Embed Size (px)
Citation preview

Thyroid stormพญ.อนตตร ดาวราย
หนวยโรคตอมไรทอ

PP: ผปวยชายไทยคอาย 26 ป อาชพท าไร ภมล าเนา จ.นครราชสมา
CC: ไข ถายเหลวมา 7 วนกอนมารพ.
PI: 5 เดอนกอนมารพ.รสกเหนอยงาย ใจสนบอยๆ มอสน กนเกงขน เหงอออกมากกวาปกต นน.ลดลง 8 กก.ใน ชวง 5 เดอนน มคนทกวาคอโตขนแตไมไดไปพบแพทย

• 7 วนกอนมารพ. มไข ถายเหลวเปนน าปนเนอไมมมกเลอดปน วนละ 4-5 ครงๆละ 1 แกวทกวน มคลนไสอาเจยนวนละ 3 ครงๆละ 1 แกว เหนอยเพลยมาก รสกใจสนมากขนกวาเดม ตอนกลางคนตองนอน หนนหมอนสงๆ หลายๆใบ นอนราบแลวรสกอดอดตองลกขนนงบอยๆ มขาบวมขน 2 ขาง ญาตสงเกตวาผปวยดกระสบกระสาย อาการไมดจงพามารพ.

PH: ปฎเสธโรคประจ าตว ไมไดกนยาอะไรประจ า ไมเคยเจบปวยตองนอนรพ.มากอน ไมเคยผาตด ไมเคยแพยา แพอาหาร ไมเคยกนยาตม ยาหมอ ยาลกกลอน ยาสมนไพร ไมเคยใชสารเสพยตด ไมมอาการเจบทคอมากอน

Personal Hx: ไมสบบหร ดมเหลาตามงานสงสรรคFH: มลกชาย 1 คนแขงแรงด ปฎเสธประวตโรคไทรอยดในครอบครว
PE: V/S: BP 128/80 mmHg.,PR 120/min, RR 20/min, T 39˚CGA: A Thai man, good consciousness, look agitatedHEENT: not pale, anicteric sclera,
exophthalmos of both eyes,lid lag and lid retraction – present
JVP: engorgedThyroid gl: diffuse enlarged 45 gm,
soft consistency, smooth surface, not tender, bruit – present

Lymph node: can’t palpable Heart: apex at 5th ICS MCL, no heave, no thrill,
totally irregular HR 120/min, normal S1 S2,no murmur
Lungs: fine crepitation both lungsAbd: soft, not tender, liver – 2 FB below RCM,
liver span 15 cm., spleen – not palpable

Ext: warm and moist skin, fine tremor – present,no clubbing finger, pitting edema 2+ both legs, no pretibial myxedema
Neuro: agitated, good consciousness, other- WNL

Problem list
1. Fever with diarrhea and vomiting
2. Congestive heart failure
3. AF with RVR
4. R/O Thyrotoxicosis
Thyroid storm

CBC: Hb 12 g/dL, Hct 36%, WBC 9,800 /µL(N 72%, L 21%),
Plt 230,000/µL
TFT: FT3 15.6 pg/mL (normal 2.3-6.9 pg/mL),
FT4 4.8 ng/dL (normal 0.6-1.6 ng/dL),
TSH 0.021 mIU/L (normal 0.3-5.0 mIU/L)
BUN 20 mg/dL, Cr 1.2 mg/dL
Electrolyte: Na 138 mEq/L, K 4.2 mEq/L,
Cl 102 mEq/L, C02 22 mEq/L
Lab

Burch-Wartofsky-Score
1. Thermoregulatory dysfunction
Temperature ˚F (˚C) Scoring points
99–99.9 (37.2-37.7) 5
100–100.9 (37.8-38.2) 10
101–101.9 (38.3-38.8) 15
102–102.9 (38.9-39.2) 20
103–103.9 (39.3-39.9) 25
>/= 104.0 (>/= 40.0) 30

