Embed Size (px)
Citation preview

www.gimsi.it
Corso Avanzato GIMSI sulla Sincope
Il nuovo ruolo del tilt test
Michele BrignoleCentro Aritmologico &
Syncope Unit - Lavagna

Tilt table testing: limitations
• Too often negative in pts with likely VVS (“low sensitivity”)
• Too often positive in pts without VVS syncope (“low specificity”)
• No value in assessing efficacy of treatment with drugs or pacemaker
Someone stopped to perfom it (“clinical history better than tilt table testing”)
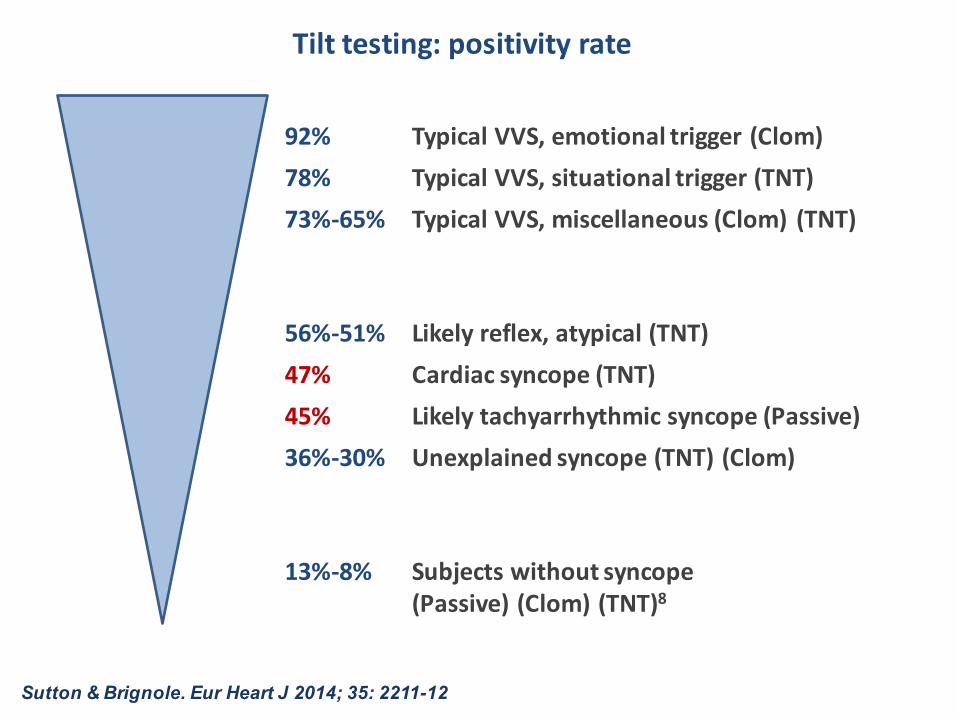
Tilttesting:positivityrate
92% Typical VVS,emotional trigger(Clom)78% Typical VVS, situational trigger(TNT)73%-65% Typical VVS,miscellaneous (Clom) (TNT)
56%-51% Likely reflex, atypical (TNT)47% Cardiac syncope (TNT)45% Likely tachyarrhythmic syncope (Passive)36%-30% Unexplained syncope (TNT) (Clom)
13%-8% Subjects withoutsyncope(Passive) (Clom) (TNT)8
Sutton & Brignole. Eur Heart J 2014; 35: 2211-12

A positive tilt test suggests the presence of a hypotensive susceptibility, which plays a role in causing syncope irrespective of the etiology and mechanism of syncope.
