Embed Size (px)
Citation preview

TIBIAL ANTIVARUS CLOSING WEDGE OSTEOTOMY
MICHAEL J. STUART, MD
Antivarus lateral closing wedge osteotomy of the proximal tibia is a time-tested surgical technique. Redistribution of weight-bearing forces within the knee joint decreases the medial compartment load and the varus knee moment. Young or middle-aged patients as well as athletes with medial unicompartmental arthritis, posterolateral instability and varus thrust, or chronic anterior cruciate ligament deficiency and varus malalignment may be candidates. The indications have expanded recently to include patients with a varus mechanical axis who are undergoing periosteal resurfacing, autogenous chondrocyte implantation, meniscal transplantation, osteochondral grafting, or multiple subchondral bone microfractures. The osteotomy is performed between the knee joint and the tibial tubercle by removing a laterally based bone wedge. The construct is stable because of osteoclasis of the medial tibial cortex, an intact periosteal hinge, and excellent apposition of broad cancellous bone surfaces. Early knee motion is possible and bone healing is expeditious. Complications can be averted by careful patient selection, precise preoperative planning, and meticulous surgical technique. The weight-bearing line method uses a full-length standing radiograph to determine the desired correction angle. The osteotomy is performed with fluoroscopic guidance through a limited exposure. Low-profile step staples provide satisfactory fixation, and no bone grafting is required. Tibial antivarus lateral closing wedge osteotomy is a useful and reliable surgical technique. KEY WORDS: osteotomy, varus, realignment, arthritis
Balance of the knee joint represents a complex interaction of st:atic and dynamic mechanical factors. Static factors include the alignment of the limb segments, the geometry of the joint surfaces, and the degree of ligamentous laxity. Dynamic factors include neuromuscular regulation and proprioceptive control during gait and stair climbing. Varus malalignment is common, especially because osteo- arthritis often involves the medial compartment of the knee. A major contribution to the overall deformity in osteoarthritis is an increase in the tibial condylar-plateau angle that reflects loss of medial compartment articular cartilage, bone, or medial meniscus along with lateral collateral ligament stretching. The resultant varus align- ment of the limb concentrates force at the medial portion of the joint.
Antivarus or valgus-producing tibial osteotomy is a surgical technique that results in redistribution of weight- bear:~ng forces within the knee joint. The medial compart- ment load and the varus knee moment are decreased. Osteotomy of the proximal tibia was first performed by Jackson I in 1958 and was popularized by Coventry 2-5 in the 1970s. Proper patient selection and satisfactory postopera- tive correction have been correlated with a greater than 90% success rate at 10 years after surgery. 6 Deterioration of results is most often attributed to arthritis progression rather than varus deformity recurrence. 7 This procedure remains a viable surgical option for unicompartmental osteoarthritis in selected patients. Total knee arthroplasty
From the Department of Orthopedics and the Sports Medicine Center, Mayo Clinic, Mayo Foundation, Rochester, MN.
Address reprint requests to Michael J. Stuart, MD, Mayo Clinic, 200 First St SW, Rochester, MN 55905.
Copyright o 2000 by W.B. Saunders Company 1060-1872/00/0801-0004510.00/0
has supplanted realignment osteotomy as a primary treat- ment for many middle-aged patients with gonarthrosis. However, the indications for an osteotomy have broad- ened to include younger patients and athletes with posttrau- matic degenerative arthritis. The procedure may also be performed in combination with ligament reconstruction, articular cartilage regeneration, and meniscal transplanta- tion in a knee with associated malalignment.
INDICATIONS AND CONTRAINDICATIONS
Antivarus osteotomy is primarily indicated for pain relief and /or mechanical axis correction as an adjunct to other reconstructive knee procedures. Patients with medial unicompartmental tibiofemoral gonarthrosis, posterolat- eral instability and varus thrust, or chronic anterior cruci- ate ligament (ACL) deficiency and mild medial compart- ment degenerative arthritis may be candidates for an osteotomy. The indications have expanded recently to include patients with a varus mechanical axis who are undergoing periosteal resurfacing, autogenous chondro- cyte implantation, meniscal transplantation, osteochondral grafting, or multiple subchondral bone microfractures. Patients should have pain and tenderness localized to the medial joint line, less than 10 ° of terminal knee extension loss and greater than 90 ° of knee flexion.
Contraindications include patients with a diagnosis of inflammatory arthritis, tricompartmental degenerative ar- thritis, obesity, or previous lateral menisectomy, s This procedure should also be avoided if there is radiographic evidence of severe medial tibial bone loss or pronounced joint line obliquity due extreme varus angulation of the proximal tibia and excessive valgus angulation of the distal femur.
