Embed Size (px)
Citation preview


PrePared By:
dr. MohaMMed Mohsen



Thoracic and Lung AssessmentEquipment: Stethoscope & Tape measures
Subjective data: Focus Questions:Difficulty in Breathing? Associated factors, relieving factors? Difficulty in Breathing when sleeping? Use of more than one pillow to sleep? Coughing? (productive- not productive) Sputum (type & amount) Dyspnea or shortness of breath ( at rest or exertion)? Chest pain Associated & precipitating factors? History of asthma, bronchitis, emphysema TB? Exposure to environmental inhalants Smoking

Thoracic and Lung AssessmentRisk Factors• Risk for respiratory disease related to
smoking• Immobilization or sedentary life style?• Aging • Environmental exposures• Morbid obesity• Risk for lung cancer related to cigarette
smoking • Genetic predisposition

Thoracic & Lung Assessment
Objective data: collected through: Inspection
Palpation
Percussion
Auscultation
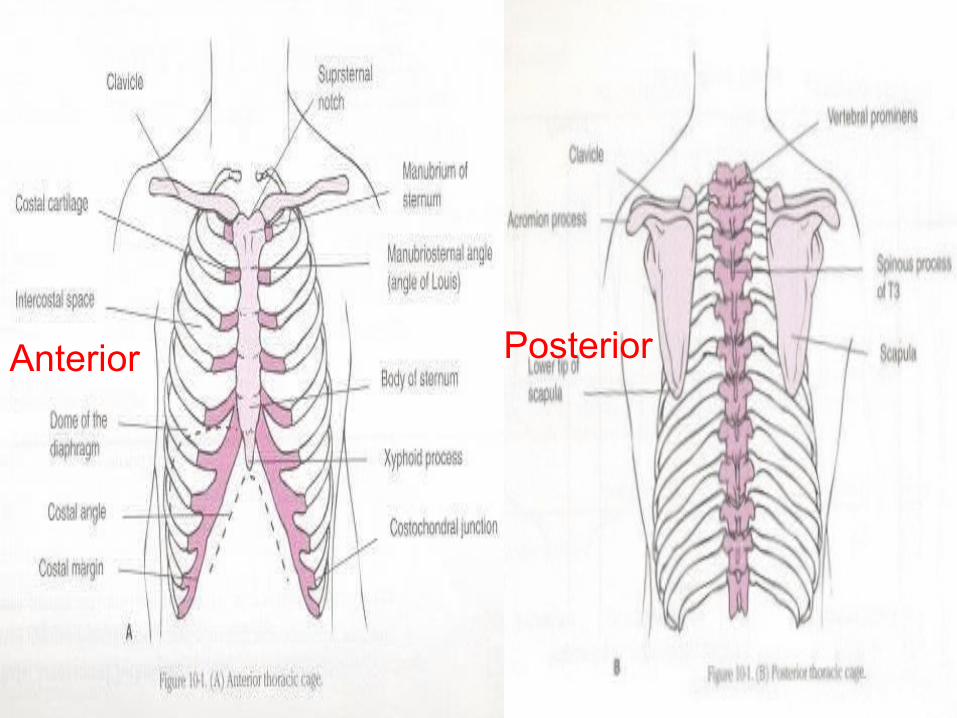
Anterior Posterior




I- inspection1- Shape:Expose patient chest Stand at the head or at the foot of the patient.
Normal shape: Symmetry Ratio of side to side diameter to anterior-
posterior diameter ( 7 : 5 )

