Embed Size (px)
Citation preview

THE VERSATILITY OF VASCULARIZED ILIAC CRESTWITH INTERNAL OBLIQUE MUSCLE FLAP FORCOMPOSITE UPPER MAXILLARY RECONSTRUCTION
MASSIMO MARANZANO, MD1* and ANDREA ATZEI, MD2
The middle third defects of the face following total or partial oncologic maxillectomy include very important facial structures, both for esthet-ical and for functional reasons. Among the outcomes, large oronasal or oromaxillary fistulas due to destruction of big bone segments andsoft tissues have long been the consequences of such extensive surgical ablations. In the last few years, immediate reconstruction of max-illary bones and soft tissues has proved to be a reliable morphofunctional reconstruction technique following surgery for large oncologicaldefects or the late effects of radiation therapy. Among other free flaps such as composite fibula, composite scapula, or composite radial,the use of vascularized iliac crest with the internal oblique flap has become our flap choice for morphofunctional maxillary reconstructionfor bone segments within 6–15 cm of length, and when there is no need for overlying facial skin or oral sphincter reconstruction. Theadvantages of this composite bone flap are its available large and resizable bone stock; the quality of the bone for transfer (optimal height,depth, and contour to maintain a good facial profile); and the possibility to properly reconstruct the oral lining, orbital content; and maxillarysoft tissues with a portion of the internal oblique muscle flap raised with the same pedicle. In addition, this flap’s soft tissue will epithelializeduring the healing stages. VVC 2007 Wiley-Liss, Inc. Microsurgery 27:000–000, 2007.
Middle third defects of the face following total or par-
tial oncologic maxillectomy involve very important facial
structures, both for esthetic and for functional reasons.
Among the outcomes, large oronasal or oromaxillary fis-
tulas due to destruction of bone segments and soft tissues
have long been the consequences of such extensive surgi-
cal ablations. In the last few years, immediate reconstruc-
tion of maxillary bones and soft tissues has been per-
formed following large oncological defects or late effects
of radiation therapy (RT), and has proved to be a reliable
morphofunctional reconstruction technique.
When the treatment plan arranged by the clinical
team and the patient is to proceed with immediate maxil-
lary reconstruction, there are many opportunities available
using free tissue transfer techniques. All these techniques
have to provide not only for bone reconstruction but also
for the adequate rebuilding of the internal oral cavity. If
the length of bone to be reconstructed is between 6 and
15 cm and the treatment plan requires internal soft tissue
reconstruction even up to the orbital content (but with no
need for overlying facial skin or oral sphincter recon-
struction), the use of vascularized iliac crest with internal
oblique muscle flap has to be considered the flap of
choice among other possible free flaps.
The vascularized iliac crest with internal oblique muscle
flap DICA was popularized by Urken et al., when they
reported few failures and low donor site morbidity in their
1998 series.1,2 The use of the internal oblique muscle had
been considered inferior in outcome when compared with
the composite fibula flap described by Hidalgo and Pusic,3
a flap which is still in use because of its pedicle length,
considered longer than other composite flaps.
The vascularized iliac crest with internal oblique mus-
cle flap is a unique flap. It offers advantages in terms of
quality and quantity of bone for contouring of the orbital
floor, and of soft tissue for reconstruction of the mouth
or the orbital content. When used to line the oral cavity,
the internal oblique muscle becomes epithelialized and
therefore provides an excellent mucosal environment.
This muscle also fills the orbital content with a good
muscular bulk, reducing the risk of fistulas to the nasal
or oral cavity. The quality of bone is a satisfactory inter-
nal lining, providing good support for the eye or for an
implant-retention prosthesis.
The aim of this study is to report our experience with
the vascularized iliac crest with internal oblique muscle
flap for upper maxillary reconstruction.
PATIENTS AND METHODS
The clinical notes of 50 consecutive patients admitted
from June 2001 to October 2006 for malignant neoplasm
of the upper maxillary region were analyzed. The diagno-
sis, ‘‘Tumor Node Metastasis (TNM) Classification,’’ and
type of defect were recorded for each patient.
