Embed Size (px)
Citation preview

w w w . e s c r i b e r . c o m
Dilip Nathwani Consultant Physician and Honorary Professor, Ninewells Hospital and
Medical School, Dundee
Healthcare associated infections(HAIs) affect around 2 million peopleadmitted to acute care hospitals inthe USA.1 Approximately 9 per centof patients in UK hospitals sufferfrom an infection acquired duringtheir hospital stay,2 many of whichare due to multi-resistant, Gram-positive and Gram-negative patho-gens. The incidence of colonisationand infection with these pathogenscontinues to rise due to failures inhospital hygiene, selective pressurescreated by overuse of antibiotics,and mobile elements that can enc-ode bacterial resistance mechanisms.
Infection with these resistantpathogens can adversely affectclinical, microbiological and
economic outcomes,3 and the costsassociated with managing infec-tions are considerable. In the UK,4
it has been estimated that costsincrease three-fold when hospitalpatients present with one or more HAI during an inpatient stay.This represents an absoluteincrease of £3154 per case in the1449 patients selected for follow-upin the study. On average, thelength of hospital stay is 2.9 times(14 days) longer for patients withan HAI, and there are also addi-tional burdens imposed on com-munity healthcare services afterdischarge. The annual cost of HAIsto the UK National Health Serviceis estimated to be £986 million.
New agents to combat serioushospital infections are urgentlyneeded. There are multiple factorsthat threaten the future of theantibiotic era: high levels of resis-tance among important pathogens;uneven supply of novel classes ofantibiotics, and a dramatic reduc-tion in the number of pharmaceu-tical companies engaged in thediscovery and development of anti-infective agents.5 The high levels ofresistance observed in hospitals in the USA, the UK and manyother parts of the world, lead to frequent outbreaks, as was illus-trated in a survey of 670 hospitalsin the USA.6 Resistance rates for oxacillin-resistant Staphylo-coccus aureus (ORSA); vancomycin-resistant enterococcus (VRE),quinolone-resistant E. coli andextended spectrum beta lactamase
(ESBL) producing Klebsiella spp,were 36 per cent, 10 per cent, 6 percent and 5 per cent, respectively.Two thirds of hospitals confirmedincreased rates of infection, andnearly a quarter reported out-breaks from these resistantpathogens. There is also an emerg-ing threat of community-acquiredstrains of E.coli and Klebsiellaspp. The presence of multidrug-resistant ESBLs7 and community-acquired methicillin-resistant Stap-hylococcus aureus (MRSA),8
confirms the need for new agentsto combat these infections both inthe hospital setting and beyond.
Tigecycline (Tygacil) is a novel,broad-spectrum glycylcycline anti-biotic that has activity against abroad range of Gram-positive,Gram-negative enterobacteriaceae,atypical organisms, anaerobic, and
F U T U R E P R E S C R I B E R V O L 7 ( 1 ) 2 9
Tigecycline: a novel broad spectrum antibiotic
D R U G P R O F I L E
t i g e c y c l i n e
Figure 1. Coloured transmission electron micrograph of methicillin-resistant Staphylococcus aureus
(MRSA), a Gram-positive, round (coccus) bacterium, resistant to many commonly prescribed antibiotics.
SCIENCE
PHO
TOLIBRA
RY
many antibiotic-resistant bacteria(including MRSA, VRE and peni-cillin-resistant Streptococcus pneumo-niae, and multiresistant Acinetobacterbaummani). It was licensed in theUSA in June 2005 and will belicensed in the UK in early 2006.
While exhibiting antibacterialactivities typical of earlier tetracy-clines, or analogues such asminocycline, it has more potentactivity against tetracycline-resistantorganisms. Unlike existing tetracy-clines, tigecycline is only availableas an intravenous preparation. It isadministered twice daily, althoughits long half-life and post-antibioticeffect may make once-daily dosingpossible. Although a bacteriostaticcompound in vitro, its effectivenessin clinical trials against cidal drugs, such as imipenem and aztre-onam, suggests a need to reassess traditional laboratory thinking concerning the use of bacteriosta-tic drugs in serious infections.
Whilst one recognises that theother key comparator vancomycinis only slowly bactericidal com-pared with beta-lactams and bacte-riostatic against enterococcal spp,tigecycline appeared to performequally well.
