Embed Size (px)
Citation preview

242
THE TREATMENT OF PERFORATEDPEPTIC ULCER
By F. AUSTIN HENLEY, M.B., B.S., F.R.C.S.Consultant Surgeon to the Central Middlesex Hospital
No greater catastrophe can happen to a patientwith a peptic ulcer than perforation.The two most important factors are the mor-
tality and the morbidity which result from treat-ment. The concern of every surgeon is to electthe correct treatment for each individual case.
MortalityIt is agrced by all authorities that the decline
in the mortality is due to the introduction of theantibiotics, the restoration of fluid and electrolytebalance, and the availability of good anaesthesia.Avery Jones et al. (1950) showed a diminishingdeath rate frcm 12 in 39 cases in 1938, to i in 54in 1948. Each intervening year revealed a steadyimprovement. The overall mortality was 96deaths in 490 cases (I9.6 per cent.) with 41 deathsin 117 perforated gastric ulcers (35 per cent.).Forty (1946) quotes a mortality figure of 42 percent. for perforated gastric ulcers, whilst thatquoted by other authors range from 5.6 per cent.for short series of cases to 25 per cent. in thebigger series. At the Utrecht University Hos-pital the mortality before 1920 was 43 per cent.,between 1920 and I930 it was 28 per cent., andfrom 1930 to 1934 it was 22 per cent. Chamber-lain (1951) gave a mortality of I7.94 per cent.following simple suture in 1,622 perforations,covering the years 1930 to I949. The otherfactors influencing the mortality are well recog-nized; for example, the time interval between theonset of the perforation and the commencementof treatment, the age of the patient, the enthusiasticand adequate post-operative treatment of the chest,and the seniority of the surgeon and anaesthetist.In one series (Gilmore, 1953) 80 per cent. of thepatients were operated upon in less than 12 hoursafter perforation with a mortality of 3 per cent.With a delay of 12-24 hours the mortality rose toI8 per cent., and over 24 hours it became 40 percent. Such figures are in accordance with thegenerally accepted fact that delay in surgery leadsto an increased mortality.With regard to age of the patient the mortality
below 40 years of age is i per cent. or less in the
best hands, but over the age of 60 figures up to20 per cent. are not uncommon. An interestingobservation was made by Gilmore (1953) that in119 patients with perforated acute ulcers therewere no deaths, but in 87 perforated chroniculcers 13 patients died, a mortality of 15 per cent.As all these patients were treated by simple sutureof the perforated ulcer the cause of death must bedue to one of the following factors: (i) Chronicill-health before perforation due to malnutrition;(2) pyloric stenosis with vomiting and consequentfluid and electrolyte imbalance; (3) continuedpyloric stenosis following suture; (4) chronic pul-monary disease exacerbated by the absorption ofpurulent material from the abdomen; (5) bleedingconsequent upon suture at the ulcer site; (6)failure to secure obliteration of the perforationbecause of immobility of the area; and (7) bleedingfrom another unrecognized ulcer.There is, therefore, still a threatening mortality
following simple suture in the treatment of aperforated peptic ulcer, and the perforated gastriculcer appears to be consistently more lethal thanthe perforated duodenal ulcer.
MorbidityIllingworth (1946) wrote that the longer the
history of peptic ulcer before perforation and thesooner the recurrence of post-operative symptomsthe worse was the prognosis.
In Forty's (1946) series 25 per cent. had recur-rence of symptoms in the first year and 38 percent. recurred over the first five years. Inaccordance with Illingworth's dictum I7 per cent.recurred in those with a three-year history or less,25.7 per cent. in those with a three to five-yearhistory, 32 per cent. in those with a five to ten-year history, and 40 per cent. in patients with aten-year or more pre-operative history.
Lassen (1952) found that 38 per cent. of hispatients developed severe ulcer symptoms post-operatively and that only 20 per cent. remainedsymptom-free. Eight other Scandinavian authorsquoted by Lassen maintained that 42. per cent.developed severe symptoms of recurrent ulcer
copyright. on 30 A
pril 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.31.355.242 on 1 M
ay 1955. Dow
nloaded from

HENLEY: The Treatment of Perforated Peptic Ulcer
post-operatively and another 28 per cent. hadsymptoms of a moderate degree. In Turner's(195I) review of 143 patients, I22 experiencedpeptic ulcer symptoms post-operatively followingsimple suture, i.e. 85.4 per cent. These symp-toms were severe in 77.5 per cent., of which38.5 per cent. underwent further surgery. InChamberlain's (1951) follow-up of 1,622 patients,of which only 56 per cent. were traced, 4 per cent.had recurrent perforation, 14 per cent. underwentfurther surgery, 33 per cent. had symptomssufficient to seek medical advice and treatment,and 2 per cent. died of their ulcer. In all, 53 percent. were unrelieved of their peptic ulcer symp-toms following simple suture of the perforation.
