Embed Size (px)
Citation preview

The Use of Radiotherapy for Treatment of Isolated Locoregional Recurrence of Breast Carcinoma
After Mastectomy
WILLIAM J. ABERIZK, MD,*.t BARBARA SILVER,* I. CRAIG HENDERSON, MD,$ BLAKE CADY, MD,§ AND JAY R. HARRIS, MD*
The role of radiotherapy in the treatment of isolated local recurrence of breast cancer after mastectomy is controversial. In an attempt to define this role, the results of moderate-dose radiotherapy in 90 such patients were reviewed. The median follow-up time for these patients was 81 months. The actuarial probability of local control after treatment was 42% at 5 years and 35% a t 10 years. Freedom from distant failure was 30% at 5 years and only 7% at 10 years. The rate of appearance of distant metastasis was fairly constant at approximately 20% of patients per year. Overall survival was 50% at 5 years and 26% at 10 years. Overall survival and relapse-free survival were both chiefly influenced by the disease-free interval (DFI). Patients who presented with a DFI of greater than or equal to 2 years had a 5-year actuarial overall survival rate of 58% compared to 33% for patients with a DFI of less than 2 years (P = 0.04). Subsequent local failures after radiotherapy were principally seen at the initial site of recurrence, but also a t other sites in or a t the edge of the radiation fields. These results strongly suggest that patients with apparently isolated local recurrence after mastectomy are incurable by further local treatment. Effective systemic therapy is required to improve the results in these patients. Radiotherapy is a useful palliative procedure in patients with long disease-free intervals. The role of radiotherapy in conjunction with systemic therapy is, as yet, undefined.
Cancer 58:1214-1218, 1986.
SOLATED LOCOREGIONAL RECURRENCE of breast cancer I after mastectomy refers to the reappearance of breast cancer on the chest wall or in regional lymph node areas in the absence of other disease on routine evaluation for metastases. Numerous mechanisms for local recurrence have been proposed and include incomplete resection of the tumor initially, transection of involved lymphatics at the time of mastectomy, and hematogenous spread to a previously traumatized site. These recurrences typically present as apparently innocent masses and historically were treated with simple excision. Such treatment, how- ever, was found to be associated with subsequent local recurrence in the large majority of patients.',2 This ex- perience with limited treatment has demonstrated that
Abstract presented October 1984, Annual Meeting of the American Society of Therapeutic Radiologists and Oncologists.
From the *Department of Radiation Therapy, Joint Center for Ra- diation Therapy, and $Department of Medicine, Dana-Farber Cancer Institute, and the SDepartment of Surgery, New England Deaconess Hospital, Harvard Medical School, Boston, Massachusetts.
t Current address: Hartford Hospital, Hartford, Connecticut. Address for reprints: J . R. Hams, MD, Joint Center for Radiation
'Therapy, Department of Radiation Therapy, Harvard Medical School, 50 Binney Street, Boston, MA 021 15.
Accepted for publication January 8, 1986.
local recurrence, even when apparently small, is typically an indication of more extensive chest wall disease. Based on these results, the conventional treatment for isolated locoregional recurrence has been excision of the recur- rence, when possible, followed by wide-field radiotherapy. The results of this treatment have been previously reported to be generally poor, in that treated patients have a high risk for the subsequent development of symptomatic metastatic breast ~ a n c e r . ~ - ~
In this report we review our experience in treating pa- tients with locoregional recurrence after mastectomy with radiotherapy. The purpose of the study is to assess more fully the results of radiotherapy with respect to local tumor control, freedom from distant relapse, and overall survival. In addition, we analyzed the patterns of failure after ra- diotherapy in an attempt to understand better the nature of isolated locoregional recurrence and to identify patients who might benefit from such treatment.
Materials and Methods
The records of 90 patients with locoregional recurrence after mastectomy for breast carcinoma were analyzed. All patients received radiation therapy at the Joint Center for
1214
No. 6 RADIOTHERAPY FOR LOCAL RECURRENCE * Aberizk et al. 1215
Radiation Therapy, Harvard Medical School between July 1968 and December 1978. All patients had a biopsy- proven recurrence and a negative metastatic work up (usually chest x-ray and bone scan) before undergoing radiotherapy. Median follow-up was 8 1 months and min- imum follow-up was 5 1 months, although 17 patients were lost to follow-up between 1 and 62 months after radiation therapy and censored at the time of last follow-up.
