Embed Size (px)
DESCRIPTION
Thorax and Lungs. Health History. Tobacco use (amount, duration, Pack year index) http://www.coquitline.org/ 2 nd hand smoke exposure Occupation/Exposure to pulmonary irritants Chemicals, vapors, dust, allergens, animals, smoke, asbestos, arsenic, coal dust, radiation) - PowerPoint PPT Presentation
Citation preview
Thorax and Lungs

Health History Tobacco use (amount, duration, Pack year
index) http://www.coquitline.org/
– 2nd hand smoke exposure Occupation/Exposure to pulmonary irritants
– Chemicals, vapors, dust, allergens, animals, smoke, asbestos, arsenic, coal dust, radiation)
PMH/FH of respiratory illness/disease/cancer or allergies– Pneumonia, TB, COPD, asthma, lung cancer– Pneumonia or influenza vaccine received?
Risk factors for TB: – HIV, substance abuse, low income or homeless,
resident of nursing home, shelter or prison, immigrant from country with high TB rate

Health History Do you have any shortness of breath?
(Dyspnea)– Occurs @ rest, with exercise, lying flat?
Have you heard any wheezing? Do you have a cough?
– Dry, productive, barking, etc..– http://www.youtube.com/watch?v=mXAxnZ4JJ6A
– Amount, color,& consistency of sputum. Presence of odor.
– Hemoptysis- coughing up blood (varies from blood streaked phlegm to frank blood)
Do you have chest pain with breathing? Have you recently had any pain in calves or
been on any long car or plane rides?

Sample Charting

Sample Electronic Charting
Respiratory SymptomsDifficulty breathingDyspnea with exertionDyspnea at restUnable to lie flatDifficulty coughingDifficulty clearing secretions

Inspection Observe symmetry, rate, rhythm, depth
and effort of breathing– Symmetry: Chest wall movement equal bilaterally– Rate: Adult 12-20 resp/min is normal
• Bradypnea: Slow (<12 per minute)• Tachypnea: Rapid (>20 per minute)
– Rhythm: Regular vs. irregular• Cheyne-Stokes, Kussmaul’s respirations, Biot’s
– Depth• Hypoventilation–rate slow, depth• Hyperventilation–rate rapid, depth deep
Respirations 16/min, symmetrical,relaxed and even

Inspection– Effort
• Unlabored vs. labored– Presence of retractions
» Suprasternal: above clavicle & sternum» Intercostal: between ribs» Subcostal: below lower costal margin» Substernal: Below Xiphoid process
– Presence of nasal flaring (inhalation) or grunting (exhalation)» Infants/children
– Use of accessory muscles» Neck/shoulders (ie Sternocleidomastoid & trapezius)» Abdominal (exhalation)
Respirations nonlabored.
http://www.youtube.com/watch?v=Hv68EQ3tCBIhttp://www.youtube.com/watch?v=J2R8MOoQtd8

Inspection
Body position– Relaxed vs. Upright/Tripod position
Color of skin, lips, nail beds– Even skin tone vs. cyanotic
Presence of clubbing
Patient relaxed. Skin and mucous membrane pink. Nail beds pink without clubbing in upper and lower extremities.

Inspect/Palpate Trachea Position
InspectShould be midline
PalpateFor tracheal shift
• Place finger in sternal notch and slip to each side.
Trachea midline.

Inspection
Wounds, scars, drains, tubes, dressings– Documentation must include location, size, amount of
drainage and discharge if present, and signs of inflammation.
– Additional terms to describe location:• Supraclavicular- Above the clavicles• Infraclavicular- Below clavicles• Interscapular- Between scapula• Infrascapular- Below scapula• Midaxillary line- Along line of armpit• Midclavicular- Along line in middle of clavicle
No wounds, scars, drains, tubes, or dressings. Or- No lesions.

