Embed Size (px)
Citation preview

Barbara J. Coffey, MD, MSProfessor, Department of PsychiatryIcahn School of Medicine at Mount SinaiChief, Tics and Tourette’s Clinical and Research ProgramNew York, New YorkResearch PsychiatristNathan Kline Institute for Psychiatric ResearchOrangeburg, New York
Tics, Tourette’s Disorder and ADHD Throughthe Lifespan
February 27, 2013ADHD Worldwide Conference

Disclosures of Potential Conflicts (2012-2013)
Source ResearchFunding
AdvisorConsult
Employee SpeakersBureau
Books,Intellectual
Property
In-kindServices
(example:travel)
Stock orEquity >$10,000
BoehringerIngelheim
X
Catalyst X
NIMH X
Otsuka X
TSA X X X
Shire X
Genco Sciences X

3

Tics, Tourette’s Disorder and ADHDThrough the LifespanLearning Objectives
• To review:• Bidirectional overlap between ADHD and
tic disorders• Prevalence and impact of tic disorders and
ADHD in youth and adults• Update on relevant clinical science
research on ADHD and tic disorders• Treatment focus: use of stimulants in
comorbid ADHD and tic disorders
Epidemiology: Bi-Directional Overlap ofADHD and Tic Disorders• 1) Rates of tic disorders are higher (10-30%) in children
with Attention Deficit Hyperactivity Disorder (ADHD) thanin children without ADHD (1-10%) (Spencer, Biederman,Coffey et al., Arch Gen Psych; 1999, 56: 842-84)
• 2) Rates of comorbid ADHD are high (50-75%) inclinically referred children with Tourette’s Disorder (TD).(Coffey, Biederman, et al. J Nerv Ment Dis; 2000;188:583-588; Freeman, TS International Data base Consortium;Eur Child Adolesc Psych 2007; 16 [suppl; 1];1/15-1/23)
• 3) Rates of ADHD in a TD community sample were higher(8.3%) than ADHD population prevalence (3.9%) (Apter etal, 1993; Scahill et al 2007)

6
Classification: DSM V: Neurodevelopmental Disorders: MotorDisorders vs. DSM-IV-TR 2000 Tic Disorders
• Transient tic disorder: one or more tics present for greater than 4weeks, but less than 12 months
• Provisional tic disorder: Single or multiple motor tics and/orvocal tics; present for less than 1 year since first tic onset.Onset before age 18.
• Chronic motor or vocal tic disorder: one or more motor or vocaltics present for greater than 1 year
• Tourette’s Disorder. Both multiple motor and one or more vocaltics have been present at some time during the illness, although notnecessarily concurrently. Tics occur many times a day (usually inbouts), nearly every day or intermittently throughout a period ofmore than 1 year, and during this period there was never a tic-freeperiod of more than 3 consecutive months. Onset before 18 years.
• The tics may wax and wane in frequency but have persisted formore than a year since first tic onset.
• Tic Disorder Not Otherwise Specified• Unspecified Tic Disorder
Tics and Tourette’s Disorder: Epidemiology(Scahill et al; Morbidity and Mortality Weekly ReportCDC; 2009)
•CDC Prevalence of Diagnosed TS inYouth age 6-17 in 2007 in US
• (National Study of Children’s Health)•0.3-1% in US•3x more common in boys than girls•2x more frequently diagnosed age 12-17
vs. 6-11

Prevalence of diagnoses age 6-17 years: ever received a diagnosis of Tourettesyndrome (TS),† by parent report(National Survey of Children's Health, United States, 2007)
• † Among children ever diagnosed with TS, 79% also had been diagnosed with at least one otherselected diagnosis. Among children who currently have TS, 73% currently have at least one additionalselected diagnosis.
• ¶ ADHD, by parent report.• ** Such as oppositional defiant disorder or conduct disorder, by parent report.

9
Cortico-
Striato-
Pallido-
Thalamic
CircuitGLOBUS
PALLIDUS
PUTAMEN
THALAMUS

TD and ADHD: Neurobiology(Seidman et al; Biol Psychiatry; 2005; 57; 1263-1272; Sukhodolsky et al; Eur ChildAdolesc Psychiatry 2007;16:1/51-1/59; Leckman et al; JCAP, 2010; 20 (4); 237-247;Dickstein et al; J Child Psych Psych; 2006: 47: 10. 1051-1062)
*Inhibition is a core deficit in both disordersExecutive functions abnormalities in both
thought to result from fronto-striatal andfrontal-parietal network dysfunction
ADHD: In youth, smaller volumes reported inDLPC, caudate, pallidum, corpus callosumand cerebellum (Seidman et al; 2005)
ADHD: Across studies, significant patterns offrontal hypoactivity reported, including ACC,DLPC, inferior prefrontal, and related regions:basal ganglia, thalamus and parietal cortex.

TD and ADHD: Neurobiology(Seidman et al; Biol Psychiatry; 2005; 57; 1263-1272; Sukhodolsky et al; Eur ChildAdolesc Psychiatry 2007;16:1/51-1/59; Leckman et al; JCAP, 2010; 20 (4); 237-247;Dickstein et al; J Child Psych Psych; 2006: 47: 10. 1051-1062)
TD: Approximate 5% reduction in caudate volumereported in both children and adults with TD(Peterson et al; 2003).
Inverse correlation between caudate volume inchildhood and tic severity in early adulthood(Bloch et al; 2005)
Cortical thinning in youth reported in sensory andmotor areas, correlating with worst ever ticseverity (Sowell et al; 2008).
TD+ ADHD: CTSC misguided neural oscillationsmay result in BG disinhibition, worsened by frontalhypoactivity in ADHD. Since both TD and ADHDimprove with time, may be due to increasedmyelinization of prefrontal regions.