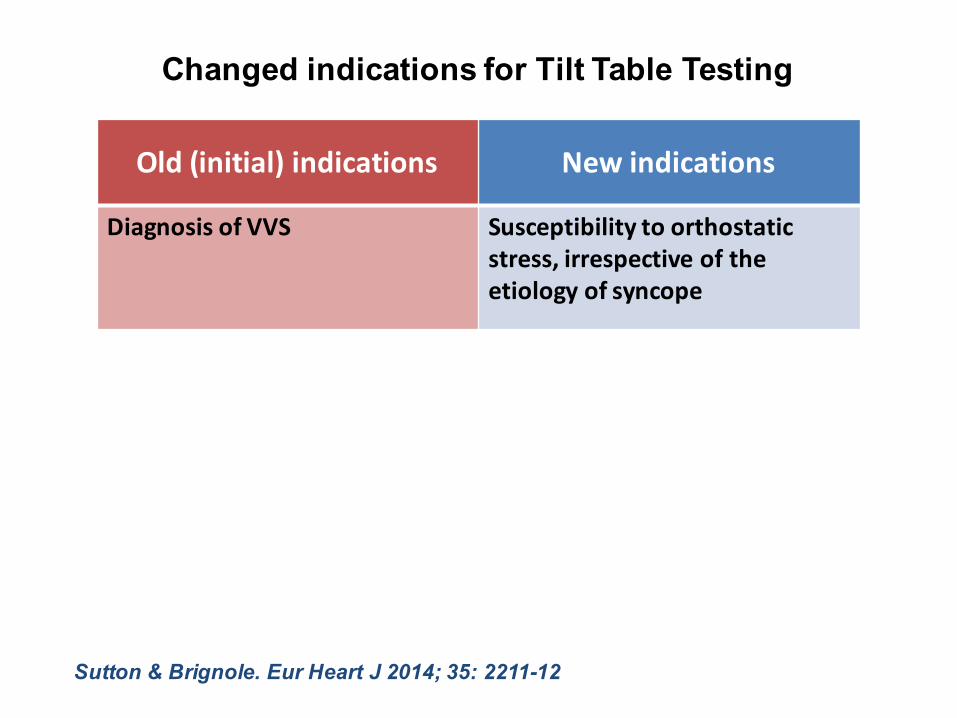
Changed indications for Tilt Table Testing
Old (initial)indications Newindications
Diagnosis of VVS Susceptibilityto orthostaticstress,irrespective of theetiology of syncope
Sutton & Brignole. Eur Heart J 2014; 35: 2211-12
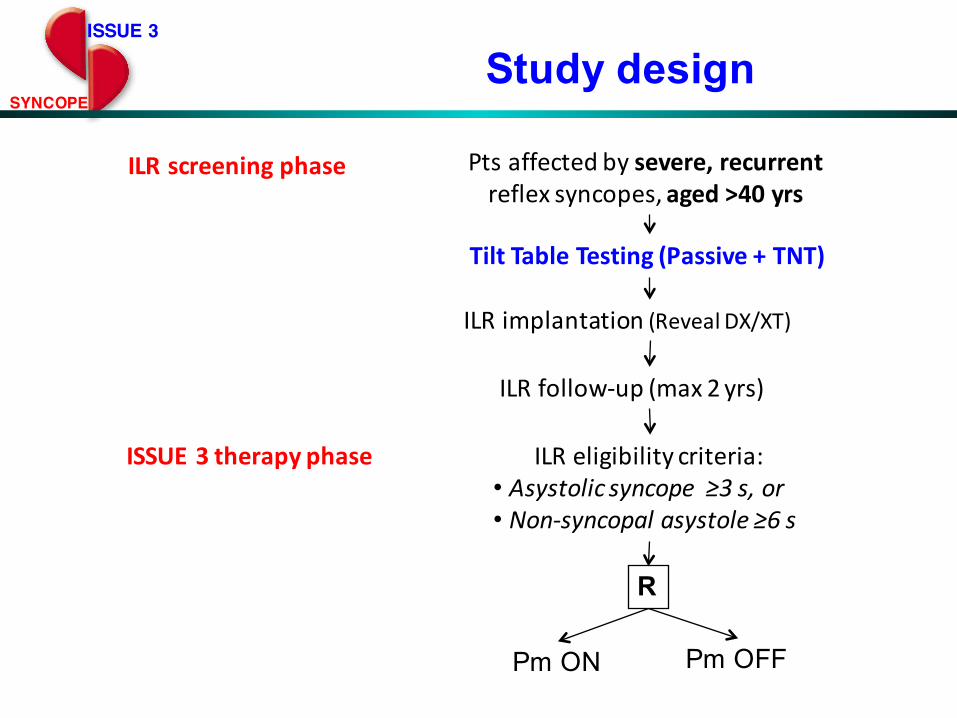
ISSUE 3
SYNCOPE
Ptsaffectedbysevere,recurrentreflexsyncopes,aged>40yrs
ILRimplantation(RevealDX/XT)
ILRfollow-up(max2yrs)
ILRscreeningphase
ISSUE3therapyphase
TiltTableTesting(Passive+TNT)
ILReligibilitycriteria:• Asystolic syncope≥3s,or• Non-syncopalasystole≥6s
R
