Embed Size (px)
Citation preview

S
V A L U E I N H E A L T H 1 4 ( 2 0 1 1 ) 4 5 8 – 4 6 4
avai lable at www.sc iencedirect .com
journal homepage: www.elsevier .com/ locate / jva l
The Use of Quality-Adjusted Life-Years in the Economic Evaluation ofHealth Technologies in Spain: A Review of the 1990–2009 LiteratureJosé Manuel Rodriguez, MSc1, Silvia Paz, MD, MSc2,*, Luis Lizan, MD, MSc, PhD3, Paloma Gonzalez, MSc4
1Johnson & Johnson, Madrid, Spain; 2Outcomes’10, Castellon, Spain; 3Outcomes’10, Castellon, Spain; Department of Economy, “Jaume I” University, Castellon,
pain; 4Medtronic Ibérica, Madrid, SpainA B S T R A C T
twpdtttetGdKt
Objective: To appraise economic evaluations of health technologiesthat included quality-adjusted life-years (QALYs) as an outcome mea-sure conducted over the past 20 years in Spain. Methods: A systematicreview of the literature was conducted. Economic evaluations that in-cluded QALYs as an outcome measure, conducted in Spain and pub-lished between January 1990 and December 2009 were identified. Pri-mary and gray literature sources were reviewed. Results: A total of 60articles and 4 health technology assessment reports were included.Key findings were 1) the vast majority of articles (77.1%) referred totherapeutic interventions; 2) 63.2% dealt with pharmaceutical productsand much fewer with preventive strategies, medical devices, or diag-nostic interventions; 3) most evaluations referred to cardiovascular-(19.8%), respiratory- (16.3%), and cancer- (13.0%) related processes; 4)80.3% were based on a theoretical model, most commonly Markov
models (71.4%); 5) 67.3% adopted the National Health System perspec- ©a at tadri
tifico
nc.
doi:10.1016/j.jval.2010.10.039
ive; 6) information on the methods used to describe the health statesas given in 45.1% of studies; 7) 40.3% used the EuroQoL-5D to elicitreferences, whereas 66.1% gave no details on the methods applied toetermine patients’ choices; 8) it was possible to state who completedhe questionnaires in only 17.7% of studies; 9) 77.1% of the interven-ions assessed were below the €30,000/QALY suggested affordablehreshold in Spain. Conclusions: An increasing number of economicvaluations using QALYs had been conducted. Most of them relied onheoretical models. Several methodological issues remain unsolved.reat disparity exists regarding the reporting of the methods used toetermine health states and utility values.eywords: cost-utility analysis, economic evaluation, healthechnologies, quality-adjusted life-years.
2011 Published by Elsevier Inc.
Introduction
Decision makers, health managers, and health professionals usethe results of the economic evaluations of health technologiesto know what the efficiency of different options is to identify themost favorable ones to more equitably allocate resources [1]. Acornerstone of such economic evaluation is the cost-utilityanalysis. It presents the distinctive feature of having as its out-come measure an index that comprises the quantity and thequality of life gained as a consequence of implementing thetechnology being assessed [2]. This measure is the quality-ad-justed life-year (QALY), which combines the effects of healthinterventions on mortality and health-related quality of life(HRQoL) into a single index that adjusts life expectancy for thequality measured [3]. The intent of developing this type of out-come measure is to provide payers, managers, and governmen-tal organizations with a standardized instrument on which tobase their decisions on interventions through the most efficientuse of constrained resources.
In Spain, several authors have called for attention to theneed for well-conducted economic evaluations from which re-liable conclusions can be drawn and recommendations on the
Conflicts of interest: J.M. Rodriguez worked at Medtronic Iberica research organization. P. Gonzalez works at Medtronic Iberica, M
* Address correspondence to: Silvia Paz, Outcomes’10, Parque CienRiu Sec, Edificio Espaitec 1, 12071 Castellon, Spain.
E-mail: [email protected]/$36.00 – see front matter © 2011 Published by Elsevier I
convenience (or not) of adopting a health technology can bemade [4,5]. Although the number of publications on the eco-nomic evaluation of health technologies has increased over thepast decades in the country, cost-utility analyses have been lessfrequently conducted [6], accounting for 10% of economic eval-uation articles published between 1990 and 2000 [7]. Instated ofdetermining QALYs, most results were based on the assessment ofintermediate variables, making it difficult to compare different stud-ies on similar technologies or to analyze changes in trends over time[8]. A guideline for the economic evaluation of health technologiesproposed by the Spanish Ministry of Health has further recom-mended the use of cost-utility analysis when decision makers seek tomeasure the results of the intervention in terms of lengthening orimproving life expectancy adjusted by quality [9]. They have alsobeen suggested as the type of analysis to be chosen when compari-sons among different interventions across different disease are de-sired [10].
