Embed Size (px)
Citation preview

Tissue Plasminogen Activator for the Treatment of
Parapneumonic Effusions in Pediatric Patients
Emily N. Israel1,2 and Allison B. Blackmer1,2,*1Department of Pharmacy Services, University of Michigan Health System, Ann Arbor, Michigan; 2Department of
Clinical, Social, and Administrative Sciences, University of Michigan College of Pharmacy, Ann Arbor, Michigan
Intrapleural fibrinolysis has been investigated for the treatment of pleural effusion for several decades.Fibrinolytics have the ability to break up fibrin and loculations that characterize complicated pleuraleffusions, facilitating drainage. Older fibrinolytics such as urokinase and streptokinase have beenreplaced by tissue plasminogen activator (tPA) for this indication due to product availability and amore favorable safety profile. The literature supports tPA as a treatment approach for this indication inadult patients, and the use of tPA has become a standard management approach in this population.Over the past decade, data on the efficacy of intrapleural fibrinolytic therapy in children have alsobeen generated, which now support the use of fibrinolysis as a treatment alternative to more invasivetherapeutic options such as surgical intervention. In this review, we discuss the pathophysiology, diag-nosis, and treatment of parapneumonic effusion and empyema, with a focus on intrapleural fibrinoly-sis, specifically tissue plasminogen activator, in the pediatric population. Recent articles providesufficient evidence to support the use of this drug in pediatric patients for the management of pleuraleffusions; however, due to study heterogeneity, questions remain that may be addressed in futurestudies.KEY WORDS pediatric, tissue plasminogen activator, pleural effusion, empyema, fibrinolytic, parapneu-monic effusion.(Pharmacotherapy 2014;34(5):521–532) doi: 10.1002/phar.1392
Pleural effusion is defined as the accumulationof excess fluid in the pleural space between thelung and the chest wall.1 Several possible etiolo-gies for pleural effusion are heart failure,trauma, liver disease, and malignancy, as well aschylous and transudative effusions.2 However, inthe pediatric population, pleural effusions aremost commonly caused by infection—typically abacterial pneumonia—and are thus termed para-pneumonic effusions.3 Empyemas are moreadvanced, organized effusions and refer to locu-lations or pus in the pleural space.1 Althoughnot all effusions require intervention, those that
are infectious in origin, are more advanced, orlarge enough in volume to affect respiratorydynamics may necessitate medical and/or surgi-cal treatment.4–6
After the introduction of routine immuniza-tion of infants with the 7-valent pneumococcalconjugate vaccine in 2000, the hospitalizationrate associated with all-cause pneumonia in chil-dren younger than 2 years of age declined by33% in the United States.7 Despite this decrease,the rate of empyema complicating community-acquired pneumonia in children has risen acrossthat same time period; specifically, the reportedrate was 3.5 cases/100,000 children from 1996–1998, whereas the rate was 7 cases/100,000 chil-dren from 2005–2007.7 Pleural effusion maycomplicate up to 60% of pneumonias.8–10 Symp-toms are related to the size and extent of thepleural effusion and may include fever, tachyp-nea, and increased oxygen requirements.9
*Address for correspondence: Allison B. Blackmer,Department of Pediatric Surgery, College of Pharmacy, C.S.Mott Children’s Hospital, The University of Michigan, 1540East Hospital Drive, Room 10-561B, Ann Arbor, MI 48109;e-mail: [email protected].� 2014 Pharmacotherapy Publications, Inc.

Effusions may subsequently progress to empy-emas, which increase the risk of morbidity andmortality. Mortality associated with empyema isroughly 20% in adults but is significantly lowerin children.4, 9 However, empyema in the pediat-ric population is still associated with significantmorbidity including restrictive lung disease andthe necessity for advanced medical and invasivesurgical interventions.4
Intrapleural fibrinolysis was initially investi-gated nearly 60 years ago for the treatment ofempyema and has now become a standard man-agement approach in adult patients.10, 11 Overthe past decade, data on the efficacy of fibrino-lytic therapy in children have been generated,which now support fibrinolysis as a treatmentalternative to invasive surgical interventions. Inthis review, we discuss the pathophysiology,diagnosis, and treatment of parapneumonic effu-sion and empyema, with a focus on intrapleuralfibrinolysis with tissue plasminogen activator(tPA), in the pediatric population.
Pathophysiology
Parapneumonic effusions and empyemas arecommonly caused by the typical pathogensresponsible for bacterial pneumonia: Streptococcuspneumoniae, Streptococcus pyogenes, Staphylococ-cus aureus, Haemophilus influenzae, Pseudomonasaeruginosa, and Mycoplasma pneumoniae.3, 4, 12, 13
In response to infection, pleural secretions andcapillary permeability are increased, resulting inan accumulation of fluid. This fluid collection—the pleural effusion—can cause a mass effect,resulting in restriction of lung expansion andeventual increased oxygen requirements.11, 12
The stimulation of the inflammatory cascade mayalso lead to subsequent activation of the coagula-tion cascade and fibrin deposition, ultimatelyleading to the formation of an empyema.11, 12 Thedisease process develops along a time continuumthrough three stages: exudative, fibrinopurulent,and organizational. The risk of poor outcomeincreases as the disease progresses. The presenceof pus is typically associated with the worst out-comes; however, any of the criteria associatedwith moderate- or high-risk effusions confer arisk of poor outcome.5
The exudative stage is characterized by a rapidaccumulation of free-flowing fluid in the pleuralspace. This is secondary to interstitial fluidcrossing the pleura and entering the pleuralspace due to inflammation and increased capil-lary permeability.1, 12 At this point, the effusion
is still considered to be uncomplicated. However,the fluid frequently becomes secondarily infectedand marks the transition of the effusion into thefibrinopurulent stage. The fluid collection at thisstage becomes increasingly complicated as theinfection leads to continued inflammation.12
Increased metabolic activity due to microbialgrowth affects the chemistry of the pleural fluidand causes the glucose concentration and pH todrop.7 Neutrophil lysis also causes a concurrentrise in the lactate dehydrogenase concentration.7
In this phase, the coagulation cascade and fibri-nolysis become imbalanced, leading to fibrindeposition, loculations, and adhesions.12 In thethird phase of disease progression, the organiza-tional phase, the fluid collection develops intoan empyema. As advanced complicated effusionsbecome organized, pus develops within the pleu-ral space, and fibroblasts produce a thick,fibrous pleural peel.12 Loculations develop fur-ther, and the thickened collection creates a masseffect, preventing effective lung expansion.12
Table 1 depicts the physiologic characteristics ofeach of these three stages.