Pm ON Pm OFF
Study design
0
.1
.2
.3
.4
.5
.6
.7
.8
.9
1
Free
dom
from
syn
copa
l rec
urre
nce
38 32 27 22 16 14 13 13 11Pm ON39 31 25 21 21 18 15 12 8Pm OFF
Number at risk
0 3 6 9 12 15 18 21 24Months
Kaplan-Meier survival estimates
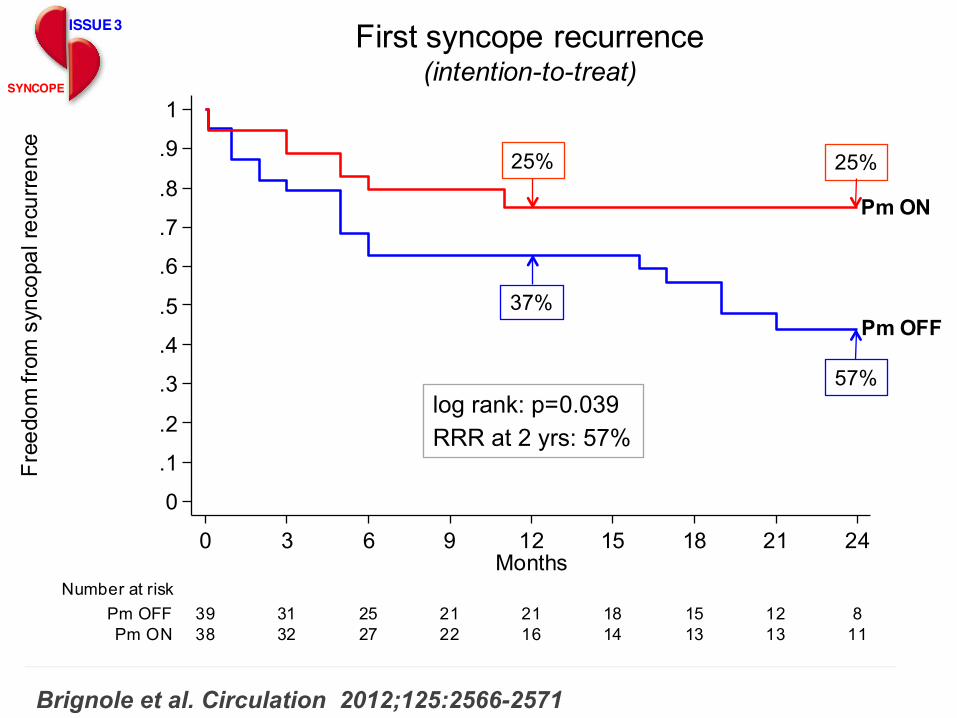
log rank: p=0.039RRR at 2 yrs: 57%
Pm ON
Pm OFF
First syncope recurrence(intention-to-treat)
ISSUE 3
SYNCOPE
25%
37%
25%
57%
Brignole et al. Circulation 2012;125:2566-2571
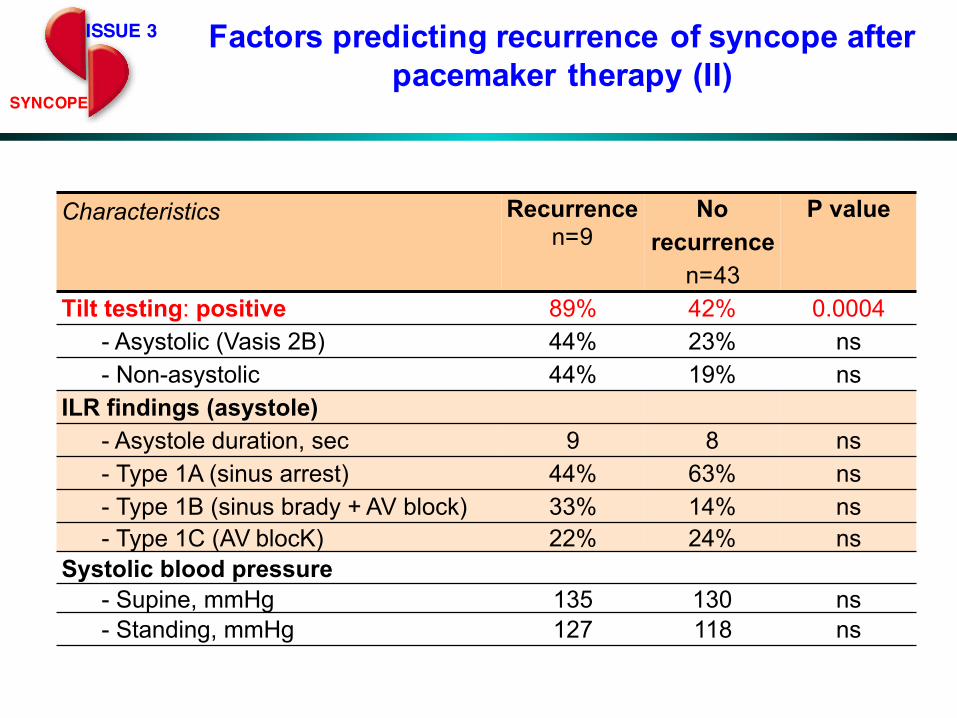
Characteristics Recurrencen=9
No recurrence
n=43
P value