Initial surgery was radical mastectomy for 54 patients and modified radical mastectomy for 36 patients. At the time of radiation therapy 43 patients were premenopausal and 47 patients were postmenopausal, Twenty patients had had prior conservative treatment (excision only or low dose radiation therapy) for recurrence after mastec- tomy. Six patients had persistence of such a recurrence for which they subsequently underwent definitive radia- tion therapy.
The chest wall alone was involved in 45 patients. Lymph node areas alone were involved in 21 patients, and both the chest wall and lymph node areas were in- volved in 24 patients. Thirty patients had excisional biop- sies of the recurrence and 60 patients had less than ex- cisional biopsy (incisional biopsy). Five patients had re- ceived adjuvant hormonal therapy or chemotherapy after mastectomy. Thirty-six patients received such treatment only after developing locoregional recurrence. Sixteen of these 36 patients received hormonal therapy or chemo- therapy concomitantly with radiation therapy for local recurrence. The interval from mastectomy to locoregional recurrence was less than 24 months in 32 patients and 24 months or greater in 58 patients.
Patients were treated with a variety of radiation therapy techniques and fields. Patients were typically treated to a dose of 4500 rad in 20 fractions over 5 weeks to the chest wall (CW) and/or draining lymph node regions (internal mammary [IM], supraclavicular [SC], axillary [AX]) on a 4 MV linear accelerator. The CW and IM nodes were usually treated with tangential fields, and the SC and/or AX nodes were treated with a single anterior photon field. Thirty-eight patients also received a “boost field” to the site of recurrence, employing smaller photon tangential fields or an electron field. The range of doses employed was 2275 to 8500 rad. The prescribed dose was less than 4500 rad in 19 patients, 4500 to 4999 rad in 30 patients, and greater than 5000 rad in 41 patients.
Twenty-three patients received treatment to the CW and IM, SC, and AX nodes. Fifty-three patients were treated to the CW and IM and/or SC and/or AX nodes. Eleven patients were treated to the CW only and three to lymph node areas only.
Complete clinical regression (CCR) was defined as the disappearance of all disease on clinical evaluation. The actuarial probabilities of local control, freedom from dis- tant failure, and survival were calculated using the Kaplan-
I I
5 10
T/#€ fveorsl
10‘
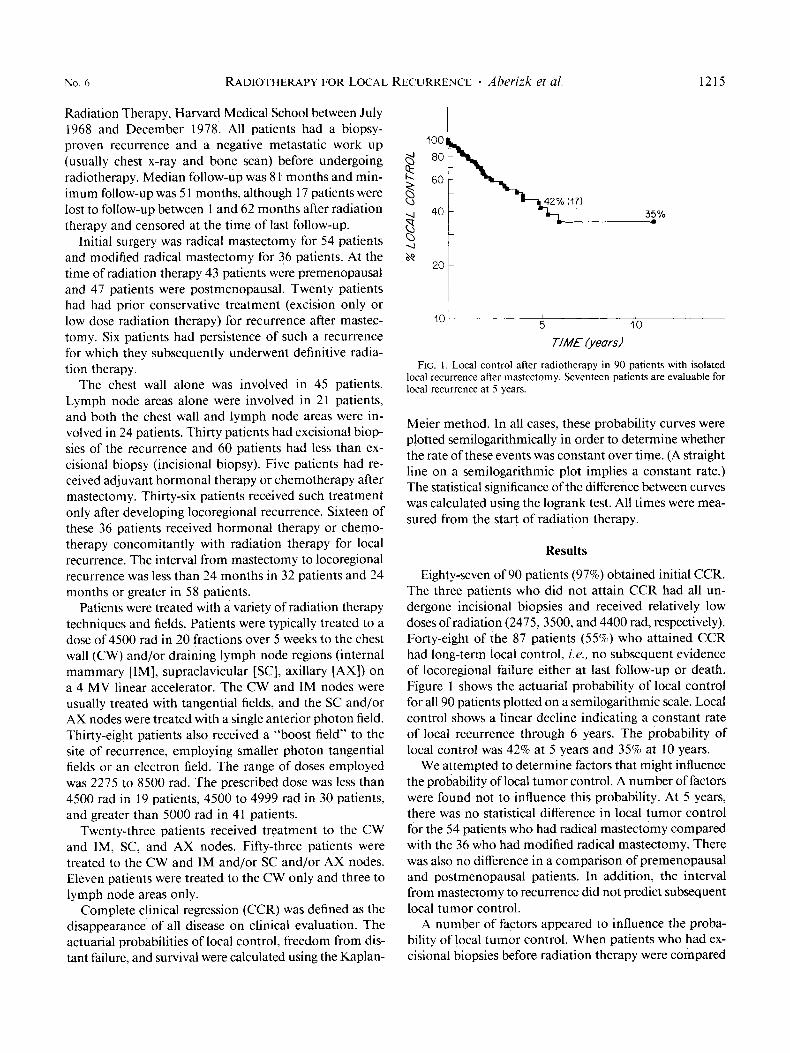
FIG. 1. Local control after radiotherapy in 90 patients with isolated local recurrence after mastectomy. Seventeen patients are evaluable for local recurrence at 5 years.
Meier method. In all cases, these probability curves were plotted semilogarithmically in order to determine whether the rate of these events was constant over time. (A straight line on a semilogarithmic plot implies a constant rate.) The statistical significance of the difference between curves was calculated using the logrank test. All times were mea- sured from the start of radiation therapy.
Results