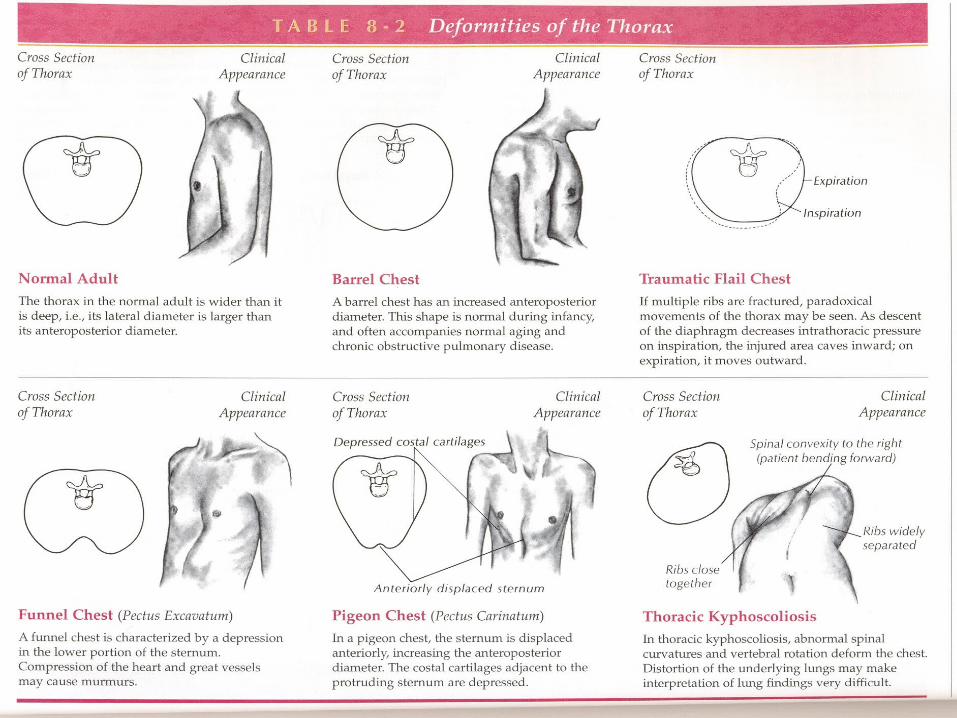
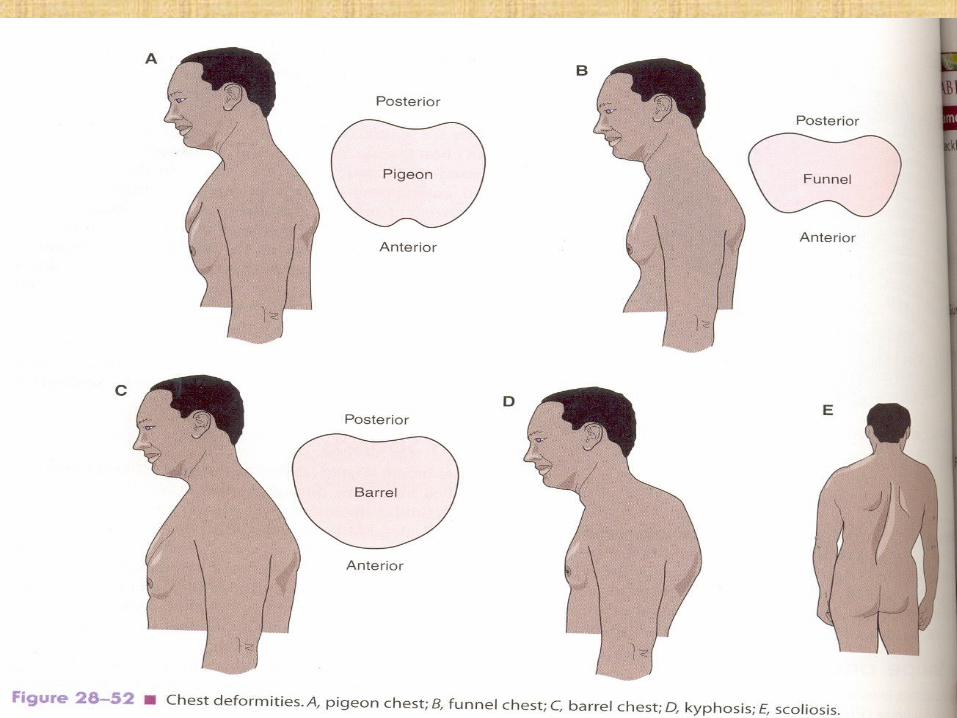
Abnormal shapeA. A- localized
B. B- generalized
A- localized localized bulge
Localized retraction
ask the patient to take deep breath
Side that move well is normal side and the another side is abnormal
Can be localized bulge as in cases of pleural effusion, tension pneumothorax or mass.
OR Localized retraction as in cases of collapse or fibrosis.
Cont,B- Generalized :
increase anterior-posterior diameter
- barrel
- alar
2- chest expansion : movement of the chest wall during respiration
Normal:- Symmetrical and better chest movement.
Abnormal :1- localized bulge or retraction.
2- Bilateral retraction : movement of both sides of chest is less than normal as in ( COPD )

3- Respiration
1- assess rate ( 12- 20 br/m).
2- Rhythm
3- types of respiration
Male: abdomino- thoracic respiration
Female : thoraco- abdomino respiration
4- accessory muscles: Normally : Don´t use in respiration Use accessory muscle when the patient is unable to breath. The most important muscle that assist with respiration “ lower
intercostal muscle”

4- pulsation1- Apex
2- Epigastric
3- Left parasternal pulsation
4- 2nd left space
5- 2nd right space
1- Apex
Q- what is the cause of absent apical beat?
Apex behind a ribs
COPD due to hyper inflation of the lung with air
Pleural effusion
Pericardial effusion
Thick wall of chest
Shifting of heart to other side

3- Left parasternal pulsation
Pulsated on 3rd, 4th & 5th left intercostal space just lateral to the sternum due to right ventricular conduction.
4- 2nd left space Equal pulmonary hypertension
5- 2nd right spaceIn case of systemic hypertension
5- any abnormality
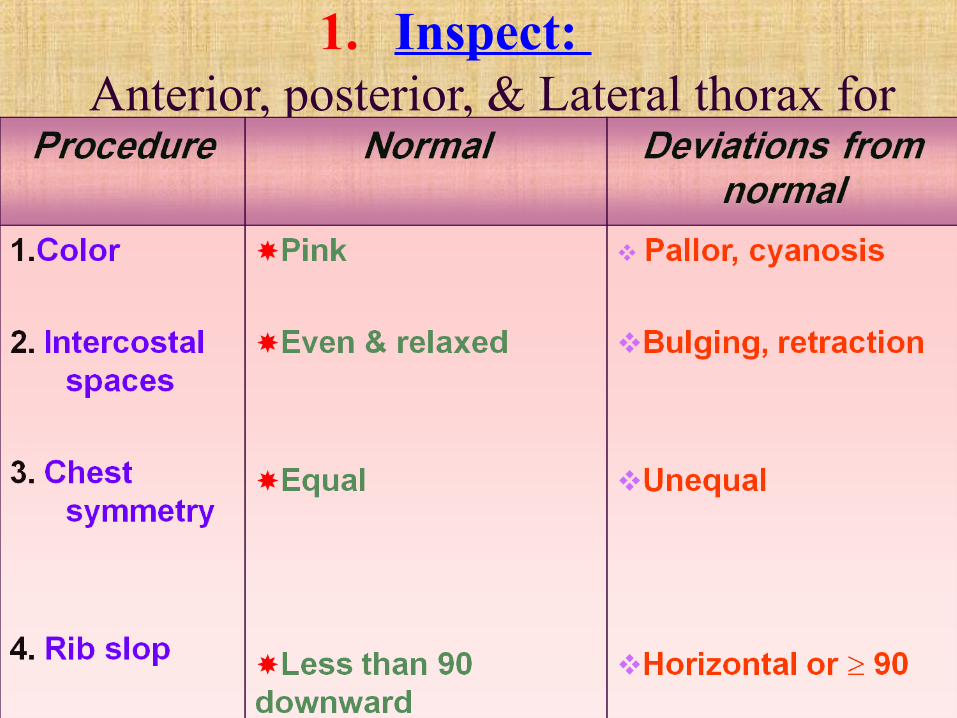
1. Inspect: Anterior, posterior, & Lateral thorax for