Inspection
Shape of Chest :– Symmetrical vs. asymmetrical– Deformities
• Pectus carniatum, Pectus excavatum, Spinal deformitiies
– Normal AP diameter vs.. increased AP diameter
• Oval vs. barrel chest
• Ribs slope downward vs. more horizontal
• Barrel chest appears as if patient in continuous inspiratory position
Chest symmetrical without deformities. AP < transverse diameter


Kyphosis
Scoliosis

Palpation Assess for masses, tenderness, or crepitus– Subcutaneous emphysema-
air escapes form lungs into subcutaneous tissue
Assess chest expansion– Posteriorly place thumbs at
level of 10th rib & place palms on posterolateral chest.
– Approx 2 inches apart before inspiration. Feel thoracic expansion during quiet & deep inspiration. Look for symmetry.
Chest expansion symmetrical. No masses or tenderness.
http://www.youtube.com/watch?v=ygD93IKorEw

Palpation Tactile Fremitus
– Palpable vibrations transmitted through bronchopulmonary tree to chest when patient speaks
– Have patient repeat 99 or 1, 1, 1 while palpate with ulnar surface or ball of hand
• Decreased or absent when vibration impeded by obstructed bronchus, tumor, or separation of pleural surfaces by fluid (pleural effusion), fibrosis (pleural thickening), or air (pneumothorax)
• Increased with gross compression or consolidation (lobular pneumonia) without bronchus obstruction
Tactile fremitus equal bilaterally.

Palpation

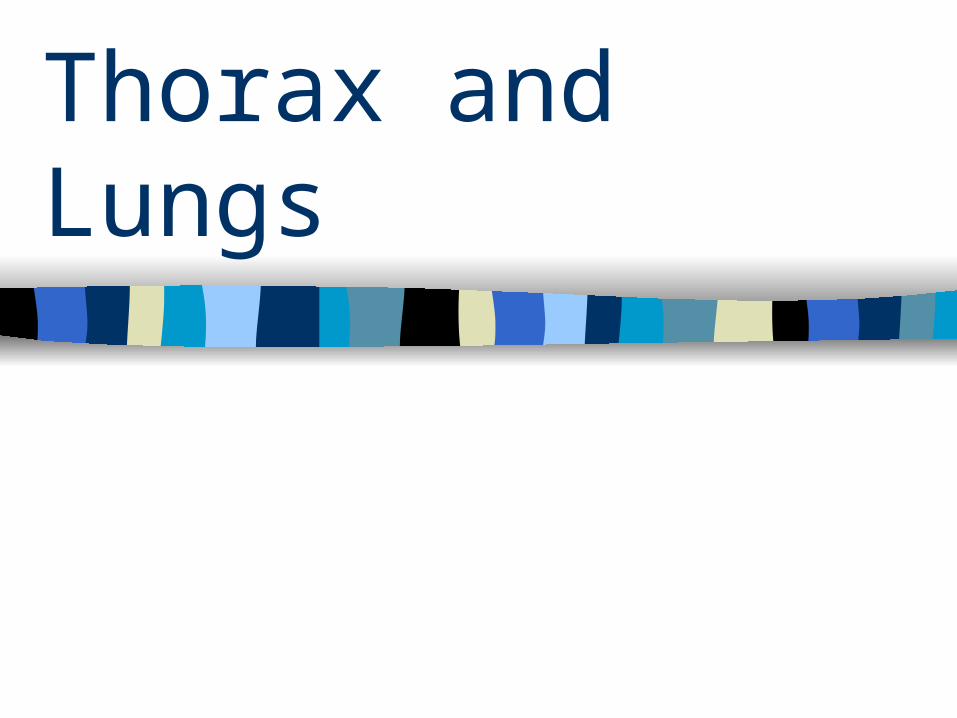
Percussion
Tapping of an chest to set chest wall and underlying tissues into motion
Helps to establish if underlying tissue air-filled, fluid-filled, or solid
Normal sound is resonance
Resonant to percussion over all lung fields.
Percussion
http://www.youtube.com/watch?v=PlUejZE6c_w

Auscultation Use diaphragm of stethoscope andhave patient breath out of their mouth.
– Peds- use smaller pediatric diaphragm or adult bell
Place stethoscope firmly on skin. Avoid movement because it may produce confusing sounds (i.e. clothing)
Auscultate at least one complete respiration Move from one side to the other Observe for hyperventilation, allow to rest if
needed Peds- transmission of sounds enhanced,
harder to localize sounds

Auscultation- Anterior Chest

Auscultation- Lateral Chest

Auscultation- Posterior Chest

Anatomy Review
Air: Mouth/Nose respiratory portion of larynx trachea right & left bronchus smaller bronchi smaller bronchioles alveolar duct individual alveoli

Auscultation Breath Sounds
– Bronchial (Tracheal)• Heard over trachea• Exp > insp• Loud, High pitch• Hollow quality
– Bronchovesicular• Heard over major bronchi• Insp = exp• Medium, Medium pitch• Blowing sound
– Peds in periphery
– Vesicular • Heard over lung
parenchyma/periphery• Insp > exp• Soft, Low pitch• Breezy quality
– Diminished