Eighty-seven of 90 patients (97%) obtained initial CCR. The three patients who did not attain CCR had all un- dergone incisional biopsies and received relatively low doses of radiation (2475, 3500, and 4400 rad, respectively). Forty-eight of the 87 patients (55%) who attained CCR had long-term local control, i.e., no subsequent evidence of locoregional failure either at last follow-up or death. Figure 1 shows the actuarial probability of local control for all 90 patients plotted on a semilogarithmic scale. Local control shows a linear decline indicating a constant rate of local recurrence through 6 years. The probability of local control was 42% at 5 years and 35% at 10 years.
We attempted to determine factors that might influence the probability of local tumor control. A number of factors were found not to influence this probability. At 5 years, there was no statistical difference in local tumor control for the 54 patients who had radical mastectomy compared with the 36 who had modified radical mastectomy. There was also no difference in a comparison of premenopausal and postmenopausal patients. In addition, the interval from mastectomy to recurrence did not predict subsequent local tumor control.
A number of factors appeared to influence the proba- bility of local tumor control. When patients who had ex- cisional biopsies before radiation therapy were compared

1216 CANCER September 15 1986 Vol. 58
TABLE 1. Analysis of Second Locoregional Failure*
Excisional biopsy lncisional biopsy Second failure (29 patients) (58 patients)
~~
In field Out of field
Total
9 I
10
20 9
29
* 39 patients total.
with patients who had less than excisional biopsies, the difference between the 5-year rates of local tumor control approached statistical significance. For the 26 patients who had excisional biopsy and doses greater than 4000 rad, 5- year local tumor control was 57% compared with 24% for the 54 patients who had incisional biopsies and doses greater than 4000 rad (P = 0.03). Of note, however, these two groups were not identical in terms of tumor bulk; patients who had less than excisional biopsies tended to have more extensive disease. Therefore, these differences in local tumor control may reflect factors other than type of biopsy. For patients with both nodal and chest wall recurrence, the 5-year rate of local tumor control was lo%, compared to 47% for patients with chest wall only disease ( P = not significant), and 78% for patients with nodal disease alone ( P = 0.05). Of note, no patient with both chest wall and nodal disease as a site of first recurrence was locally free of disease at 6 years.
We attempted to evaluate the importance of radiation dose in achieving local tumor control. This analysis of dose was limited by a fairly narrow range of doses used in treating the majority of our patients. Furthermore, physician selection resulted in the use of higher doses of radiation for patients with more extensive recurrences. We were not able to demonstrate a dose-response rela- tionship in our data, however the mean dose for patients who had a second local failure (4881 rad) was less than that for patients who did not fail (5002 rad).