This study aimed to identify, summarize, and appraise eco-nomic evaluation of health technologies that included QALYsas an outcome measure conducted over the past 20 years inSpain.
he time of writing up the manuscript. S. Paz and L. Lizan work atd, Spain., Tecnológico y Emprasarial de la Universidad Jaume I, Campus del

459V A L U E I N H E A L T H 1 4 ( 2 0 1 1 ) 4 5 8 – 4 6 4
Methodology
Search strategy
The PubMed/MEDLINE electronic database was searched applyingthe following combinations of MeSH terms: first search: “Quality-Adjusted Life Years” AND “Spain”; second search: “Cost-BenefitAnalysis” AND “Spain”; third search: “Quality-Adjusted Life Years”AND “Biomedical Technology” AND “Spain”; fourth search: “Qual-ity-Adjusted Life Years” AND “Economics, Pharmaceutical” OR“Therapeutic Equivalency” AND “Spain”; fifth search: “Economics”AND “Spain” AND “Drug Therapy”; sixth search: “Quality-AdjustedLife Years” AND “Pharmaceutical Preparations” AND “Spain”; sev-enth search: “Cost-Benefit Analysis” AND “Pharmaceutical Prepa-rations” OR “Nonprescription Drugs” OR “Drugs, Investigational”OR “Drugs, Generic” OR “Drugs, Essential” AND “Spain.”
Because it was anticipated that many relevant articles wouldbe identified in journals not indexed, sources of gray literaturewere searched, including Google Scholar beta, and the System forInformation on Grey Literature in Europe (SIGLE) using a combina-tion of English and Spanish terms. The same terms in Spanishwere used to search the Web sites of the seven health technologyassessment (HTA) agencies in Spain.
Searches were restricted to the English and Spanish languagesand to articles published between January 1990 and December2009. The Revista Española de Economia de la Salud (2000–2009),Gaceta Sanitaria (2000–2009), and PharmacoEconomics Spanish Re-search Articles (2005–2009) as well as the reference lists of selectedarticles were hand-searched for relevant studies.
Inclusion and exclusion criteria
It was agreed that to be included in the final review (inclusioncriteria) articles should 1) refer to research studies conducted inSpain; 2) have been published in either national (Spanish) or inter-national journals or as HTA reports available on the Internet; 3)relate to the economic evaluation of health technologies, includ-ing medications and medical devices for preventive, diagnostic, ortherapeutic proposes; 4) include a cost-utility analysis expressedin QALYs: 5) refer to either the adult or pediatric populations; and6) be available in abstract and full text.
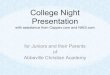
Fig. 1 – Article sele
Abstracts were rejected (exclusion criteria) if they 1) referred tomulticountry studies; 2) related to communication technologies asthey apply to health-care processes; 3) included life-years gained,disability-adjusted life-years, years of healthy life lost, deaths, ornew events avoided, estimates of the direct and indirect costs orany other final or intermediate result different from QALYs as theonly or combined outcome measures; 4) were review articles orletters to the editor; and 5) were not available in full text.
Reviewed variables
For the purpose of this review, health-care technology encom-passed all methods used by health professionals to promotehealth, prevent and treat disease, and improve rehabilitation andlong-term care [11]. These methods included pharmaceuticals, de-vices, procedures, programs, settings, and public health activities.Articles were assessed considering the year of publication; thedesign of studies, differentiating those based solely on modelsfrom the ones based on clinical studies; the perspective adopted;the type of costs estimated; the time frame taken into account; thesensitivity analysis, and the sources of funds reported by authors.Reviewed technologies were categorized according to their nature,including medical and surgical procedures, pharmaceuticals, de-vices, public health, and delivery of care programs. They wererelated to the disease condition and to the objective of the inter-vention for which they were evaluated, including preventive, di-agnostic, and therapeutic aims. It was also determined whetherthey applied to the adult or pediatric population. Special attentionwas given to establish the methods used to determine healthstates and preferences to estimate QALYs.
QALY assessment
The assessment of the QALYs estimates focused mostly on themethod applied to describe the health states, the technique usedto elicit preference weights, and whether the results could be ap-plied to the Spanish population. This final characteristic of studieswas addressed from two standpoints: first, assuming that thosestudies based on field-work data and well-established local data-bases would yield more representative and applicable information[12] and, second, contrasting the cost per QALY results. A data
ction process.

(continued on next page)
460 V A L U E I N H E A L T H 1 4 ( 2 0 1 1 ) 4 5 8 – 4 6 4
extraction sheet was specifically designed. Two researchers as-sessed the relevance and quality of the publications. Disagree-ments were resolved by consensus and, in the case of discrepan-cies, an external reviewer was consulted for final decision.