Of these patients, 24 were not included in the study
because they had a maxillectomy that was not reconstructed,
or had a reconstruction using a pedicled flap (i.e., temporalis
flap) or another free flap (i.e., latissimus dorsi or rectus
abdominis). The remaining 26 patients were then included in
our study on upper maxillary reconstruction.
1Department of Surgery-Maxillofacial Surgery Unit, Regional Hospital ‘‘Ca’Foncello,’’ Treviso, Italy2Department of Hand Surgery, University Policlinico, ‘‘G.B. Rossi,’’ Verona,Italy
*Correspondence to: Dr. Massimo Maranzano, Department of Surgery, Max-illofacial Surgery Unit, Regional Hospital ‘‘Ca’ Foncello,’’ Ospedale Sq,Treviso 31100, Italy. E-mail: [email protected]
Received 28 September 2006; Accepted 28 September 2006
Published online in Wiley InterScience(www.interscience. wiley.com). DOI10.1002/micr.20307
VVC 2007 Wiley-Liss, Inc.

Among all the classification attempts for maxillary
reconstruction that consider the entity of the remnant
defect (such as the one proposed by Cordeiro in Fig.
1),4,5 our choice was made by assessing the type of
defect and function using the classification proposed by
Brown from the Liverpool Group (Fig. 2).6–8
The flap harvesting surgical technique used was basi-
cally that described by Urken et al. in 1998,1,2,9–17 using
the superolateral approach, and the modification of this
technique described by Vaughan et al.,18 with the infero-
medial approach depending on the quantity of internal
oblique muscle needed.
Among treated cases, the flaps were raised ipsilaterlal
to the defect site in 45% of the procedures, and controlat-
erally in 55%, as in upper maxillary reconstruction there
is no significance based on the harvesting side. In all of
the cases there had been no necessity of including the an-
terior superior iliac spine (ASIS) in the flap. We per-
formed bone osteotomies to reshape the bone harvested
only when necessary.
The amount of internal oblique muscle harvested var-
ied among the patients treated and the extension of the
maxillectomy defect was between 45 and 120 sq cm,
being of minor extent in class 2A maxillectomies and
larger in 4C maxillectomies. The muscle was always well
vascularized on the ascending branch of the DICA/V.
In the oral cavity, the muscle becomes fibromucotized
and offered a good layer for implant placement. No trismus
was observed in any of our patients. In class 2–3B maxillec-
tomies, the bone portion of the flap had been positioned hor-
izontally (Figs. 3–6) or vertically (Figs. 7–9), with prevalence
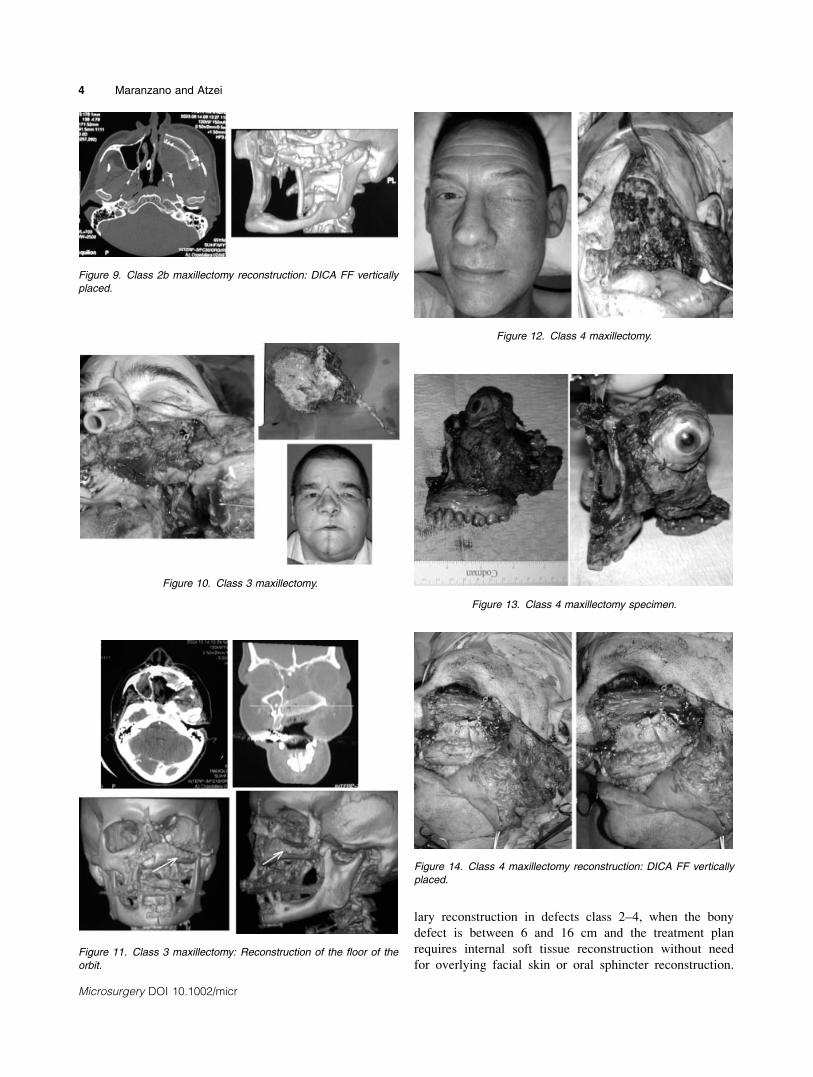
in the latter display. In class 3 maxillectomies, an important
