Embed Size (px)
Citation preview

THE VALUE O F MAINTENANCE THERAPY FOLLOWING TREATMENT OF CENTRAL NERVOUS SYSTEM
LEUKEMIA ELAINE MORGAN, MD,* MILTON H. DONALDSON, MD,+ AND ANNA T. MEADOWS, M D ~
The efficacy of intrathecal (IT) maintenance chemotherapy following central nervous system (CNS) leukemia was demonstrated in a retrospective study of 77 such episodes. The median durations of CNS and bone marrow (BM) remissions were significantly longer for the 41 maintained episodes (10f and 9.5 months, respectively) compared with the 36 unmaintained episodes (4 and 2 months, respectively). Patients were comparable in each of these two groups. For those patients receiving maintenance therapy, there appeared to be an advantage in using four or more doses of IT medications for treatment of CNS leukemia, regardless of the number of doses necessary to clear the cerebrospi- nal fluid (CSF).
Cancer 40:1005-1009, 1977.
N THE PAST, CENTRAL NERVOUS SYSTEM (CNS) I leukemia has been the most common site of extramedullary involvement in acute lympho- blastic leukemia (ALL) in childhood. Prior to the institution of effective prophylactic CNS therapy, the incidence of CNS involvement in ALL was 60-70%.'-' Even with prophylaxis, 5-10% of patients develop their initial relapse in the CNS.' Several types of treatment have been shown to be capable of inducting remission of CNS leukemia. These include intrathecal (IT) methotrexate (MTX), ' IT cytosine arabinoside (CA),' cranial' or craniospinal irradiation, and combined radiation and I T chemotherapy.' Un- fortunately, remissions of CNS leukemia are usually short-lived, lasting only 3 to 5 months.' Sullivan et al. in 1971" showed prolongation of the median duration of CNS remission in a
From The Children's Hospital of Philadelphia. Supported in part by Grant CA-08147 and Grant CA-
Children's hlemorial Hospital, Chicago, 111. ' Fox Chase Cancer Center, Philadelphia, PA. I The Children's Hospital of Philadelphia, Philadelphia.
P.4. Address for reprints: Anna T. hleadows, % I D , T h e Chil-
dren's Hospital of Philadelphia, 3400 Civic Center Boule- vard. Philadelphia, P.4 19104.
14489, National Canrer Institute.
.4ccepted for publication Ilecember 29, 1976.
group of children treated, following an initial CNS relapse, with maintenance IT MTX ad- ministered every 6-8 weeks after remission was attained.
At the Children's Hospital of Philadelphia, prolonged CNS therapy was instituted in an attempt to prevent, or at least delay, the recur- rence of a CNS relapse. This therapy consisted of monthly I T instillations of one or more medi- cations, following treatment and clearing of the cerebrospinal fluid (CSF). This report is a retro- spective comparative analysis of patients treated in this manner with those whose CNS episodes were similarly treated but who did not receive subsequent IT maintenance therapy.
MATERIALS A N D METHODS
The clinical records of 37 patients who had suffered one or more CNS leukemic relapses from 1965-1975 at the Children's Hospital of Philadelphia were reviewed. Thirty-three had ALL and four had acute nonlymphocytic leu- kemia. The initial white blood count was equal to or greater than 100,000/mm3 in eight pa- tients. Systemic chemotherapy in these patients was variable and, in general, consisted of a com- bination of agents including moderate dose (5
1005

1006 CANCER September 1977 Vol. 40
TABLE 1 . Characteristics of CNS Episodes
No. of episodes Main- Unmain- tained tained
Initial peripheral WBC < 10,00O/mm
>lOO,OOO/mma 10-99,999/mm a
unknown Marrow status at CNS episode
remission relapse
< I 0 0
>loo0
CSF WBC (per ma)
100-999
unknown lnitial CNS relapse Death-terminated CNS remission Marrow relapse prior to subsequent
CNS relapse Episodes/patierits Number of prior CNS relapses
median range
median range
Duration of disease
20 10 4 7
39 2
1 1 18 9 3
19 5
19 41/28
1 0-4
15 12 6 4
32 4
8 14 10 4
16 10
13 36/20
1 0-4
28 mo 17mo 3-91 mo 2-821110
mg/kg) intravenous infusion of methotrexate in 13 patients. Ten patients had received pro- phylactic treatment to the CNS (irradiation or repeated intrathecal medications or both) at varying intervals prior to their first CNS leu- kemic episodes.