1. Inspect: (Continue)
Anterior, posterior, & Lateral thorax for

1. Inspect: (Continue)
Anterior, posterior, & Lateral thorax for

II- chest palpation1- chest palpation
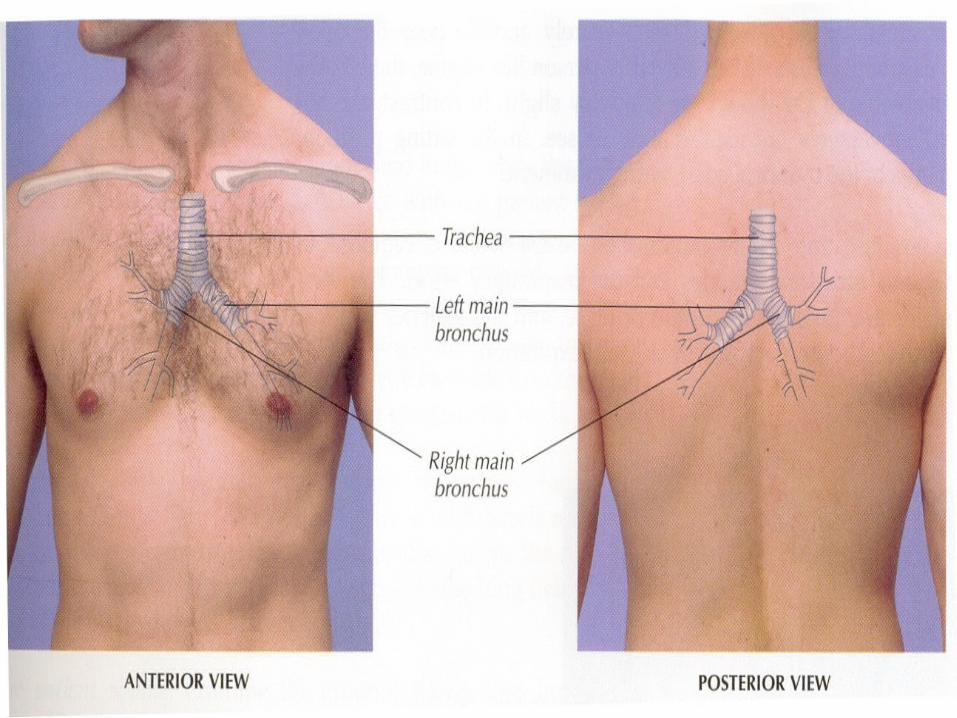
2- Tracheal examination
3- Tenderness
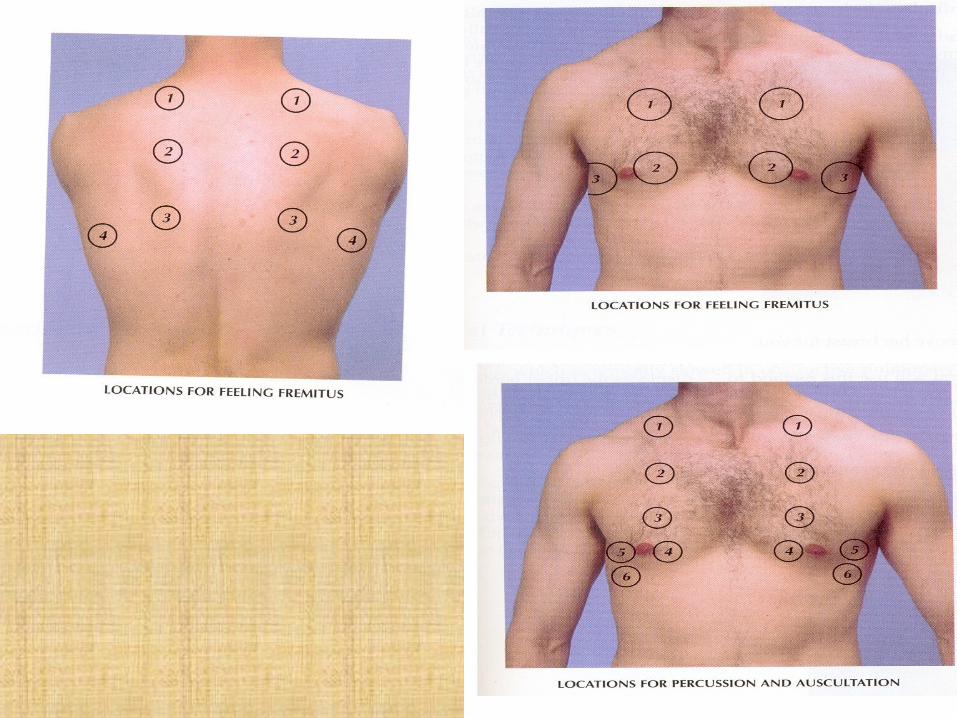
4- tactile vocal fremitus
5- Pulsation
6- Palpable sound
7- any abnormality