Operative Techniques in Sports Medicine, Vol 8, No 1 (January), 2000: pp 27-31 2 7
ANTIVARUS CLOSING WEDGE
The osteotomy is performed between the knee joint and the tibial tubercle by removing a laterally based bone wedge. The lateral closing wedge osteotomy results in a stable construct attributable to osteoclasis of the medial tibial cortex, an intact periosteal hinge, and excellent apposition of broad cancellous bone surfaces. Functional lengthening of the patellar tendon, which occurs with an opening wedge osteotomy in this location, is avoided. Early knee motion is possible and bone healing is expedi- tious. The closing wedge technique does shorten the leg, decrease the distance from the tibial plateau to the tibial tubercle, increase the laxity of the lateral collateral liga- ment (LCL), increase the quadriceps angle, and change the position of the plateau relative to the tibial axis. Closure of the osteotomy requires division of the proximal tibiotibu- lar joint ligaments, resection of the medial fibular head, resection of the entire fibular head, or osteotomy of the fibular shaft. Mobilization of the proximal tibiofibular joint by partial head resection preserves the ligament and tendon attachments. Fibular head resection requires reat- tachment of the conjoined tendon (biceps and LCL). Although suture fixation and subsequent healing are re- quired, advancement does allow tensioning of these struc- tures. If posterolateral instability is present, LCL tension- ing must be combined with the lateral closing wedge; otherwise, a medial opening wedge technique should be employed. Fibular shaft osteotomy places the peroneal nerve at risk as a result of surgical dissection or excessive retraction. The osteotomy should not be performed in the zone located between 7 to 15 cm from the fibular head.
Numerous surgical guides, instruments, and fixation devices have been developed in an attempt to improve the ease and accuracy of performing a closing wedge oste- otomy. These innovations have some merit but also require more extensive surgical dissection and increased cost. The modified Coventry technique uses fluoroscopic guidance, a limited exposure, and two-step staples to achieve the same surgical goals.
Weight-Bearing Line Method
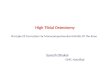
Divide the lateral tibial plateau from 0% to 100% from the medial to the lateral margin. Draw lines from the center of the femoral head and the center of the tibiotalar joint to the 62% coordinate. The angle formed by these 2 lines equals the angle of correction (Fig 1). The use of standing radiographs can overestimate the magnitude of correction because of osseous defects and /or attenuated ligaments. Each millimeter of lateral tibiofemoral joint separation causes approximately 1 ° varus angular deformity. Com- pare the amount of lateral joint space opening (in millime- ters) with the contralateral knee and subtract the difference from the calculated angle (1 ° /mm) to avoid overcorrection.
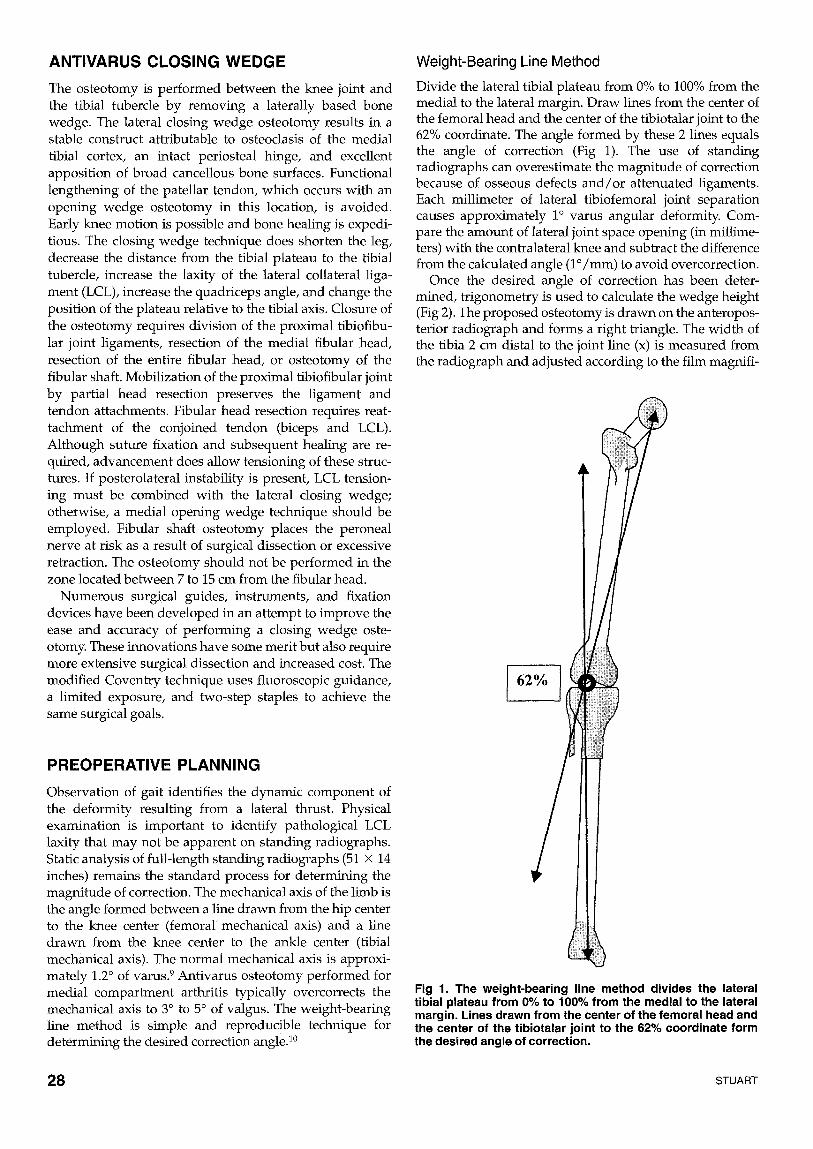