Wang et al. 2011
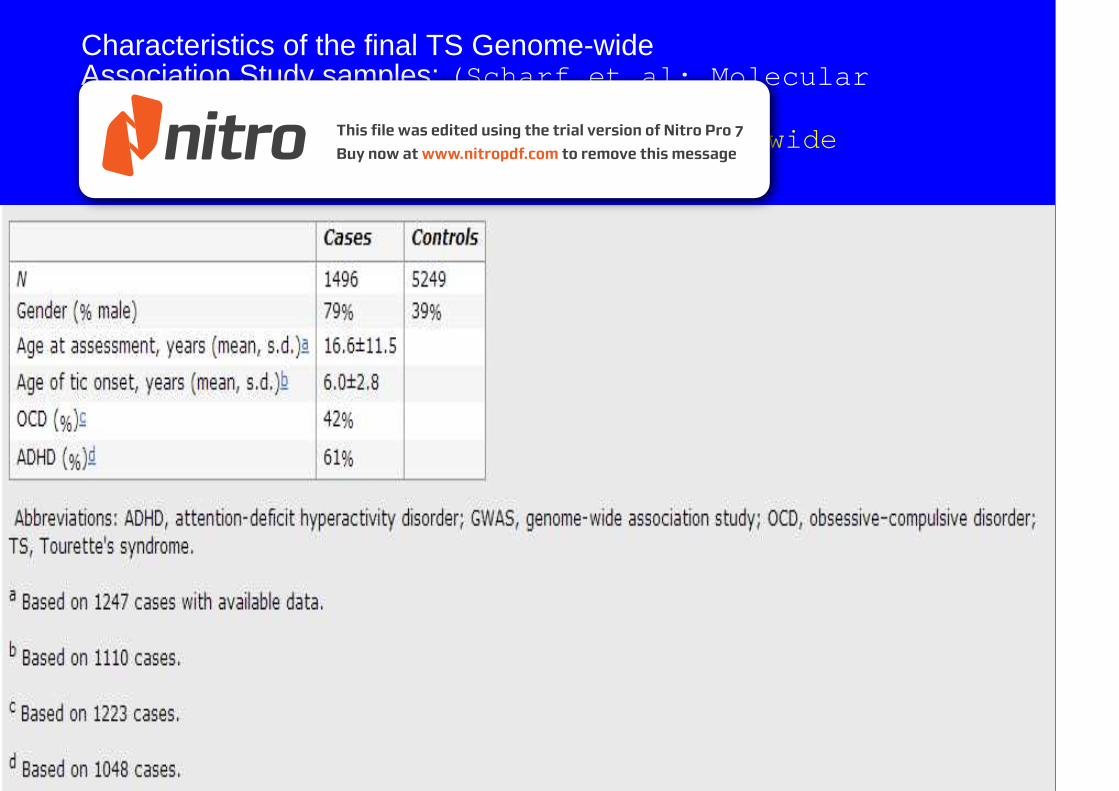
Characteristics of the final TS Genome-wideAssociation Study samples: (Scharf et al; MolecularPsychiatry; 2012; 1-8)Findings: no markers achieved a genome widethreshold of significance

Genome-wide association study of Tourettesyndrome (Scharf et al 2012)

Tourette’s Disorder: Natural History and Course:Does it Remit or Persist?What About Comorbidity?DSM IV-TR American Psychiatric Association (2000)• Course: “…….The duration of the disorder is usually
lifelong, though periods of remission lasting fromweeks to years may occur………..”
Tic severity:• Research in the past decade suggests peak severity
occurs at about age 10-11 years with improvementinto adolescence (retrospective birth cohort design)
(Leckman et al. Pediatrics. 1998; Coffey et al. JNMD.2004)

Time Course of Tic Severity Ratings(Leckman, Zhang, et al. Pediatrics. 1998;102:14-19)

Course of ADHD and Tic Disorders: What Happens to Tics in theContext of ADHD Over Time?(Spencer, Biederman, Coffey, et al. Arch Gen Psych 1999, 56: 842-847)
• Design: Prospective ADHD follow-up• Objective: To evaluate the prevalence and impact of tic
disorders at baseline and at follow-up on the course ofADHD.
• Methods: N=128 boys with ADHD; N=110 controls.Duration of follow-up: 4 years.
• Results:• Proportion of ADHD youth with tics: 34%• Remission rate for tics over 4 years: 65%• Remission rate for ADHD: 20%• Conclusion: Tic remission rate is independent of ADHD• Tic disorders did not impact ADHD course

**
Rates of Tic Disorders in ADHD & Control Probands%
ADHD ADHD ADHDControls Controls ControlsBaseline Follow-up Overall
** ***