Diagnosis
Multiple diagnostic modalities are availablefor evaluating pleural effusion in pediatricpatients. The main imaging options includechest radiograph (CXR), ultrasound, and com-puted tomography (CT).9 Initial CXR is oftenused to identify a possible effusion; however, itcannot specifically differentiate between free-flowing effusion and loculated empyema, oreven pneumonia-related lung consolidation.9, 14
Serial CXRs may be particularly helpful whenevaluating disease progression and the effect oftherapy in children who are not clinicallyimproving with standard care.3, 13 In addition,CXR can help identify other conditions associ-ated with parapneumonic effusion and empyemasuch as pneumothorax, lobar consolidation, airfluid levels, and pneumatoceoles.14
The American Pediatric Surgical Association(APSA) Outcomes and Clinical Trials Committeepublished recommendations in 2012 for thediagnosis and management of empyema in chil-dren. The APSA recommends ultrasound as thefirst-line option for imaging in children withsuspected pleural effusion based on CXR.9 Ultra-sound has many advantages in this populationincluding low relative cost, portability, and lackof associated radiation. However, the utility ofultrasound is dependent on the quality of images
522 PHARMACOTHERAPY Volume 34, Number 5, 2014

and operator expertise. Further, ultrasound maynot be readily available at all institutions. Com-puted tomography offers an alternative diagnos-tic modality. Similar to ultrasound, CT providesinformation about pleural thickening and locula-tions; however, it may be less accurate thanultrasound in identifying fibrin deposits. Com-puted tomography is significantly more expen-sive than ultrasound. Additionally, radiationexposure associated with routine CT use mayincrease the long-term risk of malignancy. TheAPSA recommends using CT only in complexcases in which ultrasound is inadequate or addi-tional information is required for surgical deci-sion making.Definitive diagnosis is possible with diagnostic
thoracentesis, a procedure involving the aspira-tion of pleural fluid from the effusion with aneedle.10 The collected fluid is analyzed forcharacteristic diagnostic findings across thestages of disease (Table 1).
Treatment
A summary of the classic treatmentapproaches across the stages of disease isincluded in Table 1. Exudative (or simple)parapneumonic effusions are often effectivelymanaged with medical therapy alone. Early initi-ation of appropriate antibiotics can decrease theseverity and duration of effusions.3 Empiric ther-
apy should be selected based on the suspicionfor community- versus hospital-acquired infec-tions, the patient’s immunization status, as wellas local resistance patterns and suspicion formore virulent organisms such as communityacquired methicillin-resistant Staphylococcusaureus.3, 4, 10, 13 The pleural fluid may also becultured, obtained either by thoracentesis ordrainage with tube thoracostomy, in order tohelp further guide and tailor antibiotic therapy.3
In patients with more advanced (or complex)pleural effusions, antibiotic therapy alone maybe insufficient, and additional drainage of thepleural fluid is necessitated.3 Initial options fordrainage of pleural fluid include therapeutic tho-racentesis or chest tube placement as monother-apy, or chest tube placement with concomitantchemical debridement (e.g., fibrinolytic ther-apy).3, 4 First-line therapy often includes chesttube drainage; but, therapeutic thoracentesis issomewhat less invasive and may be pursued ini-tially.12 If thoracentesis is used as first-line ther-apy, the 2011 British Thoracic Societypublication recommends placement of a chesttube after the first failed thoracentesis attempt(e.g., fluid reaccumulation).3 However, drainageby repeated thoracentesis has not been com-pared with chest tube placement alone.Drainage may be unachievable at more
advanced, or complex, stages of pleural effusiondue to fibrin deposition and loculations.8 In
Table 1. Phases of Pleural Effusion1, 8, 12
CharacteristicExudative Phase Fibrinopurulent Phase Organization PhaseUncomplicated Complicated
Risk of Poor Outcome Low Moderate High
Fluidcharacteristics
Thin, free-flowing,no pus or fibrinLow white bloodcell countProtein presentLow lactic aciddehydrogenaselevel (< 3 9 ULN)Normal pH (≥ 7.2)Glucose level> 60 mg/dl
Thicker, cloudy fluidFibrin presentIncreased white bloodcell countHigh lactic aciddehydrogenaselevel (> 3 9 ULN)Low pH (< 7.2)Glucose level < 60 mg/dl
Very thickPus and fibrin peel presentLoculations presentIncreased white bloodcell countHigh lactic aciddehydrogenaselevel (> 3 9 ULN)Low pH (< 7.2)Glucose level < 60 mg/dl
Gram stainand culture
Unknown or Negative Positive Positive with presenceof pus
Classic treatmentapproach
Antibiotics AntibioticsDrainage of pleural fluid bytherapeutic thoracentesis orchest tube placement
AntibioticsDrainage of pleural fluidby therapeutic thoracentesisor chest tube placementInvasive surgical procedures(video-assisted thoracoscopicsurgery, open thoracotomy)
Role for fibrinolytics No Yes Yes
ULN = upper limit of normal.
Intrapleural tPA in Pediatric Patients Israel and Blackmer 523

patients unable to achieve sufficient drainage ofpleural fluid, additional intervention is war-ranted in order to avoid continued lung restric-tion, increased oxygen requirements, andprogression to higher levels of respiratory sup-port such as mechanical ventilation or extracor-poreal membrane oxygenation.3 The historicalgold standard of care for more progressiveempyema is surgical intervention. The two mostcommon surgical procedures for progressiveempyema include minimally invasive video-assisted thoracoscopic surgery (VATS) and openthoracotomy for decortication of loculations.5
The VATS procedure is currently consideredthe first-line surgical option for qualifyingpatients. It is a newer, highly effective techniquethat allows for debridement and decortication ofloculations through minimally invasive accessand direct visual inspection of the pleural spacewith the use of a laprascope.3 As a minimallyinvasive surgery, patients may experience lesspostoperative pain and a quicker recovery per-iod compared with other surgical options. Fur-thermore, the risk of long-term associatedmorbidity is lessened. However, some patientsare not candidates for this procedure and/ormay eventually require a more invasiveapproach. Open thoracotomy with decortication,although extremely effective and thorough,remains the most invasive option for debride-ment and may be required in up to 35% ofpatients who fail conservative medical measuresor in those who fail the VATS procedure.8 Com-pared with VATS, the open thoracotomy proce-dure requires a larger surgical incision, is highlyinvasive, and is associated with significantlymore postoperative pain, a longer recovery per-iod, and additional postoperative morbidity(e.g., potential for rib fusion and scoliosis). BothVATS and open thoracotomy are associated withthe risk of postsurgical complications such asbleeding and the requirement for extended ven-tilator support.
