Embed Size (px)
Citation preview

Martin J. Citardi, MD, FACSCleveland Clinic Head & Neck Institute© 2007
The Sublime Beauty of Normal
The Comprehensive Treatment
Of Facial Paralysis
P. Daniel Knott, MD FACSDirector, Facial Plastic andReconstructive SurgeryUCSF Medical Center
November, 2013
Disclosures
• Basal Cell Carcinoma Surgical Advisory Board, Genentech Corp
2
Beauty and Perception Facial Paralysis
• The eye cannot close and constantly weeps. The mout h dribbles, the speech is interfered with and mastica tion impaired. The delicate shades of continence are los t. Joy, happiness, sorrow, shock, surprise, all the emotion s have for their common expression the same blank stare” (Bunnell, 1927)
4

Martin J. Citardi, MD, FACSCleveland Clinic Head & Neck Institute© 2007
Facial Paralysis
• Among most challenging problems in FPRS
• More difficult when reinnervation not possible
– Extensive local tumor resection
– Motor end plate degeneration
– Congenital paralysis (eg Mobius)
Overview
• General approach to assess and manage paralysis
• Surgical Rehabilitation
– Reinnervation
– Treatment
• Upper third
• Middle third
• Lower third
– Emphasis on current advances
Facial Paralysis - Implications
• Facial deformity and loss of expression
• Psychological/socioeconomic effects
• Loss of blink and eye closure, epiphora and ectropion
– Threat of permanent visual loss
• Upper and lateral visual field loss (brow ptosis)
• Loss of oromotor coordination
– Impairment of articulation and eating
– Oral incompetence
• Nasal obstruction
Initial Evaluation
• Condition of the eye
• Swallowing and speech function
– What CNs will be options for reinnervation?
• Function of nearby muscles of mastication
– �i.e. Trigeminal injury (temporalis)

Martin J. Citardi, MD, FACSCleveland Clinic Head & Neck Institute© 2007
Initial Evaluation
• Evaluate facial thirds
– Upper: sclera and cornea, brow position, lower lid, contralateral forehead
– Middle: Position of ala, nasal breathing, melolabial crease, malar fat pad
– Lower: oral competence, lip height, position of lower lip, smile pattern
• Patient ’’’’s age, health, motivation
Indications for Early Intervention/ Consultation
• Absolute
– Threats to ocular health
• Severe ectropion and lagophthalmos
– “BAD” Prognosis
• Bell’s phenomenon: absent
• Anesthesia of the cornea
• Dry eye syndome
– < 5mm Schirmer’s test
Indications for Early Intervention/ Consultation
• Relative
– Known resection/sacrifice/transection
– Severe facial ptosis
• Oral incompetence
• Visual field disturbance
– Severe psychological disturbance
Management Options in Facial Reanimation
1. Observation of spontaneous recovery
8. Contralateral dennervation (eg Botox)
7. Static procedures
6. Free microneurovascular muscle transfer
5. Regional muscle transposition
4. Nerve transposition (reinnervation)
3. Facial nerve cable graft
2. Direct neurroraphy

Martin J. Citardi, MD, FACSCleveland Clinic Head & Neck Institute© 2007
Goals of Reanimation
1. Protection of the eye
2. Facial symmetry at rest - tone and volume distribution
3. Restoration of facial movement
4. Restoration of voluntary facial movement
5. Restoration of Involuntary facial movement
Management of the Eye
• Loss of eye closure
– Loss of blink resulting in loss of conjunctival, scleral, corneal protection
– Corneal drying and irritation
– Loss of lacrimal pump function
• Loss of orbicularis oculi tone
– Ectropion formation
– Epiphora
• Options for protection
– Daytime drops/taping
– Nighttime moisture chamber and ointment
Eyelid Weighting Procedure
• Simple office procedure
• Local anesthesia
• 0.8-1.6 gram gold or platinum implant placed in subcutaneous pocket in the upper lid
• Minimal recovery time
• Immediate improvement of lagopthalmos
• Cosmetically acceptable
• REVERSIBLE
Advantages of Platinum Chain
• You can flatter your patients
• More dense…less noticeable
• Flexes to follow the contour of the globe. . . Less extrusion
• Less reactive. . . Lower need for removal
• Main disadvantage is cost

Martin J. Citardi, MD, FACSCleveland Clinic Head & Neck Institute© 2007
Platinum Chain
Paralytic Ectropion
• Epiphora
• Worsens lagophthalmos
• Severity depends upon inherent laxity of support structures
– Worsened by midface ptosis
– Age dependant
Management of the eye
• Lateral tarsal strip
– Most effective for ectropion – cornerstone
– Local outpatient procedure
– Minimal recovery time
– Immediate benefit
• Reduced epiphora
• Improved cosmesis
• Better eye protection
• Precaruncular medial canthopexy