We performed an analysis of failure among the 39 pa- tients who had a second local failure after an initial com- plete clinical response (Table 1). Ten of the 29 patients who had an excisional biopsy of their first recurrence had a subsequent local failure. Nine of these 10 patients failed within the radiation field (“in field”). Twenty-nine of the 58 patients who had an incisional biopsy for their first recurrence before radiation therapy had a second failure. Twenty of these 29 patients failed in field. Of the ten pa- tients who failed out of field (after incisional or excisional
TABLE 2. Analysis of Second Locoregional Failure In-Field Recurrence
Excisional Incisional
Original site 8 Other I
Total 9
17 3
20
biopsy) nine failed on the chest wall adjacent to the treated area, so it is appropriate to consider these failures as mar- ginal misses. In other words, 38 of 39 second failures were either in-field failures or marginal misses. Table 2 shows the analysis of failure for patients with in-field recurrence. Of the nine patients with in-field recurrence after exci- sional biopsy, eight failed at the original site of recurrence even though in many cases a boost dose had been delivered to these areas. Similarly, of the 20 patients who failed in field after incisional biopsy, 17 failed at the original site.
Figure 2 shows the actuarial probability of freedom from distant relapse for all 90 patients. Freedom from distant relapse was 30% at 5 years and only 7% at 10 years. Figure 3 shows the actuarial probability of survival in these 90 patients plotted on a semilogarithmic scale. The curve shows a straight line decline indicating a con- stant force of mortality. Overall survival was 50% at 5 years and 26% at 10 years. We attempted to evaluate fac- tors which influenced survival. Survival was not influenced by the type of mastectomy, menopausal status, or the type of biopsy performed at the time of recurrence. The only factor that appeared to influence survival was the disease- free interval (DFI), the time elapsed from mastectomy to the initial isolated local recurrence (Fig. 4). For the 58 patients with DFI greater than or equal to 24 months, 58% were alive at 5 years, versus 33% of the 32 patients with DFI less than 24 months (P = 0.04). At 10 years, the effect persists with survival rates of 36% and 7%, re- spectively ( P = 0.007). The two curves are linear on a semilogarithmic scale, indicating a constant force of mor- tality in each group.
Relapse-free survival (RFS) was also found to be influ- enced by DFI. For the 58 patients with DFI greater than or equal to 24 months, 36% were alive without evidence of relapse at 3 years compared to only 20% for patients with DFI less than 24 months ( P = 0.05). Using a dividing line of DFI equal to 36 months improves this difference in RFS only slightly (42% vs. 20%, P = 0.01).
Discussion
In this retrospective review, we have analyzed the like- lihood of freedom from distant failure, survival, and local tumor control in patients treated with radiation therapy for apparently isolated locoregional recurrence of breast cancer after mastectomy. Our results indicate that these patients have a poor prognosis similar to that noted by previous investigator^.^-^ Seventy percent of patients manifested distant failure by 5 years, and 93% by 10 years. By the use of a semilogarithmic plot, the curve denoting the probability of freedom from distant failure was found to be consistent with a straight line, indicating that these patients have a constant risk of distant failure over time. During the period of follow-up, approximately 20% of remaining patients each year failed distantly.

No. 6 RADIOTHERAPY FOR LOCAL RECURRENCE * Aberizk el al. 1217
5 10 5 10 10
FIG. 3. Overall survival after radiotherapy in 90 patients with isolated FIG. 2. Freedom from distant failure after radiotherapy in 90 Patients local recurrence after mastectomy.
with isolated local recurrence after mastectomy.
Survival after treatment similarly showed a progressive decline with time. Since breast cancer patients can survive for long periods with metastatic disease, the survival rate was significantly higher than the freedom-from-distant failure rate. At 5 years, 50% of patients were alive and at 10 years, 26% were alive. Of interest, the survival rate was found to be influenced only by the DFI, a measure of the inherent pace of the disease itself. This correlation between DFI and survival has been previously noted by Bedwinek et aL9 and Danoff e? a/.'