Fibrinolytic Pharmacology andPharmacokinetics
Since the early 1950s, fibrinolytic therapy hasemerged as a less invasive alternative treatmentapproach to the more invasive surgical proce-dures for complicated effusions described above.The theory behind the use of fibrinolytics isrooted in the idea that complicated parapneu-monic effusions and empyemas are characterizedby fibrin deposition.8 The ability to break up
fibrin and loculations with intrapleural fibrino-lytics allows for greater success in achievingdrainage without further surgical or mechanicalinterventions.Although not currently available in the United
States, the first-generation fibrinolytics, strepto-kinase and urokinase, were initially used to treatparapneumonic effusions and empyema.15–18
Streptokinase indirectly activates the fibrinolyticsystem by binding plasminogen and causing con-formational change.12, 19 An active site is subse-quently exposed and cleaves other plasminogenmolecules to promote the formation of plas-min.19 Urokinase, a thrombolytic agent obtainedfrom human neonatal kidney cells grown in cul-ture, works slightly differently; one plasmin mol-ecule can be directly activated by each urokinasemolecule.12, 20 Plasmin then promotes the break-down of fibrin.19 Although more common withstreptokinase, both agents have been associatedwith adverse effects, specifically, immunologicand hypersensitivity reactions.12 Furthermore,an antibody-mediated response that caused inef-fectiveness with repeat dosing was also associ-ated with streptokinase use because itsproduction is bacteria based.12, 17
Tissue plasminogen activator was developedas an answer to some of the drawbacks associ-ated with the first-generation agents. It bindsdirectly to fibrin and catalyzes the conversion ofplasminogen to plasmin, leading to fibrinoly-sis.12 Furthermore, tPA is not associated withhypersensitivity reactions and retains its effec-tiveness over multiple doses.12 Although thepharmacokinetic parameters of intrapleural tPAhave not been definitively determined, whengiven intravenously, the volume of distributionapproximates plasma volume. Clearance is rapidfrom the plasma through metabolism in theliver, and the half-life of tPA is less than 5 min-utes in adult patients.21
Approved indications for systemic tPA includemanagement of acute myocardial infarction, acuteischemic stroke within 3 hours of stroke symp-tom onset, and acute massive or unstable pulmo-nary embolism in adults.21 Tissue plasminogenactivator is also approved for restoring patency tocentral venous access devices.22 Unapproved indi-cations include treatment of arterial thrombosisand fistula thrombosis, ocular surgery, vasculargraft occlusion, venous thromboembolism, andintrapleural use.23
Absolute contraindications to systemic tPAtherapy include previous allergic reaction,trauma within the previous 48 hours, or bron-
524 PHARMACOTHERAPY Volume 34, Number 5, 2014

chopleural fistula.12, 19 Relative contraindica-tions include history of hemorrhagic stroke;coagulation deficiencies; and major thoracic,abdominal, or cranial surgery within the previ-ous 2 weeks.12, 19 Contraindications to intraple-ural administration of tPA are not wellestablished and are founded on clinical experi-ence and safety risks published in the literature.
Supporting Literature in Adults
The use of fibrinolytic therapy is well estab-lished in the literature in adults, with numerouscase reports, retrospective reviews, and random-ized trials supporting its use for the treatmentof complicated pleural effusions and empy-emas.24–30 A comprehensive review of the adultliterature was provided in a 2010 publication.12
Intrapleural tPA has demonstrated improvedchest tube drainage, resolution of symptoms,decreased need for invasive surgical procedures,and shorter hospital stays.12 The literaturesupporting the use of intrapleural tPA in adults,however, is heterogeneous with regard to indica-tions, therapeutic end points, dosing, frequency,duration of treatment, and dwell time.A recent investigation in the adult population
evaluated dual intrapleural therapy with tPAplus recombinant human dornase alfa.29 Empy-ema fluid typically contains large amounts ofextracellular DNA. Dornase alfa (or DNase)degrades polymerized deoxyribonucleoproteinsin bacterial and mammalian cells, theoreticallyreducing pus viscosity and facilitating drain-age.12, 29 In a multicenter, prospective trial, 210adults with parapneumonic effusions were ran-domized to receive one of four possible treat-ments: tPA plus dornase alfa, dornase alfa plusplacebo, tPA plus placebo, or double placebo.29
Dornase alfa 5 mg plus tPA 10 mg were giventwice/day for 3 days, with a dwell time of1 hour. The group receiving combination ther-apy with dornase alfa and tPA showed a signifi-cant decrease in the area of pleural opacity onCXR. Patients who received dual therapy werealso less likely to require surgical referral, hadincreased pleural fluid drainage, and haddecreased total length of hospital stay. Theother three treatment arms did not show a sta-tistically significant benefit. No significant differ-ences in adverse effects among the groups werereported. Thus, dual therapy with intrapleuraltPA and dornase alfa is concluded to be safeand effective in adults with parapneumoniceffusion.
Supporting Literature in Pediatric Patients
Since the 1990s, investigations of fibrinolytictherapy have expanded into the pediatric popu-lation. The efficacy of intrapleural fibrinolyticsin the pediatric population has been demon-strated in several retrospective studies, casestudies, and case series (Table 2), as well as oneprospective study.