2. Central nervous system effects
Burch-Wartofsky-Score
Scoring points
Absent 0
Mild (agitation) 10
Moderate (delirium, psychosis, extreme lethargy
20
Severe (seizures, coma) 30
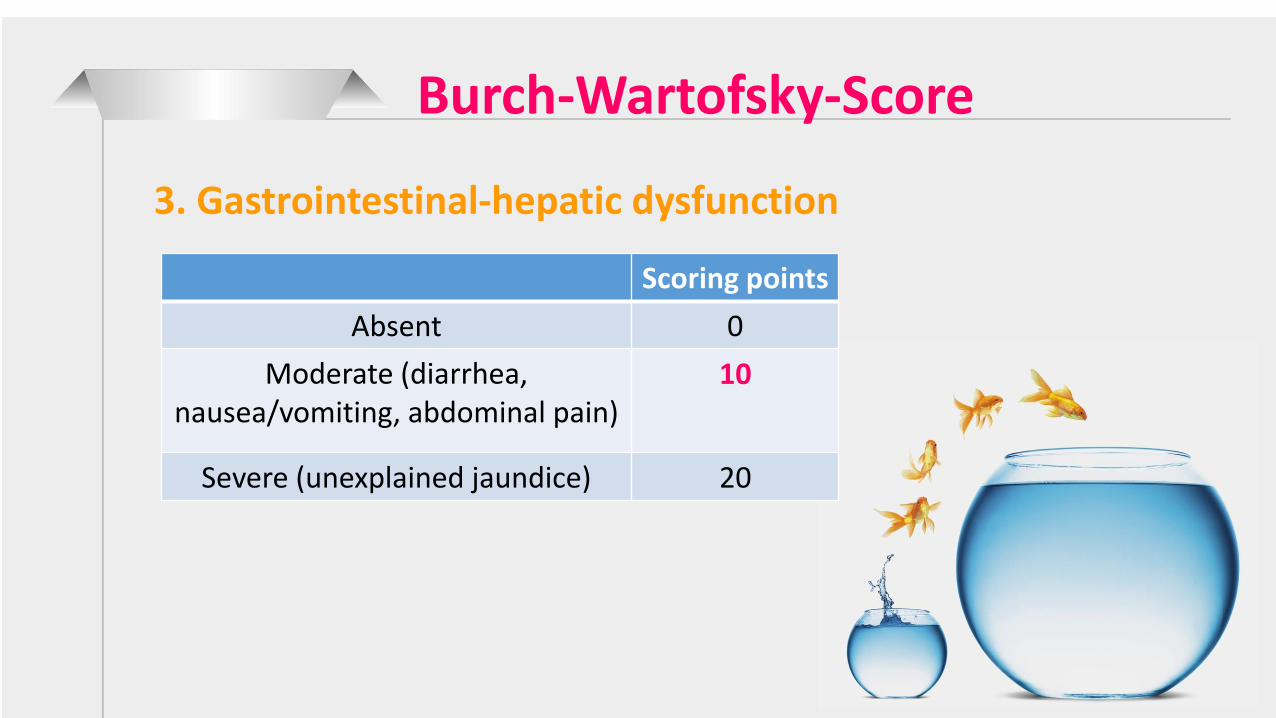
3. Gastrointestinal-hepatic dysfunction
Burch-Wartofsky-Score
Scoring points
Absent 0
Moderate (diarrhea, nausea/vomiting, abdominal pain)
10
Severe (unexplained jaundice) 20
Burch-Wartofsky-Score
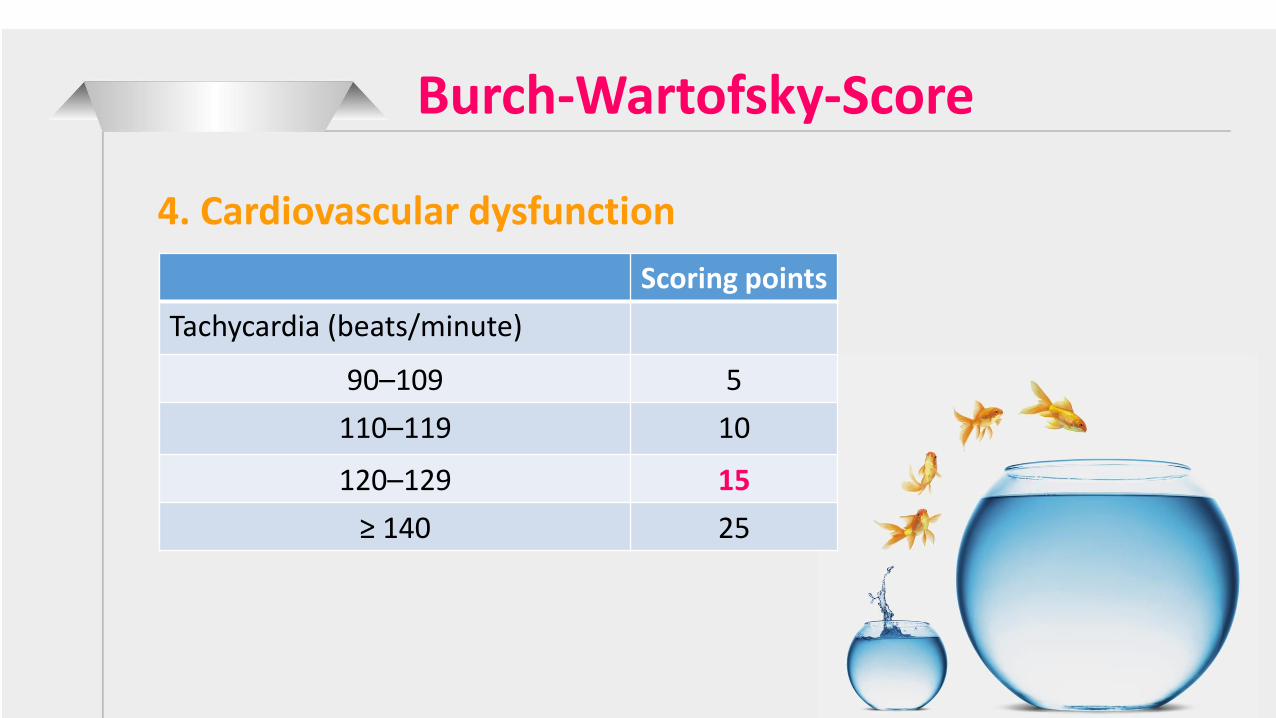
4. Cardiovascular dysfunction
Scoring points
Tachycardia (beats/minute)
90–109 5
110–119 10
120–129 15
≥ 140 25