point is that the orbit must be well supported. A vertical set-
up of the flap can accomplish this role. In this position, the
iliac crest bone can be remodeled to better reconstruct the
floor of the orbit (Figs. 10 and 11). In class 4 defects, if there
were eyelid or skin involvement, multiple flaps were raised,
namely composite DCIA and radial forearm flap (RFFF)
(Fig. 12–15) or DICA and latissimus dorsi FF, depending
on the area of skin needed or on the need of a bulky flap.
Particular care was used for the donor site closure: a
nonresorbable mesh in 2 layers was used in all patients.
No abdominal wall weakness developed in any patient
(Figs. 16 and 17).19
Neck dissections were carried out in 6 of the 26
patients, while 6 patients had secondary reconstruction
with this particular flap. A detailed assessment of the sur-
gical complications was carried out.
RESULTS
Twenty-six consecutive patients had a maxillectomy
reconstructed with a vascularized iliac crest with internal
oblique flap. There were 14 males and 12 females, with a
mean age of 56 years (range 23–72). According to the
classification proposed by JS Brown6–8 8% of our
patients were class 1 maxillectomies, 30% class 2, 40%
class 3 and 22% class 4, mainly b and c. Five patients
were operated on for secondary recurrence. All others
were treated for disease that required large ablation and
Figure 1. Cordeiro PG classification for maxillectomy defects.
Figure 2. Brown JS classification for maxillectomy defects.
2 Maranzano and Atzei
Microsurgery DOI 10.1002/micr

for which an immediate morphofunctional reconstruction
had been chosen.
The pedicle was consistently brought to the neck, ei-
ther by means of a subcutaneous tunnel in the cheek
from the maxillary region to the mandible border to use
the facial vessels in that area; or medially to the mandi-
ble ramus to the neck. One flap was lost 2 months after
RT because of major infection that led to the flap pedicle
closure. This particular patient had had high dose radio-
therapy postoperatively; however, there was no evidence
that this failure was caused directly by RT. No vein graft
had been necessary in any of our series.
DISCUSSION
The use of vascularized iliac crest with internal
oblique flap has become a flap of choice for upper maxil-
Figure 5. Class 2b maxillectomy reconstruction: DICA FF horizon-
tally placed.
Figure 6. Class 2b maxillectomy reconstruction: DICA FF horizon-
tally placed.
Figure 4. Class 2b maxillectomy defect.
Figure 7. Class 2b maxillectomy defect.
Figure 8. Class 2b maxillectomy reconstruction: DICA FF vertically
placed.