Auscultation
Adventitious Breath Sounds– Wheezes (Sibilant
wheeze)• High pitched, musical
sound heard during inhalation or exhalation
• Mild, moderate, severe
– Rhonchi (Sonorous wheeze)
• Low pitch snoring sound during inspiration or exhalation, but louder on exhalation
• May clear with coughing
Asthma

Auscultation
Bronchitis
Emphysema

Auscultation– Crackles/Rales
• Popping sounds heard on inhalation
• Fine– High pitched fine, short,
interrupted crackling sounds heard during end of inspiration
• Medium– Lower, more moist sounds
heard during middle of inspiration
• Course– Loud, bubbly sounds
heard during inspiration
http://www.med.ucla.edu/wilkes/intro.html

Auscultation
Pneumonia
Atelectasis

Auscultation
– Pleural friction rub• Dry, low pitched rubbing or grating sound on inhalation
and exhalation• Heard loudest over lower lateral anterior surface• Occurs with pleurisy or pleuritis
http://www.merckmanuals.com/professional/resources/multimedia/name/audio.html

Auscultation– Stridor
• High pitched, harsh sound heard on inspiration when trachea or larynx is obstructed
– Croup, foreign body, large airway tumor– http://www.youtube.com/watch?
v=QkaX83H31QY&feature=PlayList&p=0C59700763AFDD1E&playnext=1&index=8– http://www.youtube.com/watch?v=Z1_uKqmPyLA&feature=related

Auscultation
Breath sounds vesicular without adventitious sounds.
Or- Lungs sounds CTA in all lung fields without wheezes, rales, rhonchi, or rubs
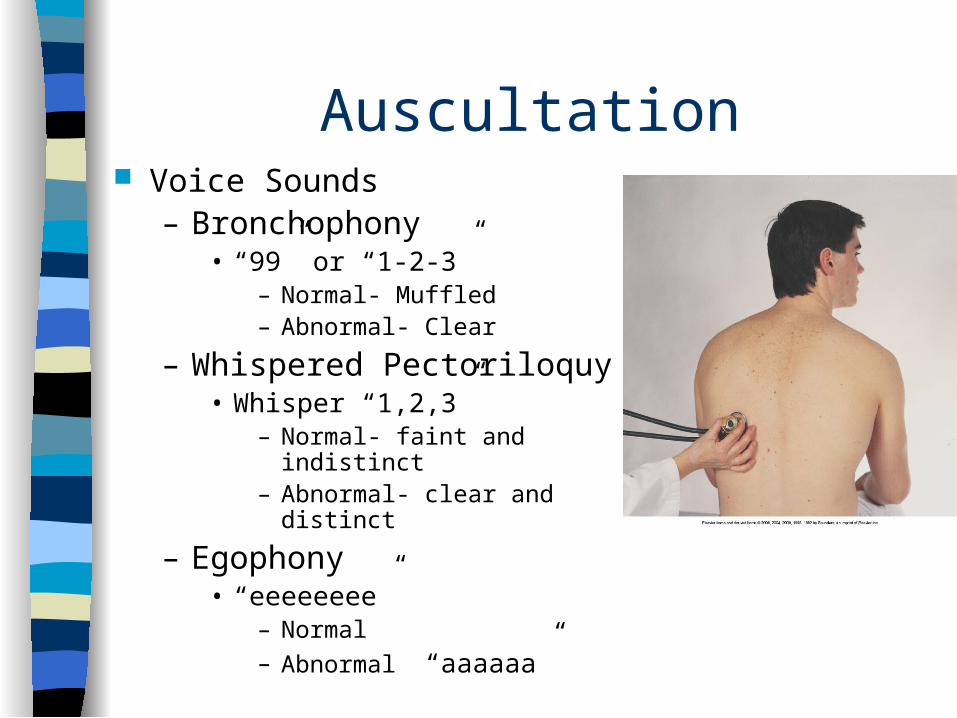
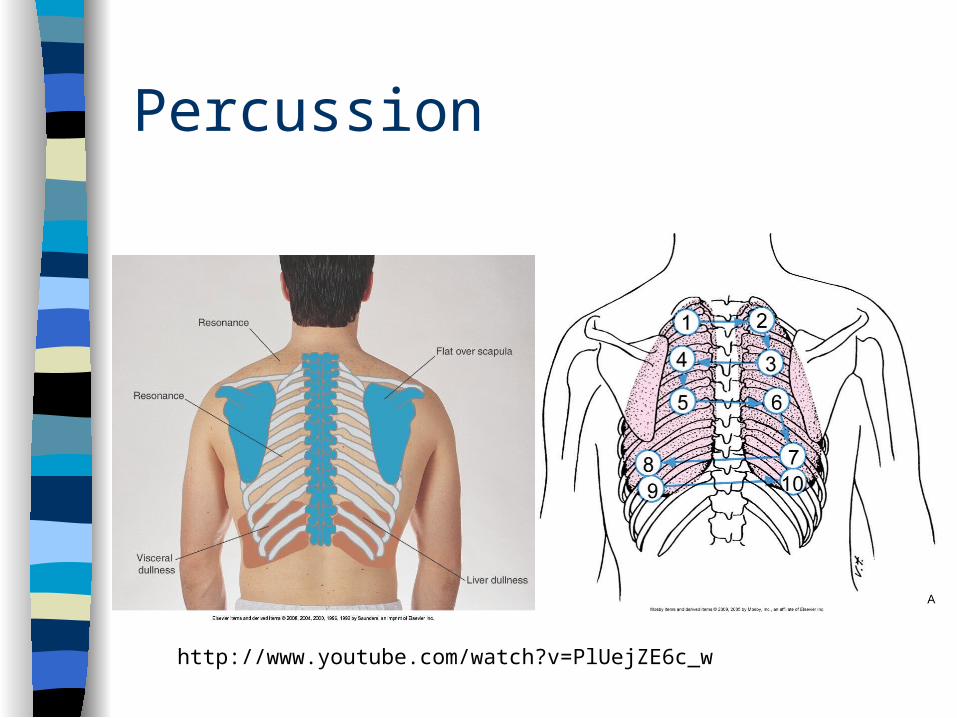
Auscultation Voice Sounds
– Bronchophony• “99” or “1-2-3”
– Normal- Muffled– Abnormal- Clear
– Whispered Pectoriloquy• Whisper “1,2,3”
– Normal- faint and indistinct– Abnormal- clear and distinct
– Egophony• “eeeeeeee”
– Normal– Abnormal “aaaaaa”