Burch-Wartofsky-Score
4. Cardiovascular dysfunctionScoring points
Congestive heart failure
Absent 0
Mild (pedal edema) 5
Moderate (bibasilar rales) 10
Severe (pulmonary edema) 15
Atrial fibrillation
Absent 0
Present 10

5. Precipitating cause
Burch-Wartofsky-Score
Scoring points
Absent 0
Present 10

Scoring system
≥ 45 highly suggestive of thyroid storm
25-44 suggestive of impending storm
< 25 unlikely to represent thyroid storm
This patient’s score was 90

Treatment
1.Specific treatment
2.Supportive treatment
3.Treatment of precipitating cause
4.Definitive treatment

Specific treatment
Principles
Inhibition of new thyroid hormone production
Inhibition of thyroid hormone release
Inhibition of peripheral conversion

Inhibition of new thyroid hormone production
• PTU 200-250 mg po q 4 hr or
• MMI 20 mg po q 4 hr

Inhibition of thyroid hormone release
• Lugol’s solution 10 drops PO q 8 hr or
• SSKI 3 drops PO q 8 hr
Start after an antithyroid drug 1-2 hr
duration : 1 week
Iodine content Lugol’s solution :
6-8 mg/dropSSKI : 38 mg/drop
Inhibition of peripheral conversion
• Dexamethasone 2 mg IV q 6 hr
duration : 3-4 days

Fever - antipyretic drug
• Acetaminophen is a preferable choice
• Salicylates should be avoided
IV fluid - IV fluids with dextrose (isotonic
saline with 5% or 10% dextrose)
Beta blockers
Supportive treatment

• Discontinuation of an antithyroid drug
• Surgery
• Trauma
• Severe infection
• Excessive ingestion or IV administration
of iodine (e.g., radiocontrast agents,
amiodarone, radioiodine therapy)
• High dose of thyroid hormone
Precipitating factors
• Subtotal thyroidectomy
• Radioactive iodine ablation
Definitive treatment
Adrenal insufficiency
Anuttree Daorai,M.D.