Retrospective Data
Early Use of tPA in Pediatric Patients
Early case reports and case series describedsuccessful treatment with tPA in pediatricpatients as demonstrated by resolution of clinicalsigns and symptoms, increased chest tube drain-age, improvements seen on CXR and CT scan,and prevention of surgical intervention.8, 31 Thefirst published case of successful intrapleuraltPA in a pediatric patient, published in 2001,suggested preliminary efficacy in the pediatricpopulation.8 A 6-year-old boy received tPA 5 mgdiluted in 50 ml of normal saline by chest tubeinstillation for management of pleural effusion.The chest tube was clamped for 1 hour, and asecond dose was given 8 hours later. Chest tubedrainage was increased, the CXR demonstratedimprovement, and invasive, surgical interven-tions were avoided.Similar findings were published in 2003.31 A
10.3-kg, 16-month-old female received tPA 2 mgdirectly instilled intrapleurally for a persistentparapneumonic effusion, decreased chest tubedrainage, and ongoing clinical signs and symp-toms despite appropriate antibiotic therapy.Over 6 days, the patient received four doses oftPA, each dwelling for a 4-hour period. Treat-ment success was measured by increased chesttube drainage, improvement of clinical signs andsymptoms, and resolution seen on both CT scanand CXR.A small case series of six children aged
2–13 years old evaluated the efficacy of tPA asmeasured by the difference in chest tube outputbefore and after tPA administration.32 Patientsreceived tPA 2–5 mg mixed in normal salinewith a dwell time ranging from 4–6 hours. Doseswere repeated every 12–24 hours until resolutionwas observed on CXR or therapy was no longerdeemed to be efficacious (e.g., volume instilledequaled volume drained). Patients received, onaverage, a total of 3–6 doses. In addition, unlikeany other published report, patients were rotated
Intrapleural tPA in Pediatric Patients Israel and Blackmer 525

Table
2.SummaryofRetrospectiveStudies,
CaseSeries,
andCaseRep
ortsofTissuePlasm
inogen
ActivatorfortheTreatmen
tofParap
neu
monic
Effusions8
,14,31–36
Publication
Typ
ePatientPopulation
tPADose,Preparation,Frequency,
andDuration
Dwell
Tim
eOutcomeMeasuresandResults
AdverseEvents
Comparative
case
series
36
54childrenwithparapneumonic
effusion,divided
into
fourgroups:
chesttubealone(n=18);chesttube+
fibrinolytics
(n=24);chesttube,
fibrinolytics,andsurgery(n=5);or
surgeryalone(n=6)
tPA2mgmixed
in20mlnorm
alsalineinstilledbychesttube,
repeatedevery12hrs
for
48–7
2hrs
1hr
Hospital
lengthofstay
increasedin
surgerygroupsvs
nonsurgerygroups;
timingoffibrinolytics
did
notaffect
outcomes
Bronchopleural
fistula
(4patients,
1in
each
group)
Retrospective
cohort
study35
53childrenaged
3mo–1
7yrs
(weigh
t5–6
4kg)
withcomplicated
parapneumonic
effusion:30children
received
tPA,administeredearly
(<24hrs
afterdiagn
osis[n=12])
or
late
(>24hrs
afterdiagn
osis[n=18]);
23childrenweremanaged
bytube
thoracostomyalone(controlgroup)
tPA4mgin
30–5
0mlnorm
alsalineinstilledbychesttube;
medianonedose/patient
(range
1–3
doses/patient)
1hr
Totalpleuralfluid
drainage,
median
(range):
Early
tPA:638ml(164–2
700ml)
LatetPA:691ml(285–7
944ml)
Control:306ml(0–2
041ml)
(p<0.05,late
tPAvs
control)
Pleuralfluid
drainagerate,median
(range):
Early
tPA:7ml/hr(2–2
9ml/hr)
LatetPA:4ml/hr(1–1
9ml/hr)
Control:3ml/hr(0–2
7ml/hr)
(p<0.01,earlytPAvs
control)
Durationofchesttube,
median
(range)
Early
tPA:84hrs
(45–1
87hrs)
LatetPA:209hrs
(87–5
28hrs)
Control:130hrs
(29–6
13hrs)
(p<0.01,earlytPAvs
late
tPA)
Nonereported
Comparative
case
series
34
71patients
aged
6mo–1
8.8
yrswith
empyemaorparapneumonic
effusion
anddecreased
thoracostomytube
outputduringan
8–2
4hrperiod:
patients
received
either
urokinase
(n=26[1995–1
998])
aortPA
(n=45[1998–2
002])
DosesofurokinaseandtPAwere
dilutedin
25–1
00mlnorm
alsalinebased
onpatientage
andsize:urokinase
25,000–1
00,000IU
(1000IU
/ml)
ortPA0.1
mg/kg;
doseswere
givenonce/day
(maxim
um
of
6doses)
untildrainage<
40ml/day
1hr
70/71patients
achievedresolution
withoutthoracicsurgery(99%
successrate):tPA98%
successrate,
urokinase100%
successrate;
decreased
pleuralthickness:70/71
patients
(99%
successrate);
decreased
lungopacification:65/71
(92%
successrate);tPAshowed
superioreffectsfordecreases
inpleuralthickness(p=0.004),lung
opacification(p=0.04),andchest
tubeoutput(p=0.001)vs
urokinase
Nosystem
icadverseeffects
noted;mildpain
ordiscomfort
(4patients);
severe
painin
1patienttreated
withtPA;minor
bleedingin
pleural
drainage
(4patients)
(continued)
526 PHARMACOTHERAPY Volume 34, Number 5, 2014

Table
2.(continued)
Publication
Typ
ePatientPopulation
tPADose,Preparation,Frequency,
andDuration
Dwell
Tim
eOutcomeMeasuresandResults
AdverseEvents
Case
series
14,33
58childrenaged
7mo–1
7yrs(m
ean
age4.8
yrs)
withcomplicated
parapneumonic
effusion
tPA0.1
mg/kg(m
axim
um
3mg)
in10–3
0mlnorm
alsaline
administeredintrapleurallyevery
8hrs
for3–4
daysuntilchesttube
drainage<25ml/12-hrperiod
(mean10doses/patient)
45–6
0min
Resolutionofeffusionin
54of58
patients;no30-day
recurrences,
nodeaths
Average
dropin
hem
oglobin
level
of2.5
g/dl
Case
series
32
6childrenaged
2–1
3yrs(w
eigh
t11.6–4
9kg)
withem
pyemaor
pleuraleffusionanddecreased
chesttubeoutputandfluid
seen
onCXR
tPA2–5
mgin
norm
alsalineevery
12–2
4hrs
untilresolutionseen
on
CXRoruntilvolumeinstilled
equaled
volumedrained
(average
3–6
doses/patient);patients
were
repositioned
4times
4–6
hrs
Chesttubedrainage6hrs
before
tPAvs
6hrs
aftertPA:mean�
SD22.5
�18.4
mlvs
141.7
�28.3
ml
(p<0.0001);5of6patients
were
afebrile
aftertreatm
ent;surgical
interventionavoided
inallpatients
Sangu
ineous
drainage(nodrop
inhem
atocrit),
decreased
serum
albumin
level,
edem
a,ascites
Case
report31
16-m
o-old,10.3-kgfemalepatient
withlargeparapneumonic
effusion
secondaryto
pneumonia
and
decreased
chesttubedrainage
andpersistentclinical
symptoms
despiteconservativemanagem
ent
tPA2mginstilledbychesttube
directlyinto
pleuralspace9
4dosesover6days
4hrs
Increasedchesttubedrainage,
resolutionofeffusiononCTscan
andCXR,resolutionofclinical
sign
sandsymptoms
Mildpain,relieved
byacetam
inophen
Case
report8
6-yr-old,19.9-kgboywithpleural
effusionsecondaryto
pneumococcal
pneumonia
andpoorchesttube
drainageandpersistentclinical
symptoms
tPA5mgin
50mlnorm
alsaline
every8hrs
92doses
1hr
Increasedchesttubedrainage,
resolutiononCXR,resolutionof
clinical
sign
sandsymptoms
Nonereported
aUrokinasewas
taken
offtheU.S.market
in1999.