The last decade has witnessed awelcome proliferation in the devel-opment of agents active againstresistant Gram-positive bacteria (eg linezolid, daptomycin) andfungi. Development of agentsactive against multi-resistant, Gram-negative bacteria, however,has been slow or non-existent.Therefore, the availability of a newagent with activity against bothgroups of resistant bacteria is a welcome addition to the thera-peutic arsenal. The emergence ofresistant and/or polymicrobialinfections in a variety of settings(intra-abdominal sepsis, hospital-acquired pneumonia, complicatedskin and soft tissue infections and
diabetic foot ulcer infections), and the need for effective, empirictherapy in critically ill patients,9
illustrates the clear clinical impor-tance of such agents. This shortreview aims to provide guidance for clinicians involved in the formulary decision on the poten-tial value of tigecycline.
TIGECYCLINE
Mechanism of action Tigecycline is a semisynthetic deriv-ative of minocycline. It is mecha-nistically similar to aminogly-cosides, macrolides, stretogramins,and oxazolidinones in that it bindsto the 30S ribosomal subunit.10,11,12
This blocks access of aminoacyltRNA to its acceptor site, and leadsto the prevention of bacterial protein synthesis and growth.Tigecycline overcomes two types ofgenetic mechanisms primarilyresponsible for clinical tetracyclineresistance: efflux and ribosomal
3 0 F U T U R E P R E S C R I B E R V O L 7 ( 1 )
D R U G P R O F I L E
t i g e c y c l i n e
w w w . e s c r i b e r . c o m
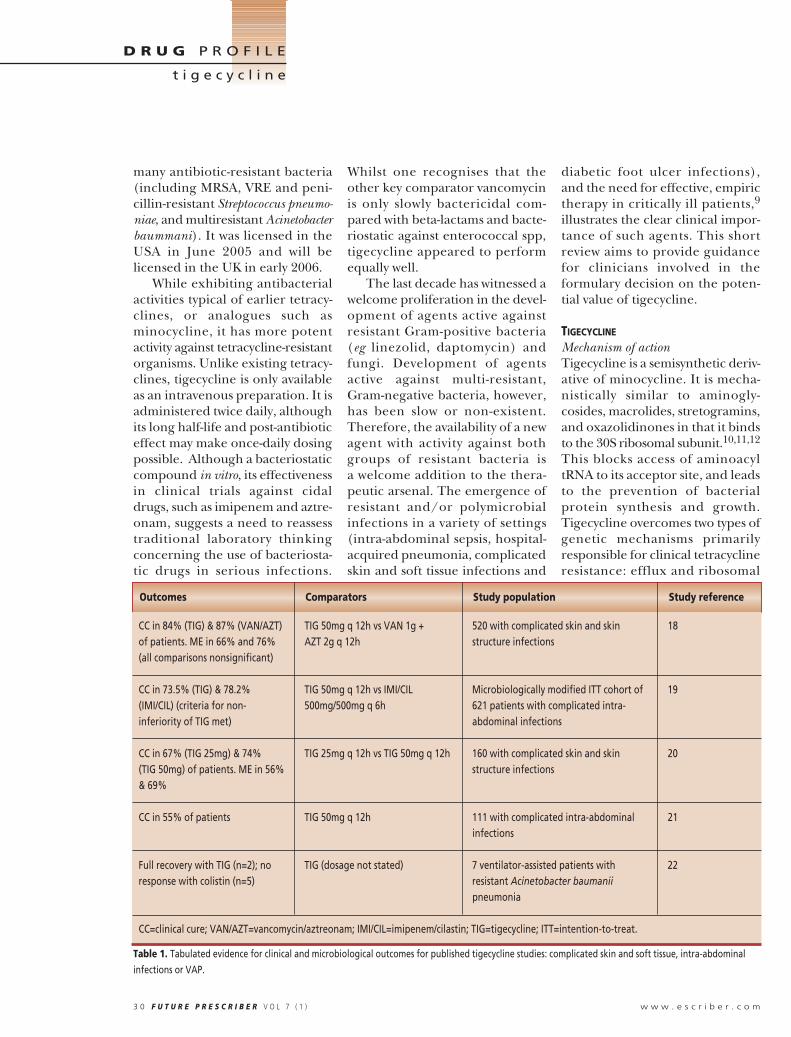
Table 1. Tabulated evidence for clinical and microbiological outcomes for published tigecycline studies: complicated skin and soft tissue, intra-abdominal
infections or VAP.