Bringing it all togetherhttp://www.youtube.com/watch?v=ygD93IKorEw
http://www.youtube.com/watch?v=nUJQvFXmTxQ&feature=related

Case StudyJuan Pablo comes to the Urgent Care Clinic for complaint of a cough that started about a week ago. He is accompanied by
his friends who work at the local chicken processing plant with him. He is from Mexico and has lived in the United States now for 2 years. He speaks English hesitantly. His family still lives in Mexico. He is 38 years old and states that he has been
in good health. He smokes one pack of cigarettes daily and occasionally drinks alcohol. Polly Curtis is a student nurse
assigned to do a health assessment and physical exam with the registered nurse. Polly is 25 years old and is in her second
year of nursing school.

Sample Charting

Sample Electronic Charting
Normal Parameters Met Breath sounds clear through all lung fields. Respirations unlabored, symmetrical,
regular rhythm and depth. No shortness of breath Cough effective Skin color within pt’s norm Sputum clear or white
Sample Electronic Charting
Sputum AmountScantSmallModerateLargeCopiousSwallowed
Sputum ColorYellowTanGreenPinkBrownBloody

Sample Electronic Charting
Sputum ConsistencyThinMucoidThickMucus plugFrothySmallTenaciousClots

Sample Electronic Charting
EffortLaboredShallowStridorAgonalAccessory muscle
useGasping laboredGrunting
Mechanical ventilated
Moderate laboredSlightly laboredNasal flaringPursed lipSplinting

Sample Electronic Charting
Retraction TypeSubsternalIntercostalSupraclavicularSubclavicularAbdominal
DepthDeepShallow
Mediastinal Shift?YesNo

Sample Electronic Charting
PatternIrregularBradypneaTachypneaGaspingGruntingKussmaulCheyne-stokes
Irregular or periodicParadoxicalAgonaApnea
Respiratory Pattern Comment: _______

Sample Electronic Charting
AuscultationClear throughoutAbsentDiminishedInspiratory wheezeExpiratory wheezeRalesRhonchiRub
Lung Characteristics Audible Decreased Diffuse Increased Slightly decreased Tight
Difference between anterior and posterior breath sounds: _______
Lung sound comments:___________

Additional Website