Tilt testing: positive 89% 42% 0.0004- Asystolic (Vasis 2B) 44% 23% ns- Non-asystolic 44% 19% ns
ILR findings (asystole)- Asystole duration, sec 9 8 ns- Type 1A (sinus arrest) 44% 63% ns- Type 1B (sinus brady + AV block) 33% 14% ns- Type 1C (AV blocK) 22% 24% ns
Systolic blood pressure- Supine, mmHg 135 130 ns- Standing, mmHg 127 118 ns
ISSUE 3
SYNCOPE
Factors predicting recurrence of syncope after pacemaker therapy (II)
0.00
0.10
0.20
0.30
0.40
0.50
0.60
0.70
0.80
0.90
1.00
Free
dom
from
syn
copa
l rec
urre
nce
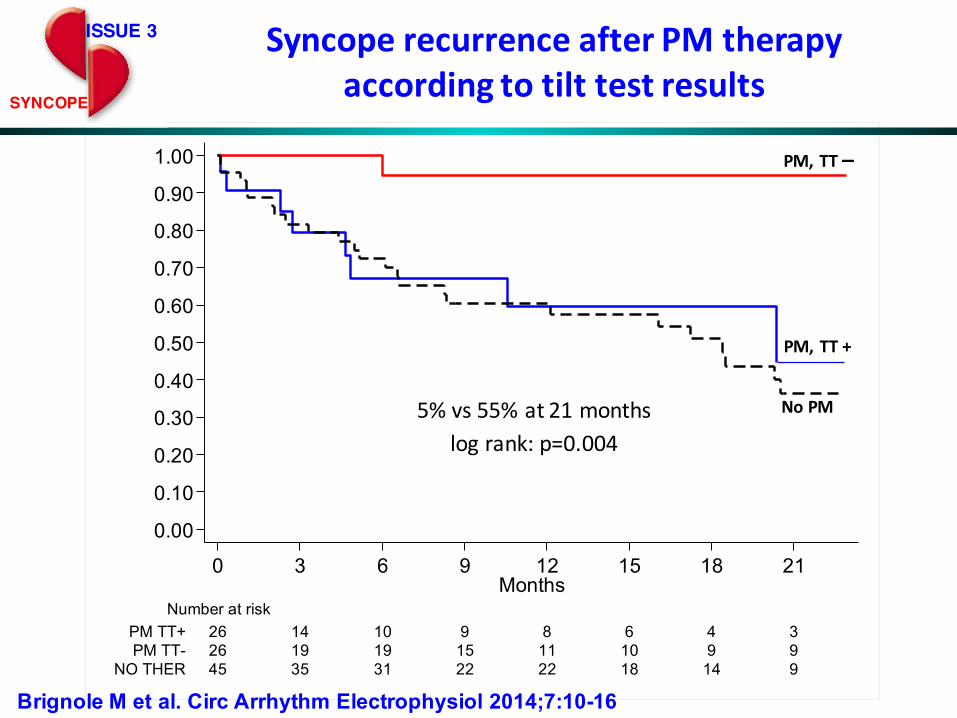
45 35 31 22 22 18 14 9NO THER26 19 19 15 11 10 9 9PM TT-26 14 10 9 8 6 4 3PM TT+