2. Palpation: Drape anterior chest & use fingers pads or palms
to palpate posterior chest
Have client fold arms across anterior chest & lean forward to ↑ area of lungs
Palpate, percuss, & auscultate posterior lung & thorax while the client is setting
Palpate, percuss, & auscultate lateral lungs & thorax while client is in the supine position
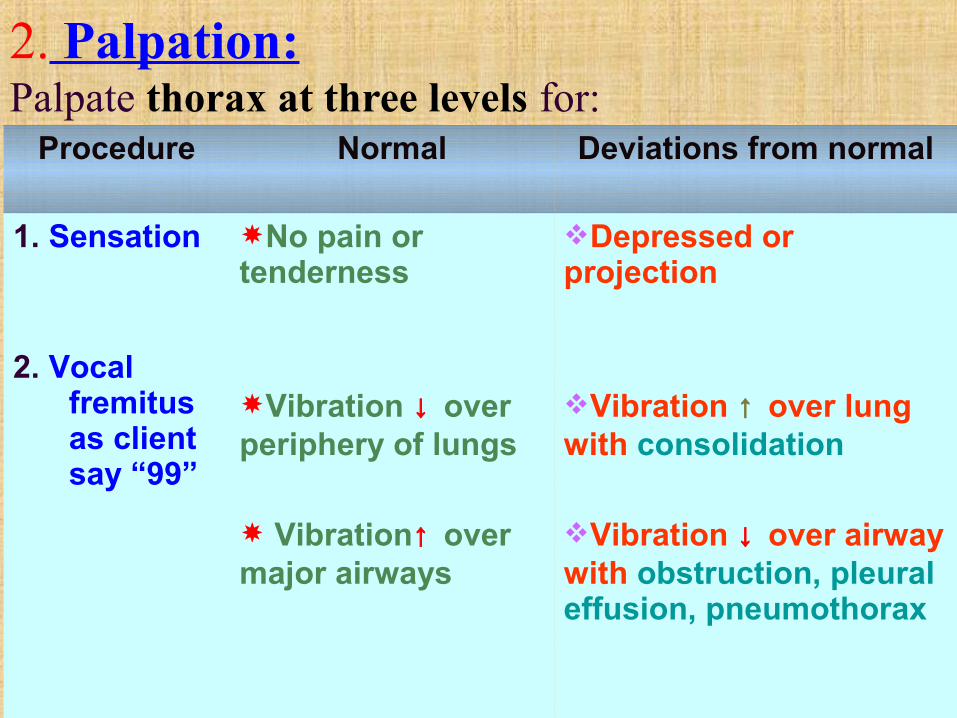
2. Palpation: Palpate thorax at three levels for:
Procedure Normal Deviations from normal
1. Sensation
2. Vocal fremitus as client say “99”
No pain or tenderness
Vibration ↓ over periphery of lungs
Vibration↑ over major airways
Depressed or projection
Vibration ↑ over lung with consolidation
Vibration ↓ over airway with obstruction, pleural effusion, pneumothorax

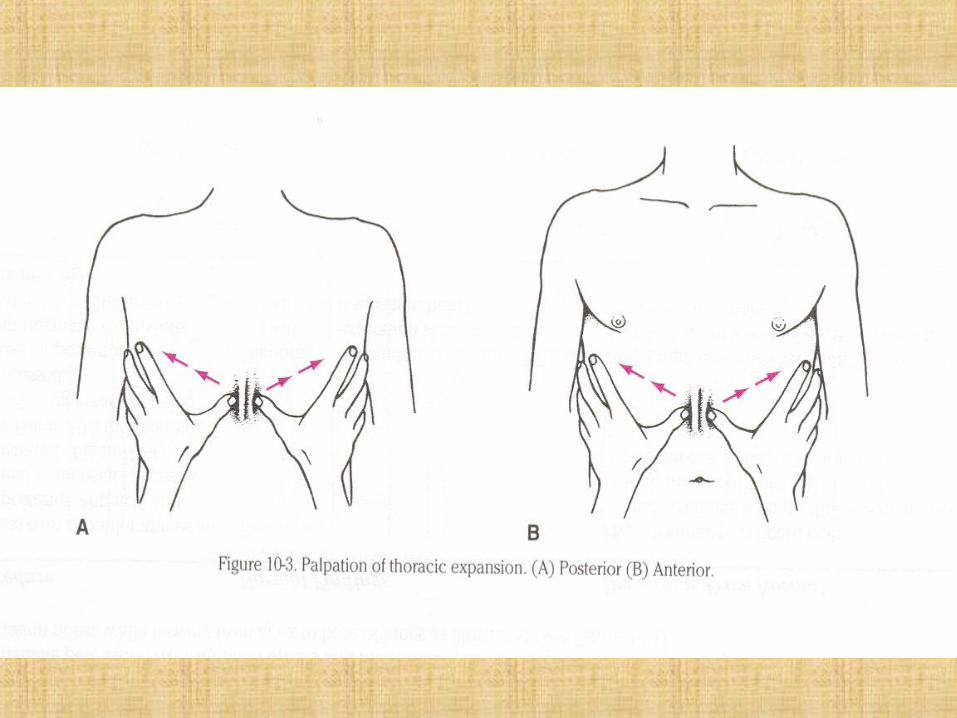
2. Palpation: (Continue) Palpate thorax for thoracic expansion by:
Procedure Normal Deviations from normal
1. Test respiratory expansion
Place hands on posterior thorax at level of 10th
Vertebra.*Gently press skinbetween thumbs &have client takedeep breath.*Observe thumbmovement
Symmetrical expansion
Thumbs move apart equal distance in both directions)
Asymmetrical expansion
Thumbs movement apart is unequal

