Embed Size (px)
Citation preview

The Science and Practice of LSVT BIG
Robert B. Leavitt PT, MPT, OCS, JSCC, LSVT cert.
VP Operations OSPTPh: 707-571-7615osptclinic.com
Copyright LSVT Global, Inc. 2011
www.lsvtglobal.com

Objectives Explain advances in neuroscience and impact on the
field of rehabilitation
Briefly discuss development and data on an efficacious speech treatment LSVT LOUD
Describe development and key aspects of limb motor treatment LSVT BIG
Introduce the LSVT HYBRID approach (simultaneous delivery of BIG and LOUD)
Copyright LSVT Global, Inc. 2011

It is an exciting time to be in rehabilitation today!
Basic science evidence for the value of exercise in PD (classically drugs, surgery, today…)
Identified key principles of exercise that drive activity-dependent neural plasticity
Demonstrated that exercise can improve brain functioning (neural plasticity) and may slow disease progression
Exercise is Medicine! Kliem & Jones, 2008; Ludlow et al, 2008
Copyright LSVT Global, Inc. 2011

Legitimate Therapeutic OptionsTo provide symptomatic relief; improve function
Pharmacological(L-dopa)
Voice and Body Exercise
Neurosurgical(DBS-STN)
Zigmond et al, 2009Copyright LSVT Global, Inc. 2011

“If only we can hear and understand her” Family of Mrs. Lee Silverman 1987

5 Stages of Grief
Denial - “There must be some mistake!”Anger – “I sure got shafted this time.”Bargaining – “There must be a cure.”Depression – “This is hopeless.”Acceptance – “ I can deal with this.”
These stages must be worked through before any meaningful process can begin.
Source: On Death and Dying. Elizabeth Kubler-Ross

20+ year journey from invention to intervention Over 8 million dollars in NIH funding
1987-89: Initial invention; Pilot data (Scottsdale)1989-91: Office of Education OE-NIDRR
1991-94: OE-NIDRR1990-95: NIH funded RCT Efficacy1995-00: NIH funded EMG, Kinematics2002-07: NIH funded RCT Spread of effects2007-12: NIH funded RCT, imaging
2001-02: Coleman Institute (PDA; LSVTC)2002-04: NIH and M J FOX Foundation PDA (R21)2002-04: Coleman Institute (VT; LSVTVT)2004-06: NIH LSVTVT (R21)2004 : Coleman Institute (LSVT Down Syndrome) 2004-07: LSVT –Dissemination2006: Technology-enhanced Clinician Training (SBIR)2010: Technology-enhanced LSVT LOUD delivery (SBIR)
Ph
ase
I, II
Ph
ase
III
Ph
ase
IV, V
Copyright LSVT Global, Inc. 2011

Administered in an intensive manner to
to challenge the impaired system.
Techniques specific to PD-specific deficits!bradykinesia/hypokinesia
and kinesthetic awareness
(sensory deficit)
LSVT Programs
Copyright LSVT Global, Inc. 2011

SOFT
LOUD
HEALTHY LOUDNESSNeural coupling (McClean and Tasko)
Loud is more than a laryngeal event – spread of effects
TARGET of LSVT LOUD

sensory
problem,
internal cueing
LearningCALIBRATION

Imaging Studies with LSVT LOUD
Liotti, Ramig, et al, 2003
Copyright LSVT Global, Inc. 2011

LSVT LOUD LSVT BIG
(Farley & Koshland, 2005; Farley, Fox, et al., 2008; Farley & Koshland, in revision)

What are the fundamentals of LSVT BIG?
TARGET: Bigness (amplitude)
MODE: Intensive and High Effort
CALIBRATION: GeneralizationSensoryInternal cueingNeuropsychological changes
Standardized, research-based, specific protocol
Copyright LSVT Global, Inc. 2011

BIG (Large amplitude whole body movement)Single Target - Triggers Activation across motor systems
SMALLBIG
NORMAL “BIGNESS“
TARGET

