Embed Size (px)
Citation preview

Preethi Polavarapu MD, Padmaja Akkireddy MD
Division of Diabetes, Endocrinology and Metabolism, Department of Internal Medicine, University of Nebraska Medical Center, Omaha, NE 68198
• Our case illustrates that patients with
preexisting Graves’ disease can develop
thyroiditis after receiving immune checkpoint
inhibitors, and hence, frequent monitoring with
thyroid function tests are needed
• Thyroid dysfunction is one of the
common immune-related adverse events
associated with immune checkpoint
inhibitors like Nivolumab
• Thyroiditis or primary hypothyroidism is
the most commonly reported
presentation. Graves’ disease is less
frequently reported
• We report a case of preexisting Graves’
disease patient on antithyroid meds who
developed thyrotoxicosis followed by
hypothyroidism after receiving Nivolumab
therapy.
CASE PRESENTATION
• 66 y/o female patient with newly
diagnosed metastatic melanoma
presented to us for evaluation of
abnormal thyroid test after her second
cycle of Nivolumab
• She has a long-standing history of
Graves’ disease and has been on
methimazole since her diagnosis
• She presented with weight loss,
palpitations, and tremors four weeks after
the start of Nivolumab
CONCLUSION
INTRODUCTION
Thyrotoxicosis from Nivolumab in a Patient with Preexisiting Graves’ Disease
• On exam, she was tachycardic with tremors
noted to outstretched hands and had diffusely
enlarged thyroid
DISCUSSION
• Endocrinopathies are the most common
immune-related adverse events
associated with the use of these agents,
with thyroid dysfunction being more
common
• Timeline for developing the thyrotoxic
phase is usually five weeks but can also
occur earlier, which is followed by the rapid
development of either euthyroid or
hypothyroid phase
• Management during the thyrotoxic phase
is usually beta-blockers
• Current guidelines recommend checking
thyroid function test before initiation of
therapy and every two weeks after the
diagnosis of thyrotoxicosis until they
become euthyroid or hypothyroid
• In patients who are euthyroid on treatment
guidelines recommend to follow thyroid
function test before every cycle
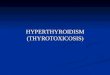
TEST 10/18 12/18 1/19 2/19 3/19
TSH
(0.4-4.5uIU/ml)
0.02 89.71 >100 16.973 4.63
Free T4
(0.8-1.6 ng/dl)
3.85 0.16 1.09
TSI
(<122%)
165
0
20
40
60
80
100
120
10/18/18 11/18/18 12/18/18 1/18/19 2/18/19
TSH
ng/
dl
DATE
Methimazole10mg daily
Methimazole Stopped
Levothyroxine 75mcg daily
Levothyroxine88mcg daily
Table 1: Thyroid Function Test
Figure 1: Treatment Course
Contact Info: Preethi Polavarapu ( [email protected] ) Padmaja Akkireddy ([email protected])