Assess lung expansion
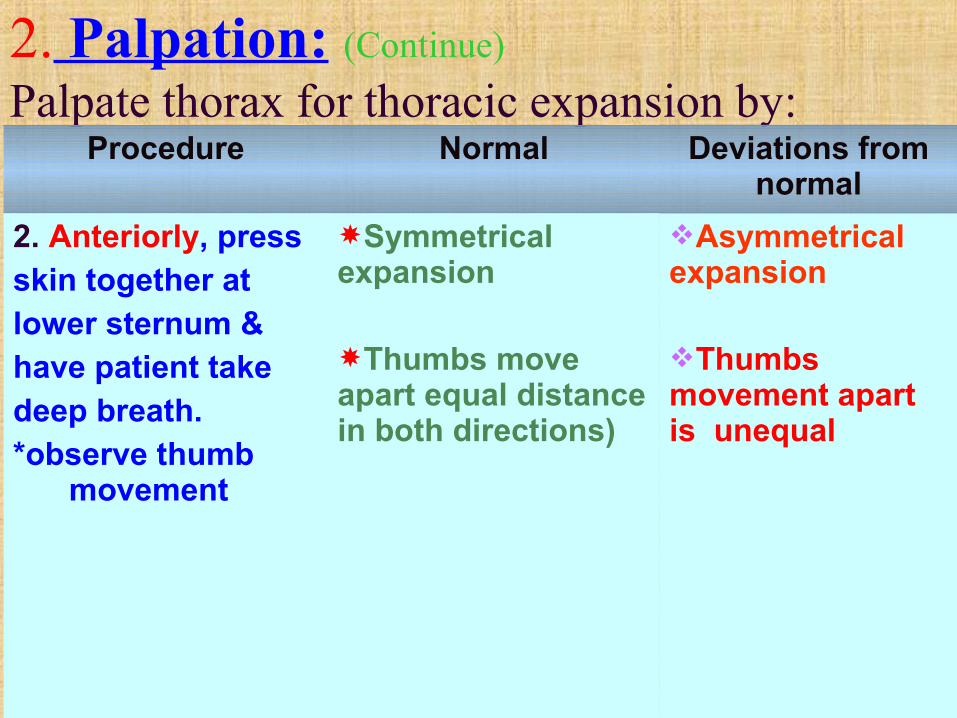
2. Palpation: (Continue) Palpate thorax for thoracic expansion by:
Procedure Normal Deviations from normal
2. Anteriorly, pressskin together atlower sternum &have patient takedeep breath. *observe thumb
movement
Symmetrical expansion
Thumbs move apart equal distance in both directions)
Asymmetrical expansion
Thumbs movement apart is unequal

3. Percussion:
Use mediate percussion over shoulder apices & intercostal spaces
Compare for symmetry of percussion notes, while moving from apex to base of lungs

3. Percussion:
Procedure Normal Deviations from normal
1. Percuss over shoulder apices & at posterior, anterior, & lateral intercostal spaces
Resonance Hyperresonance over -emphysematous lungs
Dullness heard over solid masses or fluid-pneumonia-Pleural effusion-tumor

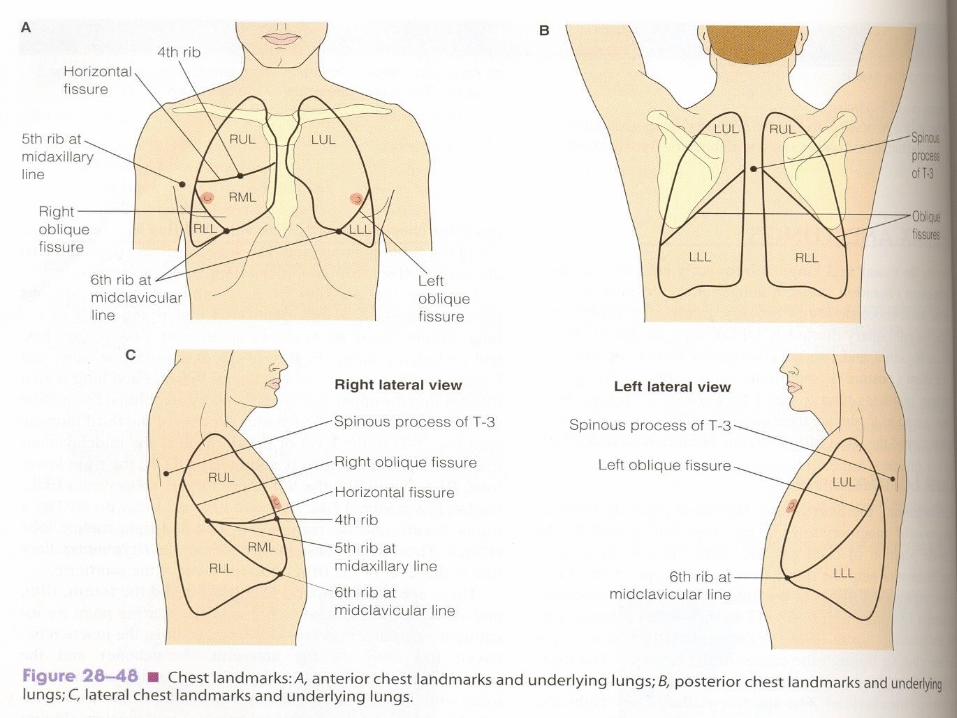
Intercostal Landmarks for percussion of thorax