Once the desired angle of correction has been deter- mined, trigonometry is used to calculate the wedge height (Fig 2). The proposed osteotomy is drawn on the anteropos- terior radiograph and forms a right triangle. The width of the tibia 2 cm distal to the joint line (x) is measured from the radiograph and adjusted according to the film magnifi-
J
PREOPERATIVE PLANNING
Observation of gait identities the dynamic component of the deformity resulting from a lateral thrust. Physical examination is important to identify pathological LCL laxity that may not be apparent on standing radiographs. Static analysis of full-length standing radiographs (51 × 14 inches) remains the standard process for determining the magnitude of correction. The mechanical axis of the limb is the angle formed between a line drawn from the hip center to the knee center (femoral' mechanical axis) and a line drawn from the knee center to the ankle center (tibial mechanical axis). The normal mechanical axis is approxi- mately 1.2 ° of varus. 9 Antivarus osteotomy performed for medial compartment arthritis typically overcorrects the mechanical axis to 3 ° to 5 ° of valgus. The weight-bearing line method is simple and reproducible technique for determining the desired correction angle. 1°
Fig 1. The weight-bearing line method divides the lateral tibial plateau from 0% to 100% from the medial to the lateral margin. Lines drawn from the center of the femoral head and the center of the tibiotalar joint to the 62% coordinate form the desired angle of correction,
28 STUART

x
y / x = t a n A
y = x ( tan A)
Fig 2. Wedge length calculation: the trigonometric method calculates the wedge height (y) using the tangent formula. The width of the tibia (x) is multiplied by the tangent of the desired correction angle (A).
cation determined by radiographic markers. The tangent of tlq.e correction angle (A) is obtained from a standard table or a calculator. The formula states that the tangent of the angle equals the length of the opposite side divided by the length of the adjacent side. Therefore, the wedge height is calculated by multiplying the width of the tibia (x) and the tangent of the correction angle (A).
CLOSING WEDGE OSTEOTOMY TEC, HNIQUE
The patient is placed supine on the image table with a sandbag under the hip and a tourniquet on the thigh. The C-arm is brought in from the contralateral side of the table to verify fluoroscopic visualization of the hip, knee, and ankle. After standard prep and draping, the leg is exsangui- nated and the tourniquet is inflated. The knee is flexed 90 ° during the exposure. A slightly oblique skin incision is made from the proximal anterior fibular head to the proximal lateral margin of the tibial tubercle (Fig 3). This exposure avoids the LCL and the peroneal nerve and does not interfere with a longitudinal anterior incision in the future if necessary.
The anterior compartment musculature is subperioste- ally dissected from the proximal lateral tibia. A bent malleable retractor is placed beneath the patellar tendon. Dissection is carried posteriorly to the proximal tibiofibu-
lar joint. The articular cartilage and subchondral bone from the medial fibular head are removed with a curved osteotome. A bent malleable retractor is placed around the posterior tibia directly on bone to protect the neurovascu- lar structures (Fig 4).