Number at risk
0 3 6 9 12 15 18 21Months
PM,TT+
PM,TT–
NoPM
ISSUE 3
SYNCOPE
SyncoperecurrenceafterPMtherapyaccordingtotilttestresults
5%vs55%at21monthslogrank:p=0.004
Brignole M et al. Circ Arrhythm Electrophysiol 2014;7:10-16
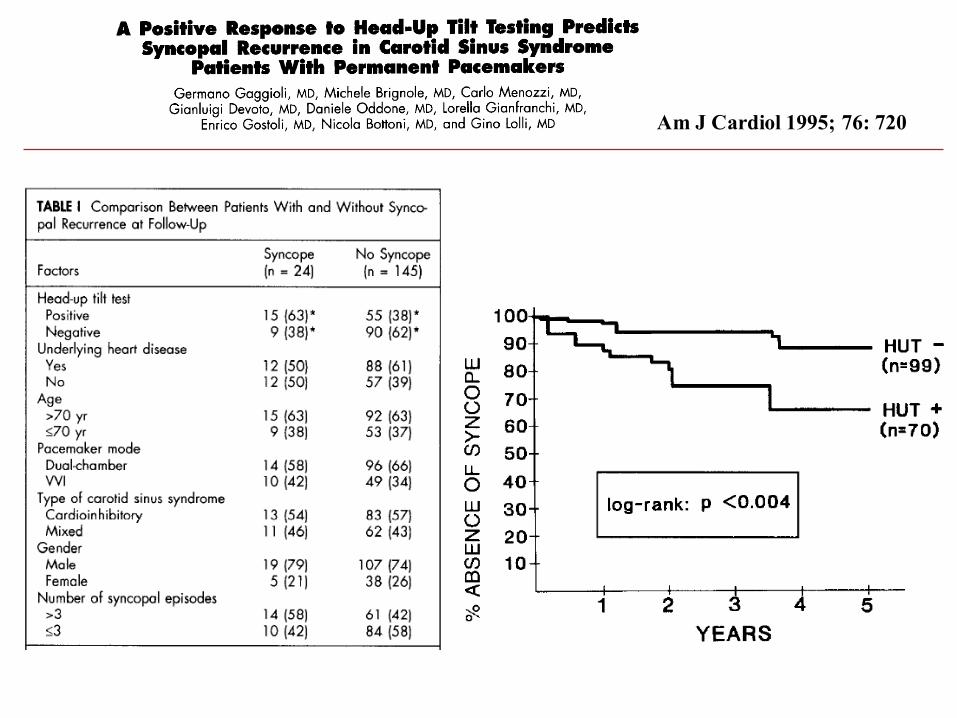
Am J Cardiol 1995; 76: 720

Non-CI forms
CI form
Negative or not performed
Recurrence of syncope according to tilt test results
Log rank: p=0.008
Solari D et al. Europace 2013

Pm, TT negative
Pm, TT Positive
No Pm, ILRLog rank for trend:p = 0.01
p = 0.03
p = n.s.