Figure 3. Class 2b maxillectomy.
Composite Upper Maxillary Reconstruction 3
Microsurgery DOI 10.1002/micr
lary reconstruction in defects class 2–4, when the bony
defect is between 6 and 16 cm and the treatment plan
requires internal soft tissue reconstruction without need
for overlying facial skin or oral sphincter reconstruction.Figure 11. Class 3 maxillectomy: Reconstruction of the floor of the
orbit.
Figure 14. Class 4 maxillectomy reconstruction: DICA FF vertically
placed.
Figure 9. Class 2b maxillectomy reconstruction: DICA FF vertically
placed.
Figure 10. Class 3 maxillectomy.
Figure 13. Class 4 maxillectomy specimen.
Figure 12. Class 4 maxillectomy.
4 Maranzano and Atzei
Microsurgery DOI 10.1002/micr
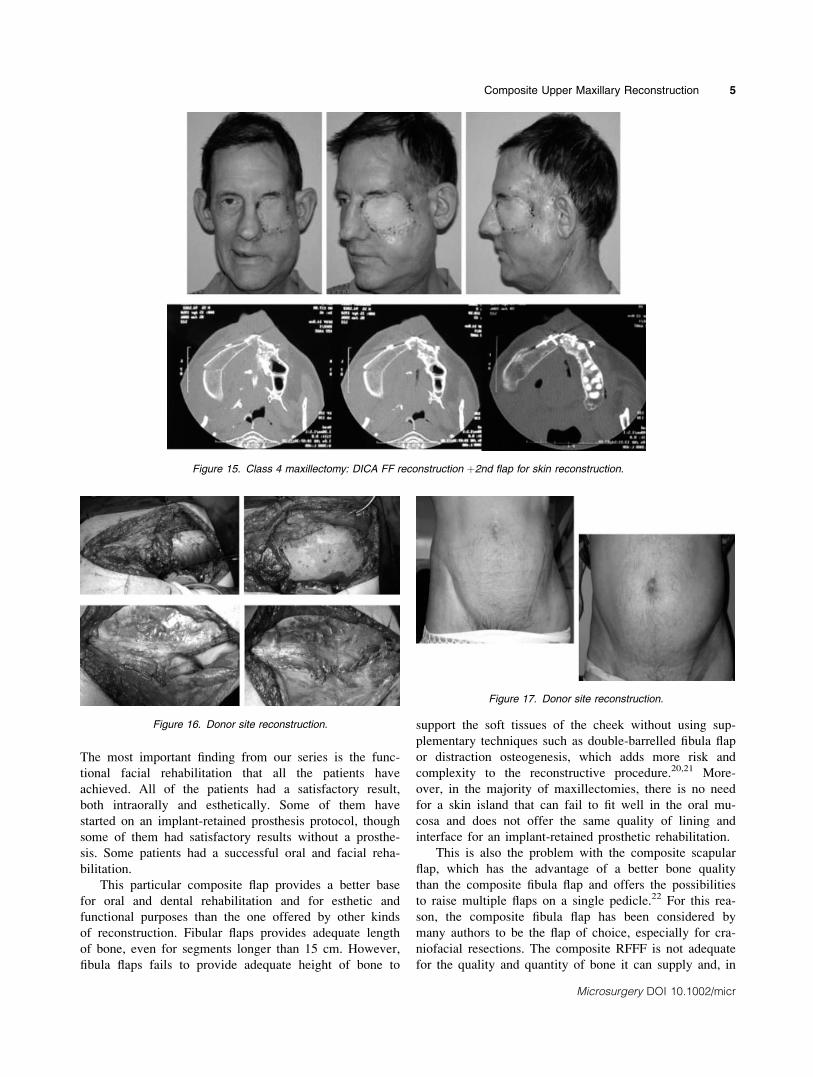
The most important finding from our series is the func-
tional facial rehabilitation that all the patients have
achieved. All of the patients had a satisfactory result,
both intraorally and esthetically. Some of them have
started on an implant-retained prosthesis protocol, though
some of them had satisfactory results without a prosthe-
sis. Some patients had a successful oral and facial reha-
bilitation.