Of the 80 episodes available for review, three are not included in the subsequent analysis since the patients failed to respond to initial therapy. The patients with the remaining 77 episodes were treated until the CSF was clear of cells. CSF was ,examined by cytocentrifuge technique beginning in 1972. Prior to that time CSF was considered positive if there were more than 10 mononuclear cells per mm*. This treatment con- sisted of radiation therapy alone, I T medication alone, or a combination. Maintenance therapy
TABLE 2. Treatment of CNS Episodes
No. of episodes Maintained Unrnaintained
Radiation alone 1 1 Radiation and IT Med(s) 8 9 I T Med(s) alone 32 26
TOTAL 41 36
consisted of monthly IT doses of the same drug(s) used to treat the preceding CNS relapse. For a patient to be eligible for maintenance ther- apy, the CSF had to be free of cells 4 weeks following cessation of treatment of the CNS epi- sode. A patient was considered to have received maintenance therapy if he received at least one dose of IT medication beginning at that time. Twenty-eight patients had 41 episodes treated with maintenance therapy while 20 patients had 36 episodes not so treated. The total is greater than 37 patients because some had episodes managed both ways.
RESULTS
Maintained and unmaintained groups were analyzed for characteristics that might influence the outcome; the groups were found to be simi- lar with respect to the following (Table 1): 1) association with initial peripheral WBC;2) mar- row status at the time of CNS episode; 3) CSF cell count at the time of CNS episode; 4) pro- portions which were initial CNS episodes; 5) episodes in which the CNS remissions were terminated by death rather than by documented antemortem CNS relapse; 6) episodes followed by marrow relapse prior to subsequent CNS relapse; and 7) median and range of number of prior CNS relapses. The median duration of disease at time of CNS relapse was somewhat longer in the maintained group (28 months vs. 17 months).
Treatment for induction of CNS remission was similar in maintained and unmaintained groups, since equal numbers of episodes in each group were treated with x-ray therapy alone, x- ray therapy and IT medications, or IT medica- tion alone (Table 2). Median CNS remission durations were similar in patients receiving IT MTX, IT MTX alternating with IT CA or triple IT therapy (MTX plus CA plus hydro- cortisone).
For consistency of calculations, length of CNS remission was computed from date of CNS epi- sode to date of subsequent CNS relapse or date of death. This may have underestimated the length of CNS remission in patients dying with- out CNS disease. However, omitting these epi- sodes did not alter the results. CSF was exam- ined every time a dose of IT medication was administered. Routine follow-up lumbar punc- tures were not performed in patients not receiv- ing IT therapy, but were done in the presence of CNS symptoms and/or systemic relapse. Al-
No. 3 MAINTENANCE THERAPY OF CNS LEUKEMIA Morgan et al. 1007
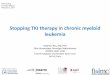
TABLE 3. CNS Remission Duration
Maintained Patients Episodes Median
Unmaintained Patients Episodes Median
Total group 28 41 10+ mo Crossover patients; 13 19 12 mo
20 36 4 mo 13 27 4 rno
* See text for definition.
though this might have delayed the diagnosis of CNS relapse, any bias so introduced would have had the effect of appearing to prolong the dura- tion of CNS remission in unmaintained patients in whom lumbar punctures were not performed routinely.