Results
The search terms and their combinations yielded 168 references. Atotal of 60 articles that met the inclusion criteria were finally re-trieved (Fig. 1). Six HTA reports on health technology evaluationsthat estimated QALYs were identified. Only 4 of them met theinclusion criteria defined for this review.
General characteristics of studies
The yearly number of publications progressively increased over thereviewed period (Table 1) in the same way as did the number ofeconomic evaluations published in international journals. HTA re-ports appeared from 2006 onward. Most assessments were con-ducted in the adult population (92%) and dealt mostly with cardio-vascular- (19.8%), respiratory- (16.3%), and cancer- (13.0%) relatedprocesses. The largest proportion referred to therapeutic interven-tions (77.1%) followed by those dealing with preventive strategies(21.4%). No studies of rehabilitation or palliative care interventionswere identified. More than half of the economic evaluations were car-riedoutonpharmaceuticalproducts (63.2%);only14.2%dealtwithmed-ical devices and 13.1% with preventive public health programs.
Specific characteristics of studies
The largest proportion of economic evaluations (80.3%) relied on atheoretical model to ascertain the impact of the intervention onthe disease process, including Markov, decision tree analyses, anddiscrete event simulations. Markov designs were the most fre-quently applied (71.4%), whereas discrete event simulations ap-peared in only two studies. Observational, open, and cohort de-signs had occasionally been reported (19.7%), although theyappeared since the earliest years reviewed.
The National Health System (NHS) perspective was the mostfrequently adopted (67.3%), the viewpoint of society was chosen inmuch fewer publications (4.9%) when the perspective of studieswas clearly stated. Almost one fourth of economic evaluations(24.6%) failed to state the study’s standpoint. Direct (medical) costswere the most frequently estimated in line with the viewpointmost commonly adopted. In 42.1% of publications, the time framewas the patient’s life span, whereas in approximately one fourth,it was shorter than 1 year. The vast majority of the studies (76.8%)discounted costs and effects.
Multivariable (56.4%) and probabilistic (39.2%) sensitivity analy-ses were the first and second most frequently conducted, respec-
Table 1 (continued)
Characteristics Number (%)of articles(N � 64)
Health state methods described to estimatequality-adjusted life-years
Yes 29 (45.1)No 35 (54.9)
Techniques used to elicit preferences describedYes 17 (27.4)No 47 (72.6)
* Including vaccination, genetic testing, and cancer screening
programs.
Table 1 – Study characteristics.
Characteristics Number (%)of articles(N � 64)
Year of publication1990–1994 01995–1999 3 (5.0)2000–2004 11 (17.0)2005–2009 50 (78.0)
Study designModeling (including Markov, decision tree,
and discrete event simulation models)51 (80.3)
Clinical studies 13 (19.7)Study perspective
National health system 43 (67.3)Social 3 (4.9)Both (national health system � social) 3 (3.2)Not performed/not stated 15 (24.6)
Type of costsDirect (medical) costs 54 (84.3)Indirect (social) costs 6 (9.3)Not performed/not stated 4 (6.2)
Time framePatients’ life span 27 (42.1)Longer than 1 year, but shorter than patients’
life span17 (26.4)
Shorter than 1 year 16 (25.0)Not performed/not stated 4 (6.5)
Sensitivity analysisProbabilistic 25 (39.2)Multivariate 36 (56.4)Univariate 2 (1.5)Not performed/not stated 1 (1.5)
Study populationAdult 59 (92.0)Pediatric 4 (6.5)Both (adult � pediatric) 1 (1.5)
Disease conditionDegenerative processes of the central nervous
system6 (9.9)
Cardiovascular processes 12 (19.8)Respiratory processes 10 (16.3)Infectious processes 7 (11.4)Skin, bone, and muscle disorders 7 (9.9)Endocrine, nutritional, and metabolic diseases 6 (9.9)Cancer 9 (13.0)Eyes and sight problems 3 (3.3)Addictions and psychiatric disorders 4 (6.5)
Type of interventionPreventive 14 (21.4)Diagnostic 2 (1.5)Therapeutic 48 (77.1)
Type of technologyMedical procedure 5 (6.5)Surgical procedure 2 (1.5)Pharmaceutical products 38 (63.2)Medical devices 10 (14.2)Public health programs* 8 (13.1)Delivery of care 1 (1.5)
Funding sourceStated 31 (48.7)
Private 23 (74.2)Public 6 (19.3)Mixed (private and public) 2 (6.4)
Not stated 33 (51.3)
tively, to confirm the robustness of the results. In relation to funding,

(ssOia
(sdtm
rvttrgneclPhgTa
iIt
461V A L U E I N H E A L T H 1 4 ( 2 0 1 1 ) 4 5 8 – 4 6 4
almost half of the studies (48.7%) reported the source of funds, and theinclusion of this information notably increased from 2005 onward.Studies privately funded constituted the largest proportion (74.2%).