Thoracic landmarks of underlying lungs

Technique of percussion

A lung affected by COPD displaces upper border of liver downward

3. Percussion: (Continue)
Procedure Normal Deviations from normal
2. Percuss over posterior, Diaphragmaticexcursions
bilaterally
Diaphragm descends 3-6 cm from T10 (with full expiration held)To T12 (with full expiration held)
Diaphragm descends less than 3 cm owing to atelectasis of lower lobes-emphysematous-ascites-tumor

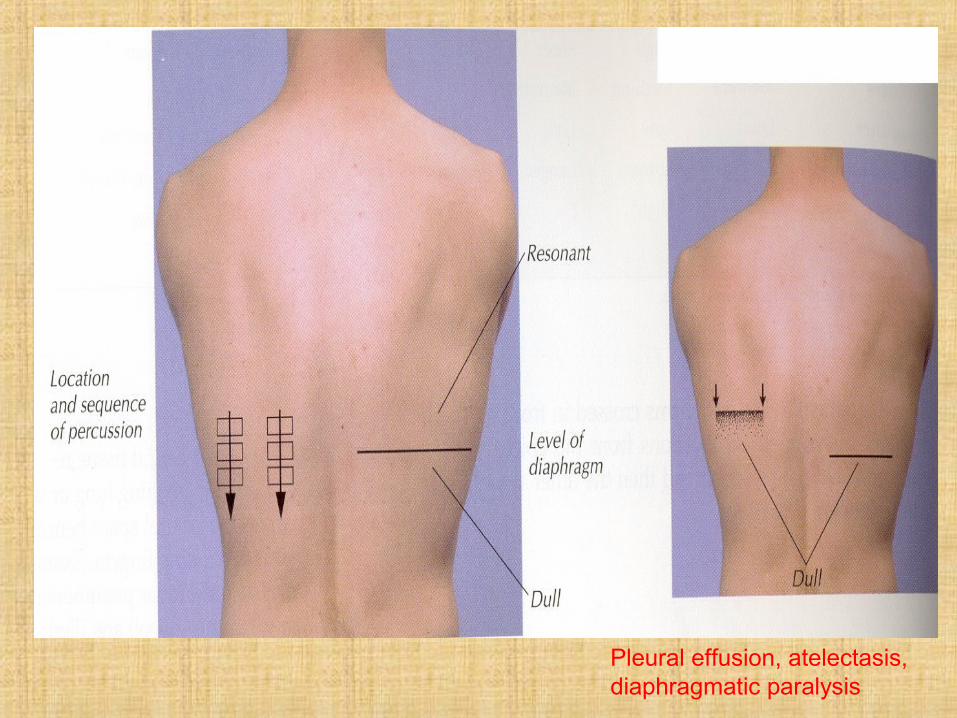
Pleural effusion, atelectasis, diaphragmatic paralysis