The overall median remission for the 41 epi- sodes in which maintenance therapy was given was 10+ months, while for the 36 unmaintained episodes, the median length of remission was 4 months. (Table 3). This difference is significant (p = 0.015). Exclusion of episodes terminating in death rather than CNS relapse yielded the same remission duration. Eight patients receiv- ing maintenance therapy are currently in remis- sion from 7+ to 19+ months; only one patient is in unmaintained remission after 66+ months and is off all therapy. .CNS relapse occurred during maintenance in 12 episodes and in 1-34 months (mean 7 months) after maintenance was discontinued in 21 episodes.
In the 13 patients in whom multiple CNS relapses were treated in both ways (“crossover” patients), 19 maintained episodes were com- pared with 27 unmaintained episodes. The mean remission durations for these subgroups were similar to those in the total groups (p < 0.005) (Table 3).
An additional factor which appeared to in- fluence length of remission in patients not re- ceiving radiation therapy was the number of IT
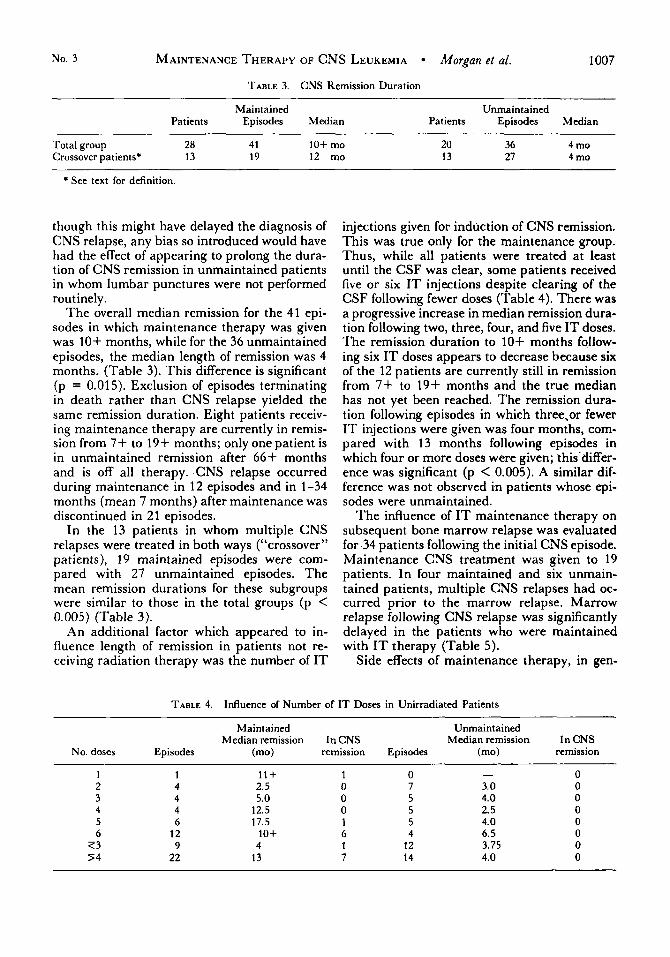
injections given for induction of CNS remission. This was true only for the maintenance group. Thus, while all patients were treated at least until the CSF was clear, some patients received five or six I T injections despite clearing of the CSF following fewer doses (Table 4). There was a progressive increase in median remission dura- tion following two, three, four, and five IT doses. The remission duration to 10+ months follow- ing six I T doses appears to decrease because six of the 12 patients are currently still in remission from 7+ to 19+ months and the true median has not yet been reached. The remission dura- tion following episodes in which three,or fewer IT injections were given was four months, com- pared with 13 months following episodes in which four or more doses were given; this’differ- ence was significant (p < 0.005). A similar dif- ference was not observed in patients whose epi- sodes were unmaintained.
The influence of I T maintenance therapy on subsequent bone marrow relapse was evaluated for 34 patients following the initial CNS episode. Maintenance CNS treatment was given to 19 patients. In four maintained and six unmain- tained patients, multiple CNS relapses had oc- curred prior to the marrow relapse. Marrow relapse following CNS relapse was significantly delayed in the patients who were maintained with I T therapy (Table 5).