QALYs estimates
Methods applied to describe health statesInformation on the methods used to describe the health states wasgiven in 45.1% of studies, but in a greater proportion (54.9%), thesedetails were not clearly stated. Twelve of the reviewed full-text arti-cles reported QALYs on actual before and after measurements usinga validated HRQoL instrument. In general, details on who completedthe questionnaire were scarce. In only 17.7% of studies, was it possi-ble to identify whether either patients (n � 10), proxies (n � 1), or bothn � 1) were directly interviewed. The most frequently reported in-trument was the EuroQoL-5D (40.3%) followed by the Rosser Indexcore (3.2%) and the Health Utility Index Mark 3 (HUI-Mark 3) (3.2%).ther reported tools included the TNO-AZL Preschool Children Qual-
ty of Life (TAP-QOL) questionnaire (1.6%), the Short Form-36 (1.6%),nd the Kurtz Expanded Disability Status (1.6%).
In most cases, authors referred either to the international38.7%) or the national (8.0%) literature to feed models’ healthtates details. The description of the sources consulted and theetails provided on methods were highly diverse when referenceo the literature was made. In almost half of the studies based on
odels (43.5%), details were either inconsistent or not given.
Techniques used to elicit preferencesIn approximately one third (27.4%) of the economic evaluationsreviewed, the technique used to elicit preferences was clearlystated. Time trade-off (n � 16) and standard gamble (n � 1) wereeported, mentioning their use in the original work in which utilityalues and tariffs were determined. Time trade-off was linked tohe EQ-5D and standard gamble to the TAP-QOL. No direct valua-ion methods were used in the reviewed evaluations. Five studieseferred to the Rosser Kind Matrix (n � 3) or the HUI-Mark 3 (n � 2) toather utility values. In more than one half of articles (66.1%), it wasot possible to identify the method applied, although authors gaveither a national (9.6%) or an international (54.8%) reference for thehosen values. In five of six studies that used national references, theocal work done by Badía X et al. [13,14] in Catalonia was mentioned.atients were asked to declare their preferences for determinedealth states in seven studies, whereas preferences from both theeneral public and the patients were measured in two evaluations.he EQ-5D was used in all of them. In 12.9% of publications, no detailst all were given on the techniques used.
Application of results to the Spanish populationA small proportion of studies gathered health states and utilitydata from field work (20.9%); information on the use of health-care resources and costs were largely based on local sources(82.7%) including patient charts, hospital records, recognizedWeb sites, face-to-face interviews, and references from theSpanish literature.
Table 2 shows the estimated cost per QALY for the vast major-ty of reviewed interventions in 2009 Euros. The Spanish Nationalnstitute of Statistics’ tool for updating currency values was usedo update costs [15]. According to Table 2, the vast majority (77.1%)
of the interventions considered fell below a €30,000/QALY thresh-old [16]. More than half of them (65.9%) corresponded to pharma-ceutical products followed by medical devices (16.3%) used to treatcardiac arrhythmias, revascularization of arteries, bladder dys-function, and respiratory conditions. Preventive programs that in-cluded influenza vaccination of people aged 50 to 64 years, geneticscreening for colorectal and breast cancer and for asthma in chil-
dren were in third place (9.0%). Only thrombolytic therapy forstroke was found to be cost saving to the system as shown by thenegative value of the cost/QALY ratio (Table 2) [17].
The least cost-effective interventions in the league table (inter-ventions located beyond a €50,000 threshold) included treatmentof cancer, dementia, epilepsy, and Alzheimer’s disease and theprevention of infections of platelet transfusion devices.
All reviewed publications have been described (Appendix 1 foundat doi:10.1016/j.val.2010.10.039). Although infrequent among the ear-liest reports, the latest studies (22.5%) tended to include a willing-ness-to-pay curve to contrast the results of the economic evaluationreported against an arbitrary efficiency threshold that varied from€6,000 to €50,000. Some reports (18.9%) included recommenda-tions on the adoption of the technology mostly based on the long-term impact of the intervention on costs and savings for thehealth-care system and addressed the issue on, for example, theway in which changes in rates of implementation of the interven-tion being assessed may affect the health-care budget over definedperiods of time [18].