Onset of ADHD and Tic Disordersin ADHD Probands
Age in Years0 5 10 15 20 250
ADHD
Tic Disorders
102030405060708090100
%
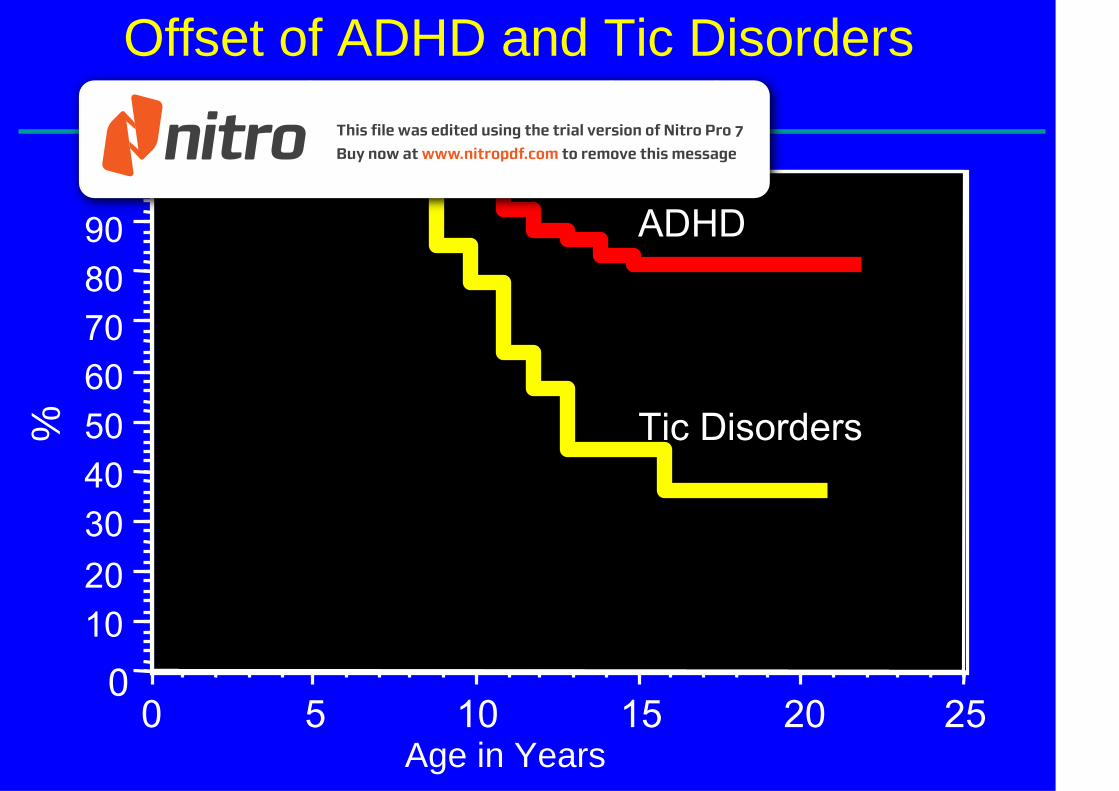
Offset of ADHD and Tic Disordersin ADHD Probands
Age in Years
00 5 10 15 20 25
Tic Disorders
ADHD
102030405060708090100
%

Informativeness of Structured DiagnosticInterviews in the Identification of Tourette’s Disorderin Referred Youth
(Coffey, B. et al.J. Nerv. Ment. Dis. 2000; Sep;188 (9):583-588)
Clinical and Demographic Characteristics of Non-specialized andSpecialized Clinic Patients with TD
Non-specializedClinic patients
(N=92)
Specialized Clinicpatients(N=103)
OverallSignificance
Mean SD Mean SD pCurrent Age 10.8 3.23 10.8 3.62 0.89SES 2.0 1.13 2.2 1.24 0.42
N % N % pPast GAS 47.9 7.50 48.6 7.57 0.54Current GAS 51.3 7.32 51.9 6.52 0.55% Male 82 90 81 80 0.06

Non-specializedClinic Patients
SpecializedClinic Patients
OverallSignificance
(N = 92) (N = 103)Diagnosis N % N % p
ADHD 76 84 74 72 .053
Conduct Disorder 18 20 14 14 .25
Oppositional DefiantDisorder
63 69 58 57 .91
Any Disruptive Disorder 83 91 86 84 .14
*Pure TD (Non-comorbid) 2 2 5 5 .31
Comorbidity: Disruptive BehaviorDisorders

Non-specializedClinic Patients
SpecializedClinic Patients
OverallSignificance
(N = 92) (N = 103)Diagnosis N % N % p
Panic Disorder 10 11 15 15 .45
Agoraphobia 21 23 27 26 .61
Social Phobia 15 16 5 5 .008
Simple Phobia 25 27 30 30 .73
OCD 19 21 37 36 .021
Separation Anxiety 22 24 39 39 .028
Multiple Anxiety Disorders(2+)
32 35 41 40 .47
Anxiety Disorders

Developmental Course of Tourette’s Disorder and ADHD
Developmental Psychopathology of Children and Adolescents withTourette Syndrome-Impact of ADHD(Roessner et al. Eur Child Adolesc Psych; 2007; 16;1/24-1/25)
Design and Subjects: TS International Data BaseConsortium
N=5060 patients in 67 tertiary centers in 27 countries:.Cross-sectional design; youth age 5-17 years
Findings:1. Higher rate of comorbidity in TD+ADHD than TD-
ADHD in children and adolescents2. Rate of OCD was higher in TD+ADHD in children
(age 5-10) but not adolescents (age 11-17).3. But OCD developed more rapidly year to year in the
TD-ADHD group