Side effects of maintenance therapy, in gen-
TABLE 4. Influence of Number of IT Doses in Unirradiated Patients ~~ ~~ ~~ ~
Maintained Unmaintained Median remission In CNS Median remission In CNS
No. doses Episodes (mo) remission Episodes (mo) remission
1 2 3 4 5 6
7 3 5 4
1 1 1 + 4 2.5 4 5.0 4 12.5 6 17.5
12 10+ 9 4
22 13
0 7 5 5 5 4
12 14
- 3.0 4.0 2.5 4.0 6.5 3.75 4.0
1008 CANCER September 1977 Vol. 40
TABLE 5. Marrow Remission Duration following Initial CNS Episode
Maintained Unmaintained Patients Median Patients Median
19 10+ months 15 4 t months
eral, were mild, and included fever, headache, nausea and vomiting, meningismus, lethargy, mouth sores, and minimal myelosuppression. Seizures occurred in four patients with multiple CNS relapses; three of them developed chronic convulsive disorders which were medically con- trolled. Three patients with multiple CNS epi- sodes have developed additional neurological abnormalities (ataxia, cerebellar signs, abnor- mal cerebral function, and hyperactivity). Three of nine patients for whom autopsy findings are available had cortical atrophy and cerebral gliosis with CNS leukemic infiltration.
Fourteen patients who received CNS mainte- nance are alive with a median survival of 39+ months. Of these, seven are in continuous bone marrow (BM) remission for 2.5 to 6 years and two are in continuous CNS remission for 19+ and 24+ months. Five additional patients have sur- vived 4.5+ to 8 years with multiple CNS and BM relapses. Only one patient in the unmaintained group is in continuous BM and CNS remission following a single CNS relapse.
DISCUSSION
This study, encompassing an 1 1-year-period from 1965 to 1975, is complicated by hetero- geneity of patients, random although represen- tative sampling, and a retrospective analysis. Nonetheless, the two groups are well matched and certain implications can be drawn.
The median duration of CNS remission and the median interval to BM relapse following an episode of CNS leukemia was significantly longer when CNS maintenance therapy was ad- ministered. The intervals in the unmaintained episodes are similar to those previously re- ported.’ The thesis that CNS remission is pro- longed by maintenance therapy is further sup- ported by comparing these durations in the maintained and unmaintained episodes (12 months versus 4 months) in the 13 patients who received both forms of treatment. The reason for the prolongation of marrow remission in pa- tients receiving IT maintenance therapy is not clear. It is unlikely that the small amount of
medication transported from the CNS to the systemic circulation once a month could have had any significant effect. It could be postulated that maintenance IT chemotherapy had an ef- fect on a subclinical population of leukemic cells in the CNS. Elimination of these cells might then have prevented “reseeding” of the marrow. If this is true, perhaps systemic reinduction at the time of CNS relapse might eliminate a cell population already “seeded” from the CSF and thus further delay or even prevent systemic re- lapse.
Another provocative feature of this analysis was the correlation between the number of in- duction doses and the length of the subsequent maintained CNS remission. The mechanism of this correlation has not been studied. In all in- stances, the CSF was clear prior to starting maintenance. Possibly, the additional IT doses further reduced residual subclinical CNS leu- kemia, which resulted in a smaller leukemic cell burden and thus a longer interval to recurrence of CNS disease.