The knee is extended and the C-arm is positioned to obtain an anteroposterior fluoroscopic view. A Keith needle is placed at the lateral joint space. A Steinmann pin is inserted 2.0 cm distal to the joint line. The pin is driven across the tibia parallel to the articular surface under fluoroscopic guidance until it engages the medial cortex. A second Steinmann pin is inserted at the calculated perpen- dicular distance from the first pin. This pin is driven across the tibia under fluoroscopic guidance to meet the first pin at the medial cortex (Fig 4).
The C-arm is withdrawn, the knee is flexed, and the malleable retractors are replaced. An oscillating saw is used to make the proximal cut by following the undersur- face of the proximal pin. The saw blade is tilted to match the posterior slope of the tibial plateau as visualized on the lateral radiograph. The saw is then used to make the distal cut following the upper surface of the distal pin. The saw blade is tilted to match the posterior slope of the proximal cut. Asymmetrical bone resection will change the tibial plateau inclination in the sagittal plane. A biplanar oste- otomy can be performed if the surgeon desires to increase the anterior or posterior slope of the tibial articular surface.
The bone wedge is removed so that the remainder of the osteotomy can be made under direct visualization (Fig 5). Anterior and posterior cortical bone must be completely removed for the osteotomy to close. The final 25% of the osteotomy is completed with an osteotome, and the bone is removed with a very small curette (Fig 6). The extent of bone removal is verified with fluoroscopy to avoid inadver- tent fracture into the medial compartment at the time of osteotomy closure. The medial cortex is perforated with the Steinmann pin in 3 sites to facilitate the osteoclasis while maintaining the medial periosteal hinge. A valgus stress is applied with the knee in extension to close the gap. A crack is often heard as the medial cortex fractures. Apposition of the bone surfaces and the limb alignment are checked with fluoroscopy. The cautery cord is stretched
Fig 3. The skin incision is slightly oblique extending from the proximal anterior fibular head to the proximal lateral margin of the tibial tubercle.
Fig 4. Malleable retractors are placed along the anterior and posterior tibial cortices. Steinmann pins are inserted under fluoroscopic guidance to outline the osteotomy wedge.
TIBIAL ANTIVARUS CLOSING WEDGE OSTEOTOMY 2 9

Fig 5. The bone wedge, including the anterior and posterior cortices, is removed to allow direct visualization and promote osteotomy closure.
from the center of the femoral head to the center of the ankle under fluoroscopic guidance. The position of the weight-bearing line is observed. Inadequate correction is remedied by slightly compressing the lateral Cancellous bone or by additional bone resection.
Two step staples are typically used for fixation. The correct size of the step off is determined by fitting the staple backward against the osteotomy site. The appropri- ate staple is then loaded onto the holder. The first staple is placed as posterior as possible, which is adjacent to the fibular head. A 3.2-ram drill bit is used to make a starter hole for the proximal tine. The best position for this hole is determined with fluoroscopy. The staple is partially driven while applying axial compression, valgus stress, and coun-
terpressure to keep the osteotomy closed and to avoid medial translation of the tibia. A second starter hole is made with the drill just inferior to the distal tine of the staple, which results in slight compression of the oste- otomy. The staple impactor is used to complete the inser- tion while visualizing the parallel placement with fluoros- copy. The staple cannot be inserted too far or the proximal fragment cortex will fracture and the fixation will be compromised. A second staple is inserted more anteriorly by the same technique. Cancellous graft from the removed wedge can be placed at the osteotomy site between the staples if desired. Fluoroscopic visualization of the oste- otomy during varus-valgus stress testing confirms the integrity of the fixation and the medial periosteal hinge. Anteroposterior and lateral radiographs are obtained on the operating table to verify osteotomy closure, staple position, and femorotibial alignment (Fig 7). The tourni- quet is deflated and hemostasis is obtained. The anterior compartment fascia is loosely closed over a drain. A soft compressive dressing with plaster splints is applied.
POSTOPERATIVE CARE
Two or 3 days after surgery, a rehabilitation brace with an extension lock is placed. Partial weight bearing is allowed with the brace locked in full extension. The brace is unlocked for active full range of motion exercises 3 times daily. The patient is also instructed on ankle pumps, quad sets, and straight-leg lifts. The knee is reexamined 2 weeks after surgery to inspect for wound healing, swelling, and range of motion. Knee radiographs are performed at 4 weeks. Patients are allowed to bear full weight with the brace locked in full extension and may remove the brace for range of motion exercises. Knee examination and repeat radiographs are performed 8 weeks following sur- gery. Clinical union is usually evident, although a persis-
Fig 6. Fluoroscopic view facilitates completion of the oste- otomy using an osteotome while avoiding compromise of the medial tibial cortex.