Local tumor control after radiotherapy in this series was not found to be permanent. Although nearly all pa- tients showed a complete clinical response (ie., idisap- pearance of the disease on gross examination) many pa- tients developed a secondary recurrence in the treated area. The doses of radiation used in this series of patients were generally modest, and it is possible that improved local tumor control would be seen using higher 'doses. The analysis of local failure presented here indicates that the predominant site of secondary local failure was the initial site of recurrence, but failures also were seen in other sites in and at the edge of the radiation fields. As a result of these findings, we have modified our treatment approach to include the use of surgical resection of gross disease when feasible, more generous radiation fields to the entire chest wall area, and higher doses of radiation to the chest wall and, in particular, to the area(s) of gross recurrence.
The question arises whether the likelihood of freedom from distant failure and survival would be improved by an increased level of local tumor control. In a recent 1-eport from Chen et al. in which somewhat higher doses of ra- diation were used, survival rates were similar to those obtained here.l0 This observation, coupled with the ob- served exponential decline in freedom from distant failure,
suggests that locoregional recurrence after mastectomy is nearly always associated with systemic involvement. As a result, we believe that increased local tumor control in this situation would be unlikely to result in improved sur- vival. Nevertheless, local tumor control should be viewed as a goal in itself since patients generally consider the presence of cancer on the chest wall to be a highly dis- turbing manifestation of the disease.
It is clear from these data that effective systemic therapy will be required to improve the results of treatment in these patients. It is not certain at this time whether cur- rently available chemotherapeutic combinations will be successful in this situation. Given the high likelihood of extensive chest wall disease generally unamenable to ad- equate surgical resection, it seems sensible to consider
10 c '1, I I I
5 10
TIM€ fyeursl
FIG. 4. Overall survival after radiotherapy compared in 58 patients with disease-free interval (DFI) greater than or equal to 24 months and 32 patients with DFI less than 24 months.

1218 CANCER September 15 1986 Vol. 58
local radiotherapy as part of an aggressive potentially cu- rative program. At the present time, however, it is un- certain if best results are achieved by local treatment alone, systemic treatment alone, or combined-modality treat- ments. These various approaches will require evaluation using controlled clinical trials in order to be certain which is preferable.
We would like to stress that the patients described here were generally treated with mastectomy alone as initial therapy. In recent years, we have increasingly seen patients who present with locoregional recurrence after mastec- tomy and adjuvant chemotherapy as initial therapy. Ad- juvant chemotherapy after mastectomy does not appear to prevent locoregional recurrence in patients at high-risk for local Only five of the patients reported here, however, received adjuvant chemotherapy. It is not certain at this time whether the natural history of the dis- ease and its response to either radiotherapy or chemo- therapy for treatment of recurrent disease are affected by the use of initial adjuvant chemotherapy.
The results presented here have provided us with new guidelines based on the DFI for the treatment of local recurrence. These guidelines are not applied strictly since the individual clinical situation can vary widely. In gen- eral, however, we believe that local radiotherapy should not be used routinely as initial treatment for patients who develop locoregional recurrence soon after mastectomy, since these patients typically manifest systemic disease shortly after such treatment. It seems preferable to perform a small biopsy for diagnostic purposes only, without at- tempting a gross excision, and to use systemic therapy initially in these patients. Whether to use radiotherapy after a good response to systemic therapy is unclear. The data presented here do not address this issue. It can be argued, however, that the use of radiotherapy would im- prove local tumor control, thereby decreasing the likeli- hood of symptomatic local disease, and possibly increase the subsequent relapse-free interval. We would like to point out that this approach of initial systemic therapy is generally applied only in patients with evaluable disease after biopsy. In patients who are rendered free-of-disease by the biopsy procedure, systemic therapy is usually with- held since they are not symptomatic and do not have disease that can be used as a measure of response. For these patients, it is generally preferable to use radiation therapy to decrease the likelihood of further local recur- rence.