Outcomes Comparators Study population Study reference
CC in 84% (TIG) & 87% (VAN/AZT) TIG 50mg q 12h vs VAN 1g + 520 with complicated skin and skin 18of patients. ME in 66% and 76% AZT 2g q 12h structure infections(all comparisons nonsignificant)
CC in 73.5% (TIG) & 78.2% TIG 50mg q 12h vs IMI/CIL Microbiologically modified ITT cohort of 19(IMI/CIL) (criteria for non- 500mg/500mg q 6h 621 patients with complicated intra-inferiority of TIG met) abdominal infections
CC in 67% (TIG 25mg) & 74% TIG 25mg q 12h vs TIG 50mg q 12h 160 with complicated skin and skin 20(TIG 50mg) of patients. ME in 56% structure infections& 69%
CC in 55% of patients TIG 50mg q 12h 111 with complicated intra-abdominal 21infections
Full recovery with TIG (n=2); no TIG (dosage not stated) 7 ventilator-assisted patients with 22response with colistin (n=5) resistant Acinetobacter baumanii
pneumonia
CC=clinical cure; VAN/AZT=vancomycin/aztreonam; IMI/CIL=imipenem/cilastin; TIG=tigecycline; ITT=intention-to-treat.

protection.10,11,12 However, itremains vulnerable to the multidrug efflux pumps of Proteeaeand Pseudomonas aeruginosa and,less frequently, Bacteroides spp via a different mechanism.13
Spectrum of coverage Tigecycline is active against a broadrange of Gram-positive, Gram-negative and anaerobic organisms,including multidrug-resistantstrains such as Acinetobacter spp,which are mostly susceptible at0.5–2mg/l. As mentioned above,the main areas of vulnerability arethe Pseudomonas and Proteeae.
It should be noted that only 5naturally occurring tigecycline-resistant isolates13 have beenobserved during phase 3 trials.This suggests that clinically relevantglycylcycline-resistant bacterialstrains would be unlikely todevelop quickly, although itspropensity to select resistanceneeds to be closely monitored. Like all anti-microbials, however, it may simply be a matter of time before these isolates becomeapparent and, subsequently, clini-cally relevant.
Pharmacokinetics and pharmaco-dynamics1,13,14
Tigecycline is a bacteriostatic agentagainst E. faecalis, E. coli, S. aureusand K. pneumoniae. It has beenreported to be both bacteriostaticand bactericidal against S. pneumo-niae. In vitro studies have demon-strated a prolonged post-antibioticeffect following a 3mg/kg tigecy-cline dose: 8.9 hours for S. pneumo-niae and 4.9 hours for E. coli. Inaddition, pharmacodynamic stud-ies have concluded that time aboveMIC (or a fraction of MIC) andAUC both correlated with efficacyfor at least S. pneumoniae, E. coli,and K. pneumoniae.
The distinction between bacte-riostatic and cidal antibiotics inclinical practice as a means of identifying or predicting clinicalefficacy of agents is less clear cut.15
The importance of combining bacteriostatic/bactericidal datawith pharmacokinetic and phar-macodynamic information for predicting in vivo efficacy has been illustrated for a variety ofagents, in various clinical scenarios.Tigecycline, although bacteriosta-tic, appears to offer a number ofthese important characteristics,including extensive and good tissue distribution, a prolongedpost-antibiotic effect, and favour-able time above MIC against keypathogens in animal studies.14 Thevery long terminal half-life (around36 hours), as a consequence ofwide tissue distribution, may haveadvantages for certain infections.On the other hand, the low serumconcentration achieved may be ofsome concern in bacteraemicpatients, although there are no clinical data to substantiate this theoretical concern.13
CLINICAL TRIALS
Two phase 2 and two phase 3 clin-ical trials involving tigecy-cline,16,17,18 and one case seriesrelated to VAP20 have beenreported to date. The key clinicaland microbiological results are pre-sented in Table 1. These clinicaldata, confined to complicated skinand soft tissue infections16,19 andintra-abdominal infections,17,19
are encouraging and should provide a platform for further clin-ical evaluation. However, it isimportant that tigecycline is alsoevaluated in other therapeuticareas in which it may prove useful.Early evidence of the benefit ofdoxycycline, minocycline and tige-cycline, combined with other
agents, in hospital pneumonia dueto Acinetobacter spp infection isencouraging. This is an area clearlyworthy of further study.20
TOLERABILITY
In all of the clinical trials presentedin this review, nausea and vomitingwere recorded as the most signifi-cant side effects. Importantly, the occurrence of these side effectsdoes not appear to result in discontinuation of treatment.Whether the nausea and vomitingare preventable by pre-emptivetherapy with anti-emetics is uncer-tain, and no one anti-emetic agentappears to be superior or prefer-able in treating this side effect. Likeall tetracyclines, use in childrenand pregnancy is to be avoided.Only one possible case of tigecy-cline-induced C. difficile infectionhas been reported. Further clinicaltrials and post-marketing surveil-lance will reveal the true incidenceof these side effects.
