Embed Size (px)
Citation preview

918
Timing weight-control measures in obesechildren
SIR,-Mossberg’s 40-year follow-up study has provided veryuseful confirmation and precision on the prognosis of childhoodobesity,1 and we share most of his conclusions. However, we wouldqualify his recommendation that weight-reducing measures bestarted early in life to improve the long-term prognosis of very obesechildren.Our two-decade follow-up (from birth to 21 years) yielded
similar results: 41 % of children fat at 1 year were still fat inadulthood2 and at all ages (early childhood,3 pre-adolescence,4 4
adulthood 5) one can be obese without being hyperphagic. Mossbergassessed overweight by weight-for-height standard deviation
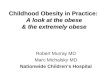
scores; we used the body mass index (BMI) which faithfullyreflects the development of adiposity.’ Using this index we havetraced the onset of persisting obesity, sometimes from an age whenthe obese-to-be are still lean. BMI growth charts, like skinfoldthickness charts,’ display three phases--an increase in adiposityduring the first year of life, a decrease over several years, and anotherincrease (figure). This second increase phase ("adiposityrebound"8) begins at 6 years on average but onset can be earlier orlater. Age at adiposity rebound was critically correlated withadiposity in adulthood.2 Some fat infants stay fat after earlierrebound (eg, at 2 years in case 1 [figure]) and most fat childrenslim. down to average BMI after a later rebound (eg, 8 years incase 2). Early, transient obesity explains the lower correlationbetween BMI in adulthood and measurements done in the first
years of life.9These observations suggest that weight-reducing measures are
not reasonable very early in life. A reducing diet could even beharmful-by impairing height development or precipitating eatingdisorders-in children set to return spontaneously to normal BMIs.Nevertheless, obese children need special attention because theyhave twice the usual risk of being obese as adults.2 The obese child’sBMI curve should be monitored carefully. During the decreasingphase nutritional control of the child’s feeding should remain "soft"(eg, avoidance of overeating, limitation of fat intake, and non-
Examples of weight/height2 monitoring on BMI referencecharts in girls.
Case 1. fat at 1 year, remained fat after early rebound (2 years).Case 2 fat at 1 year, did not stay fat after a late rebound (8 years).Case 3: lean at 1 year, did not stay lean after an early rebound (45
years).Case 4: lean at 1 year, remained lean after late rebound (8 years).
encouargement of sweet things). If the BMI increases too earlymore dramatic weight control measures can be applied. Leanchildren can also become obese after an early rebound (4-5 years incase 3) and they should not be forced to catch up with average bodysize too rapidly since to do this carries the risk of surpassing thenorm.
Monitoring the BMI, on standard charts, permits earlydiscrimination of permanent from transient weight deviations andprovides useful information that should be taken into accountbefore weight-control measures in children are embarked upon.
INSERM Nutrition Section,Centre de Recherche du Vésinet,78110 Le Vésinet, France M. H. F. ROLLAND-CACHERA
CNRS Laboratory of Neurobiologyand Nutrition,
Pierre and Marie Curie University, Paris FRANCE BELLISLE
1. Mossberg H-O. 40-year follow-up of overweight children. Lancet 1989; ii: 491-93.2. Rolland-Cachera MF, Deheeger M, Avons P, Guilloud-Bataille M, Patois E, Sempe
M. Tracking adiposity patterns from 1 month to adulthood. Ann Hum Biol 1987;14: 219-22.
3. Rolland-Cachera MF, Bellisle F, Deheeger M, Péquignot F, Guilloud-Bataille M,Vinit F. Adiposity and food intake in young children: the environmental challengeto individual susceptibility. Br Med J 1988; 276: 1037-38.
4. Rolland-Cachera MF, Bellisle F. No correlation between adiposity and food intake:why are working class children fatter? Am J Clin Nutr 1986; 44: 779-87.
5. Rolland-Cachera MF, Bellisle F, Tichet J, et al. Relationship between adiposity andfood intake: an example of pseudocontradictory results obtained in case-controlversus between-populanons studies. Int J Epidemiol (in press).
6. Rolland-Cachera MF, Sempé M, Guilloud-Bataille M, Patois E, Péquignot-Guggenbuhl F, Fautrad V. Adiposity indices in children. Am J Clin Nutr 1982; 36:178-84.
7. Tanner JM, Whitehouse RH. Revised standard for triceps and subscaplular skinfoldsin British children. Arch Dis Child 1975; 50: 142-45.
8. Rolland-Cachera MF, Deheeger M, Bellisle F, Sempé M, Guilloud-Bataille M, PatoisE. Adiposity rebound in children: a simple indicator for predicting obesity. Am JClin Nutr 1984; 39: 129-35.
9. Rolland-Cachera MF, Bellisle F, Sempé M. The prediction in boys and girls of theweight/height2 index and various skinfolds measurements in adults: a two-decadefollow-up study. Int J Obesity 1989; 13: 305-11.
Dementia in a punch-drunk wife
SiR,—Repeated blows to the head of boxers sometimes culminate inthe "punch drunk syndrome" (dementia pugilistica),1-3 a conditioncharacterised by damage to the pyramidal, extrapyramidal, andcerebellar systems and by progression from affective disturbanceand memory loss, through psychosis, to progressive dementia.Damage to the septum, widespread formation of neurofibrillarytangles in the cortex, neuronal loss in the substantia nigra, andcerebellar scarring are found at necropsy 4 Large numbers of"diffuse" cortical plaques (p-protein-immunoreactive, non-
congophilic) have also been described.5 Immunologically the
proteins of the tangles and plaques in dementia pugilistica areidentical to those found in Alzheimer’s disease,5.6 suggesting thepossibility of a common pathogenesis.5-S The idea that head injuryacts as a trigger for an Alzheimer type process is controversial. Sucha link between head injury and dementia in former professionalboxers is firmly established but the possibility of a similar sequenceoutside the boxing ring is more difficult to establish.A 76-year-old woman was admitted to hospital unconscious after
being found at home with multiple injuries. She had rib fractures,multiple bruises and abrasions to the head, and signs of left-sidedweakness. She had a history of a stroke and had become dementedover the past few years, this manifesting predominantly as memoryloss and mental confusion. Relatives told us that her husband hadbeen violent towards her for many years, particularly in relation tohis drinking, and the patient had often been seen with cuts andbruises.
She died in hospital 10 months after admission and necropsyrevealed abnormal thickening of the ears, resembling the"cauliflower ears" of pugilists. The cause of death was
bronchopneumonia. The heart showed moderate coronary arteryatheroma with focal fibrosis of the myocardium. There wasevidence of old rib fractures. Examination of the brain revealed mild