Year-wise changes of the rate of comorbidities in children andadolescents with TD versus TD+ADHD in (a) number of comorbiditiesand (b) obsessive compulsive disorder
Roessner, Eur Child Adolesc Psychiatry, 2007

Developmental Course of Tourette’s Disorder and ADHD(Roessner et al. Eur Child Adolesc Psych; 2007; 16;1/24-1/25)
International Data Base Consortium. N=5060 patients in 67tertiary centers in 27 countries: TS. Cross-sectional; youthage 5-17 years
1. Rate of comorbid ODD/CD was higher in youth withTD+ ADHD than TD-ADHD
1. Mood disorders were more frequent in children withTD+ ADHD, but the rate of increase was independentof ADHD
2. Anxiety disorders were slightly more frequent in TD+ADHD in children, but not in adolescents; rate ofanxiety disorders rose more rapidly in TD-ADHD

Year-wise changes of the rate of comorbidities in children andadolescents with TD versus TD+ADHD in (c) anxiety disorders, (d)conduct disorders/oppositional defiant disorder, (e) mood disorders
Roessner, Eur Child Adolesc Psychiatry, 2007

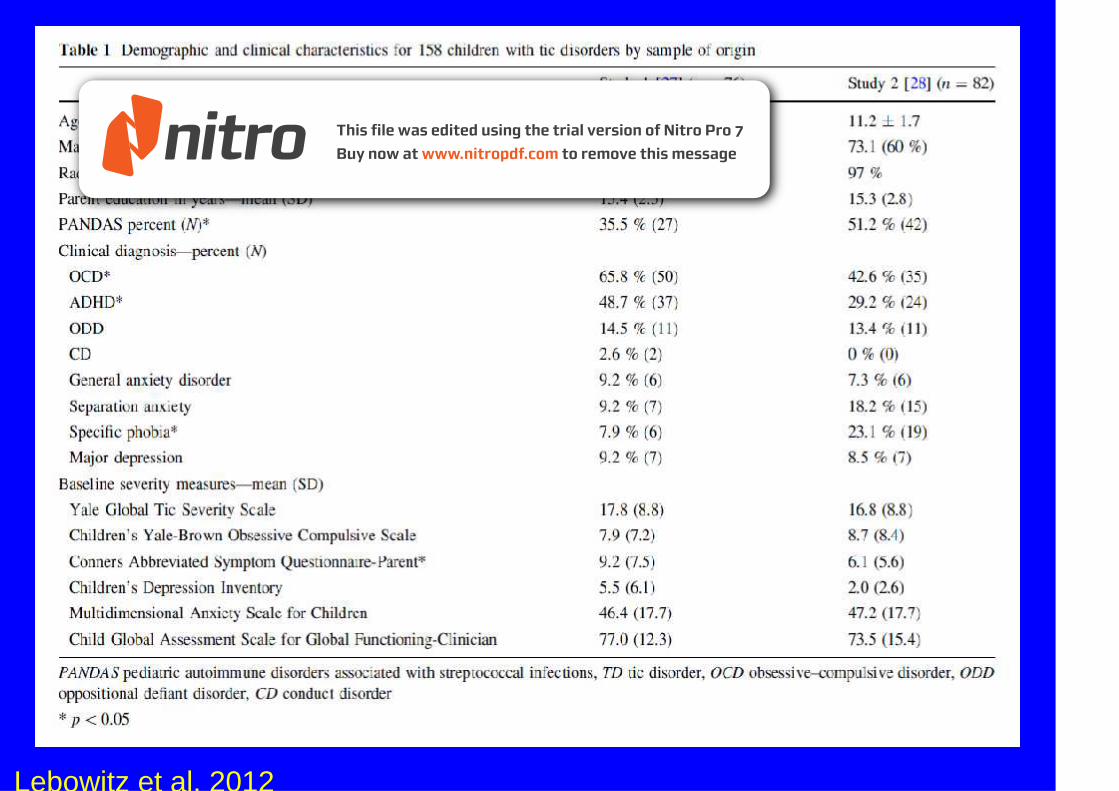
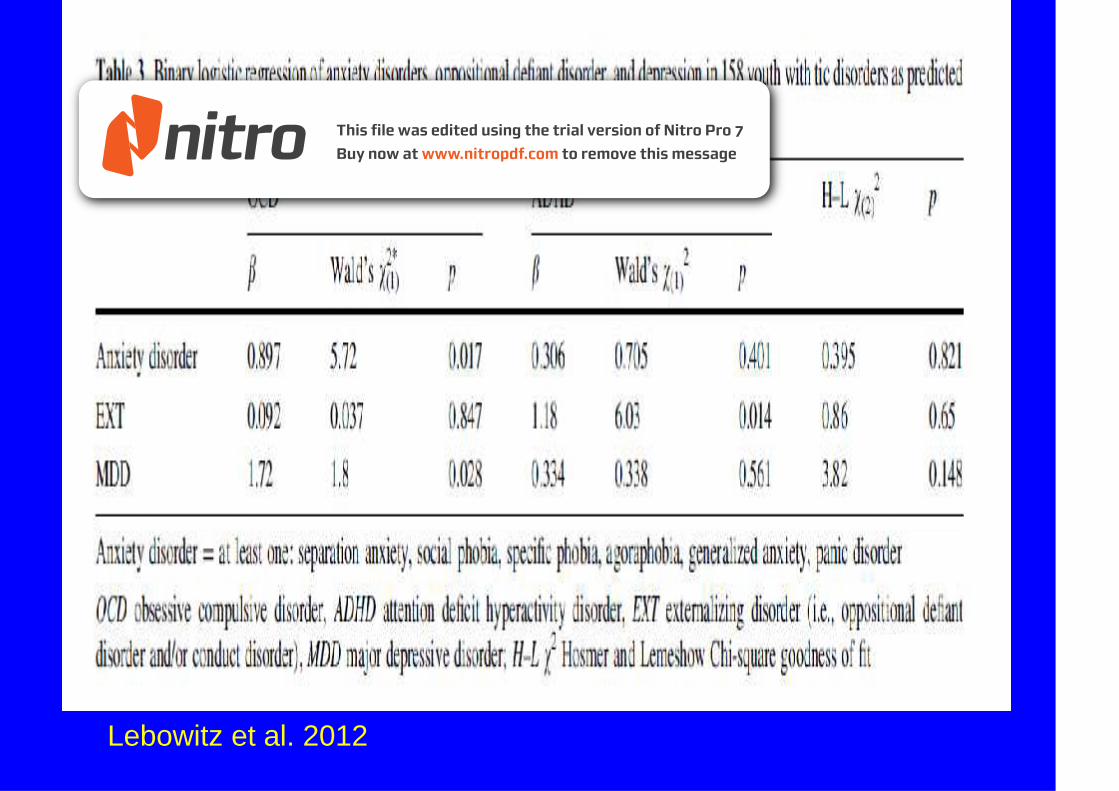
Tourette Syndrome in Youth with and without OCD andADHD(Lebowitz, E. Motlagh, M. Katsovich, L. King, R. Lombroso,Grantz, H. Line, H. Bentley, M. Gibert, D. Singer, H. Coffey,B. TSSG, Kurlan, R. Leckman, J. Eur Child Adolesc Psych2012; 21: 451-457)
• Design: Compared TS only with TS+ADHD and TS+OCD.• N=158 youth. 53% TS+OCD, 39% TS+ADHD, 24% both• Results: TS+OCD had more severe tics, more depression
and anxiety, poorer global functioning• TS+ADHD: same tic severity, but greater psychosocial
stress, more externalizing behaviors, and poorer globalfunctioning
• Conclusion: More research is needed on TS subtypes.
Lebowitz et al. 2012
Lebowitz et al. 2012

