Embed Size (px)
Citation preview

I?etection of magnetically marked capsules (MMC) via SQUID allows to monitor esophageal rsusport of solid drug forms with high temporal and spatial resolution. Thus, the aim of the study ~ns to examine et&cts of dittierent body positions and liquid volumes at swallowing on esophageal transit of sdid drug fomns by MMM Methods: Six volunteers swallowed MMCs with 5, 25, or 50 ml of water (16.1mm x 5,5ram; 5 MMCs at each volume) in upright (60 degree) and supine position, respectively Measurements were done with a 63 channel flat SQUID device, Results: (Table; Kruskal-Wallis H) Discussion: The msuhs prove that in supine and upright positkm esophageal transit time of solid drug torms is aflected by the swallowing volume Also, the rate of entrapment of capsules depends on swallowing volume. Furthermore these data show for the first time that in upright position the retention rate, corrected for the influcence of swallmving volume, is highly dependent on pharyngeal propulsion velocity This observation and the fact that it took only 1,2 s to transport the tabkt into the stomach in upright body position at 50 ml of water suggest that the transport velocity of the capsules in upright positinn was independent from the propulsive motor function of the esophagus
effe~ of volume supine I upright 5rot 25ml 50ml H) transR Ume (sue) 7,615,3 5,4/4.8 4,6/1.2 ~ n rate (%) 52145 28/7 0/0 pharyngeal propulsion velocity - 7,2/10 10,6/15 14.21 overall (cm/suc) 292 p h ~ proptd'don velocity 11,2 / 14,21 of the non-retained capsules 8,0 t 10,9 19,7 29.2 (r p~aryngeal I~pulsion velocity of I~e retained capsules 6,6 / 67 10 / 3,4 - t 4,4 (cmJ~c) eflsct of pharyngeal propulsion; n,S, / n,S, / n,S. / (K~skal-wams H) ~.05 ~,05 ~,05
p<.001 / p<.001 p<.001 I p<,001
p<.001 / p<.001
M2158
The Vide~esophagogram: Defining Normality to Evaluate Patients with Esophageal Disease Anand P, Tamhankar, James M. Halls, Ginseppe Portale, Emmanouel M. Chonstoulakis, Gidon Ahnogy, Mustala A Arain, Peter F, Crookes, Jeffrey A. Hagen, Cedric G. Bmmner, Steven R. Demeester, Jeffrey H Peters, Tom R, Deamester
Background and Aim: Barium examination of the esophagus was introduced into clinical pracuce 100 years ago. For most of tbese yem's the locus has been on the identification of anatomic abnorn~alines Surprisingly, bolus transit has never been quantified in normal popuhmon causing variation in interpretation. Utilizing a standardized barium video-esopha- gogram, this study aims to define the pattern of bolus transit m normal subjects. Methods: Fify seven healthy asymptomatic volunteers were studied prospectwely v, ath barium video- esophagugram. Esophageal motility was done m all subjects to exclude motility disorders. A tull column standardized barium video-esophagogram consisting of five 10 ml liquid barium swallows (60 % barium at morn temperature) was done in the prone position with a right anterior oblique view. Solid bolus transit was evaluated using barium coated ham- burger m the upright position. Each liquid swallow was evaluated for proximal escape and d~stal retention. Solid bolus transit was evaluated as the number of swallows required tbr complete clearanve, Resuhs: Six subjects were excluded because of ineffective esophageal motility on manometry and one because of a mucosal ring. Fifty volunteers (35 males: 15 temales) were analyzed. Median age was 33 years (range 19-47). Liquid bolus completely cleared in 5/5 swallows in 72% of subjects, 4/5 in 92%, and 3/5 in 98% (95 ~h percentile = 3/5) Proximal escape occurred in 0/5 swallows in 84% of subjects, 1/5 in 14% (95 't' percentile = 1/5). Distal retention occurred in 0/5 swallows in 84% of subjects, I/5 in 14% (95 ~h percentile = 1/5) A solid bolus was cleared by one swallow in 56 % of subjects, by 2 swallows in 84 %, by 3 swallows in 92 %, and by 4 swallows in 98 % (95 '~ percentile = 4 swallows) Conclusion: Utilizing a standardized protocol, normal subjects clear at least 3 out of 5 liquid banum boluses in one swallow in the prone posuion, and can have proximal escape and distal retention in 1 out of 5 swanows, Solid boluses clear within 4 swallows in the upright position Quality" assm'ance requires appreciation of these normal patterns. Physicians should insist on a standardized perfom~ance of the video-esophagogram for proper evaluation of patients with esophageal dlsea~.