In a study of the late results following per-forated gastric and duodenal ulcers Doll (I950)found that after two years 63 per cent. of theperforated gastric ulcer were unsatisfactory. Somepatients had died from their ulcer, some developedcarcinoma of the stomach, some were readmittedto hospital for further surgical or medical treat-ment, and others had recurrence of ulcer pain anddyspepsia. Of the duodenal ulcers 53 per cent.were similarly affected. He further stated thatbetween two and twelve years following simplesuture of a perforation the gastric ulcer figurebecame 67 per cent. and that of the duodenal ulcer60 per cent. In one series he traced 68 patientswho had had perforated gastric ulcers, and ofthese 8 (12 per cent.) had developed carcinomaof the stomach.
It therefore appears from the literature thatonly one out of every five patients treated bysimple suture of a perforation remains symptom-free, and that two out of every five are sufficientlytroubled by the disease to necessitate further treat-ment. The possibility of carcinoma of thestomach should be taken into consideration in thetreatment of a perforated gastric ulcer.
TreatmentThe treatment of the perforated peptic ulcer is
surgery.
Non-operative TreatmentWhere for medical reasons surgery is prohibited
or the patient refuses an operation, conservativetreatment should be instituted. The liability ofconservative measures under any other circum-stances places a grave responsibility on the medicalattendants both to accuracy of diagnosis andprognosis. Wangenstein (I935) first advocatedcontinuous intragastric decompression for localizedduodenal perforation. Its use, however, has beenrecorded with varying mortality: 47.5 per cent.mortality in 67 patients by Olsen and Norgore(I946), 21.3 per cent. by the late Hedley Visick
in I4 cases (I946), and in the same year Taylorlost 14 per cent. of 28 patients. An averagefigure of 8 per cent. is given for 138 cases (Ivy,Grossman and Bachrach). Are the results ob-tained in other clinics too prohibitive to record ?The procedure in the non-operative treatment
is gastric decompression by continuous suctionthrough a Ryle's tube, with the administration ofparenteral fluid and electrolytes and an accuratefluid balance record. Antibiotic therapy shouldbe started at the same time whilst pain and gastro-intestinal spasm are relieved by morphia and otheranalgesics and antispasmodics. In the perfora-tion of an acute ulcer spasm might assist thesealing off of the ulcer, but with adequate intra-gastric decompression the relief of pain and thecomfort of the patient are of paramount import-ance. These measures are maintained for seventytwo hours when feeding by mouth is commencedalong the same lines as in post-operative gastricsurgery. Subsequent treatment will depend uponthe clinical improvement or otherwise in thepatient's condition.
Operative TreatmentSurgical treatment has passed through several
very definite stages in keeping with the advance-ment in anaesthesia.
Simple closure of a perforation was the originalsurgical method of choice and is still the mostuniversally used procedure. This was followedby suture and gastro-jejunostomy. Stomal ulcera-tion followed rapidly in its wake, and this com-plication dreaded by both patient and surgeon alike,and described by Sir Gordon Gordon-Taylor asthe worst malady ever invented by the surgeon,led the operation into disrepute, and in Englandfor all practical purposes it is abandoned. Excisionof the ulcer with suture of the perforation has itsadvocates, but the end-result is similar to that ofsimple suture.
Keetley of London in I902 did the first partialgastrectomy for a perforated ulcer. It had beenadvocated by several continental surgeons before1930, including Von Haberer (I919), Duval,Schmieden and in 1933 by Noordenbos. Morerecently Lowden (1952) reported 51 cases ofperforated peptic ulcer treated by primary partialgastrectomy without mortality. Mention mustbe made of Youdine of Moscow (i939), whoreported I,400 cases.The arguments against primary partial gastrec-
tomy as the operation of choice are:i. The ulcer may be acute with little or no
history, and therefore medical treatment has notbeen given a trial. Nuboer (i951) stated that anacute ulcer never perforates and that all the ulcersremoved by him were subjected to histological
c
IAay 1955 243
copyright. on 30 A
pril 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.31.355.242 on 1 M
ay 1955. Dow
nloaded from

244 POSTGRADUATE MEDICAL JOURNAL May 1955
"":.f?̂*:;~:C! }] | ws
I:--
5s
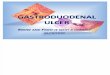
FIG. I.-Illustrates a small duodenal ulcer perforation in a girl aged 17. Althoughthere was no history of indigestion or medical treatment, this illustratesGilmore's point that a chronic ulcer is not always attended by symptoms.
examination and shown to be chronic with con-siderable changes in the submucosa and deeperlayers. Emmett also stated that the absence ofprolonged ulcer symptoms in certain perforatedulcer patients is no indication of a benign lesion.