Discussion
A detailed examination of the methods used to assess QALYs wasthe main propose of this review, which, as a consequence, wasquite limited in scope. It has, however, revealed that although thetotal number of studies identified is low compared with other re-views on QALYs [19], the number of articles published substan-tially increased throughout the reviewed period, demonstrating agrowing interest and an increasing expertise on cost-utility anal-yses in the country. Alongside the increasing number of publica-tions, there has been an increase in the proportion of articles thatappeared in international journals over the years. This finding prob-ably reflects an improved methodological quality of analyses, whichmay have progressively benefited their publication [20]. Most studieshave been conducted on pharmaceutical products, whereas muchless consideration has been given to, for example, diagnostic andrehabilitation procedures, preventive programs, and medical devices[21]. This trend could be partially explained by the key role that thepharmaceutical industry plays in sponsoring studies. Funding dis-closure is still lacking, although it should improve as soon as all jour-nals require conflict of interest disclosure. Despite the search beingcomprehensive, there exists the possibility of having left out some ofthe earliest publications. Their inclusion, however, would have un-likely altered the findings reported here.
In general, most authors failed at thoroughly reporting on thenature of the sources consulted to determine the health states andutility values used to feed the models. As a consequence, a wide-spread variation on the methods used to calculate QALYsemerged. Similar findings have been reported in a review of pub-lished cost-utility studies in pediatric health care [22]. Althoughstandard recommendations on the estimate of QALYs have beenmade available worldwide [23,24], a methodologically uncertainarea still remains for researchers to calculate them in a rigorousway [25]. The EQ-5D was the instrument most frequently used toelicit health states and to derive utility values because it is the onethat experts recommend, mostly based on its economic theoryfoundation [26,27]. It also constitutes a tool that has been validatedin Spanish, making possible the availability of a simple, compara-ble, and easy-to-use alternative [13,14].
Very few economic evaluations relied on field work–generateddata and were part of a clinical study, whereas the vast majoritywas based on modeling the disease process. Regardless of somelimitations, models constitute an acceptable and scientificallyvalid practice, particularly if the high costs of clinical studies aretaken into account [28]. As a consequence of the scarce local in-formation available, health state descriptions and utility valueswere derived from the international literature. It has been re-
ported that score values are population specific and vary accord-
462 V A L U E I N H E A L T H 1 4 ( 2 0 1 1 ) 4 5 8 – 4 6 4
Table 2 – League table*.
Therapy Cost/QALY(€, 2009)
Stroke treatment with thrombolytic therapy (women, societal costs) �20,026.25Stroke treatment with thrombolytic therapy (men, societal costs) �18,641.25Treatment of relapsing-remitting multiple sclerosis with Copaxone (glatiramer acetate) 77.25Coronary heart disease prevention with fluvastatin 80 mg/day 109.39Treatment of burn patients in a specialized center 750.48Screening and treatment of type 1 diabetes retinopathy with nonmydriatic camera 1847.88Treatment of ventilator-associated pneumonia with linezolid (all types) 2111.86Colorectal cancer screening (annual, fecal occult blood immunological test) 2154.03Usual type 2 diabetes mellitus treatment completed with acarbose 2495.86Improvement of glucose control and prevention of diabetic complications with insulin glargine: type 1
diabetes mellitus2812.68
5-Year treatment of early breast cancer with combined therapy with docetaxel 2878.31Screening and treatment of type 2 diabetes retinopathy with nonmydriatic camera 2986.34Bradycardia treatment with dual- vs. single-chamber pacemakers 4023.73Age-related macular lesions treatment with pegaptanib sodium 4058.745-Year treatment of chronic obstructive pulmonary disease with tiotropium and salmeterol 4505.09Influenza vaccination for adults aged 50–64 years (societal perspective) 4709.12Treatment of chronic hepatitis C of naïve patients with peginterferon alfa-2b plus ribavirin 4798.31Prevention of respiratory syncytial virus infection in premature infants with palivizumab (societal perspective) 5037.87Prevention of cardiovascular events in patients non–ST-segment elevation acute coronary syndrome with
clopidogrel for a high-risk 40-year-old patient6010.00
Mechanical ventilation for critically ill patients 6673.50Type 6,11,16,18 human papillomavirus vaccination 6921.54Sleep apnea treatment with nasal continuous positive airway pressure 7036.32Surgical ablation to treat atrial fibrillation in patients with concomitant valve disease 7302.198-Month aquatic treatment program for women with fibromyalgia 8618.53Primary prevention of cardiovascular disease in type 2 diabetes mellitus patients with atorvastatin 10 mg 9132.21Maintenance treatment with rituximab of resistant or recurrent follicular lymphoma 9975.635-Year treatment of moderate to severe sleep apnea with nasal continuous positive airway pressure 10,093.52Treatment of type 2 diabetes mellitus patients with rosiglitazone in combination with metformin (overweight
vs. metformin � bedtime insulin)10,675.81
Coronary artery revascularization with drug-eluting stent at 5 years 10,736.11Improvement of glucose control and prevention of diabetic complications with insulin glargine: type 2
diabetes mellitus11,110.09
Genetic screening for asthma in at-risk children 11,832.60Total hip replacement in osteoarthritis patients 11,833.21Treatment of type 2 diabetes mellitus patients with rosiglitazone in combination with metformin (obese vs.