Martin J. Citardi, MD, FACSCleveland Clinic Head & Neck Institute© 2007
Ectropion Repair - Goals
Lower eyelid at inferior limbus
Lateral canthus slightly above medial
Lid apposes eye along entire length
Inferior punctum sits in tear lake
Punctum not visible without eversion
Ectropion Repair

Martin J. Citardi, MD, FACSCleveland Clinic Head & Neck Institute© 2007
Management of the forehead
• Brow Ptosis
– Loss of visual fields superiorly and peripherally
– Difficulty with eye opening when fatigued
– Aesthetic implications
• Browlifts
– Direct
– Midforehead
– Endoscopic
Direct Brow Lift
Management of the Midface
• Midfacial droop results in numerous aesthetic and functional problems
– Oral commissure droop
• Oral incompetence and drooling
• Articulation problems
– Aesthetic implications
– Lateral nasal collapse: breathing obstruction
– Exacerbation of ectropion

Martin J. Citardi, MD, FACSCleveland Clinic Head & Neck Institute© 2007
Management of the Midface
• Static Suspensions– Static Slings : sutured from oral commisure to
zygomatic arch
• Facelift approach
• Gortex
• Alloderm
– Acceptable results but require signficant dissection and are generally reserved until return of function is ruled out
Reinnervation
• Best option when possible
• Nerve injury
– Repair/grafting within 72hrs
• Nerve resection
– Spanning grafts
– Sources
• Sural
• Great auricular
• Medial antebrachial cutaneous nerve
• Motor nerve to vastus lateralis
• Quality of results undermined by age

Martin J. Citardi, MD, FACSCleveland Clinic Head & Neck Institute© 2007
Reinnervation –When?
• Segmental defect
• Proximal transection – within 1 year
– motor end plate degeneration - after 2 years window may be lost
• Proximal injury without transection – balance between spontaneous recovery and rehabilitation
Timing of injury and intervention
• Electromyography (EMG)
– Recording of muscle potentials by needles in muscle.
– Does not permit quantitative estimate of state of nerve (i.e. percent of degenerated fibers)
– 3 possible outcomes
• Reinnervation occuring: Nascent, polyphasic or voluntary APs
• Persistent denervation: Fibrillation potentials
• Motor end plates degraded: Silence (lost the window)
Nerve Transposition
• Hypoglossal-facial trans.
– Conley J. et al. PRS 1979
– 137 patients
– Full transection of CN 12
– 95% regained tone and movement
– 78% moderate to severe tongue atrophy
– Trade (paralyzed face for slurred speech)
Campero A. et al. J Neurosurg 2007
1 month s/p platinum chainand mid-forehead brow lift,and tarsal strip
15 years s/p left translab for vestibular schwannoma
13 years s/p left hypoglossal-facial nerve transposition

Martin J. Citardi, MD, FACSCleveland Clinic Head & Neck Institute© 2007
Split XII-VII Transfer
• Problem
– Spiral distribution of axons – less predictable results
– Longer length of split = higher risk of both tongue paralysis and suboptimal facial reinnervation
• Improving results
– Maximize VII length with mastoid exposure/mobilization
• Adds about 3cm
• Shortens length of split
• Preferred method
– Disadvantages
• Additional operative time and coordination of services
Hypoglossal-Facial Nerve Transposition
39
Other options for nerve transposition
• Contralateral Facial Nerve
• Spinal Accessory
– Cervical contributions to SCM and Trapezius
– Shoulder dysfunction
• Ansa Hypoglossi/Ansa Cervicalis
– Avoid morbidity of 12/7
• Trigeminal nerves
– Nerve to temporalis
• May interfere with temporalis tendon transfer
– Nerve to Masseter

