Embed Size (px)
Citation preview

British Journal of Plastic Surgery (1996), 49. 93-96 0 1996 The British Association of Plastic Surgeons
The sternocleidomastoid myocutaneous flap: a reappraisal
P. Yugueros and J. E. Woods
Service of Plastic and Reconstructive Surgery, Mayo Clinic, Rochester MN 5.5905, USA
S UMMAR Y. The sternocleidomastoid myocutaneous flap was described 40 years ago. However, its reliability has been a matter of discussion, mainly because of its random blood supply and subsequent tendency to necrosis. This paper describes the use of the sternocleidomastoid island myocutaneous flap, superiorly based, in 10 patients with good results. In these patients, the superior thyroid artery was sacrificed and the skin paddle was incised directly over the muscle, as described by Ariyan. We believe this approach assures the usefulness of the flap and justifies its expanded utilization.
Among the options for myocutaneous reconstruction in the head and neck is the sternocleidomastoid (SCM) myocutaneous flap. While Owens’ originally described this flap using skin over the entire length of the muscle, Ariyan’ modified the technique exclud- ing the upper two thirds of the skin from the flap and raising it with the lower corresponding skin as a paddle.2 In 1980, Conley and Gullane3 cited many advantages of the sternocleidomastoid osteomuscular flap in reconstructing the mandible. Subsequently, many uses of the SCM flap have been described, which include correction of several varieties of soft tissue defects of the head and neck and other types of reconstruction.2-” Interestingly, in spite of these series with acceptable results this flap has not been widely used, probably because of the significant inci- dence of complications and the limitations of its arc of rotation when two blood vessels are preserved.
This paper re-emphasizes the utility of the SCM myocutaneous flap as a paddle of skin at the end of the pedicle of SCM muscle, with preservation of only one of three vascular pedicles to provide its blood supply, a technique previously addressed by Ariyan.2
Anatomy
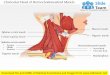
A brief review of the anatomy seems appropriate. The SCM is enveloped by the superficial cervical fascia and overlaid by the platysma. In its middle third, it is crossed by the external jugular vein and overlies the carotid sheath. It is innervated by the accessory nerve which perforates the muscle at the level of the carotid bifurcation.i2
The vascular supply has been elucidated by several methods,i3 which have confirmed previous descrip- tions; branches of the occipital artery penetrate the muscle and reach the overlying skin directly, in an axial way, by cutaneous perforators which supply the platysma and the dermal-subdermal plexus, below the mastoid region or in the superior third.r4 Also, some branches coming from the posterior auricular artery run over the SCM sulcus and reach the dermis
directly. Other branches from the trapezius and strap muscles contribute to the dermal plexus; each branch has its own vascular field and anastomoses widely to feed the dermal plexus completely except for the inferior 3-5 cm. The middle third of the SCM is supplied by the superior thyroid artery, which prob- ably reaches the whole muscle and its overlying skin. The lower third does not have a constant vascular anatomy; most commonly, unnamed branches from the thyrocervical trunk or from the cervicothoracic artery contribute to this lower region. The vascular supply for the skin paddle is provided by myocuta- neous perforators which come directly from the SCM muscle.2,‘3 This description was confirmed by Rabson et al. in cadaver dissections; in those studies, small capillaries were found to reach the skin in a per- pendicular fashion, straight from the underlying muscle.14 The veins;~ in general, follow the course of the arteries.
Types of surgical flaps
The superiorly based SCM flap is by far the most commonly used, because of its constant and well- known vascular supply from the occipital and superior thyroid arteries. Inferiorly based SCM flaps are reserved for lesions arising on the lower neck and/or the superior mediastinum.
The SCM flap is currently used for: reconstruction of the head and neck;4 closure of tracheal or pharyng- oesophageal fistulas;5q6 reconstruction of the oral cavity, including floor of mouth2,7,8 and tongue;’ reconstruction of the mandible;3 correction of facial paralysis;” major vascular neck protection;” and coverage of defects following parotidectomy.‘5,‘6
In this paper, the discussion will focus only on the superiorly based island SCM myocutaneous flap.
Surgical technique
The design of the flap follows an imaginary line which runs over the SCM in the direction of its fibres;
93

94 British Journal of Plastic Surgery
a paddle of skin is incised over the muscle in a distal position so as to allow a maximum arc of rotation.7 Once chosen, the skin paddle is dissected by incising down to the underlying muscle, without cutting it. Then, the flap is freed completely by dissecting the muscle ‘stalk’; at this point the flap is ready to be transferred to the reconstructive site. This flap must be planned using the inversion method to demonstrate if it will readily reach the defect.
Suturing the dermis or underlying soft tissue of the skin paddle to the muscle helps to avoid avulsion during manipulation of the flap.’ The skin per se should not be included in this fixation.’