metformin � bedtime insulin)12,682.49
Total knee replacement in osteoarthritis patients 14,472.27Febrile neutropenia prevention in chemotherapy breast cancer patients with an 11-day cycle of pegfilgrastim 14,852.58Prevention of respiratory syncytial virus infection in premature infants with palivizumab (NHS perspective) 15,150.81Triple antiplatelet therapy in non–ST-elevation acute coronary syndrome 16,149.90Fecal incontinence therapeutic management with InterStim (intact anal sphincter patients) 17,248.95Treatment of type 2 diabetes mellitus patients with rosiglitazone in combination with metformin (overweight
vs. metformin � sulfonylureas)18,629.89
Prevention of respiratory syncytial virus infection in chronic lung disease children with palivizumab 19,276.2824-Month treatment of mild Alzheimer’s disease with donepezil (NHS perspective) 20,353.00Breast cancer screening (50- to 69-year age group) 21,757.68Neuropathic pain control with pregabalin 22,266.18Fecal incontinence therapeutic management with InterStim (in structurally deficient anal sphincter patients) 23,659.87Treatment of children with attention-deficit/hyperactivity disorder with atomoxetine 23,836.11Partial refractory epilepsy treatment with pregabaline 26,125.81Repair of abdominal aneurysms of the aortic artery with an endovascular prosthesis (at 4 years) 27,672.6910-Year smoking treatment with varenicline 27,999.56Treatment of non–ST-elevation acute coronary syndrome with fondaparinux 29,848.005-Year treatment of HIV type 1 patients with raltegravir 32,122.4820 Years of adjuvant therapy with aromatase inhibitors in breast cancer exemestane scheme 32,743.62Prevention of fractures in osteoporosis treatment with protelos 32,953.11Improvement of glucose control and prevention of diabetic complications with insulin pumps 33,989.84Pediatric attention-deficit/hyperactivity disorder treatment with atomoxetine 35,062.78Prevention of cardiovascular events in non–ST-segment elevation acute coronary syndrome with clopidogrel
in a low-risk 80-year-old patient36,060.00
(continued on next page)

te
osodvtb
atnattm
acheou
: htt
463V A L U E I N H E A L T H 1 4 ( 2 0 1 1 ) 4 5 8 – 4 6 4
ing to the region or country [29,30] or to the sociodemographiccharacteristics of the respondents [31,32]. For instance, a studyconducted to compare Spanish and United Kingdom time trade-off values for the EQ-5D health states found statistically significantdifferences in values for more than one third of the 43 healthstates rated directly by participants [33]. Preference reversals be-tween countries were also found. For this reason, results derivedfrom economic models enhanced with health state and prefer-ences weight data of diverse nature may not entirely apply to theSpanish population [34]. Conclusions derived from them shouldherefore be made cautiously, although it is unknown how differ-nces between populations affect cost-utility analyses [33]. This
concern may be of particular interest in Spain due to the sociode-mographic, cultural, and epidemiological differences that existamong autonomous communities [35]. The way in which the re-gionalization and decentralization of the health-care system mayaffect the extrapolation of local cost-utility analyses results to theentire population may deserve further analysis.
Cost-utility ratios are used to prioritize different interventionsfor diverse diseases when the final objective is to make the most ofhealth-care spending in terms of the outcomes achieved [9]. Un-certainty emerges when a definition of an affordable threshold forhealth-care investment is needed [23]. In this review, few publica-tions were found that made clear recommendations on the adop-tion of the intervention being evaluated, and suggested thresholdsvaried greatly from €6,000 to €50,000 on average. A cost per QALY
f €30,000 is the threshold commonly accepted to be affordable byociety and the health-care system, although without official rec-gnition in Spain [16]. It has been pointed out that an importantisadvantage for making recommendations on thresholds for in-esting in health-care interventions based on literature reviews ishe disparity, uncertainty, and arbitrariness of the criteria appliedy authors with which to draw conclusions [36].