2. Thirty per cent. of patients are free fromsymptoms following simple suture. Therefore,primary gastrectomy is unnecessary in 30 out ofevery o00 patients. In the other 70 per cent.radical operation is indicated and one operation tocure one disease is better than the risk of twoanaesthetics, two operations and the economicalloss by the patient, his medical attendants and theState through bed-occupancy.
3. In these days of adverse criticisms of thedoctor-patient relationship, the patient after suturefor his perforation is most grateful, but when helearns he may have to undergo a second operationthe news is a shock to his morale. When re-admitted to the ward for gastrectomy he is acomparatively fit man and the morning afteroperation is acutely aware of his many discomforts.Further, his chances of developing an incisionalhernia are doubled.
4. It may be stated that one should treat theperitonitis and the perforation and not the ulcer.Is it not more profitable to treat the cause of theulcer and thereby the cause of the peritonitis andby so doing prevent the need for further surgery ?The mortality from primary gastrectomy is less
than for simple suture, provided a good surgicalteam is at hand. Bisgard 2.7 per cent. (I in 36),Lowden no mortality in 51 cases, Henley nomortality in I2 cases, DeBakey less than 2 percent. (i in 55), and Mathewson no mortality in5 cases. A perforated ulcer following simple suturemay bleed, inwhich case the mortality is 50 per cent.Partial gastrectomy will prevent this complication.
5. In the presence of a soiled peritoneum apartial gastrectomy does seem a major under-taking, but the operation is no more difficult tech-nically, and if the peritonitis is going to producea chest complication post-operatively, as it is soprone to do, the choice of operative procedurewill have little effect. A routine gastrectomy inthe presence of adhesions around the duodenum,and perhaps undertaken as an emergency forpyloric stenosis, is more liable to damage thecommon bile duct than one in which oedema hasseparated the tissues, with an anterior ulcer.
6. There may be more than one ulcer presentand the writer recalls an instance where the duo-denal perforation was oversewn in an elderlypatient, to be followed ten days later by a massiveintestinal haemorrhage from which the patientdied within four minutes. Autopsy revealed agastric ulcer four inches in diameter penetrating thepancreas just on the proximal side of the pylorus.Partial gastrectomy may have saved this patient.
7. The final argument is what to do with the
copyright. on 30 A
pril 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.31.355.242 on 1 M
ay 1955. Dow
nloaded from

May 1955 HENLEY: The Treatment of Perforated Peptic Ulcer 245
i:8·P
.r·.·.·
'P;·::··-·rr
·:*·*·
-i*: .
.· .r .c.
··· ·:.:·:·RI..·.rsslp··raa..i::::.::::,·rr.
;·: ··*.
:::'B
': ·· :::·:: ·sa::
" .·· ·r..·:·
r·u ·:1 8··':''
..::··,·· : .·ii:. .Uk.Y%M.ii.: g.I'::.PP .
::':'';':
P- ; hljl 'x9 i- -":.d··: ·.
.:.·i·· ::,·i···
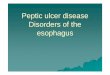
FIG. 2.-This illustration demonstrates the craggyirregularity of a perforated gastric ulcer in a managed 59.
patient under the age of 20 who presents with aperforation. If it could be ascertained that thiswas merely a single incident in the life of thepatient, simple suture would be adequate, but ifon the other hand this patient is doomed to leada life of frequent medical and hospital attendances,to swallow large quantities of alkalis and othermedicines, and maybe to receive surgery in lateryears, then partial gastrectomy would undoubtedlybe the correct treatment of the initial lesion(Fig. i).
Between August 1951 and August 1954, seventyfive perforated peptic ulcers were admitted to my-unit. Twenty-two underwent primary partial gas-trectomy, fourteen hadjejunal replacement with onedeath (from a pelvic abscess), and the remainingeight had a Billroth I operation with one death.Thirty-six underwent simple suture of the per-foration with two deaths: one was moribund on ad-
mission and the other died of a profuse haemorrhagefrom a very large gastric ulcer which had not beenrecognized when the duodenal ulcer was oversewn.Sixteen other patients had excision of the ulcerwith suture without mortality. Only one of thetotal number of perforations proved to be acarcinoma of the stomach.
SummaryIt would appear from this survey that
primary partial gastrectomy is becoming a recog-nized and rational procedure in the treatment ofthe perforated peptic ulcer.
Simple suture is adequate for patients under theage of 20 where medical treatment has received notrial, and where the history of peptic ulcer is lessthan six months.The procedure for a perforated gastric ulcer
over the age of 45 years is always a partial gastrec-
copyright. on 30 A
pril 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.31.355.242 on 1 M
ay 1955. Dow
nloaded from

246 POSTGRADUATE MEDICAL JOURNAL Mzayv 955
tomy. Where the histology of a gastric ulcer isin doubt a frozen section biopsy should be takenbefore proceeding to definitive surgery (Fig. 2).