ECONOMICS
There are no data looking directlyat the health economic benefits oftigecycline, but there are studiesthat have looked at its effect onlength of hospital stay. It has beenreported that the use of tigecyclinein patients with complicated SSTIsmay lead to a reduction in thelength of time spent in hospital.21
Yet an intention-to-treat (ITT)analysis of pooled data from therecent cSSTI clinical trials (involv-ing 1116 patients) found no difference in length of hospital stay between patients receiving tigecycline and those receiv-ing vancomycin/aztreonam. Riskadjustment for significantly longerstay (eg diabetes, trauma, Gram-negative infection, absence of cure,use of concomitant medication,infected ulcer, need for intensive
F U T U R E P R E S C R I B E R V O L 7 ( 1 ) 3 1
D R U G P R O F I L E
t i g e c y c l i n e
w w w . e s c r i b e r . c o m

care, and being in a non-US hospi-tal setting), however, reveals animportant 1-day reduction inlength of hospital stay. This obser-vation was primarily due to the sub-group of patients with Gram-negative infections (18 per cent,mostly E. coli), and so does not pro-vide unequivocal evidence ofhealth economic benefits relatedto tigecycline. This is clearly anarea requiring further study.
FORMULARY POSITIONING
A recent review of the formularypositioning of linezolid22 provides ageneric overview of the rationalebehind new drug evaluations andthe requirements of drug and ther-apeutic committees when consid-ering new agents for hospital for-mularies. The Scottish MedicinesConsortium New Product Assessm-ent Form (http://www.scottishmedi-cines.org.uk) provides a modern sys-tematic and methodical approachfor considering new agents:• Information pertaining to clini-cal indications• Identification of the major com-petitors in specific disease areas• The agent’s place in relation toexisting therapy and its relevanceto a particular country or region• Its clinical efficacy• Its comparative safety, and pharmaco-economic evaluation.
With this in mind, and havingconsidered the existing data on tigecycline, the following observations can be made:• Tigecycline offers a therapeuticoption in post-surgical woundinfections or complicated SSTIs (eginfected diabetic ulcers or infectedchronic pressure sores) whereMRSA, streptococci, enterobacte-riaceae and anaerobes are impor-tant alone, or as polymicrobialpathogens. Normally, this requiresfrequent, combination therapy, but
tigecycline offers a less complextherapeutic option, and a potentialreduction in cost.• Whether the other indicationarea of intra-abdominal infectionsis likely to be important in the UKappears less clear. There is a dearthof good quality UK microbiologicalevidence showing that resistance isa major issue among the keycausative pathogens: the enter-obacteriaceae, streptococci, ente-rococci or anaerobes. Further-more, there are few data to suggestthat the traditional surgical work-horses, cefuroxime and metron-idazole or co-amoxiclav, are notperforming adequately in the routine surgical setting. • For both the above disease areas,and in other areas, use in patientswith beta-lactam, glycopeptide orquinolone hypersensitivity or intol-erance, is a potential therapeuticniche. However, over-interpreta-tion of allergy/hypersensitivity iscommon and should not be anindication for widespread use ofalternative agents. • The emergence of clinically sig-nificant multidrug-resistant ESBLsamong enterobacteriaceae in thehospital and increasingly in thecommunity setting, presents a sig-nificant threat, but also an oppor-tunity to consider tigecycline. Themain caveat to this is that many ofthese infections affect the urinarytract, a setting where tigecycline isnot an ideal choice, owing to its biliary excretion profile. Also manypatients with complicated urinarytract infections (eg catheterisedpatients) will not be suitable asthere are concerns about tigecy-cline’s activity against Proteus andProvidencia spp.
