Embed Size (px)
Citation preview

Racial Differences in CKD
See Kovesdy et al,pages 228-235;Derose et al, pages236-244; Peralta etal, pages 261-266;and Arce et al,pages 312-321.
Thismonth’sAJKD features4stud-ies that explore different aspects ofthe strong racial disparities inESRD rates in the US. Kovesdy andcolleagues report that the survivaladvantage seen in black dialysispatients is accentuated in thosewithmoreadvancedstagesofCKD,presentingdatasuggestingthatbet-ter survival may reflect changes incase-mixand laboratorycharacter-istics occurring during the courseof kidney disease. Derose et al used observed eGFR to predict the time of kidneyfailure, finding that there were more extreme rates of eGFR decline in blackparticipants and that differences in eGFR decline and mortality contributed toracial disparities in ESRD incidence. Peralta and coworkers show that after age 35,eGFR decline was significantly steeper and started at earlier ages in blackscompared with whites. Finally, Arce et al demonstrated that, while Hispanicsexperienced lower mortality overall, differential access to kidney transplantationexplains much of the apparent survival benefit in younger Hispanics.
Aging in CKD
See Grams et al,pages 253-260;Grams et al, pages245-252; Hsu & Hsu,pages 214-216;Vassalotti &Piraino, pages217-219; Kiberd,pages 220-222.
In this issue of AJKD, 2 studiesinvestigate the rates of CKD inthe US population. In the first,Grams and colleagues evaluatethe prevalence of CKD using cys-tatin-based rather than creati-nine-based GFR estimates andnote that, based on NHANES, theprevalence of CKD increased be-tween 1988-1994 and 1999-2002. Editorialists Hsu and Hsuargue that other evidence showsthat efforts at preventing andtreating CKD have achieved somelowering of the burden of diseaseat a societal level. In the secondstudy, Grams et al report that therisk of developing CKD stage3a� over one’s lifetime is high,with eGFR below 60 mL/min/1.73 m2 the rule rather than the
B
B
B
BBB
W
W
W
WWW
H
H
H
HHH
A
A
A
AAA
*A,B,W>H
*W>B,H
*W>B
*H,B>W
0
.1
.2
.3
.4
.5
Pro
babi
lity
29 to 1544 to 3059 to 4574 to 6089 to 7590 pluseGFR Strata (mL/min/1.73m2)
THIS
MO
NTH
INA
JKD
THIS MONTH IN AJKD
Am J Kidney Dis. 2013;62(2):xviii-xxxviii
exception among the elderly, with lifetime risks of ESRD ranging from 2% to8% depending on race and sex. In one accompanying editorial, Kiberdillustrates more subtle findings in this study, including the small but substan-tial risk of kidney failure among younger African Americans, and reviews theutility of being able to quantify risk. In another accompanying editorial fromthe NKF, Vassolotti and Piraino discuss the ramifications of this study forpatient care and public health policy.
Obesity in CKD
See Chang et al,pages 267-275; andSilverwood, pages276-284.
Two of this month’s AJKD ar-ticles focus on the relationshipbetween obesity and kidney out-comes. Chang and colleagues in-vestigated the link between life-style-related factors and CKD riskand found that unhealthy dietand obesity are associated withincident microalbuminuria. Inanother article, Silverwood et aluse repeated BMI measurementsin children between the ages of 2and 20 years old to model early life overweight trajectories, and demonstratethat these early life patterns are associated with of the presence of CKD at age60-64 years, emphasizing that childhood habits can have a critical impact onlater life health.
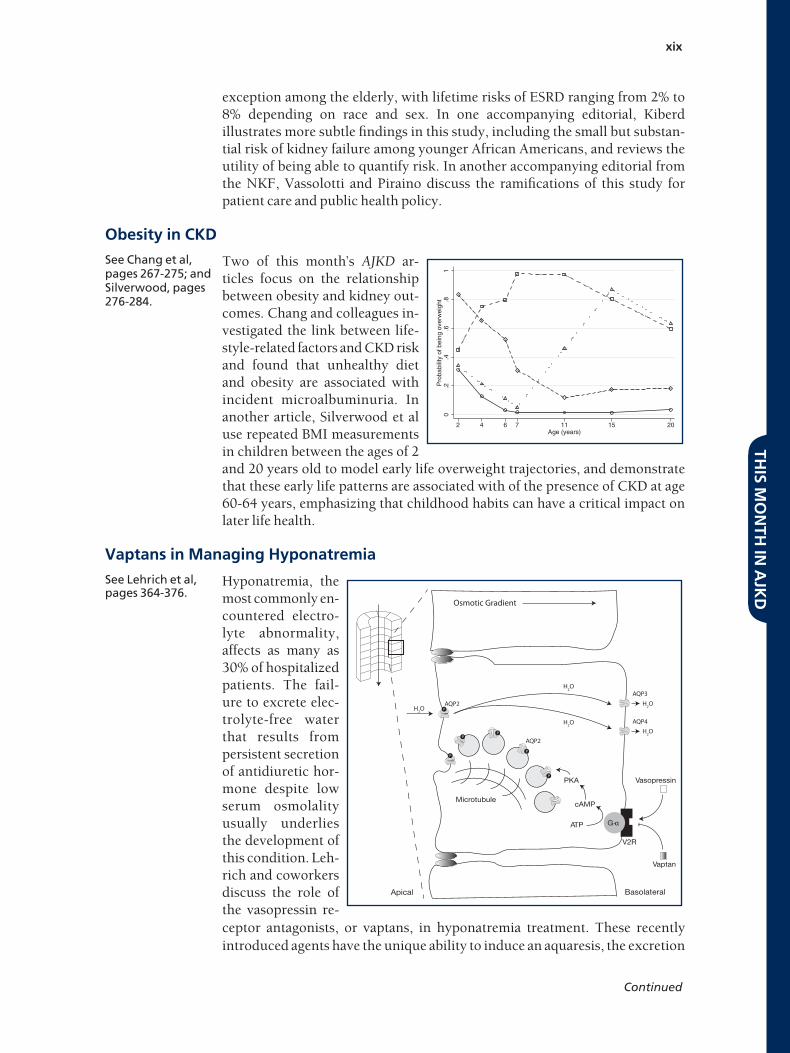
Vaptans in Managing Hyponatremia
See Lehrich et al,pages 364-376.
Hyponatremia, themost commonly en-countered electro-lyte abnormality,affects as many as30% of hospitalizedpatients. The fail-ure to excrete elec-trolyte-free waterthat results frompersistent secretionof antidiuretic hor-mone despite lowserum osmolalityusually underliesthe development ofthis condition. Leh-rich and coworkersdiscuss the role ofthe vasopressin re-ceptor antagonists, or vaptans, in hyponatremia treatment. These recentlyintroduced agents have the unique ability to induce an aquaresis, the excretion
0.2
.4.6
.81
Pro
babi
lity
of b
eing
ove
rwei
ght
2 4 6 7 11 15 20Age (years)
Vasopressin
Vaptan
V2R
cAMP
PKA
Osmotic Gradient
AQP3
AQP2
AQP2
AQP4
ATP G-α
Microtubule
P
P
P
PP
P
H2O
H2OH2O
H2OH2O
Apical Basolateral
THIS
MO
NTH
INA
JKD
xix
Continued

of electrolyte-free water without accompanying solutes. Vaptans have beenshown to increase serum sodium concentrations in patients with euvolemic orhypervolemic hyponatremia in a reproducible manner, but the authors cau-tion that their safe use requires full understanding of their indications andcontraindications.
THIS
MO
NTH
INA
JKD
This Month in AJKD, Continued xx





