Martin J. Citardi, MD, FACSCleveland Clinic Head & Neck Institute© 2007
Cross Facial Nerve Grafting
• Usually follows “baby-sitter” graft such as 12/7, or with a gracilis transfer
• Usually reserved for young, motivated patients
• 2 anastomoses made after nerve reinnervation is verified
Lee EI. Cross facial nerve graft: past and present. J plas recon aesth surg 2008
Motor Nerve to Vastus Lateralis
Reinnervation – Cross Facial Nerve Transfer
• One or two staged procedure
• Usually reserved for young, motivated patients
• Contralateral zygomatic/buccal branches with limited power
– Need for 2 anastomoses
• Need for extensive facial rehabilitation
- Ipsilateral masseter nerve provides much greater power
- No need for cross-facial grafting delay or donor nerve deficit
- Minimal morbidity
Masseteric-Facial Nerve Transposition
• Data from gracilis experience applied to patients with intact muscles and distal nerves
• Need to clench jaw to smile
• Spontaneous smile?
• 89% of patients with gracilis to masseter nerve developed spontaneous smiling 1
• Cortical reorganization through rehabilitation is key2
1 Bae YC, Zuker RM, Manktelow RT, Wade S. A comparison of commissure excursion following gracilis muscle transplantation for facial paralysis using a cross-face nerve graft versus the motor nerve to the masseter nerve. Plast Reconstr Surg. Jun 2006;117(7):2407-2413.
2Manktelow RT, Tomat LR, Zuker RM, Chang M. Smile reconstruction in adults with free muscle transfer innervated by the masseter motor nerve: effectiveness and cerebral adaptation. Plast Reconstr Surg. Sep 15 2006;118(4):885-899.

Martin J. Citardi, MD, FACSCleveland Clinic Head & Neck Institute© 2007
Masseteric-Facial Nerve Transposition
Close proximity
Good caliber match
Rapid reinnervation
Minimal morbidity
Masseteric Nerve Transfer
47
Localization: 3 cm anterior to the tragus, 1 cm inferior to the Zygomatic arch
Supplied by Babak Azizzadeh, MD and Vishad Nabili, MD
Reinnervation--Drawbacks
• Synkinesis or mass movement
– Dysregulated reinnervation
• Most common variants
– Lip movement with brow raising
– Eye closure with lip elevation
• Treatment options
– Botox
– Nerve section

Martin J. Citardi, MD, FACSCleveland Clinic Head & Neck Institute© 2007
Management of the Midface
• Dynamic muscle transfer
– Regional muscle transfer
• Temporalis
• Masseter (rarely used)
– Free muscle transfer
• Gracilis, serratus, latissimus, rectus
– Goals of rest symmetry AND voluntary smile
Management of the Midface
• Temporalis muscle transfer– Gilles originally described in 1972
– Requires intact V3
– Traditional regional approach
– Central portion of the temporalis muscle draped over zygoma tacked to the oral commisure
– Provides a resting sling with some possible movement
– Temporal hollowing and zygomatic bulge is limiting factor
• Procedure for symmetry produces asymmetry– Temporal fillers, removal zygomatic arch
Temporalis Muscle Transposition
Cummings, 4th ed, 2005
Tendon Transposition
• Temporalis Tendon Transfer (TTT)
– P. Byrne et al. Arch FPS 2007
– Similar principle as temporalis muscle transfer
– Orthodromic versus antidromic
• Improved vector
• No hollowed temporal fossa or bulge over zygomatic arch
– Immediate dynamic function
– Achieve “Mona Lisa” smile
Martin J. Citardi, MD, FACSCleveland Clinic Head & Neck Institute© 2007
Temporalis Tendon Transposition
• Byrne et al. Archives Facial Plastic Surgery
– Retrospective review 7 patients
– All had single stage TTT
– All had movement at commisure 1.6-8.5mm (mean 4.2mm)
– Satisfaction 8.5/10
– No complications
– No contour deformities
Orthodromic Temporalis Tendon Transfer
• Evolution of technique : 2 approaches
– 1) Transoral/ transfacial
• Oral and nasolabial fold approach
• Reanimation for proximal injury (ie no existing access incisions)
– 2) Transtemporal lateral approach
• In combination with oncologic resection
• Often combined with nerve grafting and free fat/fascia flaps
– Neurovascular pedicles spared (does not affect reinnervation)
– Fascia lata lower lip sling for improved support
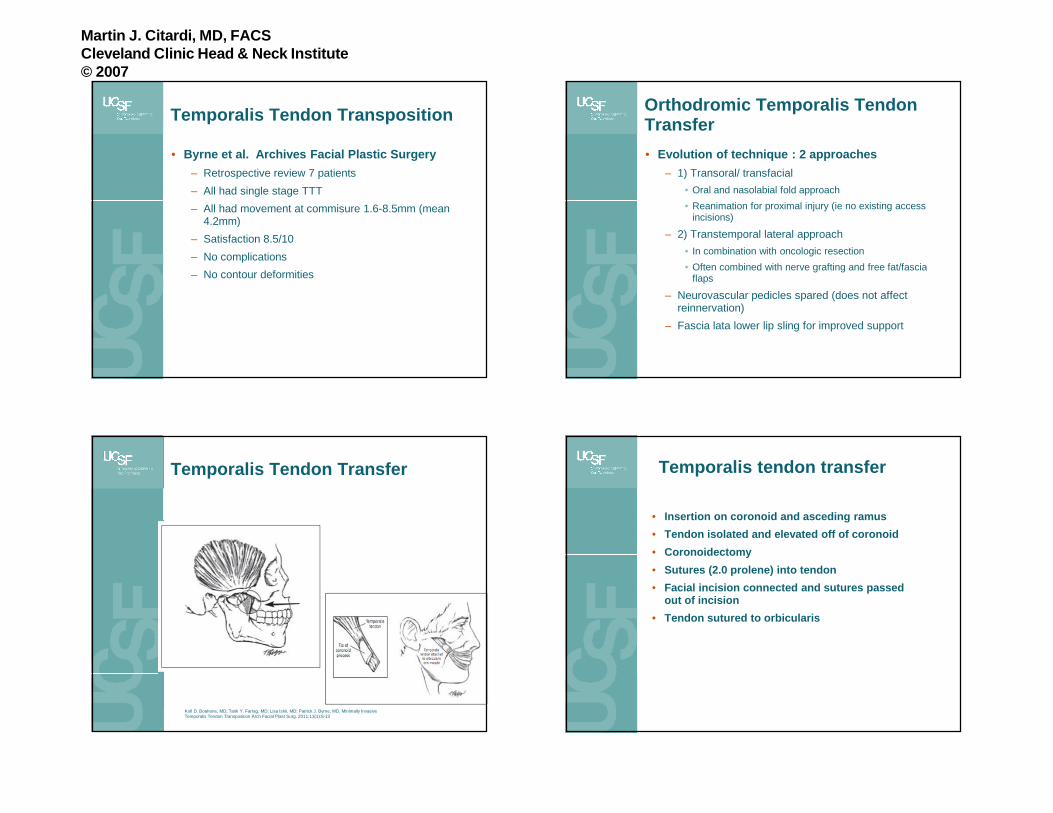
Temporalis Tendon Transfer
Kofi D. Boahene, MD; Tarik Y. Farrag, MD; Lisa Ishii, MD; Patrick J. Byrne, MD, Minimally Invasive Temporalis Tendon Transposition Arch Facial Plast Surg. 2011;13(1):8-13
Temporalis tendon transfer
• Insertion on coronoid and asceding ramus
• Tendon isolated and elevated off of coronoid
• Coronoidectomy
• Sutures (2.0 prolene) into tendon
• Facial incision connected and sutures passed out of incision
• Tendon sutured to orbicularis