Delivery– Certified LSVT BIG Physical/Occupational Therapist
• 1:1 intervention
Time of Practice– 4 consecutive days per week for 4 weeks
– 16 sessions in one month
– 60 minute sessions
– Daily carryover assignments (30 days/entire month)
– Daily homework (30 days/entire month)
MODE
Copyright LSVT Global, Inc. 2011

MISMATCH between self-perception of output and how others perceive it
“I had no idea how small my world had become”
“I can’t move like this, people will think I am crazy!!”
CALIBRATION

Retrain sensory
calibration and learn
new internal cues for
normal movement effort and
bigness
CALIBRATION
Learning
Copyright LSVT Global, Inc. 2011

Impairedself-perception
Small movements
reducedamplitude of output
Deficits in internal cues

Increase Bigness
increaseamplitude of output
Self-perception,Internal cues,
Simple, Redundant
ModeIntensive, High effort(consistent with principles of neural
plasticity)
TargetCalibration
Goal of LSVT BIG

Treatment SessionDaily Exercises1.Floor to Ceiling 2.Side to Side 3.Forward step 4.Sideways step 5.Backward step 6.Forward Rock and Reach 7.Sideways Rock and Reach
Functional Component Tasks
5 EVERYDAY TASKS– 5 reps each For Example:
-Sit-to-Stand
-Pulling keys out of pocket
-Opening refrigerator door
Walking BIG distance/time may vary
Hierarchy TasksPatient identified tasks:
Getting out of bed
Playing golf
In and out of a car
Build complexity across 4 weeks of treatment towards long term goals
Copyright LSVT Global, Inc. 2011

Daily Whole-body Maximal Amplitude Exercises Multidirectional Sustained Movements
Floor to Ceiling Side to Side
Copyright LSVT Global, Inc. 2011

Daily Whole-body Maximal Amplitude Exercises
Multidirectional Repetitive Movements
Forwards
SidewaysBackwards
Copyright LSVT Global, Inc. 2011

Rolling
Floor to Stand
Getting in or out of bed
Sit to stand
Sit & reach
Stand & reach
Walk & reach
Walk & turn
Stand & turn
Functional Component TASKS
Functional Components – Patient DRIVEN!
Sit to stand BIG
Copyright LSVT Global, Inc. 2011

Daily Hierarchical Tasks
“Real-World” BIG Tasks – Patient DRIVEN!
Examples:
Bed to BathroomIn/Out of CarWalk and TalkTennisChoresGolfHikingGardening
Copyright LSVT Global, Inc. 2011

Patient case: Bernie• 71 year-old, diagnosed with Parkinson’s disease
in 1994
• Reason for referral: slowness and difficulty walking, history of falls, freezing
• Optimized on PD medications
Copyright LSVT Global, Inc. 2011
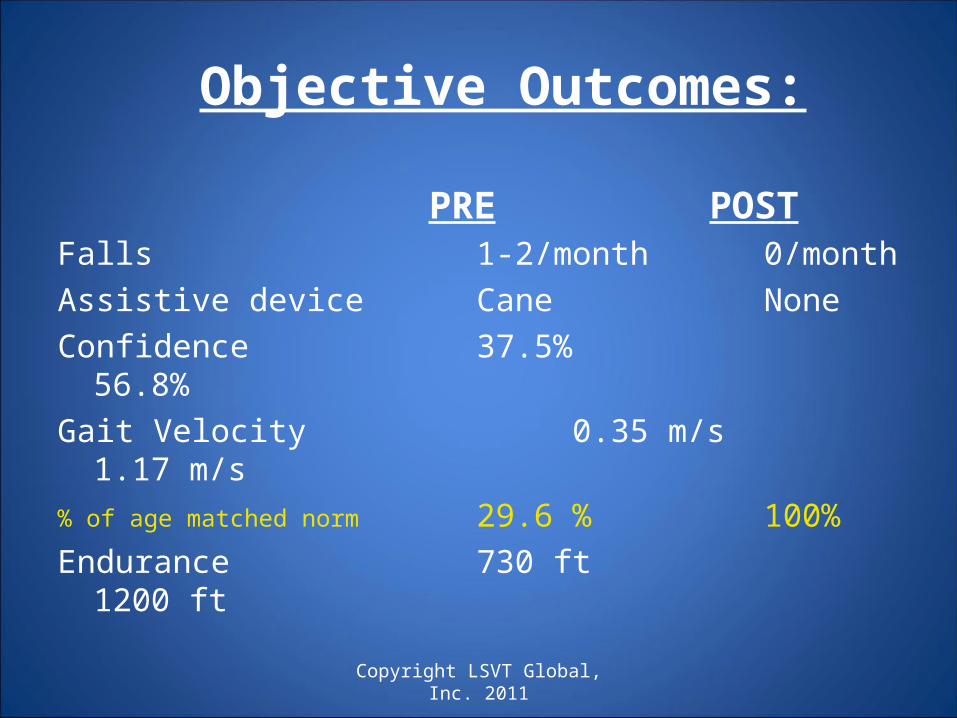
Objective Outcomes:
Falls 1-2/month 0/month
Assistive device Cane None
Confidence 37.5% 56.8%
Gait Velocity 0.35 m/s 1.17 m/s
% of age matched norm 29.6 % 100%
Endurance 730 ft 1200 ft
PRE POST
Copyright LSVT Global, Inc. 2011