tPA=tissueplasm
inogenactivator;CXR=chestradiograph;SD
=standarddeviation;CT=computedtomography
Intrapleural tPA in Pediatric Patients Israel and Blackmer 527

at 30-minute intervals into the Trendelenburg,reverse Trendelenburg, and left and right lateraldecubitus positions. The primary end point ofthe difference in pleural fluid drainage beforetPA (mean � SD 22.5 � 18.4 ml) versus aftertPA (141.7 � 28.3 ml) administration was signif-icant (p<0.0001). Further, five of the six patientsachieved effusion resolution.A larger retrospective case series of 58 chil-
dren with complicated parapneumonic effusion,confirmed results of earlier case reports.33 Chil-dren aged 7 months–17 years were treated withweight-based dosing of tPA: 0.1 mg/kg/dosemixed in 10–30 ml of normal saline (maximumdose of 3 mg). The dwell time ranged from 45–60 minutes, repeated every 8 hours for 3–4 days, until chest tube drainage was less than25 ml/12-hour period. The mean number ofdoses/patient was 10. Of the 58 patients evalu-ated, 54 achieved resolution, and there were no30-day recurrences and no deaths reported. Ofthe four patients who failed tPA therapy, threeunderwent the VATS procedure, and one patienthad open thoracotomy with decortication anddebridement. In a second large case series, 71children, aged 6 months–18.8 years, with empy-ema or parapneumonic effusion and decreasedchest tube output and pleural thickening seenon CXR were evaluated.34 This retrospectivecase series was completed between 1995 and2002. As urokinase was still on the U.S. marketfrom 1995–1998, patients received either uroki-nase 25,000–100,000 IU (26 patients) or tPA0.1 mg/kg diluted in 25–100 ml of normal saline(45 patients), depending on patient age and size.Doses were administered once/day and repeatedeach day until chest tube output was lessthan 40 ml/day, with a maximum of six doses.Efficacy was demonstrated in both groups, with70 of 71 patients achieving resolution of effusionwithout the need for invasive surgical interven-tion (99% success rate). Similarly, a decrease inpleural thickness was observed in 70 of 71patients and a decrease in lung opacificationswas observed in 65 of 71 patients (92% successrate). When compared with urokinase, tPAshowed superior effects for decrease in pleuralthickness (p=0.004), lung opacification(p=0.04), and chest tube output (p=0.001).
Timing of tPA Initiation
A large, retrospective cohort study evaluated53 children with complicated pleural effusion:30 children were treated with tPA, and 23 chil-
dren were managed by tube thoracostomy alone(control group).35 The study further evaluatedthe impact of the timing of tPA initiation bysubdividing the treatment group into twogroups: early tPA treatment (< 24 hrs after diag-nosis [12 patients]) and late tPA treatment(> 24 hrs after diagnosis [18 patients]). Patientsranged in age from 3 months–17 years old. In-trapleural tPA was dosed at 4 mg diluted in 30–50 ml of normal saline and allowed to dwell for1 hour; the median number of doses/patient wasone (range of 1–3 doses/patient). The total med-ian pleural fluid drainage was 691 ml (range285–7944 ml) in the late tPA group versus360 ml (range 0–2041) in the control group(p<0.05); however, a significant difference wasnot demonstrated between the early versus lategroups. The difference in the rate of pleuralfluid drainage between the early tPA group(7 ml/hr [range 2–29 ml/hr]) versus the controlgroup (3 ml/hr [range 0–27 ml/hr], p<0.01) wassignificant, and the difference in the duration ofchest tube placement between the early tPAgroup (84 hrs [range 45–187 hrs]) versus thelate group (209 hrs [range 87–528 hrs], p<0.01)was significant. No surgical interventions wererequired for those patients treated with tPA.
Comparison of Treatment Options
The efficacy of tPA for parapneumonic effu-sion and the timing of tPA initiation weredescribed above; however, questions remainregarding the comparative effects of tPA versusother treatment options. A retrospective studyevaluated 54 children with pleural effusion tomake this comparison.36 In this study, patientswere divided into four groups: chest tube alone(18 patients); chest tube with fibrinolytics (24patients); chest tube, fibrinolytics, and surgery(5 patients); and surgery alone (6 patients).Children treated with intrapleural tPA weregiven 2 mg diluted in 20 ml of saline every12 hours for 48–72 hours, with a dwell time of1 hour. Outcome variables included hospitallength of stay, duration of intensive care unitstay, duration of leukocytosis, days from ulti-mate therapy (i.e., the number of days from thelast required therapy [e.g., chest tube monother-apy, chest tube plus fibrinolytic, or surgery]until discharge), and average hospital charges.Patients who received surgery had a longerhospital length of stay (p=0.002), longer inten-sive care unit stay (p=0.01), and more days fromtherapy to discharge (p=0.044). In addition,
528 PHARMACOTHERAPY Volume 34, Number 5, 2014

hospital charges were lower in those patientswho did not receive surgery.
