved, the corresponding value function and policyrule in the last period were obtained and used in computing policy rules for the previousperiod. I �nd the decision rules at time T � 1 by solving the previous equation with VTand the �rst order conditions for consumption and formal insurance. This iteration iscontinued backward using Euler equations until t = 1. For all the shocks, I evaluated themodel using the Gauss-Hermite quadrature approach to discretization, and transformthe continuous problem into a discrete one with the constraint that the asymptoticproperties of the continuous and of the discrete processes should be the same. In thiscase, as shown in the model, I used Markov chains to represent each of the stochasticprocesses.The value function is directly computed at a �nite number of points within the
wealth grid, faT g40ia=1 ; the consumption grid fCT g1000ic=1, and within the formal insur-
ance grid, fFT�1g5f=1. Based on these grids, I used the decision rules to generate thethree simulated time series. On the other hand, at time t + 1, medical expenses (par-tially) and health status (totally) will be random variables. To capture uncertaintyover the stochastic components of medical expenses and health status, I convert mt
and t into discrete Markov chains, and calculate the conditional expectation of Vt+1accordingly. I integrated the value function with respect to the stochastic component ofmedical expenses, t, and of health status mt using 4-node Gauss-Hermite quadraturefor each chain. In order to be able to �nd the solution, the approach is to discretizethe consumption and formal insurance decision space and to search over these grids foreach point in the grid of wealth. Experiments with the �neness of the grids suggestedthat the grids I used (with 20 points for wealth and 5 points for the health insurance)gave reasonable approximations. In particular, I increased the number of grid pointsuntil the stage at which a further increase seemed to have a small e¤ect on the results.
APPENDIX C: DATA
As mentioned in Section 3, using data from SHARE, the true variables, chosen as
26

the benchmark for the simulated ones, are referring to the amount of formal healthinsurance that individuals are contracting, their consumption of goods and services and�nally to their total wealth, in which I included �nancial assets, real assets, as well aspension earnings/bene�ts and other annual income �ows.For the formal health insurance that individuals acquired during the last year, I con-
sidered the amount spent on all voluntary and supplementary health insurance contracts.The rationale behind this choice is based on the fact that compulsory insurance in Eu-rope is usually covered partially by the government14 (constituting its public spendingrelated to health care), and partially by the employers/employees (through contribu-tions to the health system). Consequently, the amount of formal health insurance thatindividuals actually buy is identi�ed by the supplementary, voluntary formal insurancecontracts that they acquire. In order to eliminate the missing values in the formalinsurance variable for those individuals who have reported wealth and consumption, Ipredicted formal insurance using a linear model that related the interest variable to thenon-durable expenditures, wealth and individual observable characteristic (age, proxyfor health status, number of children).The value of total consumption of goods and services was obtained by aggregating
the monthly data on consumption for all goods and services at the annual level, whilethe latter was imputed using the amount spent on food at home, food outside homeand telephone bills, each weighted by external coe¢ cients. These coe¢ cients were ob-tained using an OLS procedure on the same consumption variables but from additionaldatasets, speci�c to the countries that I analyzed.15
The pension earnings and bene�ts were considered to their extensive de�nition,meaning I considered all the types of pensions and associated bene�ts: old age/earlyretirement/pre-retirement pension, public disability/unemployment /survivor/invalidityor incapacity/war pension and private (occupational) old age/early retirement/disabilityor invalidity/survivor pension.SHARE collected comprehensive data on net worth, including level and interest
on the amount in bank accounts, government and corporate bonds, amount in stocksand correspondent dividends, amount in mutual funds and correspondent interest ordividend, amount in individual retirement accounts and contractual savings and facevalue of life policies, and net of total amount of money owed to other parties. One lastitem that it was included in the category of income �ow is the amount of income fromrenting other owned real estate, while the market values of the main property and ofother real estate and car(s) (if any owned), net of the main residence mortgage, wereconsidered to represent the real assets and income �ow that the individual possesses. I donot include bequests in the wealth measure since the age for the individuals consideredin the analysis was 65 and over, and so very few of them actually would receive anybequests.
APPENDIX D: THE HEALTH COST MODEL
The issue of medical costs is central to the analysis presented in this paper, especiallysince the aim is to properly account for the possibility of high costs associated withlong-term care and invalidity, and the informal arrangement is highly important. Thedistribution of these costs is controlled by the medical spending associated with each
14OECD in Figures 2006-2007, Demography and health - Health spending and resources. The levelsof minimum formal insurance were considered to be approximated by the public expenditure withhealth per capita in all the countries analyzed.15For Italy, Spain and Greece, the dataset used to obtain the external weights was ISTAT, while for
all the other countries I used the Dutch Consumption Dataset.
27