Bernie’s Goals
To improve his walkingTo go to the moviesTo play with his grandchildrenTo go out to dinner with friends and family
All accomplished to his satisfaction!
Copyright LSVT Global, Inc. 2011

Randomized Comparative Pilot StudyMatched Frequency/Duration
4X/week for 4 weeks; 1-hour individual sessionsN=42
Hoehn & Yahr 1-3
Intention to treat analysisFarley & Koshland, in preparation (Unpublished data)
LSVT BIG vs.
Traditional Outpatient Physical Therapy

Walking Improvements
Farley & Koshland, in preparation (Unpublished data)
Improvements occurred in both groups and lasted 3 months.
TRAD
BIG
Faster Bigger
3-months 3-months1-month 1-month
Copyright LSVT Global, Inc. 2011

Trunk Rotation
Farley & Koshland, in preparation (Unpublished data)
Only improved for LSVT BIG
TRAD
BIG
3-months1-month
Copyright LSVT Global, Inc. 2011

• Activity Matters
• LSVT BIG may be especially important for trunk rotation and balance - everyday
movements
Conclusions:

Principles of LSVT applied simultaneously to the
speech and limb motor systems.
Combined or “Hybrid” approach for PD May promote greater plasticity through greater intensity,
complexity, saliency Enhance practical, logistical, financial costs of PD
rehabilitation
LSVT HYBRID = LOUD + BIG
Copyright LSVT Global, Inc. 2011

LSVT HYBRID retrains “normal use”
“In my normal everyday life, I just exaggerate my movements.
I keep things Big when I reach for things,
or when I bend or when I walk; and when I talk –
I keep my voice strong.” Copyright LSVT Global, Inc. 2011

SummaryAdvances in neuroscience have provided
neurobiological and behavioral evidence supporting the positive impact of exercise-based protocols in people
with PD
There is a rapidly growing literature in physical therapy/exercise protocols in humans with PD
LSVT Programs have been developed and studied over the past 20 years
LSVT BIG is one type of physical therapy program that has potential to offer improvements in movement and
quality of life for people with PD
Copyright LSVT Global, Inc. 2011

“It is possible to take charge of your life, even with Parkinson’s.
It is possible for your will to override your brain.
It is possible to have Power Over Parkinson’s”
Sharon Kha, LSVT BIG and LSVT LOUD Graduate

“Fear is an emotional “germ” that will destroy the spirit. Filling your brain with “I can thoughts” will turn fear away”
“No matter what the reason for it, inactivity is unhealthy. The less active we are the weaker we become and the more likely we are to develop obesity, osteoporosis, diabetes, and heart disease.”
Source: Take Charge of Your Chronic Pain. Peter Abaci, MD. Globe Pequot Press.