Disentangling Effects of Tourette Syndrome and ADHD onCognitive and Behavioral Phenotypes(Rizzo, R. Curatolo, P. Gulisano, M. Virzi, M. Arpino, C.
Robertson, M. Brain and Development; 2007; 29; 413-420)
• Design: N=80 youth, age 6-16 years, in 4 groups: TS only,ADHD only, TS+ADHD, controls.
• Results: All cases differed significantly from controls. TSonly did not differ from controls in behavioral ratings or IQ.
• ADHD, with or without TS, was associated with morebehavioral problems and lower IQ.
• No difference in affective and anxiety symptoms betweenthree case groups, but differed from controls.
• TS patients were found to be more “delinquent” thancontrols.
• Conclusions: May be additive effect of ADHD and TS.

Rizzo et al. 2007

Tourette Syndrome-Associated Psychopathology: Roles ofComorbid ADHD and OCD(Pollak, Y. Benarroch, F. Kanengisser, L. Shilon, Y. Benpazi,
H. Shalev, R. Gross-Tsur, V. Dev Behav Pediatr; 2009; 30;413-419)• Aim: Evaluate impact of tic, ADHD and OCD on
CBCL externalizing and internalizing disorders• Design: Chart review of 180 TS subjects, age 15-18, in
Neuropediatric Clinic. Compared CBCL in TS only,ADHD only, TS+ADHD and controls.
• Results: Highest prevalence of externalizing inTS+ADHD>ADHD>TS only>controls
• Highest prevalence of internalizing in TS+ADHD>TSonly>ADHD>controls.
• Conclusion: Tics, ADHD and OCD differentially effectvariance in internalizing and externalizing problems,and TS only is a risk factor for behavioral problems.

Psychosocial Outcome and Psychiatric Comorbidity inOlder Adolescents with Tourette Syndrome(Gorman, D. Thompson, N. Plessen, K. Robertson, M.Leckman, J. and Peterson, B.; Br J Psych; 2010; 197; 36-44)
• Aim: To compare psychosocial outcome and lifetimecomorbidity rates in older adolescents with TD andcontrols
• Design: N=65 with TD identified in childhood, and 65matched community controls, assessed at age 18
• Results: Compared with controls, TD individuals hadsubstantially lower CGAS scores and higher rates ofADHD, MDD, and CD (p <0.01). In those with TD,poorer psychosocial outcomes were associated withgreater ADHD, OCD and tic severity.
• Conclusion: Clinically referred youth with TD haveimpaired psychosocial outcome and high comorbidityrates in late adolescence.