FUTURE THERAPEUTIC AREAS
It is likely that more specific anti-MRSA agents, such as the gly-
copeptides, new lipopeptides (egdaptomycin) and linezolid, will be used if resistant Gram-positiveinfections are confirmed or sus-pected. Other areas where mixedinfections are likely, or emerging,are spontaneous bacterial peri-tonitis, some renal dialysis catheterinfections with peritonitis, and surgical MESH infections. Otherpossible uses of tigecycline mayinclude nosocomial or nursinghome acquired pneumonia, wherePseudomonas spp. infection is lesslikely to be an important causativepathogen (eg early VAP or hyper-ammonia-producing bacteria,HAP). In the absence of good anti-pseudomonal activity, tigecycline’splace in febrile neutropenicpatients would seem limited. Theexceptions are patients classified asbeing at low risk of the infection,and high-risk patients, in combi-nation with a good anti-pseudo-monal activity agent.
Little is known about synergy orantagonism when combining tige-cycline with other agents. Theevolving nature of the microbiol-ogy of diabetic foot infections, withthe emergence of resistant Gram-positive and Gram-negative bacte-ria,23 suggests that tigecycline mayoffer significant potential if pene-tration into deep tissues and boneis deemed adequate. In the future,exploring the role of parenteraltigecycline in ambulatory infectioncare would also broaden theantimicrobial options as well ascost-effectiveness in this setting.24
Studies are currently beingundertaken in many of these areasto explore tigecycline’s potential.These include an open-label andnon-comparative trial in patientswith serious, resistant, Gram-nega-tive infections (eg A. baumanii, Ente-robacter spp., K. pneumoniae, etc.); arandomised and double-blind
3 2 F U T U R E P R E S C R I B E R V O L 7 ( 1 )
D R U G P R O F I L E
t i g e c y c l i n e
w w w . e s c r i b e r . c o m

comparison with levofloxacin inpatients hospitalised with comm-unity-acquired pneumonia; a randomized and double-blindcomparison with linezolid for seri-ous infections in patients with VRE,and with vancomycin for seriousinfections in patients with MRSA.Conditions covered include: bacteraemia, pneumonia, and bacterial SSTIs. There is also a randomised and double-blindcomparison with imipenem/cilas-tatin in patients with nosocomialpneumonia. The findings of theseimportant studies, as well as futurehealth economic evaluation, willfurther help with the optimal positioning of tigecycline within medical formularies.
CONCLUSION
The introduction of tigecycline is welcome at a time of increasingproblems with bacterial resist-ance. Evidence to date has beensufficient for regulatory approval for complicated SSTIs and intra-abdominal infections in the USA,and UK and European approval is imminent.
Tigecycline offers a broad spec-trum of antimicrobial activity, andhas continued activity against arange of pathogens traditionallytreated with tetracyclines. Itsenhanced activity against manypathogens (including importantresistant pathogens) predomi-nantly acquired in a healthcareenvironment, and its parenteralroute of administration, primarilyplaces it for use in patients withserious hospital infections. In thefuture, it may offer the potentialfor treating more sub-acute orchronic infections in the ambula-tory care setting.
Tigecycline appears to be welltolerated despite reports ofincreased frequency of nausea and
vomiting. It also appears to haveno significant drug interactions,which is an important considera-tion in treating sick patients whoare commonly on numerous drugs.Traditional laboratory concernsabout using bacteriostatic drugs inserious infections need to berevised in light of emerging evi-dence of the effectiveness of a vari-ety of such agents in differentclinical settings. Further good qual-ity studies and ongoing surveillancefor any emerging bacterial resis-tance will be crucial to determinethe long-term effectiveness of thisagent. A thorough economic eval-uation of its effectiveness is alsorequired in the UK.
REFERENCES1. Monitoring hospital-acquired infections topromote patient safety—United States, 1990-1999. MMWR Morb Mortal Wkly Rep 2000; 49:149-53.2. Crowcroft, N.S. Catchpole, M. Mortality frommethicillin resistant Staphylococcus aureus inEngland and Wales: analysis of death certifi-cates. BMJ 2002; 325: 1390-1. 3. Cosgrove, S.E. Carmeli, Y. The impact ofantimicrobial resistance on health and economicoutcomes. Clin Infect Dis 2003; 36: 1433-7.4. Plowman R. The socioeconomic burden ofhospital acquired infection. Euro Surveill.2000;5:49–50.5. Wenzel, R.P. The antibiotic pipeline—chal-lenges, costs, and values. N Engl J Med 2004;351: 523-6.6. Diekema, D.J., BootsMiller, B.J., Vaughn, T.E.,et al. Antimicrobial resistance trends and out-break frequency in United States hospitals. ClinInfect Dis 2004; 38: 78-85.7. Woodford N, Ward ME, Kaufmann ME, et al.Community and hospital spread of Escherichiacoli producing CTX-M extended-spectrumbeta-lactamases in the UK. J AntimicrobialChemother 2004; 54: 628-33. 8. Vandenesch F, Naimi T, Enright MC et al.Community acquired meticillin-resistantStaphylococcus aureus carrying Panton-Valen-tine leukocidin genes: worldwide emergence.Emerging Infectious Diseases 2003; 9: 978-84. 9. Kollef, M. Appropriate empirical antibacter-ial therapy for nosocomial infections: getting itright the first time. Drugs 2003; 63: 2157-68.10. Bush, K. Macielag, M. New approaches inthe treatment of bacterial infections. Curr OpinChem Biol 2000; 4: 433-9.11. Chopra, I. Glycylcyclines: third-generationtetracycline antibiotics. Current Opinion inPharmacology. 2001; 1: 464-9.