Thank you for your attention!
Presented by Robert B. Leavitt PT, MPT, OCS, JSCC
VP Operations OSPT795 Farmers Lane
Santa Rosa, CA 95405Ph: 707-571-7615
osptclinic.com
More info available at
www.lsvtglobal.com

Lee Silverman Voice Therapy: Lee Silverman Voice Therapy: Rehabilitative Therapy for People with Rehabilitative Therapy for People with
Parkinson’sParkinson’s
Parkinson’s Support GroupJanuary 19th, 2013
Oakmont
Santa Rosa, CA
Presented by:
Dr. Deborah Swain, Ed. D, CCC-SLP
The Swain Center
795 Farmers Lane, Suite 23
Santa Rosa, CA 95405
(707) 575-1468
www.theswaincenter.com

Lee Silverman Voice Therapy Lee Silverman Voice Therapy (LSVT®)(LSVT®) IntroductionIntroduction
• The LSVT® LOUD improves both the voice and speech of individuals with Parkinson’s Disease by treating the underlying physical pathology associated with the disordered voice
• Treatment focuses on improving vocal loudness and immediate carryover into daily communication enabling patients to maintain and/or improve their oral communication
• The LSVT® LOUD is administered on an intensive schedule of 16 individual, 60-minute sessions in one month’s time

LSVT® IntroductionLSVT® Introduction• 90% of patients improve vocal loudness
from pre to post-treatment• Approximately 80% of patients maintain
treatment improvements in their voice for 12-24 months post-treatment
• ALL patients report improvement in their ability to communicate
• LSVT® LOUD is being successfully delivered by over 4,000 certified LSVT®® clinicians in 41 countries

Goal of LSVT®Goal of LSVT®
• Patient uses his or her voice “automatically” in daily communication
• There is a carryover of this information for the long term

Need for LSVT® LOUDNeed for LSVT® LOUD
• Few patients with motor speech disorders receive treatment with well-documented efficacy– 89% of patients with Parkinson’s Disease
have disordered speech (Logemann et al, 1978)
– But only 4% of those individuals receive treatment (Mutch et al, 1986; Hartelius & Sveenson, 1994)

Why Treat Phonation in Why Treat Phonation in Neurological Disorders?Neurological Disorders?
• Motor speech disorders accompanying neurological disorders limit functional oral communication
• Oral communication is a vital element in:– Education– Employment– Social functioning– Self expression
• Treatment of one area of speech enhances many levels of speech production– Improves capability of treatment– Simplifies treatment

LSVT® LOUD as a TriggerLSVT® LOUD as a Trigger• Improves articulation
• Enhances “source” of speech– Turns up the volume– Improves vocal fold movements
• Acts as a trigger– Vocal tract effects
• Reduces spread of effects

Speech Behaviors in Speech Behaviors in Parkinson’s DiseaseParkinson’s Disease
• Reduced volume of speech is a key factor in Parkinson’s Disease– Patients can sometimes feel like they are
shouting to be heard
• Voice must be stimulated in order to successfully increase loudness and enable speech to be heard

Soft Voice LoopSoft Voice Loop

Origins of Speech Disorders Origins of Speech Disorders in Parkinson’s Diseasein Parkinson’s Disease
• Motor challenges
• Sensory challenges
• Neuropsychological (cueing) challenges

Neuropsychological ChallengesNeuropsychological Challenges
• Internally vs. Externally Cued Movements– Parkinson’s Disease results in patients being
unable to self-initiate speech– Deficits in self-initiated movements are due to
an under-activation of Sensory Motor Areas

Perceptual CharacteristicsPerceptual Characteristics
• Reduced loudness
• Hoarse voice quality• Monotone• Imprecise articulation• Vocal tremors
– Some patients report reduced volume, a hoarse voice or being monotone as the first symptom on Parkinson’s Disease
• Lowering of functional oral communication– Less likely to participate in conversations or have
confidence in their voice (Fox and Ramig, 1997)

LSVT® LOUD ImpactLSVT® LOUD Impact
• Some responses from LSVT® LSVT® LOUD participants:LOUD participants:– “My voice is alive again”
– “I can talk to my grandchildren!”
– “I feel like my old self”
– “I am confident I can communicate!”