Comparison of lifetime psychiatric disorders in theTourette syndrome group and community controls
Gorman, BJ Psych, 2010

Impact of Tic Disorders on ADHD Outcome Across the LifeCycle: Findings from a Large Group of Adults With andWithout ADHD(Spencer, Biederman, Faraone, Mick, Coffey, et al. Am JPsych 2001; 158: 611-617)
• Objective: To assess impact of presence of tic disorder on thecourse of ADHD in adults.
• Methods: Blinded, retrospective assessment by StructuredClinical Interview for DSM IV (SCID), supplemented with modulesfrom the K-SADS-E covering childhood diagnoses.
• N=312 adults with ADHD; N=252 adult controls• Results: Significantly greater proportion of adults with ADHD
(12%) than those without ADHD (4%) had tic disorders• Tic disorders followed mostly a remitting course and had little
impact on functional capacities.• Conclusion: Adult findings confirm and extend previous findings
in youth with ADHD, documenting that although individuals withADHD are at greater risk for tic disorders, the presence of ticshas limited impact on ADHD outcome.
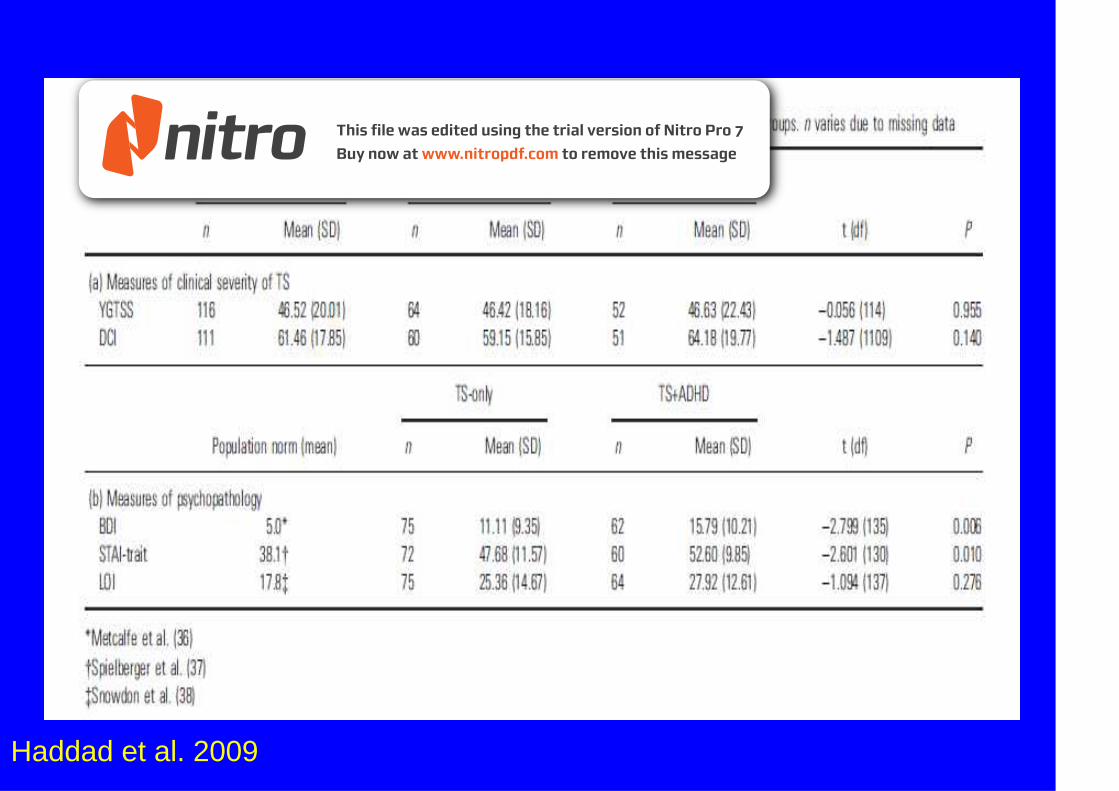
Adults with Tourette Syndrome with and without AttentionDeficit Hyperactivity Disorder(Haddad, A. Umoh, B. Robertson, M. Acta Psychiatr Scand;2009; 120; 299-307)
• Design: N=80 adults with TS only were compared to 64with TS+ADHD in a clinical interview and standardizedmeasures of depression, anxiety and OCD
• Results: No differences in tic severity.• TS+ADHD had significantly more depression, anxiety,
OCD and behavioral problems than TS only.• Conclusion: More overall behavioral problems and
psychopathology in adults with TS+ADHD vs TS only isconsistent with findings in children.
• ADHD treatment in childhood may prevent development ofbehavioral problems later in life.
Haddad et al. 2009

Haddad et al. 2009

Diagnostic Evaluation: Tics and ADHD
•• Structured diagnostic interviewsStructured diagnostic interviews,such as the Children's Schedule forAffective Disorders and Schizophrenia(K-SADS) can improve classificationand assessment of comorbidity.
•• Standardized rating scalesStandardized rating scales haveimproved diagnostic reliability inresearch studies; helpful in clinicalcare.
• The Yale-Global Tic Severity Scale(YGTSS) (Leckman, Riddle, Hardin,Ort, Swartz, Stevenson, et al., 1989)is considered “gold standard.” TheYGTSS assesses domains of ticnumber, frequency, intensity,complexity and interference (0-50),and tic related impairment (0-50).



TD/Tics + ADHD: Treatment Issues
Tics: Most patients with mild tic symptomsneed only monitoring, education, andguidance. Tic symptoms need to be treated ifcausing distress and/or impairment. In USthere are only two formally approvedmedications: haloperidol and pimozide.
ADHD: Since ADHD symptoms are more likely topersist and cause significant functionalimpairment, treatment is usually necessary..
What’s new? Behavioral treatment of tics(habit reversal training) is nowestablished. But there are no publishedstudies of combination pharmacotherapy andbehavioral treatment in comorbid ADHD andtic disorders.