Prospective Data
To our knowledge, only one prospective, ran-domized trial has evaluated intrapleural tPA inpediatric patients.37 In this trial, fibrinolysis withtPA was compared with VATS as initial treatmentin pediatric patients (< 18 yrs of age) with empy-ema. Thirty-six patients with empyema diag-nosed by CT or ultrasound or who had purulentdrainage with a white blood cell countabove 10 9 103/ll were randomly assigned toundergo VATS (n=18) or to receive intrapleuraltPA therapy (18 patients). All patients were trea-ted with similar and appropriate antibiotic regi-mens. Patients were excluded if they hadcontraindications to thoracoscopy or fibrinolysis,any additional foci of infection, immunocompro-mised state, or comorbid conditions requiringhospitalization beyond empyema treatment. Chil-dren who received tPA had 12-French chesttubes in place. At the time of chest tube place-ment, tPA 4 mg mixed in 40 ml of normal salinewas instilled directly into the tube, with a dwelltime of 1 hour. Treatment was repeated every24 hours for a total of three doses. The primaryoutcome measures were hospital length of stay,posttherapy days of oxygen therapy, days untilafebrile, number of analgesic doses, requirementsfor a second procedure, and total hospital cost.Baseline demographic data were well matched
in each group. Organisms cultured from bothgroups were consistent with the typical patho-gens associated with pleural effusion. Outcomemeasures were similar in the VATS versus fibri-nolysis groups for hospital length of stay afterintervention (mean � SD 6.9 � 3.7 vs6.8 � 2.9 days, p=0.96), posttherapy days ofoxygen (2.3 � 1.7 vs 2.3 � 2.1 days, p=0.9),days until afebrile after intervention (3.1 � 2.7vs 3.8 � 2.9 days, p=0.46), and number of anal-gesic doses (22.3 � 28.5 vs 21.4 � 12, p=0.9).Two patients in the VATS group required ongo-ing mechanical ventilation, and 3 (16.6%) of the18 patients treated with fibrinolysis requiredVATS therapy for definitive treatment. Althoughthe clinical end points were not significantly dif-ferent between groups in this study, a significantdifference in overall hospital charges wasobserved between the two groups:$11,700 � 2900 versus $7600 � 5400 in theVATS versus fibrinolysis groups (p=0.02). Thus,it may be concluded that initial treatment with
intrapleural tPA is a reasonable alternative to aninitial VATS procedure and is associated with alower total hospital cost.
Safety
Intrapleural tPA is generally well toleratedand associated with only minor adverseeffects.31–35 Early case reports and case seriesnoted mild discomfort, which was relieved byanalgesics.31 One patient was reported to experi-ence a drop in serum albumin level, with edemaand ascites; however, this was most likely sec-ondary to significant chest tube drainage.32
Sanguineous drainage without an associateddrop in hematocrit, although reported,32 wasbelieved to be secondary to initial chest tubeplacement rather than tPA treatment itself. Anaverage drop in hemoglobin of 2.5 g/dl was alsoobserved in one case series,33 and minor bleed-ing into the pleural fluid has been described.34
Conversely, several reports noted no increasedrisk for bleeding.8, 31, 35, 36 Frank bleeding wasdescribed in a recent case report of a previouslyhealthy 6-year-old boy treated with tPA 3 mg in30 ml of normal saline (0.1 mg/kg) for pleuraleffusion.38 The patient developed clinical signsand symptoms of blood loss (tachypnea, weak-ness, and pallor); however, his neurologic statusremained intact, and no other signs of bleedingwere apparent. The patient’s hemoglobin leveldropped from 12.1 g/dl to 7.6 g/dl, and an infu-sion of packed red blood cells was required. Inlight of this case report as well as conflictingsafety outcomes reported in the literature,patients should be closely monitored for changesin hematocrit and hemoglobin and for clinicalsigns and symptoms of bleeding during therapy.Few absolute contraindications for use of tPA
exist. Potential contraindications include risk forbleeding, such as trauma, surgery, or recentmajor hemorrhage, or an allergy or hypersensi-tivity to tPA.12, 14 Coagulopathy may also beconsidered to be a relative contraindication totPA; however, therapy may be considered if thecoagulopathy is mild and correctable.5, 33
Remaining Questions and Future Directions
Data for tPA in pediatrics are primarily retro-spective, with only one randomized, prospectivetrial currently published.37 Nevertheless, evi-dence supports the use of tPA as a first-lineoption in pediatric patients for the managementof complex pleural effusions.9, 13 However,
Intrapleural tPA in Pediatric Patients Israel and Blackmer 529

despite a growing body of literature and gains inclinical experience with this therapy, there areseveral questions that remain unanswered todate: timing of initiation of therapy, optimaldosing, frequency of doses, duration of therapy,dwell time, the need for positioning changes,and optimal therapeutic end points. In addition,although supported in the adult literature, theefficacy and safety of combination therapy withdornase alfa in pediatric patients has not yetbeen established.Researchers evaluated the timing of adminis-
tration of tPA and found that patients treatedwith early intervention, defined by interventionwithin 24 hours of diagnosis, experienced ashorter duration of chest tube placement.35
Although the clinical impact of this should befurther studied, the ability to remove chest tubesearlier may improve patient comfort and patientmobility, and decrease analgesic dosing. Further,cost and duration of hospital stay may be less-ened. Strong conclusions, however, cannot yetbe made with respect to optimal timing due todata limited to retrospective evaluations.The optimal dosing of tPA for pleural effusion
in pediatric patients is also debatable based onthe supporting literature. Due to heterogeneityamong the studies, the optimal dose of tPA isunknown. Although some studies used fixeddoses across age groups, others investigated a
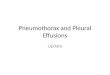
weight-based (0.1 mg/kg) approach.9, 31–37 Therecent 2012 APSA publication suggests a fixeddose of 4 mg based on the available prospectivedata.9, 37 However, an alternative suggestedweight-based dosing algorithm for tPA, con-structed on extrapolation of the current data, isdisplayed in Figure 1. This approach has beenused anecdotally with success at our institutionbut has not been validated or vigorously studiedin a controlled manner. A prospective trial evalu-ating the safety and efficacy of this approach iswarranted. Of note, the youngest patientreported in the literature to receive intrapleuraltPA was 3 months, and the patient with the low-est weight reported was 5 kg. Therefore, it issuggested that therapy be reserved for patientsolder than 3 months of age and above 5 kg inweight. The frequency of dosing, optimal dura-tion of therapy, and dwell time are also yet unde-termined due to variability in study design andpublished reports. However, the strongest evi-dence supports three doses given 24 hours apart,with a dwell time of 1 hour.37 Because the intra-pleural pharmacokinetics of tPA are unknown,predicting the optimal parameters for therapy isdifficult, and further studies are warranted.Furthermore, the majority of the published
data for intrapleural tPA in pediatric patientsreferences a dilution of 0.1 mg/ml; this dilutionis also suggested in Figure 1 and has been used
Complicated ParapneumonicEffusion
pH <7.2Loculations on US/CTAspiration of pusPositive gram stain>10,000 WBC/µL
Surgical vs. Fibrinolytic Management?