LSVT® LOUD MethodsLSVT® LOUD Methods• Assessment
– Separate from 16 sessions of LSVT® LOUD LSVT® LOUD
• OverviewOverview– 4 days a week for 4 weeks (16 sessions in 1 month)4 days a week for 4 weeks (16 sessions in 1 month)
– 50-60 minute sessions50-60 minute sessions
• Integration of five essential conceptsIntegration of five essential concepts– All focus on All focus on voicevoice
– All are All are high efforthigh effort
– All are completed All are completed dailydaily
– All are tools for All are tools for calibrationcalibration
– All are All are quantifiedquantified

LSVT® LOUD DesignLSVT® LOUD Design• Designed to allow a patient to
consistently progress to desired functional speech level
• Designed to help a patient build their ability and reduce frustration
• Designed to bring voice rescaling back into speech
• Both vocal loudness level and calibration are addressed in this hierarchy

Voice Training with LSVT® Voice Training with LSVT® LOUDLOUD
• Maximize phonatory efficiency by increasing loudness – KEY
• Rescale phonatory loudness and effort
• Voice is #1 priority• Keep it simple
LSVT® LOUD Work at HomeLSVT® LOUD Work at Home• Designed to:
– Provide additional practice– Enable patient to become comfortable with the
use of a high vocal effort– Establish a routine schedule of practice at
home• “Brush your teeth – do your ‘Ah’s”
• Methods:– 5 – 10 minutes one other time on treatment
days– 10-15 minutes twice daily on non-treatment
days

LSVT® LOUD Post-Treatment LSVT® LOUD Post-Treatment ModelModel
• Practice at home• Complete treatment tasks• LSVT® LOUD Homework Helper can be LSVT® LOUD Homework Helper can be
used at homeused at home• Six months post-treatment:Six months post-treatment:
– Check-in with clinicianCheck-in with clinician– More severe patients may check in earlier More severe patients may check in earlier
(around two months)(around two months)• Patients may end up needing:Patients may end up needing:
– One or two “tune-up sessions”One or two “tune-up sessions”– Enhanced motivationEnhanced motivation– Calibration rescalingCalibration rescaling

LOUD CrowdLOUD Crowd
• Following completion of the 4-week program each patient enters the maintenance phase of the Northern California Voice Project’s program and becomes a member of the “LOUD Crowd.”
• Meets the challenge of maintaining the speech and swallowing gains attained from the intensive Lee Silverman Voice Therapy program.
• Loud Crowd provides support, encouragement, and continued care from a certified speech-language pathologist.
• Patients who participate in continued voice maintenance have been shown to maintain their improved voices for more than five years.

LSVT® LOUD Model for LSVT® LOUD Model for Treatment of Individuals with Treatment of Individuals with
Parkinson’s DiseaseParkinson’s Disease

LSVT® LOUD Model for LSVT® LOUD Model for Treatment of Individuals with Treatment of Individuals with
Parkinson’s DiseaseParkinson’s Disease

Changes in Vocal Loudness in Individuals Changes in Vocal Loudness in Individuals with Parkinson's Disease Following LSVT®with Parkinson's Disease Following LSVT®
• Ramig, Sapir, et al. (2001)– This study assessed the impact of the Lee Silverman Voice
Treatment (LSVT®) on vocal loudness (Sound Pressure Level – SPL) in a group of individuals with Parkinson's disease
– The individuals treated with LSVT® increased voice vocal loudness (SPL) from by an average of 8 decibels (dB) and from baseline to 6 months follow-up by an average of 6 dB
• These changes were statistically significant and perceptibly audible
– Treated patients showed a significant increase in vocal loudness (SPL); this was statistically significant for all voice and speech tasks
• These findings, along with others, provide additional support for the efficacy of the LSVT®

Questions & CommentsQuestions & Comments





