Fig 7. Anteroposterior radiograph verifies closure of the osteotomy, satisfactory staple position, and accurate femoro- tibial alignment.
30 STUART

tent rad iographic lucent line is typical ly present at the os teo tomy site. Progressive resistance s t rengthening exer- cises and non impac t aerobic condit ioning are started. A full-length s tanding r ad iog raph is obta ined 3 months pos topera t ive ly to d o c u m e n t bone heal ing and l imb align- ment .
COMPLICATIONS
Complicat ions can be aver ted b y careful pa t ient selection, precise p reopera t ive planning, and met iculous surgical techn_ique. 1°45 Neurovascu la r injury is p reven ted by avoid- ance of peroneal nerve dissection, p l acement of a malleable retractor along the poster ior tibial cortex, knee flexion dur ing the osteotomy, and a we l l -padded pos topera t ive dressing. C o m p a r t m e n t s y n d r o m e is p reven ted by hemo- stasis, loose closure of the anter ior c o m p a r t m e n t fascia, and insert ion of a drain. Mainta ining p rox imal f r agment thicl~ness of at least 1.5 cm, ver i fy ing r emova l of the bone w e d g e fluoroscopically, and per fora t ing the media l tibial cortex before os teo tomy closure prevents intraart icular fracture. Failure of fixation is p reven ted by main tenance of an intact media l periosteal hinge, compress ion of the os teo tomy site, and sound purchase of the staple tines. Oppos i t ion of flat cancellous surfaces, stable internal fixa- tion, and protected weigh t bear ing prevents nonunion.
Correct ion of varus ma la l ignmen t is essential to the success of some l igament reconstruction, articular cartilage regenerat ion, and meniscal procedures . Tibial ant ivarus lateral closing w e d g e os teo tomy is a t echn ique-dependen t bu t reliable operat ion. Specific indications will continue to evolve as more experience is ga ined wi th other p rocedures such as the media l open ing w e d g e osteotomy.
REFERENCES
1. Jackson JP: Osteotomy for osteoarthritis of the knee. J Bone Joint Surg Br 40:826,1958
2. Coventry M: Osteotomy of the upper portion of the tibia for degenerative arthritis of the knee: a preliminary report. J Bone Joint Surg Am 47:984-990,1965
3. Coventry M: Stepped staple for upper tibial osteotomy. J Bone Joint Surg Am 51:1011, 1969
4. Coventry MB: Osteotomy about the knee for degenerative and rheumatoid arthritis. J Bone Joint Surg Am 55:23-48, 1973
5. Coventry MB: Proximal tibial varus osteotomy for osteoarthritis of the lateral compartment of the knee. J Bone Joint Surg Am 69:32-38, 1987
6. Coventry M, Ilstrup D, Wallrichs S: Proximal tibial osteotomy. A critical long-term study of eighty-seven cases. J Bone Joint Surg Am 75:196-201, 1993
7. Stuart MJ, Grace JN, Ilstrup DM, et al: Late recurrence of varus deformity after proximal tibia[ osteotomy. Clin Orthop 260:61-65, 1990
8. Morrey BF: Upper tibial osteotomy for secondary osteoarthritis of the knee. J Bone Joint Surg Br 71:554-559, 1989
9. Hsu RWW, Himeno S, Coventry MB, et al: Normal axial alignment of the lower extremity and load-bearing distribution at the knee. Clin Orthop 255:215-227, 1990
10. Dugdale TW, Noyes FI~ Styer D: Preoperative planning for high tibiaI osteotomy. The effect of lateral tibiofemoral separation and tibiofemo- ral length. Clin Orthop 274:248-264, 1992
11. Kettelkamp DB, Leach RE, Nasca R: Pitfalls of proximal tibial osteotomy. Clin Orthop 106:232-241, 1975
12. Engel GM, Lippert FG: Valgus tibiaI osteotomy: avoiding the pitfalls. Clin Orthop 160:137-143, 1981
13. Kirgis A, Albrecht S: Palsy of the deep peroneal nerve after proximal tibial osteotomy. An anatomical study. J Bone Joint Surg Am 74:1180- 1185, 1992
14. Soejima O, Ogata K, Ishinishi % et al: Anatomic considerations of the peroneal nerve for division of the fibula during high tibial osteotomy. Orthop Rev 23:244-247, 1994
15. Rubens F, Wellington JL, Bouchard AG: Popliteal artery injury after tibial osteotomy: report of two cases. Can J Surg 33:294-297,1990
TIBIAL ANTIVARUS CLOSING WEDGE OSTEOTOMY 31