Martin J. Citardi, MD, FACSCleveland Clinic Head & Neck Institute© 2007

Martin J. Citardi, MD, FACSCleveland Clinic Head & Neck Institute© 2007
Transoral/ transfacial temporalis tendon transfer
– Single stage outpatient operation
– Only external incision in nasolabial crease
– Movement achieved averages 4 mm of lip excursion
– Facial movement and symmetry is immediate
• Patients wait 2 weeks before aggressive attempts at movement
– No long term morbidity (temporary trismus 2mo)
Lengthening Temporalis Myoplasty
Labbe, Journal of Aesthetic Surgery. 1997

Martin J. Citardi, MD, FACSCleveland Clinic Head & Neck Institute© 2007
Lengthening Temporalis Myoplasty
75
Lengthening Temporalis Myoplasty
• Significant temporal edema for 2 weeks
• Muscle may be “shocked” for several weeks
• Some degree of posterior temporal hollowing
• Voluntary smile may be achieved
• Movement usually approaches 6 mm of upper lip excursion
76

Martin J. Citardi, MD, FACSCleveland Clinic Head & Neck Institute© 2007
Total parotidectomy with facial nerve sacrifice
ALT vascularized fat/fascia graft for contour
Motor nerve to vastus lateralis cable graft
Fascia lata harvest
Temporalis tendon transfer
…then radiation

Martin J. Citardi, MD, FACSCleveland Clinic Head & Neck Institute© 2007
Free Muscle Transfer
• Free vascularized muscle innervated by cross facial or ipsilateral masseteric nerve.
– First described 1982 – muscles used include pec minor, serratus, rectus femoris, gracilis (preferred)
• Chuang 2008
– 249 cases gracilis free muscle transfer 1986-2006
• Cross facial, masseteric, spinal accessory driver nerves
• 70-80% satisfactory results
• When successful results can approach ideal
– Movement usually approaches 1 cm of upper lip excursion
Free Muscle Transfer - Indications
• Decreasing with success of TTT
• Young, highly motivated patients
– No reinnervation potential
• Absence of ipsilateral CN 5 motor function
• Resection of temporalis muscle
Facial Reanimation - Conclusions
• Comprehensive approach can vastly improve appearance and function
• Individualized treatment
• Clear communication and patient education is critical to set appropriate expectations
• No perfect solutions exist at this time