It is my pleasure to thank Dr. F. Avery Jonesfor access to his records, Dr. Richard Doll forpersonal communications, and Mr. A. G. Bookerfor the illustrations.
BIBLIOGRAPHYARMITAGE, G. (1953), Brit. nted. J., March I4.AVERY JONES, F., et al. (1950), Ibid., January 28.AUCHINCLOSS, H. (1952), Ann. Surg., 135, No. I.DOLL, R. (I950), Brit. med. J., January 28.EMMETT, J. M., et al. (1953), Ann. Surg., 138, 320.FORGE, CLIFTON (I953), Ibid., 138, No. 3.FORTY, FRANK (1946), Brit. med. J., May 25, p. 790.
GLEN, F., et al.GRAHAM, R. R. (1946), 72, 802.HENLEY, F. A. (1952), Brit. J. Sulrg., 40, No. I60.HENLEY, F. A., (I953), Ann. R.C.S., 13, No. 3.HESLOP, T. S. (I952), Brit. J. Surg., 40, No. 159.ILLINGWORTH, C. F. N., et al. (i946), B.M.H., 1, 787.IVY, GROSMAN and BACHRACH (1950), 'Peptic Ulcer.'LASSEN, H. KRIEGER (1952), A.M.A. Arch. Surg., 65, No. 5.LOWDON, A. G. R. (1952), Lancet, I22o.MOORE, H. G., and HARKINS, H. (1952), 'The Billroth I.
Gastric Resection.'NUBOER, J. F. (195I), Lancet, 952.OLSON, H. B., and NORGORE, M. (1946), Ann. Surg., 124, 479REA, C. E. (1952), Surg. St. Louis, 32, No. 4.SPALOIZ, J. E. (1946), Lancet, i, 643.TURNER, F. P. (I95I), Surg. Gynae. Obst., 92, 281.WALLENSTEN, S. (1952), Acta Chir. Scand., 104, Fase I.WANGENSTREN, O. H. (1935), Minnesota Med., 18, 477.WRIGHT, I,. T., and SCOTT, B. E. (1950), Jour. Pedia., 37, No. 6.VISICK, A. HEDLEY (I946), Brit. med. J., p. 941.
LARGE BOWEL OBSTRUCTIONBy GUY BLACKBURN, M.Chir., F.R.C.S.
Surgeon, Guy's Hospital
The clinical picture of large gut obstruction iseasily recognized in its classical and advancedform. Improvement in the results of treating itwill come mainly from earlier diagnosis andacceptance of the fact that one of the triad ofsymptoms of colicky pain, distension and absoluteconstipation may often be sufficient to identify it.Vomiting, of course, is late and may merelysignify secondary small intestine distension, be-cause the ileo-caecal valve is no longer functioningefficiently. Alternatively, it may herald the onsetof peritonitis from perforation or strangulation.The most important maxim in dealing with
potential cases of large gut obstruction is, firstly,to suspect it, when a patient has any one symptomof it, and secondly, to keep a close watch until thesuspicion is dispelled or the diagnosis confirmed.Severe abdominal pain without diarrhoea is rarelyof anything but surgical import and timely actionin dealing with it may place a patient in surgicalhands in good time to allow conservative measuresto achieve relief, with subsequent elective surgeryin optimum circumstances.
PathologyLarge gut obstruction occurs for the most part
in elderly patients, the definition of elderly beingin the seventh or eighth decades. This alone is
the most important factor in prognosis, coupledwith the fact that carcinoma of the colon is easilythe commonest cause of the obstruction. Thisimplies that occlusion is common and strangula-tion rare, the latter supervening in volvulus, bandobstruction and rare examples of strangulatedhernia. Umbilical hernia is the commonest ofthese, involving the transverse colon.
Local oedema and faecal impaction above anannular carcinoma of the pelvic colon convert asubacute into an acute obstruction.1 Distensionabove the growth may then result in perfora-tion of the bowel, if the ileo-caecal valve isefficient enough to keep the loop ' closed ' and notallow reflux of gas into the ileum. In these cir-cumstances perforation of the pelvic colon orthinner and more distensible caecum ('pistolshot perforation') may dramatically complicatethe picture, with dire results.
Carcinoma of the right half of the colon is morecommonly papilliferous than annular and obstruc-tion is correspondingly less frequent than on theleft side (I :7) (Morgan).2 Rarely, in fact, is itthe manner in which a patient with such a lesionpresents, whereas 10-15 per cent. of patients witha ring carcinoma of the pelvic colon are first seenwith large bowel obstruction. This may easily beconfused with diverticulitis, though acute obstruc-
copyright. on 30 A
pril 2018 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.31.355.242 on 1 M
ay 1955. Dow
nloaded from