This particular composite flap provides a better base
for oral and dental rehabilitation and for esthetic and
functional purposes than the one offered by other kinds
of reconstruction. Fibular flaps provides adequate length
of bone, even for segments longer than 15 cm. However,
fibula flaps fails to provide adequate height of bone to
support the soft tissues of the cheek without using sup-
plementary techniques such as double-barrelled fibula flap
or distraction osteogenesis, which adds more risk and
complexity to the reconstructive procedure.20,21 More-
over, in the majority of maxillectomies, there is no need
for a skin island that can fail to fit well in the oral mu-
cosa and does not offer the same quality of lining and
interface for an implant-retained prosthetic rehabilitation.
This is also the problem with the composite scapular
flap, which has the advantage of a better bone quality
than the composite fibula flap and offers the possibilities
to raise multiple flaps on a single pedicle.22 For this rea-
son, the composite fibula flap has been considered by
many authors to be the flap of choice, especially for cra-
niofacial resections. The composite RFFF is not adequate
for the quality and quantity of bone it can supply and, in
Figure 15. Class 4 maxillectomy: DICA FF reconstruction þ2nd flap for skin reconstruction.
Figure 16. Donor site reconstruction.
Figure 17. Donor site reconstruction.
Composite Upper Maxillary Reconstruction 5
Microsurgery DOI 10.1002/micr

our opinion, must be considered as a second choice flap
for maxillary reconstruction23 or as a second flap in case
of defects that include skin.
The vascularized iliac crest with internal oblique mus-
cle flap provides the best bone source for functional max-
illary reconstruction in terms of quality, quantity, and es-
thetic contouring of the face. This flap has the added
advantage of providing a unique oral mucosal lining ideal
for the implant soft tissue interface. The real question is
whether to reconstruct the maxillary area primarily or to
wait in order to better evaluate the resected area for sec-
ondary tumors. There is no established evidence in the
literature showing that patients who have delayed recon-
structions have better survival rates than those who have
primary reconstructions. All of these patients need close
follow-up, consisting of clinical examination, CT, MRI,
or TC-PET scans. These techniques are successful in
detecting recurrences or secondary neoplasms in the
reconstructed area.
The aim of this particular reconstruction technique is
for a morphofunctional primary reconstruction, even in
cases of large resection, including the temporal area. Pri-
mary use of vascularized iliac crest with internal oblique
muscle flap obtained a good esthetic contour that made it
possible to fully rehabilitate the patients and improves
their quality of life than that accomplished by using only
an obturator or soft tissue flap.
REFERENCES
1. Urken ML, Vickery C, Weinberg H, Buchbinder D, Lawson W,Biller HF. The internal oblique-iliac crest osseomyocutaneous freeflap in oromandibular reconstruction. Report of 20 cases. Arch Oto-laryngol Head Neck Surg 1989;115:339–349.
2. Genden EM, Wallace D, Buchbinder D, Okay D, Urken ML. Iliaccrest internal oblique osteomusculocutaneous free flap reconstructionof the postablative palatomaxillary defect. Arch Otolaryngol HeadNeck Surg 2001;127:854–861.
3. Hidalgo DA, Pusic AL. Free flap mandibular reconstruction: A 10-yearfollow-up study. Plast Reconstr Surg 2002;110:438–501.
4. Cordeiro PG, Santamaria E. A classification system and algorithmfor reconstruction of maxillectomy and midfacial defects. PlastReconstr Surg 2000;105:2331–2346.
5. Santamaria E, Cordeiro PG. Reconstruction of maxillectomy and mid-facial defects with free tissue transfer. J Surg Oncol 2006;94:522–531.
6. Brown JS. Deep circumflex iliac artery free flap with internal obli-quemuscle as a new method of immediate reconstruction of maxil-lectomy defect. Head Neck 1996;18:412–421.