Moreover, thresholds may vary in certain circumstances, suchs in the case of serious conditions with high morbidity and mor-ality rates or with low prevalence for which few treatment alter-atives exist or for treatments that are considered as rescue ther-pies or the last treatment options [37]. That is the case ofreatments for rare conditions, antiretroviral therapies, pediatricreatments, and oncology therapies for which higher thresholds
Table 2 (continued)
Therapy
Treatment of hypertension (30-year-old men)Treatment of advanced Parkinson’s disease with bilateral subthalamNeovascular age-related macular degeneration treatment with ranib5-Year treatment of chronic obstructive pulmonary disease with salmPostmenopausal osteoporosis treatment with teriparatideTreatment of hypertension (30-year-old women)Second-line treatment of gastrointestinal stromal tumors with sunitAdjuvant therapy with aromatase inhibitors in breast cancer exemes24-Month treatment of moderate Alzheimer’s disease with donepeziPartial refractory epilepsy treatment with levetiracetamBreast cancer screening (70- to 75-year age group)Breast cancer screening (40- to 49-year age group)Prevention of pathogen infection of platelet transfusion preparations
donor platelets � INTERCEPT Blood System vs. random donor plateTreatment of typical relapsing-remitting multiple sclerosis patients wPrevention of pathogen infection of platelet transfusion preparations
donor platelets � INTERCEPT Blood System vs. single donor platele
NHS, National Health System; QALY, quality-adjusted life-year.* This table contains most interventions reviewed. The Spanish Nat
estimate the costs of the interventions in 2009 Euros (available from
ay be acceptable. In a similar sense, a different threshold may be
llowed for the implementation of health technologies that be-ome cost-effective due to the savings that they represent to theealth-care system. All these matters are to be taken into consid-ration when it comes to making social decisions on the allocationf health-care resources [38]. Cost-utility analysis appears to be aseful and practical tool for informing decision makers.
Acknowledgments
The authors appreciate the very helpful and enriching commentsthat the reviewers made to drafts of this article. Their suggestionscontributed greatly to improving the quality of this publication.
Source of financial support: This project was sponsored byMedtronic Iberica, Madrid, Spain.
Supplemental Materials
Supplemental material accompanying this article can be found inthe online version as a hyperlink at doi:10.1016/j.val.2010.10.039,or if hard copy of article, at www.valueinhealthjournal.com/issues(select volume, issue, and article).
R E F E R E N C E S
[1] American College of Physicians. Information on cost-effectiveness: anessential product of a national comparative effectiveness program.Ann Intern Med 2008;148:956–61.
[2] Drummond MF, Sculpher MJ, Torrance GW, et al. Methods for theEconomic Evaluation of Health Care Programmes (3rd ed.). Oxford:Oxford University Press, 2005.
[3] Weinstein MC, Stason WB. Foundations of cost-effectiveness analysisfor health and medical practices. N Engl J Med 1977;296:716–21.
[4] Ortu=n-Rubio V, Pinto Prades JL, Puig-Junoy J. Establishing priorities.Aten Primaria 2001;27:673–6.
[5] Sacristan JA, Rovira J, Ortu=n V García-Alonso F, et al. Utilization ofeconomic assessments of health interventions. Med Clin (Barc) 2004;122:789–95.
Cost/QALY(€, 2009)
36,135.61mulation 37,621.57ab (life span time frame) 40,264.76ol and ipratropium 42,590.52
43,172.5244,318.5450,169.98
scheme 57,665.95S perspective) 71,037.00
104,918.98175,586.55175,971.59
INTERCEPT Blood System: random 452,620.78
zathioprine 483,623.00INTERCEPT Blood System: single 1,267,221.12
Institute of Statistics’ tool for updating currency values was used to
p://www.ine.es/calcula/index.do?L�0).
ic stiizum
eter
inibtanel (NH
withletsith awithts
ional
[6] Garcia-Altés A. Twenty years of health care economic analysis inSpain: are we doing well? Health Econ 2001;10:715–29.

[
[
[
[
[
464 V A L U E I N H E A L T H 1 4 ( 2 0 1 1 ) 4 5 8 – 4 6 4
[7] Oliva J, del Llano J, Sacristán JA. Analysis of economic evaluations ofhealth technologies performed in Spain between 1990 and 2000. GacSanit 2002;16:2–11.
[8] Oliva J, del Llano JE, Sacristán JA. La Evaluación Económica deTecnologías Sanitarias en España: Situación Actual y Utilidad comoGuía en la Asignación de Recursos Sanitarios. Economía de la Salud2003;894:155–67.
[9] Lopez Bastida J, Oliva J, Antoñanzas F, et al. A proposed guideline foreconomic evaluation of health technologies. Gac Sanit 2010;24:154–70.
[10] Rovira-Forns J, Antoñanazas-Villar F. Economic evaluation studies inhealth. Med Clin (Barc) 2005;125:61–71.
11] Office of Technology Assessment. Assessing the efficacy and safety ofmedical technologies. Washington, DC: U.S. Government PrintingOffice, 1978.
12] Nord E, Daniels N, Kamlet M. QALYs: some challenges. Value Health2009;12(Suppl. 1):S10–15.
13] Badia X, Roset M, Montserrat S, Herdman M, Segura A. The Spanishversion of EuroQol: a description and its applications. EuropeanQuality of Life scale. Med Clin (Barc) 1999;112(Suppl. 1):79–86.
