Embed Size (px)
Citation preview

Journal of Neurology, Neurosurgery, and Psychiatry, 1973, 36, 194-198
Thenar motor unit count estimates in thecarpel tunnel syndrome
W. F. BROWN
From St. Joseph's Hospital, London, Ontario, Canada
SUMMARY Thenar motor unit counts were done in 19 subjects with symptoms characteristic of thecarpal tunnel syndrome. Three-quarters of the patients had motor unit count estimates less than2 SD lower limit of controls. Despite this, most did not have thenar wasting or weakness. Functionalcompensation by motor unit remodelling probably kept pace with motor axon loss and masked thetrue extent of axonal degeneration.
The carpal tunnel syndrome is common. In mostcases the clinical features are sufficiently charac-teristic to allow a confident diagnosis to bemade. Electrophysiological studies are of themost value when they provide clear evidence fora local injury to the median nerve in the carpaltunnel region, especially in patients whosesymptoms and signs are unusual or indefinite.Among present methods for studying the carpaltunnel disorder, demonstration of prolongedmotor terminal delays (Simpson, 1956; Thomas,Lambert, and Cseuz, 1967) and abnormalmedian digital sensory nerve potentials (Thomaset al., 1967) are the most useful. Electromyo-graphy may provide evidence of denervation ofthe thenar muscles. In one study, however,fibrillation potentials were found in only 410% ofcases (Thomas et al., 1967) and even less fre-quently in another report (Buchthal and Rosen-falck, 1971). A recent report clearly demon-strated abnormal sensory fibres conductionacross the carpal tunnel despite, in many sub-jects, normal conventional sensory potentialsand distal motor latencies (Buchthal andRosenfalck, 1971). Measurement of the trans-tunnel sensory conduction velocity required,however, special precautions and recordingtechniques.
These methods, unfortunately, do not providemore than a rough estimate of the extent ofmedian nerve fibre degeneration. The presentstudy was undertaken to see if an estimate of thethenar motor unit count was helpful in demon-
strating denervation by excessive motor unitloss, especially in those subjects with mild carpaltunnel syndromes, without weakness or thenarwasting.
METHODS
SUBJECTS The study was limited to a group of 19subjects, 10 of whom were female, with symptomscharacteristic of the carpal tunnel syndrome. Allsubjects were troubled, many times, during the nightand on getting up in the morning, with numbnessand prickliness in the thumb and next three fingers.The symptoms were often most severe on wakeningin the morning and, in some, were aggravated by useof the hands during the day. None had other limbsymptoms or signs to suggest a cervical root or otherperipheral nerve injury.
In five there was mild weakness of thumb abduc-tion but no wasting and, in two others, obviouswasting and severe weakness. In the rest, the thenarstrength and mass were normal. In all subjects theassessment of strength and the presence or absence ofwasting were based on the statement of at least twoneurological consultants who reached their opinionsindependently. If their reports differed, as they did intwo subjects, the more abnormal estimate wasaccepted.
194
ELECTROPHYSIOLOGICAL STUDIES A method forestimating the number of motor units in thenarmuscles has been described (Brown, 1972). For thepresent study, the Devices Model 3072 high voltagestimulator was modified by replacing the standardsingle turn 5kQ wirewound output potentiometer
Protected by copyright.
on February 25, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.36.2.194 on 1 April 1973. D
ownloaded from

Thenar motor unit counit estimates in the carpal tunnel syndrome
muleAAA
'O---
A0
A8 I
fema le0* asymptomatic
hand'V weakness
A
A0
30 40AGE YEARS
50 70 80
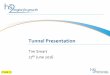
FIG. 1. Plot of the motor unit count of all 19 subjects with a clinical diagnosis of the carpal tunnel syndronme.Also shown are the mean and 2 SD lower limit of all controls under 60 years of age. The vertical bar connectsvahies in both hands of the same subject.
with a 10 turn potentiometer. This modification didnot alter the motor unit estimates but did make iteasier to separate individual motor unit thresholds.
Measurements were made of the terminal delaysto the first several motor unit potential steps, as wellas to the maximum compound action potential. Inall subjects, a careful search for spontaneous fibrilla-tion potentials in the thenar muscles was made.
Sensory nerve action potential studies were done in15 of the subjects by using needle electrodes as
described by Buchthal and Rosenfalck (1966).
RESULTS
In Fig. 1 the motor unit counts in all 19 carpaltunnel subjects are plotted against age. For com-
parison, the mean and 2 SD lower limit of allcontrols under 60 years of age reported previouslyare shown (Brown, 1972). There were five sub-jects with motor unit counts within the 2 SDlimits of the control mean. Under 60 years of
age, 11 subjects had motor unit counts less thanthe 2 SD below the lower limit and eight ofthese were judged to have no thenar wasting or
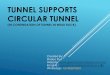
weakness. For example, a 30 year old femaleshown in Fig. 2 had typical sensory symptoms inthe right hand for two years and in the left fornine months, but no weakness or wasting ineither hand. In both hands the motor unit countwas reduced.
In another subject, the asymptomatic handshown in Fig. 3 also had a prolonged terminalmotor delay and clearly reduced motor unitcount, but normal power. However, in thesymptomatic hand, abduction was very weak,the thenar muscles obviously wasted and only 3motor units could be evoked with supramaximalmedian nerve stimulus. Fibrillation potentialswere not present in either hand.Only two subjects had severe wasting and
weakness and both had fewer than 5 motor units
MU C
0
195
Protected by copyright.
on February 25, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.36.2.194 on 1 April 1973. D
ownloaded from