For patients who present at long intervals after mas- tectomy, the use of gross excision (when feasible) and ra- diotherapy alone generally provides a reasonable relapse- free period. Many of these patients are likely to be estrogen receptor protein-positive and could also be considered for hormonal manipulation. The advantages of using radio- therapy instead of hormonal therapy in this situation are that it has a higher response rate and that it allows hor- monal manipulation to be reserved for use at the time of
systemic failure. In this series, 58 patients were treated after incisional biopsy with local radiotherapy, and 85% obtained a complete clinical regression of their disease. In contrast, hormonal therapy generally results in a com- plete or partial response in only 60% to 70% of appropriate patients. The advantage of using hormonal therapy instead of radiotherapy when a complete excision is not feasible is that the patient’s sensitivity to hormonal therapy can be determined at a time when there is an easily measurable chest wall lesion. It is not unreasonable to treat a patient initially with hormonal therapy, use radiotherapy at the time of maximal local response to hormonal therapy, and continue hormonal therapy until the patient develops a distant recurrence. At that time, one could use another hormonal therapy, confident that the patient’s tumor is actually sensitive to this form of systemic therapy.
In conclusion, these results strongly suggest that patients with apparently isolated local recurrence after mastectomy are incurable by further local treatment, and that effective systemic therapy is required to improve the results in these patients. Radiotherapy is a useful palliative procedure in patients with long disease-free intervals. The role of ra- diotherapy in conjunction with systemic therapy is, as yet, undefined.
REFERENCES
1. Zimmerman KW, Montague ED, Fletcher GH. Frequency, ana- tomical distribution and management of local recurrences after definitive therapy for breast cancer. Cancer 1966; 1:67-74.
2. Beck TM, Hart NE, Woodard DA, Smith CE. Local or regionally recurrent carcinoma of the breast: Results of therapy in 12 I patients. J C[in Oncol 1983; 1:400-405.
3. Spratt John S. Locally recurrent cancer after radical mastectomy. Cancer 1967; 20:1051-1053.
4. Toonkel LM, Fix I, Jacobson LH, Wallach CB. The significance of local recurrence of carcinoma of the breast. Int J Radiat Oncol Biol
5 . Danoff BF, Coia LR, Cantor RI, Pajak TF, Kramer S. Locally recurrent breast carcinoma: The effect of adjuvant chemotherapy on prognosis. Radiology 1983; 1472349-852.
6. Marshall KA, Redfern A, Cady B. Local recurrences of carcinoma of the breast. Surg Gynecol Obstet 1974; 139:406-408.
7. Chu FCH, Lin FJ, Kim JH, Huh SH, Garmatis CJ. Locally recurrent carcinoma of the breast. Cancer 1976; 37:2677-268 1.
8. Bedwinek JM, Fineberg B, Lee J, Ocwieza M. Analysis of failures following local treatment of isolated local-regional recurrence of breast cancer. In! J Radiat Oncol Biol Phys 1981; 7:581-585.
9. Bedwinek JM, Lee J, Fineberg B, Ocwieza M. Prognostic indicators in patients with isolated local-regional recurrence of breast cancer. Cancer
10. Chen KK, Montague ED, Oswald MJ. Results of irradiation in the treatment of locoregional breast cancer recurrence. Cancer 1985; 56:
1 I . Bonadonna G, Valagussa P, Rossi A ef al. Ten-year experience with CMF-based adjuvant chemotherapy in resectable breast cancer. Breast Cancer Res Treat 1985; 5:95-115.
12. Griem K, Henderson IC, Gelman R et a/. The role of radiotherapy in patients receiving adjuvant chemotherapy after mastectomy: Results of a randomized trial. Proc Am Soc Therapeutic Radiol Oncol 1985; (Suppl) 11:151.
13. Rao AR, Murthy AK, Hendnckson FR et al. Analysis of risk factors for loco-regional failure in stage I1 (TINIMO and T2N1MO) breast cancer treated with mastectomy and adjunctive chemotherapy. Proc Am Soc Therapeutic Radiol Oncol 1985; (Suppl) 1 1 : 15 1.
Phys 1983; 9~33-39.
1981; 4712232-2235.
1269- 1273.





