14] Badia X, Montserrat S, Roset M, Herdman M. Feasibility, validity andtest-retest reliability of scaling methods for health states: the visualanalogue scale and the time trade-off. Qual Life Res 1999;8:303–10.
15] INEbaseIIndice de Precios de consumo (Base 2006). Actualización derentas con el IPC general (sistema IPC base 2006) para periodosanuales completos. Available from: http://www.ine.es/calcula/index.do?L�0. [Accessed May 13, 2010].
[16] Sacristán JA, Oliva J, del Llano J, et al. What is an efficient healthtechnology in Spain? Gac Sanit 2002;16:334–43.
[17] Mar J, Begiristain JM, Arrazola A. Cost-effectiveness analysis ofthrombolytic treatment for stroke. Cerebrovasc Dis 2005;20:193–200.
[18] Moreu J, Cequier A, Brosa M, et al. Economic evaluation and budgetimpact analysis of the Endeavor drug-eluting stent in Spain. Gac Sanit2009;23:540–7.
[19] Räsänen P, Roine E, Sintonen H, et al. Use of quality-adjusted life yearsfor the estimation of effectiveness of health care: a systematic review.Int J Technol Assess Health Care 2006;22:235–41.
[20] Neumann PJ, Stone PW, Chapman RH, et al. The quality of reporting inpublished cost-utility analyses 1976-1997. Ann Intern Med 2000;132:964–72.
[21] Esperato A, García Altés A. Health promotion: a profitable investment?Economic efficiency of preventive interventions in Spain. Gac Sanit2007;21:150–61.
[22] Griebsch I, Coast J, Brown J. Quality-adjusted life-years lack quality inpediatric care: a critical review of published cost-utility studies inchild health. Pediatrics 2005;115:601–8.
[23] Claxton K, Schulper M, Drummond M. A rational framework for
decision making by the National Institute for Clinical Excellence(NICE). Lancet 2002;360:711–5.[24] Weinstein MC, Torrance G, McGuire A. QALYs: the basics. ValueHealth 2009;12(Suppl. 1):S5–9.
[25] Towse A, Pritchard C. National Institute for Clinical Excellence (NICE):is economic appraisal working? Pharmacoeconomics 2002;20(Suppl.3):95–105.
[26] Dolan P. Modeling valuations for EuroQoL health states. Med Care1997;35:1095–108.
[27] Dolan P, Roberts J. Modeling valuations for Eq-5d health states: analternative model using differences in valuations. Med Care 2002;40:442–6.
[28] Weinstein MC, Toy EL, Sandberg EA, et al. Modeling for health careand other policy decisions. Uses, roles and validity. Value Health 2001;4:348–61.
[29] Dolan P, Kahneman D. Interpretations of utility and their implicationsfor the valuation of health. Economic J 2008;118:215–34.
[30] Kind P, Dolan P, Gudex C, Williams A. Variations in population healthstatus: results from a United Kingdom national questionnaire survey.BMJ 1998;316:736–41.
[31] Schlander M, Schwarz O. The Norbaden Project for health careutilization research in Germany: database characteristics and firstapplication. Value Health 2005;8:199.
[32] Prieto L, Sacristan JA What is the value of social values? Theuselessness of assessing health-related quality of life throughpreference measures. BMC Med Res Methodol 2004;4:10.
[33] Badia X, Roset M, Herdman M, Kind P. A comparison of UnitedKingdom and Spanish general population time trade-off values for EQ-5D health states. Med Decis Making 2001;21:7–16.
[34] Puig Junoy J, López-Valcárcel BG. Economic evaluations of massiveHPV vaccination: within-study and between study variations inincremental cost per QALY gained. Prev Med 2009;48:444 – 8.
[35] Puig Junoy J, Pinilla J. Why are some Spanish regions so much moreefficient than others? Environ Plan C Government Policy,2008;26:1129–42. Available from: http://www.econ.upf.edu/�puig/publicacions/Any2008/GovPlanC08.pdf. [Accessed May 13, 2010].
[36] De Cock E, Miravitlles M, Gonzalez J, Azanza P. Valor umbral del costepor año de vida ganado para recomendar la adopción de tecnologíassanitarias en España: evidencias procedentes de una revisión de laliteratura. Pharmacoeconomics Spanish Research Articles 2007;4:97–107.
[37] McCabe C, Claxton K, Culyer JA. The NICE cost-effective threshold.What it is and what that means. Pharmacoeconomics 2008;26:733–44.
[38] Garrison LP. Editorial: on the benefits of modeling using QALYs for
societal resource allocation: the model is the message. Value Health2009;12(Suppl. 1):S36–7.