Surgical
VATSOpen thoracotomy
Fibrinolytic
tPA x 3 total doses (every 24 hours)Dwell time: 1 hour
5-10 kg: 1 mg in 10 mL NS10-20 kg: 2 mg in 20 mL NS20-30 kg: 3 mg in 30 mL NS
>30 kg: 4 mg in 40 mL NS
No clinical improvement withresidual pleural effusion on US or CT
Clinical improvement with clearance of pleural effusion on US or CT
Surgical Management (VATS or open thoracotomy)
Continue Antibiotics
Figure 1. Proposed algorithm using weight-based dosing of tissue plasminogen activator for treatment of pleural effusion inpediatric patients. tPA = tissue plasminogen activator; US/CT = ultrasound or computed tomography; VATS = video-assistedthoracoscopic surgery; WBC = white blood cell; NS = normal saline.
530 PHARMACOTHERAPY Volume 34, Number 5, 2014

with success at our institution. However, manu-facturer recommendations for dilution, based onintravenous administration, note a final concen-tration of 1 mg/ml, which may be diluted furtherimmediately before administration to a concen-tration of 0.5 mg/ml with either dextrose 5% inwater or normal saline.21 These solutions arestable at room temperature up to 8 hours. Alter-native dilutions of tPA have been evaluated invitro; however, the effects of these dilutions havenot been evaluated clinically. In vitro data indi-cate that a tPA concentration of 0.01 mg/ml innormal saline is stable for up to 24 hours atroom temperature.39 In that study, proteinrecovery was less than 50%; but, biologic activ-ity of the proteins recovered was preserved.Additional personal communication with Gen-entech (Caroline Smith, Pharm.D., MedicalCommunications Department, personal commu-nication, March 20, 2011) suggests that tPAremains physically and chemically stable in nor-mal saline at 0.2 mg/ml. However, diluting tPAto concentrations less than 0.2 mg/ml in normalsaline, less than 0.5 mg/ml in dextrose 5% inwater, or diluting with other base solutions hasreportedly resulted in protein precipitation.40
Although alternative dilutions are reported inthe clinical data, most commonly 0.1 mg/ml,further studies to confirm retained protein activ-ity and stability at the concentration of 0.1 mg/ml are warranted.The optimal therapeutic end point of intraple-
ural tPA has not been elucidated, as the pub-lished literature is variable with respect toclinical end points. Several end points have beenevaluated including change in pleural opacityseen on CXR, improved chest tube drainage, res-olution of signs and symptoms, or resolution seenon ultrasound or CT. Determination of the opti-mal outcome should be a focus of future studies.Furthermore, recent adult data support the
use of intrapleural combination therapy, tPAplus dornase alfa, for initial management ofparapneumonic effusion. However, the safetyand efficacy of this approach has not been inves-tigated in pediatric patients. Before consistentlyimplementing dual intrapleural therapy in chil-dren, supporting data must become available,providing opportunities for future research.
Conclusion
Empyema and parapneumonic effusion are sig-nificant complications of pediatric pneumonia.Despite the overall decline in pneumonia rates in
children, these conditions can significantlyincrease morbidity and mortality. Inadequate ordelayed treatment may lead to progressive illness;therefore, identifying the optimal treatment inaffected children is critical. Identifying patientswho will not benefit from fibrinolytic treatmentis difficult; however, surgical procedures canlikely be reserved for patients who fail fibrinoly-sis. Although surgical treatments such as VATSand open thoracotomy are effective, they carryincreased risk compared with chest tube drainagewith or without fibrinolysis. Fibrinolytic agentssuch as tPA can help degrade loculations and dis-solve fibrin deposits to facilitate drainage ofpurulent pleural fluid. Further large, random-ized, prospective trials should be performed inorder to answer some of the existing ongoingquestions that remain regarding tPA therapy inpediatric patients with pleural effusion; however,sufficient data exist that support the use of tPAin these patients, with demonstrated efficacy andminimal safety concerns.
References
1. Hamm H, Light RW. Parapneumonic effusion and empyema.Eur Res J 1997;10:1150–6.
2. Light RW. Clinical practice. Pleural effusion. N Engl J Med2002;346:1971–7.
3. Balfour-Lynn IM, Abrahamson E, Cohen G, et al. BTS guide-lines for the management of pleural infection in children. Tho-rax 2005;60(Suppl 1):i1–21.
4. Jaff�e A, Balfour-Lynn IM. Management of empyema in chil-dren. Pediatr Pulmonol 2005;40:148–56.
5. Colice GL, Curtis A, Deslauriers J, et al. Medical and surgicaltreatment of parapneumonic effusions: an evidence-basedguideline. Chest 2000;18:1158–71.
6. Carter E, Waldhausen J, Zhang W, Hoffman L, Redding G.Management of children with empyema: pleural drainage isnot always necessary. Pediatr Pulmonol 2010;45:475–80.
7. Grijalva CG, Nuorti JP, Zhu Y, Griffin MR. Increasing inci-dence of empyema complicating childhood community-acquired pneumonia in the United States. Clin Infect Dis2010;50:805–13.
8. Stevens A, Tobias JD. Tissue plasminogen activator as adjunc-tive therapy of empyema in a child. J Intensive Care Med2001;16:287–9.
9. Islam S, Calkins CM, Goldin AB, et al. The diagnosis andmanagement of empyema in children: a comprehensive reviewfrom the APSA Outcomes and Clinical Trials Committee.J Pediatr Surg 2012;47:2101–10.