In general, this maintenance program was well tolerated and side effects were minimal, although four patients suffered residual neuro- logic problems. The etiology is unclear since these patients also had multiple CNS relapses. Severe leukoencephalopathy has been seen fol- lowing a variety of therapeutic modalities, but the causative factors in this syndrome have not yet been fully elucidated. ’*’~‘*‘ Nonetheless, any management of CNS leukemia must weigh the relative morbidity, particularly, long-term se- quelae, against the benefit. Thus, while cranios- pinal irradiation may be effective in obtaining prolonged CNS remission, lo this modality car- ries with it the potential of significant myelo- suppression. Induction of CNS remission with IT therapy followed by monthly maintenance may be an effective alternative approach. This report suggests the need for further study of: a ) the relative effectiveness of CNS irradia- tion versus IT medication versus a combination of these modalities, each with maintenance IT therapy, in the treatment of CNS leukemia; b) the optimal length of CNS treatment to attain long-term CNS remissions; and c) the effective- ness of reinduction at the time of CNS relapse in prolonging BM remission.
CNS leukemia continues to be a serious but much less frequent clinical problem since the introduction of CNS prophylaxis. These results indicate that a course of four to six IT injections over 4 to 6 weeks, followed by monthly mainte-

MAINTENANCE THERAPY OF CNS LEUKEMIA Morgan el af. 1009
programs, a proportion of children .suffering CNS relapse may survive to enjoy prolonged complete remission.
No. 3
nance IT medication is effective in prolonging remission in leukemic children following CNS relapse. With further improvement of treatment
REFERENCES
1 . Duttera, M. J., Bleyer, W. A., Pomeroy, T. C., et al.: Irradiation methotrexate toxicity and the treatment of men- ingeal leukemia. Lancel 2:703-707, 1973.
2. Halikowski, B., Cylkis, R., Armato, J., et al.: Cytosine arabinoside administered intrathecally in cerebromeningeal leukemia. A d a Paediatr. Scand. 59:164-168, 1970.
3. Hendin, B., DeVito, D.C., Tarack, R., et al.: Parenchy- matous degeneration of the central nervous system in child- hood leukemia. Cancer 33:468-482, 1974.
4. Kay, H. E. M., Knapton, P. J., O’Sullivan, J. T., et 01.: Encephalopathy in acute leukemia associated with metho- trexate therapy. Arch. Dis. Child. 47:344-354, 1972.
5. Kim, T . , Nesbit, M. E., D’Angio, G. J., el al.: The role of CNS irradiation in children with ALL. Rudtolosy 104:635-641, 1972.
6. Meadows, A. T., and Evans, A. E.: Effects of chemo- therapy on the central nervous system. Cancer 37:1079-1085, 1976.
7. Price, R. A,, and Jamieson, P. A.: The CNS in child- hood leukemia. Cancer 35:306-318, 1975.
8. Sullivan, M. P., Humphrey, B., Vietti, T. .J., et al.: Superiority of conventional intrathecal methotrexate ther- apy with maintenance over intensive intrathecal methotrex- ate therapy unmaintained or radiotherapy (2000-2500 rads tumor dose) in treatment for meningeal leukemia. Cancer 35: 1066- 1073, 1975.
9. Sullivan, M. P., Vietti, T. J., Fernbach, D. J., el al.: Clinical investigations in the treatment of meningeal leu- kemia radiation therapy vs. conventional intrathecal metho- trexate. Blood 34:301-319, 1969.
10. Sullivan, M. P., Vietti, T. J., Haggard, M. E., et al.: Remission maintenance therapy for meningeal leukemia- intrathecal methotrexate vs. intravenous bis-nitrosuria. Bloud 38:680-687, 1971.
1 1 . Willoughby, M. L. N.: Treatment of overt meningeal leukemia in children-Results of second MRC meningeal leukaemia trial. Br. Med. J . 1:864-867, 1976.
















![Biochemically Directed Therapy of Leukemia with Tiazofurin ...(CANCER RESEARCH 49. 3696-3701. July I. 1989] Biochemically Directed Therapy of Leukemia with Tiazofurin, a Selective](https://img.dokumen.tips/doc/110x75/5e75c23a566ad9571f42dadf/biochemically-directed-therapy-of-leukemia-with-tiazofurin-cancer-research.jpg)