health state and by the one-period 4� 4 health state transition matrix P (t).The transition matrix for health status is parameterized by twelve elements, nine
probabilities that determine the value of P (1) (of the sixteen elements, four are �xed bythe death state being un-reversable and there are three further restrictions so that eachrow sums to one) and three parameters that control the row of probability from greaterhealth to poorer health as t increases. I selected values for these parameters to matchthe values computed by Ameriks et al. (2005) as starting points and then I estimatedthem through SMM.Some remarks on the signi�cance of the terms that I will attach to each health status
are as follow. The curative and rehabilitation expenditures16 comprises medical andparamedical services delivered during an episode of curative17 and/or rehabilitative18
care. These expenditures will be adequate to be considered in the case that the fairhealth status (3) is veri�ed. On the other hand, long-term health care19 comprisesongoing health and nursing care given to in-patients who need assistance on a continuedbasis due to chronic impairments and a reduced degree of independence and activitiesof daily living. In-patient long-term care20 is provided in institutions or communityfacilities. These expenditures will be adequate to be considered in the case that thepoor health status (2) is veri�ed.In the spirit of the Ameriks et al. (2005) paper, I consider the OECD Health Data
October 2006 Statistics reports in each country, namely 2004 average medical expensesfor non-institutionalized individuals and for assisted ones. Con�rming their study, I �ndthat among the periods the simulated retirees spend out of invalidity and death status(health states 3 and 4), a certain average amount speci�c to each country, in state 3 (fairhealth) so that h(mt(4)) = 0 and h(mt(3) > h(mt(4)) will reproduce these averages.For the invalidity state, I used Brown and Finkelstein�s (2004) approach that considersthe cost of long term care facility per capita. This leaves an annual expense for a fullyear of long term care at a lower amount than the costs of fair health. Consequently,I take h(mt(2)) < h(mt(3)). I also considered the costs associated with death to bethe highest ones, according to the formula used in the OECD calculations21 , and seth(mt(1)) > h(mt(2)). For each and every country analyzed, I �rst determined thesecosts based on the OECD Health Data October 2006 Statistics reports, and further usethis information in simulating the data.In practice, the primary data for funeral costs in the OECD countries analyzed
are drawn from the AGIR data set (Westerhout and Pellikaan 2005, based on EPC2001) for EU-15 countries, and OECD calculations for 2005.22 The cost of death forthe oldest group (95+) is assumed to be the lowest and was proxied by their observedhealth expenditure per person when available. For France, Germany, Italy, Spain, andNetherlands for which the expenditure for the oldest group were not available, the cost
16This item corresponds to HC.1+HC.2 in the ICHA-HC classi�cation of health care functions.17An episode of curative care is one in which the principal medical intent is to relieve symptoms of
illness or injury, to reduce the severity of an illness or injury or to protect against exacerbation and/orcomplication of an illness and/or injury which could threaten life or normal function.18Rehabilitative care comprises services where the emphasis lies on improving the functional levels
of the persons served and where the functional limitations are either due to a recent event of illness orinjury or of a recurrent nature (regression or progression). Included are services delivered to personswhere the onset of disease or impairment to be treated occurred further in the past or has not beensubject to prior rehabilitation services.19This item corresponds to HC.3 in the ICHA-HC classi�cation of health care functions.20Long-term care is typically a mix of medical (including nursing care) and social services. Only the
former is recorded in the SHA under health expenditure.21See Bjornerud and Oliveira Martins (2005), OECD (2006).22 I obtained the death related costs data for 2004 by applying the health expenditure real growth
rate to the 2005 serie (see OECD Health Data 2008).
28

of people aged 75-79 was taken as a proxy. In fact, when available, expenditure atage 95+ is roughly equal to the level of expenditure at age 75-79. For the countrieswhere no cost expenditures were available, the cost of death for the oldest group wasestimated by taking 3 times the average health expenditure per capita, adjusted bythe country-speci�c residual (Bjornerud and Oliveira Martins 2005, OECD 2006). Thetotal long-term care expenditure in percentage of GDP in 2005 was calibrated to �t theestimates of the OECD Long-term Care study (OECD, 2005b), when available. Datafor the countries not available in this study were obtained by applying the ratios oflong-term care to GDP observed in �similar�benchmark countries, as indicated in Table9.
Table 9. Benchmark countries in OECD studiesCountry estimated Benchmark countries
Belgium NetherlandsDenmark average (Norway, Sweden)France GermanyGreece SpainItaly average (Germany, Spain)Switzerland Germany
29