SyncopeUnitProject2(SUP2) SUP 2 study: 3-years extended follow-up
Europace 2016
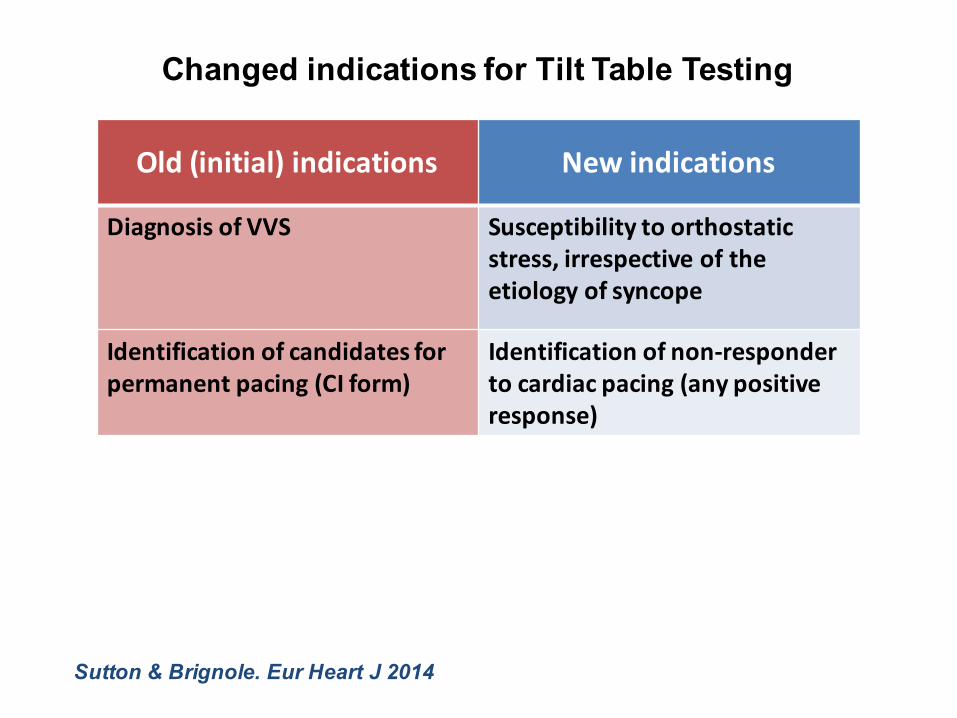
Changed indications for Tilt Table Testing
Old (initial)indications Newindications
Diagnosis of VVS Susceptibilityto orthostaticstress,irrespective of theetiology of syncope
Identification of candidates forpermanent pacing (CI form)
Identification of non-responderto cardiac pacing (any positiveresponse)
Sutton & Brignole. Eur Heart J 2014

Reflex syncope: Dual-action model
Hypotensive susceptibility
YES (Tilt +)Low reflex threshold
NO (Tilt -)High reflex threshold
Trigger(neuro and/or humoral)
Vasovagal syncope(hypotension-bradycardia)
Cardio-inhibitoryreflex syncope
+ +++
Hypotension phenotype domain(pacing low responder)
Bradycardia phenotype domain(pacing high-responder)
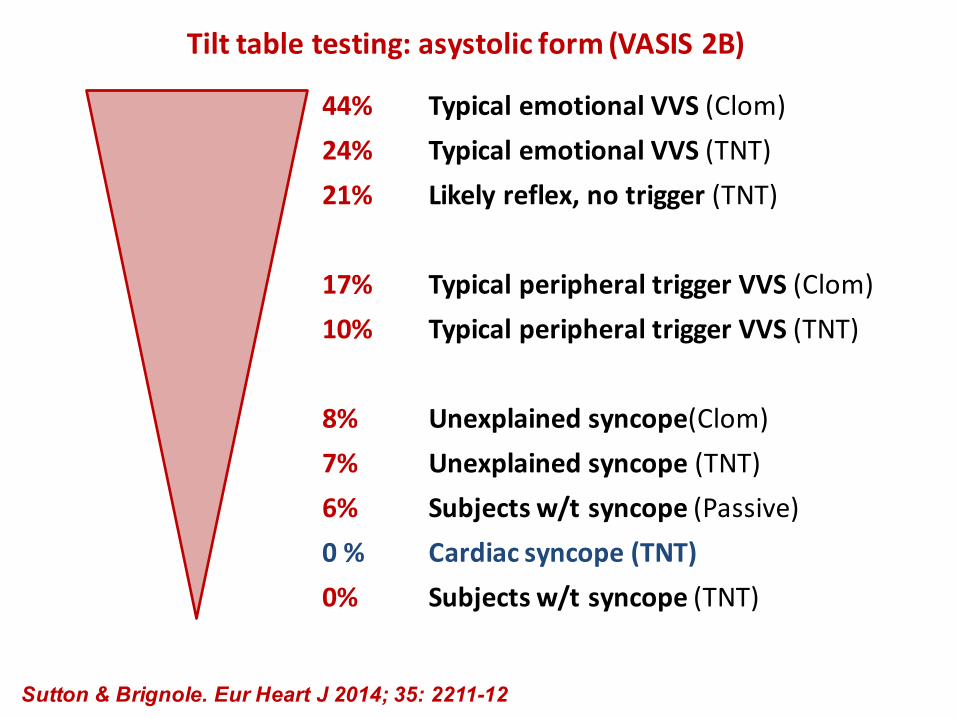
Tilttabletesting:asystolicform(VASIS2B)
44% Typical emotional VVS (Clom)24% Typical emotional VVS (TNT)21% Likely reflex,notrigger(TNT)