7. Brown JS, Jones DC, Summerwill A, Rogers SN, Howell RA,Cawood JI, Vaughan ED. Vascularized iliac crest with internaloblique muscle for immediate reconstruction after maxillectomy. BrJ Oral Maxillofac Surg 2002;40:183–190.
8. Rogers SN, Lakshmiah SR, Narayan B, Lowe D, Brownson P,Brown JS, Vaughan ED. A comparison of the long-term morbidityfollowing deep circumflex iliac and fibula free flaps for reconstruc-tion following head and neck cancer. Plast Reconstr Surg 2003;112:1517–1525.
9. Taylor GI. Reconstruction of the mandible with free composite iliacbone grafts. Ann Plast Surg 1982;9:361–376.
10. Cordeiro PG, Santamaria E, Kraus DH, Strong EW, Shah JP. Recon-struction of total maxillectomy defects with preservation of the or-bital contents. Plast Reconstr Surg 1998;102:1874–1887.
11. Villaret DB, Futran NA. The indications and outcomes in the use ofosteocutaneous radial forearm free flap. Head Neck 2003;25:475–481.
12. Vinzenz KG, Holle J, Wuringer E, Kulenkamp KJ. Prefabrication ofcombined scapula flaps for microsurgical reconstruction in oro-maxillo-facial defects: A new method. J Craniomaxillofac Surg 1996;24:214–223.
13. Kelly CP, Moreira-Gonzalez A, Ali MA, Topf J, Persiani RJ, Jack-son IT, Wiens J. Vascular iliac crest with inner table of the ilium asan option in maxillary reconstruction. J Craniofac Surg 2004;15:23–28. [Erratum in J Craniofac Surg 2004;15:705].
14. Chang YM, Coskun.rat OK, Wei FC, Tsai CY, Lin HN. Maxillaryreconstruction with a fibula osteoseptocutaneous free flap and simul-taneous insertion of osseointegrated dental implants. Plast ReconstrSurg 2004;113:1140–1145.
15. Rohner D, Jaquiery C, Kunz C, Bucher P, Maas H, Hammer B.Maxillofacial reconstruction with prefabricated osseous free flaps: A3-year experience with 24 patients. Plast Reconstr Surg 2003;112:607–609.
16. Pogrel MA, Podlesh S, Anthony JP, Alexander J. A comparison ofvascularized and nonvascularized bone grafts for reconstruction ofmandibular continuity defects. J Oral Maxillofac Surg 1997;55:1200–1206.
17. Urken ML, Buchbinder D, Constantino P. Oromandibular reconstruc-tion using microvascular composite flaps. Arch Otolaryngol Head NeckSurg 1998;124:46–55.
18. Vaughan ED, Bainton R, Martin IC. Improvements in morbidity ofmouth cancer using microvascular free flap reconstruction. J Cranio-maxillofac Surg 1992;20:132–134.
19. Cricchio G, Lundgren S. Donor site morbidity in two differentapproaches to anterior iliac crest bone harvesting. Clin Implant DentRelat Res 2003;5:161–169.
20. Hidalgo DA, Rekow A. A review of 60 consecutive fibula freeflap mandible reconstruction. Plast Reconstr Surg 1995;96:585–596.
21. Podrecca S, Salvatori P, Paradisi S, Molinari R. ATTI de La rico-struzione microchirurgica del mascellare superiore XXIX ConvegnoNazionale di Aggiornamento AOOI: La chirurgia Ricostruttiva mi-crovasscolare in oncologia cervico-facciale, Modena 15 settembre 2005:133–137.
22. Swartz WM, Banis JC, Newton ED, Ramasastry SS, Jones NF,Acland R. The osteocutaneous scapular flap for mandibular andmaxillary reconstruction. Plast Reconstr Surg 1986;77:530–545.
23. Richardson D, Fisher SE, Vaughan DE, Brown JS. Radial forearmflap donor site complications and morbidity: A prospective study.Plast Reconstr Surg 1997;99:109–115.
6 Maranzano and Atzei
Microsurgery DOI 10.1002/micr





