M2159
Esophageal Muscle Shortening During Swallow4ng Qing Dai, James Brasseur, Vinod K Thangada, Anapurna Korimiili, Chan Y. Chung, ttenry Parkman, Larry S. Miller
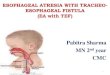
Background: Local muscle shortening can be analyzed using concurrent high-resolution ultrasound (US) and manometry dunng esophageal peristalsis applying basic principles of mechanics. Purpose 1) To determine if there are regional differences in shortening of the esuphageal muscle during dry and wet swallow induced peristaltic contraction. 2) To study the difference in the amount of shortening between the circular smooth muscle (CSM) and kmgitudinal smooth muscle (LSM) 3) To evaluate the correlation between the peak muscle thickness and the peak pressures dunng the pe~taltic contraction. Methods: Eight normal control sul!iects underwent simuhaneous high-resolution (20MHz) US/Manometry at four levels in the esophagus (5, 10, 15, 20cm above the LES) with dry swallows and wet swallows (5cc) Endoluminal US images were digitized and the cross sectional surface areas(CSA) and thickness o[ CSM, LSM and total muscle (CSM + LSM) were measured at baseline (esophagus at rest) and at peak contraction (peak plvssure) during swallowing. [CSA,.JCS& ............ = Length,,,,,,,~.,,eq~ength,, j describes muscle sbortenmg by the law" of mass conservation. Result: The percent shortening at 5cm (PS5cm) was signifcantly greater than the percent shortening at 20cm (PS20cm). For wet swallows (5cc) the difference [(PS5cm)-(PS20cm)l was, CSM: 1033% (~e Fignre), p<O001, LSM: 398%, p<O.05, Total: 66.2%, p<0.O1. For dry swallows the difterence was, CSM: 586%, p<O.001, LSM: 207%, P=0.07, Total muscle:
42,4%, p<O,01. The percent shortening due to Wet swallows was siguificantly greater than the percent shortening due to dry swallows at all levels except at 20cm, the mean difference was CSM: 47%, p<0.05; LSM: 23%, p<0.05; Total: 32%, p<0.05. The CSM shortened signifcantly more than the LSM at an levels except at 20cm, a mean difference of 31%, p<O,0001. Peak pressure correlated vdth the thickness of the total muscle (r = 0,81) and CSM (r = 0.78) but not with LSM (r = 0.55) at all levels. Conclusion: The distal esophagus shortens more than the proximal esophagus. Wet swallows induce more shortemng than dry swallows, CSM shortens more than LSM Peak intrahtminal pressure correlates with peak CSM and total muscle thickness during peristaltic contraction Funded if rough an NIH grant RO1 DK59500-01.
0.7 I I I I
Z Z LU
E O "1- O3
0.6
0.5
0.4
�9
O
0.3 i i i i 0 5 10 15 20 25
DISTANCE
M2160
Endoanal L~trasound Compared to Anorectal Manometry for the Evaluation of Fecal Incontinence: An Outcomes Study Keri L. Hill, M, Brian Fennerty, Shane Farming, Douglas O Faigel
Objective: Tests for evaluating incontinence include endoanal ultrasound (EUS) and anorectal manometq,'. The purpose of this study was to compare these techniques to determine which is more predictive of outcome for fecal incontineime. Hypothesis: EUS will be superior to anorectal manometry in identifying the subset of patients with surgically correctable sphincter defects leading to an improvement in outcome in these patients, Methods: 35 patients with incontinence were prospectively studied with EUS and anm-ectal manometry to evaluate the internal anal sphincter (1AS) and external anal sphincter (EAS). EUS was performed with Olympus GFUM20 ecboendoscope and a hy-poechoic defect in the EAS or IAS was considered a positive test. Patients with a positive EUS were recommended to have surgical repair. Anorectal manometry was performed with a standard waterrperfnsed catheter system to measure basal and squeeze pressures and sensation to an inflated balloon, All patients were administered the Cleveland Clinic Continence Grading Scale at baseline and at follow-up, Improvement in fecal control was defned as a 25% or greater decrease in continence score. EUS vs. manometry were compared with subsequent surgical treatment and outcome. P- values were calculated using Fishers exact test. Results: 32 patients (31 Females) were followed for a mean 25 months (range 13~46). 16 patients improved their symptoms (50%), There was no correlation between EUS or auorectal manometry sphincter findings and outcome(Table 1), Balloon sensation was also not predictive. 7/14 (50%) patients who subsequently underwent surgery vs. 8/17 (47%) without surgery improved (p=0,578). Conclusion: In long-term follow-up, approximately V2of patients will improve regardless of the results of EUS, anorectal manometry or whether surgery is performed. Supported by a Glaxo-Wellcome lnsitnte for Digestive Health Award
Table t, Predictive Value of EU$ and Anotectal Msuometry for Incontinence Imrpovemsut
PPV* NPV** EU$ EAS (n=32) 11/22 (50%) 5/10 (50%)
IAS (n=32) 9/17 (53%) 8/15 (53%) Manometry EAS (n=32) 12/22 (55%) 6/10 (60%)
, IA8 (n=32) 6/13 (46%) , 9/19 (47~ * positive test predicts impmven~nt ** negative test predicts no improvement
M2161
Assessment of activity of ulcerative colitis by power Doppler uhrasonography Yutaka Mitsuoka, Ken Hamma, Jiro Hata, Sbigeto Yoshida, Madoka Nakao, Mutsuhiro Hara, Hideharu Okanobu, Noriaki Manabe, Kayoko Kunihiro, Masaharu Sumii, Shin]i Tanaka, Kazuaki Chayama
(Background and aim) In ulcerative colitis (UC), assessment of disease acti~4ty is of major dimcal importance. Focal blood flow of the aftected bowel segment has been thought to be closely related to its disease activity. For this purpose, power Doppka" ukrasonography (US) is one of the non-invasive modalines. ~tle AIM of flus study was to confirm the utility
A-427 AGA Abstracts