In the superiorly based flap, for the best arc of rotation, the superior thyroid artery may be ligated if necessary, retaining only the occipital and/or pos- terior auricular arteries.’ While most authors advise preservation of at least two arteries, in this series all flaps were supplied by only one (the occipital artery), but in each instance the skin flap was designed directly over the muscle and not beyond it, following the original concepts by Ariyan7
Occasionally the arc of rotation may be limited by the accessory nerve. l7 Intravenous fluorescein may be used to determine viability of the skin paddle after elevation, though it is not entirely reliable. The use of the SCM myocutaneous flap generally allows easy closure of the donor defect.
Patients and results
The charts of patients with any type of SCM myo- cutaneous flap operated upon by the senior author (JEW) were reviewed, covering a period of 14 years from January 1980. There were no exclusions because of age, and the youngest patient was 21 years old.
The primary pathology of the patients included vascular malformations of the face, facial trauma, parotid tumour and miscellaneous neoplastic lesions of the head and neck (Table 1).
All the SCM myocutaneous flaps were superiorly based. The technique used was similar to that described above and the defect of the donor site in each case was closed primarily. The only modifi- cations from usual descriptions (aside from Ariyan’s) were in the preservation of only one artery and the design of the flap directly over the underlying muscle without extension beyond it.
Ten patients with SCM myocutaneous flaps were analysed (Table 1). Their average age was 52 years. There were 6 females and 4 males. The period of follow-up was from 1 month to 9 years. Infectious complications of the procedure were minimal; one patient developed abscess formation with subsequent skin necrosis in a previously viable flap. There was another mild infection which responded to antibiotics and local wound hygiene without skin loss.
Another patient underwent partial necrosis of the skin and, in association with it, an orocutaneous fistula. Subsequent skin grafting was required. There were no other significant complications aside from minor skin separation.
There were no deaths in the series. Most signifi-

The sternocleidomastoid myocutaneous flap 95
Table 2 Comparison of series using SCM myocutaneous flap*
Ariyan ( 1979)2 9 Oral cavity-mmoropharynx 4 9 Charles et al. ( 1987)” 27 Oral cavity 3 27 Tiwari ( 1990)17 9 3 6 Pharyngocutaneous fistula Present series ( 1995) 10 Miscellaneous -face 2 9
*Only included superiorly based, skin island flaps. ** Most of the cases had partial epithelial loss.
cantly, there was no skin necrosis except in the presence of other complicating factors, e.g. infection or fistula.
Discussion
In spite of many reports about the SCM myocuta- neous flap, it has apparently not been widely used. This is probably because of its perceived unreliability on the basis of the rather tenuous attachments and blood supply to the overlying skin.18 However, credit must be given to Ariyan, who described the modifi- cations used here more than 15 years ago.237
After the studies of Bocca and Pignataro,” mod- ifying radical neck dissection to allow the sparing of the SCM, and with the increasing use of modified neck dissection, the use of the SCM myocutaneous flap is not considered oncologically compromis- ing except when involved directly with invasive malignancy.
Only two cases of necrosis of the skin were found in ten SCM myocutaneous flaps, one only after infection in an otherwise viable flap and the other in connection with an orocutaneous fistula. It has been said that the supply of the skin is random, and that necrosis is an expected complication. Some authors have advocated the incorporation of the fascia to the muscle to avoid ischaemia.*’ However, when the skin is taken immediately over the muscle, preserving the subdermal plexus, this complication is much less likely. 2,7 This anatomical concept was demonstrated by Rabson et al. in cadaver studiesI
Larson and Goepfert questioned the reliability of the SCM flap.‘* They also mentioned the limited arc of rotation occasioned by the accessory nerve and this is a limiting factor, as is limiting the skin paddle design to be entirely over the muscle. In our series, however, the flaps were utilized to repair distant defects, without tension of the skin or necrosis except in the presence of other complicating factors.
Alvarez et al. described the splitting of the flap to avoid a flat neck deformity.*r This technique was utilized in one patient in our series, with initial cyanosis of the flap but subsequent complete survival.
Many anatomical studies support the reliability of the superiorly based SCM flap, supplied by the occipi- tal and the superior thyroid artery. In this series, however, the superior thyroid artery was not pre- served, as Ariyan suggested,’ and the viability of the flap did not appear to be ,compromised. In our opinion, the success of the flap supplied by only one
vessel depends on placement of the skin paddle directly over the nzuscle.2~7
In this series of ten patients, use of the superiorly based SCM myocutaneous flap appears to be justified as suggested by other publications.2*7.‘7,22*z3 Table 2 summarises the published series on this flap used with a skin paddle.
Finally, to reiterate the key points in planning a superiorly based SCM myocutaneous flap. The arc of rotation is theoretically limited by the accessory nerve, which should be preserved whenever possible for optimal function. This limits its use in distant coverage on occasions as does limiting the placement of the skin paddle to be directly over the muscle. This, however, provides greater reliability in our opinion.