ADHD and Tics/TD:Can We Treat with Stimulants?• Old studies suggested that stimulants
increase tics, (Lowe et al. 1980) and USpharmaceutical labeling states tics are acontraindication for stimulants (PDR, 2012)
• Recent studies demonstrated that some TDpatients with significant ADHD may becandidates for methylphenidate (MPH) whenno other treatments have been effective(Gadow, Nolan, Sverd. 1992; Gadow et al.2007; TSSG; 2002)

0102030405060708090100
0 5 10 15 20 25
Stimulant Treated
Not Stimulant Treated
Onset of Tic Disorders in ADHD ProbandsStratified by Stimulant Treatment
(Spencer, Biederman, Coffey, et al. Arch Gen Psych 1999, 56: 842-847)
Age in Years
%

0 5 10 15 20 25
Offset of Tic Disorders in ADHD ProbandsStratified by Stimulant Treatment
(Spencer, Biederman, Coffey, et al. Arch Gen Psych 1999, 56: 842-847)
Age in Years
0
Stimulant Treated
102030405060708090100
Not Stimulant Treated
%

Treatment of ADHD and Tics (TACT):Targeted Combined Pharmacotherapy Study(TSSG. TACT. Neurology. 2002; 58:527-536)
• NINDS-sponsored multicenter study of clonidine andmethylphenidate (MPH) in the treatment of children with ADHDand Tourette’s disorder or chronic tics (TACT)
• Design: 136 children (ages 7-14) were treated in the 16-week,double-blind, placebo-controlled protocolHypotheses:
• Methylphenidate and clonidine both individually and incombination are more effective than placebo for treatment ofADHD and tics in Tourette’s Disorder
Procedures:• Clonidine MPH Treatment Phase• or Pbo or Pbo• |--------------|---------------|---------------|-----------------|• BL 4 wk 8 wk 12 wk 16 wk

TACT Study: Results(TSSG, TACT. Neurology. 2002;58:527-538)
• ADHD (Teacher Conners): Compared to placebo,greatest benefit for CLON + MPH (p < 0.0001);significant improvement in CLON (p < 0.002) and MPH(p < 0.003) groups
• CLON: best for hyperactivity and impulsivity; MPH forinattention
• Tics (YGTSS): severity reduced in all treatment groupsvs. placebo; order was CLON + MPH > CLON > MPH
•• Mean doses of each drug were lowMean doses of each drug were low::0.250.25 CLONCLON // 2626 MPHMPH
• Adverse Effects: No difference in % of MPH (20%),CLON (26%) and PBO (22%) groups with worsening oftics
• There were no safety issues, particularlycardiovascular

Meta-Analysis: Treatment of Attention Deficit HyperactivityDisorder in Children with Comorbid Tic Disorders
• Aim: To determine relative efficacy of medications totreat ADHD and tic symptoms in children with bothTD and ADHD.
• Design: PubMed search for all double blind, RCTs inchildren with ADHD and tics using random effectsmeta-analysis with standardized mean difference asprimary outcome for effect size.
• Results: N=9 studies with 477 subjects. N=6medications: dextroamphetamine, methylphenidate,alpha 2 agonists (clonidine and guanfacine),desipramine, atomoxetine, and deprenyl.
(Bloch, M. Panza, K. Landeros-Weisenberger, A. andLeckman, J. JAACAP. 2009; 48 (9);884-893)

Meta-Analysis: Treatment of Attention Deficit HyperactivityDisorder in Children with Comorbid Tic Disorders
• Results: Methylphenidate, alpha 2 agonists,desipramine, and atomoxetine showed efficacy inimproving ADHD symptoms in children with comorbidtics.
• Alpha agonists and atomoxetine significantlyimproved comorbid tics
• Supra-therapeutic doses of dextroamphetamineincrease tics.
• There is no evidence that methylphenidate worsenedtic severity in the short term.
(Bloch, M. Panza ,K. Landeros-Weisenberger, A. andLeckman, J. JAACAP. 2009; 48 (9);884-893)

Methylphenidate effect on ADHD (A) and tic severity (B)
Bloch, JAACAP, 2009

Alpha-2 agonist effect on ADHD (A) and tic severity (B)
Bloch, JAACAP, 2009

Meta-Analysis: Effectiveness of medication in treatingADHD and tic disorders
Bloch, JAACAP, 2009

Meta-Analysis: Treatment of Attention Deficit HyperactivityDisorder in Children with Comorbid Tic Disorders
• Conclusion: Methylphenidate seems to offer the bestand most immediate improvement of ADHD and doesnot seem to worsen tics.
• Alpha agonists offer the best combination ofimprovement in both tics and ADHD symptoms.
• Atomoxetine and desipramine provide additionalevidence based treatment of ADHD in children withcomorbid tics.
• Supra-therapeutic doses of dextroamphetamineshould be avoided.
(Bloch, M. Panza,K. Landeros-Weisenberger, A. andLeckman, J. JAACAP. 2009; 48 (9);884-893)

56
Comprehensive Behavioral Intervention for Tics Study(CBITS) or Habit Reversal Therapy(Piacentini, J. Woods, D. Scahill et al. JAMA; 2010;303(19):1929-1937)
Two parallel studies compared behavior therapy to supportivetherapy (ST)Child study: 126 children (ages 9-17) with TD/CTD; JAMA;2010Adult study: 120 children and adults (ages 16+) withTD/CTD: Arch Gen Psych; 2012Three phases:
1) Awareness training2) Competing response training3) Social support
**In CBIT child study, children with ADHD did not do aswell (lower ES) as those without ADHD…….