Causes of Adrenal InsufficiencyPrimary
Acute Onset• Adrenal Hemorrhage
or Infarction
Slow Onset• Autoimmune Disease
- Adrenalitis
• Infectious Diseases
- Tuberculosis
- AIDS-Related
• Cancer
- Lymphoma
- Metastases
• Drugs
- Ketoconazole
- Etomidate
• Other
- CAH
-Adrenoleukodystrophy
Causes of Adrenal InsufficiencySecondaryAcute Onset
• Pituitary Apoplexy• Pituitary/hypothalamic
Surgery• Traumatic Brain InjurySlow Onset
• Autoimmune Disease - Lymphocytic
hypophysitis• Infectious Disease - Tuberculosis• Cancer - Pituitary tumors - Lymphoma
• Trauma or Other Injury - Traumatic Brain Injury - Subarachnoid
Hemorrhage - Radiation• Drugs - Megestrol Acetate

Causes of Adrenal InsufficiencySecondarySlow Onset
• Other - Discontinuation of exogenous glucocorticoids - Sarcoidosis - Empty Sella Syndrome

Clinical manifestation
Primary & Secondary AI
• Tiredness, mental depression, anorexia,
weight loss, fever
• Orthostatic hypotension
• Hypotension from hypomineralocorticoid
• Hyponatremia, normal gap met.acidosis,
hypoglycemia ,mild normocytic anemia,
lymphocytosis, eosinophilia, hypercalcemia

Clinical manifestation 10 vs. 20
Primary
• Hyperpigmentation
• Hyperkalemia
• Vitiligo,autoimmune
disorder
• CNS
adrenomyeloneuropathy
Secondary
• Pale skin without
marked anemia
• Other pituitary
hormone def.
Investigation1. Screening
• Early morning basal serum cortisol
- < 3 ug/dl, >18ug/dl
• Plasma ACTH
2. Stimulation test
• Insulin induced hypoglycemia
- RI 0.1 unit/kg iv
- 0, 30, 60, 90 min for cortisol, ACTH
• 250 ug ACTH(serum cortisol >18-20 ug/dl)
• 1 ug ACTH

• Glucocorticoid replacement
- Prednisolone 5 mg(2.5-7.5) OD
- Stress; Increase dose(2-3 times)
• Mineralocorticoid replacement in 1o AI
- Fludrocortisone 0.1mg(0.05-0.2) OD
- unnecessary if hydrocortisone > 100 mg/d
Treatment

• Dose (need to know previous
dosage, not only current dosage)
• Duration
• Dexamethasone > prednisolone >
hydrocortisone
• Also inhale, topical form
HPA axis suppression

Assumed to have HPA suppression
• Prednisolone(or equivalence) >20 mg/d > 3 wks
• Clinical Cushing’s syndrome from any steroid
dose

• Any patient who has received any
dose of glucocorticoid for < 3 weeks
• Patients who have received morning
doses of < 5 mg/day of prednisone
or its equivalent
• Patients treated with alternate-day
glucocorticoid therapy
No HPA suppression
• > 5 - < 20 mg/dl for > 3 weeks, one
can test for adrenal insufficiency or
give stress dose of glucocorticoid
Gray zone
Med Clin North Am 2001;85(5):1311-7
• In general, adrenal gland produces about
- normal basal secretion is 8 – 10 mg/d
- minor procedure or surgery : 50 mg/d
- major stress: 75 – 100 mg/d
Cortisol secretion during stress

Commonly used GCs

Guidelines for adrenal supplementation therapy
JAMA 2002;287(2):236-40

THANK YOU