W. F. Brown
FIG. 2. A 30 year oldfemale with bilateral sensory symptoms but no wasting or weakness of the thenar muscles.Right hand, A: thumb median nerve sensory potential; B: 4th and 5th finger ulnar nerve sensorYv potential.Motor unit estimate-99. Left hand, Ci-ii: motor unit estimate-46.
estimated in thenar muscles. The lowest motorunit count, in both control and carpal tunnelgroups, without wasting or weakness, was 40. Inone subject, reported to have mild weakness ofthumb abduction but without wasting, the motorunit count was in the normal range. Unfortuna-tely, a motor unit count was not done in theopposite hand for comparison.Motor unit counts were done of both hands in
six subjects. In two of these the symptoms werein one hand only and in both the motor unitcount was lower in the hand with symptoms.The motor unit count in both hands was withinthe normal range in one individual but thevalue was 20% lower in the hand with symptoms.Only two patients of the carpal tunnel group
were found to have fibrillation potentials. In
both, there was mild weakness and the motorunit count in thenar muscles was reduced.
In the control group there were only threecases with motor terminal delays over 4-7 msecand two of these were in subjects over 80 yearsof age (mean 3-8 + 0-6 msec). In the carpaltunnel group, half of the subjects had terminalmotor delays greater than 4-7 msec (mean4-8 + 1 0 msec). The longest terminal motor delayin the carpal tunnel group was 7-3 msec. Themean maximum motor conduction velocity inthe forearm in carpal tunnel subjects was 55 +1-2m/sec compared with the control group valuesof 56 + 4 9.The median digital sensory nerve action
potentials recorded just above the wrist wereabnormal in nine of the 15 subjects studied.
196
Protected by copyright.
on February 25, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.36.2.194 on 1 April 1973. D
ownloaded from

Thenar motor unit count estimates in the carpal tunnel syndrome
FIG. 3. A fifty year old male with unilateral sensorysymptoms, severe wasting and weakness. A: motorunit count in symptomatic hand shows only 3 motorunit steps with a supramaximal stimulus. B i-ii: motorunit counlt in asymptomatic hand without wasting or
weakness. Motor unit count-40.
DISCUSSION
Clinical estimates of strength and muscle mass aredifficult to quantitate. Their accuracy dependson the training and experience of the clinician.Whatever criticisms can be made of the esti-mates of muscle strength and mass, theirvalue is to provide a standard against whichthe neurophysiological estimates of the motorunit counts can be made. Judged in this light,the motor unit count was found to be of valuebecause in several subjects judged normal onclinical examination and in whom no fibrillationpotentials could be detected, the estimatedmotor unit count was clearly lower than in thecontrol values of comparable ages.The motor unit count assumes that all motor
axons are activated by the supramaximal nervestimulus. Further, the motor axon actionpotentials are assumed to propagate withoutdistal failure or block. Failure to activate all ofthe motor axons by the stimulus or axonal blockbeyond the stimulus point could result in falselylow motor unit counts.A single necropsy study of one patient with
signs and symptoms typical of the carpal tunnelsyndrome was reported by Thomas and Fullerton(1963). These authors showed that the nervefibre size was sharply reduced under the flexorretinaculum and that the nerve fibres distal tothe carpal tunnel were consistently larger. In onehand there was gross weakness and wasting ofthe abductor pollicis brevis muscle and a veryprolonged terminal motor delay. The nerve fibrecount in the carpal tunnel region was one-thirdfewer than the number at the mid forearm levelcounted in a standard strip across the widestdiameter of the nerve section.
Fullerton and Gilliatt (1967) described a localinjury to the median and ulnar nerves under acartilaginous bar in the guinea-pig. The patho-logical features included not only Wallerian de-generation but many fibres, in addition, showedthinly myelinated internodes and others com-plete myelin loss. Intermittent conduction blockwas clearly shown in demyelinated single fibresof the rat, especially in those fibres with greatlyprolonged internode conduction times (Ras-minsky and Sears, 1971).
There was no suggestion in this study ofintermittent block of single motor unit poten-
197P
rotected by copyright. on F
ebruary 25, 2021 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.36.2.194 on 1 A
pril 1973. Dow
nloaded from