4. Auscultation: Use diaphragm of stethoscope, exert pressure
over intercostal space
Instruct client to take slow, deep breaths through the mouth.
Listen for two full breaths & compare symmetrical sides of thorax while moving stethoscope from apex to base of lungs
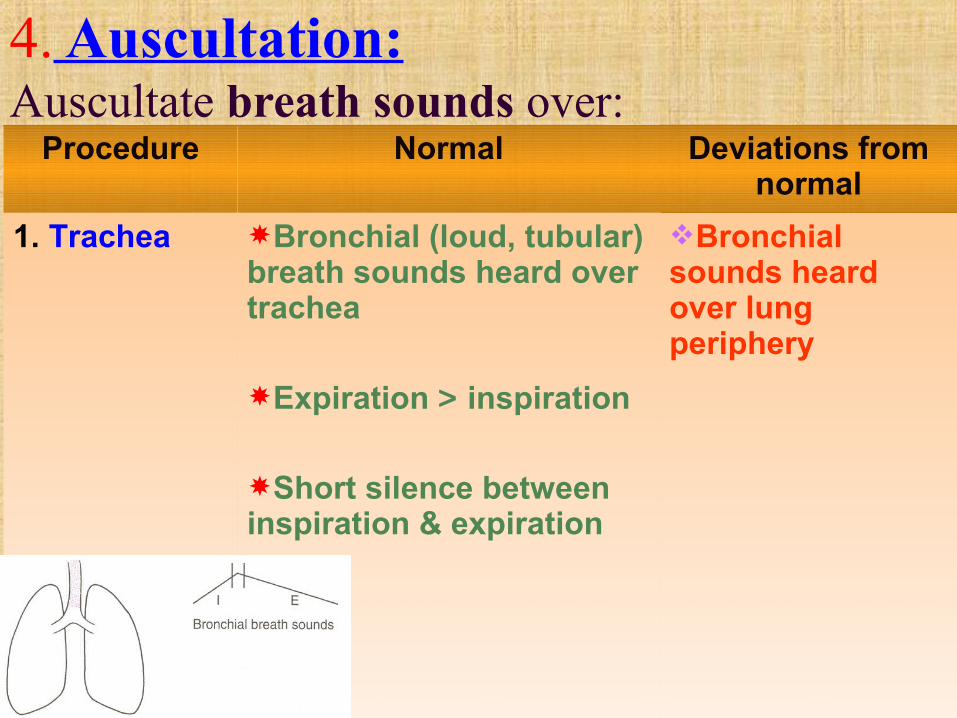
4. Auscultation: Auscultate breath sounds over:
Procedure Normal Deviations from normal
1. Trachea Bronchial (loud, tubular) breath sounds heard over trachea
Expiration > inspiration
Short silence between inspiration & expiration
Bronchial sounds heard over lung periphery
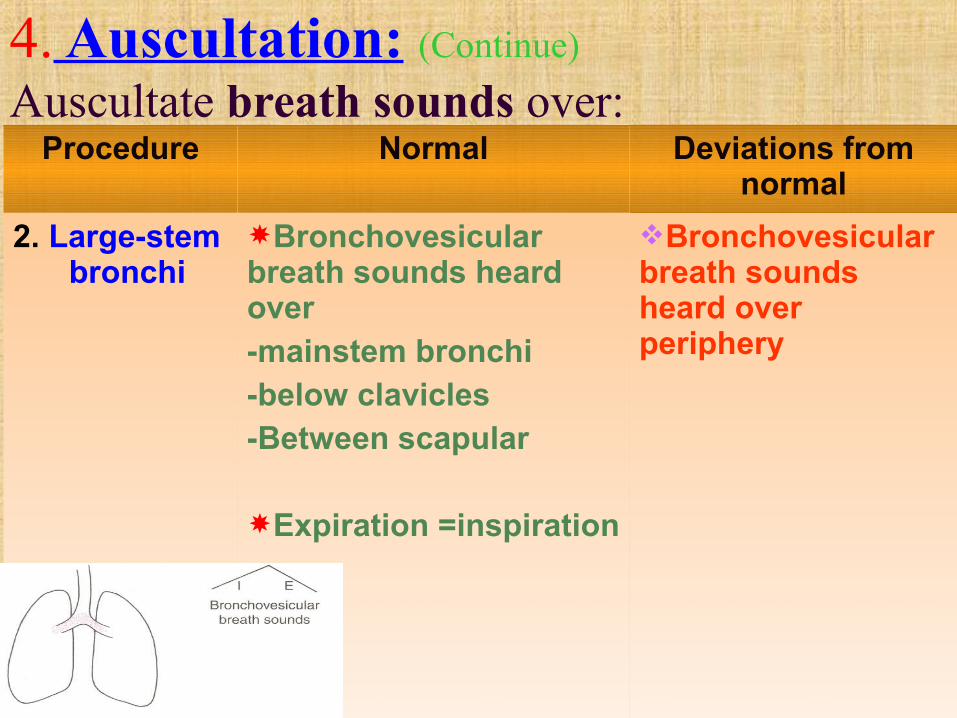
4. Auscultation: (Continue) Auscultate breath sounds over:
Procedure Normal Deviations from normal
2. Large-stem bronchi
Bronchovesicular breath sounds heard over -mainstem bronchi-below clavicles-Between scapular
Expiration =inspiration
Bronchovesicular breath sounds heard over periphery
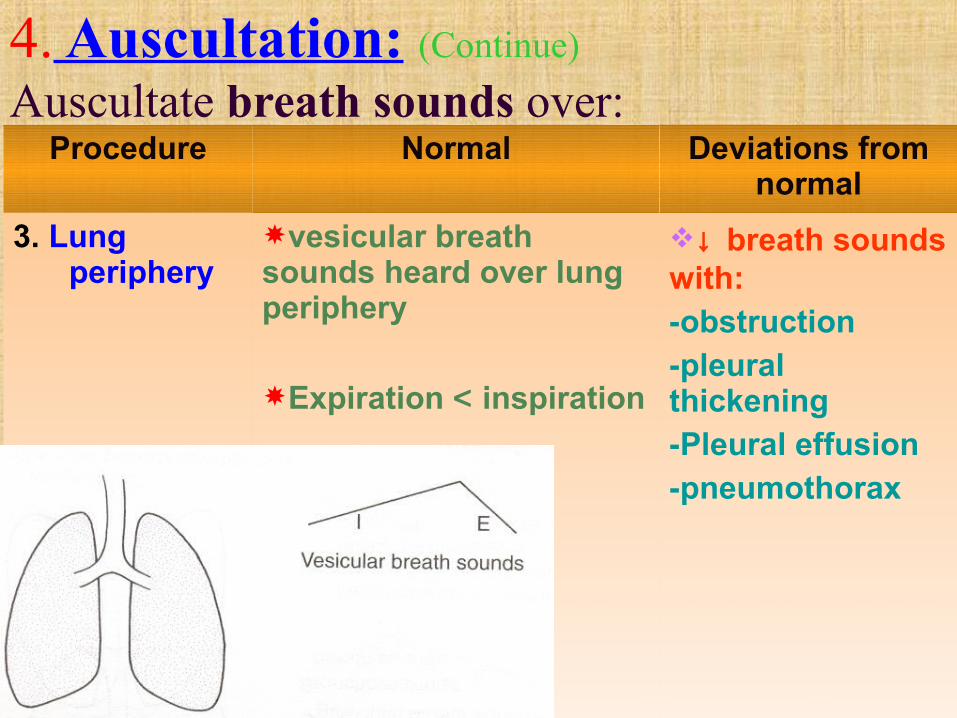
4. Auscultation: (Continue) Auscultate breath sounds over:
Procedure Normal Deviations from normal
3. Lung periphery
vesicular breath sounds heard over lung periphery
Expiration < inspiration
↓ breath sounds with:-obstruction-pleural thickening-Pleural effusion-pneumothorax