17% Typical peripheral triggerVVS(Clom)10% Typical peripheral triggerVVS(TNT)
8% Unexplained syncope(Clom)7% Unexplained syncope (TNT)6% Subjects w/tsyncope (Passive)0% Cardiac syncope (TNT)0% Subjects w/tsyncope (TNT)
Sutton & Brignole. Eur Heart J 2014; 35: 2211-12
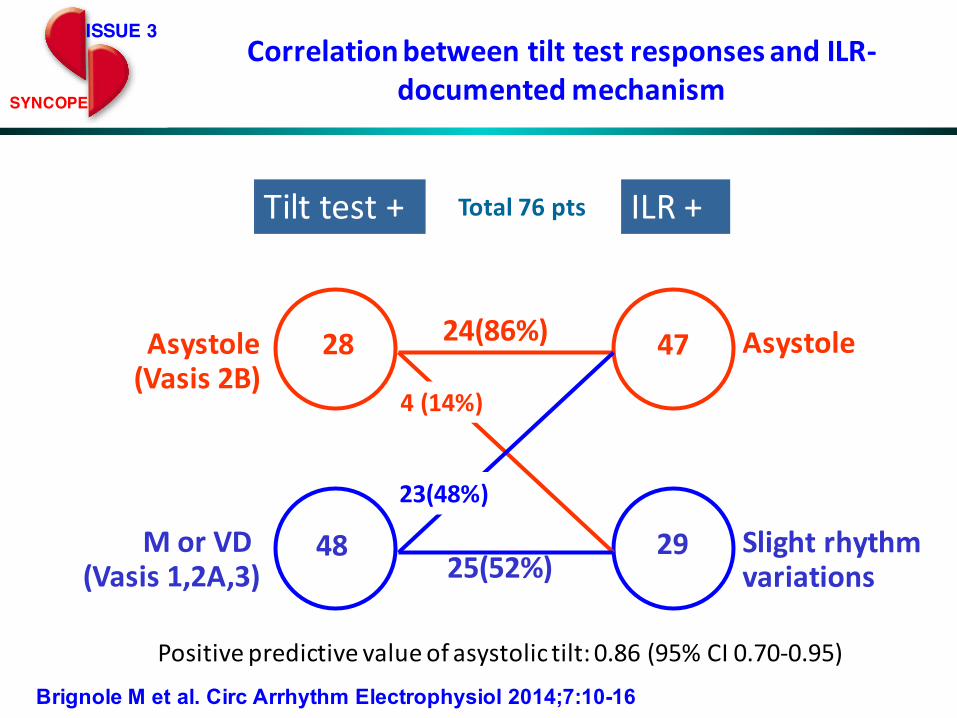
Tilttest+ ILR+
28
48
Asystole(Vasis2B)
MorVD(Vasis1,2A,3)
Asystole47
29 Slightrhythmvariations
24(86%)
4(14%)
23(48%)
25(52%)
Total76pts
Positivepredictive value of asystolictilt:0.86(95%CI 0.70-0.95)
ISSUE 3
SYNCOPE
CorrelationbetweentilttestresponsesandILR-documentedmechanism
Brignole M et al. Circ Arrhythm Electrophysiol 2014;7:10-16

Log rank for trend:p = 0.01
Pm-CSS
Pm-ILRPm-VASIS 2B
ILR
SyncopeUnitProject2(SUP2) SUP 2 study: 3-years extended follow-up
Europace 2016
18
Benefit of dual-chamber pacing with Closed Loop Stimulation (CLS) in tilt-induced cardio-inhibitory
reflex syncope.