10. Sahn SA. Diagnosis and management of parapneumonic effu-sions and empyema. Clin Infect Dis 2007;45:1480–6.
11. Light RW. Parapneumonic effusions and empyema. Proc AmThorac Soc 2006;3:75–80.
12. Hamblin SE, Furmanek DL. Intrapleural tissue plasminogenactivator for the treatment of parapneumonic effusion. Phar-macotherapy 2010;30:855–62.
13. Bradley JS, Byington CL, Shah SS, et al. Executive summary:the management of community-acquired pneumonia in infantsand children older than 3 months of age: clinical practiceguidelines by the Pediatric Infectious Diseases Society and theInfectious Diseases Society of America. Clin Infect Dis2011;53:617–30.
Intrapleural tPA in Pediatric Patients Israel and Blackmer 531

14. Hawkins JA, Scaife ES, Hillman ND, Feola GP. Current treat-ment of pediatric empyema. Semin Thorac Cardiovasc Surg2004;16:196–200.
15. Faber DL, Best LA, Orlovsky M, Lapidot M, Nir RR, KremerR. Streptokinase fibrinolysis protocol: the advantages of a non-operative treatment for stage II pediatric empyema patients. IsrMed Assoc J 2012;14:157–61.
16. Bouros D, Schiza S, Patsourakis G, Chalkiadakis G, PanagouP, Siafakas NM. Intrapleural streptokinase versus urokinase inthe treatment of complicated parapneumonic effusions: a pro-spective, double-blind study. Am J Respir Crit Care Med1997;155:291–5.
17. Stefanutti G, Ghirardo V, Barbato A, Gamba P. Evaluation ofa pediatric protocol of intrapleural urokinase for pleuralempyema: a prospective study. Surgery 2010;148:589–94.
18. Cochran JB, Tecklenburg FW, Turner RB. Intrapleural instil-lation of fibrinolytic agents for treatment of pleural empyema.Pediatr Crit Care Med 2003;4:39–43.
19. Bouros D, Tzouvelekis A, Antoniou KM, Heffner JE. Intraple-ural fibrinolytic therapy for pleural infection. Pulm PharmacolTher 2007;20:616–26.
20. Abbott Laboratories. Abbokinase (urokinase) package insert.North Chicago, IL; 2002.
21. Genentech, Inc. Activase (alteplase) package insert. San Fran-cisco, CA; 2011.
22. Genentech, Inc. Cathflo activase (alteplase) package insert.San Francisco, CA; 2010.
23. Micromedex. 2.0 [intranet database] 2013 Truven Health Ana-lytics Inc. Alteplase, Recombinant. Available from http://www.micromedexsolutions.com. Accessed July 8, 2013.
24. Gervais D, Levis D, Hahn P, Uppot RN, Arellano RS, MuellerPR. Adjunctive Intrapleural tissue plasminogen activatoradministered via chest tubes placed with imaging guidance:effectiveness and risk for hemorrhage. Radiology 2008;246:956–63.
25. Levinson GM, Pennington DW. Intrapleural fibrinolytics com-bined with image-guided chest tube drainage for pleural infec-tion. Mayo Clin Proc 2007;82:407–13.
26. Skeete DA, Rutherford EJ, Schlidt SA, Abrams JE, Parker LA,Rich PB. Intrapleural tissue plasminogen activator for compli-cated pleural effusions. J Trauma 2004;57:1178–83.
27. Thommi G, Shehan JC, Robison KL, Christensen M,Backemeyer LA, McLeay MT. A double blind randomizedcross over trial comparing rate of decortication and efficacy of
intrapleural instillation of alteplase vs. placebo in patients withempyemas and complicated parapneumonic effusions. RespirMed 2012;106:716–23.
28. Thommi G, Nair CK, Aronow WS, Shehan C, Meyers P,McLeay M. Efficacy and safety of intrapleural instillation ofalteplase in the management of complicated pleural effusion orempyema. Am J Ther 2007;14:341–5.
29. Rahman NM, Maskell NA, West A, et al. Intrapleural use oftissue plasminogen activator and DNase in pleural infection. NEngl J Med 2011;365:518–26.
30. Walker CA, Shirk MB, Tschampel MM, Visconti JA. Intraple-ural alteplase in a patient with complicated pleural effusion.Ann Pharmacother 2003;37:376–9.
31. Bishop NB, Pon S, Ushay HM, Greenwald BM. Alteplase inthe treatment of complicated parapneumonic effusion: a casereport. Pediatrics 2003;111:e188–90.
32. Ray TL, Berkenbosch JW, Russo P, Tobias JD. Tissue plas-minogen activator as an adjuvant therapy for pleural empyemain pediatric patients. J Intensive Care Med 2004;19:44–50.
33. Feola GP, Shaw LC, Coburn L. Management of complicatedparapneumonic effusions in children. Tech Vasc Interv Radiol2003;6:197–204.
34. Wells RG, Havens PL. Intrapleural fibrinolysis for parapneu-monic effusion and empyema in children. Radiology2003;228:370–8.
35. Weinstein M, Restrepo R, Chait PG, Connolly B, Temple M,Macarthur C. Effectiveness and safety of tissue plasminogenactivator in the management of complicated parapneumoniceffusions. Pediatrics 2004;113(3 Pt 1):e182–5.
36. Gates RL, Hogan M, Weinstein S, Arca MJ. Drainage, fibrino-lytics, or surgery: a comparison of treatment options in pediat-ric empyema. J Pediatr Surg 2004;39:1638–42.
37. St Peter SD, Tsao K, Spilde TL, et al. Thoracoscopic decorti-cation vs. tube thoracostomy with fibrinolysis for empyema inchildren: a prospective, randomized trial. J Pediatr Surg2009;44:106–11; discussion 111.
38. Hendaus MA, Abushahin A. Intrapleural hemorrhage due toalteplase use in a 6-year-old boy with pleural effusion. Int JGen Med 2013;6:233–6.
39. Semba C, Weck S, Patapoff T. Alteplase: stability and bioac-tivity after dilution in normal saline solution. J Vasc IntervRadiol 2003;14:99–102.
40. Frazin BS, Magnuson D. Maximal dilution of activase. Am JHosp Pharm 1990;47:1016.
532 PHARMACOTHERAPY Volume 34, Number 5, 2014