W. F. Brown
tials, even when the terminal motor delay wasprolonged. The absence of intermittent singleunit block and the very prolonged terminalmotor delays reported in other series (Simpson,1956; Thomas, 1960; and Thomas et al., 1967)made it unlikely that a functional axonal blockaccounted for the lower motor unit counts.Axonal degeneration, therefore, probably ac-counted fully for the lower motor unit count,especially in those subjects with normal or nearnormal motor terminal delays.The motor unit count record showed little
evidence of abnormal dispersion of motor unitterminal delays, even in those subjects withabnormally prolonged terminal delays. Theseobservations were, however, based on the firstseveral motor unit steps and may not haverepresented possible wider dispersions ofterminaldelays in units with higher thresholds.
Unlike the present study, previous reportshave shown a significant, although mild, slowingof forearm median nerve maximum motor con-duction velocity in the carpal tunnel syndrome(Thomas, 1960; Thomas et al., 1967). It isdifficult to compare independent studies but inboth previously reported series, one-quarter toone-third of the subjects had terminal motordelays greater than the highest value reportedhere. Thomas (1960) showed that the magnitudeof slowing of forearm conduction was related tothe degree of distal slowing. The absence of sucha large proportion of patients with very longterminal motor delays may therefore have ac-counted for the failure to show any slowing ofthe forearm motor conduction velocities in thisstudy. In fact, based on the absence of very pro-longed terminal motor delays, normal medianforearm motor conduction velocities and therelative infrequency of fibrillation potentials, itis possible that the present study included ahigher proportion of mildly affected subjectsthan previous reports.
It was surprising from the motor unit studiesof ageing and the carpal tunnel syndrome, howfew motor units were required to maintainmuscle size and strength. McComas has pre-viously reported that there was no significant fallin the maximum twitch potential of the extensor
digitorum brevis muscle unless the motor unitcount was less than 10% of the normal value(McComas, Sica, Campbell, and Upton, 1971).
In the present study, weakness and wasting,unless severe, was not a useful guide to theextent of motor unit loss except when the nervefibre loss had been severe. Functional compensa-tion by constant remodelling of motor unitsprobably masked the true extent of motor fibreaxonal degeneration. Weakness and wasting, ifpresent, may suggest that the major proportionof the axonal injury took place over a shortperiod of time and not scattered over manymonths or years, where remodelling is morelikely to mask the motor axon loss.
The author would like to thank Dr. H. Bamett, Dr.H. Barr, Dr. J. Girvin, and Dr. N. Jaatoul for pro-viding me with their clinical notes and patients forthe study. I am most grateful for the able and patientassistance of Mrs. M. Webster in the preparation ofthis manuscript.
REFERENCES
Brown, W. F. (1972). A method for estimating the number ofmotor units in the thenar muscles and the changes in motorunit count with ageing. Journal of Neurology, Neuro-surgery, and Psychiatry, 35, 845-852.
Buchthal, F., and Rosenfaick, A. (1966). Evoked actionpotentials and conduction velocity in human sensorynerves. Brain Research, 3, 1-122.
Buchthal, F., and Rosenfalck, A. (1971). Sensory conductionfrom digit to palm and from palm to wrist in the carpaltunnel syndrome. Journal of Neurology, Neurosurgery, andPsychiatry, 34, 243-252.
Fullerton, P. M., and Gilliatt, R. W. (1967). Median andulnar neuropathy in the guinea-pig. Journal of Neurology,Neurosurgery, and Psychiatry, 30, 393-402.
McComas, A. J., Sica, R. E. P., Campbell, M. J., andUpton, A. R. M. (1971). Functional compensation in par-tially denervated muscles. Journal of Neurology, Neuro-surgery, and Psychiatry, 34, 453-460.
Rasminsky, M., and Sears, T. A. (1971). Conduction timebetween nodes of Ranvier in normal and demyelinatedsingle fibres. Abstract, Fourth International Congress ofElectromyography, Brussels.
Simpson, J. A. (1956). Electrical signs in the diagnosis ofcarpal tunnel and related syndromes. Journal ofNeurology,Neurosurgery, and Psychiatry, 19, 275-280.
Thomas, P. K. (1960). Motor nerve conduction in the carpaltunnel syndrome. Neurology (Minneapolis), 10, 1045-1050.
Thomas, P. K., and Fullerton, P. M. (1963). Nerve fibre sizein the carpal tunnel syndrome. Journal of Neurology,Neurosurgery, and Psychiatry, 26, 520-527.
Thomas, J. E., Lambert, E. H., and Cseuz, K. A. (1967).Electrodiagnostic aspects of the carpal tunnel syndrome.Archives of Neurology, 16, 635-641.
198
Protected by copyright.
on February 25, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.36.2.194 on 1 April 1973. D
ownloaded from