57
Responder Status at Week 10: Effect Size 0.68(CGI-Improvement = 1 or 2) Courtesy of Piacentini, J. AACAP 2009
CBIT PSTp < 0.0001

Testing Tic Suppression: Comparing the Effects of Dexmethylphenidateto No Medication in Children and Adolescents with ADHD and TD
Aim: To test whether single dose, immediate release (IR)dexmethylphenidate (d-MPH) can facilitate behavioral ticsuppression in youth with ADHD and TD
Hypothesis: D-MPH would facilitate tic suppressioncompared to no medication
Design: N=10 children in a random cross-over design wereadministered d-MPH on one visit and no medication onanother.
Following baseline, subjects were reinforced for suppressingtics using a behavioral reinforcement tic suppressionparadigm (Woods et al; 2005)
Children were reinforced for suppressing tics with tokensfrom a “Tic Detector” for 5 minute intervals
(Lyon,G. Samar,S. Conelea, C. et al JCAP; 2010; (4) 283-289)

Sociodemographic Data: Testing Tic Suppression
Lyon, JCAP, 2010

60

Testing Tic Suppression: Yale Global Tic Severity ScaleSubscale Scores by Study Condition
Lyon, JCAP, 2010

Testing Tic Suppression: Mean number of tics perminute under the non-medication and one-time dose ofd-MPH conditions during the TSP
Lyon, JCAP, 2010
Testing Tic Suppression: Comparing the Effects of Dexmethylphenidateto No Medication in Children and Adolescents with ADHD and TD
Results: Relative to no medication, tics werereduced when subjects were given a single doseof d-MPH.
Behavioral reinforcement of tic suppressionresulted in lower tic rates compared to baseline,but d-MPH did not enhance this suppression.
Conclusion: Results replicate prior studies ofbehavioral tic suppression in youth with TDwithout ADHD
Tic reduction (vs. exacerbation) with acute d-MPHchallenge.
(Lyon,G. Samar,S. Conelea, C. et al JCAP; 2010; (4) 283-289)

New Combination Pharmacotherapy and Behavioral TreatmentStudy: Improving Tic-Related Response Inhibition: Comparing theEffects of MPH alone vs. MPH + HRT in Children and Adolescentswith ADHD and CTDs

HRT2 Subjects: Preliminary Data
Subject Phase A(Stimulant
optimization)
Phase B(HRT)
EndpointADHD
(CGI 1 or 2)
EndpointTics
(CGI 1 or 2)
1 Guanfacine +Dex-MPH
No Yes Yes
2 Dex-MPH Yes Yes Yes3 Lis-
dexamphetamine
No Yes Yes4 Guanfacine +
Oros MPHYes Still in
treatmentStill intreatment
5 Clonidine Not yet PreliminaryParent
management
PreliminaryParent
management6 Guanfacine;
could nottolerate
stimulant orclonidine
monotherapy
Not yet PreliminaryParent
management
PreliminaryParent
management

Tics, Tourette’s Disorder, and ADHD Through the Lifespan:Summary**There is bi-directional overlap of ADHD and Tic Disorders, including
common neural substrates and phenomenology.• Prevalence of ADHD in TD in clinically referred samples is 50-75%,
and tics in ADHD patients 10-30%.• ADHD symptoms persist, but tic symptoms tend to remit over time.• Much of the associated psychopathology (behavioral, neurocognitive) in
Tourette’s Disorder is secondary to ADHD• Most clinically referred patients with ADHD and tic disorders will need
treatment for ADHD, and tics may or may not need treatment.• Alpha agonist is recommended as initial pharmacotherapy for ADHD +
tics when tics are the primary issue• Recent meta-analysis reveals that methylphenidate is effective in
treatment of ADHD in children with ADHD and tics, and does notincrease tics in the short run
• Future study directions: combination pharmacotherapy and behavioraltreatment (HRT), long acting stimulants and alpha agonists in ADHD/tic disorders, predictors of tic exacerbations on stimulants


• Icahn School of Medicine at Mount Sinai• Tics and Tourette’s Clinical and Research Program/Division of Tics, OCD and
Related Disorders (DTOR)• Wayne Goodman, M.D.
Professor and Chair, Department of Psychiatry, Mount Sinai School of Medicine,• Director, Division of Tics, OCD and Related Problems• Vilma Gabbay, M.D. M.S• Associate Professor, Department of Psychiatry,• Director, Pediatric Mood and Anxiety and Disorders Clinical Research Program• Dorothy Grice, M.D.• Professor, Department of Psychiatry, Director, Pediatric OCD Program• Matthew Hopperstad, M.D• Assistant Professor, Department of Psychiatry• Ariz Rojas, Ph.D.• Assistant Professor, Department of Psychiatry• Resham Gellatly, B.A. Research Coordinator, MSSM• Laura Ibanez, B.A. Research Assistant (Nathan Kline Institute and MSSM)• Lindsay Farmer. B.A., Research Intern, MSSM
• NYU School of Medicine Collaborators:• Ruth Nass, M.D. . Xavier Castellanos, M.D. Jonathan Brodie, M.D. Ph.D. Gholson
Lyon, M.D. Ph.D. Stephanie Samar, M.A.
68





