4. Auscultation: (Continue) Auscultate breath sounds over:
Procedure Normal Deviations from normal
4. Adventitious sounds
( crackles,rhonchi, wheezes)
If an abnormalsound is heard, askclient to cough.Note if adventitioussound is stillpresent or if itcleared with cough
Lungs clear to auscultation on inspiration & expiration
Crackles are auscultated during inspiration:in late inspiration-pneumonia-congestive heart failurein early inspiration-bronchitis-asthma-emphysema

4. Auscultation: (Continue) Auscultate breath sounds over:
Procedure Normal Deviations from normal
4. Adventitious sounds
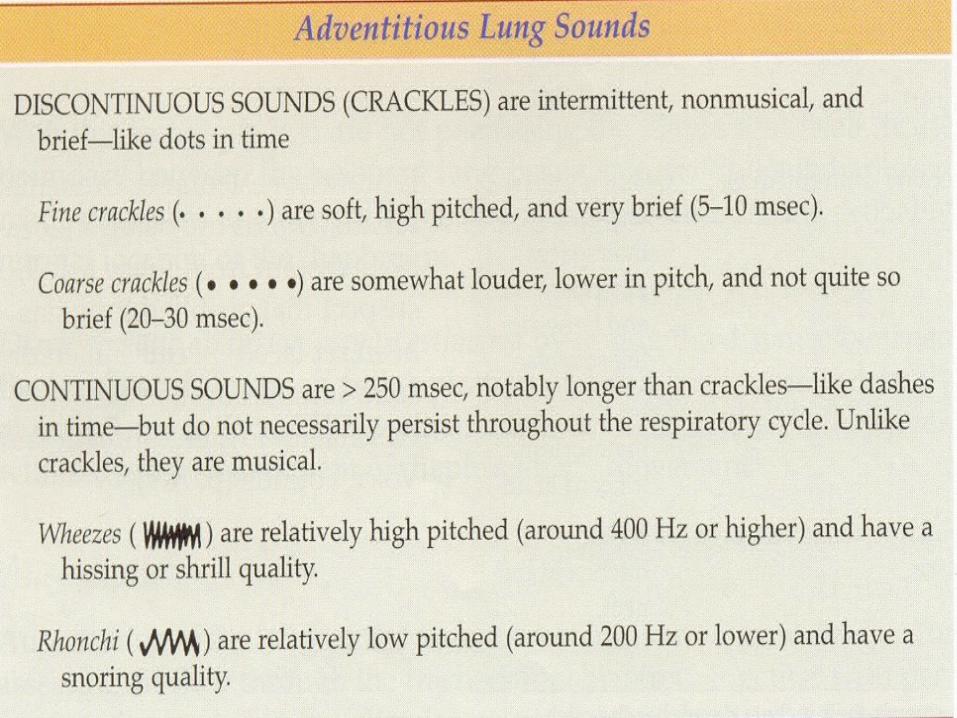
Abnormal sounds-crackles,-rhonchi, -wheezes
Lungs clear to auscultation on inspiration & expiration
Crackles are soft, high or lower pitchedRhonchi (snoring, low-pitched sounds) heard in inspiration & expirationWheezes (high-pitched musical sounds) heard on inspiration or expiration in acute asthma & chronic emphysema



4. Auscultation: Auscultate for altered voice sounds over lung periphery:
Procedure Normal Deviations from normal
1. Bronchophony Client says “99”while examinerauscultates
2. Whispered pectoriloquy
Client Whispers “one, two, three” whileExaminer auscultates
Sounds muffled
Sounds muffled
Sounds loud & clear over consolidation from -pneumonia-atelectasis-tumorSounds loud & clear over consolidation
4. Auscultation: (Continue) Auscultate for altered voice sounds over lung periphery:
Procedure Normal Deviations from normal
3. Egophony Client says “ee”while examinerauscultates
Sounds like muffled “ee”
Sounds like “ay” over areas consolidation or compression


Pediatric Variations
Subjective data: Focus questions History of wheezing , asthma, or other breathing
problems
Exposure to passive smoke
Frequent cold or congestions
Occurrence of sudden infant death syndrome (SIDS)
Pediatric Variations1. Inspection Infants: AP diameter = transverse (1:1) By age 5: AP diameter (1:2)similar to adult Thin chest wall with cartilaginous rib cage soft
& pliant Respiration rate varies according to age
2. Percussion: infant & young children: hyperresonant because of thinness of chest wall
3. Auscultation Breath sounds will be louder & harsher due to
proximity to origin of sounds from thin chest wall

Geriatric variations
Loss of elasticity , fewer functional capillaries & loss of lung resiliency
↓ ability to cough effectively due to weaker muscles and rigid thoracic wall
Kyphosis ( accentuated dorsal curve) ↓ thoracic expansion due to calcification of costal
cartilage Hyperresonance of thorax due to age related to
emphasymic changes ↓ breath sounds & ↑ retention of mucous due to ↓
pulmonary function ↑ AP diameter due to loss of resiliency & loss of
skeletal muscle strength
Possible Collaborative Problems
Examples:
Respiratory insufficiency or failure Pneumonia Pulmonary edema Airway obstruction/ atelectasis Laryngeal edema
Pleural effusion Respiratory acidosis Respiratory alkalosis
Teaching Tips for Selected Nursing Diagnoses
Example: Opportunity to enhance respiratory function Ineffective airway clearances related to shallow
coughing & thickened mucus Impaired gas exchange related to chronic lung
tissue damage Ineffective airway clearance related to chronic
allergyPediatric: Ineffective airway clearance related to bronchospasm and increased pulmonary
secretions






