A randomized double-blind parallel trial
BioSyncBioSync
M. Brignole (PI) - M. Tomaino (Co-PI)
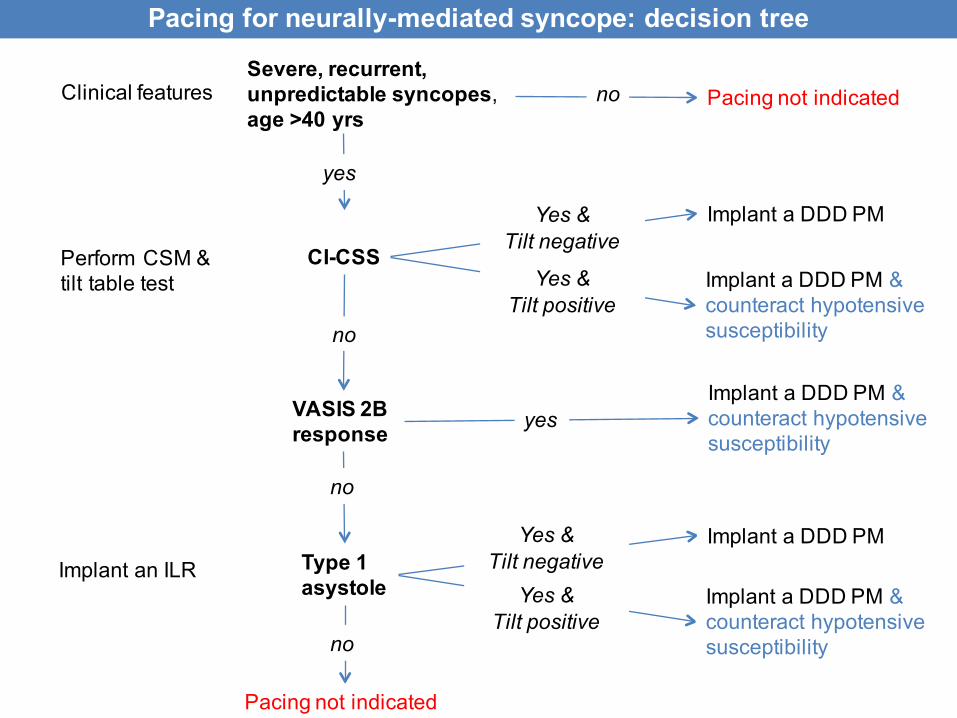
Perform CSM & tilt table test
CI-CSS
VASIS 2B response
Type 1asystole
Implant an ILR
Severe, recurrent, unpredictable syncopes, age >40 yrs
Clinical features no Pacing not indicated
yes
Implant a DDD PM & counteract hypotensivesusceptibility
yes
no
Implant a DDD PMYes & Tilt negative
no
Pacing not indicated
Implant a DDD PM & counteract hypotensivesusceptibility
Yes & Tilt positive
Pacing for neurally-mediated syncope: decision tree
no
Implant a DDD PMYes & Tilt negative
Implant a DDD PM & counteract hypotensivesusceptibility
Yes & Tilt positive

www.gimsi.it
Italian Multidisciplinary Group for the Study of Syncope:
Established in 2003 by 5 national societies:- arrhythmology, - internal medicine, - emergency medicine, - geriatrics- neurology





