The sacrifice of the superior thyroid artery has not occasioned significant problems when the flap is designed as in this series and as previously outlined by Ariyan.
We believe this experience supports its wider use.
References
I. Owens NA. Compound neck pedicle designed for the repair of massive facial defects: development, and application. Plast Reconstr Surg 1955; 15: 369-89.
2. Ariyan S. One-stage reconstruction for defects of the mouth using a sternoomastoid myocutaneous flap. Plast Reconstr Surg 1979; 63: 618-20.
3. Conley J, Gullane PJ. The sternocleidomastoid muscle flap. Head Neck Surg 1980; 2: 308 I 1.
4. Hill HL, Brown RG. The sternocleidomastoid flap to restore facial contour in mandibular reconstruction. Br J Plast Surg 1978: 31: 14336.
5. Friedman M, Mayer AD. Laryngotracheal reconstruction in adults with the sternocleidomastoid myoperiosteal flap. Ann Otol Rhino1 Larvnrol 1992: 101: 8977908.
6. Friedman M, Toriymi b, Strorigl T, et al. The sternocleidomas- toid myoperiosteal flap in esophagopharyngeal reconstruc- tion and tistula repair: clinical and experimental study. Laryngoscope 1988; 98: 1084491.
7. Ariyan S. The sternocleidomastoid myocutaneous flap. Laryngoscope 1980; 90: 67669.
8. Sasaki CT. The sternocleidomastoid myocutaneous flap. Arch Otolaryngol 1980; 106: 74-6.
9. Mikaelian DO. Reconstruction of the tongue. Laryngoscope 1984; 94: 34-l.
10. Jianu J. Paralizac faciale dupa extirparea unei tumori a paroti- dei, tratata prin operatia. Olui Gomoiu Sot de Chir de Bucharest, 22 December, 1908.
Il. Shindo ML, Sullivan MJ. Muscular and myocutaneous pedicle flaps. Otolaryngol Clin North Am 1994; 27: 161-71.
12. Marx RE, McDonald DK. The sternocleidomastoid muscle as a muscular or myocutaneous flap for oral and facial recon- struction J Oral Maxillofac Surg 1985; 43: 155562.
13. Jabaley ME, Heckler FR, Wallace WH. Knott LH.

96 British Journal of Plastic Surgery
Sternocleidomastoid regional flaps: a new look at an old concept. Br J Plast Surg 1979; 32: 106613.
14. Rabson JA, Hurwitz DJ, Futrell JW. The cutaneous blood supply of the neck: relevance to incision planning and surgical reconstruction. Br J Plast Surg 1985; 38: 208-19.
15. Bugis SP, Young JE, Archibald SD. Sternocleidomastoid flap following parotidectomy. Head Neck Surg 1990; 12: 430-5.
16. Kornblut AD, Westphal P, Miehlke A. The effectiveness of a sternocleidomastoid muscle flap in preventing post- parotidectomy occurrence of the Frey syndrome. Acta Otolaryngol 1974; 77: 368-73.
17. Tiwari R. Experiences with the sternocleidomastoid muscle and myocutaneous flap. J Laryngol Otol 1990; 104: 3 15-2 1.
18. Larson DL, Goepfert H. Limitations of the sternocleidomas- toid musculocutaneous flap in head and neck cancer recon- struction. Plast Reconstr Surg 1982; 70: 328-35.
19. Bocca E, Pignataro 0. A conservation technique in radical neck dissection. Ann Otol Rhino1 Laryngol 1967; 76: 957788.
20. Alvi A, Stegnjajic A. Sternocleidomastoid myofascial flap for head and neck reconstruction, Head Neck Surg 1994; 16: 326630.
2 1. Alvarez GE, Escamilla JT, Carranza A. The split sternocleido- mastoid myocutaneous flap. Br J Plast Surg 1983; 36: 183-6.
22. Charles GA, Hamaker RC, Singer MI. Sternocleidomastoid myocutaneous flap. Laryngoscope 1987; 97: 970-4.
23. Golabek W, Kondratowicz J. Sternocleidomastoid myocuta- neous flap for intraoral reconstruction. Eur Arch Otorhinolaryngol 1990; 24: 379-81.
The Authors
Patricia Yugueros MD, Research Fellow John E. Woods MD, PhD, FACS, Emeritus Professor
Service of Plastic and Reconstructive Surgery, Mayo Clinic, 200 First Street SW, Rochester, Minnesota, USA.
Correspondence to: John E. Woods, MD, PhD, Service of Plastic and Reconstructive Surgery, Mayo Clinic, 200 First Street SW, Rochester, MN 55905, USA.
Paper received 3 May 1995. Accepted 12 September 1995, after revision.