12. Zhanel, G.G., Homenuik, K., Nichol, K., etal. The glycylcyclines: a comparative reviewwith the tetracyclines. Drugs 2004; 64: 63-88.13. Livermore D. Tigecycline: what is it, andwhere it should be used? Journal AntimicrobChemother 2005; 56: 611-614. 14. Pankey GA. Tigecycline. Journal Antim-icrob Chemother 2005; 56: 470-480. 15. Pankey, G.A. Sabath, L.D. Clinical relevanceof bacteriostatic versus bactericidal mecha-nisms of action in the treatment of Gram-pos-itive bacterial infections. Clin Infect Dis 2004;38: 864-70.16. Dartois N, Tigecycline 305 CSSSI StudyGroup. Results of a phase 3, double-blind,safety and efficacy study comparing tigecyclinewith vancomycin/aztreonam to treat compli-cated skin and skin structure infections.Proceedings of the 44th Annual InterscienceConference on Antimicrobial Agents andChemotherapy; October 30–November 2, 2004;Washington, DC. Abstract L-986.17. Ellis-Grosse EJ, Loh E, on behalf of theTigecycline 301 Study Group. Tigecycline com-pared with imipenem/cilastatin in the treat-ment of complicated intra-abdominalinfections. 15th European Congress of ClinicalMicrobiology and Infectious Diseases; April 2–5,2005; Copenhagen, Denmark. Abstract P1317.18. Murray J, Wilson S, Klein S, Yellin A, Loh E.The clinical response to tigecycline in the treat-ment of complicated intra-abdominal infec-tions in hospitalized patients, a phase 2 clinicaltrial. Proceedings of the 43rd AnnualInterscience Conference on AntimicrobialAgents and Chemotherapy; September 14–17,2003; Chicago. Abstract L-739.19. Postier RG, Green SL, Klein SR, Ellis-GrosseEJ, Loh E, for the Tigecycline 200 Study Group.Results of a multicenter, randomized, open-label efficacy and safety study of two doses oftigecycline for complicated skin and skin struc-ture infections in hospitalized patients. ClinTher. 2004;26:704–714.20. Wilson P. Endemic, highly resistantAcinetobacter in the intensive care unit – istigecycline the answer? Clin Microbiol Infect.2004;10 (Suppl. 3):247. Abstract P938.21. Mallick R, Solomon S. The duration of hos-pitalization (length of stay) in patients hospi-talized with complicated skin and skinstructure infections: identifying clinical andmicrobiological risk factors in a comparison oftigecycline with vancomycin/aztreonam. 15thEuropean Congress of Clinical Microbiologyand Infectious Diseases; May 1–4, 2005; Prague,Czech Republic. Abstract P1181.22. Nathwani, D. Economic impact and formu-lary positioning of linezolid: a new anti-Gram-positive antimicrobial. J Hosp Infect 2001; 49Suppl A: S33-41.23. Lipsky, B.A. Medical treatment of diabeticfoot infections. Clin Infect Dis 2004; 39 Suppl2: S104-1424. Nathwani, D. The management of skin andsoft tissue infections: outpatient parenteralantibiotic therapy in the United Kingdom.Chemotherapy 2001; 47 Suppl 1: 17-23.
F U T U R E P R E S C R I B E R V O L 7 ( 1 ) 3 3
D R U G P R O F I L E
t i g e c y c l i n e
w w w . e s c r i b e r . c o m





























